")
Back to Journals » Clinical Ophthalmology » Volume 16
Scleral Buckling: A Look at the Past, Present and Future in View of Recent Findings on the Importance of Photoreceptor Re-Alignment Following Retinal Re-Attachment
Authors Cruz-Pimentel M , Huang CY , Wu L
Received 10 April 2022
Accepted for publication 8 June 2022
Published 16 June 2022 Volume 2022:16 Pages 1971—1984
DOI https://doi.org/10.2147/OPTH.S359309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Miguel Cruz-Pimentel,1 Chyong Yng Huang,2 Lihteh Wu2,3
1Department of Ophthalmology and Vision Sciences, University of Toronto, Toronto, Ontario, Canada; 2Asociados de Macula, Vitreo y Retina de Costa Rica, Primer Piso Torre Mercedes Paseo Colon, San José, Costa Rica; 3Illinois Eye and Ear Infirmary, Department of Ophthalmology, School of Medicine, University of Illinois Chicago, Chicago, IL, USA
Correspondence: Lihteh Wu, Asociados de Macula, Vitreo y Retina de Costa Rica, Primer Piso Torre Mercedes, Paseo Colon, San Jose, CR, USA, Tel +506 2222-1115, Email [email protected]
Abstract: Scleral buckling (SB) remains an important technique to master for those interested in treating rhegmatogenous retinal detachment (RRD). Several ways to repair RRD include pneumatic retinopexy (PR), pars plana vitrectomy (PPV), SB or a combination of these. There is a growing worldwide trend that favors PPV as the preferred method for retinal reattachment of primary uncomplicated RRD. Reimbursement issues, operating room access, and technological advances in PPV that improve retinal visualization and less exposure to SB during fellowship training may explain this trend. As the number of SB cases decreases over time, there is a risk that SB becomes a dying art and surgeons in training may not be trained in SB. SB is preferred in eyes with no posterior vitreous detachment and retinal dialysis. SB with minimal gas vitrectomy may be indicated for eyes with inferior pathology. Non-contact wide-angled visualization with chandelier assisted SB may be well suited for teaching new generations of aspiring vitreoretinal surgeons. Its functional and anatomic results compare favorably with conventional SB for primary uncomplicated primary RRD. The main advantage of this technique is the improved visualization even through small pupils. Better visualization ensures treatment of all breaks while avoiding complications during drainage of subretinal fluid and a safer placement of intrascleral sutures for scleral fixation of the buckling element. Recordings of the procedure are easily performed, allowing the surgeons involved to review the case and learn from it. The main disadvantage is the cost involved with the chandelier and the need to have a microscope or a 3D system with a wide angle viewing system. Photoreceptor re-alignment following retinal re-attachment is an important determinant of the post-operative functional outcomes. Different methods of retinal re-attachment apparently result in different degrees of photoreceptor re-alignment. SB may hold an advantage over PPV in this regard.
Keywords: rhegmatogenous retinal detachment, chandelier assisted scleral buckling, wide-angled illumination assisted scleral buckling, scleral buckling, pars plana vitrectomy, photoreceptor integrity
Introduction
Rhegmatogenous retinal detachment (RRD) is a relatively common cause of preventable blindness. Its incidence has been reported to vary between 6.3 and 17.9 cases per 100,000 inhabitants.1,2 Risk factors include age, myopia, cataract surgery, a history of trauma and a family history, among others. Worldwide there is a changing epidemiological trend with increases in cataract surgery, myopia and aging populations. Similarly, the incidence of RRD appears to be increasing.3–6 In Denmark, this increased incidence is driven by men ≥50 years of age.3 In Korea and the Netherlands, the increase is driven by the increasing incidence of myopia, whereas in Western Norway it is driven by the increase of pseudophakic RRD.4–6
Currently, there are several methods of repairing RRD including SB, pneumatic retinopexy (PR), pars plana vitrectomy (PPV) and a combination of these. PR is an office-based, minimally invasive, non-incisional procedure that consists of an intravitreal injection of an expandable gas bubble, post-injection head positioning to tamponade the retinal breaks and the application of cryopexy or laser retinopexy to the retinal breaks. We have recently reviewed the advantages, disadvantages and outcomes of PR.7 In the 1970s, Machemer et al,8 based on the previous work on open sky vitrectomy by Kasner et al,9 developed PPV. Historically, the main indication of vitrectomy was the removal of vitreous opacities. However, as technology and techniques evolved, the indications for PPV also evolved.10–16 In the past 2 decades, SB has fallen to the wayside and PPV has become the preferred method for surgical repair of RRD. From complex retinal detachments to primary rhegmatogenous retinal detachment, PPV is currently the preferred technique for retinal reattachment.17
There has been a recent interest and an increasing body of evidence that suggests that photoreceptor re-alignment following retinal re-attachment is an important determinant of the functional outcomes of retinal surgical repair. Different methods of retinal re-attachment apparently result in different degrees of photoreceptor re-alignment.18–25 SB may hold an advantage over PPV in this regard.26
The reasons behind the increasing preference of PPV over SB and PR in most of the world probably consist of a combination of reimbursement issues, operating room access, technological advances in PPV that have improved retinal visualization and less exposure to SB and PR during fellowship training.27 Interestingly, the PRO Study Group recently reported that surgeons with a high single surgery success rate were more likely to use an SB as part of their armamentarium in the repair of RRD compared to surgeons with a low single surgery success rate.28 As the number of SB cases performed decrease over time, there is a risk that SB becomes a dying art and vitreoretinal surgeons in training may not be trained in SB. Non-contact wide-angled visualization with chandelier assisted SB under microscope or digitally assisted 3D surgery in addition to the new findings regarding SB and photoreceptor re-alignment may help reverse this trend.
Pathophysiology of RRD
The pathophysiology of an RRD has been reviewed extensively in the past.29–31 Briefly RRD develops as a consequence of a combination of intraocular currents and dynamic vitreous traction in the presence of an open retinal break. The vast majority of RRD results from an acute posterior vitreous detachment (PVD) that causes an acute retinal break.30 It follows that to successfully treat an RRD all of these factors need to be addressed. The goal should be to flatten the retinal break against the retinal pigment epithelium (RPE), which will prevent further passage of intravitreal fluid through the break into the subretinal space. This will allow the RPE pump to reabsorb the subretinal fluid and re-attach the retina. A scleral buckle (SB) alters the ocular anatomy and physiology to facilitate the functional closure of retinal breaks, reduces vitreoretinal traction, directly closes the retinal breaks by bringing the eyewall into contact with the retina, alters intraocular currents and walls off areas of detachment and breaks.30
History of Scleral Buckling
Prior to Gonin’s 31 seminal observation a century ago that retinal breaks are causative of RRD, RRDs were rarely successfully repaired.32,33 Gonin developed a technique called ignipuncture where the retinal breaks were identified pre-operatively, subretinal fluid beneath the retinal breaks was drained and the breaks were treated directly with cautery.3 Gonin’s theory on the etiology of RRD and the development of his technique using a thermocautery resulted in an increase in the success rate from less than 1% in 1912 to about 30–40% by the 1930s.34–36 One of the drawbacks of the ignipuncture technique was that cautery was not a reliable safe method to produce a chorioretinal reaction surrounding the retinal break. One of the earliest modifications to Gonin’s ignipuncture technique was the introduction of diathermy and chemical agents to induce chorioretinal adhesions.37,38 Diathermy retinopexy gained popularity but success was limited in certain cases where the retina failed to settle against the eyewall or subretinal fluid rapidly accumulated.38 In these cases, chorioretinal adhesions could not develop fast enough and the retina remained detached. It was then recognized that scleral resection produced an inward ridge-like elevation that approximated the retinal pigment epithelium (RPE) and choroid to the detached retina. Retinal surgeons devised a myriad of procedures including full-thickness scleral resections, lamellar scleral resections, scleral outfolding procedures and scleral infolding procedures from the 1930s to the 1950s to try to produce a scleral buckling effect. However, the scleral indentation produced by these procedures was minimal and the location of the scleral ridge did not support the retinal breaks in the vast majority of procedures.39
In 1937, Jess40 noted that following penetrating diathermy and subretinal fluid drainage, the eye often became hypotonous and led to retinal folds and scleral collapse interfering with the RPE and retinal contact. He attached a thread to a cotton swab that was placed in the episcleral space against the area of the retinal break causing scleral indentation in the hopes of counteracting the effects of hypotony. The cotton swab was left in place for two weeks and then removed. A decade later, Custodis41 pioneered the use of an episcleral exoplant and a non-drainage procedure to close the retinal breaks. In the mid 1950ʹs Schepens et al42 described their technique characterized by a lamellar scleral resection, subretinal fluid drainage, diathermy and a scleral buckling implant. In 1965, Lincoff et al43 modified the Custodis procedure by introducing cryotherapy instead of diathermy, developing a flat scleral needle that allowed intrascleral passes through half thickness sclera for 6 mm and replacing the polyviol with a silicone sponge. Similar to Custodis, Lincoff advocated for not draining subretinal fluid.43–46 Over the years different materials such as polyethylene tube, silicone rubber, fascia lata, non-absorbable suture, absorbable gelatin, preserved human sclera, plantaris tendon, absorbable collagen, polyglactin 910, polyglycolic acid, polydioxanone, plain and chromic gut, dura mater, cartilage and skin were studied as possible scleral buckling materials.39
Microscope Assisted Scleral Buckling
A successful retinal re-attachment procedure depends on the identification of all the retinal breaks. Thus, an excellent visualization of the entire retina is critical for a good surgical outcome. Surgeons have traditionally relied on indirect ophthalmoscopy to perform an SB. In eyes with small pupils, pseudophakic eyes with posterior capsular opacities and eyes with small peripheral breaks, the visualization of the peripheral retina under indirect ophthalmoscopy may be fraught with difficulties. In cases where the retinal breaks are difficult to visualize, one can infer the location of retinal breaks by the distribution of subretinal fluid.47
In the 1980ʹs Bonnet pioneered the use of the operating microscope as a visualizing tool for retinal re-attachment procedures.48 She placed a Goldmann 3 mirror contact lens on the cornea and visualized the retina through a microscope with slit-lamp illumination capabilities. The main advantages of this technique are the image magnification and the erect image produced in contrast to the inverted image of the indirect ophthalmoscope. This technique never caught on outside of France because of the main disadvantages that included a steep learning curve, the longer operating time, and that in eyes with anterior segment abnormalities or a small pupil size visualization was difficult.48 In 2008, Nawrocki et al49 used the Optic Fibre Free Intravitreal Surgical System (OFFISS, Topcon Inc, Paramus, NJ, USA), which provides approximately 50 degrees of fundus visualization, to place an SB to repair seven eyes with an RRD. Successful re-attachment was achieved in six (85.7%) of the seven eyes. In 2012, Aras et al50 attempted repair of 16 eyes using non-contact wide angle visualization for placement of an SB. They were able to successfully re-attach 13 (81%) eyes. The main advantages of a non-contact wide-angle fundus visualization are that it provides an increased field of view of up to 130°, and the view is not too dependent on pupil size.51 Further improvements in the field of view with less peripheral distortion may be obtained by using a Volk HRX Vit SSV contact lens.52 In 2013, Nagpal et al52 reported a 90% re-attachment rate in a series of 10 eyes using this lens.
