")
Back to Journals » OncoTargets and Therapy » Volume 10
Safety, efficacy, and clinical utility of asparaginase in the treatment of adult patients with acute lymphoblastic leukemia
Authors Koprivnikar J, McCloskey J, Faderl S
Received 20 February 2016
Accepted for publication 6 July 2016
Published 6 March 2017 Volume 2017:10 Pages 1413—1422
DOI https://doi.org/10.2147/OTT.S106810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Li
Jamie Koprivnikar, James McCloskey, Stefan Faderl
Division of Leukemia, John Theurer Cancer Center at Hackensack University Medical Center, Hackensack, NJ, USA
Abstract: Adults with acute lymphoblastic leukemia (ALL) are known to have inferior outcomes compared to the pediatric population. Although the reasons for this are likely manyfold, the agents utilized and the increased intensity of pediatric treatments compared to adult treatments are likely significant contributing factors. Asparaginase, an enzyme that converts asparagine to aspartic acid, forms the backbone of almost all pediatric regimens and works by depleting extracellular asparagine, which ALL cells are unable to synthesize. Asparaginase toxicities, which include hypersensitivity reactions, pancreatitis, liver dysfunction, and thrombosis, have hindered its widespread use in the adult population. Here, we review the toxicity and efficacy of asparaginase in adult patients with ALL. With the proper precautions, it is a safe and effective agent in the treatment of younger adults with ALL with response rates in the frontline setting ranging from 78% to 96%, compared to most trials showing a 4-year overall survival of 50% or better. The age cutoff for consideration of treatment with pediatric-inspired regimens is not clear, but recent studies show promise particularly in the adolescent and young adult population. New formulations of asparaginase are actively in development, including erythrocyte-encapsulated asparaginase, which is designed to minimize the toxicity and improve the delivery of the drug.
Keywords: PEG-asparaginase, ALL, chemotherapy, pegaspargase, AYA, pediatric
Introduction
In 2015, there were 6,250 new cases of acute lymphoblastic leukemia (ALL) diagnosed in the USA. Despite the fact that approximately 60% of these cases were diagnosed in children, 80% of deaths secondary to ALL occurred in adults. The disparity in outcomes between adults and children with ALL represents a significant paradox in the treatment of this disease. Part of this disparity is related to disease biology as reflected by a higher incidence of poor prognosis chromosomal aberrations in adults, such as the Philadelphia chromosome, which is present in 30% of adults compared to only 3% of children. Differences in host biology, such as comorbidities and age-related pharmacokinetics, are also likely to be contributing factors. Nonetheless, these factors are unlikely to wholly account for the discordance in overall survival (OS) between adults (about 40%) and children (exceeding 80%). The use of particular agents and/or their dose intensity constitute one of the most striking differences in the management of these two populations.1–6 For instance, concerns regarding tolerability and treatment-related morbidity of asparaginase have led to its far less frequent use in adult compared to pediatric protocols. Yet, a number of recent studies emphasize the significance of asparaginase in the context of ALL treatment regimens and provide guidelines for the management of toxicities. The importance of asparaginase therapy has been highlighted in adults and adolescents (age 15–39), where disease survival approaches 70% when treated with pediatric-based regimens. Here, we discuss the role of asparaginase and pegaspargase in the treatment of adults with ALL.
Mode of action and pharmacology
Asparaginase is an enzyme that converts asparagine to aspartic acid in the extracellular fluid.7 Leukemic cells express low levels of asparaginase synthetase8–10 and are unable to produce more when exposed to asparaginase.11,12 Whereas normal cells contain high levels of asparaginase synthetase and are able to produce asparagine, leukemic cells have a heightened sensitivity to the depletion of extracellular asparagine disrupting asparagine-dependent protein synthesis and leading to cell death.13 Asparaginase levels serve as a surrogate marker for asparagine concentration demonstrating an inverse relationship, and as such, have often been used in the pediatric population to determine asparagine depletion.9–16 Serum asparaginase activity levels ≥0.1 IU/mL are felt to be adequate for asparaginase depletion in clinical practice.
Three formulations of asparaginase exist with a fourth currently in development (Table 1). Two are derived from the bacterium Escherichia coli (E. coli). The third is derived from the bacterium Erwinia chrysanthemi. The native E. coli-derived preparation has been replaced by the polyethylene-conjugated formulation, polyethylene glycol (PEG)-asparaginase. The addition of a covalently linked monomethoxypolyethylene glycol to E. coli asparaginase preserves enzyme activity and slows elimination of the drug. The half-life of pegaspargase is approximately five times longer than native E. coli asparaginase and nine times longer than Erwinia asparaginase. This longer half-life means the drug can be given at lower doses and less frequently, resulting in fewer antigenic reactions.16–19 The fourth formulation, L-asparaginase-loaded red blood cells (RBCs), which also utilizes E. coli-derived asparaginase, is currently under investigation and will be discussed later.
