")
Back to Journals » Cancer Management and Research » Volume 15
Role of PD-1 Inhibitors in the Treatment of Esophagogastric Adenocarcinoma: Patient Selection and Reported Outcomes
Authors Epistola R , Sperandio R , Wainberg Z, Iqbal S, Chao J
Received 1 October 2022
Accepted for publication 9 February 2023
Published 18 March 2023 Volume 2023:15 Pages 265—275
DOI https://doi.org/10.2147/CMAR.S341468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Raisa Epistola,1 Rubens Sperandio,2 Zev Wainberg,3 Syma Iqbal,4 Joseph Chao5
1Department of Internal Medicine, Division of Hematology and Medical Oncology, Harbor UCLA Medical Center, Torrance, CA, USA; 2Centro de Oncologia e Hematologia Einstein Família Dayan-Daycoval, Hospital Israelita Albert Einstein, São Paulo, Brazil; 3Jonsson Comprehensive Cancer Center, University of California Los Angeles, Los Angeles, CA, USA; 4Norris Comprehensive Cancer Center, University of Southern California, Los Angeles, CA, USA; 5Department of Medical Oncology and Therapeutics Research, City of Hope Comprehensive Cancer Center, Duarte, CA, USA
Correspondence: Raisa Epistola; Joseph Chao, Tel +1-310-501-9393 ; +1-626-218-2123, Fax +1 424-306-6646 ; +1 626-301-8233, Email [email protected]; [email protected]
Abstract: Esophagogastric cancers are aggressive malignancies, with poor prognosis despite current standard-of-care therapies. PD-1 inhibitors are a newer class of antitumor agents with the potential to improve outcomes among appropriately selected patients. This review provides an overview of the key trials that have guided the use of PD-1 and PD-L1 inhibitors in the refractory and first-line settings. We highlight recent studies investigating the role of genomic classification in predicting therapeutic activity of PD-1 inhibitors. In addition, there is a discussion of the use of different scoring systems and criteria to determine PD-L1 positivity, the impact on the therapeutic use of immune checkpoint inhibition with anti-PD-1 agents, and the controversies in current methods of PD-L1 testing and their implications in patient selection for anti-PD-1 therapy.
Keywords: immunotherapy, immune checkpoint inhibition, PD-L1, gastric cancer, gastroesophageal junction cancer
Introduction
Though prevalence and mortality have been declining over the last 50 years, stomach cancer remains the fifth–most frequently diagnosed and fourth-leading cause of cancer-related death globally, accounting for over 1 million new cases and 769,000 deaths globally in 2020.1 Esophageal cancer follows closely behind, ranking seventh in terms of incidence and sixth in terms of mortality, accounting for 604,000 new cases and 544,000 deaths worldwide.1 Adenocarcinoma accounts for nearly 90% of gastric cancers and approximately two-thirds of all esophageal cancer cases, with rates of gastroesophageal junction adenocarcinoma specifically rising in prevalence alongside increased rates of risk factors, such as obesity and gastroesophageal reflux disease, in industrialized countries.2–5
As patients often present later in their disease course, prognosis is poor even with treatment, and there is a global overall 5-year survival rate of 20%–30% among all patients and 5%–10% 5-year survival rate among those presenting with advanced disease.3 Given the need for more efficacious therapies, PD-1 inhibitors have emerged as a new tool in our treatment armamentarium for gastric and gastroesophageal junction (GEJ) cancer. This review article covers current applications of PD-1 inhibitors in the treatment of gastric and GEJ adenocarcinoma. Additionally, we discuss the development and use of biomarkers to predict outcomes and subsequently aid in the selection of patient populations who will benefit from immune checkpoint inhibition with anti-PD-1 agents.
Trials Studying Single-Agent PD-1 and PD-L1 Inhibitors in the Refractory-Line Setting
Immune checkpoint inhibitors were initially studied as single agents among patients with refractory metastatic gastric cancers. PD-L1-expression positivity has guided both trial and now clinical practice for the eligibility for these agents. Importantly, there are several methods of defining PD-L1 expression. Combined positive score (CPS) is the first of several scoring criteria for PD-L1 expression, calculated as the number of PD-L1-positive cells (tumor cells, macrophages, lymphocytes) divided by the total number of tumor cells and multiplied by 100. Other scoring criteria include tumor-proportion score (TPS), and immune cell (IC) scoring, which describe PD-L1 expression as the percentage of tumor and immune cells positively staining for PD-L1, respectively, as visualized in Figure 1.7
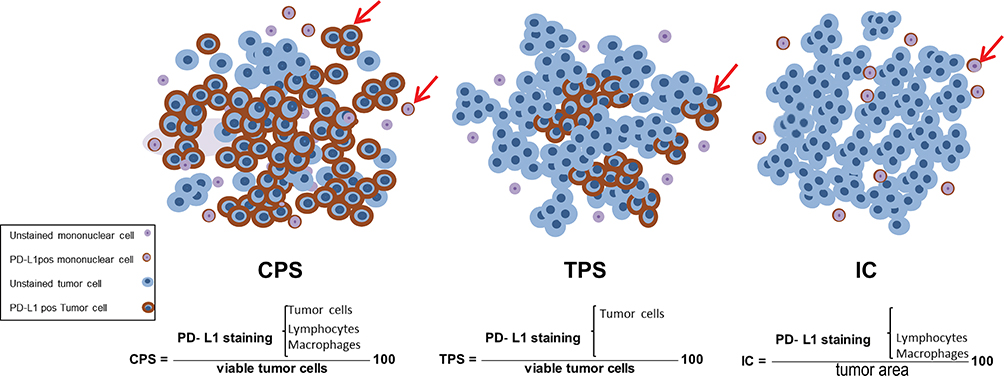 |
Figure 1 Combined positive score (CPS) of PD-L1 expression defined by (total number of stained tumor cells and immune cells divided by number of all viable tumor cells) × 100; tumor proportion score (TPS) of PD-L1 expression defined by percentage of stained tumor cells; immune cell (IC) PDL1 expression defined by percentage of stained immune cells. Arrows indicate PD-L1-positive cells accounted for in each scoring criterion’s calculations to describe PD-L1 expression. Reprinted from Sajjadi E, Venetis K, Scatena C, Fusco N. Biomarkers for precision immunotherapy in the metastatic setting: hope or reality? Ecancermedicalscience. 2020;14. Creative Commons.7 |
The first of these trials was the KEYNOTE-059 study, which evaluated the efficacy of the anti-PD-1 monoclonal antibody pembrolizumab.6 It was a single arm, three-cohort phase II, open-label study investigating the efficacy of pembrolizumab monotherapy among patients with gastric or gastroesophageal cancer, with its largest cohort, cohort 1, consisting of patients treated in the third line and beyond setting (n=259). All patients had progressed after two or more lines of chemotherapy, including a fluoropyrimidine–platinum doublet and HER2 inhibitor, if indicated. Primary outcomes were safety/tolerability and objective response rate (ORR) in all patients and those with PD-L1-positive tumors. Here, PD-L1 expression was assessed with an immunohistochemistry (IHC) assay using the 22C3 staining antibody clone, and tumors were considered positive for CPS >1. For all patients, the ORR was 11.6% (95% CI 8.0%–16.1%, 30 of 259 patients), with complete response in 2.3% (95% CI 0.9%–5.0%, six of 259 patients) and median duration of response (DOR) of 8.4 months (range 1.6–17.3 months). Among patients with PD-L1 CPS ≥1 tumors, ORR was 15.5% (95% CI 10.1%–22.4%, 23 of 148 patients) with median DOR of 16.3 months (range 1.6–17.3 months). For those with PD-L1 CPS <1, the ORR was 6.4% (95% CI 2.6%–12.8%, seven of 109 patients) with median DOR of 6.9 months (range 2.4–7.0 months). As demonstrated by the higher ORR and median DOR among patients with CPS >1, PD-L1 IHC using CPS was able to partially discriminate the likelihood of response to single-agent pembrolizumab. However, it should be noted that in their review of the KEYNOTE-059 cohort 1 data, the FDA found decreased assay sensitivity by the PD-L1 CPS ≥1 cutoff when older archival tissue specimens were used to test for PD-L1 status.8 This finding brought up concerns for possible inclusion of patients with false-negative PD-L1 tumor specimens included in the PD-L1-negative subgroup, casting uncertainty whether the reported ORR for this subgroup reliably characterized the treatment effect among PD-L1-negative patients.
