")
Back to Journals » Vascular Health and Risk Management » Volume 15
Screening of peripheral arterial disease in primary health care
Authors Tóth-Vajna Z , Tóth-Vajna G , Gombos Z, Szilágyi B, Járai Z, Berczeli M, Sótonyi P
Received 11 March 2019
Accepted for publication 1 July 2019
Published 20 August 2019 Volume 2019:15 Pages 355—363
DOI https://doi.org/10.2147/VHRM.S208302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Zsombor Tóth-Vajna,1 Gergely Tóth-Vajna,2 Zsuzsanna Gombos,1 Brigitta Szilágyi,3 Zoltán Járai,4,5 Márton Berczeli,1 Péter Sótonyi1
1Heart and Vascular Center, Department of Vascular Surgery, Semmelweis University, Budapest, Hungary; 21st Department of Pediatrics, Semmelweis University, Budapest, Hungary; 3Department of Geometry, Institute of Mathematics, Budapest University of Technology and Economics, Budapest, Hungary; 4Department of Cardiology, St. Emeric University Teaching Hospital, Budapest, Hungary; 5Heart and Vascular Center, Department of Vascular Surgery, Department of Angiology, Semmelweis University, Budapest, Hungary
Correspondence: Márton Berczeli
Heart and Vascular Center, Department of Vascular Surgery, Semmelweis University, 68 Városmajor Street, Budapest 1122, Hungary
Tel +36 20 666 3354
Email [email protected]
Background and purpose: The screening tool for diagnosing lower extremity arterial disease is the assessment of the ankle-brachial index (ABI), which is widely used in general practice. However, resting ABI can easily produce a false negative result. In light of this, our goal was to determine the proportion of definitive diagnoses (peripheral arterial disease [PAD] confirmed or refuted) among patients screened in general practice, and the rate of cases in which the need for further specialized examination is necessary, with special attention to groups having non-compressible arteries and ABI negative symptomatic status. The aim of our work is to improve the efficiency of primary health care screening in PAD and reduce the extremely high domestic amputation ratio.
Patients and methods: Eight hundred and sixteen patients were screened. We used the Edinburgh Questionnaire and recorded medical histories, major risk factors, current complaints, and medication. Physical examinations were performed, including ABI testing.
Results: Thirty-three percent complained about lower extremity claudication; 23% had abnormal ABI values; 13% of the patients within the normal ABI range had complaints of dysbasia; and 12% were in the non-compressible artery group. The ABI-negative symptomatic group’s risk factor profile showed a close similarity to the clear PAD-positive and non-compressible artery groups.
Conclusion: The percentage of PAD could be higher than the number of patients diagnosed by ABI screening. Nearly a quarter of the population fell into the non-compressible artery and ABI-negative symptomatic groups, together defined as the “murky zone”. When screening purposely for PAD, these patients deserve special attention due to the insufficient selectivity and sensitivity of measurements. If there is high clinical suspicion of PAD in spite of normal ABI values, further assessment may be considered.
Keywords: peripheral arterial disease, ankle-brachial index, diabetes, screening method, ABI-negative symptomatic, non-compressible artery
Introduction
Cardiovascular diseases (CVDs) are a leading cause of death in Europe.
Early recognition of lower extremity peripheral arterial disease (PAD) is of crucial importance, as patients with vascular diseases are at 2–4 times the risk of a future cardiovascular or cerebrovascular event.1–3 Early recognition and adequate treatment significantly decrease associated risks and mortality.4
Lower extremity PAD is a common disease. Among the age 55+ demographic, its prevalence increases exponentially; for ages 65 and above, prevalence can be as high as 20%.1,6 The majority of patients is asymptomatic, and remains undiscovered without special screening.1,4
The largest Hungarian epidemiological study in this field was the ÉRV Programme which estimated the prevalence of lower limb PAD to be at 14.4% among hypertensive patients.7
The most important risk factors of lower extremity PAD are: smoking, diabetes mellitus, dyslipidemia, hypertension, and aging.4
In Hungary, major amputations are estimated at triple the international average, one of the causes being the late recognition of lower limb PAD.8
The dual purpose of our study was to measure the prevalence and severity of lower extremity PAD and to develop a low-cost, complex screening method for general practitioners (GPs) that is easy to perform, requires few instruments, and may quickly yet accurately identify both PAD patients and at-risk patients, thus promoting early disease recognition. We decided to define the characteristics of two specific groups particularly difficult to diagnose at GP level. One such group is where the ankle-brachial index (ABI) shows normal or borderline values, but the Edinburgh Questionnaire (ECQ) clearly suggests lower limb PAD (we refer to this group as “ABI-negative symptomatic”); the second group consists of those who suffer from identifiable atherosclerosis, but the hardening of their arterial walls results in false high ABI values, making evaluation impossible. This population is referred to as the “non-compressible artery group”.
