")
Back to Journals » International Medical Case Reports Journal » Volume 7
Sacral insufficiency fractures: a case of mistaken identity
Received 5 January 2014
Accepted for publication 1 March 2014
Published 30 May 2014 Volume 2014:7 Pages 93—98
DOI https://doi.org/10.2147/IMCRJ.S60133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Mathew J Baldwin, Laura J Tucker
Oxford Deanery, Oxford, UK
Introduction: Sacral insufficiency fractures are an important cause of lower back pain in the elderly. Clinically and radiologically, they must be distinguished from osseous metastases, which frequently coexist. To date, no case report has comprehensively explored the full range of diagnostic hurdles and potential pitfalls.
Case presentation: We report the case of a 70-year-old Caucasian female who presented to our services with a short history of progressive back pain without any history of trauma. A prior history of breast cancer was noted. Bone scintigraphy was initially reported as consistent with metastatic sacral deposits. Further characterization with magnetic resonance imaging and computed tomography revealed bilateral insufficiency fractures of the sacral alar. The patient responded well to conservative management.
Conclusion: To avoid misdiagnosis, particularly in those who are also at risk of osseous metastases, sacral insufficiency fractures must always be considered as a cause of lower back pain.
Keywords: sacral fractures, insufficiency fractures, misdiagnosis, metastatic disease
Introduction
Stress fractures can be classified as either fatigue or insufficiency fractures.1 Intuitively, the first describes fractures occurring within normal bone architecture that has been exposed to abnormal or repetitive stresses.2 Conversely, insufficiency fractures occur in abnormal bone under normal stress. Insufficiency fractures of the sacrum (SIFs) were first described by Lourie in 1982.3 Patients undergoing radiotherapy to treat malignant tumors may be at particular risk of SIFs,4 with a prevalence of 89% for patients undergoing radiotherapy for cervical cancer.5 Elderly women with osteoporosis are also at high risk,6 with almost all patients with SIFs demonstrating severe osteopenia on dual X-ray absorptiometry.7 Additionally, rheumatoid arthritis, Paget’s disease, renal osteodystrophy, and hyperparathyroidism have been reported as risk factors.8,9 Sacral stress fractures have occasionally been reported during the last trimester of pregnancy and the early postpartum period.10,11 While preceding trauma may be reported, it is usually minor12 or often completely absent.13
Patients suffering from SIFs often present with limited mobility caused by acute and intractable lumbar or pelvic pain without clear evidence of trauma. Neurological symptoms are usually absent, but radiculopathy has a reported incidence of 5%–6%7 and sphincter disturbance has also been described.14 Pain typically improves on lying supine and increases on weight-bearing. Patients may also complain of parasymphyseal discomfort due to the high incidence of concomitant pubic rami fractures.15
The lack of specific clinical findings makes diagnosis challenging and SIFs remain an under-recognized cause of lower back pain. In fact, there is often a delay of up to 2 months before dedicated sacral imaging is performed.16 In this report, we describe the diagnostic challenge of detecting SIFs and aim to increase awareness of the potential pitfalls.
Case presentation
A 70-year-old Caucasian patient was admitted through the emergency department with severe back pain. She had first experienced discomfort 14 days previously, which had progressively worsened. No history of trauma, however minor, could be recalled. The pain was localized to her lower back with no radicular symptoms. One week after the initial discomfort, the patient was unable to mobilize and had become bedridden. No neurology was demonstrable on examination. Palpation of the lumbar vertebrae was unremarkable but direct pressure over both sacroiliac joints resulted in a marked exacerbation of her pain.
A history of primary breast cancer was reported. The disease was detected during mammographic screening with no radiographic or histological evidence of distant metastasis. As such, the patient had undergone a wide local excision and local radiotherapy 4 years prior. Additionally, she described a longstanding history of rheumatoid arthritis which was controlled with disease-modifying antirheumatic drugs.
Upon admission, our patient was apyrexial and had a normal white blood cell count. Interestingly, raised alkaline phosphatase (ALP) was found at 278 IU/L (reference range: 30–130 IU/L) with normal adjusted calcium. The remaining liver function tests were normal. Marginally raised C-reactive protein was seen at 15 mg/L (reference range: <10 mg/L).