A study that validated the overall survival (OS) benefit of PD-1 inhibitors was ATTRACTION-02, a double-blind, randomized placebo controlled phase III trial investigating the use of the single-agent PD-1 inhibitor nivolumab among Asian patients with unresectable, advanced, or recurrent gastric and GEJ cancer in the third-line and beyond setting.9 Patients were randomized in a 2:1 ratio, with 330 receiving nivolumab and 163 receiving placebo/best supportive care. The primary end point was OS, with patients in the nivolumab group showing a significant survival benefit, where median OS in the nivolumab group was 5.26 months versus 4.14 months in the placebo group (HR 0.63, p<0.0001). Notably, tissue collection for PD-L1 tumor expression was not required for enrollment in this study, though PD-L1 IHC was retrospectively studied as a biomarker using the 28–8 antibody clone for patients with available tumor samples (n=192, 39% of enrolled patients), with PD-L1 positivity defined as TPS >1% (Figure 1). An exploratory analysis of available PD-L1 tumor-expression data did not show any differences in treatment response between PD-L1-positive and PD-L1-negative groups defined by TPS. For patients with PD-L1-positive (TPS ≥1%) tumors, median OS was 5.22 months with nivolumab versus 3.83 months in the placebo group (HR 0.51, 95% CI 0.21–1.25). Among patients with PD-L1-negative (TPS <1%) tumors, median OS was 6.05 months in the nivolumab arm and 4.19 months in the placebo arm (HR 0.72, 95% CI 0.49–1.05). This exploratory analysis of treatment response by PD-L1 TPS status highlighted its shortcomings as a predictive biomarker, given both biomarker-positive and -negative subgroups seemingly derived benefit from immune checkpoint inhibition. In addition, later studies have shown that PD-L1 positivity defined by enumeration of only tumor cells with a TPS cutoff of 1%, as was done in this study, typically finds a lower percentage of PD-L1-positive gastric/GEJ adenocarcinomas compared to the CPS methodology at an equivalent 1% cutoff, suggesting that PD-L1 appears to have higher rates of expression in immune cells in this disease.10
JAVELIN Gastric 300 was another study investigating the benefits of anti-PD-L1 treatment in the third-line setting for patients with advanced gastric and GEJ cancer.11 This phase III, randomized, open-label trial compared the anti-PD-L1 agent avelumab to an active comparator — physician’s choice of chemotherapy — as opposed to placebo, and had a primary end point of OS. In the intention to treat (ITT) population, 185 patients were enrolled in the experimental avelumab arm and 196 in the chemotherapy arm. Patients in the chemotherapy arm could receive paclitaxel, irinotecan, or best supportive care without chemotherapy. In this arm, 174 patients received either irinotecan or paclitaxel, with only three receiving best supportive care. This study did not meet its primary end point, reporting a median OS of 4.6 months in the avelumab arm and 5.0 months in the chemotherapy arm (HR 1.1, p=0.81). The ITT analysis did not select patients for any biomarker, though a retrospective OS analysis of PD-L1 expression quantified solely by tumor-cell enumeration using a 73–10 staining antibody clone did not distinguish patients with either a TPS of 1% or 0% as deriving any survival benefit from being randomized to avelumab. Specifically, median OS in the PD-L1 TPS >1% subgroup was 4.0 months with avelumab vs 4.5 months with chemotherapy, and median OS in the PD-L1 TPS <1% subgroup was 4.6 months with avelumab and 5.3 months with chemotherapy.
In light of KEYNOTE-059 demonstrating pembrolizumab’s antitumor activity and the positive results of anti-PD-1 treatment with nivolumab from ATTRACTION-02 in the third-line, the KEYNOTE-061 investigators sought to assess the efficacy of pembrolizumab in the second-line setting. KEYNOTE-061 was a phase III, randomized, open-label trial comparing pembrolizumab to paclitaxel among patients with advanced or metastatic gastric and GEJ cancers.12 All patients had to provide a tumor sample for PD-L1 assessment, which was conducted using the 22C3 assay to calculate CPS. Of the 592 patients randomly assigned, 395 had PD-L1 CPS >1. These patients were evenly distributed between the pembrolizumab (n=196) and chemotherapy (n=199) groups. Despite a majority of patients having at least some degree of PD-L1 expression, this study did not meet its primary OS end point. Among patients with CPS >1, pembrolizumab did not significantly prolong OS versus paclitaxel chemotherapy (HR 0.82, 95% CI 0.66–1.03; p=0.0421). Median OS was 9.1 (95% CI 6.2–10.7) months for the pembrolizumab arm and 8.3 (95% CI 7.6–9.0) months for the paclitaxel arm. However, post hoc analysis did suggest greater pembrolizumab treatment effect for patients with PD-L1 CPS >10, with median OS of 10.4 months among those treated with pembrolizumab versus 8.0 months among those treated with paclitaxel (HR 0.64, 95% CI 0.41–1.02).
