")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 13
Safety and Efficacy of Lenvatinib Treatment in Child–Pugh A and B Patients with Unresectable Hepatocellular Carcinoma in Clinical Practice: A Multicenter Analysis
Authors Ogushi K , Chuma M , Uojima H, Hidaka H , Numata K , Kobayashi S, Hirose S, Hattori N, Fujikawa T, Nakazawa T, Wada N, Iwasaki S, Fukushima T, Sano Y , Ueno M , Kawano K, Tsuruya K , Shomura M, Watanabe T, Matsunaga K, Kunishi Y, Saigusa Y , Irie K, Iwabuchi S, Kako M, Morimoto M, Kagawa T, Tanaka K, Maeda S
Received 23 April 2020
Accepted for publication 4 August 2020
Published 1 October 2020 Volume 2020:13 Pages 385—396
DOI https://doi.org/10.2147/CEG.S256691
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Everson L.A. Artifon
Katsuaki Ogushi,1,* Makoto Chuma,1,* Haruki Uojima,2 Hisashi Hidaka,2 Kazushi Numata,1 Satoshi Kobayashi,3 Shunji Hirose,4 Nobuhiro Hattori,5 Tomoaki Fujikawa,6 Takahide Nakazawa,2 Naohisa Wada,2 Shuitirou Iwasaki,2 Taito Fukushima,3 Yusuke Sano,3 Makoto Ueno,3 Kuniyuki Kawano,3 Kota Tsuruya,4 Masako Shomura,4 Tsunamasa Watanabe,5 Kotaro Matsunaga,5 Yosuke Kunishi,7 Yusuke Saigusa,8 Kuniyasu Irie,9 Shogo Iwabuchi,6 Makoto Kako,10 Manabu Morimoto,3 Tatehiro Kagawa,4 Katsuaki Tanaka,11 Shin Maeda9
1Gastroenterological Center, Yokohama City University Medical Center, Yokohama, Japan; 2Department of Gastroenterology, Internal Medicine, Kitasato University School of Medicine, Sagamihara, Japan; 3Hepatobiliary and Pancreatic Medical Oncology, Kanagawa Cancer Center Hospital, Yokohama, Japan; 4Division of Gastroenterology and Hepatology, Department of Internal Medicine, Tokai University School of Medicine, Isehara, Japan; 5Division of Gastroenterology and Hepatology, Department of Internal Medicine, St. Marianna University School of Medicine, Kawasaki, Japan; 6Department of Gastroenterology, Shonan Fujisawa General Hospital, Fujisawa, Japan; 7Department of Gastroenterology, Kanagawa Prefectural Ashigarakami Hospital, Kanagawa, Japan; 8Department of Biostatistics, Yokohama City University Graduate School of Medicine, Yokohama, Japan; 9Department of Gastroenterology, Yokohama City University Hospital, Yokohama, Japan; 10Department of Gastroenterology, Shonan Kamakura General Hospital, Kamakura, Japan; 11Gastroenterology Division, Hadano Red Cross Hospital, Hadano, Japan
*These authors contributed equally to this work
Correspondence: Makoto Chuma Gastroenterological Center
Yokohama City University Medical Center, 4-57 Urafune-Cho, Minami-Ku, Yokohama, Kanagawa 2320024, Japan
Tel +81 45 261 5656
Fax +81 45 253 9955
Email [email protected]
Purpose: To assess the safety, efficacy and prognostic impact of clinical factors related to lenvatinib treatment in Child-Pugh class A (CP-A) and class B (CP-B) patients with unresectable hepatocellular carcinoma (u-HCC).
Methods: Patients with u-HCC who were treated with lenvatinib at multiple centers in Japan were retrospectively analyzed for treatment outcomes according to their respective CP status. Radiological objective response (OR) was assessed using modified response evaluation criteria in solid tumors (mRECIST) guidelines.
Results: Baseline demographic parameters were comparable between 126 (69.6%) patients with CP-A disease and 55 patients (30.4%) with CP-B disease. Frequency of lenvatinib-related adverse events, including decreased appetite (P=0.034), diarrhea (P=0.040), elevated serum bilirubin (P=0.016) and vomiting (P=0.009), were higher in CP-B than in CP-A patients. Relative dose intensity (RDI) was significantly higher in CP-A (0.69) than CP-B patients (0.50, P < 0.001). Furthermore, OR rate (44.0%) was markedly higher in CP-A5 patients as compared to CP-A6 (25.5%), CP-B7 (22.2%), and CP-B8 patients (5.3%), respectively (P=0.002). In multivariable analysis, performance status (0 vs 1, 2, P=0.026), CP class (A vs B, P=0.045) and RDI (≥ 0.7 vs < 0.7, P=0.034) were identified as factors associated with response to lenvatinib treatment. Overall survival (OS) at 12 months was significantly different between CP-A (66.3%) and CP-B patients (30.0%, P=0.002), and between CP 5– 7 (59.2%) and CP 8 patients (34.8%, P=0.003). In multivariable analysis, CP class (A vs B, P=0.007) and Barcelona clinic liver cancer (BCLC) stage (B vs C, P=0.002) were associated with OS following lenvatinib treatment.
Conclusion: Lenvatinib treatment offers significant benefits in patients with good liver function in real-world practice. The various characteristics identified in this study might be helpful as clinical predictors of response to lenvatinib and survival in clinical practice. Further studies are required to address eligibility for lenvatinib treatment in CP 7 patients.
Keywords: lenvatinib, tyrosine kinase inhibitor, hepatocellular carcinoma, Child-Pugh, adverse events, overall survival
Introduction
Globally, hepatocellular carcinoma (HCC) is one of the leading causes of cancer-related deaths.1,2 Systemic therapy using molecular targeted agents is the recommended standard treatment for advanced unresectable HCC.3
Lenvatinib is a multitargeted tyrosine kinase inhibitor of fibroblast growth factor (FGF) receptors 1–4 (FGFR), vascular endothelial growth factor (VEGF) receptors 1–3 (VEGFR), platelet-derived growth factor (PDGF) receptor, the rearranged during transfection (RET) oncogene, and KIT.4 Based on the results of the Phase III REFLECT trial, lenvatinib was recently approved for use as a first-line tyrosine kinase inhibitor for patients with unresectable HCC in Japan, the USA, the EU and Asia.5 The therapeutic potential of lenvatinib for u-HCC in clinical practice has also been reported in several recent studies.6–9 However, factors associated with outcomes following lenvatinib have not been clarified in large-scale studies evaluating actual clinical practice. Although several recent studies reported that patients with Child–Pugh A (CP-A) or modified albumin-bilirubin (mALBI)-grade 1/2a were predictive of a higher response rate,6,7 it is not always possible to select patients with well-preserved hepatic function since many HCC patients have hepatic dysfunction at the time of clinical presentation (CP-B). Additionally, the safety and efficacy of lenvatinib in CP-B patients with u-HCC has not been sufficiently investigated. Therefore, it is necessary to validate the results obtained in field studies using real-life studies.
