")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Safety of high-dose daptomycin in patients with severe renal impairment
Authors Tai CH, Shao CH, Chen CY, Lin SW , Wu CC
Received 12 December 2017
Accepted for publication 22 February 2018
Published 13 March 2018 Volume 2018:14 Pages 493—499
DOI https://doi.org/10.2147/TCRM.S159587
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Chih-Hsun Tai,1 Chi-Hao Shao,2 Chen-You Chen,2 Shu-Wen Lin,1–3 Chien-Chih Wu1,2
1Department of Pharmacy, National Taiwan University Hospital, College of Medicine, National Taiwan University, Taipei, Taiwan; 2School of Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan; 3Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan
Background: Treatment options are limited for infections due to multidrug-resistant Gram-positive pathogens. Daptomycin is a lipopeptide antibiotic with concentration-dependent killing characteristic and dose-dependent post-antibiotic effect. To achieve optimized pharmacodynamic effect, some experts advocated using a high dose of daptomycin (≥9 mg/kg) for severe infections. However, the safety of high-dose therapy in patients with renal impairment remains unknown. This study was aimed to evaluate the safety of daptomycin in patients with severe renal impairment.
Methods: This was a retrospective study performed by reviewing electronic medical records. Patients with severe renal impairment who were treated with daptomycin in a tertiary teaching hospital between January 1, 2013, and June 30, 2016, were included for evaluation. The incidence rates of creatine kinase (CK) elevation between high-dose (≥9 mg/kg) and standard-dose (<9 mg/kg) groups were compared.
Results: Overall, 164 patients met the inclusion criteria, and 114 (69.5%) of them were on renal replacement therapy. Vancomycin-resistant enterococci were the most common pathogens (61.3%) of the patients with documented pathogens. The treatment success rate was 51.6% in the 91 patients with bacteremia. The average dose of daptomycin was 8.0±2.3 mg/kg, and 37 (22.6%) patients received ≥9 mg/kg. CK levels were followed in 108 (65.9%) patients. Significantly higher incidence of CK elevation was found in the high-dose group compared with that in the standard-dose group (10.8% vs 1.6%, P<0.05). Moreover, patients with elevated CK received a higher dose of daptomycin than those without (9.3±1.2 vs 7.9±2.3 mg/kg, P<0.05). There was no significant difference in the rate of CK elevation between patients treated with different dosing frequency or with the concurrent use of statins, fibrate, or colchicine.
Conclusions: In patients with severe renal impairment, high-dose (≥9 mg/kg) daptomycin therapy may result in a significantly higher incidence of CK elevation. More frequent CK monitoring is warranted to avoid potential harm in this population.
Keywords: daptomycin, safety, renal impairment, rhabdomyolysis
Introduction
Infections caused by multidrug-resistant Gram-positive pathogens, such as methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE), usually result in significant morbidity and mortality. According to the Taiwan surveillance data, the proportion of VRE among all enterococcal isolates causing nosocomial infections in intensive care units (ICUs) in medical centers increased from 12.4% in 2007 to 42.9% in 2016, and the proportion of MRSA among all staphylococcus isolates decreased from 83.7% in 2007 to 68.5% in 2016.1 However, therapeutic options for these resistant pathogens are limited, particularly for strains with high minimum inhibitory concentration.
Daptomycin is a lipopeptide antibiotic approved for the treatment of Gram-positive pathogens-associated complicated skin infections and bacteremia. The recommended dose is 4–6 mg/kg once daily by manufacturer information. The optimal dose for certain difficult-to-treat infections has not been defined. Because of its characteristic of concentration-dependent killing and dose-dependent post-antibiotic effect, recent guidelines advocated increasing daptomycin dose to 8–10 mg/kg once daily to optimize therapy for infective endocarditis.2,3 Indeed, a multicenter prospective cohort study conducted at our hospital system revealed that high-dose daptomycin (≥9 mg/kg/day) was associated with better survival rates in the treatment of VRE bacteremia.4 In the present study, we adapted the same criteria and defined daptomycin use of ≥9 mg/kg/day as the high dose, and that <9 mg/kg/day was defined as the standard dose.