The more recent KEYNOTE-181 was a phase III, open-label study that randomized patients with advanced/metastatic esophageal squamous cell carcinoma (SCC) and Siewert I GEJ adenocarcinomas to pembrolizumab or investigator’s choice of chemotherapy (paclitaxel, docetaxel, or irinotecan) in the second-line setting.13 All patients provided new or archival tissue samples for PD-L1 testing using the 22C3 IHC assay. PD-L1 positivity was defined by a cutoff of CPS >10. The study tested three primary end points: OS in patients with PD-L1 CPS >10, OS in patients with SCC, and OS in all patients. The ITT population comprised 314 patients assigned to pembrolizumab and 314 assigned to chemotherapy. In the PD-L1-positive subgroup, 222 patients received pembrolizumab and 115 chemotherapy. This trial was considered positive for patients with PD-L1 CPS >10, demonstrating significantly longer median OS in the pembrolizumab group versus chemotherapy (median OS 9.3 versus 6.7 months, respectively, HR, 0.69; p=0.0074). Among patients with SCC, OS was longer in the pembrolizumab group (8.2 versus 7.1 months), but did not meet the threshold for significance (HR 0.78, p=0.0095). Though this study did not meet the primary end point of OS among all patients with SCC, it did show clinically meaningful improvements in 12-month survival rate in the pembrolizumab group compared to chemotherapy (38.4% versus 24.9%). In a post hoc analysis, the greatest benefit of pembrolizumab among patients with SCC was in those whose tumors were CPS >10. In this subgroup, median OS was 10.3 months among those who received pembrolizumab versus 6.7 months among those who received chemotherapy (HR 0.64, 95% CI 0.46–0.90).
Trials Studying Single-Agent PD-1 Inhibitors or Chemotherapy Combinations in the First-Line Setting
Following the mixed success of immune checkpoint inhibition in the refractory setting, KEYNOTE-062 was one of the first phase III randomized controlled trials investigating the efficacy of PD-1 inhibition in the first-line setting among patients with advanced, unresectable gastric and GEJ adenocarcinomas.14 This trial had three arms comparing pembrolizumab monotherapy (n=256), pembrolizumab plus chemotherapy (n=257), and placebo plus chemotherapy (n=250). The chemotherapy comparator was cisplatin plus fluorouracil or capecitabine. All patients provided newly obtained or archival tumor samples for PD-L1 testing, and tumors needed to be PD-L1 CPS >1 to be eligible for enrollment. Primary end points were OS and progression-free survival (PFS) in patients with PD-L1 CPS >1 and CPS >10 tumors tested hierarchically. This study met its noninferiority end point for OS with pembrolizumab monotherapy versus chemotherapy for patients with CPS >1 (HR, 0.91, 99.2% CI 0.69–1.18, noninferiority margin 1.2), though pembrolizumab was not found to be superior to chemotherapy in this patient population (HR 0.91, 95% CI 0.71–1.10). Reported median OS was 10.6 months with pembrolizumab versus 11.1 months with chemotherapy. For patients with CPS >10, median OS was 17.4 months with pembrolizumab versus 10.8 months with chemotherapy, suggesting a clinically meaningful benefit in this subgroup. However, this difference was not formally tested as per the study’s prespecified statistical analysis plan, given that the initial hierarchical testing for the PDL1 CPS >1 population did not achieve its primary end point of pembrolizumab demonstrating improved OS. Notably, PFS was inferior with pembrolizumab compared to chemotherapy in both groups, with median PFS of 2.0 months versus 6.4 months in the CPS >1 population and 2.9 months versus 6.1 months in the CPS >10 population. Such inferior progression-free outcomes bring into question the clinical applicability of these trial results. Additionally, the OS end points for pembrolizumab plus chemotherapy versus chemotherapy did not meet the criteria for superiority for either the CPS >1 or CPS >10 group (median OS 12.5 months versus 11.1 months, p=0.05 and 12.3 months versus 10.8 months, p=0.16, respectively).
CheckMate-649 was another three-arm, phase III trial investigating the efficacy of PD-1 inhibition as first-line treatment for patients with unresectable HER2-negative gastric, GEJ, and esophageal adenocarcinoma.15 This open-label phase III trial compared nivolumab plus chemotherapy (fluorouracil, leucovorin, and oxaliplatin or capecitabine, and oxaliplatin), nivolumab plus ipilimumab (a CTLA4 immune checkpoint inhibitor), and chemotherapy alone. All patients provided fresh or archival tumor samples to evaluate PD-L1 expression, which was determined using the 28–8 pharmDx IHC assay to calculate TPS and CPS. Patients were not selected for PD-L1 expression; however, TPS ≥1% versus 0% was a stratification factor during randomization. The protocol was subsequently amended to use CPS to define its co–primary endpoint population. The study met its primary endpoint of OS for nivolumab plus chemotherapy versus chemotherapy alone for patients with PD-L1 CPS ≥5, with median OS 14.4 months in the combination group compared to 11.1 months in the chemotherapy-only group. This also translated into a 29% relative reduction in the risk of death in the combination group (HR 0.71, p<0.0001). The secondary primary endpoint of PFS was also met in patients with CPS >5, with median PFS of 7.7 months in the nivolumab plus chemotherapy group versus 6.0 months and a 32% relative reduction in risk of progression or death compared to chemotherapy alone (HR 0.68, p<0.0001). Hierarchically tested secondary endpoints of OS in patients with PD-L1 CPS >1 (14.0 versus 11.3 months, HR 0.77; p<0.0001) and in all-comers (13.8 versus 11.6 months, HR 0.80, p=0.0002) were also met. Notably, this study had a high prevalence of patients with CPS >5 (60% of all randomized patients), who would have been included in the all-comer analysis. Given these results, the US Food and Drug administration approved combination nivolumab with fluoropyrimidine and platinum chemotherapy for all patients with advanced or metastatic gastric, GEJ, and esophageal carcinomas.
Similar to CheckMate-649, ATTRACTION-4 was a phase III double-blind, placebo-controlled trial investigating nivolumab plus chemotherapy (n=362) versus chemotherapy alone (n=362) in the first-line setting for patients with HER2-negative, unresectable advanced, or recurrent gastric or GEJ adenocarcinoma.16 Chemotherapy was oxaliplatin plus S1 or oral capecitabine. This study exclusively enrolled patients from Japan, South Korea, and Taiwan, and patients were not selected for PD-L1 expression. Primary end points were PFS and OS among all patients. While the PFS end point was met for the nivolumab-plus-chemotherapy group (10.45 months versus 8.34 months, HR 0.68; p=0.0007), it did not meet its OS end point, reporting median OS of 17.45 months in the nivolumab-plus-chemotherapy arm versus 17.15 months in the chemotherapy-only arm (p=0.25). Though the study did not select for PD-L1 expression, all patients were required to provide tumor tissue samples for PD-L1 expression, with positivity defined as TPS >1 for stratification during randomization. Notably, a majority of patients in both arms were not PD-L1-positive by TPS in this negative study (n=304 [84%] and n=306 [85%] in the nivolumab and placebo arms, respectively). Though smaller in scale than CheckMate 649, the negative results of the ATTRACTION-4 trial call into question if adding nivolumab to first-line therapy will be of benefit if not enriching for patients whose tumors exhibit higher PD-L1 expression by the CPS methodology.
