")
Back to Journals » Journal of Pain Research » Volume 13
Role of Inhaled Methoxyflurane in the Management of Acute Trauma Pain
Authors Fabbri A , Ruggiano G, Garcia Collado S, Ricard-Hibon A, Restelli U , Sbrana G , Marinangeli F , Farina A , Coffey F
Received 3 March 2020
Accepted for publication 6 June 2020
Published 25 June 2020 Volume 2020:13 Pages 1547—1555
DOI https://doi.org/10.2147/JPR.S252222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Andrea Fabbri,1 Germana Ruggiano,2 Sergio Garcia Collado,3 Agnes Ricard-Hibon,4 Umberto Restelli,5,6 Giovanni Sbrana,7 Franco Marinangeli,8 Alberto Farina,9 Frank Coffey10
1Department of Emergency Medicine, Morgagni-Pierantoni Hospital, Forlì, Italy; 2Emergency Medicine Department, Santa Maria Annunziata Hospital, Florence, Italy; 3Hospital Recoletas Campo Grande, Valladolid, Spain; 4Service SAMU-SMUR-SAU, GHT Nord Ouest Vexin Val d’Oise, Pontoise 95, France; 5Center for Health Economics, Social and Health Care Management, LIUC - Università Cattaneo, Castellanza, VA, Italy; 6School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa; 7Anaesthesia, Intensive Care, Emergency Medicine, Grosseto HEMS, ASL Toscana Sud Est, Grosseto, Italy; 8Department of Anesthesiology and Intensive Care, University of L’Aquila, L’Aquila, Italy; 9Medical Affairs Department, Mundipharma Pharmaceuticals Srl, Milan, Italy; 10DREEAM - Department of Research and Education in Emergency Medicine Acute Medicine and Major Trauma, Nottingham University Hospitals’ NHS Trust, Nottingham, UK
Correspondence: Andrea Fabbri
Department of Emergency Medicine, Morgagni-Pierantoni Hospital, Via C. Forlanini 34, Forlì 47100, Italy
Tel +39 0543735156
Email [email protected]
Abstract: Adequate treatment of trauma pain is an integral part of the management of trauma patients, not just for ethical reasons but also because undertreated pain can lead to increased morbidities and worse long-term outcomes. Trauma pain management presents challenges in the pre-hospital setting, particularly in adverse or hostile environments as well as in busy emergency departments (EDs). Inhaled methoxyflurane, administered at analgesic doses via a disposable inhaler, has recently become available in Europe for the emergency treatment of moderate to severe pain in conscious adult trauma patients. A growing body of evidence demonstrates that inhaled methoxyflurane is well tolerated and effective in providing a rapid onset of analgesia. In this paper, we discuss the rationale for methoxyflurane use in trauma pain management, data from clinical trials recently conducted in Europe, its efficacy and safety profile compared to current standard treatments, its place in therapy and organizational impact. We conclude that inhaled methoxyflurane represents an effective treatment option in the different settings where trauma patients require rapid and flexible pain resolution, with potential organizational advantages.
Keywords: emergency, pre-hospital, analgesia, non-opioid pain management
Introduction
Pain management is a human right of all patients, regardless of the nature and origin of pain (cancer pain, non-cancer chronic pain or acute trauma pain). This concept can be found in various reports and standards from the United Nations and other regional human rights organizations, and has direct implications on the practice of medicine and on the access to pain management resources.1
Acute trauma pain has usually limited duration and has a rapid onset caused by a specific event.2 Trauma patients frequently report pain: up to 70% in the pre-hospital setting3,4 and 60–90% in the emergency department (ED). Pain itself is one of the main reasons why patients seek treatment from the ED.5–7
Besides ethical considerations, pain relief is a therapeutic endpoint per se,5 and an efficient management of acute trauma pain is a medical need: pain can be an obstacle to effective trauma treatment, since a patient with pain may be unable to provide his medical history, may have movement restrictions, and may be agitated, frustrated, or aggressive. The under-treatment of acute pain may result in tachycardia, hypertension, delayed recovery, inability to sleep, reduced mobility, worse quality of life, reduced immunity, and pain chronification.8–10
However, acute trauma pain is often overlooked, and not adequately assessed, and/or undertreated (oligoanalgesia), both in pre-hospital and ED settings.4,10–15 Inadequate assessment and under-treatment of acute pain may be attributed to a number of reasons, including lack of specific training, unavailability of analgesic drugs, reluctance to prescribe certain drugs (e.g., opioids), failure to adhere to pain management guidelines or protocols, overcrowding of the ED.10,11,15–22
The availability of a non-narcotic, well-tolerated, rapid-acting, effective and easy to use treatment option may help overcome at least some of these barriers and improve acute trauma pain management.