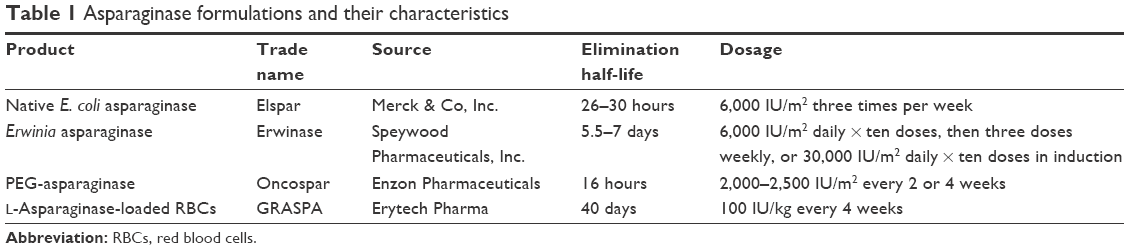 | Table 1 Asparaginase formulations and their characteristics |
Hypersensitivity
As foreign proteins, derived either from E. coli or Erwinia chrysanthemi, asparaginases have the potential to induce an immune response when administered to patients. These immune responses may result in either clinical or subclinical hypersensitivity reactions. Clinical hypersensitivity runs the gamut from localized, transient erythema and rash at the site of injection to acute life-threatening anaphylaxis. The most common symptoms are pain, tenderness, swelling, and erythema at the injection site when given intramuscularly, and dyspnea, bronchospasm, pruritus, skin rash, and urticaria when given intravenously (IV); uncommon symptoms include angioedema, laryngospasm, and hypotension.17 Such hypersensitivity reactions are associated with the production of antiasparaginase antibodies.18,19 Even in the absence of clinical signs and symptoms of hypersensitivity, up to one-third of patients may develop asparaginase-inactivating antibodies leading to decreased concentrations of asparaginase, increased levels of extracellular asparagine, and therefore drug resistance.18 This is known as silent inactivation and is the rationale for monitoring of serum asparaginase activity levels. The incidence of hypersensitivity differs markedly among asparaginase preparations and is less common with the administration of pegylated products.20–24
Thrombotic complications
Thrombosis is a well-known complication associated with asparaginase. Increased rates of thrombosis in patients receiving L-asparaginase are generally felt to be secondary to the inhibition of hepatic synthesis of L-asparagine-dependent hemostatic proteins, specifically antithrombin. Thrombosis can occur with asparaginase during induction or postremission treatment and appears to be higher in adult populations.25,26 In one prospective study of 548 patients, 5% of pediatric patients compared to 34% of adults experienced thrombotic complications with L-asparaginase.27 Venous thrombosis is more common than arterial thrombosis, with upper central venous thrombosis being the most common.28 However, arterial and central nervous system (CNS) thrombotic events have been observed.
The occurrence of CNS thrombosis was retrospectively reviewed from the Group for Research on Adult Acute Lymphoblastic Leukemia (GRAALL) 2003, GRAALL 2005, and LL03 protocols in patients from April 2004 to July 2011.29 Events were prospectively reported to the GRAALL data management center. GRAALL 2003 was a multicenter, Phase II, prospective study evaluating the feasibility of a pediatric-based treatment in adults aged 18–59 years. GRAALL 2005 was a randomized trial evaluating high-dose cyclophosphamide and rituximab in patients with CD20+ ALL, and the LL03 study was a multicenter, Phase II trial evaluating the safety and efficacy of intensive chemotherapy for the treatment of ALL in young adult patients with lymphoblastic lymphoma. Induction therapy was very similar across the three studies including eight E. coli asparaginase injections at 6,000 UI/m2, changed to Erwinia chrysanthemi injections at 12,000 UI/m2 IV in case of allergic reactions.
The recommended thromboprophylaxis included evaluation of antithrombin and fibrinogen levels prior to each asparaginase infusion and supplementation with fresh frozen plasma for fibrinogen levels below 0.5 g/L and with antithrombin concentrate for antithrombin levels below 60%. Platelet transfusion was recommended for platelet counts less than 20,000/μL. Unfractionated heparin at 100 UI/kg/d continuous infusion prophylaxis was recommended as long as platelets remained above 20,000/μL inclusive of transfusion. A total of 708 patients were enrolled on the three protocols, with CNS thrombosis reported in 22% or 3.1% of these patients including 2.8% of ALL patients and 4.4% of lymphoblastic lymphoma patients. The GRAALL 2005 study exhibited an overall rate of thrombosis of 9.5% (33/347). The relative proportions of the thrombotic complications included 36% CNS thromboses, 30% lower limb thromboses, 18% upper limb thromboses, 9% pulmonary embolisms, 3% portal systemic thrombosis, and 3% arterial thromboses.
CNS thrombosis occurred in two patients prior to L-asparaginase infusions (2/708 or 0.28%) bringing the post-L-asparaginase rate of CNS thrombosis to 2.8% (20/708 or 2.8%) (P=0.0001). Of patients who experienced thrombosis during asparaginase treatment, the median age was 29 with a range of 18–50 years. Three-quarters of the patients were male, and there was an increased risk of CNS thrombosis in patients with T-cell-ALL (13/262, 5%) compared to B-cell-ALL (7/394, 1.8%) (P=0.034). None of the patients with CNS thrombosis experienced an allergic reaction to E. coli L-asparaginase. One patient died 5 days after CNS thrombosis because of associated cerebral hemorrhage, while four other patients (20%) experienced neurological sequelae including persistent headaches, epilepsy, and motor or cognitive deficiency. CNS thrombosis occurred from day 11 through day 31 (median: day 18) after starting induction therapy, after a median of 3 L-asparagine injections (range 2–7). Prophylactic anticoagulation did not seem to protect from CNS thrombosis, as it was performed in 90% of patients with CNS thrombosis and in only 64.9% of the patients without CNS thrombosis.29 The 3.1% rate of CNS thrombosis seen in this study is higher than the 1%–2% incidence rate reported in children30 (see Table 2 for additional asparaginase side effects and recommended management).
