")
Back to Journals » Clinical Ophthalmology » Volume 9
Scleral buckle hemorrhagic cyst masquerading as an orbital tumor
Authors Almeida D, Chin E , Boldt C, Mahajan V
Received 24 October 2014
Accepted for publication 26 November 2014
Published 13 February 2015 Volume 2015:9 Pages 343—345
DOI https://doi.org/10.2147/OPTH.S76351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
David RP Almeida,1 Eric K Chin,1 H Culver Boldt,1 Vinit B Mahajan1,2
1Department of Ophthalmology and Visual Sciences; 2Omics Laboratory, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
Abstract: We present a case of a 41-year-old man who was referred for evaluation of a choroidal tumor with a remote history of scleral buckle placement for traumatic retinal detachment. Ocular imaging, echography, and magnetic resonance imaging could not rule out a neoplastic process so the patient was taken for surgical exploration where a hemorrhagic cyst was discovered. This is the first case in the literature of a silicone scleral buckle–associated hemorrhagic cyst presenting as orbital mass.
Keywords: choroidal mass, choroidal lesion, choroidal melanoma, echography, optical coherence tomography, magnetic resonance imaging
Introduction
Scleral buckle (SB) placement is a common procedure for the management of rhegmatogenous retinal detachments. Complications from SB surgery include exposure or migration, infection, strabismus, and foreign body sensation.1 There have been cases of expansile hydrogel SBs simulating orbital masses2,3 but here we report the first case of a silicone SB with a periocular hemorrhagic cyst masquerading as an orbital tumor.
Case report
A 41-year-old man was referred for evaluation of a choroidal tumor. He had decreased vision and a new nasal visual field defect OS. There was no recent trauma or eye surgery; however, at 10 years of age he underwent SB procedure for a traumatic retinal detachment in his OS. Operative reports indicated that a segmental concave 281-type silicone tire was placed superotemporally. He was being treated with aspirin, lisinopril, and metoprolol for chronic heart failure. There was no history of cancer.
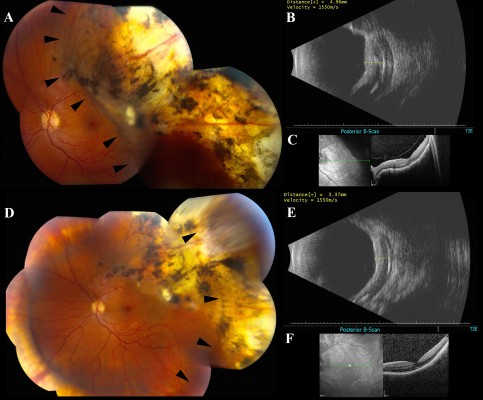
His vision measured 20/20 OD and 20/150 OS and his intraocular pressure was 18 mmHg OU. A dilated fundus exam OS suggested that there was an elevated choroidal mass in the superotemporal mid-periphery with overlying chorioretinal scarring and a buckle with moderate height (Figure 1A). Echography detected an extrascleral lesion outside the choroid between the SB and the globe centered at 2 o’clock with a maximum apical thickness of 4.96 mm (Figure 1B). Optical coherence tomography (OCT) displayed distortion of the outer retina and choroid with intact retinal pigment epithelium (Figure 1C).