KEYNOTE-590 was a phase III double-blind, placebo controlled trial comparing pembrolizumab plus chemotherapy (n=373) to chemotherapy alone (n=376) in the first-line setting among patients with locally advanced, unresectable, or metastatic HER2-negative esophageal adenocarcinoma, SCC, and Siewert type 1 GEJ adenocarcinoma.17 Though this study had separate analyses for the SCC population (which consisted of 73% of patients in both study arms), it also included endpoints for all patients with PDL1 CPS >10 and for all randomized patients, which included the 99 patients with adenocarcinoma in the pembrolizumab-plus-chemotherapy arm (n=58 esophageal cancers, n=41 GEJ cancers) and 102 patients with adenocarcinoma in the chemotherapy arm (n=52 esophageal cancers, n=50 GEJ cancers). Chemotherapy was a doublet of 5-fluorouracil and cisplatin. All patients provided newly obtained or archival tissue for PD-L1 IHC analysis, though they were not stratified by PD-L1 status during randomization. Primary end points were OS and PFS. This study met its OS end point for superiority of pembrolizumab plus chemotherapy compared to chemotherapy alone for patients with PD-L1 CPS >10 (13.5 versus 9.4 months, respectively, HR 0.62; p<0.0001) and all randomized patients (12.4 versus 9.8 months, respectively, HR 0.73; p<0.0001). PFS endpoints were also met for the PD-L1 CPS >10 (7.5 vs 5.5 months, HR 0.51; p<0.0001) and all randomized patients (6.3 vs 5.8 months, HR 0.65; p<0.0001). Among all patients with adenocarcinoma, OS (median OS 11.6 vs 9.9 months, HR 0.74) and PFS (6.3 vs 5.7 months, HR 0.65) was longer in the pembrolizumab-plus-chemotherapy group compared to chemotherapy alone, regardless of PD-L1-expression status. In particular, post hoc subgroup analysis did not show clear benefit in PD-L1 CPS <10, reporting median OS of 10.5 versus 10.6 months and median PFS of 6.2 versus 6.0 months in the pembrolizumab combination versus chemotherapy-only arms, respectively. Notably, analysis of the adenocarcinoma subgroup was limited by small numbers and not powered to assess within-subgroup differences. In an exploratory analysis of PD-L1 CPS ≥10 adenocarcinoma patients — 43 receiving pembrolizumab plus chemotherapy versus 54 who received chemotherapy alone — median OS numerically favored addition of pembrolizumab (12.1 versus 10.7 months). This difference was not statistically significant (HR 0.83, 95% CI 0.52–1.34), likely due to small numbers, but draws some parallels to the PD-L1 CPS ≥10 analysis in KEYNOTE-062 also reporting a nonsignificant trend in favor of adding pembrolizumab to first-line chemotherapy. As such, the positive OS benefit for the entire study population may have been primarily driven by the PD-L1 CPS ≥10 SCC patients. Despite this, following this study, the FDA approved pembrolizumab in the first-line setting for all patients with esophageal and GEJ adenocarcinoma, regardless of PD-L1 CPS status.
Despite FDA approval for nivolumab and pembrolizumab for use in the first-line setting in advanced gastric or esophageal adenocarcinoma, there was a lack of clear data regarding the efficacy of immune checkpoint inhibitors among patients with low PD-L1-expressing tumors within these trial populations. Therefore, Zhao et al conducted a reconstruction of unreported Kaplan–Meier plots of unreported PD-L1 CPS-expression subgroups of randomized phase III trials that compared immunotherapy alone or in combination with chemotherapy in the first-line setting among patients with metastatic gastric, GEJ, or esophageal adenocarcinoma, namely CheckMate 649 and KEYNOTE-062.18 Specifically, they aimed to clarify treatment outcomes among patients with low PD-L1-expressing tumors using a graphical reconstructive algorithm to estimate time-to-event outcomes for unreported subgroup cohorts: PD-L1 CPS 1–4 for CheckMate-649 and PD-L1 CPS 1–9 for KEYNOTE-062. This study concluded that there was no significant OS difference in the CheckMate-649 CPS 1–4 subgroup for nivolumab plus chemotherapy versus chemotherapy alone (HR 0.950, p=0.678) nor in the KEYNOTE-062 PD-L1 CPS 1–9 subgroups in either comparative analysis, specifically, pembrolizumab vs chemotherapy (HR 1.027, p=0.872) and pembrolizumab plus chemotherapy vs chemotherapy alone (HR 0.836, p=0.141). Furthermore, there was no significant difference in PFS outcomes for these subgroups in CheckMate-649 (nivolumab plus chemotherapy vs chemotherapy, HR 0.958, p=0.743) or KEYNOTE-062 (pembrolizumab plus chemotherapy vs chemotherapy, HR 0.924, p=0.510). Interestingly, they also found that patients given pembrolizumab alone were at increased risk of tumor progression compared to chemotherapy alone (HR 2.092, p<0.001) in KEYNOTE-062. These findings suggest lack of efficacy in the low PD-L1-expressing subset of patients. Acknowledging possible lack of efficacy in the low PD-L1-expressing subgroups, the National Comprehensive Cancer Network (NCCN) gave a category 1 recommendation for the addition of checkpoint inhibition with nivolumab to fluoropyrimidine and oxaliplatin chemotherapy among patients with HER2-negative gastric and esophageal adenocarcinoma with PD-L1 CPS >5 in the first-line setting and a category 2B recommendation for those lower-expressing patients with CPS <5.19 Similarly, the NCCN gave a category 1 recommendation for pembrolizumab in combination with fluoropyrimidine and platinum (oxaliplatin, cisplatin) chemotherapy for patients with esophageal and GEJ cancers with PD-L1 CPS >10 and a category 2B recommendation for those with PD-L1 CPS <10.20
Finally, JAVELIN Gastric 100 was a phase III trial investigating anti-PD-L1 maintenance with avelumab following first-line induction chemotherapy (n=249) vs continuation of chemotherapy (n=250) for patients with unresectable locally advanced or metastatic gastric and GEJ cancer.21 Induction chemotherapy included up to 12 weeks of oxaliplatin + fluoropyrimidine. The primary end point was OS after induction chemotherapy. Here, PD-L1 positivity was defined as TPS >1 on the 73–10 assay. The primary endpoint of median OS was not met among all-comers (10.4 vs 10.9 months in the avelumab versus chemotherapy groups, HR 0.91, 95% CI 0.74–1.11; p=0.1779) or among patients with PD-L1 positivity (16.2 vs 17.7 months, HR 1.13, p=0.6352). The authors suggest that given the low numbers of patients with PD-L1 positivity, OS analysis was underpowered. Indeed, there were only 30 patients in the avelumab arm versus 24 patients in the chemotherapy arm who were PD-L1-positive by TPS. A post hoc exploratory analysis of the PD-L1-positive population redefined as PD-L1 CPS >1 using the 22C3 assay suggested improved median OS in the avelumab group vs continuation of chemotherapy (14.9 vs 11.6 months, unstratified HR 0.91, 95% CI 0.74–1.11; p=0.1779), further highlighting the difference between the TPS and CPS schemata in predicting response to anti-PD-1 therapy.
