")
Back to Journals » International Journal of General Medicine » Volume 15
Root Morphology and Canal Configuration of Permanent Canines Among Saudi Population: Systematic Review and Comparison with Worldwide Studies
Authors Asiri AA, AlQahtani KW, Tarrosh MY, Shaiban AS, Al Shawkani HA, Alaajam WH, Bamasud MS, Alqahtani M, Alyousefy MA, Al Moaleem MM
Received 26 June 2022
Accepted for publication 15 August 2022
Published 29 August 2022 Volume 2022:15 Pages 6849—6860
DOI https://doi.org/10.2147/IJGM.S380084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Abdulaziz A Asiri,1 Khalil W AlQahtani,1 Mohammed Y Tarrosh,2 Amal S Shaiban,3 Hamed A Al Shawkani,2 Wafa H Alaajam,3 Maryam S Bamasud,4 Muqbil Alqahtani,5 Mohanad A Alyousefy,6 Mohammed M Al Moaleem7,8
1Endodontic Department, King Saud Medical City, Riyadh, Saudi Arabia; 2Department of Restorative Dental Sciences, College of Dentistry, Jazan University, Jazan, Saudi Arabia; 3Department of Restorative Dental Sciences, Faculty of Dentistry, King Khalid University, Abha, Saudi Arabia; 4Dental Department, Ministry of Health, Sakaka City, Jouf Region, Saudi Arabia; 5General Practitioner, King Faisal University, Alhafuf City, Saudi Arabia; 6Department of Oral Medicine and Periodontology, College of Dentistry, Sana’a University, Sana’a, Yemen; 7Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan, 45142, Saudi Arabia; 8Faculty of Dentistry, University of Ibn al-Nafis for Medical Sciences, Sana’a, 4337, Yemen
Correspondence: Mohammed M Al Moaleem, Prosthetic Dental Sciences, College of Dentistry, Jazan University, Jazan, Kingdom of Saudi Arabia, Tel +00966-550599553, Email [email protected]; [email protected]
Aim: The root morphology and canal configuration (RMCC) of mandibular and maxillary canines among Saudi population is systematically reviewed and compared with international studies in this research.
Methods: This study was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations. The electronic databases of PubMed, Science Direct, Scopus, Wiley Library, Google website search, and Web of Science were searched. Only local and international cross-sectional, comparative, evaluation, and validation studies or case reports published between 2016 and 2022 that directly evaluated canine RMCC and assessed participants using cone beam computed tomography were included.
Results: Forty-three studies that investigated RMCCs (17 local and 26 international) were involved in this review. The original Saudi research recorded that almost 100% of maxillary canines had one root and one canal, whereas 98.4% and 94.1% had one root and one canal in the mandibular arch. Vertucci’s class I had the highest percentages in the maxillary and mandibular arches at 98.3% and 95.8%, respectively, followed by class III with 0.7% and 1.9% for the same arches, respectively. International studies recorded that 100% of maxillary canines had one canal and root; the percentages of the mandibular arch were 92.3 and 98% for single canal and root, respectively; and the highest percentage was obtained by Vertucci’s class I (91.1%), followed by class III (4.7%).
Conclusion: This review reports and confirmed the symmetry of the RMCCs of maxillary and mandibular canines between Saudi studies and other populations. Moreover, Vertucci’s classes I and III were the most frequent RMCCs, and two-rooted canines in both arches were considerably less frequently than single-rooted ones.
Keywords: Vertucci’s classification, mandibular canine, maxillary canine, root morphology, canal configuration, number of canals, number of roots, Saudi population
Background
The preservation of natural teeth in function and aesthetics is the golden goal of endodontic treatment; achieving this objective depends on many stages, starting from the proper selection of the case and treatment plan up to the final restoration.1–3 Root canal (RC) preparation is considered the most critical step owing to its direct effect on the subsequent stages of the procedure.4 The success of root canal therapy (RCT) is attributed to the correct shaping, cleaning, and filling of the RC system, which requires thorough knowledge of the external and internal anatomy of the canal system and its morphological variations.5,6
Failure due to incomplete RCT may lead to postoperative disease, pain, and complications.7 One of the major causes of RCT failure is the clinician’s inability to detect additional canals because of the unexpected anatomy of some RC systems.8 An unexpected anatomy is known as an anatomical variation.3,9 These variations are common because the internal morphology of the RC is more complex than the external morphology of the tooth.10–13 Negligence to treat a few millimeters of tissue pulp can lead to an unsuccessful RCT.10 Likewise, if not all existing RCs are treated, microbes and dead tissue will remain in the RCs, affecting the treatment results and the long-term prognosis of the tooth.13 A dentist must be familiar with the root morphology and canal configuration (RMCC) of the tooth before starting treatment to avoid these failures.2,5
Therefore, a broad knowledge of RMCC and its variations is imperative to improve the prognosis of RCT.14,15 Researchers have used a variety of methods and techniques to evaluate RMCC, including serial sectioning;16,17 canal staining and clearing;18,19 and radiographs, such as periapical or digital radiograph5,19 and cone beam computed tomography.2,3,20–28 CBCT is a highly useful tool for noninvasive, 3D imaging. It is an accurate diagnostic tool for the effective diagnosis of RC morphology, including the length and number of roots and curvatures in sagittal and axial planes.22,29–31
Many researchers proposed different classifications of RMCC.17,19,34,35 Other classifications used other ways for RMCC classification.36,37 The most common classification used as the standard is Vertucci’s classification, in which RMCC is categorized into eight types19,34 as follows (Figure 1):
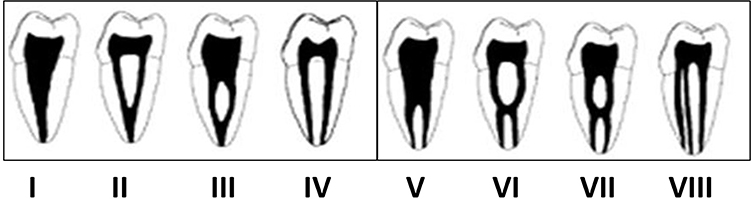 |
Figure 1 Vertucci’s classification of canal configuration. |
Several studies have demonstrated that RMCC varies with race and ethnic group,38,39 as well as with gender.3,40 Therefore, these variations must be involved in the pretreatment analysis for RCT. Previously published research has described the RMCCs of several permanent teeth, including the anterior teeth. Maxillary anterior teeth often have a straightforward morphology that presents with one root and one canal.6,29–31 However, mandibular anterior teeth have a more complex anatomy and often have two canals.19,41–44 Mandibular canines usually have a single root with a single RC.7,8 Several studies of anatomical variations in mandibular canines have been reported in the literature, in which single-root and two-root canals account for about 15%,43,45–48 and double roots and double canals account for 5%.41,49,50 Conversely, few local original studies have investigated canine morphology.2,3,29–33 Maxillary canines usually have one root and one canal and rarely have two roots or two channels. This condition explains local or/and international case reports involving maxillary canines with double roots or canals are few.50,51 Mandibular canines with two canals and one root were recorded in many published Saudi case reports.43,45–48 Other studies reported mandibular canines with two canals and two roots.41,42,44,49,50
Among the Saudi population, quite a few number of peer-reviewed original studies and research2,3,29–33 or case reports41–50 have investigated the RMCC of permanent canine as shown in Table 1. Most other original research studies that investigated the canine has been conducted outside the Saudi population20–26,52–60 as presented in Table 2. Other papers, such as case report studies,51,61–67 studied the RMCC among Western populations. Therefore, this review aimed to search studies in the form of original research and/or case reports on canine RMCC on the basis of Vertucci’s classification19,34 among Saudis. Then, the results were compared with studies from other countries. This study contributes to the structural knowledge prerequisite for a successful RCT.