The major safety concern with daptomycin is the elevation of creatine kinase (CK) level, which may progress to rhabdomyolysis. Although the incidence of CK elevation was quite low, few studies examined the safety of daptomycin in patients with renal impairment, and most of the study populations were treated with the standard dose of <9 mg/kg.5–8 Accumulation of daptomycin was documented in patients with renal impairment due to decreasing renal clearance,9 and the previous study showed that higher daptomycin trough concentration (>24.3 mg/L) was associated with a higher probability of CK elevation. Therefore, the primary aim of this study was to investigate the safety of daptomycin use in this fragile population.
Methods
Study design and setting
This was a retrospective single-center study conducted at National Taiwan University Hospital (NTUH), a 2600-bed tertiary medical center located in Taipei City, Taiwan. The Research Ethics Committee of NTUH approved the study protocol (201503064RINB). The requirement for informed consent was waived because of the retrospective nature of the study and using data from which the patients’ identification information had been removed.
Patient inclusion and data collection
We retrospectively reviewed the electronic medical records for data collection. All adult patients treated with daptomycin at NTUH from January 1, 2013, to June 30, 2016, were included if they had renal impairment. Patients were excluded if the medical records were incomplete or the treatment duration of daptomycin was <3 days. A standardized case report form was used to collect data including demographic characteristics (age, gender, body weight, body height, body mass index [BMI]), creatinine clearance (CLCr), type of renal replacement therapy, concurrent use of medication (statins, fibrates, and colchicine), and use of antimicrobial agents, isolated pathogens, indications for daptomycin, dosage, dosing frequency, treatment duration and response, frequency of CK monitoring, and CK level.
Definition
Renal impairment was defined as CLCr <30 mL/min or receiving renal replacement therapy. The Cockcroft–Gault equation was used to calculate CLCr.10 Patients with a BMI ≥30 were considered obese according to WHO definition. High-dose daptomycin therapy was defined as doses of daptomycin ≥9 mg/kg, and doses <9 mg/kg were defined as the standard dose. Daptomycin treatment success was defined by resolving clinical signs and symptoms, no additional antibiotic therapy, and eradication of the causative pathogen documented at the end of daptomycin therapy. Elevated CK level was defined as CK level >1,000 U/L during daptomycin therapy. Evaluation of daptomycin-related CK elevation was based on the judgment of two clinical pharmacists who retrospectively reviewed the medical records. Surgery, trauma, and seizure attack during daptomycin therapy were considered the possible causes for CK elevation, and subjects were excluded for safety analysis if these conditions were attributed to the main causes for CK elevation according to the clinical pharmacists’ judgment. Patients with no record of CK level during the treatment course were considered as no CK elevation. The primary outcome was to compare the percentages of patients with elevated CK between the groups receiving high doses vs standard doses of daptomycin.
Statistical analysis
Data were described as means ± SDs or numbers with percentages. The Mann–Whitney U-test was used for continuous data; either chi-square or Fisher’s exact test was used for categorical data. A P-value ≤0.05 was considered statistically significant. Multivariate logistic regression was performed to identify the factors associated with CK elevation. Explanatory variables were included in the multivariate analysis if they showed significance in univariate analysis (P<0.2). The statistical analysis was performed by Microsoft Office Excel 2003 (Microsoft, Redmond, WA, USA) and SPSS 18 (SPSS Inc, Chicago, IL, USA).
Results
Patient characteristics
From January 1, 2013, through June 30, 2016, 365 patients treated with daptomycin were screened, and 164 patients met the inclusion criteria. The demographic characteristics of the patients included are listed in Table 1. Patients had a mean age of 68.1±16.5 years, and 62.2% were >65 years old. Eighty-seven patients (53.0%) were male, and 10 patients (6%) were obese. One hundred and seven patients (65.2%) were admitted in ICU. There were 114 patients (69.5%) who received concurrent renal replacement therapy during the treatment course. Before the use of daptomycin, 105 (64%) patients received other antibiotic treatments. More patients in high-dose group had been treated with other antibiotic before daptomycin than those in the standard-dose group (81.1% vs 59.1%, respectively; P=0.014). Significant differences in body weight existed between high- and standard-dose groups (P<0.001); there was only one obese patient in the high-dose group, whereas nine patients were obese in the standard-dose group.