Activity of PD-1 Inhibitors in Accordance with Genomic Classification
Immunotherapy has revolutionized cancer treatment. However, treatment with checkpoint inhibitors for gastric and GEJ cancers yielded an ORR ranging from 12% to 27% in early trials.22 Reliable predictive biomarkers that enable better selection of candidates for immunotherapy remain an unmet need in the management of these malignancies. Practice-guiding classifications of gastric and gastroesophageal cancers, such as the Lauren and WHO histopathological classifications have little predictability of treatment response to these agents. Only in the last decade, with increased access to molecular techniques, have unique genomic features been identified as possible actionable targets for therapy and thus predictors of treatment response. The Cancer Genome Atlas (TCGA) initiative applied multiplatform high-throughput multi-omic analyses through six molecular platforms: somatic copy-number analysis, whole-exome sequencing, DNA-methylation profiling, microRNA sequencing, and reverse-phase protein array.23 Clustering of the obtained data yielded four subgroups — Epstein–Barr virus (EBV)–positive tumors, microsatellite instability high (MSI-H), genomically stable (GS), and chromosomal instability (CIN) — allowing for a translational framework being increasingly applied to clinical practice.
Two TCGA gastric/GEJ cancer molecular categories are remarkable for their relatively impressive response to single-agent immune checkpoint inhibitors: MSI-H and EBV-positive tumors. A single-center phase II trial conducted in South Korea enrolled 61 patients with metastatic gastric cancer treated with salvage pembrolizumab in the second- and third-line setting.24 Efficacy data and pattern of response based on the four TCGA subcategories of gastric cancer were analyzed. The patients’ pretreatment tissue underwent molecular profiling through whole-exome sequencing, RNA sequencing, and EBV DNA sequencing. Almost 10% (n=6) of their study population had EBV-positive gastric cancer, while 11.5% (n=7) had MSI-H disease. Among the entire population, almost 5% (n=3) of patients achieved a complete response and 19.7% (n=12) had a partial response. All of the EBV-positive patients demonstrated a lasting partial response (100% RR). Among the MSI-H gastric cancer patients (n=7), six achieved significant response (three CRs and three PRs), with one patient refractory to treatment. This study also found that PD-L1 positivity using a CPS of 1 cutoff showed a correlation with response, with ORR 50% for patients with CPS >1 vs 0% with CPS <1 (p<0.001).
While both MSI-H tumors and EBV-positive cancers are known to show high expression of PD-L1, EBV-positive tumors were not found to have high mutational load in this study. In addition, the only MSI-H case that was refractory to pembrolizumab was further analyzed and found to exhibit spatial intratumoral heterogeneity for loss of MLH1 expression by IHC as a likely mechanism of resistance. Despite the small sample, when ORRs were cross-compared with TCGA subgroups as defined by DNA genomic alterations, ORR for EBV-positive (six of six) and MSI-H (six of seven) patients were nearly 100%. It was also noteworthy that ORRs in the other two subgroups were minimal, with ORR of 12% (n=25) and 5% (n=20), respectively, for GS and CIN.
Postulated reasons for this correlation with EBV-positivity and response to checkpoint inhibition include evidence that EBV-positive tumors demonstrate high immune cell infiltration; high expression of PD-L1/2 and other immune checkpoint pathway genes, and enrichment of IFNγ response genes, which play a role in PD-L1 expression and activation in both tumor and immune cells. It is important to note that EBV-positive and MSI-H subgroups were mutually exclusive in an analysis of the TCGA gastric cancer cohort, which included EBV-positive (n=25), MSI-H (n=80), and microsatellite stable (MSS, n= 310) subgroups.25 This study found that EBV-positive tumors had a similar mutation burden to MSS tumors (median 2.07 vs 2.06 in log10 scale, p=0.71), and significantly lower mutational burden than MSI-H tumors (median 2.07 vs 3.13, p<10−12). However, overall immune cell infiltration and expression of the T-cell marker CD8A were higher in EBV-positive vs MSI-H tumors. This study also found that EBV-positive and MSI-H tumors had a higher expression of immune checkpoint genes, including PD-1, CTLA-4, and PD-L1, than MSS tumors. Interestingly, EBV-positive tumors had a significantly higher expression of PD-1 than even MSI-H tumors. Finally, this study also showed that EBV-positive tumors showed higher lymphocytic infiltration by histology than MSS tumors (median tumor-infiltrating lymphocyte score 3 vs 2, p<0.001).
Another analysis of the TCGA cohort examined PD-L1 status and gene expression of IFNγ immune signatures among EBV-positive and -negative gastric adenocarcinomas to identify possible markers predictive of response to PD-1 targeted therapy.22 IHC analysis showed PD-L1 expression in both tumor (50%, 16 of 32 cases) and immune cells (94%, 30 of 32 cases) among patients with EBV-positive tumors. EBV-negative tumors had significantly less PD-L1 staining of tumors (10%, five of 49; p<0.001) and immune cells (39%, 19 of 49; p<0.001) than EBV-positive tumors. MSI-H gastric cancers also had significantly higher PD-L1 staining of tumor cells (33%, five of 15 vs 0 of 34; p<0.001) and immune cells (46%, seven of 15 vs 35%, 12 of 34; p<0.001) compared to EBV-negative MSS gastric cancers. Interestingly, both EBV-positive and MSI-H cancers showed a tumor-infiltrating pattern of inflammatory cells (57% in PD-L1-positive and EBV-positive cases, 43% in MSI-H cases) compared to none of the PD-L1-positive, EBV-negative, or MSS cases (p<0.001), where PD-L1-positive inflammatory cells remained at the border. A gene-set enrichment analysis search for genetic signatures found that an IFNγ-response signature was most strongly enriched in EBV-positive cancers. High IFNγ–response gene expression was seen more commonly in MSI-H gastric cancers than GS and CIN TCGA subgroups (p<0.001). Additionally, high IFNγ–response gene expression was strongly associated with PD-L1 mRNA expression among all subgroups (p<0.001).