The aim of this study was to assess the safety, efficacy and prognostic impact of clinical factors related to lenvatinib therapy in CP-A and CP-B patients with u-HCC.
Methods
Study Design and Patients
In this retrospective study, lenvatinib (Lenvima®; Eisai Co., Ltd., Tokyo, Japan) was administered orally to patients with u-HCC. The dose of lenvatinib was based on body weight, and it was administered at an initial dose of 12 mg/day for those weighing over 60 kg and 8 mg/day for those weighing less than 60 kg. For patients with CP-B disease, the initial dose was reduced from 12 mg to 8 mg once daily, as described in a clinical Phase I trial.10 Lenvatinib therapy was recommended for patients with u-HCC and patients that met the criteria shown in Figure 1A–C. Furthermore, inclusion criteria for patients treated with lenvatinib were: 1) patients with only HCC, 2) those who did not receive combination chemotherapy with other treatments, 3) in whom physical function was preserved, and 4) patients with complete clinical and follow-up data.
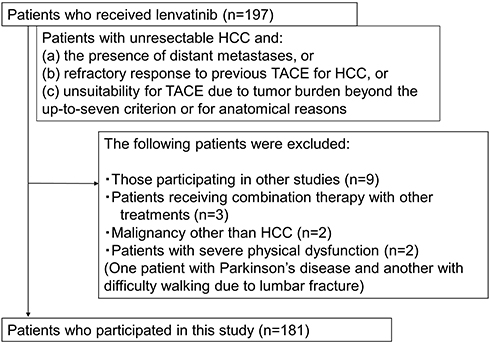 |
Figure 1 Flow chart showing patient enrollment in the study. |
We administered lenvatinib to 197 patients with unresectable or transarterial chemoembolization (TACE)-refractory HCC from March 2018 to March 2019. As shown in Figure 1, since nine patients who participated in other observational studies, two patients with cancer other than HCC, three patients who received combination chemotherapy with other treatments and two patients with severe physical dysfunction were excluded, a total of 181 patients were enrolled in this study. This retrospective study was conducted at 11 institutions in Kanagawa, Japan; Yokohama City Medical Center [n=29], Yokohama City University Hospital [n=1], Kitasato University Hospital [n=37], Kanagawa Cancer Center [n=35], Tokai University Hospital [n=27], St. Marianna University School of Medicine hospital [n=13], Shonan Kamakura General Hospital [n=20], Shonan Fujisawa Tokushukai Hospital [n=12], Japanese Red Cross Hadano Hospital [n=3], Yokohama Minami Kyosai Hospital [n=3], and Kanagawa Prefectural Ashigarakami Hospital [n=1]. Since in an actual clinical setting, u-HCC patients with reduced hepatic reserve are often considered for treatment, the analysis focused on CP class and CP score.
Diagnosis and Evaluation of Therapeutic Response
Clinical diagnoses of HCC were made according to the diagnostic criteria of the European Association for the Study of the Liver (EASL) guidelines.2 Treatment response was evaluated by enhanced CT or MRI at 4–8 weeks after introducing lenvatinib, in accordance with the modified Response Evaluation Criteria in Solid Tumors (RECIST) protocol.11,12
We calculated relative dose intensity (RDI) as the total lenvatinib dose delivered for the first 4–8 weeks after introducing therapy as a percentage of the planned dose. Lenvatinib was continued until identification of progressive disease (PD), occurrence of unmanageable adverse events (AEs), or if patients wished to discontinue treatment at their own discretion. Hepatic reserve was assessed using the Child Pugh classification. We analyzed response rate, overall survival (OS) and AEs associated with lenvatinib treatment in CP-A and CP-B patients.
Statistical Analysis
Categorical variables were compared by Fisher’s exact test, and continuous variables were evaluated by the Mann–Whitney U-test. PFS and OS were estimated by the Kaplan–Meier method, and differences were evaluated using the Log rank test. In multivariable analysis of lenvatinib response and OS, factors that were related to the prognosis of HCC according to previous literature8,9,13-18 were selected, which included CP class, Barcelona clinic liver cancer (BCLC) stage, age, Eastern Cooperative Oncology Group (ECOG) performance status (PS), RDI, sex, experience of TACE, experience of other tyrosine kinase inhibitor (TKI) treatments, cause of hepatitis, α-fetoprotein (AFP) level, des-gamma-carboxy prothrombin (DCP) level, body mass index (BMI), extrahepatic metastasis (EHM), major venous invasion (MVI) and liver tumor occupancy rate. Multivariable analysis of response was performed by logistic regression analysis, and the number of explanatory variables was set at 15 for 181 events.19 Multivariable analysis of OS was performed by Cox proportional hazard regression analysis, and the number of explanatory variables was set at 5 for 56 events. All statistical analyses were two-sided, and P values of <0.05 were considered statistically significant. For P values less than 0.001, we reported the value as P<0.001. All statistical analyses were performed with EZR version 1.40 software (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
Patients’ background characteristics at baseline, before lenvatinib treatment, are shown in Table 1. Median patient age was 72 years (range, 34–90), and 140 of the 181 patients (77.3%) were male. ECOG PS was 0 in 145 patients (80.1%). In this study, there were 75, 51, 36, 15 and 4 patients with CP scores of A5, A6, B7 and B8, respectively. In the BCLC stage classification, there were 82 stage B patients and 99 stage C patients; further, there were 55 patients (30.4%) with MVI, 65 patients (35.9%) with EHM and 18 patients (9.9%) with liver tumor occupancy of over 50%. Before the start of the study, 33 patients (18.2%) had a history of TKI treatments. The median serum AFP level was 69.3 ng/mL and median DCP level was 772 mAU/mL. The median observation period was 194 days. CP-A patients were older than CP-B patients, median AFP was higher in CP-B patients than CP-A patients, and median observation period was longer in CP-A patients than in CP-B patients. Other characteristics were not significantly different between CP-A and CP-B patients.