Participants and methods
Our study took place between November 2015 and April 2017, with 816 participants from 33 GP practices. The participation of GPs was voluntary.
We advertised the screening one month prior to the examination at GP offices, randomly chosen from the capital, major cities, and small villages.9 The target demographic included men and women aged 50+. We screened every patient aged 50–65 with at least one major vascular risk factor or CV events in their personal or family medical history, as well as everyone aged 65 and above. All participants received a written informed consent before involvement in the study. Everyone signed and agreed the participants’ consent, which was performed according to the Helsinki Declaration. Our study has been approved by all the authors and the Research Ethics Committee of the Semmelweis University (285/2015).
We began the examination by completing the Edinburgh Claudication Questionnaire (ECQ), a validated and frequently used method of screening for intermittent claudication (IC).10
We recorded the patient’s medical history, any CV events in their family’s medical history, any currently prescribed medications, as well as the details of major risk factors (smoking, diabetes, hypertension, or hyperlipidemia).
Figure 1 shows us the screening method and algorithm that we used.
 |
Figure 1 Screening procedure algorithm. Abbreviation: ABI, ankle-brachial index. |
Basic body measurements (height, weight) as well as serum glucose and cholesterol-level measurements with test strips were performed. After a 5-mins rest, we measured blood pressure and pulse rate on both upper extremities (blood pressure manometer, Bosch Konstante). In accordance with current guidelines, a continuous wave Doppler-US instrument (8 MHz; MultiDOPPY) was used to measure systolic blood pressure in all four extremities, and ankle-branchial index (ABI) was calculated from the pressure values.1,11
We performed a walking test for patients whose ECQ revealed IC complaints. They had to walk along a precisely measured course at normal walking pace, while we registered various data. We recorded if the pain occurred before or after walking 200 meters. These data were used for Fontaine-stage classification. Patients walked for 6 mins at most (for calculating a 6-mins walking distance). We determined pain-free walking distance (the distance at which lower limb pain first occurred) as well as maximum walking distance (the distance at which the pain forced the patient to stop).
In patients with lower extremity symptoms, additional examinations were performed to differentiate the origin of the pain.
Mean values and percentages were calculated in cases of continuous and categorical variables, respectively. Group differences were compared using the Fisher’s exact test for categorical variables, two-samples t-test (where the homogeneity of variances and the similar sample sizes made it possible), and unequal variances t-test for continuous variables.
Results
Total population data
The screened population’s baseline parameters are shown in Table 1. More than half (62%) of the participants at our screenings were women. Patients were mainly from the elderly age group, average age being 65.6±7.9 years. The most frequent vascular risk factor was hypertension at 77%, followed by hyperlipidemia (55%), diabetes (33%), and active smoking (24%). Based on the ECQ, a significant percentage (33%) of the total population had IC complaints.
 |
Table 1 Baseline parameters |
Patients with negative at-rest ABI results and no symptoms indicating sclerosis were classified as clear PAD-negative. Patients with normal at-rest ABI results but whose ECQ results revealed symptoms of IC were classified as ABI-negative symptomatic.
The clear PAD-positive group comprises patients whose ABI results were positive, and clearly suffer from atherosclerosis, the asymptomatic or symptomatic stenosis or occlusion reducing blood flow. Patients whose major arteries are hardened (such as hardening caused by medial sclerosis) have non-compressible arteries. Due to this, blood pressure values at the ankle often show false high values, and the ABI is over 1.4. This category is referred to as the non-compressible artery group.
