")
Back to Journals » OncoTargets and Therapy » Volume 16
Role of Systemic Immunoinflammation Landscape in the Overall Survival of Patients with Leptomeningeal Metastases from Lung Cancer
Authors Wang JW , Yuan Q, Li L, Cao KH, Liu Q, Wang HL , Hu K, Wu X, Wan JH
Received 22 December 2022
Accepted for publication 10 March 2023
Published 23 March 2023 Volume 2023:16 Pages 179—187
DOI https://doi.org/10.2147/OTT.S402389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Arseniy Yuzhalin
Jia-Wei Wang,1 Qing Yuan,1 Li Li,2 Kai-Hua Cao,1 Qi Liu,1 Hong-Liang Wang,3 Ke Hu,1,* Xi Wu,4,* Jing-Hai Wan1
1Department of Neurosurgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Medical Records Department, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3Department of Neurosurgery, Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui Province, People’s Republic of China; 4General Department, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ke Hu, Department of Neurosurgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 17 Nanli Panjiayuan, Chaoyang District, Beijing, 100021, People’s Republic of China, Tel/Fax +86-10-87787350, Email [email protected] Xi Wu, General Department, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 17 Nanli Panjiayuan, Chaoyang District, Beijing, 100021, People’s Republic of China, Tel/Fax +86-10-87788200, Email [email protected]
Purpose: Several biomarkers, such as baseline neutrophil-to-lymphocyte ratio (NLR), have been more investigated in patients with brain metastases (BM), while their role in patients with leptomeningeal metastases (LM) has not been clarified. Considering the difference between the clinical behaviour of BM and LM, there is the need for addressing the role of these biomarkers in LM.
Methods: The present study retrospectively analyzed 95 consecutive patients with LM from lung cancer who were diagnosed at the National Cancer Center, Cancer Hospital of Chinese Academy of Medical Sciences between January 2016 and December 2019. Baseline NLR, platelet-to-lymphocyte ratio (PLR), systemic immunoinflammation index (SII), and lymphocyte‐to-monocyte ratio at diagnosis of LM were calculated based on complete blood count and correlated, along with other characteristics, with overall survival (OS) using univariate and multivariate analyses. The best cutoff values for systemic immunoinflammation biomarkers were derived using the surv_cutpoint function in R software, which optimized the significance of the split between Kaplan–Meier survival curves.
Results: Median OS of patients with LM was 12 months (95% CI 9– 17 months). On univariate analysis, NLR, PLR, SII, LMR, sex, smoking history, ECOG performance status (PS) scores, histological subtypes and targeted therapy were all significantly associated with OS. Only NLR (P=0.034, 95% CI 1.060– 4.578) and ECOG PS scores (P=0.019, 95% CI 0.137– 0.839) maintained a significant association with OS on multivariate analysis. Furthermore, patients with baseline NLR > 3.57 had significantly worse OS than patients with NLR ≤ 3.57 (median OS 7 vs 17 months), as did patients with ECOG PS scores > 2 vs ≤ 2 (median OS 4 vs 15 months).
Conclusion: Both baseline NLR and PS scores at the time of LM diagnosis are helpful and available prognostic biomarkers for patients with LM from lung cancer.
Keywords: systemic immunoinflammation index, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte‐to-monocyte ratio, leptomeningeal metastases, lung cancer
Introduction
As a leading cause of mortality and morbidity following lung cancer worldwide, leptomeningeal metastases (LM) have received considerable attention in the clinical and preclinical scenario, occurring in about 10% of patients with lung cancer during the advanced metastatic stages.1,2 With the advent of molecularly targeted therapy and immunotherapy, survival from lung cancer continues to improve.3,4 These patients are at greater risk of developing LM in the course of disease. Median survival for LM after lung cancer has ranged from the historical 6–8 weeks without tumor-specific treatment to the current 3–11 months in the context of LM-directed treatment.1,5 Unfortunately, although the well-known unfavorable outcomes of LM from lung cancer have long been recognized, therapeutic strategies for LM, which mainly include intrathecal pharmacotherapy, radiotherapy, and systemic pharmacotherapy, remain limited and unsatisfactory.2,6,7 Furthermore, considering that an accurate assessment of prognosis across the extremely heterogeneous population of LM is very important and may facilitate clinical decision-making and appropriate stratification of future clinical trials, extensive efforts have focused on predicting outcomes for patients with LM from lung cancer.
In recent years, systemic immunoinflammation perturbation has been revealed as a hallmark of solid cancer, and plays an important role in tumorigenesis, tumor growth, cancer progression, and patient survival.8–10 Therefore, predictive biomarkers that can reflect the systemic immunoinflammatory state are widely explored in the clinic and labs, including various types of immune cells, blood cells, and other biochemical or hematological cells.10,11 For example, biomarkers such as systemic immunoinflammation index (SII), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte‐to-monocyte ratio (LMR) have been investigated more in patients with brain metastases (BM) and other various human malignancies8,12,13 based on complete blood count (CBC), a test that is accessible, convenient, and routinely measured in the clinic. Considering the difference between the clinical behaviour of BM and LM,14,15 there is a need to address the role of these biomarkers in LM. Recently, Hong et al investigated a total of 109 patients with LM treated from 2009 to 2019 in four tertiary centers in China, and they found that lower NLR was an independent favorable factor for outcome in patients with LM from lung cancer.16 To the best of our knowledge, the prognostic relevance of the systemic immunoinflammation landscape in LM from lung cancer based on CBC tests remains not fully understood. In the present study, we conducted a retrospective investigation of our experience with 95 patients with LM from lung cancer that aimed to evaluate clinical factors and baseline systemic immunoinflammation biomarkers to identify pretreatment factors associated with overall survival (OS) in this subtype of patients.