We have previously reported that non-contact wide-angled visualization with chandelier assisted SB compares favorably with conventional SB for primary uncomplicated primary RRD.53 In the largest series to date, Roca et al53 reported an 85.1% re-attachment rate in their series of 282 eyes. Other smaller series, where the surgeons used a similar technique and compared it to conventional SB, reported similar re-attachment rates.54–66 Roca et al’s53 functional results also compare favorably with the literature. In their study, two thirds of eyes presented with the macula detached. Following non-contact wide-angled visualization with chandelier assisted SB, the pre-op visual acuity improved from 1.21 to 0.76 logMAR at 6 months, which is similar to other reports in the literature.54–63
Digitally assisted 3D surgery provides improved depth, increased field of view, more magnification, less need for illumination, better contrast, improved sharpness, color and digital imaging, which all enhance visualization compared to traditional microscope viewing. Time lag has been a concern for anterior segment procedures. A recent comparative study demonstrated that digitally assisted 3D surgery was non-inferior and safe when performing SB compared to traditional microscope viewing.67 La Spina et al68 reported a primary success rate of 94% (101 of 107) with a 3-month follow-up in eyes treated with chandelier-assisted SB. Interestingly, 8.9% of eyes had retinal breaks not detected in the preoperative evaluation. 3D systems have greatly improved visualization in vitreoretinal surgery; however, despite their availability, they have not been widely accepted perhaps because of an elevated cost and also because of its learning curve. Some experienced surgeons report a very good image for macular surgery but a decrease in the details in the visualization of the periphery, and many assistants report difficulty and fatigue when having to visualize the screen with their head tilted.69 Table 1 compares and summarizes the outcomes of chandelier assisted SB and conventional SB.
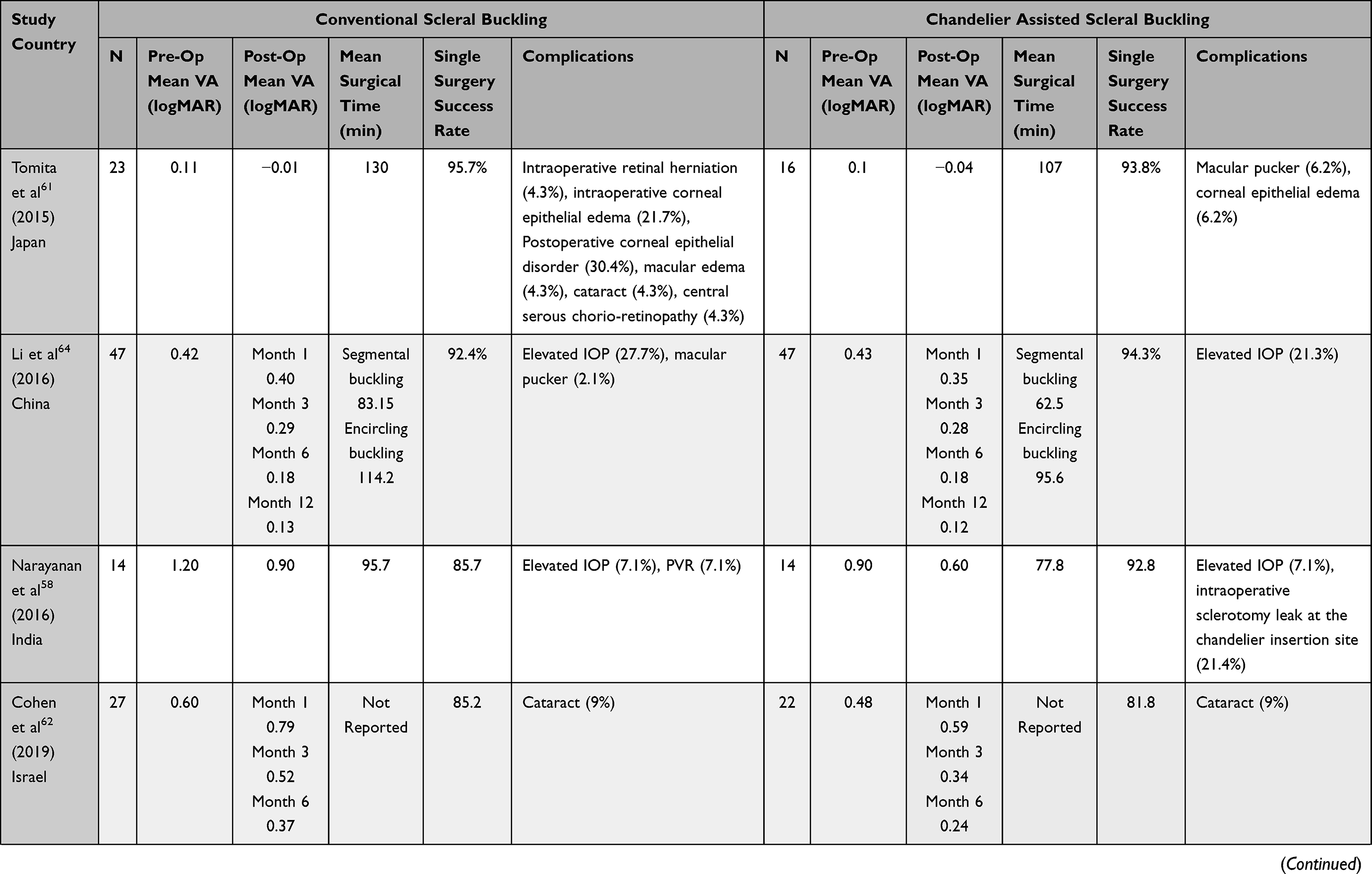 | 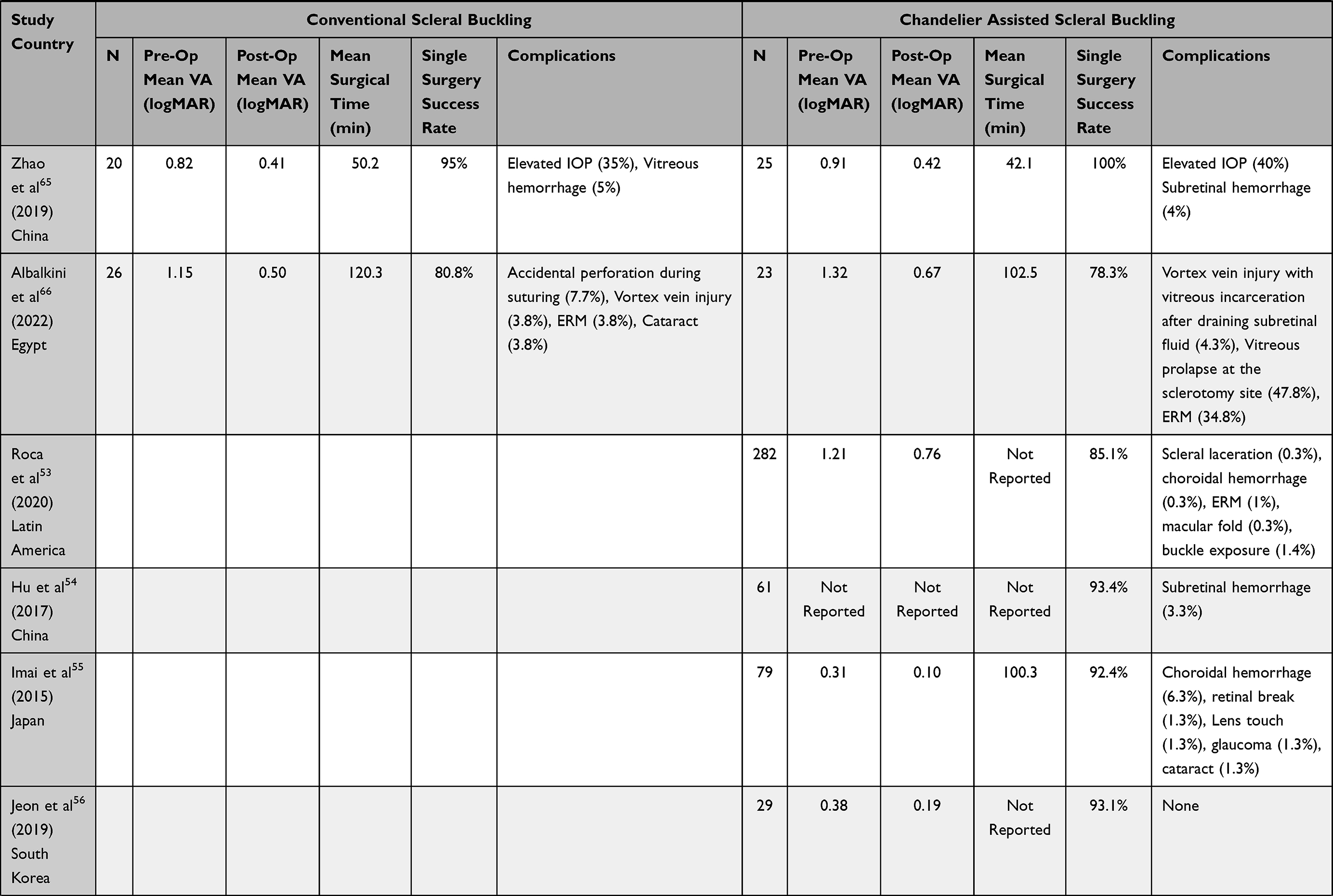 | 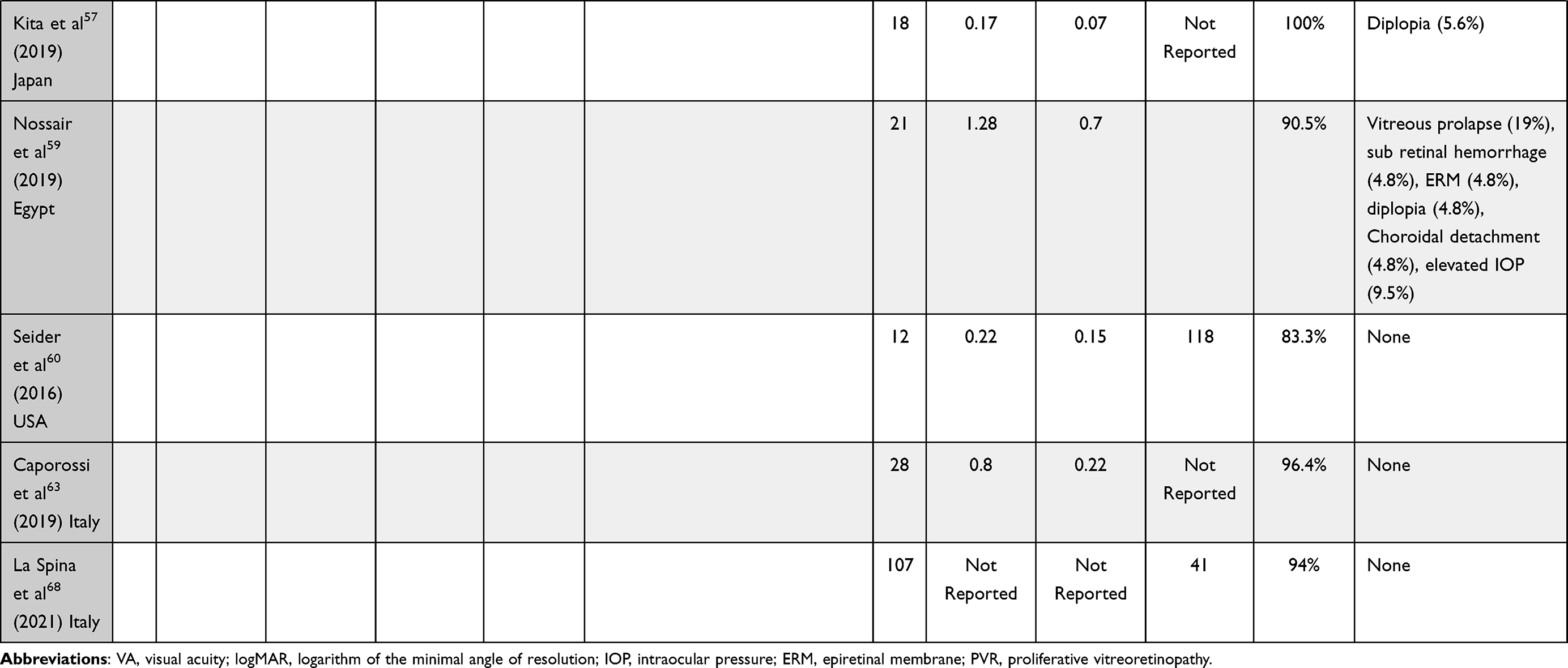 |
Table 1 Comparative Outcomes of Chandelier Assisted Scleral Buckle and Conventional Scleral Buckle |
Both microscope and digitally assisted 3D surgery allow for recordings, which are a valuable tool in educating vitreoretinal fellows and providing feedback even to experienced surgeons. Digitally assisted 3D surgery is an advantageous system for teaching since all personnel in the room can follow each step of the surgery.70,71 In addition, some have claimed ergonomic benefits afforded to the surgeon.68,72