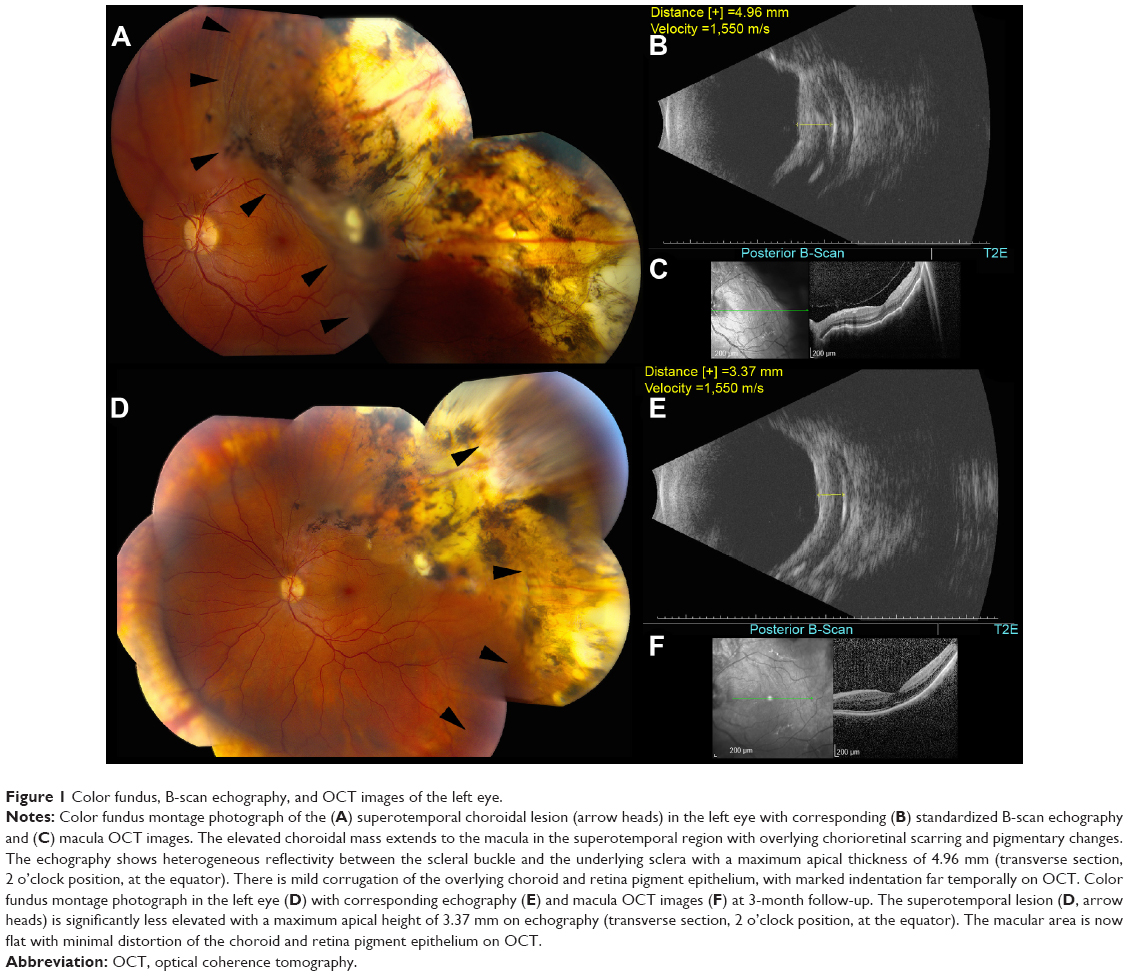 | Figure 1 Color fundus, B-scan echography, and OCT images of the left eye. |
Magnetic resonance imaging (MRI) of the orbits and brain revealed a relatively homogeneous crescent mass between the globe and SB (Figure 2A). Consistent with a 281-style concave silicone tire, the anterior–posterior chord length of the SB element measured 12.5 mm (Figure 2C), and extended circumferentially around the globe from 11.30 to clockwise 4 o’clock (Figure 2B). No other scans other than the native T1 sequences were done and this is a limitation of the study. Consequently, because of his concern for an orbital neoplastic process, the patient underwent orbital exploration; pathology revealed a hemorrhagic cyst within the silicone SB capsule and no neoplastic tissue. The patient began oral prednisone 60 mg daily with a taper over 3 weeks, as an anti-inflammatory agent to minimize tissue edema of the hemorrhagic cyst.