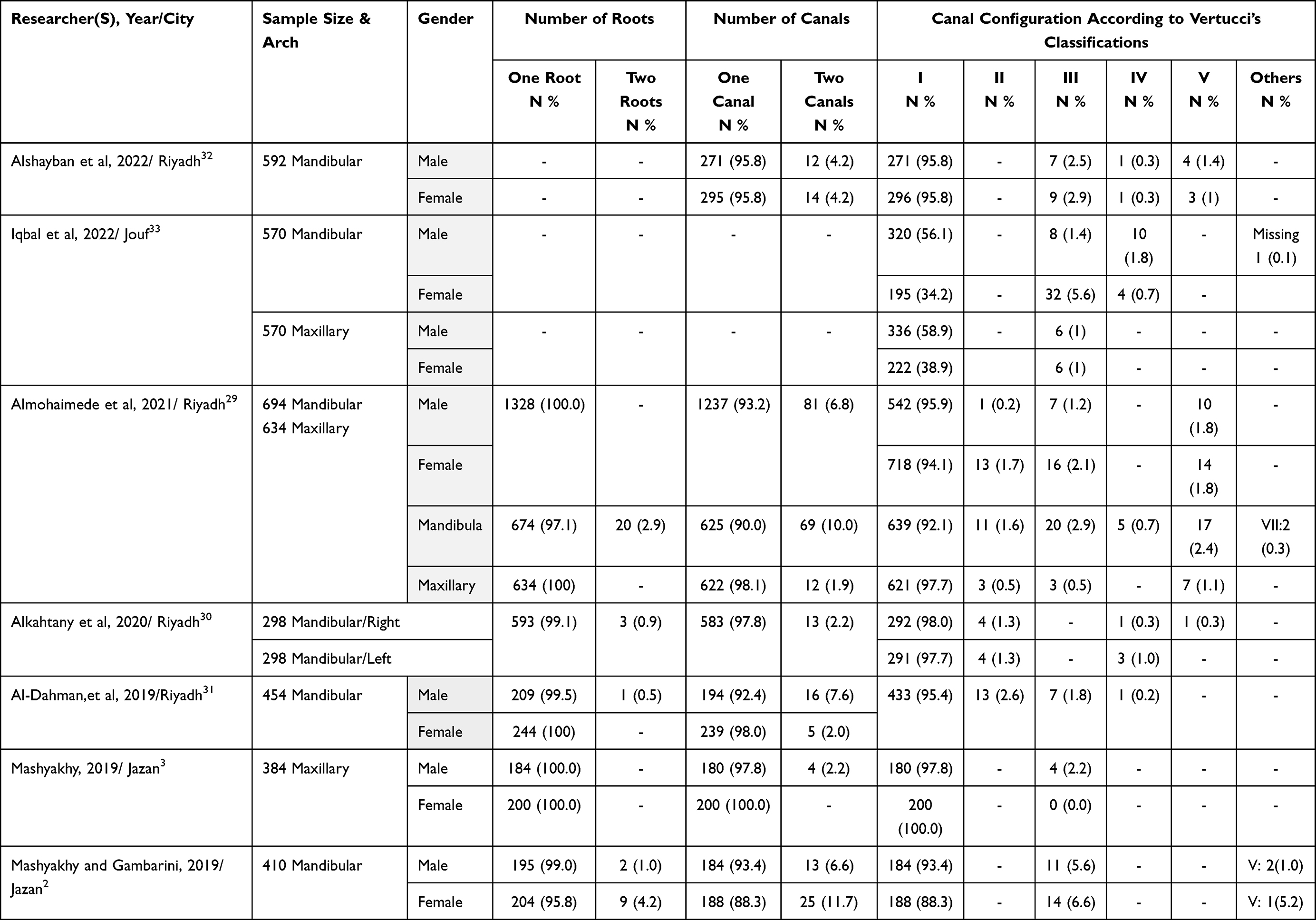 |
Table 1 Original Articles of Canines with Variations in Arch, Gender, Root and Canal Numbers, and RMCC According to Vertucci’s Classification Conducted at Saudi Arabia (n=7) |
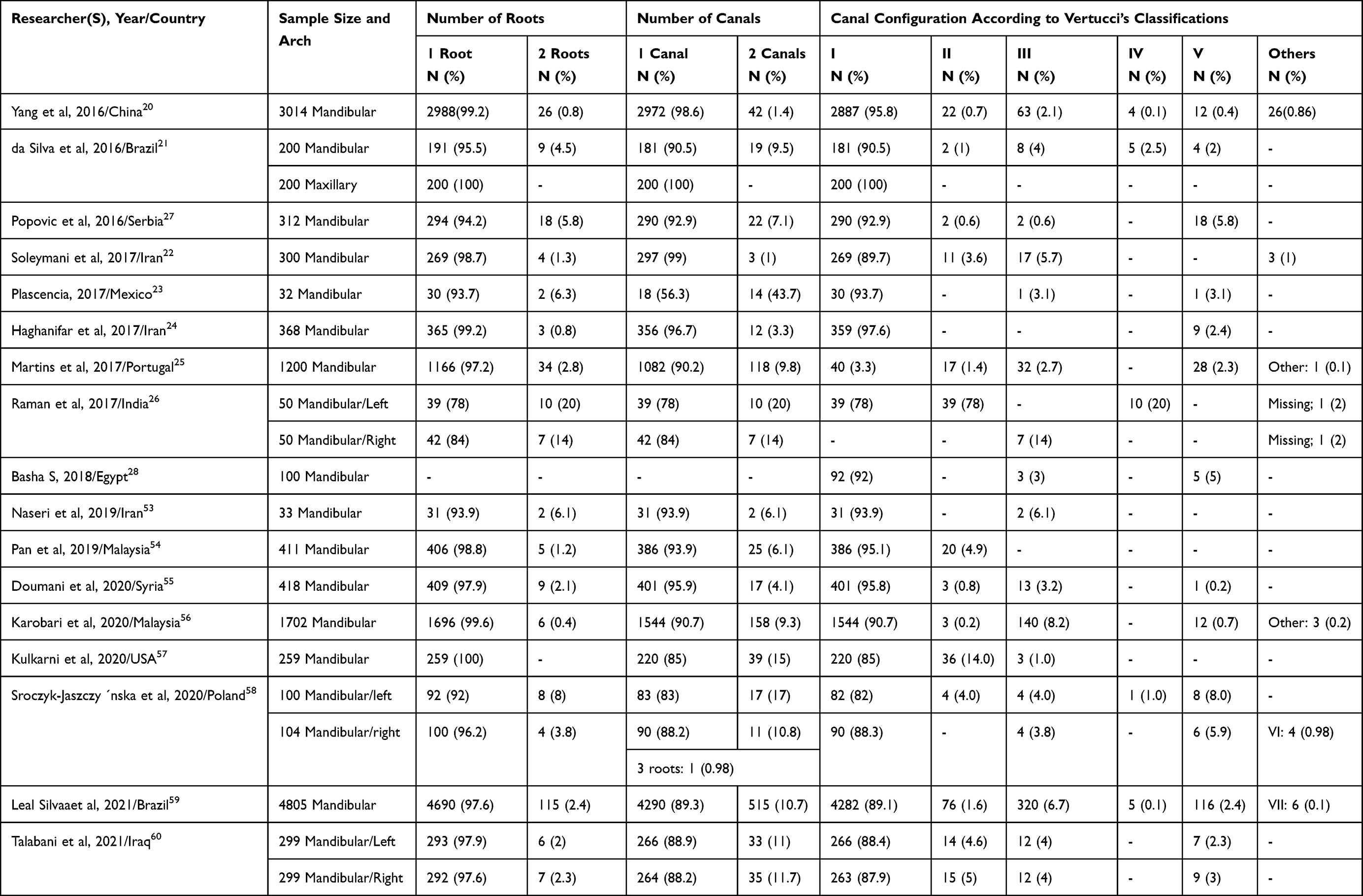 |
Table 2 Original Articles of Canines with Variations in Arch, Root, and Canal Numbers, and RMCC According to Vertucci’s Classification Conducted Internationally (n=17) |
Materials and Methods
The current systematic review was constructed and designed according to the Preferred Reporting Items for Systematic Review and Meta-analysis.68–70
Research Protocols and Eligible Criteria
The authors conducted the search plan using the state, context, and population framework to systematically review the RMCC of maxillary and mandibular canines among the Saudi population and compared the results with other international studies. The questions were “what is the root canal morphology and configuration of canines among the Saudi population?” and “is the canine RMCC among the Saudi population similar or different from the international schema in published research?” Hence, only local, or international cross-sectional studies or case reports that directly evaluated canine RCMC and data by CBCT were included. The inclusive criteria were studies published as original research and/or case report(s) from 2016 until January 2022 and conducted among Saudis; papers comparing the site/arch, sides, and data collected from CBCT technique; and studies published in English. Then, these papers were compared with international original studies and case reports.
Search Method for Identification and Screening of Studies
All peer-reviewed original research articles on RMCCs were selected. PubMed, Science Direct, Scopus, Wiley Library, Google website search, and Web of Science were searched to identify the most relevant cross-sectional studies that assessed and measured the RMCC using CBCT. The first research question was “what is the root morphology and canal configuration of the canine tooth among the Saudi and international populations according to Vertucci’s classification?” The second question was “what are the numbers