")
Back to Journals » OncoTargets and Therapy » Volume 10
Role of postmastectomy radiotherapy in early-stage (T1–2N0–1M0) triple-negative breast cancer: a systematic review
Received 4 October 2016
Accepted for publication 11 January 2017
Published 6 April 2017 Volume 2017:10 Pages 2009—2016
DOI https://doi.org/10.2147/OTT.S123803
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Fengxia Chen,1 Feifei Pu2
1Department of Medical Oncology, General Hospital of The Yangtze River Shipping, 2Department of Orthopedics, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
Abstract: Triple-negative breast cancer (TNBC), which represents 15%–20% of all breast cancers, is defined by the absence of estrogen receptor (ER) and progesterone receptor (PR) and overexpression of human epidermal growth factor receptor 2 (HER2). Owing to the absence of specific therapeutic targets and its aggressive biologic characteristics, TNBC patients often experience a high risk of disease progression and poor overall survival. Furthermore, TNBC exhibits an early pattern of recurrence with a peak recurrence risk at 2–3 years after surgery. Currently, chemotherapy continues to be the mainstay in TNBC patients; however, such treatment leaves them associated with a high rate of local and systemic relapses even in early-stage (T1–2N0–1M0). Therefore, in early-stage disease, greater emphasis is placed on locoregional treatments, based on radiation therapy (RT) after surgery, to reduce local and systemic relapses. However, there are no specific treatment guidelines for early-stage (T1–2N0–1M0) TNBC patients. In this review, we discuss the type of surgery received and the relevant adverse clinicopathologic factors and underlying BRCA1 mutation status regarding the influence of tailing postmastectomy radiotherapy (PMRT). In addition, we assess the role of PMRT in early-stage (T1–2N0–1M0) TNBC patients.
Keywords: triple-negative breast cancer, postmastectomy radiotherapy, early stage, review
Introduction
Triple-negative breast cancer (TNBC) is a highly heterogeneous disease that is defined by a lack of expression of estrogen receptor (ER) and progesterone receptor (PR) and overexpression of human epidermal growth factor receptor 2 (HER2). This subgroup accounts for 15%–20% of all breast cancers, and is associated with patients of younger age, black race and BRCA1 mutation carriers.1–5 Because of its aggressive biologic characteristics and lack of effective targeted agents, patients diagnosed with TNBC typically experience a more aggressive clinical course with a high risk of early relapse, disease progression and a poor prognosis.1,2,6,7 Currently, there are no specific clinical guidelines for treating TNBC, making it a clinical challenge for optimal patient management.
For patients with early-stage TNBC, surgery can merely remove detectable macroscopic tumor, but some microscopic tumor foci might still remain in the locoregional tissue (ie, chest wall or regional lymph nodes) that could, if untreated, lead to recurrence and breast cancer mortality.8 Owing to the paucity of therapeutic targets, women with TNBC do not benefit from endocrine therapy or targeted agents, and systematic chemotherapy continues to be the mainstay in TNBC patients.9 Particularly for the neoadjuvant chemotherapy, it is reported that TNBC patients with pathologic complete response (pCR) after neoadjuvant chemotherapy have an improved prognosis compared to those without pCR.5 The absence of therapeutic options emphasizes the urgent need to optimize the locoregional management of TNBC patients and reduce their risk of locoregional recurrence (LRR) and distant metastasis (DM).10,11 Therefore, postmastectomy radiotherapy (PMRT) is an important strategy for the local management of TNBC patients.12 Contemporary guidelines and international expert consensus recommend PMRT for patients who have high disease burden, defined as locally advanced (tumors >5 cm in the greatest dimension) and extensive axillary lymph node (ALN) involvement (more than three positive ALNs).13–19 Currently, the controversy is focused on whether patients with tumors ≤5 cm and zero to three positive ALNs should receive and benefit from PMRT.20–24 This controversy is related to the difference in the reported LRR risks in the absence of radiotherapy among these patients.25 Hence, there is insufficient evidence to make firm recommendations of PMRT for this subgroup.
It is generally considered that PMRT in early-stage breast cancer patients has a small absolute magnitude of benefit compared with patients who have advanced disease because their baseline LRR rate is relatively low.23,24 However, in 2014, a systematic review and meta-analysis, which was published in Lancet by Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), showed that PMRT had no significant effect on LRR, overall recurrence or breast cancer mortality in patients with no positive nodes. Yet for patients with one to three positive nodes, PMRT reduced LRR, overall recurrence and breast cancer mortality.8
It is noteworthy that the arguments described earlier solely incorporate tumor (T) size and lymph node (N) status regardless of the heterogeneous molecular subtype of breast cancer. Since 2000, when breast cancer subtype was first defined,26 it has been widely used clinically to predict the prognosis and decide systemic treatment strategies. Multiple retrospective studies indicated that TNBC has consistently been a predictive factor for worse biological behavior and prognosis including those who are in this early-stage (T1–2N0–1M0).27–31 A large sample meta-analysis of 12,592 breast cancer patients indicated that the LRR rate following breast-conserving surgery (BCS) and mastectomy (M) was significantly higher in TNBC patients (13.5% and 12.9%, respectively) compared to that in non-TNBC patients.32 This observation is consistent with previous reports that the TNBC subtype of breast cancer is an aggressive form of tumor associated with increased metastatic potential and decreased overall survival (OS).2,33 A high postmastectomy LRR in the early-stage TNBC group seems to highlight the need for adjuvant radiotherapy. TNBC is a subtype that represents a challenge to many current guidelines and consensus in breast cancer management. Accordingly, in the era of precision medicine, it is necessary to reevaluate the role of PMRT in early-stage TNBC.