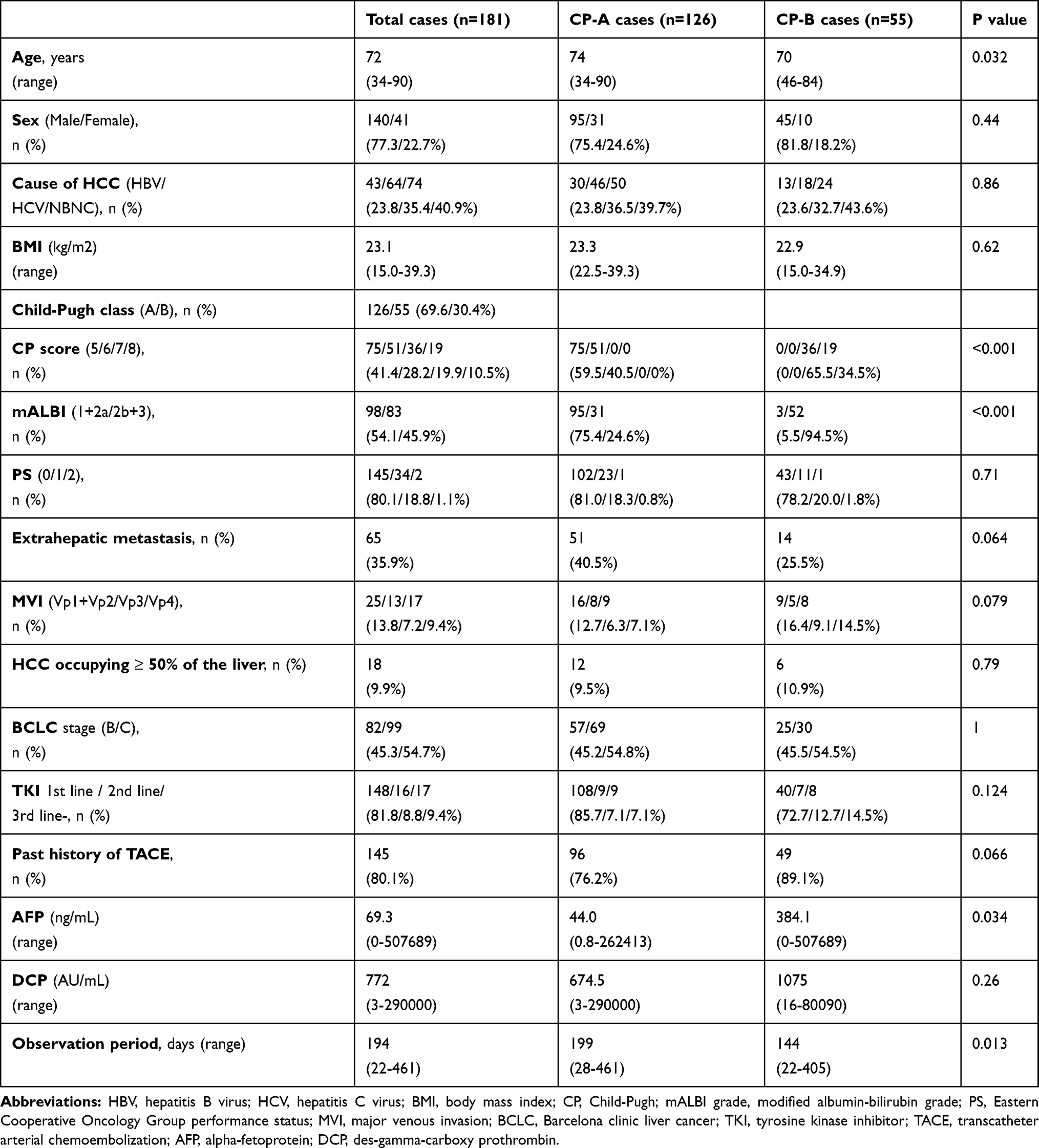 |
Table 1 Baseline Characteristics of Patients |
Adverse Events
A safety analysis was conducted of the 181 patients who received lenvatinib (Table 2). The overall incidence of drug-related AEs was 97.2% (176 of 181 patients). The most frequent drug-related AEs were decreased appetite (56.9%), fatigue (51.4%), hypertension (40.9%), proteinuria (36.5%) and hand-foot-syndrome (HFS) (35.4%). Although proteinuria was more common in CP-A than CP-B patients (P=0.007), the frequency of other AEs, including decreased appetite (P=0.034), diarrhea (P=0.040), vomiting (P=0.009) and increased serum bilirubin levels (P=0.016), were significantly higher in CP-B patients than in CP-A patients. However, the incidence of all grade 3/4 adverse events, except proteinuria, were not significantly different between CP-A and CP-B patients (Table 2A). Further, the total incidence of major AEs leading to treatment interruption and/or withdrawal was not significantly different between CP-A and CP-B patients (Table 2B).
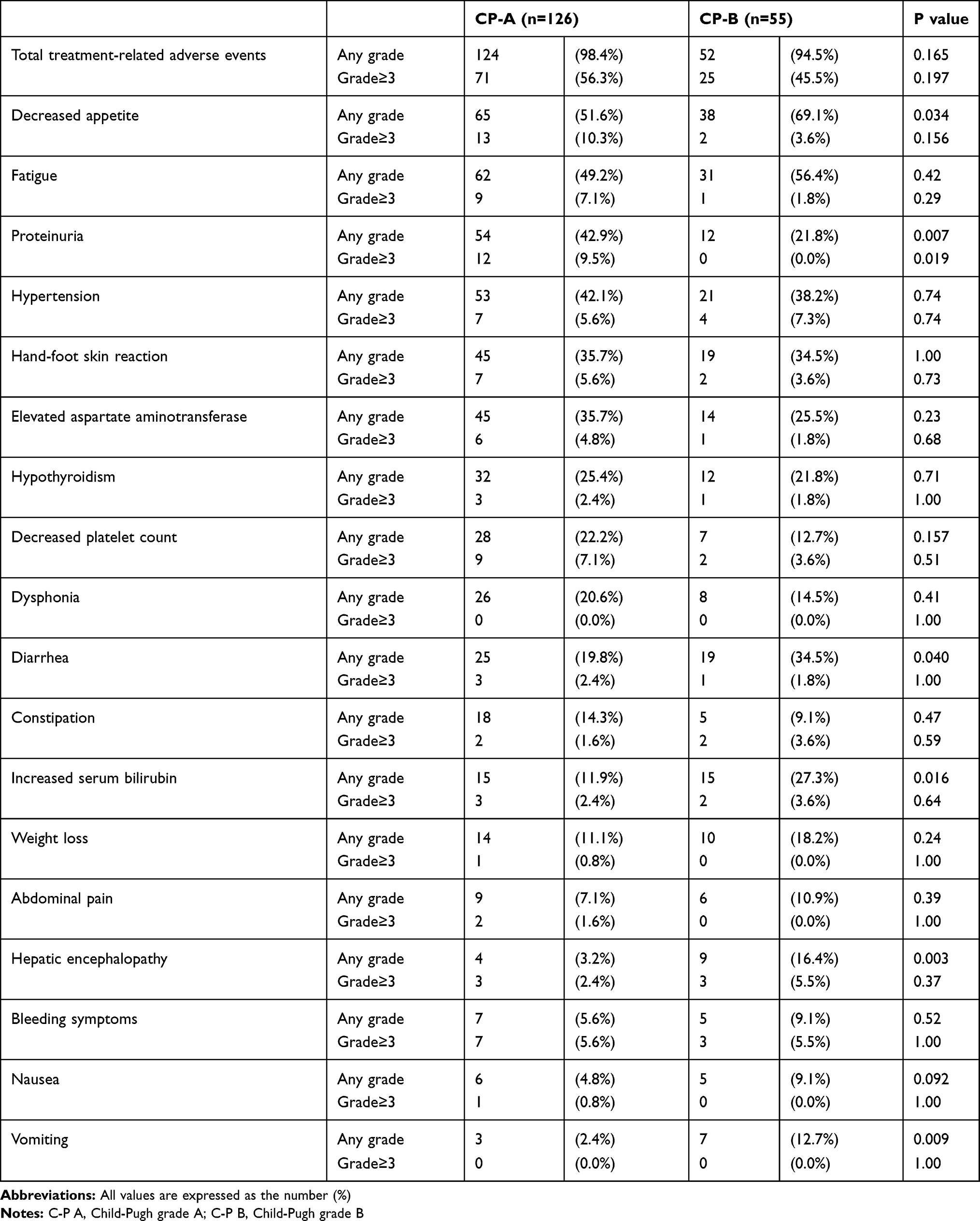 |
Table 2A Comparison of Adverse Events According to CP Class |
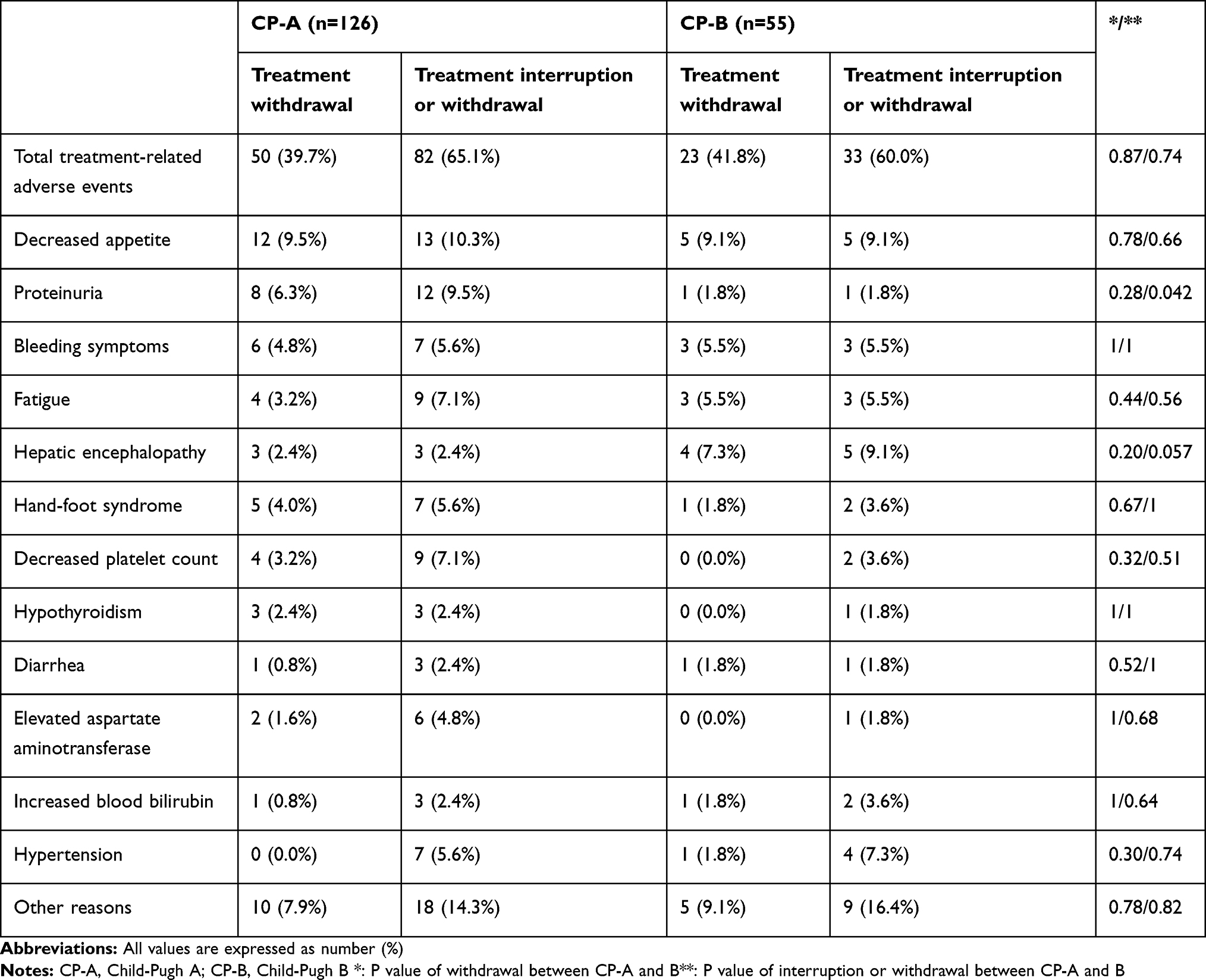 |
Table 2B Comparison of Adverse Events According to CP Class |
Treatment Response