Scleral Buckling Technique
SB techniques have been reviewed extensively in the past.73 Common variables in contemporary SB include choices in the type of buckling material, extent of scleral buckling, to drain or not to drain subretinal fluid, type of chorioretinal adhesion, supplemental vitreous injections and retinal visualization techniques. It is beyond the scope of this review to describe in detail every single technique. We will briefly review some of these.
For microscope assisted SB, patients undergo the procedure under peribulbar anesthesia with bupivacaine or general anesthesia depending on the surgeon’s preference. Under direct visualization through the oculars of the microscope, a conjunctival peritomy of 360° is performed. Isolation of the rectus muscles is followed by placement of traction sutures under the insertion of each rectus muscle tendon. A chandelier is inserted through a trocar 3.5–4.0 mm from the limbus at 180 degrees from the retinal tear. The retina is indented with the cryo probe under direct visualization through the oculars of the microscope with a wide-field viewing system (Resight®, Biom®) in place. Cryopexy is placed around the tears.53 Alternatively, a curved illuminated endolaser may be inserted through the chandelier port. By using a continuous mode with a power of 300 mW, it may be possible to reach areas distal to the tip of the laser probe without advancing the laser probe too much into the vitreous cavity, thus minimizing vitreous traction.74
Scleral buckles can be oriented radially or circumferentially and an encircling element may also be placed. The placement of radial elements requires precise localization of the retinal break. Radial buckles avoid fish-mouthing of the breaks and radial folds.75–77 Circumferential segmental buckling may be preferred by some surgeons by supporting undetected breaks and vitreoretinal traction in the vicinity of the detachment. Fish-mouthing and radial folds may occur following segmental circumferential buckling.78 Eyes with small peripheral breaks along the vitreous base may benefit from an encircling element.79 A spatulated needle with a 5.0 non-absorbable suture is used to place the sutures at least 2 mm from the edges of the buckle at one-half to three-fourths scleral depth in a mattress fashion parallel to the long axis of the buckle being supported. If an encircling element is used, scleral tunnels or non-absorbable sutures may be used to hold it in place.