In this review, we aim to assess the effect of PMRT in patients with early-stage (T1–2N0–1M0) TNBC and discuss the type of surgery received and the relevant adverse clinicopathologic factors regarding the influence of tailing PMRT in this subgroup based on the current evidence of evidence-based medicine and through deeper interpretation of classic literature.
Methods
We conducted a systematic literature search of PubMed, EMBASE, Web of Science and Google Scholar in English literature in order to identify relevant articles from January 2000 to September 2016. The year 2000 was chosen as a cutoff, as it was the year when molecular subtypes of breast cancer were first defined.26 To maximize the inclusion of eligible articles, the following keywords were used in combination: triple-negative breast cancer or TNBC, adjuvant radiotherapy or postoperative/postmastectomy radiotherapy, BCS/breast-conserving therapy (BCT), and M/modified radical mastectomy (MRM). Additional studies were sought from the references of all the retrieved articles; only studies describing related information were included.
Inclusion/exclusion criteria of literature
The studies were included if they satisfied the following criteria:
- the papers should be published after January 2000;
- the article should contain molecular subtypes of breast cancer;
- the article should provide information on early-stage TNBC (T1–2N0–1M0);
- the papers had to provide the size of the samples, surgical approach, postoperative radiotherapy and survival estimates.
The studies were excluded if one of the following criteria existed:
- studies that contained overlapping data;
- not TNBC;
- not offering the outcomes assessed or surgical type or molecular subtype or other essential information;
- if more than one study from the same group occurred, only the most recent or complete study was included.
Discussion
Assessment of the surgical approach on the effect of tailing PMRT
Breast conservation therapy versus M
In contemporary clinical practice, two major surgical approaches including BCS, which is currently adopted in small cT1 and some cT2 breast cancers, and M, which is often applied in larger tumors (T≥4 cm) and multifocal/multicentric tumors, are widely used in early-stage TNBC patients.13,14 Currently, the strategy of locoregional management in early-stage TNBC involves surgical excision of breast tumor mass by M or BCS with radiotherapy BCT: BCS and adjuvant radiation or without radiotherapy. Owing to high proliferation rate and increased aggressiveness compared with other subtypes, TNBC patients constantly deem that M is superior to BCS, which leads to a more aggressive locoregional surgical approach. Accordingly, this sparked the enthusiasm to challenge the general longstanding principle in early-stage TNBC.
A retrospective study of a single center by Abdulkarim et al showed higher LRR rates in patients with T1–2N0 TNBC treated with M only, compared with those treated with BCT; the five-year LRR-free survival was 90% and 96%, respectively. There was no significant difference in the OS between these groups.34 Moreover, findings from a meta-analysis showed that the ipsilateral locoregional recurrence (ILRR) rate of patients undergoing M was 2.5-fold as much as that of patients undergoing BCT in a subgroup analysis for stages I–II TNBC. Hence, the meta-analysis concluded that BCT could benefit patients with early-stage TNBC compared to M. Furthermore, the favorable outcome from BCT might be because of the contribution from the postoperative radiotherapy.35