Treatment response at 4–8 weeks after treatment initiation was evaluated in the 181 patients who received lenvatinib treatment. Of the 181 patients, 3 (1.7%), 52 (28.7%), 66 (36.5%), 44 (24.3%) and 16 (8.8%) showed complete response (CR), partial response (PR), stable disease (SD), progressive disease (PD) and not estimated (NE), respectively (Figure 2A). The ORR (ie the total rate of patients with CR and PR) was 30.4%, and the disease control rate (DCR, ie the total rate of patients with CR, PR and SD) was 68.5%, respectively. The ORR in CP-A patients was 36.5%, which was almost consistent with the results of the REFLECT trial and was significantly higher than the ORR of 16.3% in CP-B patients (P=0.008). Furthermore, according to CP class, the ORR (44.0%) was significantly higher in CP-A5 patients as compared to CP-A6 patients (25.5%), CP-B7 patients (22.2%) and CP-B8 patients (5.3%), respectively (P=0.002) (Figure 2B). Although the ORR was higher in CP-B7 patients as compared with CP-B8 patients, the difference was not statistically significant (P=0.105). Likewise, the ORR (38.8%) was significantly higher in the mALBI (1+2a) group as compared with ORR in the mALBI (2b+3) group (20.5%, P=0.009, Figure 2C). Regarding the association between HCC stage and treatment response, ORR in BCLC-B patients (32.9%) and BCLC-C (28.7%) patients were not significantly different (P=0.52) (Figure 2D).