Plain film radiographs of her lumbar spine demonstrated scoliosis but no fractures or suspicious lesions. Similarly, radiographs of her pelvis did not detect any abnormalities. In view of her medical history, bone scintigraphy was performed. This demonstrated a bilateral increase in uptake of technetium-99m in the sacrum and pubic rami (Figure 1). Initially, this was thought to be consistent with metastatic disease. Subsequently, spinal magnetic resonance imaging (MRI) was performed to characterize the extent of the lesions. T1-weighted images of the sacrum demonstrated symmetrical hypointense areas within both sacral alar (Figure 2). Whilst symmetry was not in keeping with a neoplastic process, no fracture line was evident. A computed tomography (CT) scan of the sacral region highlighted bilateral fracture lines through the sacral alar in keeping with insufficiency fractures (Figure 3). CT also demonstrated a right-sided anterior pubic rami fracture.
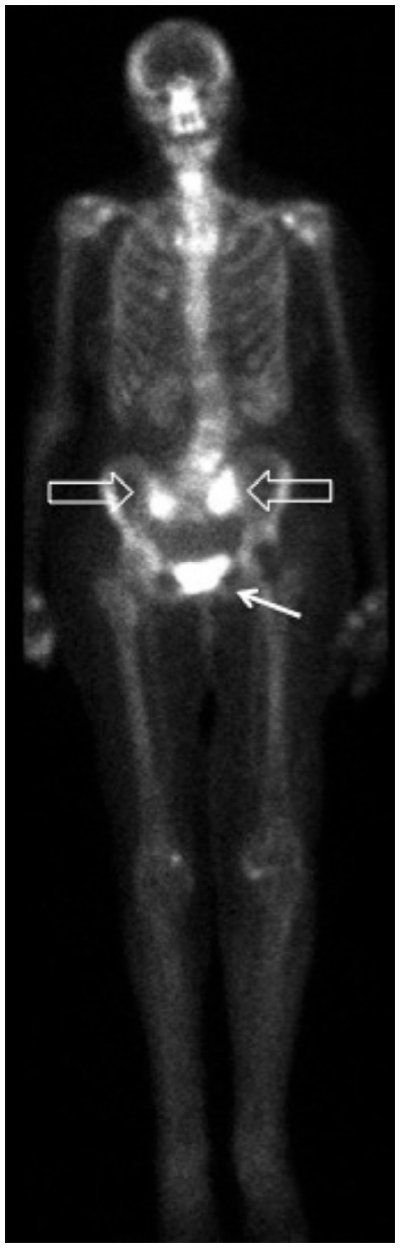 | Figure 1 Bone scintigraphy showing increased sacral uptake bilaterally (hollow arrows) and pubic bone (solid arrow). |
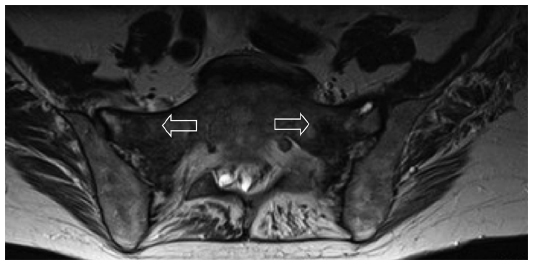 | Figure 2 Axial T1-weighted MRI image of sacrum. |
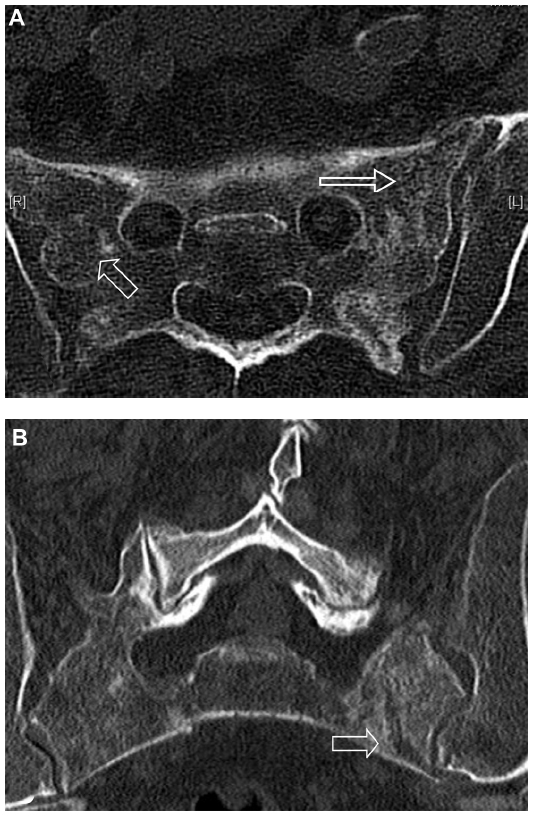 | Figure 3 CT images of sacrum. |
Her pain was successfully managed with a combination of simple and transcutaneous opioid analgesia. The patient was able to mobilize with the aid of a walking frame and was discharged home on day 12 of admission. Subsequent follow-up at 1 month found her pain, mobility, and independence to be gradually improving.