Methods
This retrospective research was approved by the Ethics Committee of the Cancer Hospital of the Chinese Academy of Medical Sciences (22/052-3253) and performed in accordance with the World Medical Association and Declaration of Helsinki. Informed consent was obtained from all participants.
Patients and Data Collection
Medical records from patients with LM from lung cancer admitted to the National Cancer Center, Cancer Hospital of the Chinese Academy of Medical Sciences between January 2016 and December 2019 were retrospectively reviewed. The diagnosis of LM was based on the positive cerebrospinal fluid (CSF) cytology or concurrent presence of typical clinical signs and neuroimaging. Single intracranial parenchymal metastasis without LM, LM from solid cancers other than lung cancer, and a diagnosis of LM with discrepancies failing to reach consensus were excluded from the final analysis. Data on demographic parameters and baseline CBC test results of each patient were retracted from the medical records, including age and sex at the time of diagnosis of LM, smoking history, Eastern Cooperative Oncology Group (ECOG) performance status (PS) scores at the time of diagnosis of LM, diagnostic criteria, presence of concurrent BM and extracranial transfer at the time of diagnosis of LM, histology subtypes, treatment information after the diagnosis of LM (eg, radiotherapy, intrathecal chemotherapy, and molecularly targeted therapy), and peripheral neutrophil, lymphocyte, monocyte and platelet counts at the time of diagnosis of LM. OS was defined as the interval between the date of diagnosis of LM and the date of death from all causes or the date of the last follow-up for survivors.
Systemic Immunoinflammation Biomarkers
Based on peripheral blood cell counts on CBC tests at the time of diagnosis of LM, four systemic immunoinflammation biomarkers (NLR, PLR, SII, and LMR) were calculated: NLR = neutrophils/lymphocytes, PLR = platelets/lymphocytes, SII = (neutrophils × platelets)/lymphocytes, and LMR = lymphocytes/monocytes.
Statistical Analysis
All statistical analyses and graphing were performed using R software (R version 4.1.0: http://www.r-project.org/), SPSS 26, and Prism 9.0 (GraphPad software, San Diego, CA, USA). Survival and survminer packages were loaded in R software. The Surv_cutpoint function was used to determine the optimal cutoff points for NLR, PLR, SII, and LMR in the data sets, dividing the samples into high- and low-expression groups according to the protocols in our lab.17,18 OS curves were plotted according to the Kaplan–Meier method, with the log-rank test applied for comparison. A multiple Cox proportional hazard model was used to predict independent prognostic factors that significantly impacted patient survival. Then, time-dependent receiver-operating characteristic curve analysis in Prism based on the independent prognostic factors was performed, Finally, a nomogram model of independent prognostic factors was established through the rms package in R to predict survival prognosis for those with LM in 1, 2, and 3 years. P<0.05 was considered statistically significant.
Results
Demographic Characteristics
A total of 95 patients with LM from lung cancer were included for the analysis. The demographic characteristics are listed in Table 1. The median age at the time of LM diagnosis was 55 years (range 36–77 years). Most patients were female (56.84%), nonsmokers (71.58%), relatively fit (ECOG PS scores 0–2, 88.42%), had accompanying extracranial transfer (86.32%), and had a histological subtype of non–small cell lung cancer (NSCLC; adenocarcinoma 92.63%, squamous-cell carcinoma 3.16%, large‐cell carcinoma 1.05%). All these patients showed typical neurological manifestations and findings on enhanced cerebrospinal MRI, with 71.58% of patients having positive CSF cytology indicating presence of tumor cells. In addition, 84.21% of patients with LM had concurrent BM at the time of LM diagnosis. In our center, treatment of lung cancer and LM is performed by a multidisciplinary team for integrated care, and is mainly based on pathological type, disease stage, and molecular subtypes. In the present cohort, whole-brain radiotherapy, intrathecal chemotherapy, and molecularly targeted therapy were used to treat LM in 42.11%, 71.58%, and 74.74% of patients, respectively.