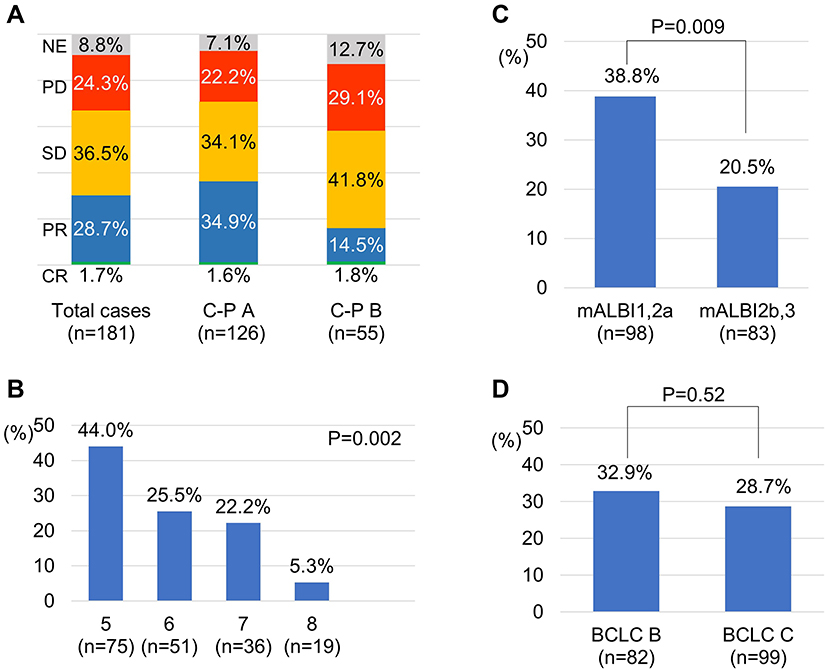 |
Figure 2 Radiological response as assessed by modified Response Evaluation Criteria in Solid Tumors (mRECIST) according to Child-Pugh (CP) class (A), CP score (B), modified albumin-bilirubin (mALBI)-grade (C) and Barcelona clinic liver cancer (BCLC) stage (D). Abbreviations: CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; NE, not estimated. |
Factors Associated with Treatment Response
To verify the ability of RDI to predict objective response (OR), receiver operating characteristic (ROC) curve analysis of RDI was performed. Excluding 16 patients who were not assessed by radiological evaluation and one patient in whom we did not calculate RDI, we examined the association between RDI and OR in 164 patients. ROC curve analysis revealed an area under the ROC (AUROC) of 0.68 and the optimal cut-off of 0.70 for RDI, with 88.9% sensitivity and 66.7% specificity in discriminating the OR group from the non-OR group (Figure 3A). ORR in patients with an RDI of more than 0.70 was significantly higher than those in patients with an RDI of less than 0.70 (47.7% vs 23.8%, P=0.002, Figure 3B). RDI in CP-A patients (0.69) was significantly higher than that in CP-B patients (0.50, P<0.001) (Figure 3C). RDI in patients with CP scores of 5, 6, 7 and 8 were 0.75, 0.67, 0.50 and 0.44, respectively (P<0.001) (Supplementary Figure 1). Additionally, RDI declined gradually in both CP-A and CP-B patients from the start of treatment to 2 months later, as shown in Figure 3D.
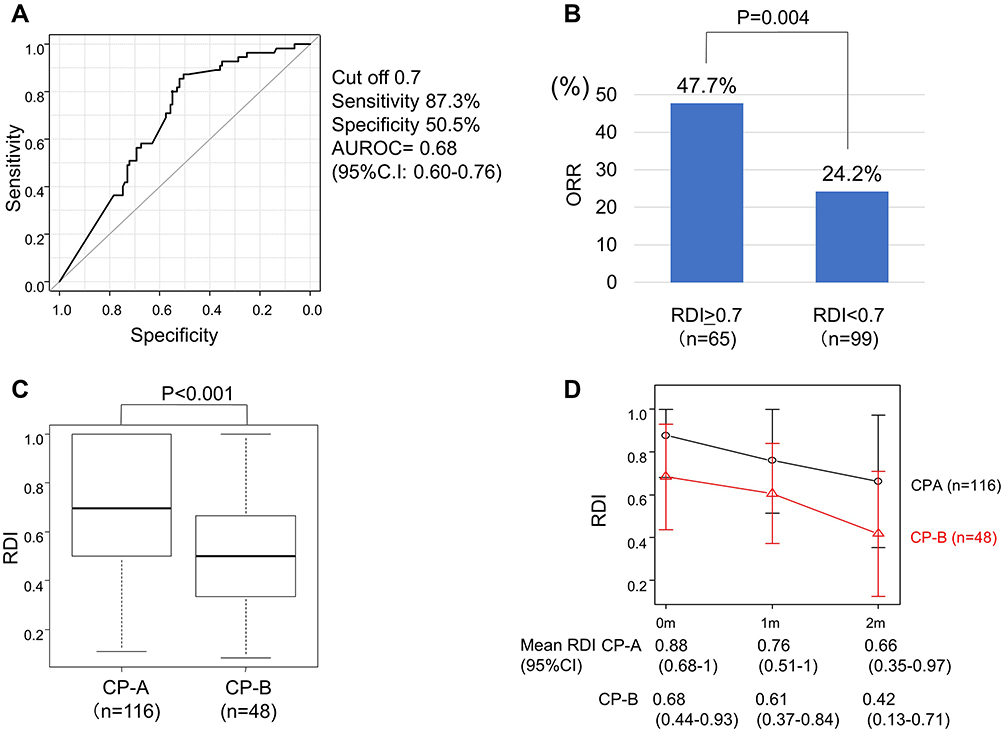 |
Figure 3 Association between optimal relative dose intensity (RDI) and objective response (OR) following lenvatinib treatment. Receiver operating characteristic (ROC) curve analyses of the RDI up to 8 weeks (A). Difference in OR according to RDI up to 8 weeks (B). Difference in RDI up to 8 weeks according to Child-Pugh (CP) class (C). The box plots show the median and quartiles, and the whisker caps of the box plots show the mean 10th and 90th percentile values. RDI in CP-A and CP-B patients every month from the start of treatment to 2 months later (D). AUROC, area under the ROC revealed by ROC curve analysis. |
Furthermore, to evaluate the factors affecting lenvatinib response, the variables of interest (Table 3) were included in multivariable analyses. We excluded mALBI to avoid confounding with CP class. In multivariable analysis, CP-A (odds ratio, 2.72; 95% confidence interval (CI), 1.02–7.24; P=0.045), performance status (PS) (odds ratio, 4.00; 95% CI, 1.18–13.5; P=0.026) and RDI (odds ratio, 2.40; 95% CI, 1.07–5.39; P=0.034) were independent factors associated with lenvatinib response. Moreover, in CP-A patients, DCP (odds ratio, 2.72; 95% CI, 1.02–7.13; P=0.045) was an independent factor associated with lenvatinib response, while there were no factors associated with lenvatinib response in CP-B patients (Supplementary Table 1A and B).
