")
Back to Journals » Clinical Ophthalmology » Volume 8
Safety and efficacy of fixed-combination travoprost/timolol in patients with open-angle glaucoma or ocular hypertension not controlled with timolol monotherapy
Authors da Silva Jordão, Hatanaka M, Ogundele A, de Moraes Silva MR, Vessani R
Received 22 April 2014
Accepted for publication 10 June 2014
Published 18 August 2014 Volume 2014:8 Pages 1527—1534
DOI https://doi.org/10.2147/OPTH.S66613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Marcelo Lopes da Silva Jordão,1 Marcelo Hatanaka,2 Abayomi Ogundele,3 Maria Rosa Bet de Moraes Silva,4 Roberto Murad Vessani5
1Faculty of Medicine of Ribeirão Preto, University of São Paulo, São Paulo, Brazil; 2University of São Paulo School of Medicine, São Paulo, Brazil; 3Global Medical Affairs, Alcon Laboratories, Inc., Fort Worth, TX, USA; 4Faculty of Medicine of Botucatu, Universidade Estadual Paulista (UNESP), São Paulo, Brazil; 5General Hospital of Itapecerica da Serra, Serviço Social da Construção Civil do Estado de São Paulo (SECONCI-SP) São Paulo, Brazil
Objective: To assess the intraocular pressure (IOP)-lowering effect of travoprost 0.004%/timolol 0.5% fixed-dose combination (TRAV/TIM–FC) in patients not achieving the target IOP of ≤18 mmHg while on timolol 0.5% (TIM) monotherapy.
Methods: A multicenter, prospective, open-label study (NCT01336569) was conducted in patients with open-angle glaucoma or ocular hypertension. Eligible patients were receiving TIM monotherapy with a screening/baseline IOP of 19–35 mmHg in ≥1 eye. TIM was discontinued on the baseline visit day (no washout period) and TRAV/TIM–FC was initiated and administered once daily at 8 pm for 4–6 weeks. The primary efficacy variable was mean change in IOP from TIM-treated baseline to study end, measured by Goldmann applanation tonometry. Results were analyzed by analysis of variance and paired samples t-test (5% significance).
Results: A total of 49 patients were enrolled (mean age, 63 [range, 42–82] years; 55.1% White; 73.5% women), and 45 were included in the intent-to-treat (ITT) population. Mean duration of treatment with TRAV/TIM–FC was 31 days. Mean ± standard deviation IOP reduction from baseline (TIM) to the follow-up visit (TRAV/TIM–FC) was -5.0±3.6 mmHg. IOP decreased significantly (P<0.0001) from baseline (22.1±2.6 mmHg) to study end (17.1±3.9 mmHg) in the ITT population, with a mean IOP reduction of 22.3%. Most patients (n=33/45; 73.3%) achieved IOP ≤18 mmHg. Two patients experienced a total of four adverse events (AEs), including a patient who reported one serious AE (enterorrhagia) that was considered unrelated to treatment, and a patient who reported one event each of drug-related redness, pruritus, and foreign body sensation. Most patients (n=47/49; 95.9%) reported no AEs.
Conclusions: TRAV/TIM–FC lowered IOP in patients who were not at target IOP while receiving TIM monotherapy, with most patients achieving an IOP ≤18 mmHg with TRAV/TIM–FC. TRAV/TIM–FC was well tolerated in this population.