In turn, MSI-enriched cancers are characterized by hypermutation, due to loss of mismatch repair during DNA replication, which introduces a large number of frameshift mutations and production of tumor neoantigen peptide sequences.23 A retrospective single-institution analysis (n=410) investigated the efficacy of second-line and later anti-PD-1 therapy following first-line combination fluoropyrimidine + platinum ± trastuzumab with or without second-line taxane ± ramucirumab chemotherapy among four molecular subtypes: MSI-H (n=24, 5.9%), EBV-positive (n=17, 4.1%), HER2-positive (n=56, 13.7%), and all-negative (n=313, 76.3%) advanced gastric cancers.26 There was no overlap among subtypes. Outcomes included ORR and PFS. A total of 110 patients received subsequent anti-PD-1 therapy. MSI-H patients had significantly higher ORR (58% vs 13%, p=0.001) and median PFS (13.0 vs 1.9 months, p<0.0001) compared to all-negative patients. A trend toward longer PFS with anti-PD-1 therapy was also seen among EBV-positive patients (HR 0.48, p=0.064).
This evidence shows that MSI-H and EBV-positive status are useful predictive biomarkers for immunotherapy and should be implemented as routine testing. Relevantly, while comprehensive sequencing methods are still in the process of becoming widely available, MSI may be more easily performed in standardized clinical laboratory settings via mismatch-repair protein IHC or polymerase chain-reaction sequencing of prototypical microsatellite markers. EBV status is routinely assayed with chromogenic in situ hybridization for EBV-encoded RNA using fluorescein-labeled oligonucleotide probes (EBER-ISH). There is currently consensus on testing MSI status in every patient, but EBV status is more controversial, given the lowest prevalence of this TCGA subgroup and biomarker, variability in ORRs, and association with high PD-L1 expression such that routine PD-L1 testing will likely incidentally already capture those patients with EBV-positive tumors. Indeed, current NCCN guidelines for gastric cancer recommend routine MSI and PD-L1 CPS testing without EBV status testing to determine eligibility for immune checkpoint inhibitors.19
More recently, other novel biomarkers besides the partially reliable PD-L1 expression have been investigated. The role of B cells when aggregated in tertiary lymphoid structures (TLS) alter the tumor microenvironment and modulate immune system activation through antigen presentation, cytokine release, and antibody production. Therefore, the role of tumor-infiltrating B cells, particularly those found in TLSs, both as a predictor of treatment response and as an active modulator of immune activity, is under investigation. An RNA-sequencing analysis of longitudinal tumor samples among patients with metastatic melanoma who responded to immune checkpoint inhibition showed significantly higher expression of B cell–related genes (p<0.001) than in nonresponders.27 In addition, histological analysis showed that there was a significantly higher density of CD20-positive B cells (p=0.0008) and TLSs (p=0.001) with a significantly higher ratio of TLS-to-tumor area (p=0.002) in responders than nonresponders.
Studies of tumor-immune cells and the presence of TLSs have been expanded into the gastric cancer space. An analysis of tumor-immune microenvironments for gastroesophageal adenocarcinomas among the TCGA subgroups used both genomic/transcriptomic information from the TCGA database (n=453) and a second series of patients who provided archival pretreatment samples for spatial immune characterization, such as IHC and mRNA-expression analysis (n=73).28 This study showed that 50% of cases in the GS subgroup had enrichment of intratumoral TLSs, which were not present among CIN cases. IHC analysis showed that the TLSs observed in these gastroesophageal adenocarcinomas contained CD8+ T-cell aggregates and were enriched with CD208+ dendritic cells, endothelial venules important for migration of T cells, and CD20+ B cells. The presence of TLSs in GS cancers was also associated with higher T-cell and B-cell function scores, suggesting that the presence of TLSs may also be predictive of immunotherapy response among this subset of gastroesophageal cancers. The enrichment of TLSs among GS cancers is a possible mechanism for the 12% ORR — and third-highest ORR to pembrolizumab — seen in the previously discussed South Korean phase II trial.24
Controversies in PD-L1 Testing as a Predictive Biomarker of PD-1 Benefit
PD-L1 testing in multiple subtypes of cancer has demonstrated some clinical utility; however, analytical methods vary, and its interpretation may be subject to uncertainties and controversies. Different cutoffs have been utilized; which in turn complicates standardization of testing methods. For instance, recent studies investigating the addition of PD-1 inhibitors to first-line chemotherapy in metastatic gastric cancer, such as KEYNOTE-062 and ORIENT-16, used the 22C3 assay, whereas CheckMate 649 utilized the 28–8 assay.14,15,29 It should be noted that each of these studies had differing PD-L1-positivity cutoffs for the statistical powering of efficacy end points in prespecified PD-L1-biomarker subgroups, with KEYNOTE-062 using CPS >10 and CheckMate 649 and ORIENT-16 using CPS >5. With the caveat of cross-trial comparisons, the proportion of enrolled patients with CPS ≥10 tumors determined by the 28–8 assay was 49% in CheckMate 649, concordant with the 44% reported in ORIENT-16, which used 22C3. However, both of these trials were discordant with the 37% of patients with PD-L1 CPS ≥10 tumors in KEYNOTE-062, despite this study population excluding patients who were PD-L1 CPS <1, as opposed to both CheckMate 649 and ORIENT-16 still permitting enrollment of these patients.
A single-center study in South Korea demonstrated a high level of concordance between the 22C3 and 28–8 assays on CPS 1, 10, and 50 cutoffs among gastric adenocarcinomas.30 The 28–8 assay was performed on formalin-fixed paraffin-embedded (FFPE) pathology blocks initially tested via the 22C3 assay from 55 patients with advanced gastric cancer. Concordance was high, with overall agreement between the two assays of 96.4% for both CPS 1 and 10 and 100% overall agreement with CPS 50. When CPS was categorized as a continuous variable, the 28–8 assay yielded higher scores than the 22C3 assay in 29.1% of cases, whereas the 22C3 assay yielded higher scores in only 3.6% of cases. Only a small number (37 of 55) of patients had linked clinical annotation to single-agent anti-PD-1 or anti-PD-L1 therapies, though the two assays did not differ significantly in their ability to predict immunotherapy responses, with both showing higher ORR in patients with PD-L1 CPS >1 than PD-L1 CPS <1 treated with immunotherapy (22C3 pharmDx, p=0.001; 28–8 pharmDx, p=0.002). Likewise, a single-center study of FFPE gastrectomy specimens from 226 patients in Japan noted relatively high concordance (87%) between the 22C3 and 28–8 assays, though 11% of cases scored higher for PD-L1 CPS expression using 22C3.31 There was no differentiation in prognosis between the 22C3 and 28–8 assessments. However, a single-center, cross-sectional study of 344 gastrectomy specimens, the largest data set comparing 28–8 and 22C3 assays, noted discrepancies in positivity rates at the clinically relevant PD-L1 CPS 1, 5, and 10 cutoffs.32 PD-L1 28–8 and 22C3 staining was done by immunofluorescence protocol with quantitative CPS scoring. Specifically, this study demonstrated a significantly higher proportion of PD-L1-positive samples when using the 28–8 assay versus 22C3 at cutoffs of CPS >1 (70.3% vs 49.4%, p<0.001), CPS >5 (29.1% vs 13.4%, p<0.001), and CPS >10 (13.7% vs 7.0%, p=0.004). The authors of this study concluded that caution must be exercised in considering differing PD-L1 assays to be interchangeable when selecting patients for PD-1 inhibitors.