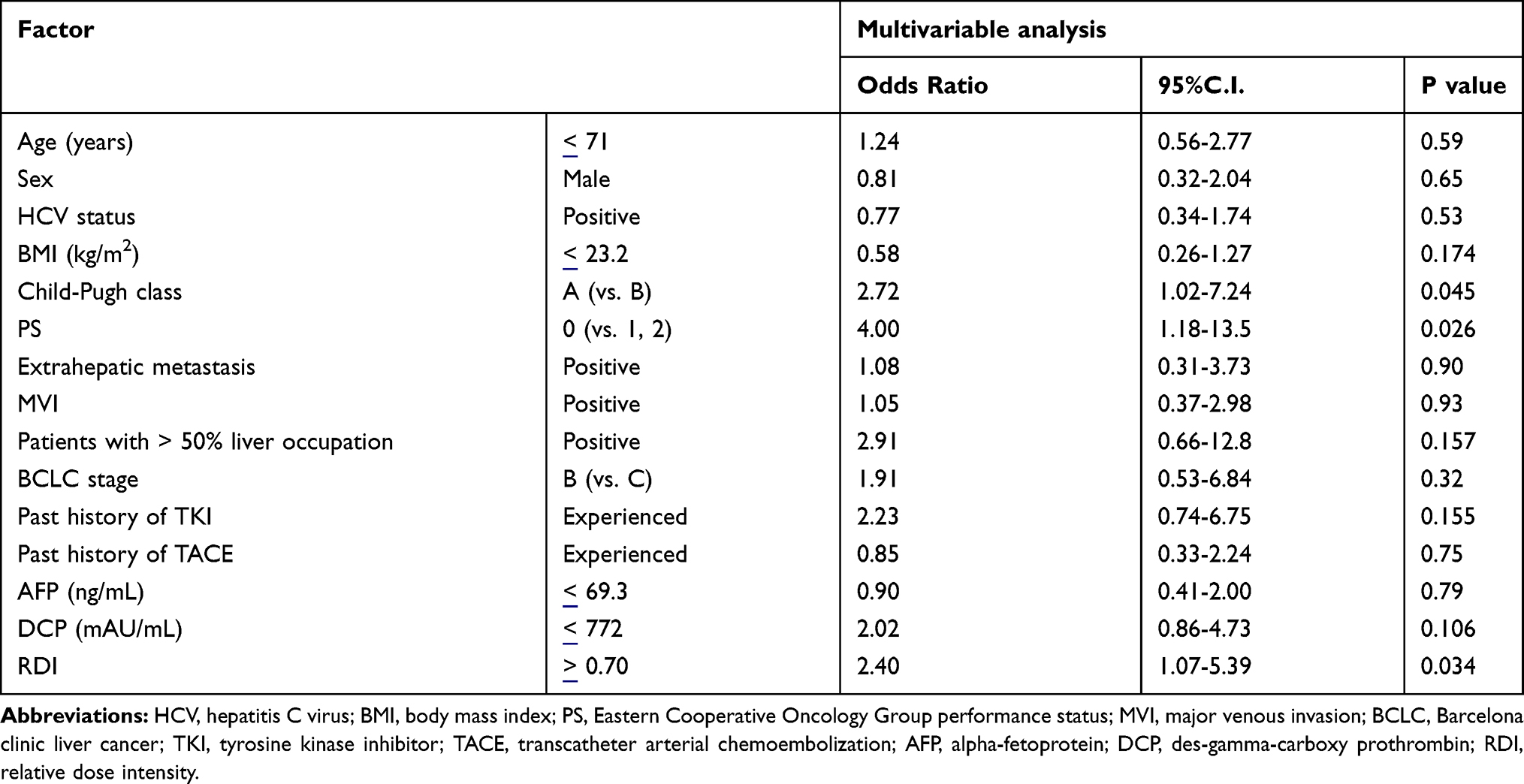 |
Table 3 Factors Associated with Object Response |
Analysis of Factors Affecting Overall Survival Among Patients Receiving Lenvatinib Treatment
We performed Kaplan-Meier estimates of OS according to CP class, CP score, mALBI score, RDI and BCLC stage. The median OS was 369 days (95% CI, range: 308 days – NA). The OS of patients with scores of CP-A (1-year OS 68.3%) was longer as compared to those with scores of CP-B (1-year OS 30.3%, P=0.002) (Figure 4A). Likewise, the OS of patients with mALBI (1+2a) was longer as compared to those with mALBI (2b+3) (P=0.003) (Figure 4B). OS was found to correlate with CP score (P=0.002) (Figure 4C); moreover, OS of patients with scores of CP-A and those with a score of CP B7 (1-year OS 59.2%) was longer as compared to those with CP scores of B8 (1-year OS 34.8%, P=0.003) (Figure 4D). The OS of patients with high RDI (≥0.7) was higher as compared to that of patients with low RDI (<0.7), but the difference was statistically insignificant (P=0.051, data not shown). The OS of patients with BCLC-C was worse than that of patients with BCLC-B (P=0.001, Figure 4E). In particular, in BCLC-C patients, OS of CP-B patients (1-year OS 17.3%) was worse than that of CP-A patients (1-year OS 55.4%, P=0.003, Figure 4F). In order to determine the association between AEs and OS, we performed Kaplan-Meier estimates of OS in terms of the most frequent AEs, ie, decreased appetite, fatigue, hypertension and HFS, although the results revealed no significant association between OS and these AEs (Supplementary Figure 2A–D). (To resolve bias between the group with and without the occurrence of AEs, we selected patients who were administered lenvatinib for more than 2 months. There were 151 such cases in this study.)
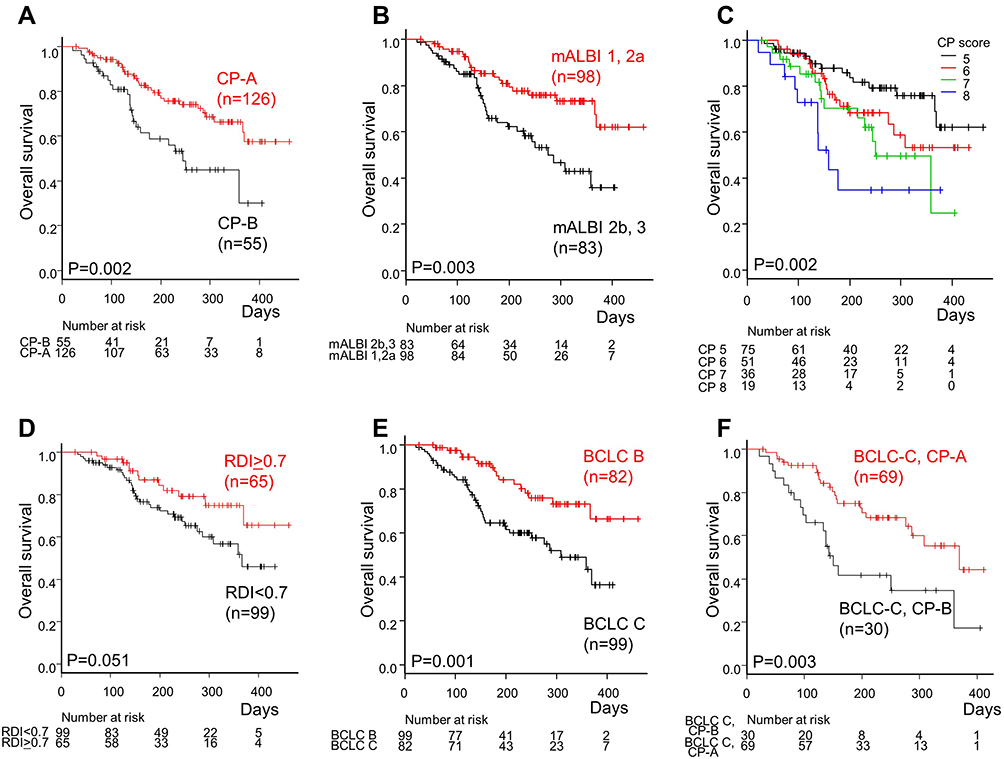 |
Figure 4 Association between overall survival (OS) and several clinical factors. Kaplan-Meier analysis of 181 hepatocellular carcinoma (HCC) patients who received lenvatinib treatment, stratified by Child-Pugh (CP) class (A), modified albumin-bilirubin (mALBI)-grade (B), CP score (C), CP score of 5–7 vs 8–9 (D) and Barcelona Clinic Liver Cancer (BCLC) stage (E). Kaplan–Meier analysis of 99 BCLC-C HCC patients who received lenvatinib treatment stratified by C-P class (F). |
In multivariable analysis, CP class (hazard ratio (HR), 0.41; 95% CI, 0.21–0.78; P=0.007) and BCLC stage (HR, 0.35; 95% CI, 0.18–0.69; P=0.002) were significant predictive factors of OS in HCC patients receiving lenvatinib treatment (Table 4).