of canals and roots in the maxillary and mandibular canines among the Saudi and international studies?” The search terms used were “maxillary and/or mandibular canine”, “root morphology”, “canal configuration”, “canal morphology”, “root and canal numbers”, “CBCT”, “dental colleges”, and “medical colleges.” The keywords were used individually or in combination using the Boolean operators “AND”, “OR”, and “NOT” to search for the terms “root morphology” and “canal configuration ” independently. Two reviewers manually completed the search by assessing the selected journals that focus on dentistry, particularly on the RMCC of canines.
Study Selection, Data Collection, and Data Items
Aside from the aforementioned criteria, this study also assessed papers published in English that used CBCT for data collection and any study that investigated the RMCCs according to Vertucci’s classifications, as well as root and canal numbers among Saudi subjects. Then, the findings were compare with the findings of international studies, including original studies or case reports. Moreover, the site of the tooth/teeth and the numbers of canal(s) and root(s) were assessed. A researcher evaluated the validity and duplications of the studies. Studies that did not assess the RMCC, longitudinal studies, case–control studies, and systemic reviews were excluded. Articles that did not indicate the number of subjects and participants or whose specimens had been partly evaluated in other clinical or laboratory studies were also excluded. Two investigators (Al M.M and M.Y) individually read all the titles and abstracts and carefully evaluated them. The researchers had to agree whether each study was related to the study questions. Finally, 38 studies were included, including 15 locally published papers and 18 international studies.
Data Extraction and Analysis
The data from each study were extracted using unique tables designed by the investigators. The information included the author(s)’ name(s), year of publication, name of city or country, sample size, gender, arch, number of roots, number of canals, RMCC according to Vertucci’s classification, side, and clinical findings.