However, Zumsteg et al36 who investigated a retrospective study of 646 T1–2N0 TNBC patients in the USA reported no significant difference in LRR between BCT and M. A large multicenter retrospective study of 775 TNBC patients with T1–2N0–1M0 tumors found that survival of patients treated with M only was not significantly different compared to patients receiving BCT.37 Ly et al38 retrospectively reviewed patients with T1–2N0–1M0 invasive TNBC treated from 2004 to 2010 in their single cancer center and concluded that there was no statistically significant difference between M and BCT with respect to cumulative incidence of LRR. Finally, a recently published population-based study, which enrolled 37,207 primary, invasive, stage T1–2N0–1M0 breast cancer patients, indicated that BCT showed significantly improved 10-year OS and relative survival compared with M in early breast cancer (Table 1).39
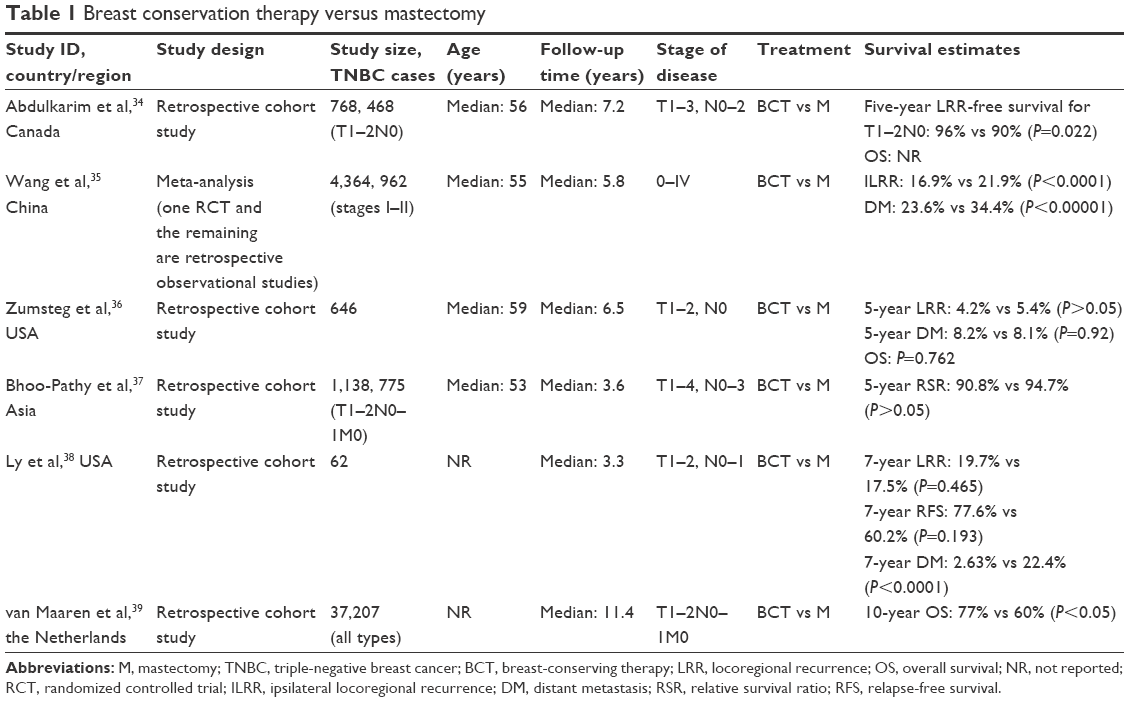 | Table 1 Breast conservation therapy versus mastectomy |
Taken together, based on the pooled data, breast conservation therapy, which routinely incorporates radiation, can be considered a candidate for early-stage TNBC patients as it is at least equivalent to M with respect to local control and OS in early TNBC. One possible explanation is that patients who underwent BCT were older at diagnosis, were less likely to have lymphovascular invasion (LVI) and had smaller and lower grade tumors than patients undergoing M. Hence, how to identify this specific subgroup that is suitable for BCT is critical and challenging for clinicians.
M versus M + PMRT
Although current international consensuses and guidelines do not recommend the routine use of PMRT for patients with stage T1–2N0–1M0 disease, there is contradictory data with respect to this inherently heterogeneous subtype. In a retrospective study conducted by Chen et al40 from a single institution, it was shown that PMRT was associated with a longer disease-free survival (DFS) time than M only in the intermediate-risk group (stages T1–2N1) with a median follow-up of 65 months. In another study by Kong and Hong,41 it was reported that PMRT might be beneficial in a subgroup analysis of T1–2N1 patients of TNBC subtype. Similarly, Gabos et al42 deemed that PMRT is important in decreasing LRR after modified radical M, particularly in women with T1–2N0 TNBC subtype. Likewise in a phase 3 trial from China, which included 681 patients with triple-negative stages I–II breast cancer, all patients treated with M plus chemotherapy and then randomly assigned to receive PMRT or no radiation showed that 5-year relapse-free survival and OS were significantly higher with the addition of PMRT compared with no radiation.43 Jagsi et al44 and Truong et al45 also concluded that PMRT is needed after MRM in T1–2N0 TNBC patients. However, a study from China by Shen et al revealed exactly the opposite result, that in patients of the TNBC group with T1–2N1, PMRT showed significantly worse locoregional control with LRR 34.0% in the PMRT group compared with 19.2% in the no-PMRT group. Shen et al46 explained that ~95% of TNBC patients received chemotherapy; hence, the benefit of PMRT in patients may decrease due to the progress of adjuvant therapy (Table 2).