Importantly, such factors as specimen age and tumor heterogeneity, both intra- and interlesional, may also influence CPS results. A retrospective, single-center US-based study of 189 gastroesophageal adenocarcinoma patients examined spatial and temporal heterogeneity of PD-L1 expression.33 A total of 407 tumor samples were included due to multiple/repeated biopsies, as well as a small minority of samples collected via surgical resection and fluid aspiration. CPS data were collected with the 22C3 assay. This study showed interlesional spatial heterogeneity with meaningful discordance in PD-L1 expression between primary tumors and metastatic sites at baseline biopsy. Concordance in PD-L1 expression status between primary and metastatic biopsies was only 61%, with metastatic sites having significantly lower rates of PD-L1 positivity defined by CPS >1 (concordance in only 40% of metastatic biopsies being PD-L1-positive if the primary tumor biopsy was PD-L1-positive). Temporal heterogeneity was also demonstrated, with a meaningful discordance between pre-treatment and post-treatment tumor PD-L1 expression. PD-L1 status was concordant in only 63% of pre- and post-treatment primary tumors. As a retrospective analysis, this study was limited in assessing if the observed PD-L1 heterogeneity made any impact on response to anti-PD-1 therapies, given the limited number of patients who received immune checkpoint inhibitors in this cohort.
Intrapatient tumoral genomic heterogeneity has already been widely accepted to exist and serve as a mechanism of adaptive resistance to therapy. As PD-L1 is dynamically expressed in its role as an immune checkpoint molecule and for tumors leveraging it for adaptive immune resistance, it is intuitive to anticipate both inter- and intratumoral spatial and temporal heterogeneity of its expression within the tumor immune microenvironment. A single-center study of 152 patients in China who underwent upfront resection for gastric cancer examined intratumoral (ie, intralesional) heterogeneity of PD-L1 expression to better determine the number of biopsy specimens needed to accurately reflect PD-L1 expression of whole sections.34 To simulate endoscopic sampling, six randomly selected cores from a representative FFPE block of each case were used to create tissue microarrays (TMAs) that were subsequently compared to the corresponding whole-tumor sections. PD-L1 testing was done with the 22C3 assay, with PD-L1 positivity defined as PD-L1 expression in at least 1% of tumor or immune cells. Concordance in PD-L1-expression status between the whole section and TMAs appeared to increase when more cores were represented: with one core, concordance was 60.4%, two cores 72.5%, four cores 82.2%, five cores 92.4%, and six cores 95.2%. This study highlights how increased sampling likely more accurately reflects PD-L1 expression across the whole tumor due to intralesional heterogeneity manifesting as non-uniform spatial PD-L1 expression. In addition, the percentage of cases categorized as being PD-L1-positive increased when more cores were represented, with only 38% of cases categorized as PD-L1-positive with one core versus 69% and 72% of cases when five and six cores were represented, respectively. These findings raise caveats of false-negative reporting of PD-L1-expression status with endoscopic undersampling, and the authors propose testing of five biopsies as optimal for determination of PD-L1 positivity.
Conclusion
In summary, immune checkpoint inhibition with anti-PD-1 agents has been shown to be efficacious among appropriately selected patients with gastric and GEJ adenocarcinomas. Though determination of PD-L1-expression status described by CPS is currently recommended for predicting treatment response and thus assessing eligibility for anti-PD-1 agents, such methodology for patient selection is not without controversy. These concerns include differing definitions for PD-L1-positivity cutoffs by CPS, unclear consensus on the interchangeability of the various IHC assays used to assess PD-L1 positivity in gastric adenocarcinomas, and whether spatiotemporal heterogeneity of PD-L1 expression impacts response to anti-PD-1 therapies. Future directions to optimize patient selection may include composite testing strategies to include not only PD-L1 status but also multiple immune biomarkers through novel platforms, such as multiplex IHC and spatial transcriptomics. To circumvent the challenges inherent to gastric and GEJ adenocarcinoma spatiotemporal molecular heterogeneity, multiparametric biomarker assessment combining primary and metastatic PD-L1 status, as well as molecular subtyping35 may better predict response and optimize the identification of patients for immune checkpoint inhibition.
Acknowledgments
The authors would like to acknowledge the important work of other investigators who were unable to be cited due to space constraints.
Disclosure
J Chao has received consultant/advisory fees from Lilly Oncology, AstraZeneca, Merck, Daiichi Sankyo, Macrogenics, Amgen, Ono Pharmaceutical, Bristol Myers Squibb, Astellas, Turning Point Therapeutics, Silverback Therapeutics, Novartis, Coherus Biosciences, Geneos, Roche, and Foundation Medicine, research funding (institutional) from Merck and Brooklyn Immunotherapeutics, and serves on the speaker’s bureau for Merck and Bristol Myers Squibb. Z Wainberg has received consultant/advisory fees from Lilly Oncology, AstraZeneca, Merck, Daiichi Sankyo, Macrogenics, Amgen, Bristol Myers Squibb, Astellas, Ipsen, Arcus, Novartis, Roche, and Pfizer and received research funding (institutional) from Arcus, Plexxikon, Novartis and Merck. S Iqbal has received consultant/advisory fees from AstraZeneca, BeiGene, Daiichi Sankyo, BMS, and Merck. The other authors have no conflicts of interest to declare for this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. doi:10.3322/caac.21708
3. Casamayor M, Morlock R, Maeda H, Anjani J. Targeted literature review of the global burden of gastric cancer. Ecancermedicalscience. 2018;12:1–22. doi:10.3332/ecancer.2018.883
4. Thrift AP, El-Serag HB. Burden of gastric cancer. Clin Gastroenterol Hepatol. 2020;18(3):534–542. doi:10.1016/j.cgh.2019.07.045
5. Arnold M, Laversanne M, Brown LM, Devesa SS, Bray F. Predicting the future burden of esophageal cancer by histological subtype: international trends in incidence up to 2030. Am J Gastroenterol. 2017;112(8):1247–1255. doi:10.1038/ajg.2017.155