Results
Study Selection
A total of 254 studies were gathered and analyzed, of which 171 were excluded because they were duplicates or not related to the present systematic review. Among the 88 remaining papers, 50 were further excluded, because they were not related to the question of the review. Finally, 42 studies (17 local studies [7 original studies and 10 case reports] and 26 international studies [17 original studies and 9 case reports]) were involved in this review (Figure 2). All extracted data are summarized in Tables 1 and 2.
 |
Figure 2 Flowchart of the study selection process based on the Preferred Reporting Items for Systematic Review and Meta-Analyses. |
Study Characteristics and Quality of the Included Studies
The value of the involved published original research and case reports studies was evaluated using the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology.68–70 For the Saudi studies, five studies had good quality, whereas most of the case reports were had low or fair quality. The international studies in both forms as original and/or case reports papers were good quality reports. All of the original studies used CBCT in studying RMCC, whereas 80% and 70% of the local and international case studies were diagnosed with CBCT, respectively. All studies were assessed and checked by two investigators (Al M. M and M. Y) who independently screened the published articles and assessed the risk of bias.
Data Synthesis of Results
All the papers and research included herein were cross-sectional in nature, studied in vivo, and in the form of case reports, and most of them used CBCT. The Saudi original research recorded that 100% of cases had one root and one canal in the maxillary arch, but the percentages of mandibular canines with one root and one canal were 98.4% and 94.1%, respectively. According to Vertucci’s classification, Class I had the highest percentages in the maxillary and mandibular arches at 98.3% and 95.8%, respectively followed by class III at 0.7% and 1.9% for the same arches, respectively (Table 1).
The Saudi case reports revealed that 79% of cases were recorded in females, 100% were found in the mandibular arch, 64% were Vertucci’s class IV, whereas the remaining cases were class II. Among the reported cases in the mandibular arches, 71% were in the left side, 64% had two roots, and 100% had one canal; the non-vital was the common cause of RCT of canine and documented in 43%, followed by 36% of teeth with vital pulp (Figure 3). All maxillary canines had one canal and root and classified as Vertucci’s class I in the international studies. The percentages of the canines with one canal and root were 92.3% and 98%, respectively; Vertucci’s class I had the highest percentage (91.1%), followed by class III (4.7%) (Table 2). In the international case reports, the percentage of males to females were 36%–64%. Among the mandibular canines, 73% were found on the left side, 55% had two roots, 91%had two canals, and 64% were vitally treated. The frequency of Vertucci’s classes III, IV, and VIII were 36%, 55%, and 9%, respectively (Figure 4).
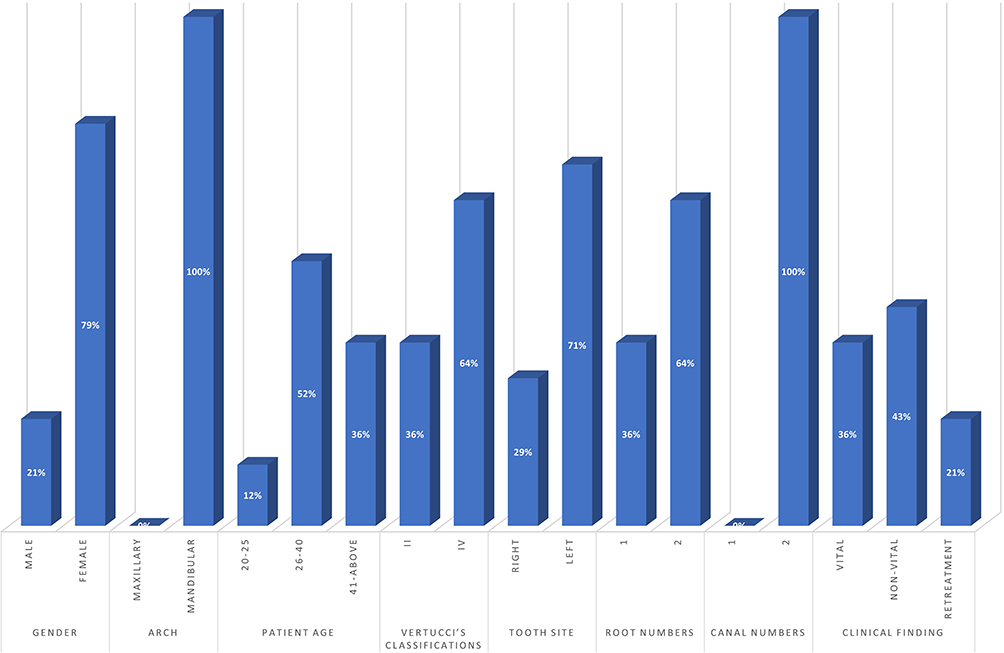 |
Figure 3 Previous published Saudi case reports of canines with variations in gender, arch, root and canal numbers, and RMCC according to Vertucci’s classification (n=10). |
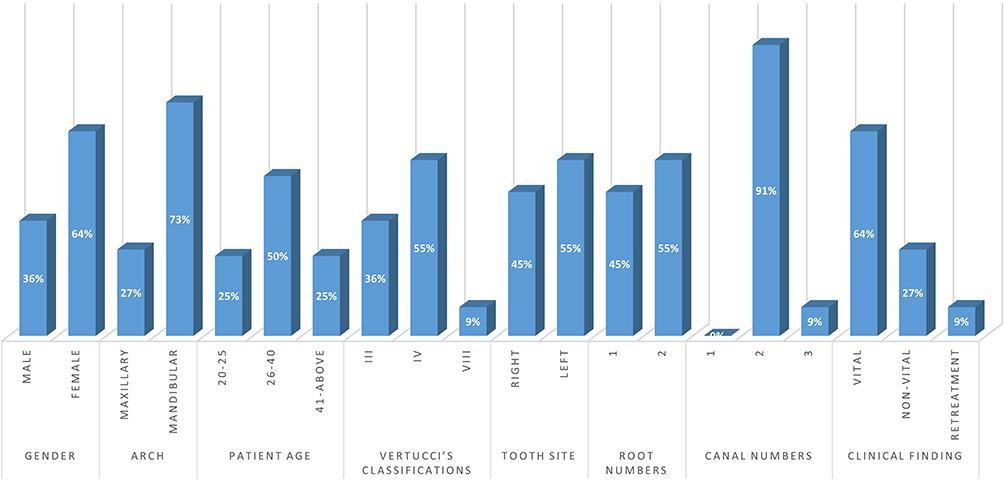 |
Figure 4 Case reports of canines with variations in gender, tooth type, side, root and canal numbers, and RMCC according to Vertucci’s classification in other countries (9 studies and 11 tooth). |
Discussion
Populations with different demographic origins may have variations in tooth morphology.71,72 Since the 1870s, the literature has documented various studies on the anatomy of the RCS of teeth in different populations using various and improved analytical techniques.73,74 Most of these methods involve an invasive procedure that can alter the actual morphology of the canal.75 Recent studies have used computed tomography, a noninvasive 3D imaging, as it is an accurate diagnostic means for the effective diagnosis of RCMCs.22,29–31 Dentists must be aware of the anatomical changes of the RCSs to avoid procedural errors caused by a lack of knowledge and to ensure the success of RCT.73,74 Therefore, knowledge of RMCC is one of the most important keys to successful RCTs. Each type of tooth has common characteristics through which the operator can determine the initial access position and the size of the first file to be used; this approach could be used to deal with any problems that arise during treatment. The canine’s role in mastication is tearing, mediating between the incision of the anterior teeth and the grinding of the posterior teeth.76 CBCT was chosen as the assessment tool in the present study, because it is a reliable resource for analyzing the prevalence of RC configuration and is currently considered the most reliable clinical approach for estimating the proportion of individuals presenting a specific RMCC.77,78
Canines are very long and stable teeth with two canines each in the maxilla and mandible at the corner of the mouth, which is why they are called the “cornerstones” of the dentition. Typically, a canine has a singlepointed cusp, also called a cuspid, and presents with a single root and RC; canines have the most number of dens invaginatus or dens in dente variations.79 The present study was designed and conducted as a systematic review aimed at analyzing the root and RC configuration of maxillary and mandibular canines in the Saudi population based on available anatomic prevalence studies using CBCT and then compared the findings with international studies.