In cases where the surgeon elects to drain the subretinal fluid, visualization of the external trans-scleral drainage procedure is done through the microscope with a wide-field viewing system. Alternatively, internal drainage with a sharp needle or cannula has been described.80 In eyes with a very bullous RRD, drainage of subretinal fluid facilitates the apposition of the retinal break to the RPE. Nevertheless, subretinal fluid drainage remains controversial. In most cases, retinal reattachment rates are equally effective regardless of whether or not drainage of subretinal fluid was performed.81,82 The sclerotomies are closed with a 7.0 Vicryl stitch and the conjunctiva is sutured closed.53
Scleral Buckling Complications
The most important intraoperative complications of SB include those associated with drainage of subretinal fluid and the inadvertent scleral perforation during scleral suture placement.83,84 Serious complications include retinal incarceration, intraocular hemorrhage, retinal perforation, vitreous incarceration and hypotony.83 Magnification by a microscope or 3D viewing system may decrease the risk of these complications. There are few reports of complications secondary to chandelier assisted SB. Theoretically, bacteria may be inoculated into the vitreous cavity as the chandelier fiber tip is inserted into the vitreous cavity through the conjunctiva. Endophthalmitis has been reported in a few cases.85,86 In addition, after removal of the chandelier, vitreous may incarcerate in the sclerostomy. Vitreous prolapse at the chandelier sclerotomy site,59 a retinal break thought to be related to the insertion of the chandelier55 and a case of lens touch during cryoretinopexy have been attributed to chandelier assisted SB.55 Other reported complications that were not attributed to the visualization technique or the insertion of the chandelier include subretinal hemorrhage at the site of drainage,59 choroidal hemorrhage, 53,55,59 buckle exposure,53 scleral laceration and perforation attributed to excessive indentation during surgery.50,53
Post-operative SB complications include persistent post-surgical diplopia, glaucoma, anterior segment ischemia, buckle infection and extrusion, choroidal detachment, cystoid macular edema, epiretinal membranes, motility disturbances and refractive changes.87,88 These have not been reported to occur more frequently following chandelier assisted SB.53
SB Indications
Although most vitreoretinal surgeons worldwide have embraced PPV as its preferred technique to repair an uncomplicated primary RRD, there are certain situations where SB is preferred over PPV. RRD secondary to retinal breaks without a posterior vitreous detachment may be preferably treated with an SB rather than PPV. In these eyes, induction of a posterior vitreous detachment may lead to iatrogenic breaks. Furthermore, SB will avoid the need for positioning, premature cataract formation and all the complications associated with gas or silicone oil tamponade. RRD secondary to round retinal holes are characterized by the absence of a PVD. These are usually found in young female myopic patients. The RRD is usually shallow and progresses slowly. SB is very effective in these groups of patients.89 Retinal dialysis results from the disinsertion of the retina from the vitreous base. Most cases are secondary to developmental conditions or trauma.90–93 SB is also the preferred method for surgical re-attachment in these eyes.94–96 Recent evidence suggests that SB with minimal gas vitrectomy may be indicated for eyes with inferior pathology.97,98
Outcomes of Retinal Re-Attachment Procedures
Traditionally, single operation anatomic success rate has been used as a measure of surgical success. Two recent meta-analysiss recently concluded that there were no significant differences between the re-attachment rates of PPV vs SB.99,100 A meta-analysis that included 15,661 eyes from 38 studies compared the outcomes of eyes treated with PPV and those treated with PPV plus SB. PPV plus SB had a higher single operation success rate, but the final reattachment rate was similar between the two groups.101 A recent Cochrane review concluded that PR had a lower reattachment rate and a higher recurrence rate but a lower burden of post-operative complications compared to SB.102 Data from a commercial insurance database from the USA showed that almost 30% of cases managed by primary PR compared to 20% of cases managed by either SB or PPV required a reoperation within 90 days of the primary repair.103 More recently, the Primary Retinal Detachment Outcomes104 Study reported that in phakic patients there was, not only a higher success rate with a single procedure with SB compared to patients undergoing PPV (91.7% vs 83.1%) but also a better visual acuity in patients undergoing SB.105,106 The PIVOT trial showed that eyes treated with PPV had a higher success rate (93% vs 80%) with a single procedure than eyes treated with PR.107
PPV was associated with a higher incidence of cataract, progression of cataract and iatrogenic retinal breaks, whereas SB was associated with hypotony, choroidal detachment, subretinal hemorrhage, residual subretinal fluid, strabismus and diplopia.99,100,108
Functional Outcomes
Recently, researchers from Toronto have questioned the historical emphasis placed on single operation anatomic success rate as a measure of surgical success.24,107 Recent systematic reviews and meta-analysis of randomized clinical trials comparing SB, PR and PPV for RRD reported that there were no significant differences in final visual acuity between the different techniques.99,101,108 Despite retinal re-attachment and excellent visual acuity, patients may be dissatisfied following retinal reattachment surgery due to aniseikonia and vertical metamorphopsia. Clinical examination with indirect ophthalmoscopy or slit-lamp biomicroscopy of the macular area usually reveals no abnormalities. For eyes with RRD that involved the macula, successful anatomic re-attachment by PPV was accompanied by aniseikonia in 42% to 58% of cases.109–112 Similarly the rates of post-PPV metamorphopsia are high, ranging anywhere from 50% to 90%.113–118
The PIVOT was a single center, randomized clinical trial that compared the outcomes of primary PR in 77 eyes versus primary PPV in 73 eyes with primary RRD.107 Despite a lower anatomic and single operation success rate, eyes that were treated with PR had visual acuity outcomes superior to those obtained with PPV. Visual acuity outcomes with PR were superior to those obtained with PPV.107 The ETDRS best corrected VA was better at 3, 6 and 12 months of follow-up. The mean best corrected VA at 12 months was 79.9 letters in the PR group compared to 75 letters in the PPV group. In addition, the proportion of eyes achieving ≥20/40 was 90.3% compared to 75.3% in the PPV group.107 Furthermore, eyes treated with PPV experienced significantly more vertical metamorphopsia than eyes treated with PR.107 These functional changes have been ascribed to anatomical changes only observed in multimodal imaging.18,23,119–123
Unintentional retinal displacement following retinal re-attachment with a PPV has been described anywhere from 45% to 72%.23 In contrast, the PIVOT trial demonstrated that the retinal displacement induced by PR to those induced by PPV was significantly less.18 There are very limited data regarding retinal displacement following SB. Lee et al119 reported no retinal displacement in 9 eyes that underwent SB. Of these 9 eyes, 3 eyes had the macula involved. In contrast, displacement was observed in 72% (23/32) of eyes with foveal involved RRD and in 29% (5/17) of eyes with fovea spared RRD following PPV.119
Fundus autofluorescence (FAF) may be used to assess the degree of retinal displacement by comparing the hyper-FAF lines located superior and parallel to the retinal vessels.124 The original position of retinal vessels prior to the RRD is most likely represented by the hyper-FAF lines. They have been named as retinal vessel printings or ghost vessels.119,122,123 Some have suggested that immediate strict face-down positioning for a few hours may reduce the rate of retinal displacement following retinal re-attachment.123,125,126 Silicone oil apparently causes less retinal displacement compared to gas.20,119,127,128 This retinal displacement may account for the post-operative vertical metamorphopsia experienced by some patients. Muni et al24 introduced the concept of photoreceptor integrity following retinal re-attachment. Eyes with retinal displacement are considered to have a low integrity retinal reattachment, whereas those eyes without retinal displacement have a high integrity retinal reattachment.
Ellipsoid zone (EZ) disruption, EZ-RPE thickness, external limiting membrane (ELM) disruption, outer retinal folds (ORF) and EZ hyporeflectivity on en face SD-OCT have all been associated with post-operative visual acuity.120,121,129–137 ORF, unlike full thickness retinal folds, are not clinically visible and are only detected by OCT. ORF are protrusions of the photoreceptors that cause infolding of the ELM and EZ.121 They were first described in 2006 using time domain OCT.136 A post-hoc analysis from the PIVOT trial showed that the presence of ORF was associated with a poorer visual acuity at 12 months. Furthermore, there were more eyes in the PPV group than the PR group that developed ORF.121 Similarly, PPV produces more post-operative EZ and ELM disruptions compared to PR.24
An intravitreal gas bubble exerts a buoyant force on the retina.19,22,127 Once the detached retina comes into contact with the gas bubble, the subretinal fluid beneath the detached retina is displaced to regions away from the bubble. The retina in contact with the bubble is brought into contact with the RPE. The residual subretinal fluid is squeezed and pushed in a gravity-dependent fashion causing retinal stretching and displacement.