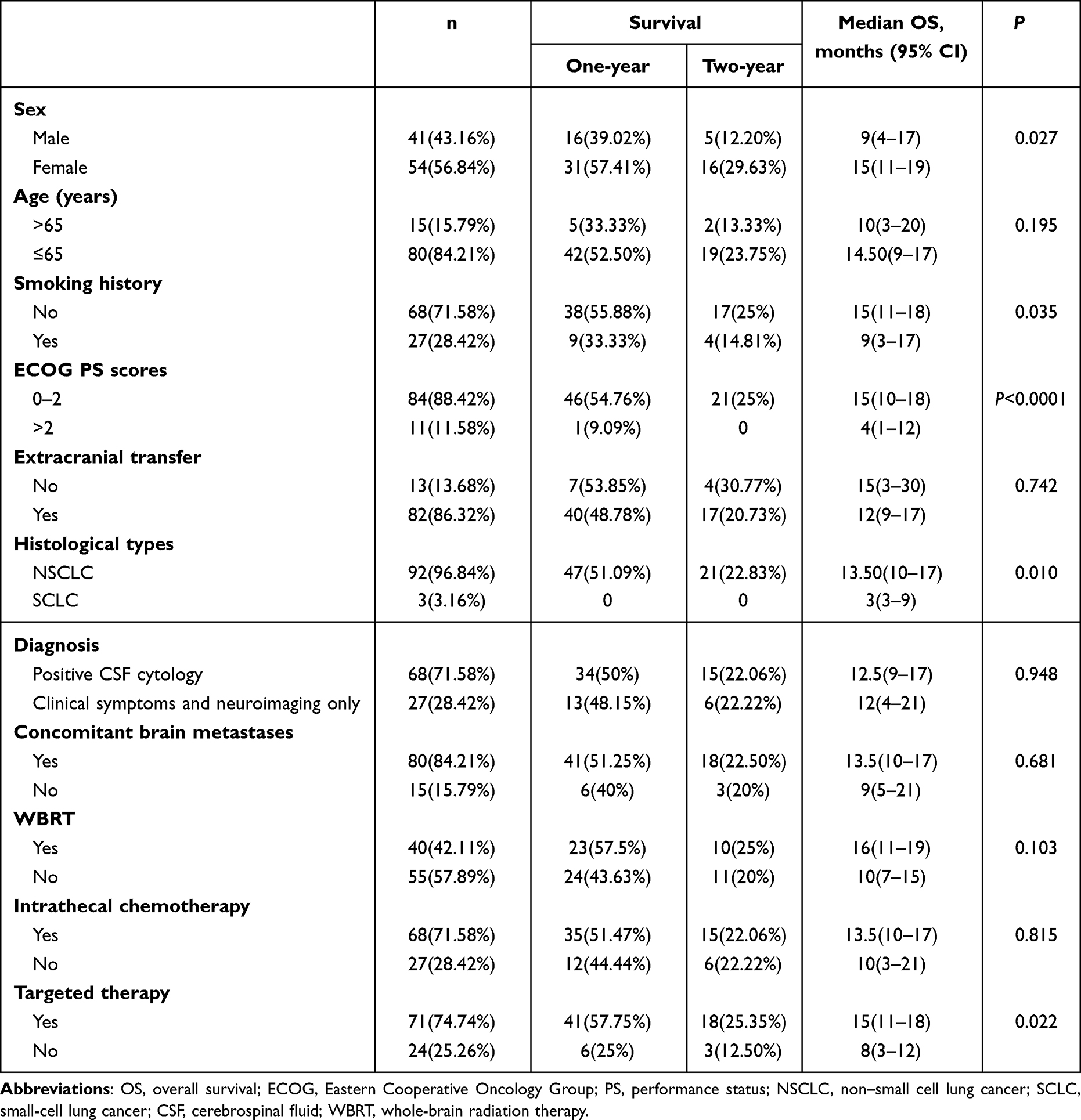 |
Table 1 Demographic characteristics and prognosis in patients with LM from lung cancer |
Prognostic Factors Based on Univariate and Multivariate Analyses
Follow-up continued until September 2022. At the end of follow-up, six patients (6.32%) were still alive and 89 (93.68%) had died. Median OS was 12 months (range 1–80 months, 95% CI 9–17 months). Median time to onset of LM from diagnosis of lung cancer was 18 months (range 0–67 months, 95% CI 13–21 months) and median time from diagnosis of lung cancer to last follow-up was 32 months (range 5–122 months, 95% CI 28–37 months). As shown in Table 1 and Table 2, on univariate analysis of the entire cohort, male sex (P=0.027), smoking history (P=0.035), poor performance status (ECOG PS score >2, P<0.0001), SCLC (P=0.010), NLR >3.57 (P<0.0001), PLR >209.77 (P=0.047), and SII >1139.25 (P<0.0001) predicted poor OS. In contrast, the application of molecularly targeted therapy (P=0.0215) and LMR >1.68 (P<0.0001) predicted favorable OS. Figure 1A–I shows the Kaplan–Meier OS curves stratified according to sex, smoking history, ECOG PS scores, histological subtypes, molecularly targeted therapy, and baseline NLR, PLR, SII, and LMR levels. No other clinicopathological parameter — age, extracranial transfer, diagnostic criteria, concomitant BM, whole-brain radiation therapy (WBRT), or intrathecal therapy — was associated with patient prognosis (P>0.05). On multivariate Cox analysis, NLR remained an independent survival factor (P=0.034), together with ECOG PS score (P=0.019; Table 3). Figure 2A and B show the receiver-operating characteristic curves according to the NLR and ECOG PS scores. Based on the previous multivariate Cox model, two variates (ECOG PS scores and NLR) were integrated into the nomogram to predict 1-, 2-, 3-year OS (Figure 2C).