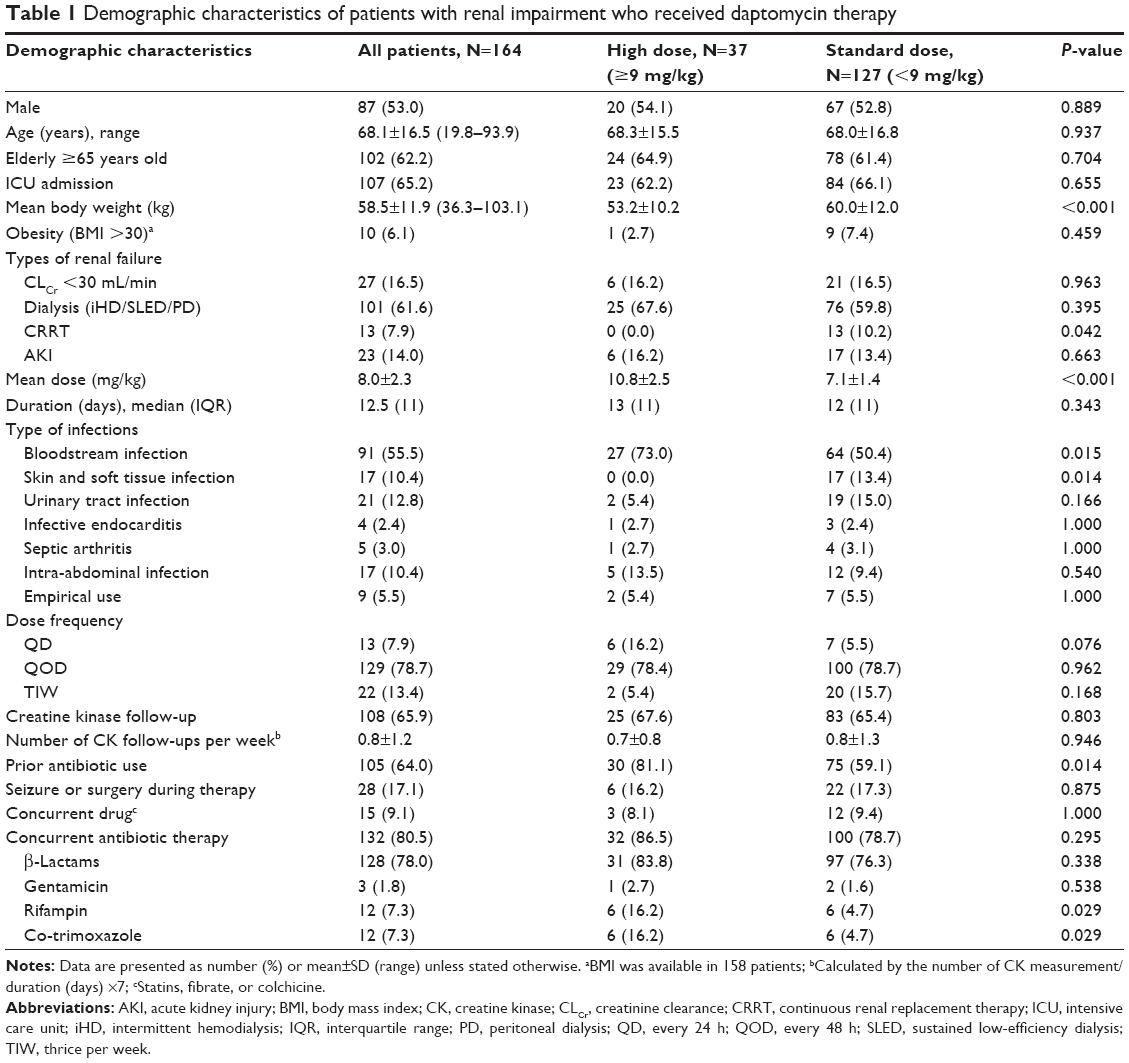 | Table 1 Demographic characteristics of patients with renal impairment who received daptomycin therapy |
Antimicrobial therapy and microbiological results
The most documented type of infection treated with daptomycin was bloodstream infection (55.5%), followed by urinary tract infection (12.8%) and intra-abdominal infection (11.0%). VRE was the most frequently isolated pathogen (61.3%) among the 142 patients with documented pathogens. The mean daptomycin dose was 8.0±2.3 mg/kg, and 37 (22.6%) patients received the high dose (≥9 mg/kg) of daptomycin therapy. The dosing frequency of every 48 h was prescribed in 129 patients (78.7%). The median treatment duration was 12.5 (11) days. One hundred and thirty-two patients had concurrent antibiotic therapy including β-lactams (78%), rifampin (7.3%), co-trimoxazole (7.3%), and gentamicin (1.8%). In our study, obese patients received a significantly lower dose of daptomycin than nonobese patients (6.8±1.7 vs 8.1±2.3 mg/kg, P=0.027).