Keywords: DuoTrav®, intraocular pressure, primary open-angle glaucoma, time since diagnosis
Introduction
Glaucoma and ocular hypertension are associated with elevated intraocular pressure (IOP) and progressive visual field deterioration. An analysis of published data estimated the number of people with glaucoma worldwide to be more than 60 million in 2010 and nearly 80 million by 2020, with 74% of these individuals diagnosed with open-angle glaucoma.1 Elevated IOP is a causal risk factor for optic nerve damage and vision loss and is one of the only readily treatable causes or symptoms of glaucoma and ocular hypertension.2,3
Topical administration of pharmacologic IOP-lowering agents is the first line of therapy for glaucoma and ocular hypertension. β-blockers like the nonselective β-adrenergic receptor antagonist timolol maleate have historically been the first choice of treatment.2–4 Prostaglandin analogs (PGAs), such as travoprost, reduce IOP in patients with glaucoma or ocular hypertension more effectively than timolol, and PGAs are generally well tolerated.5 Pharmacologic therapy is typically initiated with a single agent, but many patients require one or more additional agents to maintain sufficient IOP reduction after the first year of treatment.6 Compared with multiple agents in individual bottles or administered at different times of day, fixed-combination medications are associated with better treatment adherence.7,8 Additionally, fixed combinations do not introduce risk of drug washout, additive exposure to preservatives, or increased treatment complexity, which can occur when multiple individual ocular hypotensive therapies are administered concomitantly.9–12 A meta-analysis of 18 clinical trials that compared the efficacy and tolerability of fixed combinations of PGAs and β-blockers versus their components in unfixed combinations or as monotherapies found that the fixed combinations resulted in lower risk of hyperemia than unfixed combinations or PGA monotherapies.13 Fixed-combination therapies were found to be more effective in reducing IOP compared with monotherapies. Fixed-combination therapies were not as effective in reducing IOP as unfixed combinations; however, the analysis of fixed versus unfixed combinations was limited to five studies, and dosing times of the components may have been different (eg, once daily versus twice daily).13
As discussed elsewhere,14 travoprost and timolol have complementary ocular hypotensive mechanisms, similar pharmacokinetics, and compatible physiochemical properties; furthermore, the safety and IOP-lowering efficacy of a fixed combination of travoprost and timolol has been demonstrated.14 Fixed-combination travoprost 0.004% (TRAV)/timolol 0.5% (TIM) is currently available in formulations preserved with benzalkonium chloride (BAK; TRAV/TIM–FC [DuoTrav®; Alcon Laboratories, Fort Worth, TX, USA]) or polyquaternium-1 (POLYQUAD® [Alcon Laboratories]).14 These two formulations were demonstrated to be equally effective in reducing IOP in patients with open-angle glaucoma or ocular hypertension.15 It is not yet clear whether disease duration influences the IOP-lowering efficacy of TRAV/TIM–FC or its components.
The objective of this study was to assess the safety and IOP-lowering efficacy of changing to BAK-preserved TRAV/TIM–FC in patients with open-angle glaucoma or ocular hypertension uncontrolled with TIM monotherapy.
Methods
Study design and treatment
This was a prospective, multicenter, phase IV, open-label, noncomparative, single-arm study (www.ClinicalTrials.gov identifier, NCT01336569) conducted at four study centers in Brazil between February 2011 and March 2012. The purpose of this study was to assess the safety and IOP-lowering efficacy of changing to TRAV/TIM–FC in patients with open-angle glaucoma or ocular hypertension not sufficiently controlled by TIM monotherapy (ie, with IOP ≥19 mmHg) and requiring additional IOP reduction. The study consisted of two visits: the screening/baseline visit (visit 1), and a follow-up visit conducted at the end of treatment, 4–6 weeks after screening (visit 2). Before participation in the current study, patients were receiving TIM monotherapy. At the conclusion of visit 1, patients discontinued TIM monotherapy and initiated once-daily TRAV/TIM–FC treatment, with no washout period. One eye from each patient was chosen as the study eye; only the study eye was used in the efficacy analysis. If only one eye received medication, that eye was the study eye; if both eyes received medication, the eye with higher IOP at visit 1 was selected as the study eye. If baseline IOP was equal in both eyes, the right eye was chosen. Patients were instructed to instill one drop of TRAV/TIM–FC in the eye(s) to be treated once per day at 8 pm for 4–6 weeks.
The study was conducted in accordance with the Declaration of Helsinki, and all study protocols and consent forms were reviewed and approved by the ethics committees of all study centers. Participating patients gave written informed consent before enrollment.
Patients
Eligible participants were aged ≥18 years and were diagnosed with primary open-angle glaucoma, pigmentary glaucoma, or ocular hypertension. Additional inclusion criteria were a stable IOP-lowering medication regimen for ≥1 week before screening; IOP considered safe in both eyes to ensure clinical stability of vision and optic nerve throughout the study; IOP between 19–35 mmHg in ≥1 eye; IOP in the non-study eye able to be controlled with either the study drug or no treatment; and best corrected visual acuity (BCVA) better than 20/200 (Snellen) or <1.0 logMAR in both eyes. Key exclusion criteria were history of allergy, hypersensitivity, or low tolerance to components of TRAV/TIM–FC; abnormalities preventing applanation tonometry or fundus/anterior chamber examination; corneal dystrophy; concomitant conjunctivitis, keratitis, or uveitis; conventional or laser surgery in either eye within 3 months before screening; progressive retinal or optic nerve disease; history or risk of uveitis or cystoid macular edema; history of Herpes simplex eye infection; heart conditions presenting a risk to administration of topical β-blockers (ie, sinus bradycardia, sinoatrial or atrioventricular block, heart failure, or cardiogenic shock); asthma or severe chronic obstructive pulmonary disease; severe allergic rhinitis or bronchial hyper-responsiveness; women who were pregnant, nursing, or planning to become pregnant; or participation in another clinical study within 30 days before the screening visit. Patients receiving systemic treatments that could affect IOP were required to be on a stable regimen for ≥7 days before screening without requiring a dosage change during the study period.