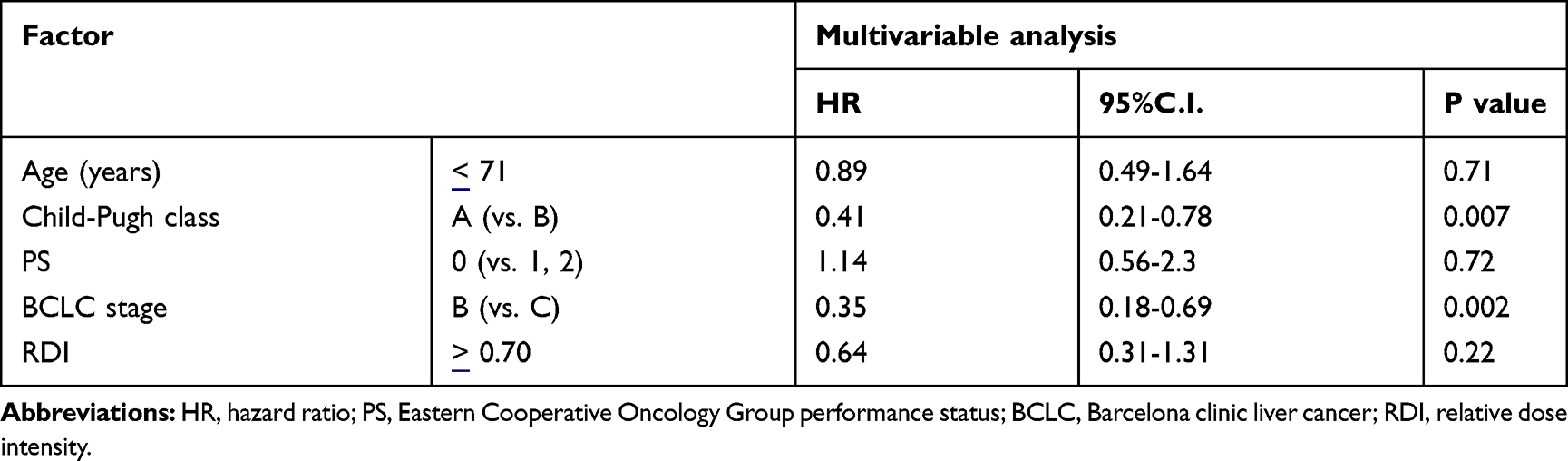 |
Table 4 Factors Associated with Overall Survival Time |
Moreover, BCLC stage was independently related to OS in both CP-A and CP-B patients (Supplementary Table 2A and B)
Discussion
In this retrospective study, we compared the clinical benefits and incidence of AEs with lenvatinib therapy among patients with HCC of different CP class. The efficacy of lenvatinib has not been adequately proven in patients with advanced HCC and a score of CP-B in clinical trials. Hence, the utility of lenvatinib in patients with advanced HCC and CP-B cirrhosis is an unresolved issue. As far as we know, to date, this is the largest study evaluating OS and AEs of lenvatinib in CP-B patients with HCC.
Our results showed that OR in CP-A patients was higher than that in patients with CP-B disease. These results were probably related to the higher RDI and lower frequency of AEs in CP-A patients. On the other hand, multivariable analysis revealed that CP class was related to OR regardless of RDI and AEs. In terms of the incidence of lenvatinib-related AEs, decreased appetite, diarrhea, vomiting and increased serum bilirubin level were significantly higher in CP-B patients than in CP-A patients. RDI was found to be significantly related to OR. Recently, the dose-related therapeutic effects of lenvatinib have been reported.9,20 We showed that ORR in patients with an RDI at 8 weeks of more than 0.70 was remarkably higher than ORR in patients with an RDI of less than 0.70, which is similar to the results of other recent reports.9,20 Although we did not explore the correlation between RDI after 8 weeks and OR in this study, Sasaki et al reported that RDI at 8 weeks is most useful for predicting OR achievement as compared to other time points between the start of therapy and 16 weeks later.9 Based on our results and previous reports, a high anti-tumor effect can be expected if the 8-week RDI is sufficient.
In particular, RDI in CP-A patients was higher than in CP-B patients. From the first administration of lenvatinib, the dose of lenvatinib was reduced from 12 mg to 8 mg in patients with CP-B whose body weight was over 60 kg. Furthermore, because the frequency of the above-mentioned AEs were significantly higher in CP-B than in CP-A patients, it was difficult to maintain a high RDI in patients with CP-B. Although the number of grade 3/4 AEs leading to treatment interruption and/or withdrawal was not significantly different between CP-A and CP-B patients, lenvatinib dose reduction was required more frequently in CP-B than CP-A patients due to some intolerable Grade 2 AEs. Therefore, RDI was significantly higher in CP-A patients than in CP-B patients not only at the start of lenvatinib therapy but also over the entire duration of treatment. Therefore, the ORR in CP-A patients was higher than that in CP-B patients. On the other hand, CP class was related to OR regardless of RDI and AEs by multivariable analysis. Lenvatinib undergoes hepatic metabolism (predominantly by CYP3A), which could potentially be influenced by the presence of underlying liver disease.21 Although the reason why CP class correlates with OR regardless of RDI or AEs remains unclear, the difference in hepatic metabolism of lenvatinib between CP-A and CP-B might influence OR. Further investigations of the influence of hepatic impairment on lenvatinib pharmacokinetics are needed.
Moreover, our results showed that ORR in cases with a CP score of B7 was over 20%, and that patients with a CP score of B7 seemingly derive slightly higher clinical and survival benefits from lenvatinib treatment than patients with scores of B8. A CP score of B7 might represent a mild decrease in serum albumin and mild hyperbilirubinemia compared to a CP score of B8. Thus, u-HCC patients with CP-B cirrhosis constitute a heterogeneous population.22 Our results indicated that it is important to consider CP score before lenvatinib treatment when determining the treatment strategy, and that treatment in CP-B patients should be performed discretely and that other treatments should be considered in patients with CP scores of B8 because of insufficient OR and OS in CP-B8 patients.