Treatment safety and response
CK levels were measured in 108 (65.9%) patients. Six patients had significant CK elevation during daptomycin therapy, and three of them had muscle symptoms, as detailed in Table 2. Recovery from CK elevation was observed in all patients after the discontinuation of daptomycin treatment. We also found a significantly higher incidence rate of CK elevation in the high-dose group compared with that in the standard-dose group (10.8% vs 1.6%, P=0.025; Table 3). Patients with CK elevation received a significantly higher average dose of daptomycin than those who did not have elevated CK (9.3±1.2 vs 7.9±2.3 mg/kg, P=0.034). For multivariate analysis, ICU admission, acute kidney injury, septic arthritis, and high dose of daptomycin use were put in the final model, and the result confirmed that high-dose daptomycin was the only significant factor associated with CK elevation (odds ratio 7.46; 95% CI, 1.22–45.69; P=0.03.)
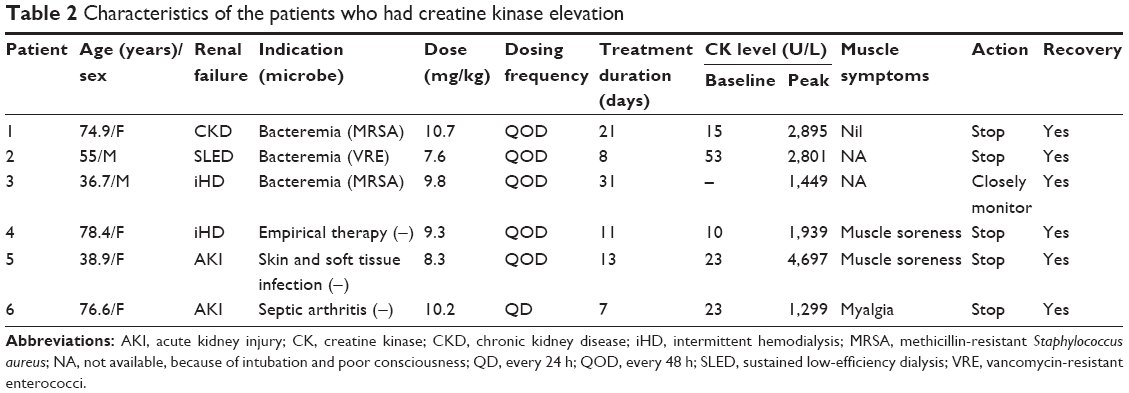 | Table 2 Characteristics of the patients who had creatine kinase elevation |
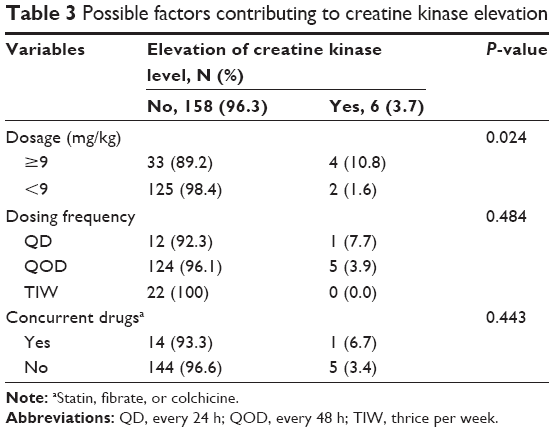 | Table 3 Possible factors contributing to creatine kinase elevation |
There was no significant difference in the incidence rate of CK elevation between patients with different dosing frequency or the concurrent use of statins, fibrates, or colchicine. The overall treatment success rate was 51.6% in the 91 patients with bloodstream infection. Among patients with monomicrobial bloodstream infections, the treatment success rates were 60.9% for MRSA and 40.6% for VRE, respectively.