Standard Pharmacological Treatment of Acute Trauma Pain
Current options for the management of acute pain in trauma settings include a plethora of different opioid and non-opioid drugs, available in many formulations and administered via different routes (Table 1). The choice of the most appropriate pain management strategy should take into consideration pain severity, setting (e.g., ED – pre-hospital – hostile environment), patient’s characteristics, and availability of drugs and/or personnel able to prescribe and administer analgesics.23
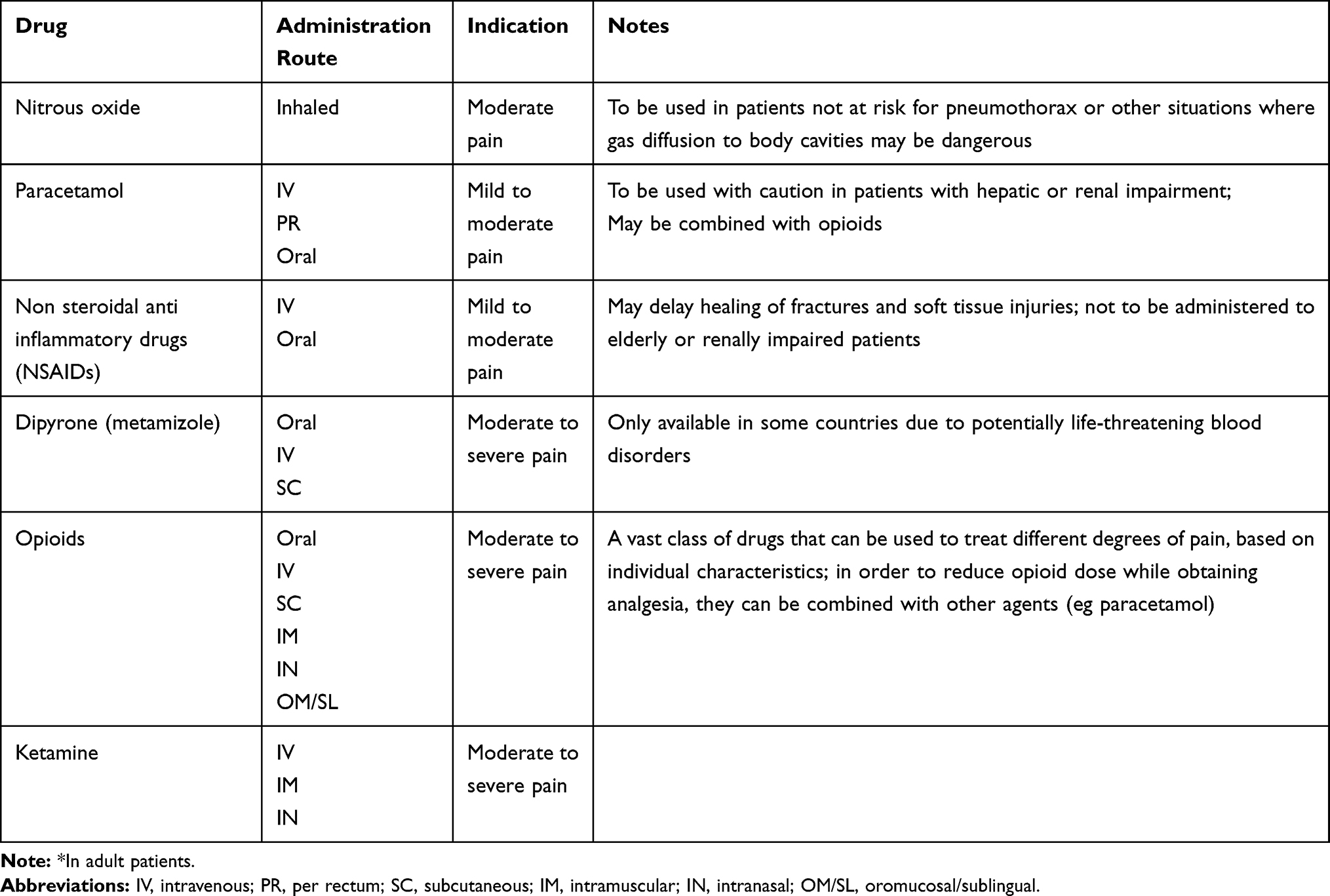 |
Table 1 Commonly Used Pharmacological Treatments for Acute Trauma Pain* |
There is no consolidated pain management practice throughout Europe, and treatment choice may vary greatly between countries and even within the same country, based on Regional or institutional guidelines. The Guidelines for the management of acute pain in emergency situations recently released by the European Society for Emergency Medicine (EUSEM) may help unify pain management strategies and grant patients access to pain relief.23
Inhaled Methoxyflurane
Methoxyflurane is a highly volatile hydrocarbon and is administered through a portable inhaler. It has an effective and rapid analgesic effect and is indicated as an emergency treatment for moderate to severe pain in adult conscious patients with trauma and associated pain. However the exact mechanism of action is not known.