6. Fuchs CS, Doi T, Jang RW, et al. Safety and efficacy of pembrolizumab monotherapy in patients with previously treated advanced gastric and gastroesophageal junction cancer: phase 2 clinical KEYNOTE-059 trial. JAMA Oncol. 2018;4(5):1–8. doi:10.1001/jamaoncol.2018.0013
7. Sajjadi E, Venetis K, Scatena C, Fusco N. Biomarkers for precision immunotherapy in the metastatic setting: hope or reality? Ecancermedicalscience. 2020;14. doi:10.3332/ECANCER.2020.1150
8. Fashoyin-Aje L, Donoghue M, Chen H, et al. FDA approval summary: pembrolizumab for recurrent locally advanced or metastatic gastric or gastroesophageal junction adenocarcinoma expressing PD-L1. Oncologist. 2019;24(1):103–109. doi:10.1634/theoncologist.2018-0221
9. Kang YK, Boku N, Satoh T, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;390(10111):2461–2471. doi:10.1016/S0140-6736(17)31827-5
10. Yamashita K, Iwatsuki M, Harada K, et al. Prognostic impacts of the combined positive score and the tumor proportion score for programmed death ligand-1 expression by double immunohistochemical staining in patients with advanced gastric cancer. Gastric Cancer. 2020;23(1):95–104. doi:10.1007/s10120-019-00999-9
11. Bang YJ, Yañez Ruiz E, Van Cutsem E, et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: primary analysis of JAVELIN gastric 300. Ann Oncol. 2018;29(10):2052–2060. doi:10.1093/annonc/mdy264
12. Shitara K, Özgüroğlu M, Bang YJ, et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): a randomised, open-label, controlled, phase 3 trial. Lancet. 2018;392(10142):123–133. doi:10.1016/S0140-6736(18)31257-1
13. Kojima T, Shah MA, Muro K, et al. Randomized Phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J Clin Oncol. 2020;38(35):4138–4148. doi:10.1200/JCO.20.01888
14. Shitara K, Van Cutsem E, Bang YJ, et al. Efficacy and safety of pembrolizumab or pembrolizumab plus chemotherapy vs chemotherapy alone for patients with first-line, advanced gastric cancer: the KEYNOTE-062 phase 3 randomized clinical trial. JAMA Oncol. 2020;6(10):1571–1580. doi:10.1001/jamaoncol.2020.3370
15. Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398(10294):27–40. doi:10.1016/S0140-6736(21)00797-2
16. Kang PY, Chen PL, Ryu PM, et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER2-negative, untreated, unresectable advanced or recurrent gastric or gastro- oesophageal junction cancer (ATTRACTION-4): a randomised, multicentre, double-blind, placebo. Lancet Oncol. 2022;23(2):234–247. doi:10.1016/S1470-2045(21)00692-6
17. Sun JM, Shen L, Shah MA, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398(10302):759–771. doi:10.1016/S0140-6736(21)01234-4
18. Zhao JJ, Yap DWT, Chan YH, et al. Low programmed death-ligand 1-expressing subgroup outcomes of first-line immune checkpoint inhibitors in gastric or esophageal adenocarcinoma. J Clin Oncol. 2022;40(4):392–402. doi:10.1200/JCO.21.01862
19. Ajani JA, D’Amico TA, Bentrem DJ, et al. Gastric cancer, version 2.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2022;20(2):167–192. doi:10.6004/jnccn.2022.0008
20. Ajani JA, D’Amico TA, Bentrem DJ, et al. Esophageal and esophagogastric junction cancers, version 2.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(7):855–883. doi:10.6004/jnccn.2019.0033
21. Moehler M, Dvorkin M, Boku N, et al. Phase III trial of avelumab maintenance after first-line induction chemotherapy versus continuation of chemotherapy in patients with gastric cancers: results from JAVELIN gastric 100. J Clin Oncol. 2021;39(9):966–977. doi:10.1200/JCO.20.00892
22. Derks S, Liao X, Chiaravalli AM, et al. Abundant PD-L1 expression in Epstein-Barr Virus-infected gastric cancers. Oncotarget. 2016;7(22):32925–32932. doi:10.18632/oncotarget.9076
23. Bass AJ, Thorsson V, Shmulevich I, et al. Comprehensive molecular characterization of gastric adenocarcinoma. Nature. 2014;513(7517):202–209. doi:10.1038/nature13480
24. Kim ST, Cristescu R, Bass AJ, et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat Med. 2018;24(9):1449–1458. doi:10.1038/s41591-018-0101-z
25. Panda A, Mehnert JM, Hirshfield KM, et al. Immune activation and benefit from avelumab in EBV-positive gastric cancer. J Natl Cancer Inst. 2018;110(3):316–320. doi:10.1093/jnci/djx213
26. Kubota Y, Kawazoe A, Sasaki A, et al. The impact of molecular subtype on efficacy of chemotherapy and checkpoint inhibition in advanced gastric cancer. Clin Cancer Res. 2020;26(14):3784–3790. doi:10.1158/1078-0432.CCR-20-0075
27. Helmink BA, Reddy SM, Gao J, et al. B cells and tertiary lymphoid structures promote immunotherapy response. Nature. 2020;577(7791):549–555. doi:10.1038/s41586-019-1922-8
28. Derks S, de Klerk LK, Xu X, et al. Characterizing diversity in the tumor-immune microenvironment of distinct subclasses of gastroesophageal adenocarcinomas. Ann Oncol. 2020;31(8):1011–1020. doi:10.1016/j.annonc.2020.04.011
29. Xu J, Jiang H, Pan Y, et al. LBA53 Sintilimab plus chemotherapy (chemo) versus chemo as first-line treatment for advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma (ORIENT-16): first results of a randomized, double-blind, phase III study. Ann Oncol. 2021;32:S1331. doi:10.1016/j.annonc.2021.08.2133
30. Ahn S, Kim KM. PD-L1 expression in gastric cancer: interchangeability of 22C3 and 28-8 pharmDx assays for responses to immunotherapy. Mod Pathol. 2021;34(9):1719–1727. doi:10.1038/s41379-021-00823-9
31. Narita Y, Sasaki E, Masuishi T, et al. PD-L1 immunohistochemistry comparison of 22C3 and 28-8 assays for gastric cancer. J Gastrointest Oncol. 2021;13(6):2696–2705. doi:10.21037/jgo-21-505
32. Yeong J, Lum HYJ, Teo CB, et al. Choice of PD-L1 immunohistochemistry assay influences clinical eligibility for gastric cancer immunotherapy. Gastric Cancer. 2022;25(4):741–750. doi:10.1007/s10120-022-01301-0
33. Zhou KI, Peterson B, Serritella A, et al. Spatial and temporal heterogeneity of pd-l1 expression and tumor mutational burden in gastroesophageal adenocarcinoma at baseline diagnosis and after chemotherapy. Clin Cancer Res. 2020;26(24):6453–6463. doi:10.1158/1078-0432.CCR-20-2085
34. Ye M, Huang D, Zhang Q, Weng W, Tan C, Qin G, Jiang W, Sheng W and Wang L. (2020). Heterogeneous programmed death-ligand 1 expression in gastric cancer: comparison of tissue microarrays and whole sections. Cancer Cell Int, 20(1), 10.1186/s12935-020-01273-0
35. Klempner SJ, Upadhyay V, Chao J. A space-time continuum for immunotherapy biomarkers in gastroesophageal cancer? Clin Cancer Res. 2020;26(24):6401–6403. doi:10.1158/1078-0432.CCR-20-3389
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.