Discussion
This study explored the important safety issue of using high doses of daptomycin in patients with renal impairment. Almost 70% of our patients were under renal replacement therapy during daptomycin treatment course. In patients with renal impairment, especially those treated with hemodialysis, the administration of various antimicrobial agents remains a challenging job. The recommended dosing regimen of daptomycin for the patients with CLCr <30 mL/min or under renal replacement therapy is 4–6 mg/kg every 48 h based on approved indications.11 However, there may be a discrepancy between the approved dosing regimen and the hemodialysis schedule. Daptomycin can be removed by hemodialysis, and dosing regimen to give the doses three times a week coinciding with each dialysis session was proposed.12 Twenty-two patients in our study were treated with daptomycin according to this thrice-weekly dosing. A previous research has shown that the pharmacokinetics of daptomycin was linear with doses up to 12 mg/kg in healthy volunteers.13 Compared with healthy subjects, exposure to daptomycin was increased two- to threefold in patients with severe renal impairment and those on hemodialysis.14 Daptomycin accumulated in patients with renal impairment may result in higher trough levels and therefore increase the probability of CK elevation.15 As recommended by the prescribing information, CK level should be monitored at least once per week during daptomycin treatment. In adult patients with renal impairment, both renal function and CK should be monitored more frequently than once a week.9 A pooled analysis of CORE (Cubicin® Outcomes Registry and Experience) and EUCORE (European Cubicin Outcomes Registry and Experience) revealed that blood CK levels were measured only in 43.5% of patients during daptomycin therapy.16 Monitoring of CK level was performed in 65.9% of patients in our study. In previous studies, the incidence rate of CK elevation due to daptomycin was considered low (1.9%–2.0%, CK level >5× the normal upper limit),5,6,16 and there was no significant difference of CK elevation rate between different dosage groups.16 This low incidence rate might be explained by the low percentage of patients with renal impairement5,16 or a relatively lower dose of daptomycin.6
Although the rate of CK monitoring in our study was greater than that in previous studies, 34.1% of our patients did not have CK level for assessment, and we assumed these patients did not have CK elevation. Comparisons between patients with or without CK measurement are listed in Table 4. Significantly different factors between two groups were types of renal failure, treatment duration, seizure or surgery during therapy, and concurrent antibiotic therapy with gentamicin. It is reasonable to monitor CK if treatment duration is longer and patients had seizure or surgery, which are the well-known etiologies for CK elevation. Patients receiving dialysis may lead to more drug accumulation, which could increase the risk of CK elevation. Therefore, it would be reasonable to assume that patients without CK measurement during treatment had normal CK because of shorter treatment duration, less dialysis, seizure, and surgery in this group. The issue of antibiotic doses is a critical one in the era of antibiotic resistance. Updated guidelines for infectious diseases advocate optimizing antibiotic pharmacokinetics and pharmacodynamics for better outcome.17,18 A trend toward the use of higher doses over time was observed.16 We defined daptomycin dose ≥9 mg/kg as the high-dose therapy based on