Low-dose (3 mL) methoxyflurane has recently become available in Europe. Treatment must be supervised by a healthcare professional and it is self-administered through patient-controlled analgesia. In the emergency setting, key advantages are represented by the easy handling of the formulation and the rapid onset of action.
The active ingredient is administered through a disposable inhaler (Penthrox®, 3 mL dose, Medical Developments International, Scoresby, Australia): liquid methoxyflurane contained in a 3 mL vial is absorbed by a polypropylene wick and immediately vaporizes. The patient inhales methoxyflurane from the mouthpiece and exhales through an active carbon chamber connected to the device, so that bystanders are not exposed to the drug. Each inhaler dispenses 3 mL of methoxyflurane. The maximum analgesic dose is 2 x 3 mL in 24 hours, and the second 3 mL bottle should only be used where needed. Administration on consecutive days is not recommended, and the total dose in a week should not exceed 15 mL.24
Methoxyflurane has been used as an inhaled anesthetic starting in the 1960s but was discontinued in this setting in the late 1970s, since anesthetic doses were associated with nephrotoxicity and hepatotoxicity.25–27 Methoxyflurane remained in use in Australia and New Zealand at sub-anesthetic doses as an analgesic, and has an established safety profile having been administered to over six million patients. Methoxyflurane is contraindicated for anesthetic purposes, and in patients with specific conditions and characteristics (Box 1).24
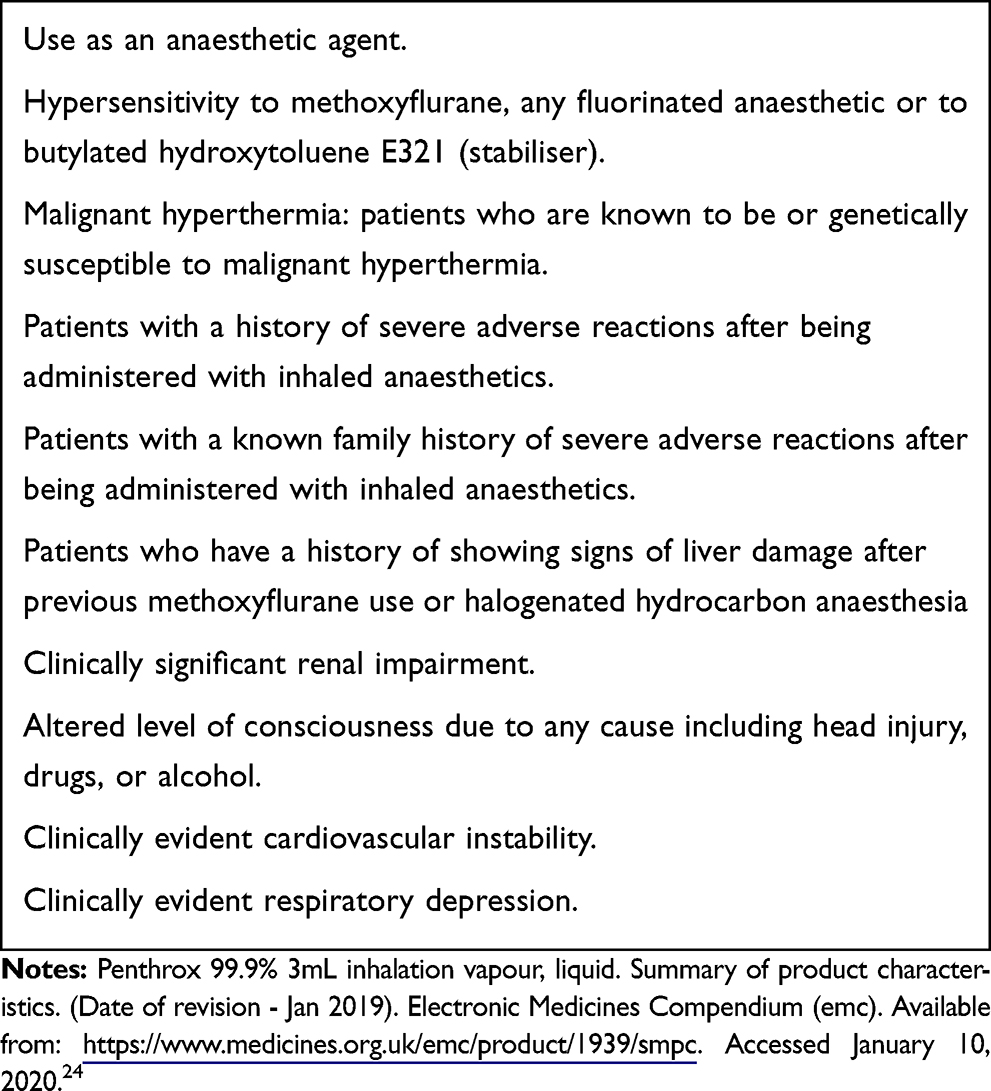 |
Box 1 Contraindications to Inhaled Methoxyflurane |
Recently methoxyflurane has been approved in Europe for the relief of moderate to severe trauma pain in adult conscious patients, based on the results of the STOP! Phase III study.