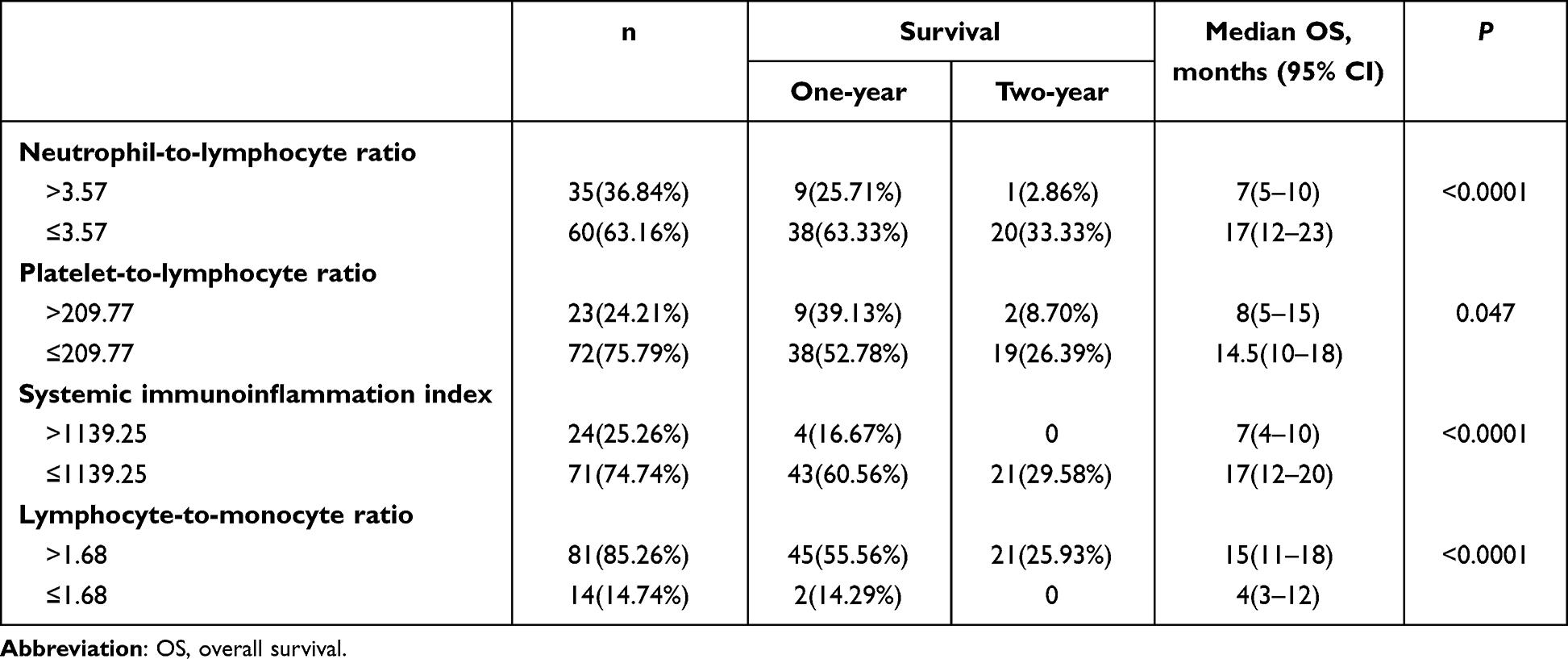 |
Table 2 Systemic immunoinflammation biomarkers and prognosis in patients with LM from lung cancer |
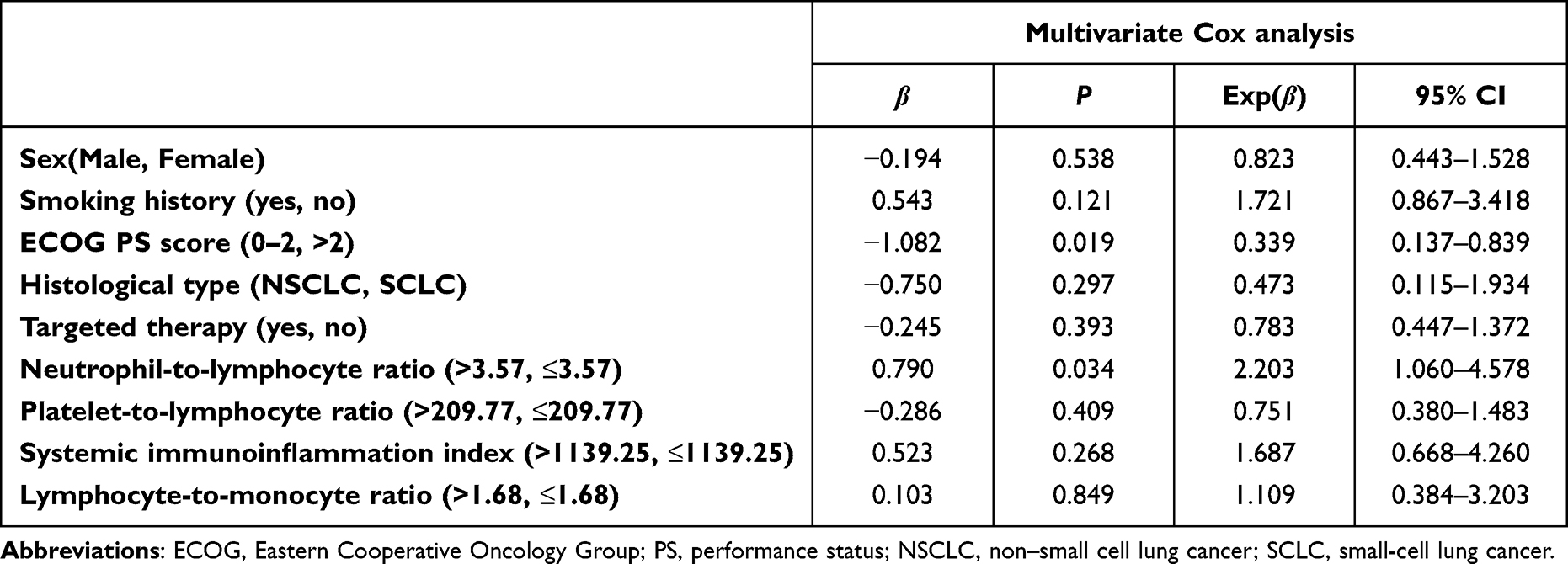 |
Table 3 Multivariate analyses of prognostic factors associated with OS in LM from lung cancer |
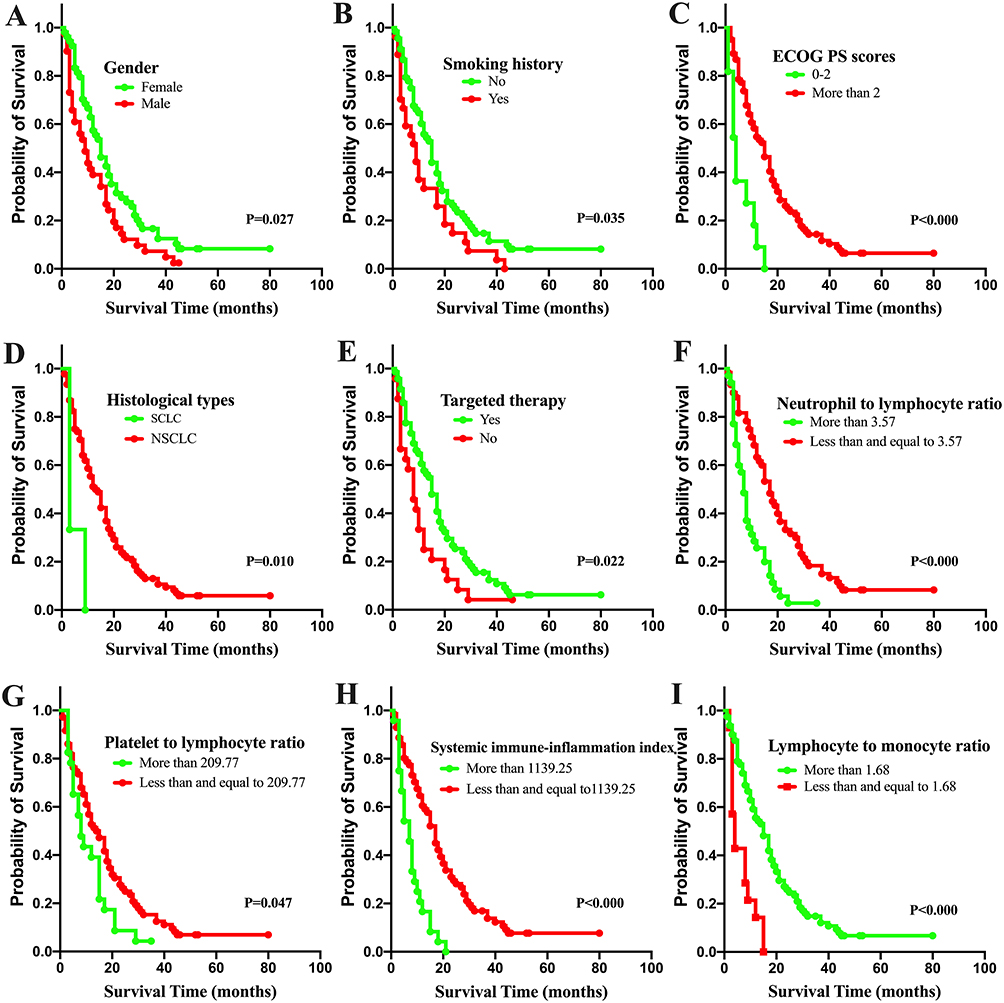 |
Figure 1 Kaplan–Meier curves showing overall survival for LM from lung cancer according to clinical parameters and systemic immunoinflammation biomarkers. Univariate analysis showed sex (A), smoking history (B), ECOG performance status scores (C), histological subtypes (D), targeted therapy (E), NLR (F), PLR (G), SII (H), and LMR (I) were all significantly associated with OS (P<0.05). Abbreviations: ECOG, Eastern Cooperative Oncology Group; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SII, systemic immunoinflammation index; LMR, lymphocyte‐to-monocyte ratio. |
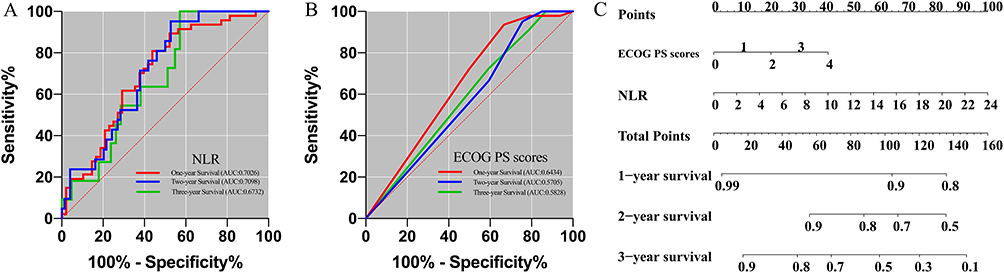 |
Figure 2 ROC-curve analysis (A and B) and nomogram (C) of NLR and ECOG PS scores in LM from lung cancer for survival prediction of 1, 2, 3 years. Abbreviations: ROC, receiver-operating characteristic; NLR, neutrophil-to-lymphocyte ratio; ECOG PS, Eastern Cooperative Oncology Group performance status; AUC, area under the curve. |
Discussion
To date, promising advances have been made in several aspects of LM from lung cancer,2 mainly involving improved acknowledgment of genetic profiles from CSF biopsy19 and the advent of novel therapeutic agents with greater central nervous system penetration, especially in EGFR-mutant and ALK-rearranged subtypes.20,21 However, LM remains a serious complication of advanced lung cancer with poor prognosis, and its management is still challenging in the clinic. In order to improve survival and maintain quality of life by delaying neurological deterioration, an individualized combination of different therapeutic options is commonly considered in the treatment of LM from lung cancer,1,5,6 which includes molecularly targeted therapy, intrathecal chemotherapy, radiotherapy, and supportive care. These combinations have shown promising results, but not all patients benefit. Because of this, it is important to be able to identify which patients are most likely to benefit from treatment. Therefore, substantial efforts are made in order to reveal and predict the prognosis of LM across this extremely heterogeneous population. Moreover, given the expanding landscape and ongoing studies of LM-directed therapies,7,22,23 accessible and affordable prognostic or predictive markers will continue to be a growing need.