the finding of a previous study conducted at our hospital system.4 We found that patients with CK elevation received higher doses of daptomycin than those with no documented CK elevation and a significantly higher rate of CK elevation in the high-dose group than that in the standard-dose group. In addition, the difference remained significant when the patients without records of CK levels were excluded (16.0% vs 2.4%, P=0.025). Although the number of events was small, we observed a trend of decreasing rate of CK elevation as the dosing frequency decreased: 7.7% (1/13) for once daily, 3.9% (5/129) for once every 48 h, and 0.0% for thrice weekly. The result was not statistically significant (P=0.52), but it was consistent with the finding of a previous study reporting more frequent dosing led to increased muscle toxicity.11 Use of high-dose daptomycin in patients with renal impairment is still a concern, and the dosing frequency should be included for clinical consideration.7
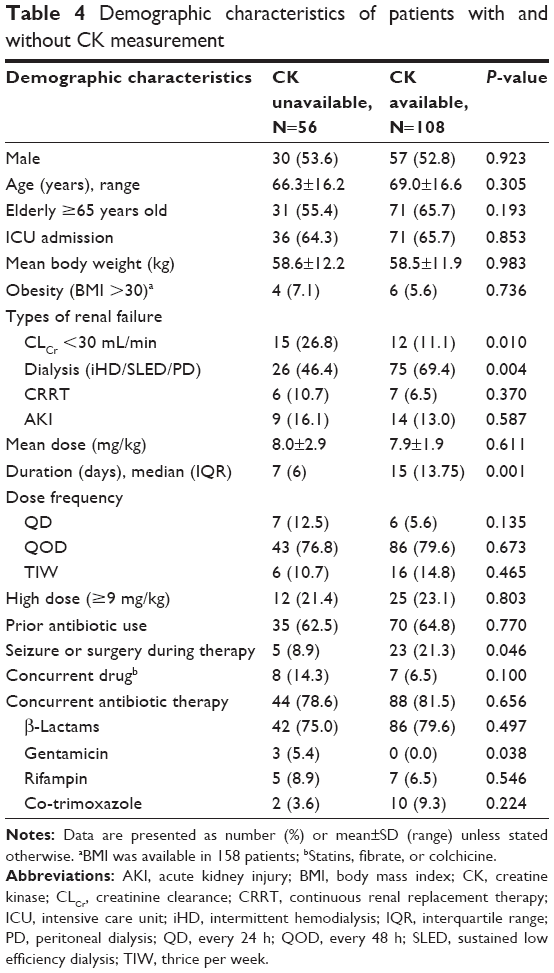 | Table 4 Demographic characteristics of patients with and without CK measurement |
Obese patients in our study received relatively lower doses of daptomycin per kg of body weight. Renal clearance of daptomycin is reduced in obese patients, and they have been identified as a high-risk population for CK elevation.19 The prescribing information recommends to use total body weight for daptomycin dosing, and no dosage adjustment is warranted in obese subjects. While most available studies used the recommended dose of 4–6 mg/kg in obese patients,20 the safety of high-dose daptomycin in this patient group had not been examined. In the present study, 70% of the obese patients received 500 mg of daptomycin, which was the dose supplied in each single-dose vial, resulting in the relatively lower doses than that in the other patients in this study. The efficacy and safety of daptomycin in obese patients with renal impairment need to be carefully evaluated to establish an appropriate dosing regimen for this population.
Lower treatment success rates of daptomycin in treating bloodstream infections were found in our study as compared with a large-scale study by Seaton et al reporting success rates of 78.1% for MRSA and 68.8% for VRE.16 This is partly because, in our hospital, daptomycin is reserved for rescue therapy after first-line treatment failed. Also, more than half of our patients (65.2%) were admitted to the ICU and had multiple organ failures. Therefore, the higher disease severity has likely contributed to the lower treatment success rates in our study.
Limitations
The most important limitation of the present study is the retrospective nature of the study design, which prevented a delineation of the causality of CK elevation. Also, the serum concentrations of daptomycin were unavailable for risk evaluation. In addition, we cannot address the risk of CK elevation in the patients without renal impairment, who were treated with high doses of daptomycin. Although the rate of CK monitoring in our study was greater than previous studies, 34.1% of our patients did not have CK level for assessment. This may lead to an underestimation of the real incidence of CK elevation.
Conclusion
Our study revealed that compared with standard doses, high-dose daptomycin therapy was associated with a significantly higher rate of CK elevation in patients with severe renal impairment. When increasing the doses of daptomycin to optimize its pharmacokinetic and pharmacodynamic effects, more frequent CK monitoring is highly recommended in this fragile population.