Mandibular canines usually have a single root with a single RC.7,8 However, they can have double roots.43,45–48,56 After a qualitative summary of the included studies, the results identified similarities and differences among the subpopulations analyzed. The results of the current systematic review showed that 98.4% and 100% of maxillary and mandibular canines respectively have a single root, whereas double root was observed only in 1.6% of mandibular canines. However, the prevalence of two-rooted maxillary canines in the Saudi population in this study was 0%. This finding suggests that the existence of two roots in maxillary canines is infrequent. In Iranian populations, the rates of mandibular canines with two roots found by Aminsobhani et al and Rahimi et al that were 4.7% and 12.08% higher than those observed in the present study, respectively.80,81 However, our rates were higher than those of Zhao et al (0.7%) among the Chinese population,82 Singh and Pawar in the South Asian Indian population (0%),83 Zhengyan et al (0.8%) in the Chongqing population,20 Pan et al (1.21%) in the Malaysian population,54 and Soleymani et al (1.3%) among the Iranian population.22
Concerning Vertucci’s classification among maxillary canines, our study showed that type I canal configuration was observed in 98.3%, followed by types III and V (0.7%). These results differ from a study conducted by Amardeepet et al in the Indian population, in which type I was found in 74.5% of cases, followed by type III (11.6%).75 In another study among the Malaysian population, a type I canal configuration was found in all maxillary canines examined (100%).54 The present study recorded that type I canal configuration was found in most mandibular canines (95.8%), followed by type III (1.9%) and Type II (1.1%). Our findings are inconsistent with a study by Wolf et al in the German population, in which type I was presented as 74.5%, followed by 14.3% for the type II class.84 These results differed from other studies, in which type I prevalence was reported as 81.5% in the Mexican population,1 80.4% in the Turkish population,66 95.4% in the Hamadani population in Iran,85 and 92% in the South Asian Indian population.83 These differences in RMCC can be attributed to racial differences in patients even within the same population, which is considered an important factor that can affect clinicians’ perceptions of anatomical suspicion about RMCCs.39
The present study reported differences in root and canal numbers between genders. Notably, 79% of case reports conducted in the Saudi population that are reported in this review were females with two roots and two canals in mandibular canines. Interestingly, Martinns et al and Mancino and Kharouf reported findings that coincide with these results, that is, females have considerably more roots and RCs in mandibular canines than males.40,52 On the contrary, Soleimani et al22 reported that mandibular canines with two roots and two canals are much more common in male than in females. The differences and inconsistencies in the results can be explained by regional differences and differences due to anonymous analysis, race, and the populations investigated.
The present review also investigated bilateral symmetry, as 71% of the two canals were located on the left side in comparison with 29% on the right side in all local case reports, which indicates asymmetry in canal number. These findings are inconsistent with studies carried out among Iranian populations, which reported a high probability of bilateral symmetry of 95.4% in the number of roots and canal configuration.22 Moreover, similarities in RCMC were recorded in a local study conducted by Alkahtany et al30 and among studies conducted outside Saudi Arabia by Raman et al and Sroczyk-Jaszczy´nska et al in India and Poland, respectively.26,58 Finally, no similarities were documented in the clinical findings among the local (36%) and international case reports (64%). This finding could be explained by the regularity of dental check-up and follow-up appointments, as well as proper charting, diagnosis, and treatment plan for each patient during the first visit to dental clinics.
We could not make a comparison between gender in relation to canals or root number and Vertucci’s classification because published research and case reports locally and internationally that deal with gender specification are limited. Other drawbacks may be related to the similarity of the root and canal numbers between the right and left sites and sides of the face.
Conclusions
The following conclusions can be drawn within the limitation of this systematic review. Saudi original research recorded that almost 100% of maxillary canines had one root and one canal, whereas 98.4% and 94.1% of mandibular canines had one root and one canal, respectively. Vertucci’s class I had the highest percentages in the maxillary and mandibular arches at 98.3% and 95.8%, respectively, followed by class III at 0.7% and 1.9%, respectively. International studies recorded that 100% of maxillary canines had one canal and root, and the percentages for single canal and single root in the mandibular arch were 92.3% and 98%, respectively. Vertucci’s class I was found in 100% of the maxillary arches, and Vertucci’s classes I and III had percentages of 91.1% and 4.7% in the mandibular arches, respectively. This review reports and confirms the symmetry in the RMCCs of maxillary and mandibular canines between Saudi studies and other populations. Moreover, Vertucci’s classes I and III were the most frequent RMCCs, and two-rooted canines were considerably less frequently than single-rooted ones in both arches.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7275 root canals. Oral Surg Oral Med Oral Pathol. 1972;33(1):101–110. doi:10.1016/0030-4220(72)90214-9
2. Mashyakhy M. Prevalence of a second root and canal in mandibular and maxillary canines in a Saudi Arabian population: a cone-beam computed tomography study. J Conte Dent Pract. 2019;20(7):773–777.