Previous studies on prognostic factors in LM have mainly included such clinicopathological variables as patient sex, smoking history, ECOG PS score, histological subtype, and molecularly targeted therapy,4,24,25 which have also been further demonstrated by the present study. Moreover, multivariate analysis in our study showed that ECOG PS score at the time of LM diagnosis is a unique independent prognostic factor among these clinicopathological factors, which is consistent with the current consensus that PS is the most important prognostic factor.1,5 In recent years, the role of WBRT in the management of LM from lung cancer has been decreasing, because most retrospective studies of patients with LM did not show a survival benefit,1,2,5 which is also supported by our study (median OS in WBRT vs non-WBRT group: 16 vs 10 months, P=0.103). Now it is generally accepted that WBRT may be indicated in rigorously selected patients with extensive nodular lesions or symptomatic linear meningeal lesions in the presence of concomitant BM. In the present study, methotrexate was of the first choice for the administration of intrathecal chemotherapy (66 of 68, 97.06%). Intrathecal chemotherapy did not show OS benefit compared to no intrathecal chemotherapy (median OS 13.5 vs 10 months, P=0.815). Recently, the Depo-Sein trial (NCT01645839) explored the role of systemic therapy plus intrathecal liposomal cytarabine in patients with newly diagnosed LM from breast cancer, and showed that the addition of intrathecal chemotherapy improved LM-related PFS (3.8 months vs 2.2 months, P=0.04) in comparison with systemic therapy alone. However, the difference in median OS was not significant between the two groups (7.3 months vs 4.0 months, P=0.51).26,27 Not surprisingly, improved outcomes in patients with molecularly targeted therapy were found in comparison to without (median OS 15 vs 8 months, P=0.022). In patients with specific actionable genetic alterations, there is considerable evidence that molecularly targeted therapies are effective either alone or in combination with other strategies in the management of LM as well as BM from lung cancer,3,28–30 especially in the era of new generations of tyrosine-kinase inhibitors with greater central nervous system efficacy. This field is rapidly evolving, and its emerging role involving different combination regimens in the management of LM needs to better studied in prospective clinical trials.
As a hallmark of cancer, systemic immunoinflammation perturbation induced by tumor burden has been extensively explored in clinical and preclinical scenarios,8–10,31,32 and it is considered a potent stimulator of cancer development and progression. Therefore, significant interest in the development of predictive biomarkers leveraging systemic immunoinflammation status has developed. This drove us to depict the systemic immunoinflammation landscape of LM from lung cancer in the present study using baseline NLR, PLR, SII and LMR levels at the time of LM diagnosis and further explore the relationship between these biomarkers and LM-patient survival.
Our study provides evidence that all the four systemic immunoinflammation biomarkers are significantly correlated with prognosis in LM from lung cancer. Moreover, NLR is an independent predictor of survival for LM from lung cancer. Our study further combined NLR with ECOG PS score to predict survival. Our findings are consistent with previous reports addressing NLR as an independent predictor of survival in the context of solid tumors,16,33 especially BM and LM. For example, Zhang et al found pretreatment NLR >3.3 inversely predicted local control, distant control, and OS in patients with BM undergoing gamma knife radiosurgery.34 Another study on patients with BM who underwent neurosurgical resection showed that median OS in those with preoperative NLR >5 was only 5 months in comparison with 15 months in patients with NLR ≤5.35 Similarly, posttreatment NLR >6 after stereotactic radiosurgery in patients with BM was associated with worse 1- and 2-year OS (59.9% vs 72.9% and 24.6% vs 43.8%, respectively).36 Recently, Hong et al found baseline NLR <2.43 was associated with better OS in LM patients.16 To date, the optimal dichotomous cutoff values of NLR to predict survival in patients with several cancers remains unknown, and ranged from 2.18 to 7.5 according to previous studies.33,37,38 In addition, NLR can be used to aid in the evaluation of optimal systemic therapy in patients with cancer, especially in advanced stages.39,40 However, this should be assessed with caution when simply using NLR to guide treatment decisions at the individual patient level. Since biomarkers based on CBC are commonly accessible and feasible in the clinic, these biomarkers could easily be integrated into daily clinical practice if ultimately shown to be predictive of outcome.
It should be noted that there are some limitations in the present study. There are several inevitable biases resulting from retrospective design. For example, a bias induced by selection procedures for decision of specific treatment strategies in this cohort cannot be excluded. Therefore, analysis of outcomes according to baseline NLR in a randomized controlled trial setting may be able to clarify this issue, and further prospective validation accounting for the best thresholds for NLR in this population of LM from lung cancer is warranted. On the other hand, our study indicates that the baseline NLR level in peripheral blood is associated with OS. However, the mechanisms underlying this correlation and the subsequent biological function of this correlation are unknown and were not explored in the present study. Further studies have been carried out in our institution to investigate the characterization of the biological mechanism, which may help in fully understanding and exploiting the value of these parameters. In addition, the present study included LM from SCLC with only three patients for final analysis. Considering the small sample and its difference from other types of lung cancer, further trials focusing on LM from SCLC alone with more samples may be convincing.