Acknowledgment
The authors acknowledge statistical assistance provided by the Department of Medical Research in National Taiwan University Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
Statistics of Taiwan Nosocomial Infection Surveillance Report. Centers for Disease Control, Ministry of Health and Welfare: Taiwan; 2016. Available from: https://www.syndriver.com/portal/#/sharing/d1b39e56648849f898802e0c01259a17. Accessed March 8, 2018. | ||
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 2015;32(15):1435–1486. | ||
Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075–3128. | ||
Chuang YC, Lin HY, Chen PY, Lin CY, Wang JT, Chang SC. Daptomycin versus linezolid for the treatment of vancomycin-resistant enterococcal bacteraemia: implications of daptomycin dose. Clin Microbiol Infect. 2016;10:890.e1–890.e7. | ||
Durante-Mangoni E, Andini R, Parrella A, et al. Safety of treatment with high-dose daptomycin in 102 patients with infective endocarditis. Int J Antimicrob Agents. 2016;48(1):61–68. | ||
Lai CC, Sheng WH, Wang JT, et al. Safety and efficacy of daptomycin for the treatment of hospitalized adult patients in Taiwan with severe staphylococcal infections. J Microbiol Immunol Infect. 2012;45(1):52–57. | ||
Kullar R, McClellan I, Geriak M, Sakoulas G. Efficacy and safety of daptomycin in patients with renal impairment: a multicenter retrospective analysis. Pharmacotherapy. 2014;34(6):582–589. | ||
Moise PA, Amodio-Groton M, Rashid M, et al. Multicenter evaluation of the clinical outcomes of daptomycin with and without concomitant beta-lactams in patients with Staphylococcus aureus bacteremia and mild to moderate renal impairment. Antimicrob Agents Chemother. 2013;57(3):1192–1200. | ||
Cubicin® (daptomycin for injection): US [prescribing information]. Lexington, MA: Cubist Pharmaceuticals Inc; 2007. | ||
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. | ||
Mueller BA, Crompton JA, Donovan BJ, Yankalev S, Lamp KC. Safety of daptomycin in patients receiving hemodialysis. Pharmacotherapy. 2011;31(7):665–672. | ||
Haselden M, Leach M, Bohm N. Daptomycin dosing strategies in patients receiving thrice-weekly intermittent hemodialysis. Ann Pharmacother. 2013;47(10):1342–1347. | ||
Gould IM, Miro JM, Rybak MJ. Daptomycin: the role of high-dose and combination therapy for Gram-positive infections. Int J Antimicrob Agents. 2013;42(3):202–210. | ||
Hair PI, Keam SJ. Daptomycin: a review of its use in the management of complicated skin and soft-tissue infections and Staphylococcus aureus bacteraemia. Drugs. 2007;67(10):1483–1512. | ||
Bhavnani SM, Rubino CM, Ambrose PG, Drusano GL. Daptomycin exposure and the probability of elevations in the creatine phosphokinase level: data from a randomized trial of patients with bacteremia and endocarditis. Clin Infect Dis. 2010;50(12):1568–1574. | ||
Seaton RA, Gonzalez-Ruiz A, Cleveland KO, Couch KA, Pathan R, Hamed K. Real-world daptomycin use across wide geographical regions: results from a pooled analysis of CORE and EU-CORE. Ann Clin Microbiol Antimicrob. 2016;15:18. | ||
Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017;43(3):304–377. | ||
Erb CT, Patel B, Orr JE, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia. Ann Am Thorac Soc. 2016;3(12):2258–2260. | ||
Bookstaver PB, Bland CM, Qureshi ZP, et al; SERGE-45 Investigators. Safety and effectiveness of daptomycin across a hospitalized obese population: results of a multicenter investigation in the southeastern United States. Pharmacotherapy. 2013;33(12):1322–1330. | ||
Polso AK, Lassiter JL, Nagel JL. Impact of hospital guideline for weight-based antimicrobial dosing in morbidly obese adults and comprehensive literature review. J Clin Pharm Ther. 2014;39(6):584–608. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.