Efficacy assessments
The primary efficacy endpoint was mean IOP change from baseline (patients receiving TIM) at visit 2 (patients receiving TRAV/TIM–FC), measured at approximately the same time of day. IOP was assessed by Goldmann applanation tonometry twice consecutively at each visit; if the two measurements for the same eye differed by >2 mmHg, a third measurement was taken and the two IOP measurements closest to each other were averaged. If the three measurements differed by equal amounts, the three measurements were averaged. All IOP assessments for any one patient were performed by the same operator using the same standard tonometer. Overall IOP percent change from baseline, as well as mean IOP levels and percent IOP reduction from baseline in patients diagnosed with glaucoma for ≤4 years versus >4 years, were assessed as additional efficacy endpoints. An arbitrary treatment duration cutoff of 4 years was chosen to allow assessment of whether time since diagnosis might affect IOP response to TRAV/TIM–FC.
Safety assessments
Adverse events (AEs) were recorded at visit 2, or as necessary, and assessed for causality by study investigators. BCVA was measured using the Snellen visual acuity chart at visits 1 and 2; if more than one error was recorded on a given line, the results were rounded up. Slit lamp fundus biomicroscopy of both eyes, including the cornea, sclera, eyelids, conjunctiva, anterior chamber, and iris, was performed for each patient at visits 1 and 2, before IOP assessment.
Statistical analysis
Patient demographics and baseline characteristics were summarized using descriptive statistics. Mean IOP change from baseline was evaluated in the intent-to-treat (ITT) population (ie, all patients receiving study medication and attending visits 1 and 2) and the per-protocol (PP) population (ie, all patients receiving study medication, attending visits 1 and 2, and meeting medication compliance criteria) by paired t-tests. Efficacy endpoints, stratified by time since diagnosis, were evaluated by analysis of variance and t-test. AEs were evaluated in the safety population (ie, all patients receiving study medication) and were summarized descriptively. BCVA and biomicroscopy observations were analyzed in the safety population; biomicroscopy observations at visits 1 and 2 were compared by McNemar’s test. Statistical analyses were performed using Statistica (version 5.1/97; StatSoft, Inc., Tulsa, OK, USA) with significance established at the 5% level.