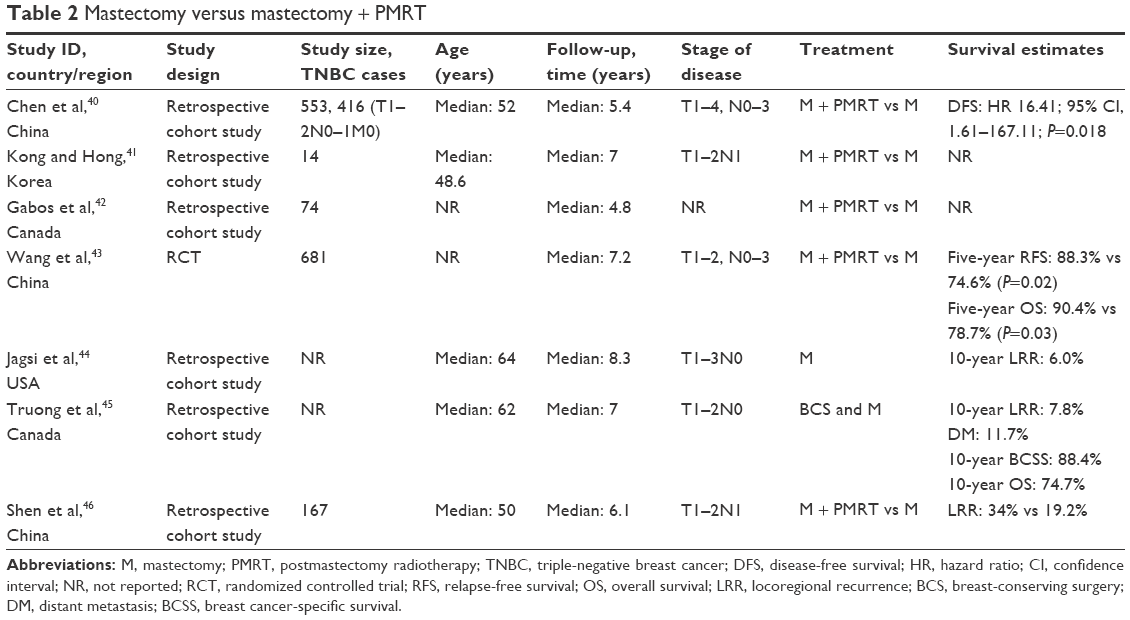 | Table 2 Mastectomy versus mastectomy + PMRT |
Association with clinicopathologic factors
In the assessment of adjuvant radiotherapy for early-stage TNBC, there are related clinicopathologic factors that need to be addressed. In clinical practice, the most common risk factors include age, LVI, grade, the number of axillary lymph nodes removed, the number of positive lymph nodes, margin status, pCR, menopausal status and neoadjuvant/adjuvant chemotherapy. In a retrospective study, Chen et al demonstrated that younger age (<50 years), the presence of LVI, grade 3 tumor, and three positive ALNs are associated with an increased risk of LRR among patients with pT1–2N0-N1 TNBC who undergo MRM and receive chemotherapy without PMRT through multivariate analysis. Furthermore, patients with two or more of the risk factors involved had a significantly higher 5-year LRR rate of >25%.47 Similarly, in another retrospective study, the authors’ results supported that PMRT showed significantly decreased LRR in T1–2N1 patients with age <40 years, LVI, two and three positive lymph nodes and ratio of positive LNs >25%.46 Trovo et al48 demonstrated that LVI, grade 3 disease, ER-negative tumors and premenopausal status were significant risk factors for LRR, and patients who had three or more risk factors with a 5-year LRR rate of >20% were recommended for PMRT in stage I–II breast cancer patients. Truong et al49 reported that patients aged <45 years with >25% positive axillary nodes and patients aged ≥45 years with >25% positive axillary nodes, medial tumor location and ER negative were recommended for PMRT in a retrospective analysis including 821 T1–2N1 breast cancer patients. In addition, Houvenaeghel et al50 showed that axillary lymph node involvement is a key prognostic feature for early TNBC when isolated tumor cells were identified in lymph nodes. pN0 cases had longer DFS than pN0(i+)/pN1mic51 (isolated tumor cell [<0.2 mm; pN0(i+], micrometastases [<2 mm; pN1mic]).50 What is more, in a subgroup analysis from an article, the authors showed that in patients with a low-risk disease (stages T1–2N0) without PMRT, LVI was the only strong predictor of both LRR and disease recurrence (DR), which causes a significantly higher 5-year LRR rate and 5-year DR rate than those without LVI (Table 3).40 Taken together, when counseling TNBC patients with stage T1–2N0–1M0 to receive PMRT, we should still consider the high-risk factors listed earlier. In addition, when making radiotherapy strategies, we should also consider the radiotherapy field; the National Comprehensive Cancer Network (NCCN) guidelines of version 1 2016 recommend that for BCS and negative axillary nodes, radiation is needed to whole breast with or without boost to tumor bed or take consideration of partial breast irradiation in selected patients; for one to three positive axillary nodes, regardless of BCS or M, strongly consider radiotherapy to chest wall, infraclavicular region, supraclavicular area, internal mammary nodes and any part of axillary bed at risk; for M and negative axillary nodes, when tumor ≤5 cm and margin ≥1 mm, no radiotherapy is needed and when tumor ≤5 cm and margin <1 mm, consider radiotherapy to chest wall.14
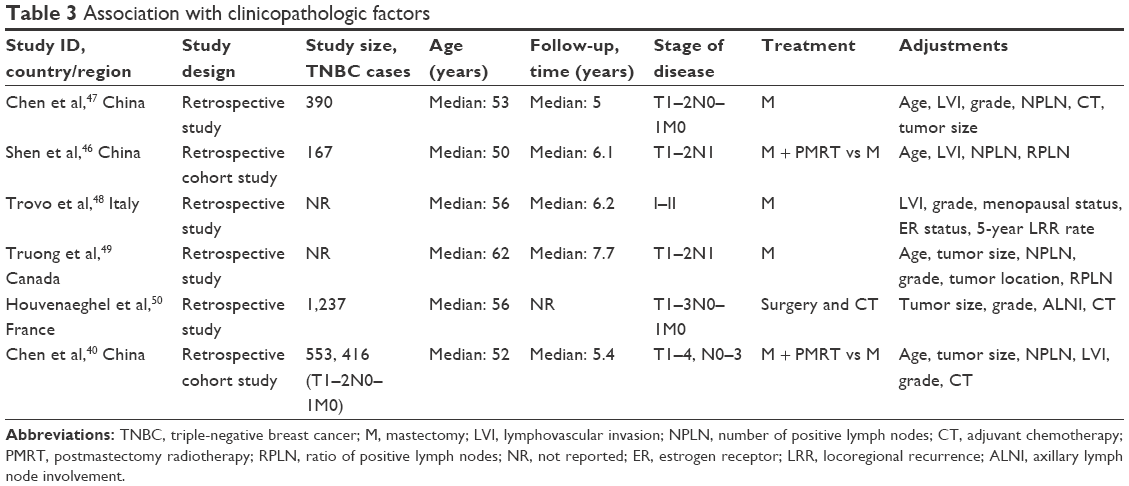 | Table 3 Association with clinicopathologic factors |
Association with BRCA1 mutations