The following paragraph summarizes the main studies, completed or ongoing in Europe, following a meeting where investigators discussed key data from each study, and intends to provide a narrative review. A systematic literature review has not been conducted.
European Clinical Trials
STOP! Study – Methoxyflurane vs. Placebo
STOP! (ClinicalTrials.gov Identifier: NCT01420159) was a Phase 3, randomized, double blind trial comparing inhaled methoxyflurane to placebo in the ED setting. In this study, 300 patients (of whom 210 were adults ≥18 years of age) with moderate (Numeric Rating Scale [NRS] 4–7) trauma (burn, contusion, dislocation, fracture, injury due to foreign body, laceration) pain were randomized 1:1 to receive an inhaler with 3 mL of methoxyflurane or placebo. The patient could request a second inhaler, if necessary. Patients treated with methoxyflurane reported significantly greater and faster reduction in pain scores as compared to placebo: the overall difference between the methoxyflurane and placebo arms was −15.1 mm on the VAS scale (95% CI −19.2 to −11.0; p<0.0001), with the greatest effect being observed at 15 min (−18.5 mm). Pain relief was reported by 87.2% of patients on methoxyflurane, with a median time to first pain relief of 4 minutes (95% CI 2.0 to 5.0). The majority of patients in the methoxyflurane arm (84.6%) reported their first pain relief within 10 inhalations (1–5 inhalations: 49.7%; 6–10 inhalations: 34.9%). No serious toxicities were observed, and the main safety findings were transient headache and dizziness. Both patients and health care professionals expressed satisfaction with methoxyflurane.28
The STOP! Study was instrumental in establishing the efficacy and safety profile of inhaled methoxyflurane in controlling trauma pain, yet a comparison to commonly used analgesics in terms of efficacy was missing, therefore additional trials with an active comparator arm were conducted.
Table 2 provides a summary of the study designs and outcomes of the clinical studies of inhaled methoxyflurane included in this discussion.
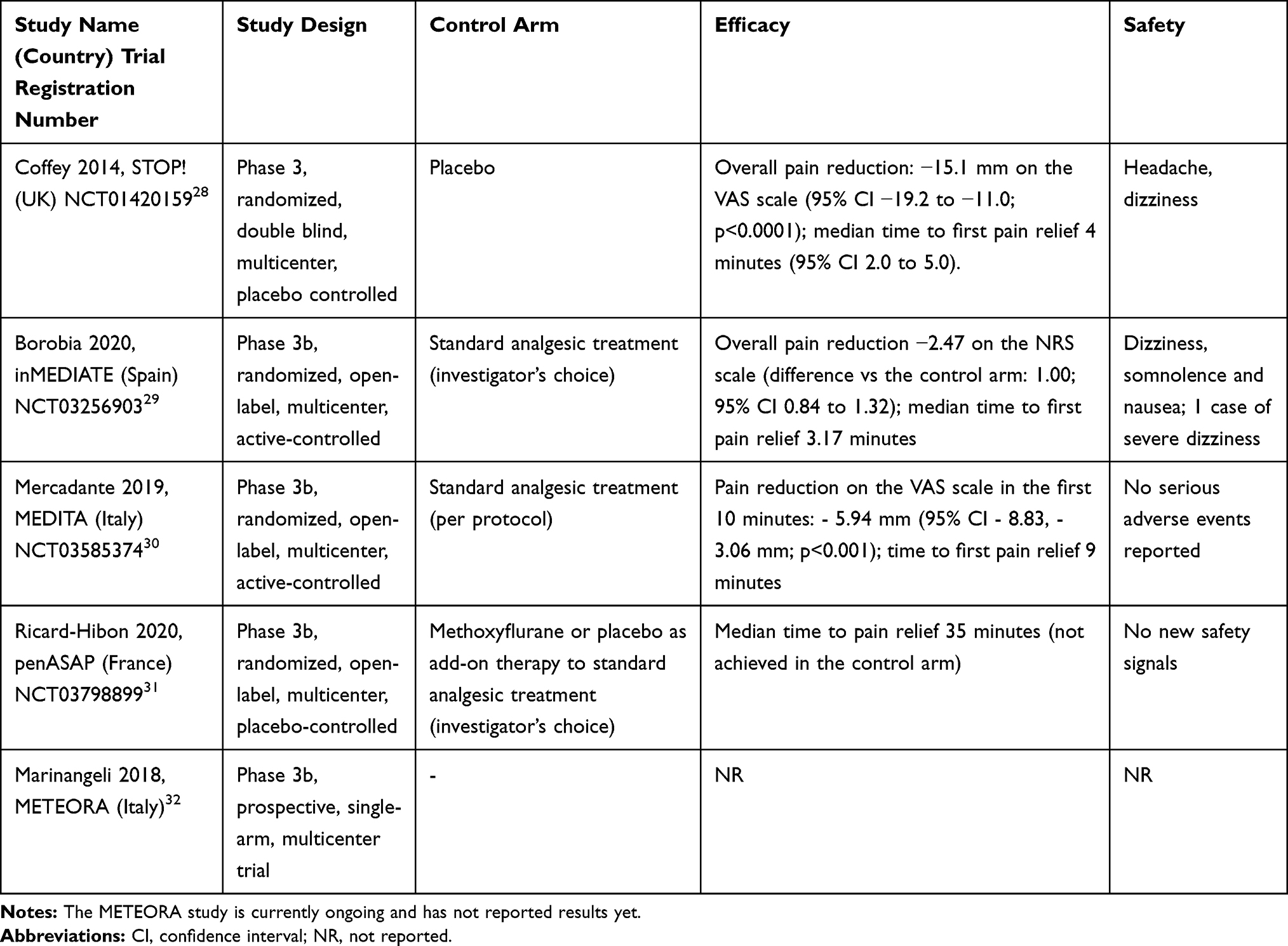 |
Table 2 Summary of Inhaled Methoxyflurane Study Design and Outcomes |
inMEDIATE Study – Methoxyflurane vs. Active Therapy According to Investigator’s Choice
inMEDIATE was a phase 3b, randomized, multicenter, open-label trial (ClinicalTrials.gov Identifier: NCT03256903) that compared inhaled methoxyflurane to standard pain management therapies as per investigator choice (1:1 randomization) during the first 20 minutes of administration in patients presenting to Spanish EDs with moderate to severe trauma pain (≥4 on the NRS). Traumas were represented by: contusion, fracture, swelling, dislocation, laceration, burn. The study enrolled 305 patients. In the comparator arm 