We named the clear PAD-positive and the clear PAD-negative groups the “light zone”, because, using our screening method, these patients can be diagnosed with great confidence by primary care practitioners. On the other hand, the ABI-negative symptomatic and the non-compressible artery groups are called the “murky zone”, referring to the diagnostic difficulties of these groups (Table 2).
 |
Table 2 Distribution of patients according to ABI results and symptoms |
Tables 3 and 4 show the results of the risk factor distribution and differences between the observed groups of patients, Table 5 shows the distribution of clear PAD patients according to the Fontaine classification, while Table 6 shows the results of the walking test.
 |
Table 3 Risk factor, comorbidity, and medication differences compared to the clear PAD-negative group |
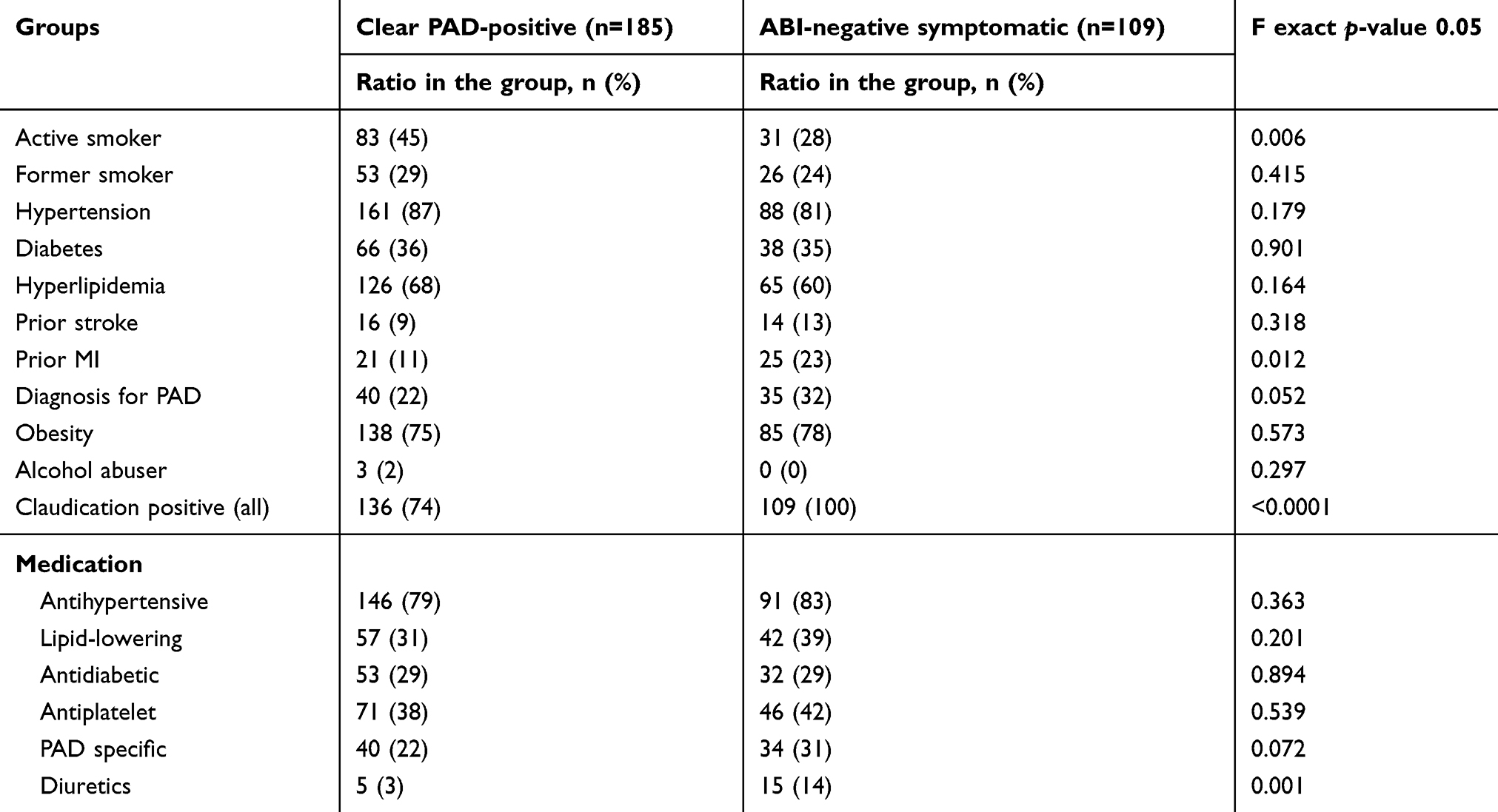 |
Table 4 Risk factor, comorbidity, and medication differences between clear PAD-positive and ABI-negative symptomatic groups |
 |
Table 5 The distribution of PAD-positive patients according to the fontaine classification |
 |
Table 6 Differences in average walking distances in the observed groups of symptomatic patients during walking test compared to the clear PAD-positive patients |
Clear PAD-negative group
Fifty-two percent of the population were categorized into the negative at-rest ABI group. Average age was the lowest here, 64.7±7.8 years. In this group, the most frequent risk factor was hypertension (72%), followed by hyperlipidemia (50%), and diabetes (28%). The number of active smokers was also the lowest here (15%).