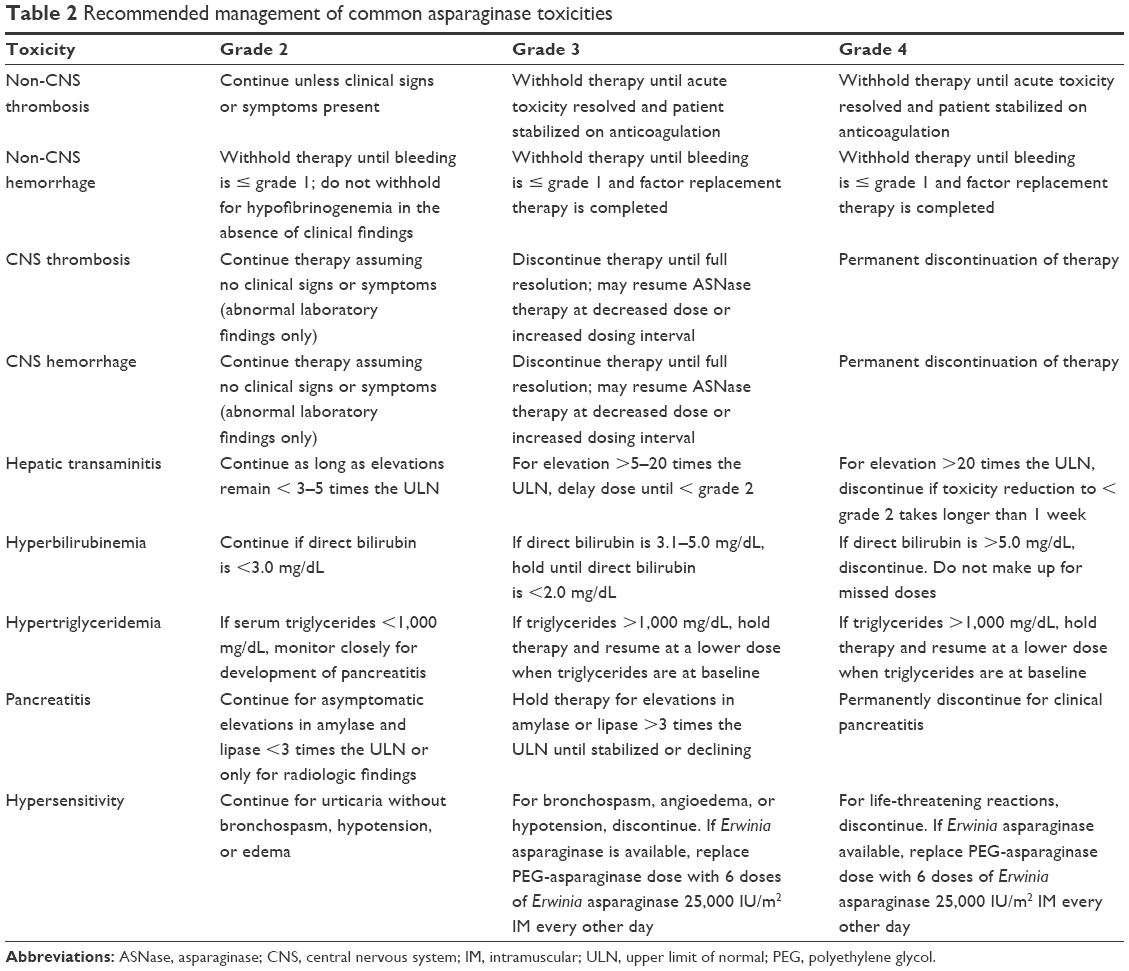 | Table 2 Recommended management of common asparaginase toxicities |
The development of newer oral anticoagulants that directly target the enzymatic activity of thrombin and factor Xa presents a potential opportunity for chemothromboprophylaxis in patients receiving asparaginase. Drugs in these classes include dabigatran etexilate (Pradaxa, Boehringer Ingelheim, Ingelheim, Germany), rivaroxaban (Xarelto, Janssen Pharmaceutica, Beerse, Belgium), apixaban (Eliquis, Bristol-Myers Squibb, New York, NY, USA), and edoxaban (Lixiana, Savaysa, Daiichi Sankyo, Tokyo, Japan). These agents are advantageous in that they do not require routine monitoring of therapeutic levels, are orally administered, have relatively few drug–drug interactions, and are available at a prophylactic dosage. Thus, they are easy to administer both in the inpatient and outpatient setting. In our practice, we have started to incorporate these drugs as primary thromboprophylaxis in adult patients receiving asparaginase.
Asparaginase in newly diagnosed ALL
Hoelzer et al31 used a modified pediatric regimen to treat 162 patients aged 15–65 years with either ALL or acute undifferentiated leukemia. Treatment consisted of a two-phase, 8-week induction regimen, consisting of prednisone, vincristine, daunorubicin, and L-asparaginase during the 4-week Phase I portion and cyclophosphamide, cytosine arabinoside, and 6-mercaptopurine (6-MP) during the Phase II portion. Patients older than 35 years had L-asparaginase administration delayed until their platelet count was greater than 50,000 to prevent bleeding complications.
Of the 162 patients enrolled, 126 (77.8%) achieved complete (CR) and 6 (3.7%) partial remission (PR). Seventeen patients (10%) died during induction, while 13 (8%) did not respond. With a median follow-up of 26 months, 56 patients (44%) were in a continuous CR. The median OS was 26 months. This was increased to 32 months for those who achieved CR.31
Infection, sepsis, hemorrhage, gastrointestinal side effects, hepatotoxicity, and neurotoxicity accounted for the most frequent adverse events. Hemorrhage and hepatotoxicity attributable to asparaginase administration occurred in 12% and 13% of patients, respectively. During induction, a total of 17 deaths occurred. Causes of death included hemorrhage in seven cases (five cerebral) and uncontrolled infection in six.31
DeAngelo et al32 applied a pediatric-inspired regimen in 92 adults aged 18–50 with newly diagnosed ALL with a primary focus of determining the feasibility of treatment with weekly intramuscular E. coli asparaginase during the 30-week intensification phase. Induction therapy consisted of vincristine 2 mg weekly on days 1, 8, 15, and 22, prednisone 30 mg/m2/d on days 1 through 28, doxorubicin 30 mg/m2 on days 1 and 2, and methotrexate 4 g/m2 with leucovorin rescue on day 3 in addition to intrathecal (IT) therapy. Intensification consisted of 3-week cycles of vincristine 2 mg given on day 1, dexamethasone 18 mg/m2 twice daily on days 1 through 5, doxorubicin 30 mg/m2 given on day 1, 6-MP 50 mg/m2 daily for 14 days, methotrexate 30 mg/m2 on day 1, and E. coli asparaginase given with individualized dosing based on nadir serum asparaginase levels. The continuation phase of 74 weeks was similar except that asparaginase was omitted and dexamethasone was given at a lower dose. Of those enrolled on trial, 57 patients were evaluable for the asparaginase end point. The majority of patients who were not evaluable in this analysis had either undergone allogenic stem cell transplantation (16 patients) or were resistant to induction (ten patients). Of those evaluable, 36 (63%) completed all 30 doses, with 41 (72%) patients completing 26 or more doses.