It is reported that ~60%–80% of BRCA1-mutated breast tumors display a TNBC phenotype.3,52 Furthermore, additional studies have identified that this subtype has high proliferative indices, high grade, lymphocytic infiltrate, pushing margins, a greater propensity for visceral than bone or lymphatic metastases and an elevated risk of ipsilateral or contralateral recurrence.53,54 In aggregate, patients with BRCA1-mutated TNBC present a poor prognosis. Based on the risk factors associated with BRCA1-mutated TNBC, BRCA mutation status is crucial in making decisions for locoregional management. The present NCCN guidelines for genetic screening recommend that patients diagnosed with TNBC younger than 60 years should be considered for genetic testing irrespective of family history.55 BRCA1-mutated TNBC patients are typically characterized by a high rate of DNA aberrations and defective DNA repair process. The exact mechanism is that normal BRCA1 plays a critical role in the recognition of DNA damage and repair of double-strand breaks by homologous recombination, nonhomologous end-joining. BRCA1 mutation results in defects in DNA repair and in turn increases the toxicity of DNA damage, which ultimately enhances radiosensitivity and chemosensitivity to specific chemotherapeutic drugs (ie, platinum-based drugs).56,57 However, whether TNBC is radiosensitive or radioresistant is conflicting because the mechanism of preclinical data is different.8,58–60
Conclusion
TNBC is a group of clinically heterogeneous disease. Six subtypes of TNBC are defined according to gene-expression profiles, which are basal-like 1, basal-like 2, immunomodulatory, mesenchymal, mesenchymal stem like and luminal androgen receptor.61 Furthermore, TNBC is a more aggressive disease with a high grade, high proliferative potential, increased risk of disease progression and poorer OS, compared with other subtypes of breast cancer.62,63 It is reported that TNBC exhibits an early pattern of recurrence with a peak recurrence risk at 2–3 years after surgery.2 Chemotherapy continues to be the mainstay of systemic medical treatment for TNBC patients. The feature of predisposition to early relapse of TNBC highlights the importance of locoregional treatment. Like other subtypes, PMRT is recommended to TNBC patients after surgery, with tumors >5 cm or more than three positive nodes involved, according to guidelines and consensuses.12–18 Although it has clinically aggressive characteristics, there are currently no specific guidelines for TNBC. Until now, the role of PMRT in early-stage (T1–2N0–1M0) TNBC patients has not been clearly clarified. There are controversies about whether adjuvant PMRT is needed. The present data discussed earlier are not sufficient enough to recommend either M or M followed by PMRT for patients with stage T1–2N0–1M0 TNBC because no single locoregional management approach has consistently been demonstrated better than another.
Therefore, for patients with early-stage TNBC, some researchers think that PMRT is a helping hand that can eliminate subclinical tumor foci remaining in locoregional tissue to reduce the risk of LRR and DM, but others consider it overtreatment, which not only increases the financial burden of patients but also brings a series of complications, including arm edema and cardiopulmonary radiation damage. However, whether PMRT is beneficial or harmful for early-stage TNBC has no accurate answer. The ultimate purpose of PMRT is to improve the survival of local control and patients, but short-term and long-term adverse effects should not be forgotten. In contemporary clinical practice, we should evaluate the benefits and toxicity of PMRT comprehensively to optimize the individualized treatment strategy according to individual disease specifics with respect to T1–2N0–1M0 TNBC patients. Owing to the limitations of previous prospective or retrospective study, systematic review and meta-analysis, prospective multicenter randomized controlled phase 3 studies are needed in regard to the PMRT for T1–2N0–1M0 TNBC patients. While age, histological grade, LVI, the number of axillary lymph nodes removed, the number of positive lymph nodes, surgical margin status, menopausal status, BRCA1 status, pCR, menopausal status and neoadjuvant/adjuvant treatment should be pre-stratified, to further clarify the subgroup which can benefit from PMRT and the radiation field which is more important and safer for PMRT to bring on better locoregional control and longer survival for patients.