70% of patients received intravenous (IV - NSAIDs in most cases) analgesia, and 9.4% were treated with opioids. Pain relief, as measured by the decrease in NRS pain score from baseline, was significantly greater in the methoxyflurane arm at all timepoints (5, 10, 15 and 20 minutes), regardless of baseline pain intensity and class of comparator analgesic. The global reduction in pain scores on the NRS scale during the first 20 minutes was 2.47 with methoxyflurane, versus 1.39 in the control arm (difference 1.00; 95% CI 0.84 to 1.32), and the proportion of responders, defined as patients who experienced a reduction of at least 30% in pain intensity, was significantly greater in the methoxyflurane arm (87.9% versus 57.7% in the control group). The median time to first pain relief was shorter in the methoxyflurane arm (3.17 minutes, versus 10.00 minutes with standard analgesic treatment), and patients on methoxyflurane spent less time in the ED compared to those who received standard treatment.
Patients and health care professionals expressed greater satisfaction in pain reduction and in comfort of treatment with methoxyflurane than with standard analgesics: methoxyflurane exceeded patients’ expectations in 77% of cases (vs 38% for standard analgesic treatment) and clinicians’ expectations in 72% of cases (vs 19% for standard analgesic treatment). Methoxyflurane was well tolerated in the inMEDIATE study; the reported adverse events were dizziness, somnolence and nausea, and were mild or moderate in intensity, except for one case of severe treatment-related dizziness.29
MEDITA Study – Methoxyflurane vs. Active Therapy According to Study Protocol
MEDITA, a phase 3b, randomized, multicenter, open-label, active-controlled clinical trial (ClinicalTrials.gov Identifier: NCT03585374), enrolled 270 patients with a single trauma (fracture, dislocation, crushing or contusion) based on clinical suspicion. As in the inMEDIATE trial inhaled methoxyflurane was compared to standard analgesic treatment (SAT), but in this case the comparator drugs were defined by protocol: intravenous (IV) paracetamol or ketoprofen in moderate pain (NRS 4–6) and IV morphine in severe pain (NRS ≥7). The primary outcome was the change in pain score on the VAS scale from randomization (baseline) to 3, 5 and 10 minutes. During the first 10 minutes from randomization, patients on methoxyflurane reported a significantly greater pain reduction compared to patients on SAT (adjusted mean treatment difference - 5.94 mm; 95% CI - 8.83, - 3.06 mm; p<0.001). Similar results were obtained in the patient subgroups defined by pain intensity at baseline (moderate pain: - 5.97 mm; 95% CI - 9.55, - 2.39 mm; p = 0.001; severe pain: - 5.54 mm; 95% CI - 10.49, - 0.59 mm; p = 0.029) in a post-hoc exploratory analysis.