3. Mashyakhy M, Gambarini G. Root and root canal morphology differences between genders: a comprehensive in-vivo CBCT study in a Saudi population. Acta Stomatol Croat. 2019;53(3):231–246. doi:10.15644/asc53/3/5
4. Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod. 2004;30(8):559–567. doi:10.1097/01.DON.0000129039.59003.9D
5. Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10(1):3–29. doi:10.1111/j.1601-1546.2005.00129.x
6. Dallak AE, Moafa WM, Malhan SM, et al. Root and canal morphology of permanent maxillary and mandibular incisor teeth: a systematic review and comparison with Saudi Arabian population. Biosc Biotech Res Comm. 2020;13(4):1723–1733. doi:10.21786/bbrc/13.4/14
7. Sjögren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990;16(10):498–504. doi:10.1016/S0099-2399(07)80180-4
8. Friedman S. Prognosis of initial endodontic therapy. Endod Topics. 2002;2(1):59–88. doi:10.1034/j.1601-1546.2002.20105.x
9. Mashyakhy M, Awawdeh M, Abu-Melha A, et al. Anatomical evaluation of root and root canal configuration of permanent maxillary dentition in the population of the Kingdom of Saudi Arabia. Biomed Res Int. 2022. doi:10.1155/2022/3428229
10. Kharouf N, Haïkel Y, Mancino D. Unusual maxillary first molars with c-shaped morphology on the same patient: variation in root canal anatomy. Case Rep Dent. 2019;2019:1–10. doi:10.1155/2019/1857289
11. Versiani M, Pécora J, Sousa‐Neto M. The anatomy of two‐rooted mandibular canines determined using micro‐computed tomography. Int Endod J. 2011;44(7):682–687. doi:10.1111/j.1365-2591.2011.01879.x
12. Victorino FR, Bernardes RA, Baldi JV, et al. Bilateral mandibular canines with two roots and two separate canals: case report. Braz Dent J. 2009;20(1):84–86. doi:10.1590/s0103-64402009000100015
13. Neelakantan P, Subbarao C, Subbarao CV. Comparative evaluation of modified canal staining and clearing technique, cone-beam computed tomography, peripheral quantitative computed tomography, spiral computed tomography, and plain and contrast medium–enhanced digital radiography in studying root canal morphology. J Endod. 2010;36(9):1547–1551. doi:10.1016/j.joen.2010.05.008
14. Castellucci A. Access cavity and endodontic anatomy. Endodontics. 2015;1:244–329.
15. Mohammadi Z, Asgary S, Shalavi S, Abbott PV. Methods to decrease the possibility of missed root canals: a clinical update. Iran Endod J. 2016;11(3):209–214. doi:10.7508/iej.2016.03.012
16. Kulid JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod. 1990;16(7):311–317. doi:10.1016/S0099-2399(06)81940-0
17. Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance”. Oral Surg Oral Med Oral Pathol. 1969;28(3):419–425. doi:10.1016/0030-4220(69)90237-0
18. Weng X-L, Yu S-B, Zhao S-L, et al. Root canal morphology of permanent maxillary teeth in the Han nationality in Chinese Guanzhong area: a new modified root canal staining technique. J Endod. 2009;35(5):651–656. doi:10.1016/j.joen.2009.02.010
19. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol Oral Radiol. 1984;58(5):589–599. doi:10.1016/0030-4220(84)90085-9
20. Yang Z, Keke L, Fei W, Yueheng L, Zhi Z. Cone-beam computed tomography study of the root and canal morphology of mandibular permanent anterior teeth in a Chongqing population. Ther Clin Risk Manag. 2016;12:19–25. doi:10.2147/TCRM.S95657
21. da Silva EJ, Queiroz de Castro RW, Nejaim Y, et al. Evaluation of root canal configuration of maxillary and mandibular anterior teeth using cone beam computed tomography: an in-vivo study. Quintessence International. 2016;47(1):19–24. doi:10.3290/j.qi.a34807
22. Soleymani A, Namaryan N, Moudi E, Gholinia A. Root canal morphology of mandibular canine in an Iranian population: a CBCT assessment. Iran Endod J. 2017;12(1):78–82. doi:10.22037/iej.2017.16
23. Plascencia H, Cruz Á, Gascón G, Ramírez B, Díaz M. Mandibular canines with two roots and two root canals: case report and literature review. Case Rep Dent. 2017;2017:8459840. doi:10.1155/2017/8459840
24. Haghanifar S, Moudi E, Bijani A, Ghanbarabadi MK. Morphologic assessment of mandibular anterior teeth root canal using CBCT. Acta Med Acad. 2017;46(2):85–93. doi:10.5644/ama2006-124.193
25. Martins JNR, Marques D, Mata A, Caramês J. Root and root canal morphology of the permanent dentition in a Caucasian population: a cone-beam computed tomography study. Int Endod J. 2017;50:1013–1026. doi:10.1111/iej.12724
26. Raman S, Kumar VJ. A cone-beam computed tomography study of the prevalence of two or more canals in mandibular anteriors in the Chennai population. J Adv Pharm Educ Res. 2017;7(2):1.
27. Popovic M, Papic M, Zivanovic S, Acovic E, Loncarevic S, Ristic V. Cone-beam computed tomography study of the root canal morphology of mandibular anterior teeth in Serbian population. Ser J Exp Clin Res. 2018;19(1):27–34. doi:10.1515/SJECR-2017-0024
28. Basha S. Evaluation of root canal configuration of permanent mandibular anterior teeth in Egyptian subpopulation: a cone beam computed tomography study. Egypt Dent J. 2018;64:1283e91.
29. Almohaimede AA, Alqahtani AA, Alhatlani NM, Alsaloom NS, Alqahtani SA. Interpretation of root canal anatomy of maxillary and mandibular permanent canines in Saudi subpopulation: a cone-beam computed tomography (CBCT) study. Int J Dent. 2021;12:2021.
30. Alkahtany M, Almadhi K, Madwas A, et al. Root canal morphology of mandibular anterior teeth using cone beam computerized tomography in Saudi Sub-population. Int J Dent Oral Heal. 2020;6(4):1–6.
31. Al-Dahman Y, Alqedairi A, Alfawaz H, Alnassar F, Al-Jebaly A. Cone-beam computed tomographic evaluation of root canal morphology of mandibular canines in a Saudi subpopulation. Saud Endo J. 2019;9(2):113.