Toxicity was the primary reason that patients were unable to complete asparaginase therapy. Pancreatitis developed in seven of the 21 patients, while two experienced allergic reactions to all asparaginase preparations. Six of these patients were unable to complete therapy because of either a deep vein thrombosis or hepatic toxicity, while two relapsed during the intensification phase, one withdrew because of noncompliance, and three had other toxicities. Asparaginase-related toxicities included allergic reactions in five patients (5%), thrombosis in 16 (17%), bone fracture in seven (8%), avascular necrosis in five (5%), and pancreatitis in ten (11%) with one death related to pancreatitis. During the intensification phase, more than half of patients developed hepatic toxicity with ten developing grade ≥3 hyperbilirubinemia and one death as a result of liver failure.32
All patients started the intensification phase by taking 12,500 IU/m2 of E. coli asparaginase. This dose was subsequently adjusted either up or down based on the nadir serum asparaginase activity resulting in a median delivered asparaginase dose of 15,000 IU/m2. A plateau in the nadir serum asparaginase activity was seen after six doses. Prior to this, a progressive incline was noted. Serial nadir serum asparaginase activity was also used to identify 12 patients with a suspected silent asparaginase allergy who had repeatedly low nadir serum asparaginase activity. Three of these patients were switched to Erwinia asparaginase, attaining an overall median nadir serum asparaginase activity of 0.057 IU/mL, which was lower than the targeted therapeutic concentration of 0.1 to <0.14 IU/mL. The remaining nine patients received pegaspargase, ultimately reaching a median nadir serum asparaginase activity of 0.44 IU/mL.
The 4-year disease-free survival rate reported for patients enrolled in this study was 69%. The majority of patients (72%) were able to complete at least 26 doses of asparaginase, which is felt to be of significance based on pediatric data showing that completion of at least 26 weeks of asparaginase correlates with improved treatment outcomes.33
Douer et al34 examined a pharmacokinetically based dosing schedule of pegaspargase in 51 adults aged 18–57 years with newly diagnosed ALL treated with a regimen adapted from a pediatric trial. The protocol consisted of two induction phases, both of which included pegaspargase 2,000 IU/m2 on day 15. This was followed by an intensification phase with pegaspargase 2,000 IU/m2 administered on day 16. Following a consolidation phase, patients received delayed reinduction including pegaspargase 2,000 IU/m2 on day 15. Maintenance was carried out monthly for 24 months.
The mean number of pegaspargase doses received by patients was 3.8, with 23 patients (45%) receiving all six pegaspargase doses. One patient received four doses of pegaspargase and seven patients received three doses. Nine patients received two doses and eleven patients were only able to tolerate a single dose. In total, 31 patients (61%) were able to receive three or more doses. Toxicity resulted in discontinuation of pegaspargase in ten patients (20%). Toxicities included pancreatitis in seven patients, severe allergy in three, and deep vein thrombosis in one. Treatment failure or death during consolidation occurred in nine patients (18%). Grade ≥3 asparaginase-related toxicities occurring in 5% or more of patients included pancreatitis in seven (13%), allergy in three (5.9%), deep vein thrombosis in eight (15.7%), transaminitis in 32 (62.7%), hyperbilirubinemia in 16 (31.3%), hyperglycemia in 17 (33.3%), hypertriglyceridemia in nine (17.6%), fatigue in four (7.8%), and nausea in three (5.9%). No deaths have been attributed to pegaspargase. Hepatotoxicity caused a delay in subsequent chemotherapy following 14 pegaspargase doses.
The 7-year OS rate for all patients was 51%, with a 58% 7-year OS for the 40 Philadelphia chromosome-negative patients. The OS of 17 patients with standard-risk disease was 73%, with an OS of 40% for the 24 patients with high-risk disease. The OS of patients not undergoing transplantation was 55%. All of the five patients with T-cell ALL treated on the protocol were alive and in first remission at 28–66 months of follow-up.34
The Dutch–Belgian HOVON study group investigated the feasibility of intensified chemotherapy inspired by the pediatric FRALLE 93 regimen combined with allogeneic transplantation in 54 adults aged 17–40 years with untreated B-cell ALL.35 Patients who presented with a white blood cell count greater than 30,000/μL with B-ALL or 100,000/μL with T-ALL, had t(9;22) or t(4;11), and/or the BCR-ABL or MLL-AF4 fusion gene product, or patients who did not reach CR after remission induction were considered as having high-risk disease. Patients were treated by a 7-day “pre-phase” consisting of twice-daily prednisone and one dose of IT methotrexate followed by induction on days 8 through 28 consisting of twice-daily prednisone, vincristine, daunorubicin, cyclophosphamide, L-asparaginase, and IT methotrexate. Consolidation A was scheduled before day 45 and consisted of 6-thioguanine, cyclophosphamide, cytarabine, and methotrexate. Consolidation B was scheduled before day 75 and consisted of prednisone, vincristine, 6-MP, and oral, IV, and IT methotrexate. Intensification IA was scheduled before day 105 and consisted of dexamethasone, vindesine, adriamycin, L-asparaginase, and IT methotrexate. Intensification IB was scheduled before day 135 and consisted of 6-thioguanine, etoposide, cytarabine, and IT methotrexate. Interphases A and B were scheduled before days 165 and 195, respectively, and consisted of the same agents used in Consolidation B. Intensification IIA was scheduled before day 225 and mirrored induction, but omitted cyclophosphamide and used a lower dose of daunorubicin. Intensification IIB, scheduled before day 255, was similar to Consolidation A. Maintenance consisted of oral 6-MP and methotrexate given over the course of 21 days. Patients then completed 12-week-long reinduction courses consisting of daily prednisone and weekly doses of vincristine and IT methotrexate. Standard-risk patients with a sibling donor and high-risk patients with either a sibling or unrelated donor underwent allogeneic stem cell transplant after intensification course IA and B. L-Asparaginase was administered IV at a dose of 6,000 IU/m2 on days 8, 10, 12, 15, 17, 19, 22, 24, and 26 of induction and on days 4, 6, 8, 10, 12, and 15 of Intensification IA and IIA.