The time to first pain relief was reported by 82.7% of patients on methoxyflurane and by 78.9% on SAT; even against the strong comparator drugs in the SAT arm, inhaled methoxyflurane provided a more rapid relief from pain (9 min; 95% CI 7.72, 10.28 min vs 15 min; 95% CI 14.17,15.83 min). Patients provided a higher rating of methoxyflurane efficacy as compared to SAT (“Excellent”, “Very Good” or “Good”: 72.7% vs. 60.9%; p = 0.001), while physicians were asked about the practicality of the different interventions and rated methoxyflurane as “Excellent”, “Very Good” or “Good” in a significantly higher proportion with respect to SAT (90.3% vs. 64.4%; p<0.001). Overall, 17% of patients on methoxyflurane experienced adverse events, none were serious.30
PenASAP Study – Methoxyflurane as Part of Multi-Modal Analgesia
In the French PenASAP study (ClinicalTrials.gov Identifier: NCT03798899), trauma patients with moderate to severe pain were randomized 1:1 to receive either methoxyflurane or placebo as an add-on therapy to the standard of care, as defined by the investigator. The data presented at the 2019 EUSEM congress show that the addition of methoxyflurane to standard analgesics is effective in relieving trauma pain (contusion, fracture, sprain, wound, dislocation, muscular injury, burn); the primary endpoint of median time to pain relief (defined as 30mm or less on the visual analogue scale) was 35 minutes in the methoxyflurane arm, while pain relief was not achieved in the control arm; no new safety signals were reported. While indirectly confirming that trauma pain undertreatment is still an unresolved issue in many EDs across Europe, the results of the PenASAP study establish inhaled methoxyflurane as a viable option in the context of multi-modal pain management strategies in trauma patients.31
METEORA Study – Methoxyflurane in Hostile Environments
METEORA, a phase 3b, prospective, single-arm, multicenter trial, was designed to assess whether inhaled methoxyflurane is effective, safe and practical in treating trauma pain (fracture, dislocation, crushing or contusion) in hostile environments, given its specific characteristics (portability, easy use and rapid pain relief). This currently ongoing study will enroll approximately 200 patients with a single limb trauma (based on clinical suspicion) and moderate to severe pain in the context of rescue missions performed by the Helicopter Emergency Medical Service (HEMS) in Italy. Pain intensity will be measured on the VAS scale at baseline (start of methoxyflurane inhalation), 5, 10, 15, 20, 30, 45 and 60 minutes and when positioning the patient on a spinal board or stretcher, and also on the NRS scale at baseline and at 10 minutes. Patients will rate methoxyflurane efficacy and health care professionals will rate practicality at two timepoints (30 and 60 minutes). The primary endpoint of the METEORA study is the proportion of trauma patients who achieve at least 30% reduction in pain score on the VAS scale within 10 minutes from methoxyflurane inhalation.32
Practicality of Inhaled Methoxyflurane
Pre-Hospital Setting
The methoxyflurane inhaler is small and lightweight and can be easily transported and stored at a wide range of temperatures (−20 to 40° Celsius). These characteristics make it fit for use in the pre-hospital setting, where practicality is necessary.
The quick onset of analgesia provided by methoxyflurane, besides relieving the patients, allows rapid intervention when the patient needs to be extricated to be transported to the ED and in case of dislocations or fractures.
In the emergency setting, inhaled analgesics represent a great advantage because a rapid intervention is required and the time it takes to administer IV analgesics may delay rescue operations and transfer to the ED. Venous access can be troublesome in emergency situations, thus reducing the chance to provide rapid relief to the suffering patient and causing reduced patient throughput and waste of resources.
Inhaled methoxyflurane is self-administered by the patient after a brief training and typically provides pain relief within 6–10 inhalations. It requires no cannulation or other invasive procedures.
In pre-hospital settings, where interventions are made by a variety of professionals (e.g., paramedics, mountain or water rescue, police, firemen) and physicians may not be present, the practical and safe administration route of methoxyflurane is a clear advantage.
Exhalation through the active carbon chamber adsorbs exhaled methoxyflurane, avoiding dispersion in the environment and exposure of nearby individuals. This can be an advantage in small, secluded spaces (e.g., ambulance, rescue mission helicopter) and in busy EDs.
Hospital Setting
In the hospital setting the availability of analgesics is wider and medical personnel are present. The choice of pain management strategy should therefore be based on the patient’s specific needs and characteristics, as well as the risk/benefit profile of the available drugs.
Pain relief should be provided as quickly as possible; ideally, the triage nurse should perform pain assessment and provide analgesia where necessary as part of the triage protocol. Time to analgesia is not merely related to the time it takes for a drug to relieve the pain, but also to the time to prescribe, obtain and administer the drug. When patients present to the ED with severe trauma pain, opioids are an obvious choice in terms of efficacy, yet the administrative burden associated to the administration of controlled substances, the availability of personnel with specific training and qualifications, the necessity to monitor patients after administration and to manage opioid side effects may become barriers to opioid utilization in emergency situations.