The post-lenvatinib treatments administered in this study, which could have affected outcomes, are shown in Supplementary Table 3. Sixty percent of CP-B patients received best supportive care post-lenvatinib treatment. However, because of the short duration of observation and the small number of cases that received post-lenvatinib treatments, further evaluation is needed to clearly determine the association between post-lenvatinib treatment and overall survival in CP-A patients.
In this study, we also showed that BCLC stage was associated with OS in multivariable analysis. Although ORR was not significantly different between BCLC stage B and C, the reason why OS of BCLC-C cases was much worse than that of BCLC-B might be the aggressive behavior of BCLC-C grade tumors. Based on these results, treatment of BCLC-C patients should be performed discretely and with caution even if OR is obtained at first radiological evaluation. Moreover, since the prognosis is severe in BCLC-C with CP-B patients, other treatments are desired in BCLC-C with CP-B patients.
This study has some limitations. First is the retrospective nature of this study. Additionally, this study was based on multicenter data, and the mRECIST criteria are sometimes difficult to evaluate with consistent accuracy. Second, the number of patients included in the CP-B7 and CP-B8 subgroups was relatively small, and, thus, the study might not have had enough statistical power to provide precise estimates. Based on these limitations, our findings should be regarded as exploratory.
Conclusion
Lenvatinib treatment offers significant benefit in patients with good liver function in real-world practice. The various characteristics identified in this study might be helpful as clinical predictors of response to lenvatinib and survival in field practice. Further studies are required to address eligibility for lenvatinib treatment in CP-B7 patients. Moreover, prospective studies are required to address these limitations, by recruiting more patients in a multicenter setting using the same protocols.
Abbreviations
HCC, hepatocellular carcinoma; RECIST, response evaluation criteria in solid tumors; mRECIST, modified response evaluation criteria in solid tumors; VEGFR, vascular endothelial growth factor receptor; FGF, fibroblast growth factor; FGFR, fibroblast growth factor receptor; OS, overall survival; PFS, progression-free survival; OR, objective response; ORR, objective response rate; RDI, relative dose intensity; AFP, α-fetoprotein; AFP-L3, lens culinaris agglutinin-reactive fraction of α-fetoprotein; DCP, des-gamma-carboxy prothrombin; TNM, tumor node metastasis classification; BCLC, Barcelona clinic liver cancer, CP; Child-Pugh; mALBI, modified albumin-bilirubin; ROC, receiver operating characteristic; AUROC, area under the ROC curve.
Data Sharing Statement
The authors do not intend to share the individual de-identified participant data and the data and document will be available on the University Hospital Medical Information Network Clinical Trials Registry website (UMIN000037054).
Ethical Considerations
Written informed consent for obtaining serum and using it in future studies was obtained from all patients. The study protocol conformed to the ethical guidelines of the World Medical Association Declaration of Helsinki and was approved by the respective institutional ethics committees (approval numbers: B180400020).
Acknowledgments
The authors would like to thank all the patients and their families, as well as the investigators and staff of the participating institutions.
Disclosure
Makoto Ueno and Tatehiro Kagawa have received research funding from Eisai Co., Ltd. The authors report no other conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Kulik L, El-Serag HB. Epidemiology and management of hepatocellular carcinoma. Gastroenterology. 2019;156(2):477–491. doi:10.1053/j.gastro.2018.08.065
3. Galle PR, Forner A, Llovet JM; European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
4. Boss DS, Glen H, Beijnen JH, et al. A phase I study of E7080, a multitargeted tyrosine kinase inhibitor, in patients with advanced solid tumours. Br J Cancer. 2012;106(10):1598–1604. doi:10.1038/bjc.2012.154
5. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
6. Hiraoka A, Kumada T, Atsukawa M, et al. Prognostic factor of Lenvatinib for unresectable hepatocellular carcinoma in real-world conditions-multicenter analysis. Cancer Med. 2019;8(8):3719–3728. doi:10.1002/cam4.1909
7. Ueshima K, Nishida N, Hagiwara S, et al. Impact of baseline ALBI grade on the outcomes of hepatocellular carcinoma patients treated with lenvatinib: a multicenter study. Cancers (Basel). 2019;11(7):e952. doi:10.3390/cancers11070952
8. Tada T, Kumada T, Hiraoka A, et al. Safety and efficacy of lenvatinib in elderly patients with unresectable hepatocellular carcinoma: a multicenter analysis with propensity score matching. Hepatol Res. 2020;50(1):75–83. doi:10.1111/hepr.13427
9. Sasaki R, Fukushima M, Haraguchi M, et al. Response to lenvatinib is associated with optimal relative dose intensity in hepatocellular carcinoma: experience in clinical settings. Cancers (Basel). 2019;11(11):1769. doi:10.3390/cancers11111769
10. Ikeda M, Okusaka T, Mitsunaga S, et al. Safety and pharmacokinetics of lenvatinib in patients with advanced hepatocellular carcinoma. Clin Cancer Res. 2016;22(6):1385–1394. doi:10.1158/1078-0432.CCR-15-1354
11. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
12. Llovet JM, Lencioni R. mRECIST for HCC: performance and novel refinements. J Hepatol. 2020;72(2):288–306. doi:10.1016/j.jhep.2019.09.026
13. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
14. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
15. Bruix J, Cheng AL, Meinhardt G, et al. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: analysis of two phase III studies. J. Journal of Hepatology. 2017;67(5):999–1008. doi:10.1016/j.jhep.2017.06.026
16. Hyun MH, Lee YS, Kim JH, et al. Hepatic resection compared to chemoembolization in intermediate- to advanced-stage hepatocellular carcinoma: a meta-analysis of high-quality studies. Hepatology. 2018;68(3):977–993. doi:10.1002/hep.29883
17. Youssef AA, Issa HA, Omar MZ, et al. Serum human endothelial cell-specific molecule-1 (endocan) and vascular endothelial growth factor in cirrhotic HCV patients with hepatocellular carcinoma as predictors of mortality. Clin Exp Gastroenterol. 2018;11:431–438. doi:10.2147/CEG.S171339
18. Morimoto M, Numata K, Kondo M, et al. Field practice study of half-dose sorafenib treatment on safety and efficacy for hepatocellular carcinoma: a propensity score analysis. Hepatol Res. 2015;45(3):279–287. doi:10.1111/hepr.12354
19. Harrell FE. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis.
20. Eso Y, Nakano S, Mishima M, et al. Dose intensity/body surface area ratio is a novel marker useful for predicting response to lenvatinib against hepatocellular carcinoma. Cancers (Basel). 2019;12(1):49. doi:10.3390/cancers12010049
21. Ogasawara S, Chiba T, Ooka Y, et al. Sorafenib treatment in Child-Pugh A and B patients with advanced hepatocellular carcinoma: safety, efficacy and prognostic factors. Invest New Drugs. 2015;33(3):729–739. doi:10.1007/s10637-015-0237-3
22. Di Maio M, Daniele B, Perrone F. Targeted therapies: role of sorafenib in HCC patients with compromised liver function. Nat Rev Clin Oncol. 2009;6(9):505–506. doi:10.1038/nrclinonc.2009.114
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.