Clear PAD-positive group
Based on at-rest ABI values, 23% of the examined patients could be clearly categorized as suffering from atherosclerosis. Of these, 57% were men. The mean age was 66.6±7.7 years. The most frequent risk factor was hypertension at 87%, followed by hyperlipidemia at 68%. The numbers of both active (45%) and former (29%) smokers were the highest here. The percentage of diabetes patients was 36%. A significant number of patients had a medical history of stroke (9%) and infarction (11%). The percentage of claudicating patients was the highest, at 74%. The most frequently prescribed medications were antihypertensives (79%) and antiplatelets (38%). PAD-specific medication had been previously prescribed to 22%. The majority of patients in this group were in Stage IIb of the Fontaine classification (49%).
ABI-negative symptomatic group
Thirteen percent of the total population were categorized into this subgroup. The most frequent risk factor was hypertension (81%). This subgroup has the second highest percentage of active smokers (28%). Medical histories most frequently revealed associated diseases, including stroke (13%) and myocardial infarction (23%). These patients were most commonly diagnosed with PAD (32%). Patients were most commonly prescribed antihypertensives (83%), while 31% received PAD-specific medication.
Non-compressible artery group
This group comprised 12% of the examined population. Average age was the highest at 67.3±8.5 years. The most frequent risk factors were again hypertension (81%), followed by hyperlipidemia (49%). The percentage of diabetes patients was the highest here (37%). This group had the highest percentage of obese patients (87%). A significant 28% of the patients had IC complaints. Of this, 65% were women. The most frequently prescribed medications were antihypertensives (73%).
Discussion
Lower extremity PAD is often diagnosed late in GP practices. Current recommendations suggest the use of non-invasive ABI measurement for screening. Its sensitivity and specificity for lower extremity PAD can be estimated between 79% and 96%.10 It may indicate abnormalities even before the patient develops complaints of dysbasia.12,13
In our screenings, we have made the same important observation similar studies had also faced: in spite of having adequate equipment and trained personnel, the regular performance of ABI measurements is not guaranteed if the importance and associated risks of PAD remain unknown.14,15
Based on ABI measurements, our study categorized nearly a quarter of all examined patients into the clear PAD-positive group. This result matches the data of similar studies.1,5–8,12 It is important that a quarter of these patients were asymptomatic, as the lack of complaints further hinders the recognition of PAD by the GP. The average age within this group was almost 1 year above the average age of the total population, which indicates the importance of age as an independent risk factor. Although a higher number of women participated in the screening, both the number and percentage of PAD were almost one and a half times higher among men. This correlates with literature data.1,4,16
We have found a significant presence of risk factors, and in most cases, the co-occurrence of multiple risk factors.
Smoking is a particularly important risk factor. It increases the risk of occurrence by 2–6 times, and this increases with the amount and years of smoking.2,17,18 Smoking has a closer connection with lower extremity PAD than with coronary diseases.17 The percentage of active smokers was highest in the clear PAD-positive group – one and a half times the Hungarian average.19 The percentage of former smokers was also the highest, as opposed to the clear PAD-negative group, where it was at half the Hungarian average. Quitting smoking rapidly decreases the occurrence of IC complaints.20
Diabetes mellitus patients are at 2.4 times the risk of PAD, and also face a higher risk of developing critical limb ischemia (CLI).21 The risk of future amputation is five times higher for them, and this risk increases with the number of years they suffer from diabetes.22 Approximately, one-third of the examined population was diabetic. The percentage of DM was the highest in the non-compressible artery group, followed closely by the clear PAD-positive and the ABI-negative symptomatic groups. It is important that among the patients of the non-compressible artery and ABI-negative symptomatic groups, it is most frequently impossible to accurately screen for PAD in primary health care using the means available to GPs.