Results
Patients
A total of 49 patients were enrolled, received TRAV/TIM–FC at visit 1, and were included in the safety population. At screening, patients had a mean age ± standard deviation (SD) of 63±11 years; most (73.5%, n=36/49) were women, and 55.1% (n=27/49) were White (Table 1). Most patients (79.6%, n=39/49) were diagnosed with primary open-angle glaucoma, and all patients had IOPs ranging from 19–28 mmHg while receiving TIM. Four patients were lost to follow-up because of non-attendance at visit 2; 45 patients attended visits 1 and 2 and were included in the ITT population. Mean time ± SD on TRAV/TIM–FC treatment was 31.1±4.7 days (range, 27–50 days; median, 30 days).
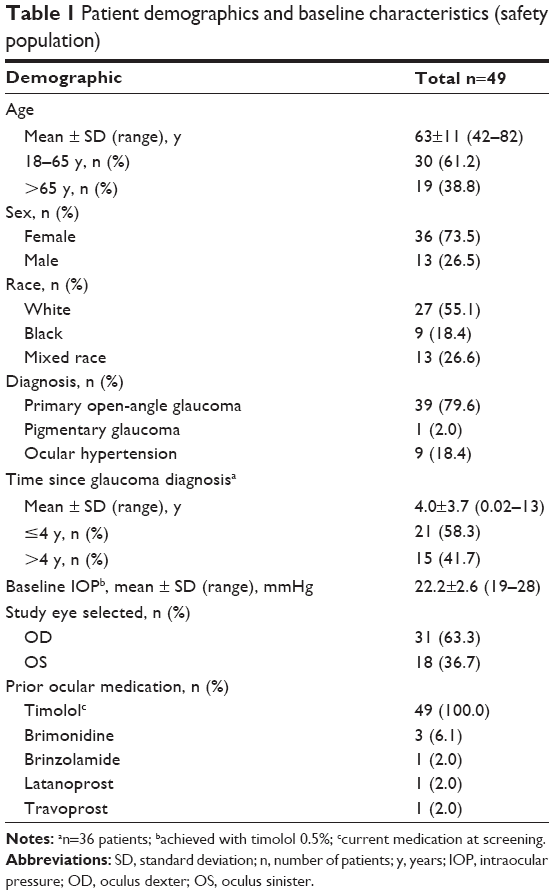 | Table 1 Patient demographics and baseline characteristics (safety population) |
Efficacy
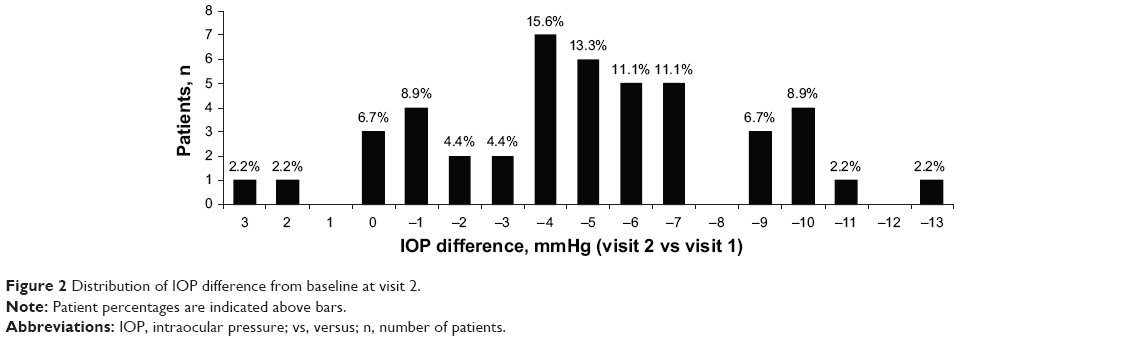
Efficacy data for the ITT and PP data sets were similar; therefore, results for the ITT population are presented. Mean ± SD IOP reduction from baseline to visit 2 (primary endpoint) was -5.0±3.6 mmHg (Figure 1A); IOP decreased from 22.1±2.6 (range, 19–28) mmHg at visit 1 to 17.1±3.9 (range, 10–27) mmHg at visit 2 (P<0.0001). At visit 1, 0/45 ITT patients had IOP ≤18 mmHg; at visit 2, 33/45 (73.3%) patients had IOP ≤18 mmHg (Figure 1B). Individual IOP changes from baseline ranged from +3 to -13 mmHg (Figure 2).
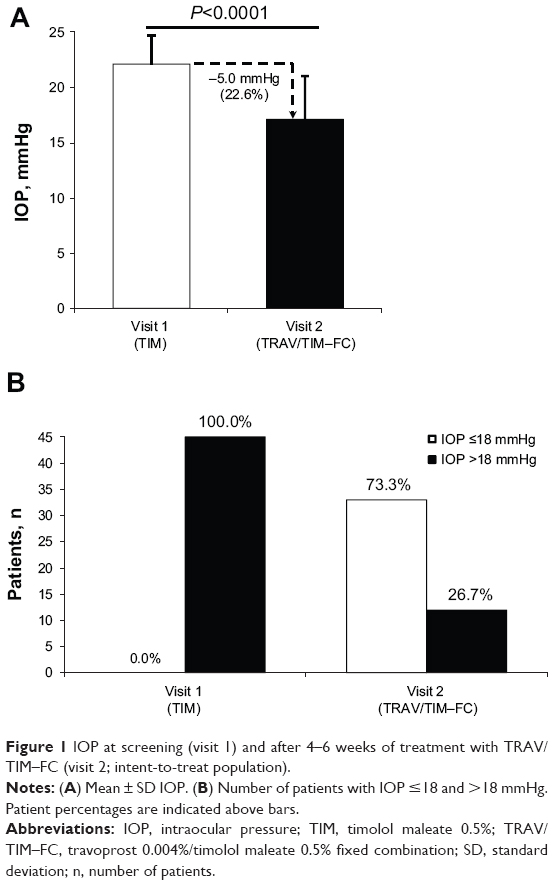 | Figure 1 IOP at screening (visit 1) and after 4–6 weeks of treatment with TRAV/TIM–FC (visit 2; intent-to-treat population). |
 | Figure 2 Distribution of IOP difference from baseline at visit 2. |
Baseline IOP (mean ± SD) was not significantly different for patients diagnosed for ≤4 years (21.6±2.1 mmHg; n=19) compared with patients diagnosed for >4 years (23.5±3.4 mmHg, n=13; P=0.0585). At visit 2, mean IOP levels were significantly lower in patients diagnosed with glaucoma for ≤4 years (15.4 mmHg, n=19) compared with patients diagnosed for >4 years (19.2 mmHg, n=13; P<0.05; Figure 3A). Mean IOP reduction from baseline was 28.9% for patients diagnosed with glaucoma for ≤4 years compared with 18.4% for patients diagnosed with glaucoma for >4 years (Figure 3B). Overall, mean percentage IOP reduction ± SD was -22.3%±15.7%.