There are certain limitations of this review. The most important of all, owing to the absence of prospective clinical trials, the majority of the pertinent data are from retrospective studies. Hence, it is conceivable that clinicopathologic characteristics of patients involved, systematic treatment such as chemotherapy regimen, radiation field and radiation dose intensity may have varied between different studies. Second, the classification criteria for TNBC through immunohistochemistry and fluorescence in situ hybridization are both varied with the progress of medicine. Third, the duration of follow-up is varied between studies. Therefore, more prospective studies are needed to identify the specific high-risk TNBC patients with T1–2N0–1M0 to determine which subgroup can truly derive the greatest survival benefit from PMRT.
Disclosure
The authors report no conflicts of interest in this work.
References
Carey LA, Perou CM, Livasy CA, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006;295(21):2492–2502. | ||
Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13(15 pt 1):4429–4434. | ||
Lakhani SR, Van De Vijver MJ, Jacquemier J, et al. The pathology of familial breast cancer: predictive value of immunohistochemical markers estrogen receptor, progesterone receptor, HER-2, and p53 in patients with mutations in BRCA1 and BRCA2. J Clin Oncol. 2002;20(9):2310–2318. | ||
Moran MS, Yang Q, Harris LN, Jones B, Tuck DP, Haffty BG. Long-term outcomes and clinicopathologic differences of African-American versus white patients treated with breast conservation therapy for early-stage breast cancer. Cancer. 2008;113(9):2565–2574. | ||
Bonsang-Kitzis H, Chaltier L, Belin L, et al. Beyond axillary lymph node metastasis, BMI and menopausal status are prognostic determinants for triple-negative breast cancer treated by neoadjuvant chemotherapy. PLoS One. 2015;10(12):e0144359. | ||
Nielsen TO, Hsu FD, Jensen K, et al. Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin Cancer Res. 2004;10(16):5367–5374. | ||
Sotiriou C, Neo SY, McShane LM, et al. Breast cancer classification and prognosis based on gene expression profiles from a population-based study. Proc Natl Acad Sci U S A. 2003;100(18):10393–10398. | ||
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Darby S, McGale P, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378(9804):1707–1716. | ||
Eiermann W, Vallis KA. Locoregional treatments for triple-negative breast cancer. Ann Oncol. 2012;23(suppl 6):vi30–vi34. | ||
Bryan BB, Schnitt SJ, Collins LC. Ductal carcinoma in situ with basal-like phenotype: a possible precursor to invasive basal-like breast cancer. Mod Pathol. 2006;19:617–621. | ||
Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363(20):1938–1948. | ||
Pignol JP, Rakovitch E, Olivotto IA. Is breast conservation therapy superior to mastectomy for women with triple-negative breast cancers? J Clin Oncol. 2011;29(21):2841–2843. | ||
Aebi S, Davidson T, Gruber G, Cardoso F. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2011;22(suppl 6):vi12–vi24. | ||
National Comprehensive Cancer Network (NCCN). Clinical Practice Guidelines in Oncology: Breast Cancer v2. 2016. Available from: https://www.nccn.org/patients/guidelines/stage_i_ii_breast/index.html. Accessed July 15, 2016. | ||
Coates AS, Winer EP, Goldhirsch A, et al. Tailoring therapies – improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann Oncol. 2015;26(8):1533–1546. | ||
Recht A, Edge SB, Solin LJ, et al; American Society of Clinical Oncology. Postmastectomy radiotherapy: clinical practice guidelines of the American Society of Clinical Oncology. J Clin Oncol. 2001;19(5): 1539–1569. | ||
Taylor ME, Haffty BG, Rabinovitch R, et al. ACR appropriateness criteria on postmastectomy radiotherapy expert panel on radiation oncology-breast. Int J Radiat Oncol Biol Phys. 2009;73(4):997–1002. | ||
Harnett A, Smallwood J, Titshall V, Champion A. Diagnosis and treatment of early breast cancer, including locally advanced disease – summary of NICE guidance. BMJ. 2009;338:b438. | ||
Sautter-Bihl ML, Souchon R, Budach W, et al. DEGRO practical guidelines for radiotherapy of breast cancer II. Postmastectomy radiotherapy, irradiation of regional lymphatics, and treatment of locally advanced disease. Strahlenther Onkol. 2008;184(7):347–353. | ||
EBCTCG (Early Breast Cancer Trialists’ Collaborative Group), McGale P, Taylor C, et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8,135 women in 22 randomised trials. Lancet. 2014;383(9935):2127–2135. | ||