Discussion
Several reports have previously highlighted the variable and nonspecific presentation of SIFs that makes diagnosis challenging.6,9 Whilst not specific for SIFs, Denis et al have classified traumatic sacral fractures into zones,17 which can help predict the clinical features. Zone 1 fractures lie laterally, involving the sacral alar, with zones 2 and 3 fractures progressing medially to involve the neural foramina and sacral bodies, respectively. Consequently, unilateral radicular symptoms are often reported with zone 2 fractures and bilateral neurological symptoms with sphincter dysfunction can occur with involvement of zone 3.
Laboratory investigations are of limited value. Often, no abnormality is found, although a mildly raised ALP, a marker of bone formation, is sometimes seen.18 Of note, ALP is also raised in metastatic disease.19 Radiographs of the pelvis, sacrum, and lumbar spine may initially be used to identify fractures. However, the presence of fecal material, vascular calcifications, and bowel gas can mask incomplete fractures, and radiographs detect SIFs in less than 40% of cases.20
Diagnostic difficulty is compounded by a history of malignancy in approximately 45% of patients with SIFs.21 Consideration of this clinical entity is therefore paramount if overdiagnosis of osseous metastasis is to be avoided. Bone scintigraphy with technetium-99m-labeled medronic acid is one of the most sensitive (96%) examinations.22 While present in less than 40% of patients, the H-sign is considered pathognomonic for SIFs.23 However, isolated sacral metastases presenting with focal sacral uptake have also been reported.24
MRI, with sensitivity approaching 100%, is considered to be the gold standard for identifying SIFs.24 Most cases demonstrate both marrow edema and a fracture line, although the latter is absent in 7% of cases.24 The absence of a fracture line can create uncertainty. Although less sensitive (60%–75%),24 CT can be used in combination with MRI. Previous reports have noted that the absence of cortical destruction and/or a soft tissue mass effectively rules out bone metastases (Table 1).25,26
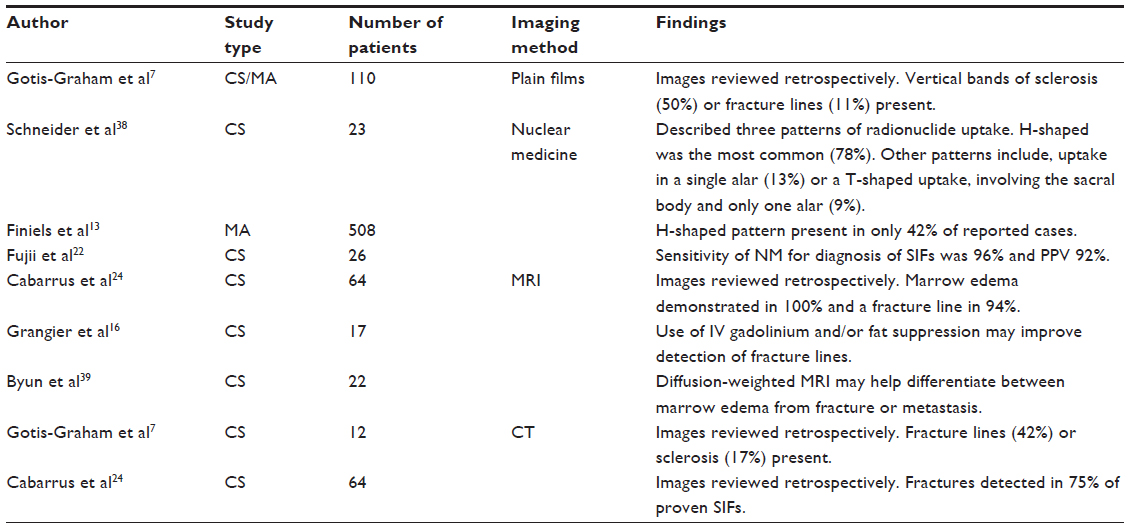 | Table 1 Summary of articles published on the imaging modalities utilized for the investigation of SIFs |
Traditionally, treatment of SIFs has been limited to conservative management strategies comprising bed rest, pain control, and physical therapy, with symptoms usually improving within 12 months.27,28 However, prolonged bed rest, particularly in elderly patients, has a significant morbidity. In particular, high incidences of deep vein thrombosis and pulmonary embolism have been reported.29 Early physical therapy has been advocated as a means of reducing this morbidity and encouraging fracture healing through the promotion of osteoblast-mediated bone formation.30 However, good quality prospective trials supporting early physical therapy in SIFs are currently lacking.