These findings have led these investigators to suggest that how one achieves surgical reattachment has implications for the post-operative functional outcomes. Fluid air exchange coupled to large intraocular gas tamponade may lead to higher rates of low integrity retinal reattachment compared to procedures where the RPE pump removes the subretinal fluid. A slower more physiologic reabsorption of subretinal fluid directed by the RPE may allow the photoreceptors to orient and align themselves correctly with the RPE. In contrast, fluid–air exchange or transscleral subretinal fluid drainage cause an abrupt contact between the photoreceptors and the RPE.22,24,137 Based on these findings, Muni et al97,98 have suggested modifying PPV by avoiding a fluid–air exchange. Following completion of PPV, they inject a small expansile gas bubble instead and let the RPE pump remove the subretinal fluid similar to a PR. Post-operative patients are positioned similar to PR. The breaks are treated intraoperatively with cryotherapy or alternatively with laser retinopexy post-operatively once the retina reattaches. In eyes with inferior breaks, a segmental buckle is added.97
Conclusions and Future Directions
In summary, the incidence of RRD is on the rise. There are several ways to repair an RRD including PR, PPV, SB or a combination of these techniques. Recent trends show that vitreoretinal surgeons prefer PPV over other techniques to repair most cases of RRD. A key advantage of PPV is the superior visualization of the entire retina in comparison to other techniques. Non-contact wide-angled visualization with chandelier assisted SB with either a microscope or a 3D head up system provides a superior retinal visualization than conventional SB with indirect ophthalmoscopy. This modification to conventional SB may be well suited for teaching new generations of aspiring vitreoretinal surgeons. Its functional and anatomic results compare favorably with conventional SB for primary uncomplicated primary RRD. It may help turn the tide against the declining use of SB.
Traditionally emphasis has been placed on single operation anatomic success rate as a measure of surgical success. Despite retinal re-attachment and excellent visual acuity, patients may be dissatisfied following retinal re-attachment surgery due to aniseikonia and vertical metamorphopsia. Both of these complaints appear to be caused by a low integrity retinal reattachment. How we achieve retinal re-attachment appears to influence photoreceptor re-alignment. PPV with fluid air exchange and full gas tamponade may not be the best way to re-attach the retina. Modifications to conventional PPV such as avoiding an air–fluid exchange and adding a segmental inferior buckle in eyes with inferior retinal tears and breaks have been suggested to avoid low integrity retinal re-attachment.
The theoretical concept of photoreceptor realignment following retinal reattachment was raised almost fifty years ago.137 However, it was not until recently with the advent of multimodal imaging that it was tested and assessed in different scenarios including PPV with gas tamponade, PPV with silicone oil tamponade and PR.18–24 Validation of these results by other researchers should be encouraged. Researchers interested in the subject should consider studying the effects of external trans-scleral drainage of subretinal fluid during SB on the integrity of retinal reattachment. A preliminary study suggests that retinal displacement is not a common occurrence following SB.26 Further understanding of how a retina reattaches may lead to improved functional outcomes in patients with an RRD.
Disclosure
Dr Lihteh Wu reports personal fees from Quantel Medical, Bayer, and Roche, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Li JQ, Welchowski T, Schmid M, et al. Incidence of rhegmatogenous retinal detachment in Europe - A systematic review and meta-analysis. Ophthalmologica. 2019;242(2):81–86. doi:10.1159/000499489
2. Mitry D, Charteris DG, Fleck BW, et al. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. Br J Ophthalmol. 2010;94(6):678–684. doi:10.1136/bjo.2009.157727
3. Nielsen BR, Alberti M, Bjerrum SS, la Cour M. The incidence of rhegmatogenous retinal detachment is increasing. Acta Ophthalmol. 2020;98(6):603–606. doi:10.1111/aos.14380
4. Park JY, Byun SJ, Woo SJ, et al. Increasing trend in rhegmatogenous retinal detachment in Korea from 2004 to 2015. BMC Ophthalmol. 2021;21(1):406. doi:10.1186/s12886-021-02157-1
5. van Leeuwen R, Haarman AEG, van de Put MAJ, et al. Association of rhegmatogenous retinal detachment incidence with myopia prevalence in the Netherlands. JAMA Ophthalmol. 2021;139(1):85–92. doi:10.1001/jamaophthalmol.2020.5114
6. Achour H, Thomseth VM, Kvaloy JT, et al. Substantial increase in the incidence of rhegmatogenous retinal detachment in Western Norway over 20 years. Acta Ophthalmol. 2022. doi:10.1111/aos.15119
7. Huang CY, Mikowski M, Wu L. Pneumatic retinopexy: an update. Graefes Arch Clin Exp Ophthalmol. 2021:1–2. doi:10.1007/s00417-021-05448-x
8. Machemer R, Buettner H, Norton EW, Parel JM. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75(4):813–820.
9. Kasner D, Miller GR, Taylor WH, et al. Surgical treatment of amyloidosis of the vitreous. Trans Am Acad Ophthalmol Otolaryngol. 1968;72(3):410–418.
10. Machemer R. A new concept for vitreous surgery. 2. Surgical technique and complications. Am J Ophthalmol. 1972;74(6):1022–1033. doi:10.1016/0002-9394(72)90719-2
11. Machemer R. A new concept for vitreous surgery. 7. Two instrument techniques in pars plana vitrectomy. Arch Ophthalmol. 1974;92(5):407–412. doi:10.1001/archopht.1974.01010010419009
12. Machemer R. A new concept for vitreous surgery. 6. Anesthesia and improvements in surgical techniques. Arch Ophthalmol. 1974;92(5):402–406. doi:10.1001/archopht.1974.01010010414008
13. Machemer R, Buettner H, Parel JM. Vitrectomy, a pars plana approach. Instrumentation. Mod Probl Ophthalmol. 1972;10:172–177.
14. Machemer R, Norton EW. Vitrectomy, a pars plana approach. II. Clinical experience. Mod Probl Ophthalmol. 1972;10:178–185.
15. Machemer R, Norton EW. A new concept for vitreous surgery. 3. Indications and results. Am J Ophthalmol. 1972;74(6):1034–1056. doi:10.1016/0002-9394(72)90720-9
16. Machemer R, Parel JM, Buettner H. A new concept for vitreous surgery. I. Instrumentation. Am J Ophthalmol. 1972;73(1):1–7. doi:10.1016/0002-9394(72)90295-4
17. Ong SS, Ahmed I, Gonzales A, et al. Management of uncomplicated rhegmatogenous retinal detachments: a comparison of practice patterns and clinical outcomes in a real-world setting. Eye. 2022. doi:10.1038/s41433-022-02028-z
18. Brosh K, Francisconi CLM, Qian J, et al. Retinal displacement following pneumatic retinopexy vs pars plana vitrectomy for rhegmatogenous retinal detachment. JAMA Ophthalmol. 2020;138(6):652–659. doi:10.1001/jamaophthalmol.2020.1046
19. Farahvash A, Marafon SB, Juncal VR, et al. Understanding the mechanism of retinal displacement following rhegmatogenous retinal detachment repair: a computer simulation model. Acta Ophthalmol. 2021. doi:10.1111/aos.15050
20. Farahvash A, Marafon SB, Juncal VR, et al. Impact of tamponade agent on retinal displacement following pars plana vitrectomy for rhegmatogenous retinal detachment repair: a computer simulation model. Acta Ophthalmol. 2022. doi:10.1111/aos.15118
21. Francisconi CLM, Marafon SB, Figueiredo NA, et al. Retinal displacement after pneumatic retinopexy versus vitrectomy for rhegmatogenous retinal detachment (ALIGN). Ophthalmology. 2021:129(4):458–461.