Sauer R, Schulz KD, Hellriegel KP. Strahlentherapie nach Mastektomie – Interdisziplinärer Konsensus beendet Kontroverse [Radiation therapy after mastectomy – interdisciplinary consensus puts and end to a controversy. German Society of Senology]. Strahlenther Onkol. 2001;177(1):1–9. | ||
Hojris I, Overgaard M, Christensen JJ, Overgaard J. Morbidity and mortality of ischaemic heart disease in high-risk breast-cancer patients after adjuvant postmastectomy systemic treatment with or without radiotherapy: analysis of DBCG 82b and 82c randomised trials. Radiotherapy Committee of the Danish Breast Cancer Cooperative Group. Lancet. 1999;354(9188):1425–1430. | ||
Favourable and unfavourable effects on long-term survival of radiotherapy for early breast cancer: an overview of the randomised trials. Early Breast Cancer Trialists’ Collaborative Group. Lancet. 2000;355(9217):1757–1770. | ||
Overgaard M, Nielsen HM, Overgaard J. Is the benefit of postmastectomy irradiation limited to patients with four or more positive nodes, as recommended in international consensus reports? A subgroup analysis of the DBCG 82 b&c randomized trials. Radiother Oncol. 2007;82(3):247–253. | ||
Li Y, Moran MS, Huo Q, Yang Q, Haffty BG. Post-mastectomy radiotherapy for breast cancer patients with t1–t2 and 1–3 positive lymph nodes: a meta-analysis. PLoS One. 2013;8(12):e81765. | ||
Perou CM, Sørlie T, Eisen MB, et al. Molecular portraits of human breast tumours. Nature. 2000;406(6797):747–752. | ||
Rakha EA, Reis-Filho JS, Ellis IO. Basal-like breast cancer: a critical review. J Clin Oncol. 2008;26(15):2568–2581. | ||
Weigelt B, Baehner FL, Reis-Filho JS. The contribution of gene expression profiling to breast cancer classification, prognostication and prediction: a retrospective of the last decade. J Pathol. 2010;220(2):263–280. | ||
Sotiriou C, Pusztai L. Gene-expression signatures in breast cancer. N Engl J Med. 2009;360(8):790–800. | ||
Kreike B, van Kouwenhove M, Horlings H, et al. Gene expression profiling and histopathological characterization of triple-negative/basal-like breast carcinomas. Breast Cancer Res. 2007;9(5):R65. | ||
Reis-Filho JS, Tutt AN. Triple negative tumours: a critical review. Histopathology. 2008;52(1):108–118. | ||
Lowery AJ, Kell MR, Glynn RW, Kerin MJ, Sweeney KJ. Locoregional recurrence after breast cancer surgery: a systematic review by receptor phenotype. Breast Cancer Res Treat. 2012;133(3):831–841. | ||
Billar JA, Dueck AC, Stucky CC, et al. Triple-negative breast cancers: unique clinical presentations and outcomes. Ann Surg Oncol. 2010;17(suppl 3):384–390. | ||
Abdulkarim BS, Cuartero J, Hanson J, Deschênes J, Lesniak D, Sabri S. Increased risk of locoregional recurrence for women with T1–2N0 triple-negative breast cancer treated with modified radical mastectomy without adjuvant radiation therapy compared with breast-conserving therapy. J Clin Oncol. 2011;29(21):2852–2858. | ||
Wang J, Xie X, Wang X, et al. Locoregional and distant recurrences after breast conserving therapy in patients with triple-negative breast cancer: a meta-analysis. Surg Oncol. 2013;22(4):247–255. | ||
Zumsteg ZS, Morrow M, Arnold B, et al. Breast-conserving therapy achieves locoregional outcomes comparable to mastectomy in women with T1–2N0 triple-negative breast cancer. Ann Surg Oncol. 2013;20(11):3469–3476. | ||
Bhoo-Pathy N, Verkooijen HM, Wong FY, et al. Prognostic role of adjuvant radiotherapy in triple-negative breast cancer: a historical cohort study. Int J Cancer. 2015;137(10):2504–2512. | ||
Ly B, Kwon D, Reis I, et al. Comparison of clinical outcomes in early stage triple negative breast cancer treated with mastectomy versus breast conserving therapy. Int J Radiat Oncol Biol Phys. 2012;84:S258–S259. | ||
van Maaren MC, de Munck L, de Bock GH, et al. 10 year survival after breast-conserving surgery plus radiotherapy compared with mastectomy in early breast cancer in the Netherlands: a population-based study. Lancet Oncol. 2016;17(8):1158–1170. | ||
Chen X, Yu X, Chen J, et al. Radiotherapy can improve the disease-free survival rate in triple-negative breast cancer patients with T1–T2 disease and one to three positive lymph nodes after mastectomy. Oncologist. 2013;18(2):141–147. | ||