Sacroplasty has also emerged as a potential treatment and involves fluoroscopic or CT-guided injection of cement into the fractured sacrum. Initially used as a treatment for sacral metastases, it was first described as a treatment for SIFs in 2002 by Garant.31 As yet, no randomized trials are available, and the literature is restricted to small retrospective case series with variable, and often invalidated, outcome measures. Whilst these need to be interpreted cautiously, they suggest a rapid and sustained improvement in pain, reduced use of narcotic analgesia, and improvement in mobility scores.32,33 In addition, an improved ability to perform activities of daily living has also been reported.34 The main risk of sacroplasty is leakage of cement outside of the fracture line, with risk of neurological compromise. Leakage of cement has been reported but in only one case did this result in transient radiculopathy,32 and in none were long-term sequelae described.33 As a means of reducing complications, augmentation with a balloon-assisted technique, sacral kyphoplasty, has been proposed.35 The creation of a compacted bony layer outside the balloon could, in theory, reduce cement extravasation. Supporting this technique, a cadaveric study demonstrated that cement deposition was better localized within the cortical boundaries.36
Clearly, stronger evidence is required before the widespread use of sacroplasty over conservative management can be supported. It has also been suggested that since sacroplasty disrupts normal osseous healing, it may only be indicated in patients with delayed union or pain not responding to conservative measures.37 However, the best method of conservative management remains equally uncertain. This is an area of much needed research (Table 2).
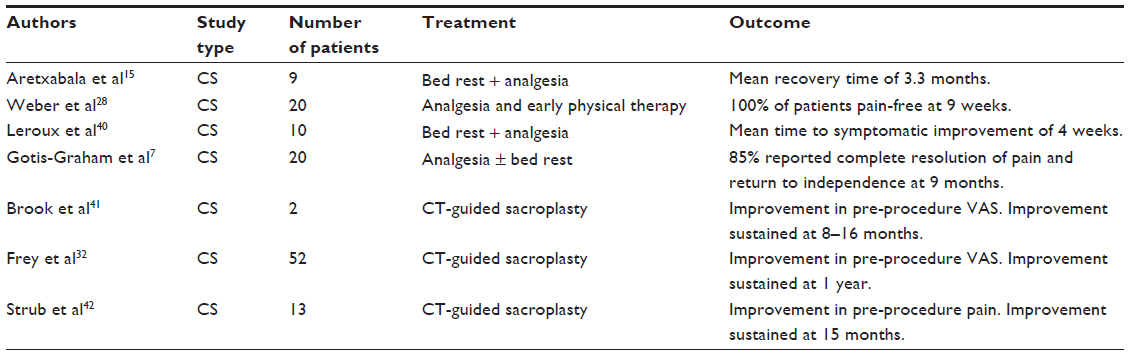 | Table 2 A selection of previously reported case series on the various treatments of SIFs |
Conclusion
The diagnostic difficulty of SIFs has previously been recognized. To our knowledge, this is the first report to highlight the full range of diagnostic hurdles; in particular, we draw attention to the limitations of each imaging modality. Awareness of SIFs is important if an erroneous misinterpretation for metastatic disease is to be avoided.
Consent
Written informed consent was obtained from the patient for publication of this manuscript and any accompanying images. A copy of the written consent is available for review from the Editor-in-Chief of this journal.