The average age of patients enrolled on the study was 26 years. The majority of the patients (57%) had standard-risk disease. CR was reached by 49 (91%) patients. A total of 33 (61%) patients were able to complete chemotherapy within the prespecified time of 49 weeks for maintenance chemotherapy and 34 weeks for allogeneic stem cell transplant. With a median follow-up of 32 months, the estimated 2-year event-free survival and OS were 66% and 72%, respectively. One asparaginase-related death occurred because of pulmonary embolism. Four grade 4 toxicities were attributed to asparaginase including a thromboembolic event and three severe liver disturbances. Nine thrombotic events were noted, with seven of these occurring during induction accounting for thromboembolic events in 13% of all patient undergoing induction. No pancreatitis was observed, and one allergic reaction to asparagine was noted. Asparaginase administration following induction chemotherapy was largely uneventful. Overall, the authors concluded that this asparaginase-containing regimen was feasible and had acceptable toxicities. The OS of 87% for standard-risk patients and 57% for high-risk patients was compared favorably to that of patients treated with prior, more conventional treatment regimen.35
GRAALL examined the efficacy and tolerability of pediatric-inspired therapy in adults with Ph-negative ALL in 225 patients aged 15–60 years.36 Treatment consisted of a corticosteroid prophase followed by a 28-day induction consisting of prednisone, daunorubicin, vincristine, E. coli asparaginase 6,000 U/m2/d on days 8, 10, 12, 20, 22, 24, 26, and 28, cyclophosphamide, and growth factor support. Responders went on to receive six consolidation blocks. Blocks 1 and 4 consisted of cytarabine, dexamethasone, and L-asparaginase 10,000 U/m2 on day 16. Blocks 2 and 5 consisted of methotrexate, vincristine, L-asparaginase dosed at 10,000 U/m2 on day 16, and 6-MP. Blocks 3 and 6 consisted of cyclophosphamide, etoposide, and methotrexate. Following consolidation block 6, patients entered late intensification consisting of prednisone, vincristine, daunorubicin, L-asparaginase dosed on 6,000 U/m2/d on days 8, 10, 12, 20, and 22, cyclophosphamide, and growth factor support. An alternate regimen was given to those who required salvage following the induction course. Patients then completed consolidation blocks 7, 8, and 9 (identical to blocks 1, 2, and 3). This was followed by CNS irradiation and 24 months of maintenance therapy.
The CR rate was 93% with an OS of 60% at 42 months. Survival was affected significantly by age with an OS of 66% for patients under the age of 45 and 41% for patients over the age of 45. Older patients experienced a high incidence of chemotherapy-related death (23%) and did not tolerate the chemotherapy as well, leading to dose reduction and delay in treatment. Older patients received a lower cumulative dose of L-asparaginase than patients under the age of 45 (36,000 U/m2 versus 48,000 U/m2).36 This study provides an important clue to the upper age limit at which asparaginase dosing is safe and tolerable for the average patient.
In a retrospective analysis, investigators at Princess Margaret Hospital analyzed 85 consecutive patients between the ages of 18 and 60 with newly diagnosed BCR–ABL-negative B-ALL who received therapy with a pediatric-inspired regimen.37 This regimen was based on the CFCI 91-01 protocol and consisted of E. coli asparaginase given at 25,000 IU/m2 on day 4 of induction as well as on days 1, 8, and 15 of ten 21-day maintenance cycles at a dose of 12,500 IU/m2. A complete response was achieved in 89% of patients with four primary induction failures. Five patients died from infectious causes during induction. Age predicted for a complete response with a CR rate of 98% in those 35 years of age or younger compared to 81% for those older than 35. A trend was also seen in increased induction mortality with increasing age with a 0% mortality in those aged 25 or younger compared to a 20% mortality in those aged 50 or over. Again, these data suggest a possible upper age limit beyond which the average patient may have difficulty tolerating asparaginase therapy.
With a median follow-up of 48 months, the 3-year OS was 67%. There were 12 patients who received less than 80% of the total planned asparaginase dose during intensification because of intolerance. Half of these were older than 35. Hypersensitivity reactions, pancreatitis, and decline in performance status accounted for the reduced dose. Notably, patients who received at least 80% of the planned asparaginase dosing had a significantly higher 3-year OS (P=0.003) and relapse-free survival (P=0.002), and lower risk of relapse (P=0.01), compared to those who received less than 80% of the planned dosing because of intolerance. The most common toxicity noted during induction was infection. Toxicities other than infection included steroid-induced hyperglycemia, mucositis, neuropathy/ileus, seizures, acute renal failure, myopathy, gastrointestinal bleeding, neutropenic enterocolitis, and myocardial infarction. Toxicities occurring during the intensification phase included infections, osteonecrosis, venous thromboembolism (23%), neuropathy, elevations in serum aspartate aminotransferase/alkaline phosphatase more than five times the upper limit of normal (13%), pancreatitis (7%), hyperglycemia requiring insulin, hypersensitivity reaction to asparaginase (5%), and steroid myopathy. Thrombotic events included nine instances of deep vein thrombosis, three instances of pulmonary embolism, three instances of central venous catheter-associated thrombosis, and one instance of retinal vein thrombosis. Most patients experiencing thrombotic complications were safely treated with a 2- to 3-week period of asparaginase interruption followed by resumption of the drug with continued anticoagulation without recurrence37 (see Table 3 for a summary of asparaginase trials in the frontline treatment of ALL).