Kong M, Hong SE. Which patients might benefit from postmastectomy radiotherapy in breast cancer patients with t1–2 tumor and 1–3 axillary lymph nodes metastasis? Cancer Res Treat. 2013;45(2):103–111. | ||
Gabos Z, Thoms J, Ghosh S, et al. The association between biological subtype and locoregional recurrence in newly diagnosed breast cancer. Breast Cancer Res Treat. 2010;124(1):187–194. | ||
Wang J, Shi M, Ling R, et al. Adjuvant chemotherapy and radiotherapy in triple-negative breast carcinoma: a prospective randomized controlled multi-center trial. Radiother Oncol. 2011;100(2):200–204. | ||
Jagsi R, Raad RA, Goldberg S, et al. Locoregional recurrence rates and prognostic factors for failure in node-negative patients treated with mastectomy: implications for postmastectomy radiation. Int J Radiat Oncol Biol Phys. 2005;62(4):1035–1039. | ||
Truong PT, Lesperance M, Culhaci A, Kader HA, Speers CH, Olivotto IA. Patient subsets with T1–T2, node-negative breast cancer at high locoregional recurrence risk after mastectomy. Int J Radiat Oncol Biol Phys. 2005;62(1):175–182. | ||
Shen H, Zhao L, Wang L, et al. Postmastectomy radiotherapy benefit in Chinese breast cancer patients with T1–T2 tumor and 1–3 positive axillary lymph nodes by molecular subtypes: an analysis of 1369 cases. Tumour Biol. 2016;37(5):6465–6475. | ||
Chen X, Yu X, Chen J, et al. Analysis in early stage triple-negative breast cancer treated with mastectomy without adjuvant radiotherapy: patterns of failure and prognostic factors. Cancer. 2013;119(13):2366–2374. | ||
Trovo M, Durofil E, Polesel J, et al. Locoregional failure in early-stage breast cancer patients treated with radical mastectomy and adjuvant systemic therapy: which patients benefit from postmastectomy irradiation? Int J Radiat Oncol Biol Phys. 2012;83(2):e153–e157. | ||
Truong PT, Olivotto IA, Kader HA, Panades M, Speers CH, Berthelet E. Selecting breast cancer patients with T1–T2 tumors and one to three positive axillary nodes at high postmastectomy locoregional recurrence risk for adjuvant radiotherapy. Int J Radiat Oncol Biol Phys. 2005;61(5): 1337–1347. | ||
Houvenaeghel G, Sabatier R, Reyal F, et al. Axillary lymph node micrometastases decrease triple-negative early breast cancer survival. Br J Cancer. 2016;115(9):1024–1031. | ||
Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editor. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010. | ||
Atchley DP, Albarracin CT, Lopez A, et al. Clinical and pathologic characteristics of patients with BRCA-positive and BRCA-negative breast cancer. J Clin Oncol. 2008;26(26):4282–4288. | ||
Yehiely F, Moyano JV, Evans JR, Nielsen TO, Cryns VL. Deconstructing the molecular portrait of basal-like breast cancer. Trends Mol Med. 2006;12(11):537–544. | ||
Pierce LJ, Phillips KA, Griffith KA, et al. Local therapy in BRCA1 and BRCA2 mutation carriers with operable breast cancer: comparison of breast conservation and mastectomy. Breast Cancer Res Treat. 2010;121(2):389–398. | ||
Robson ME, Bradbury AR, Arun B, et al. American Society of Clinical Oncology Policy Statement Update: genetic and genomic testing for cancer susceptibility. J Clin Oncol. 2015;33(31):3660–3667. | ||
Scully R, Livingston DM. In search of the tumour-suppressor functions of BRCA1 and BRCA2. Nature. 2000;408(6811):429–432. | ||
Moran MS. Radiation therapy in the locoregional treatment of triple-negative breast cancer. Lancet Oncol. 2015;16(3):e113–e122. | ||
Kyndi M, Sørensen FB, Knudsen H, et al; Danish Breast Cancer Cooperative Group. Estrogen receptor, progesterone receptor, HER-2, and response to postmastectomy radiotherapy in high-risk breast cancer: the Danish Breast Cancer Cooperative Group. J Clin Oncol. 2008;26(9):1419–1426. | ||
Baeyens A, Thierens H, Claes K, Poppe B, de Ridder L, Vral A. Chromosomal radiosensitivity in BRCA1 and BRCA2 mutation carriers. Int J Radiat Biol. 2004;80(10):745–756. | ||
Trenz K, Lugowski S, Jahrsdörfer U, Jainta S, Vogel W, Speit G. Enhanced sensitivity of peripheral blood lymphocytes from women carrying a BRCA1 mutation towards the mutagenic effects of various cytostatics. Mutat Res. 2003;544(2–3):279–288. | ||
Lehmann BD, Bauer JA, Chen X, et al. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Invest. 2011;121(7):2750–2767. | ||
Nishimura R, Arima N. Is triple negative a prognostic factor in breast cancer? Breast Cancer. 2008;15(4):303–308. | ||
Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer. 2007;109(9):1721–1728. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.