22. Lee WW, Ramachandran A, Hamli H, et al. Immediate subretinal fluid displacement from the buoyant force of a small gas bubble in pneumatic retinopexy: insights into the potential mechanism of retinal displacement following retinal detachment repair. Retin Cases Brief Rep. 2021. doi:10.1097/ICB.0000000000001187
23. Mason RH, Minaker SA, Marafon SB, et al. Retinal displacement following rhegmatogenous retinal detachment: a systematic review and meta-analysis. Surv Ophthalmol. 2022;67(4):950–964. doi:10.1016/j.survophthal.2022.01.002
24. Muni RH, Felfeli T, Sadda SR, et al. Postoperative photoreceptor integrity following pneumatic retinopexy vs pars plana vitrectomy for retinal detachment repair: a post hoc optical coherence tomography analysis from the pneumatic retinopexy versus vitrectomy for the management of primary rhegmatogenous retinal detachment outcomes randomized trial. JAMA Ophthalmol. 2021;139(6):620–627. doi:10.1001/jamaophthalmol.2021.0803
25. Muni RH, Francisconi CLM, Felfeli T, et al. Vision-Related Functioning in Patients Undergoing pneumatic retinopexy vs vitrectomy for primary rhegmatogenous retinal detachment: a post hoc exploratory analysis of the PIVOT randomized clinical trial. JAMA Ophthalmol. 2020;138(8):826–833. doi:10.1001/jamaophthalmol.2020.2007
26. Rohowetz LJ, Shaheen AR, Russell JF, et al. Evaluation of retinal displacement following primary scleral buckling for macula-involving rhegmatogenous retinal detachment. Retina. 2022. doi:10.1097/IAE.0000000000003499
27. Chong DY, Fuller DG. The declining use of scleral buckling with vitrectomy for primary retinal detachments. Arch Ophthalmol. 2010;128(9):1206–1207. doi:10.1001/archophthalmol.2010.190
28. Starr MR, Hsu J, Yonekawa Y, et al. Surgical techniques for primary rhegmatogenous retinal detachments between surgeons with high versus low single surgery success rates. Acta Ophthalmol. 2021;99(8):e1501–e8. doi:10.1111/aos.14821
29. Machemer R. The importance of fluid absorption, traction, intraocular currents, and chorioretinal scars in the therapy of rhegmatogenous retinal detachments. XLI Edward Jackson memorial lecture. Am J Ophthalmol. 1984;98(6):681–693. doi:10.1016/0002-9394(84)90682-2
30. Wong D, Chan YK, Bek T, et al. Intraocular currents, Bernoulli’s principle and non-drainage scleral buckling for rhegmatogenous retinal detachment. Eye. 2018;32(2):213–221. doi:10.1038/eye.2017.312
31. Gonin J. Le Décollement de la Rétine. Pathogenié. Traitement. Lausanne: Librairie Payot & Cia Lausanne; 1934.
32. Vail DT. An inquiry into results of the established treatment of detachment of the retina and a new theory. Trans Am Acad Ophthalmol Otolaryngol. 1912;17:29.
33. Report of committee on detachment of the retina. Trans Ophthalmol Soc UK. 1916;36:352.
34. Wolfensberger TJ. Jules Gonin. Pioneer of retinal detachment surgery. Indian J Ophthalmol. 2003;51(4):303–308.
35. Gloor BP, Marmor MF. Controversy over the etiology and therapy of retinal detachment: the struggles of Jules Gonin. Surv Ophthalmol. 2013;58(2):184–195. doi:10.1016/j.survophthal.2012.09.002
36. Polkinghorne PJ. One hundred years of retinal detachment surgery. Br J Ophthalmol. 2016;100(10):1309–1311. doi:10.1136/bjophthalmol-2016-309113
37. Larsson S. Electro-endothermy in detachment of the retina. Arch Ophthalmol. 1932;7(5):661–680. doi:10.1001/archopht.1932.00820120011001
38. Pischel DK. Diathermy operation for retinal detachment; comparative results of different types of electrodes. Trans Am Ophthalmol Soc. 1944;42:543–567.
39. Wilkinson CP, Rice TA. History of retinal detachment surgery. In: Michels Retinal Detachment.
40. Jess A. Temporare Skleraleindellung als Hilfsmittel bei der Operation der Neetzhautablösung. Klin Monatsbl Augenheillkd. 1937;99:318.
41. Custodis E. Die Behandlung der Netzhautablösung durch umschriebene Diathermiekoagulation und einer mittels Plombenaufnähung erzeugten Eindellung der Sklera im Bereich des Risses. [Treatment of retinal detachment by circumscribed diathermy coagulation and indentation of the sclera in the area of the tear]. Klin Monatsbl Augenheillkd. 1956;129:476–495.
42. Schepens CL, Okamura ID, Brockhurst RJ. The scleral buckling procedures. I. Surgical techniques and management. AMA Arch Ophthalmol. 1957;58(6):797–811. doi:10.1001/archopht.1957.00940010819003
43. Lincoff HA, Baras I, McLean J. Modifications to the custodis procedure for retinal detachment. Arch Ophthalmol. 1965;73(2):160–163. doi:10.1001/archopht.1965.00970030162004
44. Rezaei KA, Abrams GW. The history of retinal detachment surgery. In: Kreissig I, editor. Primary Retinal Detachment: Options for Repair. Berlin, Heidelberg: Springer Berlin Heidelberg; 2005.
45. Lincoff H, Kreissig I. The treatment of retinal detachment without drainage of subretinal fluid. (Modifications of the Custodis procedure. VI). Trans Am Acad Ophthalmol Otolaryngol. 1972;76(5):1121–1133.
46. Lincoff HA, Nano H. A new needle for scleral surgery. Am J Ophthalmol. 1965;60(1):146–148. doi:10.1016/0002-9394(65)92414-1
47. Lincoff H, Gieser R. Finding the retinal hole. Arch Ophthalmol. 1971;85(5):565–569. doi:10.1001/archopht.1971.00990050567007
48. Bonnet M. Microsurgery for retinal detachment repair. Dev Ophthalmol. 1987;14:5–10.
49. Nawrocki J, Michalewska Z, Michalewski J. Optic Fibre Free Intravitreal Surgical System (OFFISS) in retinal detachment surgery. Ophthalmic Surg Lasers Imaging. 2008;39(6):466–470. doi:10.3928/15428877-20081101-10
50. Aras C, Ucar D, Koytak A, Yetik H. Scleral buckling with a non-contact wide-angle viewing system. Ophthalmologica. 2012;227(2):107–110. doi:10.1159/000333101
51. Chalam KV, Shah VA. Optics of wide-angle panoramic viewing system-assisted vitreous surgery. Surv Ophthalmol. 2004;49(4):437–445. doi:10.1016/j.survophthal.2004.04.010
52. Nagpal M, Bhardwaj S, Mehrotra N. Scleral buckling for rhegmatogenous retinal detachment using vitrectomy-based visualization systems and chandelier illumination. Asia Pac J Ophthalmol. 2013;2(3):165–168. doi:10.1097/APO.0b013e3182929b75
53. Roca JA, Maia M, da Cruz NFS, et al. Non-contact wide-angled visualization with chandelier-assisted scleral buckling for primary uncomplicated rhegmatogenous retinal detachment. Graefes Arch Clin Exp Ophthalmol. 2020;258(9):1857–1861. doi:10.1007/s00417-020-04737-1
54. Hu Y, Si S, Xu K, et al. Outcomes of scleral buckling using chandelier endoillumination. Acta Ophthalmol. 2017;95(6):591–594. doi:10.1111/aos.13326
55. Imai H, Tagami M, Azumi A. Scleral buckling for primary rhegmatogenous retinal detachment using noncontact wide-angle viewing system with a cannula-based 25 G chandelier endoilluminator. Clin Ophthalmol. 2015;9:2103–2107. doi:10.2147/OPTH.S91339
56. Jeon GS, Han JR. Effectiveness of scleral buckling with a wide-field surgical microscope and chandelier illumination in retinal detachment repair. Ophthalmologica. 2019;242(1):31–37. doi:10.1159/000496165
57. Kita M, Kusaka M, Yamada H, Hama S. Updated chandelier illumination-assisted scleral buckling using 3D visualization system. Clin Ophthalmol. 2019;13:1743–1748. doi:10.2147/OPTH.S218975
58. Narayanan R, Tyagi M, Hussein A, et al. Scleral buckling with wide-angled endoillumination as a surgical educational tool. Retina. 2016;36(4):830–833. doi:10.1097/IAE.0000000000000792
59. Nossair AA, Ewais WA, Eissa SA. Chandelier-assisted scleral buckling using wide angle viewing contact lens for pseudophakic retinal detachment repair. Int J Ophthalmol. 2019;12(4):627–633. doi:10.18240/ijo.2019.04.17
60. Seider MI, Nomides RE, Hahn P, et al. Scleral buckling with chandelier illumination. J Ophthalmic Vis Res. 2016;11(3):304–309. doi:10.4103/2008-322X.188402
61. Tomita Y, Kurihara T, Uchida A, et al. Wide-angle viewing system versus conventional indirect ophthalmoscopy for scleral buckling. Sci Rep. 2015;5(1):13256. doi:10.1038/srep13256
62. Cohen E, Rosenblatt A, Bornstein S, et al. Wide-angled endoillumination vs traditional scleral buckling surgery for retinal detachment - a comparative study. Clin Ophthalmol. 2019;13:287–293. doi:10.2147/OPTH.S182751
63. Caporossi T, Finocchio L, Barca F, et al. Scleral buckling for primary rhegmatogenous retinal detachment using a noncontact wide-angle viewing system with a cannula-based 27-G Chandelier endoilluminator. Retina. 2019;39(Suppl 1):S144–S50. doi:10.1097/IAE.0000000000001891
64. Li XJ, Yang XP, Lyu XB. Comparison of scleral buckling using wide-angle viewing systems and indirect ophthalmoscope for rhegmatogenous retinal detachment. Int J Ophthalmol. 2016;9(9):1310–1314. doi:10.18240/ijo.2016.09.13
65. Zhao T, Yan Y, Chen Y, et al. Endo-illumination-aided scleral buckling combined with intravitreal injection of hyaluronate for treatment of rhegmatogenous retinal detachment. Ophthalmologica. 2020;243(4):316–322. doi:10.1159/000504714
66. Albalkini AS, Abdullatif AM, Albalkini MS, et al. Chandelier-assisted versus standard scleral buckling for primary rhegmatogenous retinal detachment: a randomized clinical study. Retina. 2022. doi:10.1097/IAE.0000000000003519
67. Bawankule PK, Narnaware SH, Chakraborty M, et al. Digitally assisted three-dimensional surgery - beyond vitreous. Indian J Ophthalmol. 2021;69(7):1793–1800. doi:10.4103/ijo.IJO_3111_20
68. La Spina C, Del Turco C, Bogetto C, et al. Wide-angle 3D viewing system with valved trocar applied to chandelier-assisted scleral buckling. Eur J Ophthalmol. 2021;31(2):804–806. doi:10.1177/1120672120945091
69. Zhang Z, Wang L, Wei Y, et al. The preliminary experiences with three-dimensional heads-up display viewing system for vitreoretinal surgery under various status. Curr Eye Res. 2019;44(1):102–109. doi:10.1080/02713683.2018.1526305
70. Eckardt C, Paulo EB. Heads-up surgery for vitreoretinal procedures: an experimental and clinical study. Retina. 2016;36(1):137–147. doi:10.1097/IAE.0000000000000689
71. Freeman WR, Chen KC, Ho J, et al. Resolution, depth of field, and physician satisfaction during digitally assisted vitreoretinal surgery. Retina. 2019;39(9):1768–1771. doi:10.1097/IAE.0000000000002236
72. AlAkeely AG, Alageely A, Alageely O. Heads up sutureless chandelier assisted scleral buckle. Am J Ophthalmol Case Rep. 2020;20:100900. doi:10.1016/j.ajoc.2020.100900
73. Michels RG. Scleral buckling methods for rhegmatogenous retinal detachment. Retina. 1986;6(1):1–49. doi:10.1097/00006982-198600610-00002
74. Yannuzzi NA, Patel NA, Berrocal AM, Sridhar J. Encircling scleral buckle with chandelier endoillumination and endolaser for repair of rhegmatogenous retinal detachment. Clin Ophthalmol. 2020;14:609–612. doi:10.2147/OPTH.S238241