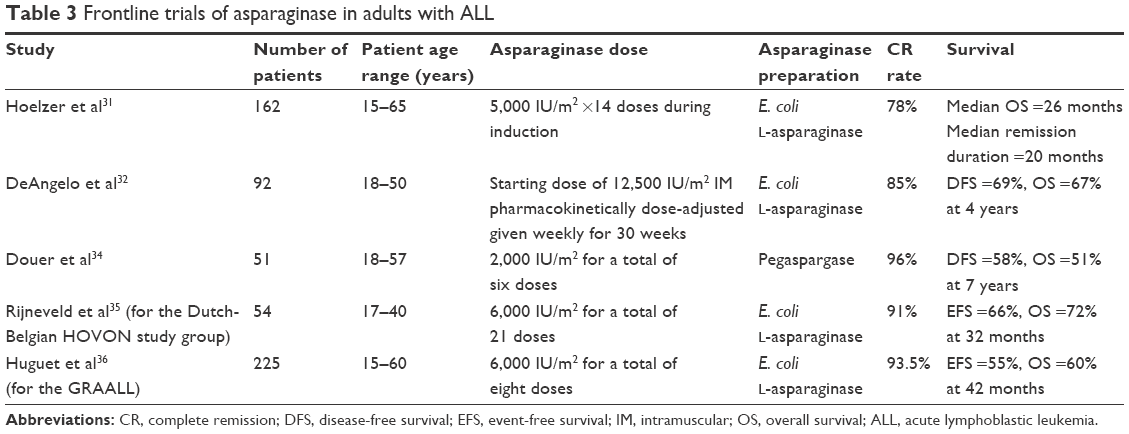 | Table 3 Frontline trials of asparaginase in adults with ALL |
Asparaginase in ALL salvage
Kadia et al38 enrolled 37 patients on a Phase II trial of methotrexate 200 mg/m2 IV on days 1 and 15, vincristine 1.4 mg/m2 IV (maximum dose 2 mg) on days 1, 8, and 15, PEG-L-asparaginase 2,500 IU/m2 IV on days 2 and 16, and dexamethasone 40 mg IV or per os daily on days 1–4 and 15–18. An amendment because of toxicity limited the maximum dose of PEG-L-asparaginase to 3,750 units per dose. Patients enrolled on the trial received a median of 2 prior therapies with a range of 1–6. Thirty-six patients received treatment on study and were evaluable for response. Patients who were treated in second-salvage and beyond exhibited refractory disease in 72% of cases, CR in 20% of cases, and PR in 8% of cases. The overall response among the 36 evaluable patients was 39%. Patients who responded had a median survival of 10.4 months compared with 3.4 months for nonresponders. The median CR duration was 4.3 months overall and was not reached in 12 patients with T-cell disease. Half of patients did not receive day 15 PEG-asparaginase and/or vincristine because of abnormal liver function tests (42%), mucositis, infection, elevated amylase or lipase (11%), death (11%), peripheral neuropathy, CNS disease, decreased fibrinogen (5%), or thrombosis (5%). Although elevations in liver function tests were generally transient, there was one case that progressed to liver failure and death. Elevations in amylase and lipase were also generally transient and responded to interruption in therapy with the exception of one case of clinical pancreatitis treated successfully with medical management. Although 70% of patients were noted to have a decrease in fibrinogen, the incidence of thrombosis was much lower at 14%.38
Erythrocyte-encapsulated asparaginase
L-Asparaginase-loaded RBC have been tested in several early-phase clinical trials. This preparation consists of L-asparaginase loaded into homologous RBC at a concentration of 50% and then suspended in saline, adenine, glucose, and mannitol. The L-asparaginase then theoretically remains sequestered within the erythrocyte and is carried throughout the circulation. Asparagine is continuously pumped into the erythrocyte, resulting in cleavage and plasma asparagine depletion. Because the asparaginase remains encapsulated in the RBC, antibodies are unable to bind, preventing the rapid clearance of asparaginase and decreasing the risk of allergic reactions.
A French Phase I/II study compared three doses of L-asparaginase encapsulated within erythrocytes and a control arm of IV E. coli asparaginase.39 Eligible patients included those aged 1–55 with ALL in first relapse or ALL refractory to induction therapy. The COOPERALL schedule was used as a backbone chemotherapy. A total of 24 patients were randomized to receive either 10,000 IU/m2 of IV E. coli asparaginase every 3 days or to receive one of three doses of erythrocyte-encapsulated L-asparaginase: 50, 100, or 150 IU/kg administered approximately once per month for 2 months. The mean age of all adults treated was 30.3 years with a range of 19.3–46.8.
Patients received readministration of the encapsulated asparaginase only if the serum asparagine level was greater than 2 μmol/L prior to planned administration, major complications had not occurred, and there was no indication for hematopoietic stem cell transplant. Two patients given the lowest dose, 50 IU/kg, of encapsulated asparaginase were withdrawn for asparagine depletion failure at day 7. A patient receiving the highest tested dose of encapsulated asparaginase at 150 IU/kg continued to exhibit asparaginase depletion at the time of the planned second injection and thus did not receive a second dose. The mean half-life of the RBC-encapsulated asparaginase was 40 days. The mean depletion of asparagine duration as analyzed after the second dose was 6.97 days for those receiving a dose of 50 IU/kg, 2.79 days for those receiving a dose of 100 IU/kg, and 23.95 days for those dosed at 150 IU/kg. Duration of asparagine depletion at the 150 IU/kg dose was similar to that observed after the administration of eight injections of E. coli asparaginase. Following one cycle of treatment, fewer allergic reactions were seen in patients receiving RBC-encapsulated asparaginase (0% versus 33%). Trends toward decreased hepatic disorders and hypoalbuminemia were seen in those receiving RBC-encapsulated asparaginase (50% versus 38% and 33% versus 0%, respectively). Patients receiving the study drug had trends toward higher fibrinogen levels (30.2 versus 15.8) and higher antithrombin III levels (787 versus 634). Although one patient enrolled to the E. coli asparaginase arm experienced a clinically significant thrombosis, no patients enrolled on the experimental arm were found to have clinical signs of thrombosis. Clinically silent thrombotic events were detected in 50% of control subjects and 16% of patients receiving RBC-encapsulated asparaginase.