Acknowledgment
With thanks to Sarah Brice for her support and academic input.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathologic fractures. JAMA. 1964;187:1001–1004. | |
Pommering TL, Kluchurosky L. Overuse injuries in adolescents. Adolesc Med State Art Rev. 2007;18(1):95–120, ix. | |
Lourie H. Spontaneous osteoporotic fracture of the sacrum. An unrecognized syndrome of the elderly. JAMA. 1982;248(6):715–717. | |
Mammone JF, Schweitzer ME. MRI of occult sacral insufficiency fractures following radiotherapy. Skeletal Radiol. 1995;24(2):101–104. | |
Blomlie V, Rofstad E, Talle K, Sundfør K, Winderen M, Lien HH. Incidence of radiation-induced insufficiency fractures of the female pelvis: evaluation with MR imaging. AJR Am J Roentgenol. 1996; 167(5):1205–1210. | |
Wild A, Jaeger M, Haak H, Mehdian SH. Sacral insufficiency fracture, an unsuspected cause of low back pain in elderly women. Arch Orthop Trauma Surg. 2002;122(1):58–60. | |
Gotis-Graham I, McGuigan L, Diamond T, et al. Sacral insufficiency fractures in the elderly. J Bone Joint Surg Br. 1994;76(6):882–886. | |
De Smet AA, Neff JR. Pubic and sacral insufficiency fractures: clinical course and radiologic findings. AJR Am J Roentgenol. 1985;145(3):601–606. | |
Dasgupta B, Shah N, Brown H, Gordon TE, Tanqueray AB, Mellor JA. Sacral insufficiency fractures: an unsuspected cause of low back pain. Br J Rheumatol. 1998;37(7):789–793. | |
Rousière M, Kahan A, Job-Deslandre C. Postpartal sacral fracture without osteoporosis. Joint Bone Spine. 2001;68(1):71–73. | |
Schmid L, Pfirrmann C, Hess T, Schlumpf U. Bilateral fracture of the sacrum associated with pregnancy: a case report. Osteoporos Int. 1999;10(1):91–93. | |
Newhouse KE, el-Khoury GY, Buckwalter JA. Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am. 1992;74(10):1472–1477. | |
Finiels H, Finiels PJ, Jacquot JM, Strubel D. Fractures du sacrum par insuffisance osseuse: meta-analyse de 508 cas [Fractures of the sacrum caused by bone insufficiency: meta-analysis of 508 cases]. La Presse Medicale. 1997;26(33):1568–1573. French. | |
Muthukumar T, Butt SH, Cassar-Pullicino VN, McCall IW. Cauda equina syndrome presentation of sacral insufficiency fractures. Skeletal Radiol. 2007;36(4):309–313. | |
Aretxabala I, Fraiz E, Pérez-Ruiz F, Ríos G, Calabozo M, Alonso-Ruiz A. Sacral insufficiency fractures. High association with pubic rami fractures. Clin Rheumatol. 2000;19(5):399–401. | |
Grangier C, Garcia J, Howarth NR, May M, Rossier P. Role of MRI in the diagnosis of insufficiency fractures of the sacrum and acetabular roof. Skeletal Radiol. 1997;26(9):517–524. | |
Denis F, Davis S, Comfort T. Sacral fractures: an important problem. Retrospective analysis of 236 cases. Clin Orthop Relat Res. 1988;227:67–81. | |
Schindler OS, Watura R, Cobby M. Sacral insufficiency fracture: an under-recognized condition. Curr Orthopaed. 2003;17(3):234–239. | |
Mayne PD, Thakrar S, Rosalki SB, Foo AY, Parbhoo S. Identification of bone and liver metastasis from breast cancer by measurement of plasma alkaline phosphatase isoenzyme activity. J Clin Pathol. 1987;40(4):398–403. | |
Peh WC, Khong PL, Sham JS, Ho WY, Yeung HW. Sacral and pubic insufficiency fractures after irradiation of gynaecological malignancies. Clin Oncol (R Coll Radiol). 1995;7(2):117–122. | |
Lundin B, Björkholm E, Lundell M, Jacobsson H. Insufficiency fractures of the sacrum after radiotherapy for gynaecological malignancy. Acta Oncol. 1990;29(2):211–215. | |