75. Lincoff H. The rationale for radial buckling. Mod Probl Ophthalmol. 1974;12:484–491.
76. Lincoff H. Radial buckling in the repair of retinal detachment. Int Ophthalmol Clin. 1976;16(1):127–134. doi:10.1097/00004397-197601610-00012
77. Lincoff H, Kreissig I. Advantages of radial buckling. Am J Ophthalmol. 1975;79(6):955–957. doi:10.1016/0002-9394(75)90677-7
78. Kreissig I, Simader E, Fahle M, Lincoff H. Visual acuity after segmental buckling and non-drainage: a 15-year follow-up. Eur J Ophthalmol. 1995;5(4):240–246. doi:10.1177/112067219500500408
79. Norton EW. Retinal detachment in Aphakia. Am J Ophthalmol. 1964;58:111–124. doi:10.1016/0002-9394(64)90600-2
80. Ankamah E, Siemerink MJ, Polkinghorne PJ, et al. Internal drainage of subretinal fluid during chandelier-assisted scleral buckling. Retin Cases Brief Rep. 2022;16(1):77–80. doi:10.1097/ICB.0000000000000921
81. Hammer ME, Burch TG, Rinder D. Viscosity of subretinal fluid and its clinical correlations. Retina. 1986;6(4):234–238. doi:10.1097/00006982-198606040-00008
82. Hilton GF, Grizzard WS, Avins LR, Heilbron DC. The drainage of subretinal fluid: a randomized controlled clinical trial. Retina. 1981;1(4):271–280. doi:10.1097/00006982-198101040-00002
83. Wilkinson CP, Bradford RH
84. Okamura JD, Schepens CL, Brockhurst RJ, et al. Scleral buckling procedures. IX. Complications during operation. Arch Ophthalmol. 1966;75(5):615–625. doi:10.1001/archopht.1966.00970050617006
85. English JF, Barry R, Essex RW. Postoperative endophthalmitis following chandelier-assisted scleral buckle for primary repair of rhegmatogenous retinal detachment. Acta Ophthalmol. 2019;97(1):e130–e1. doi:10.1111/aos.13764
86. Sakono T, Otsuka H, Shiihara H, et al. Acute bacterial endophthalmitis after scleral buckling surgery with chandelier endoillumination. Am J Ophthalmol Case Rep. 2017;8:7–10. doi:10.1016/j.ajoc.2017.07.007
87. Papakostas TD, Vavvas D. Postoperative complications of scleral buckling. Semin Ophthalmol. 2018;33(1):70–74. doi:10.1080/08820538.2017.1353816
88. Velez FG. A 2020 update on 20/20 X 2 diplopia after ocular surgery: strabismus following retinal detachment surgery. J Binocul Vis Ocul Motil. 2021;71(4):132–137.
89. Ung T, Comer MB, Ang AJ, et al. Clinical features and surgical management of retinal detachment secondary to round retinal holes. Eye. 2005;19(6):665–669. doi:10.1038/sj.eye.6701618
90. Kennedy CJ, Parker CE, McAllister IL. Retinal detachment caused by retinal dialysis. Aust N Z J Ophthalmol. 1997;25(1):25–30. doi:10.1111/j.1442-9071.1997.tb01271.x
91. Kinyoun JL, Knobloch WH. Idiopathic retinal dialysis. Retina. 1984;4(1):9–14. doi:10.1097/00006982-198400410-00003
92. Hollander DA, Irvine AR, Poothullil AM, Bhisitkul RB. Distinguishing features of nontraumatic and traumatic retinal dialyses. Retina. 2004;24(5):669–675.
93. Smiddy WE, Green WR. Retinal dialysis: pathology and pathogenesis. Retina. 1982;2(2):94–116. doi:10.1097/00006982-198200220-00007
94. Chang JS, Marra K, Flynn HW
95. Qiang Kwong T, Shunmugam M, Williamson TH. Characteristics of rhegmatogenous retinal detachments secondary to retinal dialyses. Can J Ophthalmol. 2014;49(2):196–199. doi:10.1016/j.jcjo.2013.12.013
96. Jan S, Hussain Z, Khan U, et al. Retinal detachment due to retinal dialysis: surgical outcome after scleral buckling. Asia Pac J Ophthalmol. 2015;4(5):259–262. doi:10.1097/APO.0000000000000084
97. Muni RH, Bansal A, Lee WW, Escaf LC. Minimal gas vitrectomy with scleral buckle to minimize retinal displacement in rhegmatogenous retinal detachment with inferior breaks. Retin Cases Brief Rep. 2021. doi:10.1097/ICB.0000000000001174
98. Muni RH, Felfeli T, Figueiredo N, et al. Minimal gas vitrectomy technique for reducing risk of retinal displacement following rhegmatogenous retinal detachment repair. Retin Cases Brief Rep. 2020. doi:10.1097/ICB.0000000000001076
99. Popovic MM, Muni RH, Nichani P, Kertes PJ. Pars plana vitrectomy, scleral buckle, and pneumatic retinopexy for the management of rhegmatogenous retinal detachment: a meta-analysis. Surv Ophthalmol. 2022;67(1):184–196. doi:10.1016/j.survophthal.2021.05.008
100. Dhoot AS, Popovic MM, Nichani PAH, et al. Pars plana vitrectomy versus scleral buckle: a comprehensive meta-analysis of 15,947 eyes. Surv Ophthalmol. 2021;67(4):932–949. doi:10.1016/j.survophthal.2021.12.005
101. Eshtiaghi A, Dhoot AS, Mihalache A, et al. Pars plana vitrectomy with and without supplemental scleral buckle for the repair of rhegmatogenous retinal detachment: a meta-analysis. Ophthalmol Retina. 2022. doi:10.1016/j.oret.2022.02.009
102. Sena DF, Kilian R, Liu SH, et al. Pneumatic retinopexy versus scleral buckle for repairing simple rhegmatogenous retinal detachments. Cochrane Database Syst Rev. 2021:11):CD008350.