Self-administration of analgesics by the patient can represent an advantage, both in terms of pain control and resource utilization. Fast and effective provision of analgesia can ultimately result in organizational advantages, by allowing higher patient throughput and reducing ED overcrowding.
Safety
Over forty years of experience with low-dose methoxyflurane in Australia and New Zealand and the recent European studies have established its favorable safety profile in the setting of acute trauma pain treatment. The common non-serious adverse reactions observed at analgesic doses are CNS type reactions such as dizziness and somnolence, and are generally easily reversible.24 Laboratory tests performed shortly after methoxyflurane administration in clinical trials revealed no evidence of nephrotoxicity or hepatotoxicity.28,29 Treatment with methoxyflurane had no clinically significant effects on cardiovascular or respiratory parameters.29 Methoxyflurane can be administered to trauma patients in need of pain relief, with no need of constant monitoring by health care professionals.
Organizational Impact
The organizational and financial impact of methoxyflurane for acute pain management in the context of moderate to severe pain in patients with trauma (fracture, dislocation and contusion) presenting to the ED in Italy is currently the object of quali-quantitative research (METAMORPHOSIS study – see Table 3 for study design). The study is currently being conducted through a structured interview administered to 14 key opinion leaders (10 ED directors, 2 doctors, 2 nurses) within 10 EDs located in 8 Italian Regions.
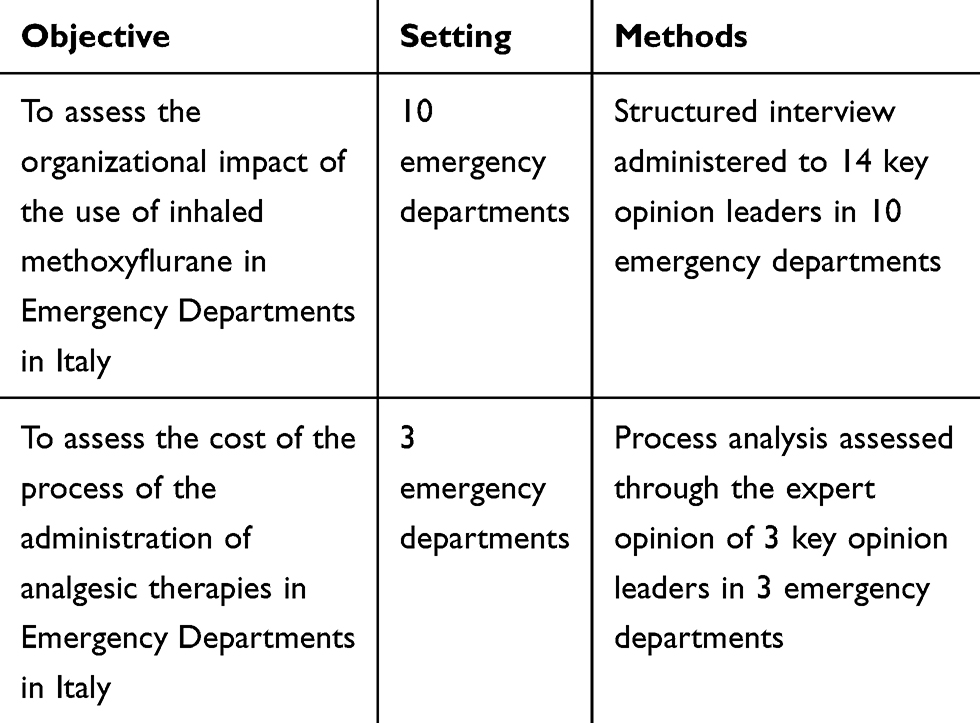 |
Table 3 Summary of the METAMORPHOSIS Study Design |
The results of the analysis showed a positive organizational impact compared to the standard of care and this was related to an increase of the efficiency of the administration processes (not requiring intravenous administration and due to its “easy and simple way of use”), to a more rapid analgesic effect and to a reduced monitoring activity.
Rapid pain relief is also instrumental in establishing trust in the ED personnel by reducing patient stress and agitation. Considering patients’ hospital pathway, the use of methoxyflurane would not inhibit the use of further therapies (due to the absence of drugs interactions) and would not limit patients’ activities after discharge (as in the case of use of opioids). Considering the possibility to transport patients to other departments compared with analgesics administered by the IV route, inhaled methoxyflurane allows better safety and comfort with respect to patient transportation.
In terms of cost of administration and monitoring process, as estimated through process analysis based on expert opinion of clinicians involved in the research conducted at 3 of 10 participating EDs, the use of inhaled methoxyflurane compared with paracetamol IV plus morphine IV, would lead to a reduced use of human resources and consumables, with a lower cost per process of more than 30 € (not considering the cost of the device).
Finally, the use of inhaled methoxyflurane was associated with a positive acceptance by both health care professionals and patients (as reported by the key opinion leaders interviewed).