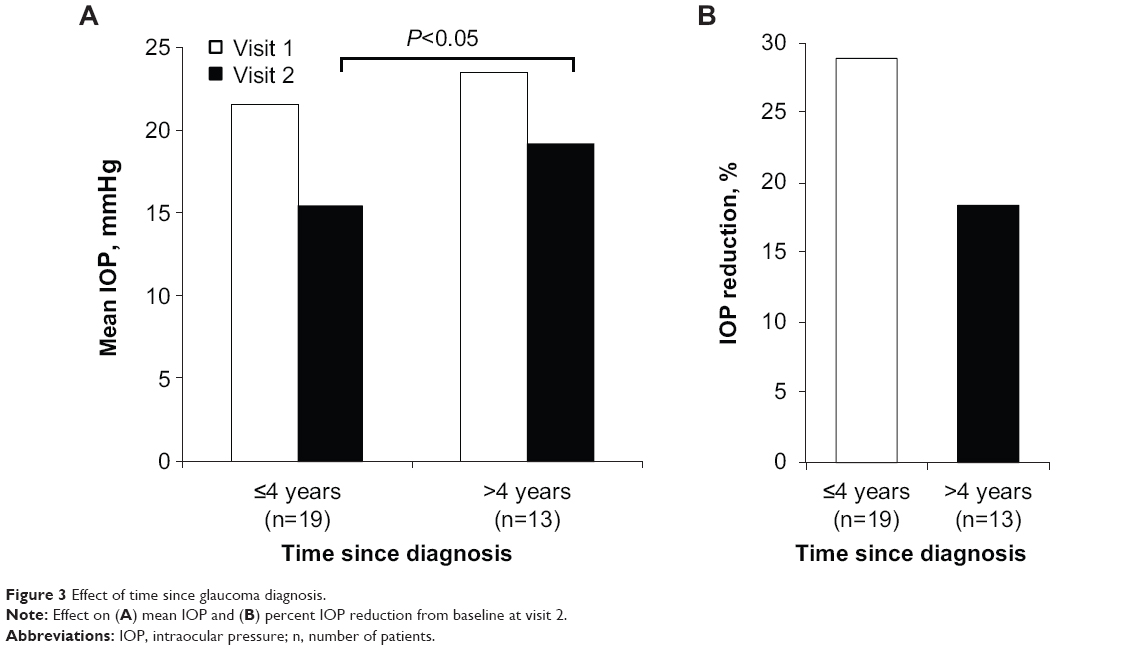 | Figure 3 Effect of time since glaucoma diagnosis. |
Safety
Treatment with TRAV/TIM–FC was generally well tolerated. Most patients (95.9%, n=47/49) reported no AEs. A total of four AEs, including one serious AE (SAE), were reported. One event each of redness, pruritus, and foreign body sensation was reported by the same patient; these AEs were considered related to the study drug. Pruritus was reported as severe, and redness and foreign body sensation were moderate. One patient reported enterorrhagia, which was classified as an SAE and considered unrelated to the study drug. No patient discontinued because of an AE or SAE.
Distribution of BCVA was similar between visits 1 and 2. The percentage of patients with BCVA better than 20/80 was unchanged between visits (visit 1, n=42/49 [85.7%]; visit 2, 39/45 [86.7%]). Biomicroscopy observations were similar at visits 1 and 2 (Table 2). The only statistically significant finding for this safety endpoint was redness of eyelids or conjunctiva, which was observed in 24.4% of patients at visit 2 compared with 2.0% of patients at visit 1 (P=0.0026).
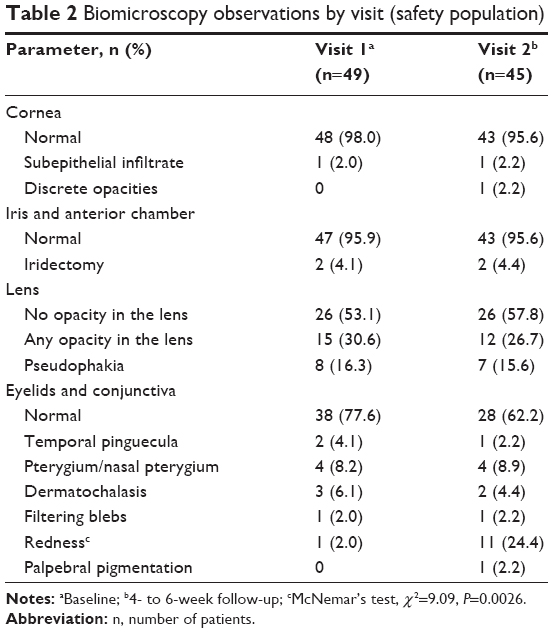 | Table 2 Biomicroscopy observations by visit (safety population) |
Discussion
Pharmacologic management of IOP with one or more ocular hypotensive agents is the standard of care for glaucoma; most patients require multiple medications to maintain sufficient IOP reduction after the first year of treatment.6 Fixed-combination therapies provide multiple IOP-lowering agents in a single bottle, simplifying administration and improving adherence.8,16 The goal of this study was to evaluate the IOP-lowering efficacy and safety of the PGA/β-blocker ocular hypotensive TRAV/TIM–FC in patients diagnosed with glaucoma or ocular hypertension with IOP not controlled with TIM monotherapy.