Conclusion
The findings of the present study suggest that both baseline NLR and PS scores at the time of LM diagnosis are helpful and available prognostic biomarkers for patients with LM from lung cancer. Further prospective validation with more samples and in the context of multiple clinical settings will be of great benefit for amplification of our findings.
Acknowledgments
This work was supported by grants from the CAMS Innovation Fund for Medical Sciences (2022-I2M-C&T-B-064, 2021-I2M-1-012) and Beijing Xisike Clinical Oncology Research Foundation (Y-QL202101-0094).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Le Rhun E, Weller M, Brandsma D, et al. EANO-ESMO clinical practice guidelines for diagnosis, treatment and follow-up of patients with leptomeningeal metastasis from solid tumours. Ann Oncol. 2017;28(suppl_4):iv84–iv99. doi:10.1093/annonc/mdx221
2. Cheng H, Perez-Soler R. Leptomeningeal metastases in non-small-cell lung cancer. Lancet Oncol. 2018;19(1):e43–e55. doi:10.1016/S1470-2045(17)30689-7
3. Suh JH, Kotecha R, Chao ST, Ahluwalia MS, Sahgal A, Chang EL. Current approaches to the management of brain metastases. Nat Rev Clin Oncol. 2020;17(5):279–299. doi:10.1038/s41571-019-0320-3
4. Sperduto PW, Yang TJ, Beal K, et al. Estimating survival in patients with lung cancer and brain metastases: an update of the graded prognostic assessment for lung cancer using molecular markers (Lung-molGPA). JAMA Oncol. 2017;3(6):827–831. doi:10.1001/jamaoncol.2016.3834
5. Le Rhun E, Preusser M, van den Bent M, Andratschke N, Weller M. How we treat patients with leptomeningeal metastases. ESMO Open. 2019;4(Suppl 2):e000507. doi:10.1136/esmoopen-2019-000507
6. Alexander M, Lin E, Cheng H. Leptomeningeal metastases in non-small cell lung cancer: optimal systemic management in NSCLC with and without driver mutations. Curr Treat Options Oncol. 2020;21(9):72. doi:10.1007/s11864-020-00759-3
7. Ozcan G, Singh M, Vredenburgh JJ. Leptomeningeal metastasis from non-small cell lung cancer and current landscape of treatments. Clin Cancer Res. 2022;29:11–29.
8. Hiam-Galvez KJ, Allen BM, Spitzer MH. Systemic immunity in cancer. Nat Rev Cancer. 2021;21(6):345–359. doi:10.1038/s41568-021-00347-z
9. Nost TH, Alcala K, Urbarova I, et al. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur J Epidemiol. 2021;36(8):841–848. doi:10.1007/s10654-021-00752-6
10. Thorsson V, Gibbs DL, Brown SD, et al. The immune landscape of cancer. Immunity. 2018;48(4):812–830 e814. doi:10.1016/j.immuni.2018.03.023
11. Prinz M, Priller J. The role of peripheral immune cells in the CNS in steady state and disease. Nat Neurosci. 2017;20(2):136–144. doi:10.1038/nn.4475
12. Ferrucci PF, Ascierto PA, Pigozzo J, et al. Baseline neutrophils and derived neutrophil-to-lymphocyte ratio: prognostic relevance in metastatic melanoma patients receiving ipilimumab. Ann Oncol. 2016;27(4):732–738. doi:10.1093/annonc/mdw016
13. Capone M, Giannarelli D, Mallardo D, et al. Baseline neutrophil-to-lymphocyte ratio (NLR) and derived NLR could predict overall survival in patients with advanced melanoma treated with nivolumab. J Immunother Cancer. 2018;6(1):74. doi:10.1186/s40425-018-0383-1
14. Li Q, Lin Z, Hong Y, et al. Brain parenchymal and leptomeningeal metastasis in non-small cell lung cancer. Sci Rep. 2022;12(1):22372. doi:10.1038/s41598-022-26131-z
15. Vavala T, Menis J. Editorial: brain and leptomeningeal metastases in lung cancer. Front Oncol. 2022;12:1115126. doi:10.3389/fonc.2022.1115126
16. Hong Y, Duan P, He L, et al. Systematic immunological level determined the prognosis of leptomeningeal metastasis in lung cancer. Cancer Manag Res. 2022;14:1153–1164. doi:10.2147/CMAR.S347323
17. Cai HQ, Liu AS, Zhang MJ, et al. Identifying predictive gene expression and signature related to temozolomide sensitivity of glioblastomas. Front Oncol. 2020;10:669. doi:10.3389/fonc.2020.00669
18. Yuan Q, Wang SQ, Zhang GT, et al. Highly expressed of SERPINA3 indicated poor prognosis and involved in immune suppression in glioma. Immun Inflamm Dis. 2021;9(4):1618–1630. doi:10.1002/iid3.515
19. Jiang BY, Li YS, Guo WB, et al. Detection of driver and resistance mutations in leptomeningeal metastases of NSCLC by next-generation sequencing of cerebrospinal fluid circulating tumor cells. Clin Cancer Res. 2017;23(18):5480–5488. doi:10.1158/1078-0432.CCR-17-0047
20. Hida T, Nokihara H, Kondo M, et al. Alectinib versus crizotinib in patients with ALK-positive non-small-cell lung cancer (J-ALEX): an open-label, randomised Phase 3 trial. Lancet. 2017;390(10089):29–39. doi:10.1016/S0140-6736(17)30565-2