Fujii M, Abe K, Hayashi K, et al. Honda sign and variants in patients suspected of having a sacral insufficiency fracture. Clin Nucl Med. 2005;30(3):165–169. | |
Ries T. Detection of osteoporotic sacral fractures with radionuclides. Radiology. 1983;146(3):783–785. | |
Cabarrus MC, Ambekar A, Lu Y, Link TM. MRI and CT of insufficiency fractures of the pelvis and the proximal femur. AJR Am J Roentgenol. 2008;191(4):995–1001. | |
Gacetta DJ, Yandow DR. Computed tomography of spontaneous osteoporotic sacral fractures. J Comput Assist Tomogr. 1984;8(6):1190–1191. | |
Tsuchida T, Kosaka N, Sugimoto K, Itoh H. Sacral insufficiency fracture detected by FDG-PET/CT: report of 2 cases. Ann Nucl Med. 2006;20(6):445–448. | |
Rawlings CE 3rd, Wilkins RH, Martinez S, Wilkinson RH Jr. Osteoporotic sacral fractures: a clinical study. Neurosurgery. 1988; 22(1 Pt 1):72–76. | |
Weber M, Hasler P, Gerber H. Insufficiency fractures of the sacrum. Twenty cases and review of the literature. Spine (Phila Pa 1976). 1993;18(16):2507–2512. | |
Babayev M, Lachmann E, Nagler W. The controversy surrounding sacral insufficiency fractures: to ambulate or not to ambulate? Am J Phys Med Rehabil. 2000;79(4):404–409. | |
Chao EY, Inoue N, Koo TK, Kim YH. Biomechanical considerations of fracture treatment and bone quality maintenance in elderly patients and patients with osteoporosis. Clin Orthop Relat Res. 2004;(425):12–25. | |
Garant M. Sacroplasty: a new treatment for sacral insufficiency fracture. J Vasc Interv Radiol. 2002;13(12):1265–1267. | |
Frey ME, Depalma MJ, Cifu DX, Bhagia SM, Carne W, Daitch JS. Percutaneous sacroplasty for osteoporotic sacral insufficiency fractures: a prospective, multicenter, observational pilot study. Spine J. 2008;8(2):367–373. | |
Bayley E, Srinivas S, Boszczyk BM. Clinical outcomes of sacroplasty in sacral insufficiency fractures: a review of the literature. Eur Spine J. Sep 2009;18(9):1266–1271. | |
Whitlow CT, Mussat-Whitlow BJ, Mattern CW, Baker MD, Morris PP. Sacroplasty versus vertebroplasty: comparable clinical outcomes for the treatment of fracture-related pain. AJNR Am J Neuroradiol. 2007;28(7):1266–1270. | |
Deen HG, Nottmeier EW. Balloon kyphoplasty for treatment of sacral insufficiency fractures. Report of three cases. Neurosurg Focus. 2005;18(3):e7. | |
Betts A. Sacral vertebral augmentation: confirmation of fluoroscopic landmarks by open dissection. Pain Physician. 2008;11(1):57–65. | |
Ehara S. Percutaneous sacroplasty for osteoporotic insufficiency fractures. AJR Am J Roentgenol. 2006;186(2):580; author reply 580–581. | |
Schneider R, Yacovone J, Ghelman B. Unsuspected sacral fractures: detection by radionuclide bone scanning. AJR Am J Roentgenol. 1985;144(2):337–341. | |
Byun WM, Jang HW, Kim SW, Jang SH, Ahn SH, Ahn MW. Diffusion-weighted magnetic resonance imaging of sacral insufficiency fractures: comparison with metastases of the sacrum. Spine (Phila Pa 1976). 2007;32(26):E820–E824. | |
Leroux JL, Denat B, Thomas E, Blotman F, Bonnel F. Sacral insufficiency fractures presenting as acute low-back pain. Biomechanical aspects. Spine (Phila Pa 1976). 1993;18(16):2502–2506. | |
Brook AL, Mirsky DM, Bello JA. Computerized tomography guided sacroplasty: a practical treatment for sacral insufficiency fracture: case report. Spine (Phila Pa 1976). 2005;30(15):E450–E454. | |
Strub WM, Hoffmann M, Ernst RJ, Bulas RV. Sacroplasty by CT and fluoroscopic guidance: is the procedure right for your patient? AJNR Am J Neuroradiol. 2007;28(1):38–41. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.