Treatment with TRAV/TIM–FC demonstrated increased IOP-lowering efficacy compared with TIM monotherapy. Specifically, an average of 31 days of TRAV/TIM–FC lowered IOP from TIM-treated baseline by approximately 5 mmHg, or 22%. At baseline, no patients receiving TIM had an IOP ≤18 mmHg; with TRAV/TIM–FC treatment, nearly 75% of patients achieved IOP ≤18 mmHg. The Advanced Glaucoma Intervention Study previously found that maintaining IOP <18 mmHg decreased visual field degeneration throughout 6 years of follow-up.17 TRAV/TIM–FC was well tolerated. A total of three non-serious AEs were considered related to study treatment, and 96% of patients reported no AEs throughout the study. The most frequent change from baseline in biomicroscopy observations was an increase in redness, which was observed in 2% of patients at visit 1 and 24% of patients at visit 2.
The findings of this study are consistent with previous reports of the IOP-lowering safety and efficacy of TRAV/TIM–FC. In prior studies, as in the current work, redness or hyperemia was the most frequently observed AE associated with TRAV/TIM–FC and was reported in approximately 6%–14% of patients; TRAV/TIM–FC was generally well tolerated and associated with minimal changes in ocular signs and biomicroscopy observations.18–21 In three non-interventional, open-label, multicenter studies, patients with glaucoma or ocular hypertension receiving once-daily TRAV/TIM–FC for 4–6 weeks achieved significant IOP reductions of 4.6–5.5 mmHg, or 21%–25%, from TIM-treated baseline.19,20,22 Furthermore, two double-masked, randomized, active-controlled, parallel-group trials demonstrated that, after 6 weeks of treatment, once-daily TRAV/TIM–FC reduced IOP to a significantly greater extent than twice-daily TIM.18,21 In the current study, IOP change from baseline ranged from +3 mmHg to −13 mmHg with TRAV/TIM–FC. Most patients (n=36/45, 80%) achieved IOP reduction of at least 2 mmHg from baseline TIM-treated levels. Seven patients experienced an IOP change from baseline of 0 or 1 mmHg, suggesting that these patients may not have been responsive to TRAV. IOP was increased from baseline in two patients (+2 mmHg and +3 mmHg, respectively); these patients may have been non-responsive to TRAV and experienced increased IOP because of a potential reduction in TIM dosing (ie, twice-daily before enrollment versus once-daily during the study). However, because TIM dosing schedules prior to study enrollment were not evaluated at screening, support for this hypothesis is limited.
Interestingly, in the current study, patients diagnosed with glaucoma or ocular hypertension for ≤4 years achieved significantly greater IOP reductions compared with patients diagnosed for >4 years. IOP reductions from baseline were nearly 30% in patients who had been diagnosed within 4 years, but were <20% in those who were diagnosed over 4 years. Baseline IOP in patients diagnosed for >4 years was slightly higher than in those diagnosed for ≤4 years; however, this difference was of small magnitude and was not statistically significant. Taken together, these data suggest that patients switched to TRAV/TIM–FC therapy earlier may respond better to treatment.