21. Nanjo S, Hata A, Okuda C, et al. Standard-dose osimertinib for refractory leptomeningeal metastases in T790M-positive EGFR-mutant non-small cell lung cancer. Br J Cancer. 2018;118(1):32–37. doi:10.1038/bjc.2017.394
22. Hendriks LEL, Bootsma G, Mourlanette J, et al. Survival of patients with non-small cell lung cancer having leptomeningeal metastases treated with immune checkpoint inhibitors. Eur J Cancer. 2019;116:182–189. doi:10.1016/j.ejca.2019.05.019
23. Naidoo J, Schreck KC, Fu W, et al. Pembrolizumab for patients with leptomeningeal metastasis from solid tumors: efficacy, safety, and cerebrospinal fluid biomarkers. J Immunother Cancer. 2021;9(8):e002473. doi:10.1136/jitc-2021-002473
24. Waki F, Ando M, Takashima A, et al. Prognostic factors and clinical outcomes in patients with leptomeningeal metastasis from solid tumors. J Neurooncol. 2009;93(2):205–212. doi:10.1007/s11060-008-9758-3
25. Yan W, Jing W, An N, et al. The clinical characteristic and prognostic factors of leptomeningeal metastasis in patients with non-small-cell lung cancer-a retrospective study from one single cancer institute. Cancer Med. 2019;8(6):2769–2776. doi:10.1002/cam4.2156
26. Le Rhun E, Wallet J, Mailliez A, et al. Intrathecal liposomal cytarabine plus systemic therapy versus systemic chemotherapy alone for newly diagnosed leptomeningeal metastasis from breast cancer. Neuro Oncol. 2020;22(4):524–538. doi:10.1093/neuonc/noz201
27. Palmisciano P, Watanabe G, Conching A, Ogasawara C, Vojnic M, D’Amico RS. Intrathecal therapy for the management of leptomeningeal metastatic disease: a scoping review of the current literature and ongoing clinical trials. J Neurooncol. 2022;160(1):79–100. doi:10.1007/s11060-022-04118-0
28. Valiente M, Ahluwalia MS, Boire A, et al. The evolving landscape of brain metastasis. Trends Cancer. 2018;4(3):176–196. doi:10.1016/j.trecan.2018.01.003
29. Boire A, Brastianos PK, Garzia L, Valiente M. Brain metastasis. Nat Rev Cancer. 2020;20(1):4–11. doi:10.1038/s41568-019-0220-y
30. Soffietti R, Ahluwalia M, Lin N, Ruda R. Management of brain metastases according to molecular subtypes. Nat Rev Neurol. 2020;16(10):557–574. doi:10.1038/s41582-020-0391-x
31. Gonzalez H, Hagerling C, Werb Z. Roles of the immune system in cancer: from tumor initiation to metastatic progression. Genes Dev. 2018;32(19–20):1267–1284. doi:10.1101/gad.314617.118
32. Shaked Y. The pro-tumorigenic host response to cancer therapies. Nat Rev Cancer. 2019;19(12):667–685. doi:10.1038/s41568-019-0209-6
33. Lin YJ, Wei KC, Chen PY, Lim M, Hwang TL. Roles of neutrophils in glioma and brain metastases. Front Immunol. 2021;12:701383. doi:10.3389/fimmu.2021.701383
34. Zhang L, Hu Y, Chen W, Tian Y, Xie Y, Chen J. Pre-stereotactic radiosurgery neutrophil-to-lymphocyte ratio is a predictor of the prognosis for brain metastases. J Neurooncol. 2020;147(3):691–700. doi:10.1007/s11060-020-03477-w
35. Mitsuya K, Nakasu Y, Kurakane T, Hayashi N, Harada H, Nozaki K. Elevated preoperative neutrophil-to-lymphocyte ratio as a predictor of worse survival after resection in patients with brain metastasis. J Neurosurg. 2017;127(2):433–437. doi:10.3171/2016.8.JNS16899
36. Chowdhary M, Switchenko JM, Press RH, et al. Post-treatment neutrophil-to-lymphocyte ratio predicts for overall survival in brain metastases treated with stereotactic radiosurgery. J Neurooncol. 2018;139(3):689–697. doi:10.1007/s11060-018-2914-5
37. Mason M, Maurice C, McNamara MG, et al. Neutrophil-lymphocyte ratio dynamics during concurrent chemo-radiotherapy for glioblastoma is an independent predictor for overall survival. J Neurooncol. 2017;132(3):463–471. doi:10.1007/s11060-017-2395-y
38. Shaverdian N, Veruttipong D, Wang J, Schaue D, Kupelian P, Lee P. Pretreatment immune parameters predict for overall survival and toxicity in early-stage non-small-cell lung cancer patients treated with stereotactic body radiation therapy. Clin Lung Cancer. 2016;17(1):39–46. doi:10.1016/j.cllc.2015.07.007
39. Chua W, Charles KA, Baracos VE, Clarke SJ. Neutrophil/lymphocyte ratio predicts chemotherapy outcomes in patients with advanced colorectal cancer. Br J Cancer. 2011;104(8):1288–1295. doi:10.1038/bjc.2011.100
40. Lalani AA, Xie W, Martini DJ, et al. Change in Neutrophil-to-lymphocyte ratio (NLR) in response to immune checkpoint blockade for metastatic renal cell carcinoma. J Immunother Cancer. 2018;6(1):5. doi:10.1186/s40425-018-0315-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.