Hunault-Berger et al40 conducted a Phase IIa dose-finding study of erythrocyte-encapsulated L-asparaginase in adults aged 55 or older with Ph-negative ALL. Patients were treated using the EWALL backbone with two successive induction phases. Here, 50, 100, or 150 IU/kg of erythrocyte-encapsulated L-asparaginase was infused on day 3 of induction Phase I and day 6 of induction Phase II. The median age of patients enrolled on the trial was 67 years of age with a range of 59–77. Three patients were enrolled on the 50-IU/kg group, while 13 and 14 patients were enrolled on the 100- and 150-IU/kg groups, respectively. A death rate of 20% was reported during the two induction cycles. The primary efficacy end point of asparagine depletion of less than 2 μmol/L for a minimum of 7 days after GRASPA infusion was reached in 0%, 85%, and 71% of patients treated with 50, 100, and 150 IU/kg, respectively. No clinically significant allergic reactions developed after the infusion of erythrocyte-encapsulated L-asparaginase. Baseline cerebrospinal fluid asparaginase concentration was 7.30 prior to erythrocyte-encapsulated L-asparaginase infusion. It became undetectable following erythrocyte-encapsulated L-asparaginase infusion in approximately 70% of patients. The overall CR rate following two inductions was 70% with 20% of patients dying during induction and 10% of patients failing to achieve CR. At a median follow-up of 42.2 months, the median OS was 11.8 months, with OSs of 15.8 months in the 100-IU/kg cohort and 9.7 months in the 150-IU/kg cohort. The optimal erythrocyte-encapsulated L-asparaginase dose was determined to be 100 IU/kg based on tolerability and asparagine depletion.
Conclusion
Treatment with asparaginase is both feasible and effective in children, adolescents and young adults (AYA), and adults with ALL. Unique toxicities of asparaginase administration include pancreatitis, hypercoagulability, liver dysfunction, and allergic reactions. Given a different milieu of host factors, many of these toxicities are magnified in the adult population, particularly during induction chemotherapy where active leukemia and increased rates of tumor cell death further contribute to the presence of a proinflammatory state. The optimal schedule and dose of asparaginase in the adult population remain unclear as does the upper age limit at which asparaginase may be safely tolerated, although treatment is generally poorly tolerated in patients over the age of 45. Treatment of AYA patients represents a particular challenge. Growing data show improved survival in AYA patients treated with pediatric regimens incorporating asparaginase, but often with the cost of toxicity. The development of PEG-asparaginase represents a more convenient and likely less immunogenic form of treatment. As investigators continue to study L-asparaginase encapsulated in erythrocytes, there is hope that further improvements in drug delivery may increase the tolerability of asparaginase allowing its use in an even broader population of patients with ALL.
Looking forward to the future care of patients with ALL, we see asparaginase continuing to play a role in the treatment of AYA patients. Rather than being paired with cytotoxic chemotherapy, it is possible that asparaginase will instead be further investigated in combination with targeted therapies such as blinatumomab (Blincyto, Amgen Inc., Thousand Oaks, CA, USA), a monoclonal bispecific T-cell engager, or other targeted therapies that remain in development. With the significant toxicity seen in patients greater than 40–45 years of age, asparaginase therapy may lose favor compared to less toxic targeted therapies. Currently, no such targeted agents are approved for T-cell ALL, and asparaginase will likely continue to play an important role in its treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
Nachman J. Clinical characteristics, biologic features and outcome for young adult patients with acute lymphoblastic leukaemia. Br J Haematol. 2005;130:166–173. | ||
Nachman JB, Sather HN, Sensel MG, et al. Augmented post-induction therapy for children with high-risk acute lymphoblastic leukemia and a slow response to initial therapy. N Engl J Med. 1998;338:1663–1671. | ||
Rowe JM, Buck G, Burnett AK, et al. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. Blood. 2005;106:3760–3767. | ||
Kantarjian H, Thomas D, O’Brien S, et al. Long-term follow-up results of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (Hyper-CVAD), a dose-intensive regimen, in adult acute lymphocytic leukemia. Cancer. 2004;101(12):2788–2801. | ||
Gokbuget N, Hoelzer D, Arnold R, et al. Treatment of adult ALL according to protocols of the German Multicenter Study Group for Adult ALL (GMALL). Hematol Oncol Clin North Am. 2000;14:1307–1325. | ||
Annino L, Vegna ML, Camera A, et al. Treatment of adult acute lymphoblastic leukemia (ALL): long-term follow-up of the GIMEMA ALL 0288 randomized study. Blood. 2002;99:863–871. | ||
Capizzi RL, Bertino JR, Skeel RT, et al. L-asparaginase: clinical, biochemical, pharmacological, and immunological studies. Ann Intern Med. 1971;74:893–901. | ||
Horowitz B, Madras BK, Meister A, Old LJ, Boyes EA, Stockert E. Asparagine synthetase activity of mouse leukemias. Science. 1968;160:533–535. | ||
Haskell CM, Canellos GP. L-asparaginase resistance in human leukemia–asparagine synthetase. Biochem Pharmacol. 1969;18:2578–2580. | ||
Kiriyama Y, Kubota M, Takimoto T, et al. Biochemical characterization of U937 cells resistant to L-asparaginase: the role of asparagine synthetase. Leukemia. 1989;3:294–297. | ||
Aslanian AM, Fletcher BS, Kilberg MS. Asparagine synthetase expression alone is sufficient to induce L-asparaginase resistance in MOLT-4 human leukaemia cells. Biochem J. 2001;357:321–328. | ||
Hutson RG, Kitoh T, Moraga Amador DA, Cosic S, Schuster SM, Kilberg MS. Amino acid control of asparagine synthetase: relation to asparaginase resistance in human leukemia cells. Am J Physiol. 1997;272:C1691–C1699. | ||
Asselin BL, Ryan D, Frantz CN, et al. In vitro and in vivo killing of acute lymphoblastic leukemia cells by L-asparaginase. Cancer Res. 1989;49:4363–4368. | ||