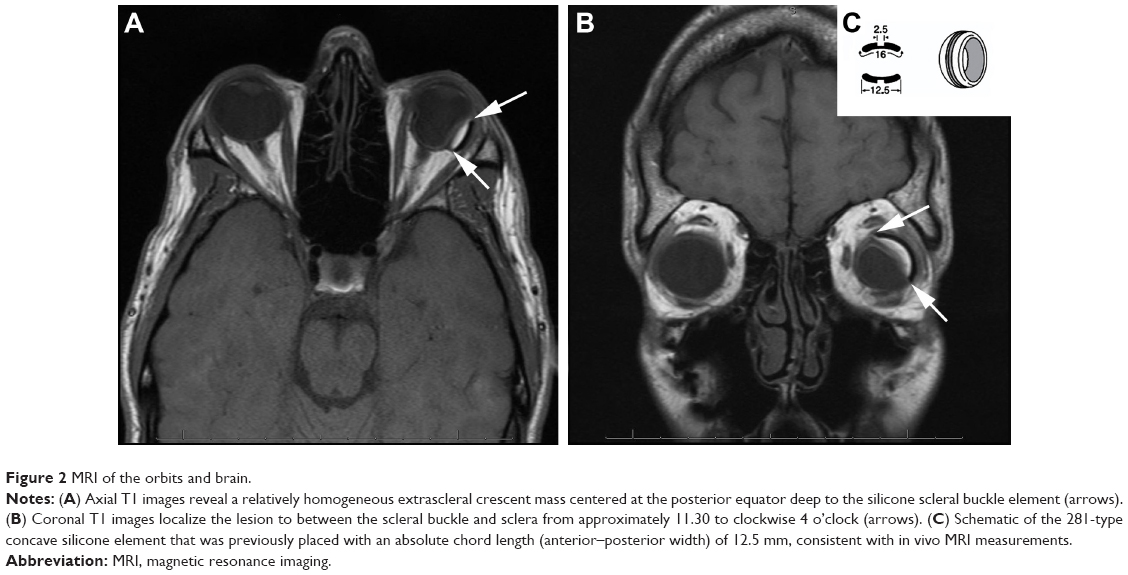 | Figure 2 MRI of the orbits and brain. |
Over the next 3 months, the patient’s visual field defect resolved. The choroidal indentation became progressively smaller (Figure 1D) and the visual acuity improved to his baseline of 20/40. Echography showed a decreased maximum apical height of 3.37 mm (Figure 1E). The temporal macula flattened with minimal distortion of the choroid on OCT (Figure 1F). A recurrent episode resolved without surgery using only oral prednisone.
Discussion
Orbital foreign body simulating an ocular tumor is uncommon, occurring in less than 1% of cases presenting with an intraorbital mass.4 Even less common is SB presenting as an orbital lesion with enlargement of the SB elements. To date, these reports have involved the use of hydrogel implants (MIRAgel; Waltham, MA, USA), which were popular in the 1980s and early 1990s before being discontinued. These hydrogel implants were marketed as soft, flexible implants with physical properties allowing them to swell over time. The implant was discontinued due to complications, and it is currently recommended that MIRAgel buckling elements be promptly removed at the onset of discomfort to avoid late complications.5
We present the first case of a silicone SB-associated hemorrhagic cyst presenting as an orbital mass. Silicone is inert and unable to enlarge like hydrogel implants; consequently, the possibility of this type of SB presenting as an orbital mass has not been previously reported. Clinicians should be aware of this entity in patients with a previous silicone SB. Standardized echography and MRI imaging can localize the mass between the SB and sclera, for which the changes in choroidal elevation are secondary to the mass effect from the hemorrhagic cyst.
Ethics statement
Full adherence to the Declaration of Helsinki and all Federal and State laws was observed.
Author contributions
Dr Almeida and Dr Mahajan had full access to all the data in the study and take full responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed to the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, and approval of the manuscript; and the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
Covert DJ, Wirostko WJ, Han DP, et al. Risk factors for scleral buckle removal: a matched, case-control study. Am J Ophthalmol. 2008;146(3):434–439. | ||
Roldán-Pallarés M, del Castillo Sanz JL, Awad-El Susi S, Refojo MF. Long-term complications of silicone and hydrogel explants in retinal reattachment surgery. Arch Ophthalmol. 1999;117(2):197–201. | ||
Shields CL, Demirci H, Marr BP, Mashayekhi A, Materin MA, Shields JA. Expanding MIRAgel scleral buckle simulating an orbital tumor in four cases. Ophthal Plast Reconstr Surg. 2005;21(1):32–38. | ||
Shields JA, Shields CL, Scartozzi R. Survey of 1,264 patients with orbital tumors and simulating lesions: The 2002 Montgomery Lecture, part 1. Ophthalmology. 2004;111(5):997–1008. | ||
Roldán-Pallarés M, Hernández-Montero J, Llanes F, Fernández-Rubio JE, Ortega F. MIRAgel: hydrolytic degradation and long-term observations. Arch Ophthalmol. 2007;125(4):511–514. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.