Hypertension is one of the most significant risk factors, although its connection to PAD is weaker than to coronary diseases.23,24 Three quarters of the examined patients had hypertension, which was also the most common risk factor across all examined groups. Its occurrence was highest in the clear PAD-positive group and lowest in the clear PAD-negative group.
Atherosclerosis has a close connection to low HDL and high LDL and triglyceride levels.4,25–27 In the examined population, the prevalence of dyslipidemia was 55%. The highest percentage was in the clearPAD-positive group, and a similarly high prevalence can be seen in the ABI-negative symptomatic group.
The occurrence of stroke in the medical history of either parent triples the risk of a similar event for the descendants.28 Some studies suggest that early-developing CVDs are much more common among individuals whose parents suffered in PAD, and the tendency to develop IC is, in all likelihood, hereditary.29,30 We found the highest percentage of stroke and AMI among the first degree relatives of the ABI-negative symptomatic group.
The ABI-negative symptomatic group comprises patients whose at-rest ABI values were normal or borderline, but show symptoms of IC based on the ECQ. Such situations reveal that at-rest ABI measurement in itself is often insufficient for accurate diagnosis. If the patient’s at-rest ABI measurement results are normal or borderline, but the patient has complaints, a further exercise test is needed (Treadmill test, Strandness protocol: 3 km/hr, 10% slope). In our cohort, one-fifth of normal or borderline ABI value patients had lower limb complaints connected to walking. If systolic pressure falls by more than 30 Hgmm at the ankle by the end of the Treadmill test (reaching maximum walk distance), or if ABI decrease is more than 20% after exercise, a diagnosis of PAD can be established.1 We found the second highest number of active smokers among ABI-negative symptomatic patients. The same is true for hypertension and hyperlipidemia. This group showed the highest incidence for stroke, myocardial infarction, all other heart diseases, and patients in this group most frequently had a previous diagnosis of atherosclerosis and PAD. These results show the importance of not relying solely on at-rest ABI values for establishing a diagnosis of lower limb PAD. Instead, it is highly recommended to take a multi-directional approach even at GP level.
The non-compressible artery group also requires special attention. This group comprises over one-tenth of the examined population, and has the highest average age and the most frequent occurrence of DM. Besides physical examination (such as the palpation of peripheral blood vessels), it is recommended to perform both the ECQ and a walk test, in order to determine whether the patient has complaints of dysbasia. Guidelines advise the use of TBI, which can be performed by angiology specialists. If the TBI value is below 0.7, the patient is diagnosed with lower limb PAD.1,4
Between the clear PAD-positive and clear PAD-negative groups, we found statistically significant differences in the following cases: active smoking, hypertension, hyperlipidemia, obesity, prior myocardial infarction, and prior PAD diagnosis. Differences were also significant regarding antihypertensives, antidiabetics, antiplatelets, and PAD-specific medicines. Analysis of the clear PAD-negative and ABI-negative symptomatic groups yielded the following results: active smoking, prior stroke, MI and PAD diagnosis, furthermore each medication except diuretics. The non-compressible artery group and the ABI-negative symptomatic group differed only in the “prior PAD diagnosis” and “PAD-specific medication” factors.
The difference between the clear PAD-positive and ABI-negative symptomatic groups was significant only in the active smoking, prior MI, claudication, and diuretics categories.
The lowest average pain-free walking distance was measured among the patients of the ABI-negative symptomatic group (the subgroup in which pain was reported during the assessment). Additionally, the same group produced the lowest average maximal walking distance. The clear PAD-positive and ABI-negative symptomatic groups showed significant difference in both pain-free walking distance and maximum walking distance; and so did the ABI-negative symptomatic and non-compressible artery groups. The difference between the clear PAD-positive and non-compressible artery groups was not significant.
On Figure 2 is our proposed screening algorithm for GPs. The whole process takes 15–20 mins, requires little equipment, and considerably improves the quality of life and life expectancy of screened patients potentially at risk. Furthermore, the long-term benefit of screening for lower extremity PAD in GP is the diagnosis of the disease in an early stage, thus allowing for an earlier commencing of treatment, leading to a decrease in future health care costs.
 |
Figure 2 Screening algorithm based on ABI values.Abbreviation: ABI, ankle-brachial index. |
Conclusions
The role of the GP is particularly important in the prevention and early recognition of PAD. The complex approach of our method enables the practitioner to identify at-risk patients who belong to the murky zone. These patients would remain invisible to doctors using instrumental measurements only, and require further examinations from a differential diagnostic perspective. On the long run, launching a complex screening program at GP level makes PAD patients easier to diagnose, which would lead to an earlier start of treatment, significantly improving both the patients’ quality of life and life expectancy.