Grigoryan RS, Panosyan EH, Seibel NL, Gaynon PS, Avramis IA, Avramis VI. Changes of amino acid serum levels in pediatric patients with higher-risk acute lymphoblastic leukemia (CCG-1961). In Vivo. 2004;18(2):107–112. | ||
Boos J, Werber G, Ahlke E, et al. Monitoring of asparaginase activity and asparagine levels in children on different asparaginase preparations. Eur J Cancer. 1996;32A(9):1544–1550. | ||
Avramis VI, Sencer S, Periclou AP, et al. A randomized comparison of native Escherichia coli asparaginase and polyethylene glycol conjugated asparaginase for treatment of children with newly diagnosed standard-risk acute lymphoblastic leukemia: a Children’s Cancer Group study. Blood. 2002;99(6):1986–1994. | ||
Lenz HJ. Management and preparedness for infusion and hypersensitivity reactions. Oncologist. 2007;12(5):601. | ||
Liu C, Kawedia JD, Cheng C, et al. Clinical utility and implications of asparaginase antibodies in acute lymphoblastic leukemia. Leukemia. 2012;26(11):2303–2309. | ||
Tong WH, Pieters R, Kaspers GJ, et al. A prospective study on drug monitoring of PEGasparaginase and Erwinia asparaginase and asparaginase antibodies in pediatric acute lymphoblastic leukemia. Blood. 2014;123(13):2026–2033. | ||
Wang B, Relling MV, Storm MC, et al. Evaluation of immunologic cross reaction of anti asparaginase antibodies in acute lymphoblastic leukemia (ALL) and lymphoma patients. Leukemia. 2003;17(8):1583. | ||
Avramis VI, Sencer S, Periclou AP, et al. A randomized comparison of native Escherichia coli asparaginase and polyethylene glycol conjugated asparaginase for treatment of children with newly diagnosed standard-risk acute lymphoblastic leukemia: a Children’s Cancer Group study. Blood. 2002;99(6):1986. | ||
Albertsen BK, Schrøder H, Jakobsen P, et al. Antibody formation during intravenous and intramuscular therapy with Erwinia asparaginase. Med Pediatr Oncol. 2002;38(5):310. | ||
Woo MH, Hak LJ, Storm MC, et al. Hypersensitivity or development of antibodies to asparaginase does not impact treatment outcome of childhood acute lymphoblastic leukemia. Clin Oncol. 2000;18(7):1525. | ||
Panosyan EH, Seibel NL, Martin-Aragon S, et al. Asparaginase antibody and asparaginase activity in children with higher-risk acute lymphoblastic leukemia: Children’s Cancer Group Study CCG-1961. J Pediatr Hematol Oncol. 2004;26(4):217. | ||
Caruso V, Iacoviello L, Di Castelnuovo A, et al. Thrombotic complications in childhood acute lymphoblastic: a meta-analysis of 17 prospective studies comprising 1752 pediatric patients. Blood. 2006;108:2216–2222. | ||
Elliot MA, Wolf RC, Hook CC, et al. Thromboembolism in adults with acute lymphoblastic leukemia during induction with L-asparaginase-containing multi-agent regimens: incidence, risk factors, and possible role of antithrombin. Leuk Lymphoma. 2004;45:1545–1549. | ||
Grace RF, Dahlberg SE, Neuberg D, et al. The frequency and management of asparaginase-related thrombosis in paediatric and adult patients with acute lymphoblastic leukaemia treated on Dana-Farber Cancer Institute consortium protocols. Br J Haematol. 2011;152:452–459. | ||
Mitchell LG, Andrew M, Hanna K, et al. A prospective cohort study determining the prevalence of thrombotic events in children with acute lymphoblastic leukemia and a central venous line who are treated with L-asparaginase: results of the prophylactic antithrombin replacement in kids treated with acute lymphoblastic leukemia treated with asparaginase (PARKAA) study. Cancer. 2003;97:508–516. | ||
Couturier MA, Huguet F, Chevallier P, et al. Cerebral venous thrombosis in adult patients with acute lymphoblastic leukemia or lymphoblastic lymphoma during induction chemotherapy with L-asparaginase: The GRAALL experience. Am J Hematol. 2015;90(11):986–991. | ||
Ranta S, Tuckuviene R, Mäkiperaa A, et al. Cerebral sinus venous thromboses in children with acute lymphoblastic leukaemia – a mulitcentre study from the Nordic Society of Paediatric Haematology and Oncology. Br J Haematol. 2015;168(4):547–552. | ||
Hoelzer D, Thiel E, Löffler H, et al. Intensified therapy in acute lymphoblastic and acute undifferentiated leukemia in adults. Blood. 1984;64(1):38–47. | ||
DeAngelo DJ, Stevenson KE, Dahlberg SE, et al. Long-term outcome of a pediatric-inspired regimen used for adults aged 18–50 years with newly diagnosed acute lymphoblastic leukemia. Leukemia. 2015;29:526–534. | ||
Silverman LB, Gelber RD, Dalton VK, et al. Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood. 2001;97(5):1211–1218. | ||
Douer D, Aldoss I, Lunning MA, et al. Pharmacokinetics-based integration of multiple doses of intravenous pegaspargase in a pediatric regimen for adults with newly diagnosed acute lymphoblastic leukemia. J Clin Oncol. 2014;32(9):905–911. | ||
Rijneveld AW, van der Holt B, Daenen SM, et al. Intensified chemotherapy inspired by a pediatric regimen combined with allogeneic transplantation in adult patients with acute lymphoblastic leukemia up to the age of 40. Leukemia. 2011;25(11):1697–1703. | ||
Huguet F, Leguay T, Raffoux E, et al. Pediatric-inspired therapy in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia: the GRAALL-2003 study. J Clin Oncol. 2009;27(6):911–918. | ||
Storring JM, Minden MD, Kao S, et al. Treatment of adults with BCR-ABL negative acute lymphoblastic leukaemia with a modified paediatric regimen. Br J Haematol. 2009;146(1):76–85. | ||
Kadia TM, Kantarjian HM, Thomas DA, et al. Phase II study of methotrexate, vincristine, pegylated-asparaginase, and dexamethasone (MOpAD) in patients with relapsed/refractory acute lymphoblastic leukemia. Am J Hematol. 2015;90(2):120–124. | ||
Domenech C, Thomas X, Chabaud S, et al. L-asparaginase loaded red blood cells in refractory or relapsing acute lymphoblastic leukaemia in children and adults: results of the GRASPALL 2005-01 randomized trial. Br J Haematol. 2011;153(1):58–65. | ||
Hunault-Berger M, Leguay T, Dombret H, et al. A Phase 2 study of L-asparaginase encapsulated in erythrocytes in elderly patients with Philadelphia chromosome negative acute lymphoblastic leukemia: The GRASPALL/GRAALL-SA2-2008 study. Am J Hematol. 2015;90(9):811–818. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.