103. Reeves MR, Afshar AR, Pershing S. Need for retinal detachment reoperation based on primary repair method among commercially insured patients, 2003–2016. Am J Ophthalmol. 2021;229:71–81. doi:10.1016/j.ajo.2021.04.007
104. Committee TAoUPoOAfc. Surgical retinal fellow volume registry; 2021.
105. Joseph DP, Ryan EH, Ryan CM, et al. Primary retinal detachment outcomes study: pseudophakic retinal detachment outcomes: primary retinal detachment outcomes study report number 3. Ophthalmology. 2020;127(11):1507–1514. doi:10.1016/j.ophtha.2020.05.005
106. Ryan EH, Ryan CM, Forbes NJ, et al. Primary retinal detachment outcomes study report number 2: phakic retinal detachment outcomes. Ophthalmology. 2020;127(8):1077–1085. doi:10.1016/j.ophtha.2020.03.007
107. Hillier RJ, Felfeli T, Berger AR, et al. The pneumatic retinopexy versus vitrectomy for the management of primary rhegmatogenous retinal detachment outcomes randomized trial (PIVOT). Ophthalmology. 2019;126(4):531–539. doi:10.1016/j.ophtha.2018.11.014
108. Muni RH, Minaker SA, Mason RH, et al. Novel classification system for management of rhegmatogenous retinal detachment with minimally invasive detachment surgery: a network meta-analysis of randomized trials focused on patient-centred outcomes. Can J Ophthalmol. 2021. doi:10.1016/j.jcjo.2021.10.002
109. Ng H, Vermeer KA, van Meurs JC, La Heij EC. Visual acuity inadequately reflects vision-related quality of life in patients after macula-off retinal detachment surgery. Invest Ophthalmol Vis Sci. 2020;61(10):34. doi:10.1167/iovs.61.10.34
110. Okamoto F, Sugiura Y, Okamoto Y, et al. Aniseikonia and foveal microstructure after retinal detachment surgery. Invest Ophthalmol Vis Sci. 2014;55(8):4880. doi:10.1167/iovs.14-14618
111. Murakami T, Okamoto F, Sugiura Y, et al. Changes in aniseikonia and influencing-factors following successful macula-off retinal detachment surgery. Sci Rep. 2019;9(1):11588. doi:10.1038/s41598-019-48112-5
112. Fukuyama H, Ishikawa H, Komuku Y, et al. Comparative analysis of metamorphopsia and aniseikonia after vitrectomy for epiretinal membrane, macular hole, or rhegmatogenous retinal detachment. PLoS One. 2020;15(5):e0232758. doi:10.1371/journal.pone.0232758
113. van de Put MA, Vehof J, Hooymans JM, Los LI. Postoperative metamorphopsia in macula-off rhegmatogenous retinal detachment: associations with visual function, vision related quality of life, and optical coherence tomography findings. PLoS One. 2015;10(4):e0120543. doi:10.1371/journal.pone.0120543
114. Lina G, Xuemin Q, Qinmei W, Lijun S. Vision-related quality of life, metamorphopsia, and stereopsis after successful surgery for rhegmatogenous retinal detachment. Eye. 2016;30(1):40–45. doi:10.1038/eye.2015.171
115. Okamoto F, Sugiura Y, Okamoto Y, et al. Metamorphopsia and optical coherence tomography findings after rhegmatogenous retinal detachment surgery. Am J Ophthalmol. 2014;157(1):214–20 e1. doi:10.1016/j.ajo.2013.08.007
116. Zhou C, Lin Q, Chen F. Prevalence and predictors of metamorphopsia after successful rhegmatogenous retinal detachment surgery: a cross-sectional, comparative study. Br J Ophthalmol. 2017;101(6):725–729. doi:10.1136/bjophthalmol-2016-309097
117. Okuda T, Higashide T, Sugiyama K. Metamorphopsia and outer retinal morphologic changes after successful vitrectomy surgery for macula-off rhegmatogenous retinal detachment. Retina. 2018;38(1):148–154. doi:10.1097/IAE.0000000000001510
118. Saleh M, Gauthier AS, Delbosc B, Castelbou M. Impact of metamorphopsia on quality of life after successful retinal detachment surgery. Ophthalmologica. 2018;240(3):121–128. doi:10.1159/000486164
119. Lee E, Williamson TH, Hysi P, et al. Macular displacement following rhegmatogenous retinal detachment repair. Br J Ophthalmol. 2013;97(10):1297–1302. doi:10.1136/bjophthalmol-2013-303637
120. Figueiredo N, Sarraf D, Gunnemann F, et al. Longitudinal assessment of ellipsoid zone recovery using en face optical coherence tomography after retinal detachment repair. Am J Ophthalmol. 2021;236:212–220. doi:10.1016/j.ajo.2021.10.012
121. Lee WW, Bansal A, Sadda SR, et al. Outer retinal folds after pars plana vitrectomy vs. pneumatic retinopexy for retinal detachment repair: post hoc analysis from PIVOT. Ophthalmol Retina. 2021;6(3):234–242. doi:10.1016/j.oret.2021.09.001
122. Dell’Omo R, Mura M, Lesnik Oberstein SY, et al. Early simultaneous fundus autofluorescence and optical coherence tomography features after pars plana vitrectomy for primary rhegmatogenous retinal detachment. Retina. 2012;32(4):719–728. doi:10.1097/IAE.0b013e31822c293e
123. Casswell EJ, Yorston D, Lee E, et al. Effect of face-down positioning vs support-the-break positioning after macula-involving retinal detachment repair: the PostRD randomized clinical trial. JAMA Ophthalmol. 2020;138(6):634–642. doi:10.1001/jamaophthalmol.2020.0997
124. Shiragami C, Shiraga F, Yamaji H, et al. Unintentional displacement of the retina after standard vitrectomy for rhegmatogenous retinal detachment. Ophthalmology. 2010;117(1):86–92 e1. doi:10.1016/j.ophtha.2009.06.025
125. dell’Omo R, Semeraro F, Guerra G, et al. Short-time prone posturing is well-tolerated and reduces the rate of unintentional retinal displacement in elderly patients operated on for retinal detachment. BMC Surg. 2013;13(Suppl 2):S55. doi:10.1186/1471-2482-13-S2-S55
126. Shiragami C, Fukuda K, Yamaji H, et al. A method to decrease the frequency of unintentional slippage after vitrectomy for rhegmatogenous retinal detachment. Retina. 2015;35(4):758–763. doi:10.1097/IAE.0000000000000383
127. dell’Omo R, Scupola A, Viggiano D, et al. Incidence and factors influencing retinal displacement in eyes treated for rhegmatogenous retinal detachment with vitrectomy and gas or silicone oil. Invest Ophthalmol Vis Sci. 2017;58(6):BIO191–BIO9. doi:10.1167/iovs.17-21466
128. Codenotti M, Fogliato G, Iuliano L, et al. Influence of intraocular tamponade on unintentional retinal displacement after vitrectomy for rhegmatogenous retinal detachment. Retina. 2013;33(2):349–355. doi:10.1097/IAE.0b013e318263d180
129. Schocket LS, Witkin AJ, Fujimoto JG, et al. Ultrahigh-resolution optical coherence tomography in patients with decreased visual acuity after retinal detachment repair. Ophthalmology. 2006;113(4):666–672. doi:10.1016/j.ophtha.2006.01.003
130. Smith AJ, Telander DG, Zawadzki RJ, et al. High-resolution Fourier-domain optical coherence tomography and microperimetric findings after macula-off retinal detachment repair. Ophthalmology. 2008;115(11):1923–1929. doi:10.1016/j.ophtha.2008.05.025
131. Nakanishi H, Hangai M, Unoki N, et al. Spectral-domain optical coherence tomography imaging of the detached macula in rhegmatogenous retinal detachment. Retina. 2009;29(2):232–242. doi:10.1097/IAE.0b013e31818bcd30
132. Lai WW, Leung GY, Chan CW, et al. Simultaneous spectral domain OCT and fundus autofluorescence imaging of the macula and microperimetric correspondence after successful repair of rhegmatogenous retinal detachment. Br J Ophthalmol. 2010;94(3):311–318. doi:10.1136/bjo.2009.163584
133. Gharbiya M, Grandinetti F, Scavella V, et al. Correlation between spectral-domain optical coherence tomography findings and visual outcome after primary rhegmatogenous retinal detachment repair. Retina. 2012;32(1):43–53. doi:10.1097/IAE.0b013e3182180114
134. Kobayashi M, Iwase T, Yamamoto K, et al. Association between photoreceptor regeneration and visual acuity following surgery for rhegmatogenous retinal detachment. Invest Ophthalmol Vis Sci. 2016;57(3):889–898. doi:10.1167/iovs.15-18403
135. Abraham JR, Srivastava SK, Reese JL, Ehlers JP. Intraoperative OCT features and postoperative ellipsoid mapping in primary macula-involving retinal detachments from the PIONEER study. Ophthalmol Retina. 2019;3(3):252–257. doi:10.1016/j.oret.2018.10.006
136. Benson SE, Schlottmann PG, Bunce C, et al. Optical coherence tomography analysis of the macula after vitrectomy surgery for retinal detachment. Ophthalmology. 2006;113(7):1179–1183. doi:10.1016/j.ophtha.2006.01.039
137. Enoch JM, Van Loo JA
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.