Ethics approval
Our study received ethical approval no. 285/2015 from Semmelweis University’s Research Ethics Committee.
Consent for publication
Every patient involved in our study signed a form of consent for publication.
Abbreviations
ABI, ankle-brachial index; CVD, cardiovascular disease; CV, cardiovascular; DM, diabetes mellitus; ECQ, Edinburgh Claudication Questionnaire; GP, general practitioner; IC, intermittent claudication; PAD, peripheral arterial disease; TBI, toe-brachial index.
Acknowledgments
We would like to thank all the GPs for their cooperation. This work was supported by the Higher Education Excellence Program of the Ministry of Human Capacities in the framework of the biotechnology research area of Budapest University of Technology and Economics (BME FIKP-BIO). Gergely Tóth-Vajna and Márton Berczeli received a scholarship (“Kiegészítő Kutatási Kiválósági Ösztöndíj”) from Semmelweis University (EFOP-3.6.3-VEKOP-16-2017-00009).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aboyans V, Ricco J-B, Bartelink M-LE-L, et al. ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur Heart J. 2017;2018(39):763–816.
2. Criqui MH, Denenberg JO, Langer RD, Fronek A. The epidemiology of peripheral arterial disease: importance of identifying the population at risk. Vasc Med. 1997;2:221–226. doi:10.1177/1358863X9700200310
3. Ness J, Aronow WS. Prevalence of coexistence of coronary artery disease, ischemic stroke, and peripheral arterial disease in older persons, mean age 80 years, in an academic hospital-based geriatrics practice. J Am Geriatr Soc. 1999;47:1255–1256. doi:10.1111/j.1532-5415.1999.tb05208.x
4. European Stroke Organisation, Tendera M, Aboyans V, et al. ESC guidelines on the diagnosis and treatment of peripheral artery diseases: document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries * The task force on the diagnosis and treatment of peripheral artery diseases of the European Society of Cardiology (ESC). Eur Heart J. 2011;32(22):2851–2906.
5. Criqui MH. Peripheral arterial disease - epidemiological aspects. Vasc Med. 2001;6:3–7. doi:10.1177/1358836X0100600i102
6. Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the united states: results from the national health and nutrition examination survey, 1999-2000. Circulation. 2004;110:738–743. doi:10.1161/01.CIR.0000137913.26087.F0
7. Farkas K, Járai Z, Kolossváry E, Ludányi A, Clement DL, Kiss I. High prevalence of peripheral arterial disease in hypertensive patients: the evaluation of ankle-brachial index in hungarian hypertensives screening program. J Hypertens. 2012;30:1526–1532. doi:10.1097/HJH.0b013e3283559a6a
8. Kolossváry E, Bánsághi Z, Szabó GV, et al. A diabeteses láb ischaemiás eredete. Epidemiológia, a diagnózis nehézségei, prevenciós és revascularisatiós lehetőségek.[The background of the diabetic ischaemic foot. Epidemiology, difficulties in diagnosis, prevention and revascularisation options] Orvosi Hetilap. 2017;158:203–211.
9. Eurostat regional yearbook 2018 [Internet]. 2018 Available from: https://ec.europa.eu/eurostat/documents/3217494/9210140/KS-HA-18-001-EN-N.pdf/655a00cc-6789-4b0c-9d6d-eda24d412188.
10. Leng GC, Fowkes FG. The Edinburgh claudication questionnaire: an improved version of the WHO/rose questionnaire for use in epidemiological surveys. J Clin Epidemiol. 1992;45:1101–1109.
11. Lijmer JG, Hunink MG, van den Dungen JJ, et al. ROC analysis of noninvasive tests for peripheral arterial disease. Ultrasound Med Biol. 1996;22:391–398.