32. Alshayban M, Abughosh T, Almalki W, Alrasheed M. Cone-beam computed tomographic evaluation of root canal morphology of mandibular anterior teeth in a Saudi subpopulation, retrospective in-vivo study. Saudi Dent J. 2022;34:390–396. doi:10.1016/j.sdentj.2022.04.008
33. Iqbal A, Karobari MI, Alam MK, et al. Evaluation of root canal morphology in permanent maxillary and mandibular anterior teeth in Saudi subpopulation using two classification systems: a CBCT study. BMC Oral Health. 2022;22:171. doi:10.1186/s12903-022-02187-1
34. Al-Kadhima AH, Rajionb ZA, Malika NAB, Jaafara AB. Morphology of maxillary first molars analyzed by cone-beam computed tomography among Malaysian: variations in the number of roots and canals and the incidence of fusion. Int Medical J Malaysia. 2017;16(2):33–49. doi:10.31436/imjm.v16i2.322
35. Ahmed HMA, Aziz ZAC, Azami NH, et al. Application of a new system for classifying root canal morphology in undergraduate teaching and clinical practice: a national survey in Malaysia. Inte Endo J. 2020;53(6):871–879. doi:10.1111/iej.13271
36. Karobari MI, Parveen A, Mirza MB, et al. Root and root canal morphology classification systems. Int J Dent. 2021;6. doi:10.1155/2021/6682189
37. Ahmed HMA, Versiani MA, De-Deus G, Dummer PMH. A new system for classifying root and root canal Morphology. Int Endod J. 2017;50:761–770. doi:10.1111/iej.12685
38. Kottoor J, Albuquerque D, Velmurugan N, Kuruvilla J. Root anatomy and root canal configuration of human permanent mandibular premolars: a systematic review. Anat Res Int. 2013;2013:14. doi:10.1155/2013/254250
39. Martins JNR, Gu Y, Marques D, Francisco H, Caramês J. Differences on the root and root canal morphologies between asian and white ethnic groups analyzed by cone-beam computed tomography. J Endod. 2018;44(7):1096–1104. doi:10.1016/j.joen.2018.04.001
40. Martins JNR, Marques D, Francisco H, Caramês J. Gender influence on the number of roots and root canal system configuration in human permanent teeth of a Portuguese subpopulation. Quintessence Int. 2018;49(2):103–111. doi:10.3290/j.qi.a39508
41. Rahaf A, Manar A, Barakat R. Endodontic treatment of uncommon morphology of two-rooted mandibular canine: a case report. Int J Dentistry Oral Sci. 2021;8(8):4133–4135.
42. Alhomaidhi LM. Endodontic retreatment of a mandibular canine with two roots and two canals: a case report. Inte J Medi Develo Count. 2021;5(1):403–406. doi:10.24911/IJMDC.51-1606133450
43. Alfahadi HR, Alghamdi AM. Endodontic management of permanent mandibular canine with Type II canal configuration using cone-beam computed tomography. Saud Endo J. 2020;10:271–273.
44. Arora S, Gill GS, Abdulla AM, et al. Multidisciplinary approach for the management of mandibular canines with rare configuration. J Pharm Bioall Sci. 2020;12:S635–9. doi:10.4103/jpbs.JPBS_82_20
45. Abulhassan EH, Almohammed IE, Alkahtany SM. Mandibular canine with two canals: a case report in Saudi Arabia. Int J Med Sci Public Health. 2019;8(12):12–16.
46. Doumani M, Habib A, Alhenaky MA, Alotaibi KS, Alanazi MS, Alsalhani A. Root canal treatment of mandibular canine with two root canals: a case report series. J Family Med Prim Care. 2019;8:3763–3765. doi:10.4103/jfmpc.jfmpc_782_19
47. Al Dahman YH, Al Hawwas AY. Root canal retreatment of permanent mandibular canine with two canals-A case report. J Advan Research Dent Oral Health. 2017;4(1):555626.
48. Alenezi MA, Al-Hawwas AY. Permanent mandibular canine with two roots and two root canals: two case reports. Saudi Endod J. 2016;6:98–100. doi:10.4103/1658-5984.180624
49. Almobarraz R. Endodontic retreatment of a mandibular canine with two roots and two canals CBCT. J Pak Dent Assoc. 2019;28(2):98–100. doi:10.25301/JPDA.282.98
50. Abdelgawad RA, Aljohani MZ, Taymour NM. Mandibular permanent canine with two root canals, two roots: case report, Al-Medina, Saudi Arabia. Biomed J Sci Tech Res. 2019;20(1):14729–14732. doi:10.26717/BJSTR.2019.20.003385
51. Sahoo HS, KurinjiAmalavathy R, Pavani D. A case report on endodontic management of a rare vertucci type III maxillary canine. Case Rep Dent. 2019;2019:1–4. doi:10.1155/2019/4154067
52. Mancino D, Kharouf N. Endodontic anatomy of human mandibular canines: three case reports. Chin J Dent Res. 2019;22(2):139–143. doi:10.3290/j.cjdr.a42518
53. Naseri M, Ahangari Z, Bagheri N, Jabbari S, Gohari A. Comparative accuracy of cone-beam computed tomography and clearing technique in studying root canal and apical morphology of mandibular canines. Iran Endod J. 2019;14(4):271–277.
54. Pan JYY, Parolia A, Chuah SR, Bhatia S, Mutalik S, Pau A. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC Oral Health. 2019;19(1):14. doi:10.1186/s12903-019-0710-z
55. Doumani M, Habib A, Alhalak AB, Al-Nahlawi TF, Al Hussain F, Alanazi SM. Root canal morphology of mandibular canines in the Syrian population: a CBCT Assessment. J Family Med Prim Care. 2020;9(2):552–555. doi:10.4103/jfmpc.jfmpc_655_19
56. Karobari MI, Noorani TY, Halim MS, Ahmed HMA. Root and canal morphology of the anterior permanent dentition in Malaysian population using two classification systems: a CBCT clinical study. Aust Endod J. 2021;47(2):202–216. doi:10.1111/aej.12454
57. Kulkarni V, Duruel O, Ataman-Duruel ET, Tözüm MD, Nares S, Tözüm TF. In-depth morphological evaluation of tooth anatomic lengths with root canal configurations using cone beam computed tomography in North American population. J Appl Oral Sci. 2020;28:e20190103. doi:10.1590/1678-7757-2019-0103
58. Sroczyk-Jaszczyńska M, Kołecki J, Lipski M, et al. A study of the symmetry of roots and root canal morphology in mandibular anterior teeth using cone-beam computed tomographic imaging in a Polish population. Folia Morphol. 2020;79(4):835–844. doi:10.5603/FM.a2019.0128
59. Leal Silvaa EJN, Pradob MC, Duartec AH, Versianid MA, Marquese D, Martinse JNR. Prevalence of root canal system configurations in the Brazilian population analyzed by cone-beam computed tomography – a systematic review. Rev Port Estomatol Med Dent Cir Maxilofac. 2021;62(1):1–13.