Previous studies have shown that TRAV/TIM–FC is also more effective than TRAV monotherapy in reducing IOP; furthermore, the two drugs have similar safety profiles.18,23,24 In a prospective, open-label, historical-controlled, single-arm trial of patients in Brazil who were switched from PGA monotherapy (travoprost, bimatoprost, or latanoprost) to TRAV/TIM–FC because of insufficient IOP reduction, 4 weeks of TRAV/TIM–FC reduced IOP by an additional ~19% from baseline values maintained with PGA monotherapy.23 Similarly, in a randomized, double-masked, 8-week trial of TRAV/TIM–FC versus TRAV, TRAV/TIM–FC maintained significantly lower mean IOP than TRAV, with less 24-hour fluctuation.24 These findings are supported by the results of a meta-analysis that demonstrated greater IOP-lowering efficacy of PGA/β-blocker fixed combinations compared with monotherapy with one of their components.13 Compared with fixed and unfixed combinations of latanoprost/TIM, TRAV/TIM–FC produced similar IOP reduction from baseline25–27 with significantly lower mean IOP 24 hours after dosing.27 Treatments had similar safety profiles. Hyperemia has been observed with TRAV, TRAV/TIM–FC, and fixed and unfixed combinations of latanoprost/TIM; in these studies, rates of hyperemia with TRAV/TIM–FC varied from 2.5%–15%.24,26,27 Additional studies are needed to establish hyperemia rates of fixed-combination, polyquaternium-1-preserved TRAV/TIM compared with TRAV/TIM–FC. It has been hypothesized that BAK-free TRAV/TIM–FC may have less ocular surface toxicity without compromising IOP-lowering efficacy and therefore may be a preferred option for patients with ocular surface disease.14
The relatively small study population and single-arm, historical-control design are potential limitations of the current study. Compliance with TIM treatment before study initiation may have been lower than with TRAV/TIM–FC during the study period because of potential effects of participation in a clinical trial.28 Typical patient adherence to glaucoma treatment has been low; depending on the stringency of the definition of “non-adherent” used, rates of non-adherence to ocular hypotensive medication have ranged from 5%–80%.29 Additional studies are needed to investigate the effect of increasing duration after diagnosis on magnitude of IOP reduction with TRAV/TIM–FC.
Conclusion
This study demonstrated the safety and IOP-lowering efficacy of changing from TIM monotherapy to TRAV/TIM–FC in patients with open-angle glaucoma or ocular hypertension uncontrolled with TIM. A significant decrease in mean IOP was observed after 4–6 weeks of treatment, demonstrating that TRAV/TIM–FC was effective in controlling IOP for patients with glaucoma who could not achieve target IOP with TIM monotherapy alone. The magnitude of IOP reduction was greater in patients diagnosed with glaucoma for ≤4 years compared with patients diagnosed for >4 years. TRAV/TIM–FC was generally well tolerated, with only four AEs reported in two patients. No differences in BCVA were observed between visits 1 and 2. The only safety measure that was significantly more frequent at visit 2 (with TRAV/TIM–FC treatment) versus visit 1 (with TIM treatment) was redness of the eyelids or conjunctiva.
Acknowledgments
Dr Roberto Freire Santiago Malta (Faculty of Medicine, University of São Paulo, São Paulo, Brazil) is gratefully acknowledged for his participation in the study and for his review of early drafts of the manuscript. The authors further thank Virgilio Freitas Costa for his role as sub-principal investigator. This study was sponsored by Alcon Laboratories, Inc. (Fort Worth, TX, USA). Medical writing support was provided by Heather D Starkey, PhD, of Complete Healthcare Communications, Inc. (Chadds Ford, PA, USA) and was funded by Alcon.
Disclosure
AO is an Alcon employee; MJLDS, MH, MRBDMS, and RMV have no conflicts of interest related to this work to report.
References
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267. | ||
van Gestel A, Webers CA, Severens JL, et al. The long-term outcomes of four alternative treatment strategies for primary open-angle glaucoma. Acta Ophthalmol. 2012;90(1):20–31. | ||
Webers CA, Beckers HJ, Nuijts RM, Schouten JS. Pharmacological management of primary open-angle glaucoma: second-line options and beyond. Drugs Aging. 2008;25(9):729–759. | ||
Boyle JE, Ghosh K, Gieser DK, Adamsons IA; Dorzolamide-Timolol Study Group. A randomized trial comparing the dorzolamide-timolol combination given twice daily to monotherapy with timolol and dorzolamide. Ophthalmology. 1998;105(10):1945–1951. | ||
Alexander CL, Miller SJ, Abel SR. Prostaglandin analog treatment of glaucoma and ocular hypertension. Ann Pharmacother. 2002;36(3):504–511. | ||
Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):701–713. | ||
Tsai JC, McClure CA, Ramos SE, Schlundt DG, Pichert JW. Compliance barriers in glaucoma: a systematic classification. J Glaucoma. 2003;12(5):393–398. | ||
Djafari F, Lesk MR, Harasymowycz PJ, Desjardins D, Lachaine J. Determinants of adherence to glaucoma medical therapy in a long-term patient population. J Glaucoma. 2009;18(3):238–243. | ||
Chrai SS, Makoid MC, Eriksen SP, Robinson JR. Drop size and initial dosing frequency problems of topically applied ophthalmic drugs. J Pharm Sci. 1974;63(3):333–338. | ||
Higginbotham EJ. Considerations in glaucoma therapy: fixed combinations versus their component medications. Clin Ophthalmol. 2010;4:1–9. | ||
Pisella PJ, Pouliquen P, Baudouin C. Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br J Ophthalmol. 2002;86(4):418–423. | ||
Robin AL, Novack GD, Covert DW, Crockett RS, Marcic TS. Adherence in glaucoma: objective measurements of once-daily and adjunctive medication use. Am J Ophthalmol. 2007;144(4):533–540. | ||
Quaranta L, Biagioli E, Riva I, et al. Prostaglandin analogs and timolol-fixed versus unfixed combinations or monotherapy for open-angle glaucoma: a systematic review and meta-analysis. J Ocul Pharmacol Ther. 2013;29(4):382–389. | ||
Konstas AG, Quaranta L, Realini T. Overview of the [corrected] travoprost/timolol BAK-free fixed combination. Expert Opin Pharmacother. 2012;13(5):757–766. | ||
Kitazawa Y, Smith P, Sasaki N, Kotaki S, Bae K, Iwamoto Y. Travoprost 0.004%/timolol 0.5%-fixed combination with and without benzalkonium chloride: a prospective, randomized, doubled-masked comparison of safety and efficacy. Eye (Lond). 2011;25(9):1161–1169. | ||
Sleath B, Robin AL, Covert D, Byrd JE, Tudor G, Svarstad B. Patient-reported behavior and problems in using glaucoma medications. Ophthalmology. 2006;113(3):431–436. | ||
The Advanced Glaucoma Intervention Study (AGIS) Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130(4):429–440. | ||
Barnebey HS, Orengo-Nania S, Flowers BE, et al. The safety and efficacy of travoprost 0.004%/timolol 0.5% fixed combination ophthalmic solution. Am J Ophthalmol. 2005;140(1):1–7. | ||
Mandić Z, Novak-Laus K, Bojić L, et al. Safety and efficacy of monotherapy change to fixed combination (travoprost 0.004%/timolol 0.5%) in 6 months follow up period. Acta Clin Croat. 2010;49(4):411–419. | ||
Pfeiffer N, Scherzer ML, Maier H, et al. Safety and efficacy of changing to the travoprost/timolol maleate fixed combination (DuoTrav) from prior mono- or adjunctive therapy. Clin Ophthalmol. 2010;4: 459–466. | ||
Schuman JS, Katz GJ, Lewis RA, et al. Efficacy and safety of a fixed combination of travoprost 0.004%/timolol 0.5% ophthalmic solution once daily for open-angle glaucoma or ocular hypertension. Am J Ophthalmol. 2005;140(2):242–250. | ||
Arend KO, Raber T. Observational study results in glaucoma patients undergoing a regimen replacement to fixed combination travoprost 0.004%/timolol 0.5% in Germany. J Ocul Pharmacol Ther. 2008;24(4):414–420. | ||
Costa VP, Moreira H, Paolera MD, de Moraes Silva MR. Efficacy and safety of travoprost 0.004%/timolol 0.5% fixed combination as transition therapy in patients previously on prostaglandin analog monotherapy. Clin Ophthalmol. 2012;6:699–706. | ||
Konstas AG, Mikropoulos D, Haidich AB, Ntampos KS, Stewart WC. Twenty-four-hour intraocular pressure control with the travoprost/timolol maleate fixed combination compared with travoprost when both are dosed in the evening in primary open-angle glaucoma. Br J Ophthalmol. 2009;93(4):481–485. | ||
Pachimkul P, Yuttitham K, Thoophom P. 24-Hour intraocular pressure control between travoprost/timolol fixed combination, latanoprost/timolol fixed combination and standard timolol in primary open angle glaucoma and ocular hypertension. J Med Assoc Thai. 2011;94(S2):S81–S87. | ||
Rhee DJ, Peace JH, Mallick S, et al; Study Group. A study of the safety and efficacy of travoprost 0.004%/timolol 0.5% ophthalmic solution compared to latanoprost 0.005% and timolol 0.5% dosed concomitantly in patients with open-angle glaucoma or ocular hypertension. Clin Ophthalmol. 2008;2(2):313–319. | ||
Topouzis F, Melamed S, Danesh-Meyer H, et al. A 1-year study to compare the efficacy and safety of once-daily travoprost 0.004%/timolol 0.5% to once-daily latanoprost 0.005%/timolol 0.5% in patients with open-angle glaucoma or ocular hypertension. Eur J Ophthalmol. 2007; 17(2):183–190. | ||
Andrade S. Compliance in the real world. Value Health. 1998;1(3): 171–173. | ||
Olthoff CM, Schouten JS, van de Borne BW, Webers CA. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension an evidence-based review. Ophthalmology. 2005;112(6):953–961. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.