12. Diehm C. Association of low ankle brachial index with high mortality in primary care. Eur Heart J. 2006;27:1743–1749. doi:10.1093/eurheartj/ehl092
13. Wild SH, Byrne CD, Smith FB, et al. Low ankle-brachial pressure index predicts increased risk of cardiovascular disease independent of the metabolic syndrome and conventional cardiovascular risk factors in the Edinburgh artery study. Diabetes Care. 2006;29:637–642. doi:10.2337/diacare.29.03.06.dc05-1637
14. Yap Kannan R, Dattani N, Sayers RD, et al. Survey of ankle–brachial pressure index use and its perceived barriers by general practitioners in the UK. Postgrad Med J. 2016;92:322–327. doi:10.1136/postgradmedj-2015-133375
15. Davies JH, Kenkre J, Williams EM. Current utility of the ankle-brachial index (ABI) in general practice: implications for its use in cardiovascular disease screening. BMC Fam Pract. [Internet]. 2014;15(1): 69. Available from: http://bmcfampract.biomedcentral.com/articles/10.1186/1471-2296-15-69. [cited 2018 Jul 22].
16. Fowkes FGR, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329–1340. doi:10.1016/S0140-6736(13)61249-0
17. Price JF, Mowbray PI, Lee AJ, et al. Relationship between smoking and cardiovascular risk factors in the development of peripheral arterial disease and coronary artery disease: edinburgh artery study. Eur Heart J. 1999;20:344–353. doi:10.1053/euhj.1998.1194
18. Powell JT, Edwards RJ, Worrell PC, et al. Risk factors associated with the development of peripheral arterial disease in smokers: a case-control study. Atherosclerosis. 1997;129:41–48. doi:10.1016/s0021-9150(96)06034-0
19. Tombor I, Paksi B, Urbán R, et al. Epidemiology of smoking in the hungarian population, based on national representative data. Clin Exp Med J. 2011;5:27–37. doi:10.1556/CEMEd.4.2010.28817
20. Ingolfsson IO, Sigurdsson G, Sigvaldason H, Thorgeirsson G, Sigfusson N. A marked decline in the prevalence and incidence of intermittent claudication in Icelandic men 1968-1986: a strong relationship to smoking and serum cholesterol–the Reykjavik study. J Clin Epidemiol. 1994;47:1237–1243. doi:10.1016/0895-4356(94)90128-7
21. Hiatt WR, Hoag S, Hamman RF. Effect of diagnostic criteria on the prevalence of peripheral arterial disease. The San Luis valley diabetes study. Circulation. 1995;91:1472–1479. doi:10.1161/01.cir.91.5.1480
22. Jude EB, Oyibo SO, Chalmers N, et al. Peripheral arterial disease in diabetic and nondiabetic patients: a comparison of severity and outcome. Diabetes Care. 2001;24:1433–1437. doi:10.2337/diacare.24.2.350
23. Murabito JM, D’Agostino RB, Silbershatz H, Wilson PWF. Intermittent claudication. A risk profile from the framingham heart study. Circulation. 1997;96:44–49. doi:10.1161/01.CIR.96.1.44
24. Hooi JD, Stoffers HE, Kester AD, et al. Risk factors and cardiovascular diseases associated with asymptomatic peripheral arterial occlusive disease. The limburg PAOD study. Peripheral arterial occlusive disease. Scand J Prim Health Care. 1998;16:177–182. doi:10.1080/028134398750003142
25. Sanderson K. Lipid peroxidation of circulating low density lipoproteins with age, smoking and in peripheral vascular disease. Atherosclerosis. 1995;118:45–51. doi:10.1016/0021-9150(95)05591-J
26. Horby J, Grande P, Vestergaard A, Grauholt AM. High density lipoprotein cholesterol and arteriography in intermittent claudication. Eur J Vasc Surg. 1989;3:333–337.
27. Bradby GV, Valente AJ, Walton KW. Serum high-density lipoproteins in peripheral vascular disease. Lancet. 1978;2:1271–1274. doi:10.1016/S0140-6736(78)92038-X
28. Seshadri S, Beiser A, Pikula A, et al. Parental occurrence of stroke and risk of stroke in their children: the framingham study. Circulation. 2010;121:1304–1312. doi:10.1161/CIRCULATIONAHA.109.854240
29. Valentine RJ, Verstraete R, Clagett GP, Cohen JC. Premature cardiovascular disease is common in relatives of patients with premature peripheral atherosclerosis. Arch Intern Med. 2000;160:1343–1348. doi:10.1001/archinte.160.9.1343
30. Prushik SG, Farber A, Gona P, et al. Parental intermittent claudication as risk factor for claudication in adults. Am J Cardiol. 2012;109:736–741. doi:10.1016/j.amjcard.2011.10.032
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.