60. Talabani RM. Assessment of root canal morphology of mandibular permanent anterior teeth in an Iraqi subpopulation by cone-beam computed tomography. J Dent Sci. 2021. doi:10.1016/j.jds.2021.02.010
61. Victorino FR, Rocha IS, Lazarin R, Seron MA, Sivieri-Araujo G, Almeida RS. Maxillary Canine with two roots and two canals: a case report. Res Soc Dev. 2021;10(2):e36410212599. doi:10.33448/rsd-v10i2.12599
62. Bhaskar A, Kumar R, Nawal RR, Talwar S. Demystifying the complexity: a case report on the management of mandibular canine with two roots. Cureus. 2020;12(2):e7072. doi:10.7759/cureus.7072
63. Krishna EM. A case report on endodontic management of mandibular canine with 2 root canals. WJPMR. 2020;6(7):184–188.
64. Agarwal K, Samant PS, Srivastava V, Jain G. Demystifying anatomical variations – endodontic therapy of twin rooted mandibular canine with concomitant root canals: an unusual case report. IP Indian J Cons Endod. 2020;5(3):150–153.
65. Roy DK, Cohen S, Singh VP, Marla V, Ghimire S. Endodontic management of mandibular canine with two roots and two canals: a rare case report. BMC Res Notes. 2018;11(1):111. doi:10.1186/s13104-018-3226-8
66. Kunmar D, Adhikari B, Gautam V, Arora C, Subham S, Tripathi R. A rare root canal configuration of maxillary canine: a case report. J Univ Coll Med Sci. 2017;5(2):53–56.
67. Kulkarni NR, Kamat SB, Hugar SI, Nanjannawar GS. Mandibular canine with two roots and two root canals - a rare case. J Clin Diagn Res. 2016;10(9):ZJ07–ZJ08. doi:10.7860/JCDR/2016/20766.8474
68. Salameh JP, Bossuyt PM, McGrath TA, et al. Preferred reporting items for systematic review and meta-analysis of diagnostic test accuracy studies (PRISMA-DTA): explanation, elaboration, and checklist. BMJ Clinical Res. 2020;370:m2632. doi:10.1136/bmj.m2632
69. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. PubMed PMID: 18313558. doi:10.1016/j.jclinepi.2007.11.008
70. Wolf TG, Anderegg AL, Yilmaz B, Campus G. Root canal morphology and configuration of the mandibular canine: a systematic review. Int J Environ Res Public Health. 2021;18:10197. doi:10.3390/ijerph181910197
71. von Zuben M, Martins JNR, Berti L, et al. Worldwide prevalence of mandibular second molar c-shaped morphologies evaluated by cone-beam computed tomography. J Endod. 2017;43(9):1442–1447. doi:10.1016/j.joen.2017.04.016
72. Martins JNR, Alkhawas MAM, Altaki Z, et al. Worldwide analyses of maxillary first molar second mesiobuccal prevalence: a multicenter cone-beam computed tomographic study. J Endod. 2018;44(11):1641–1649.e1. doi:10.1016/j.joen.2018.07.027
73. Calişkan MK, Pehlivan Y, Sepetçioğlu F, Türkün M, Tuncer SS. Root canal morphology of human permanent teeth in a Turkish population. J Endod. 1995;21(4):200–204. doi:10.1016/S0099-2399(06)80566-2
74. Miccoli G, Cicconetti A, Gambarini G, et al. A new device to test the bending resistance of mechanical endodontic instruments. Appl Sci. 2020;10(20):7215. doi:10.3390/app10207215
75. Amardeep NS, Raghu S, Natanasabapathy V. Root canal morphology of permanent maxillary and mandibular canines in Indian population using cone beam computed tomography. Anat Res Int. 2014;2014:731859. doi:10.1155/2014/731859
76. Fuller TL, Denehy GE, Schulein TM. Concise Dental Anatomy and Morphology.
77. Martins JNR, Marques D, Silva EJNL, Caramês J, Versiani MA. Prevalence studies on root canal anatomy using cone-beam computed tomographic imaging: a systematic review. J Endod. 2019;45(4):372–386.e4. doi:10.1016/j.joen.2018.12.016
78. Low KM, Dula K, Bürgin W, von Arx T. Comparison of periapical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J Endod. 2008;34(5):557–562. doi:10.1016/j.joen.2008.02.022
79. Clarke P, Longridge N, Gartshore L. A multidisciplinary management of a type III dens invaginatus in a maxillary permanent canine. Eur Arch Paediatr Dent. 2016;17(2):131–136. doi:10.1007/s40368-015-0204-x
80. Aminsobhani M, Sadegh M, Meraji N, Razmi H, Kharazifard MJ. Evaluation of the root and canal morphology of mandibular permanent anterior teeth in an Iranian population by cone-beam computed tomography. J Dent. 2013;10(4):358–366. PMID: 24396355; PMCID: PMC3875510.
81. Rahimi S, Milani AS, Shahi S, Sergiz Y, Nezafati S, Lotfi M. Prevalence of two root canals in human mandibular anterior teeth in an Iranian population. Indian. 2013;24(2):234–236. PMID: 23965453. doi:10.4103/0970-9290.116694
82. Zhao Y, Dong YT, Wang XY, et al. Cone-beam computed tomography analysis of root canal configuration of 4 674 mandibular anterior teeth. Beijing Da Xue Xue Bao Yi Xue Ban. 2014;46(1):95–99. Chinese. PMID: 24535357.
83. Singh S, Pawar M. Root and canal morphology of mandibular incisors and canines in South Asian Indian population by canal staining and tooth clearing technique. Endodontology. 2016;28(2):148. doi:10.4103/0970-7212.195435
84. Wolf TG, Anderegg AL, Haberthür D, et al. Internal morphology of 101 mandibular canines of a Swiss-German population by means of micro-CT: an ex vivo study. Sci Rep. 2021;11(1):21281. doi:10.1038/s41598-021-00758-w
85. Mirzaie M, Zaban PT. Cone-beam computed tomography study of root canals in a Hamadani population in Iran. Avicenna J Dent Res. 2018;4(2):93–99.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.