Discussion
Fast and efficient management of moderate to severe pain in trauma patients is a medical need, yet oligoanalgesia remains a problem despite the availability of several therapeutic options.
The recent introduction of low-dose inhaled methoxyflurane represents a new approach to acute trauma pain treatment.
Several randomized controlled trials have been recently conducted, comparing methoxyflurane to placebo28 or to standard analgesic treatments29,30 (either defined by protocol or by the investigators) and in the context of multi-modal analgesia.31 All have reported consistent results: low-dose methoxyflurane is an effective analgesic and provides pain relief faster than the comparators (i.e., time to first pain relief 3–5 minutes; 6–10 inhalations). Methoxyflurane is generally well tolerated, with mild and transient adverse events (mainly headache and dizziness).
When patient and health care professional satisfaction was assessed, methoxyflurane scored higher points than the comparators in terms of pain control, comfort and ease of use.
Data from the control arms of the studies that compared methoxyflurane to standard treatment as per investigator choice also showed that trauma pain is often undertreated in current clinical practice, and there is no established standard of care (e.g., in the inMEDIATE study29 only 23% of the patients with severe pain [>7 on the NRS scale] received opioids in the standard of care arm or as a rescue medication; in the PenASAP study31 patients in the control arm did not achieve pain control).
There are several barriers to effective trauma pain control, and they are not only complex but also generally associated with a lack of time and resources. The availability of a fast-acting, self-administered, well tolerated and effective non-narcotic alternative such as inhaled methoxyflurane represents a useful addition to current options, particularly in situations where flexibility, practicality of use and rapid effect are needed. In the pre-hospital setting inhaled methoxyflurane can be particularly useful since it is portable, non-flammable, and can be self-administered by the patients while the rescue personnel perform vital operations. The fast analgesic action enables the patient to be moved quickly and without excessive discomfort. Inhaled methoxyflurane is administered at fixed dose and requires no invasive procedures. The exhalation of methoxyflurane through an active carbon chamber reduces professional exposure to the drug and is an advantage in small spaces, such as an ambulance or a helicopter.
In the hospital setting, methoxyflurane may offer an organizational advantage, being fast and easy to administer, with reduced patient monitoring required. It could save resources by allowing ED personnel to perform other duties while the patient self-administers the drug under supervision. Methoxyflurane may be particularly useful for patients who present with traumas that are easy to treat when severe pain prevents procedures (e.g., dislocations and fractures).
Depending on local regulations, specific protocols could be necessary to allow non-medical staff to prescribe and administer inhaled methoxyflurane. Besides rescue staff at emergency scenes, this would also apply to the triage nurse who could perform pain assessment and prescribe methoxyflurane where appropriate, thus relieving the patient from pain as quickly as possible. Methoxyflurane does not interfere with other drugs, thus allowing the patient to receive other medications or anaesthetics if necessary.
Additional research on low-dose inhaled methoxyflurane could be useful to clearly establish its relative efficacy compared to opioids (including inhaled opioids) in patients with severe trauma pain, and in identifying the trauma patient profiles who could benefit the most from this acute pain treatment option. Finally, since METEORA32 and METAMORPHOSIS studies are not yet complete, it is not possible to draw definitive conclusions on the use of methoxyflurane in hostile environments and on the organizational impact.
Conclusion
Low-dose methoxyflurane, administered through a portable, handheld, disposable device, is a well-tolerated and effective option in the management of acute, moderate to severe trauma pain in adult patients. Its ease of use, portability and fast action make it particularly useful in all the situations where rapid analgesia is required, including pre-hospital/hostile environments where practicality is necessary.
Acknowledgments
The present paper was developed by the authors after an advisory board meeting sponsored by Mundipharma Pharmaceuticals srl. Editorial assistance for the preparation and submission of the manuscript was provided by Mundipharma Pharmaceuticals srl. Penthrox® is a registered trade mark of Medical Developments International (MDI) Limited and used under license.
Disclosure
Dr Umberto Restelli and Dr Frank Coffey report grants from Mundipharma, during the conduct of the study. Dr Alberto Farina is an employee for Mundipharma Pharmaceuticals srl. The authors report no other conflicts of interest in this work.
References
1. Brennan F, Lohman D, Gwyther L. Access to pain management as a human right. Am J Public Health. 2019;109:61–65. doi:10.2105/AJPH.2018.304743
2. Grichnik KP, Ferrante FM. The difference between acute and chronic pain. Mt Sinai J Med. 1991;58(3):217–220.
3. Berben SA, Schoonhoven L, Meijs TH, van Vugt AB, van Grunsven PM. Prevalence and relief of pain in trauma patients in emergency medical services. Clin J Pain. 2011;27:587–592. doi:10.1097/AJP.0b013e3182169036
4. Galinski M, Ruscev M, Gonzalez G, et al. Prevalence and management of acute pain in prehospital emergency medicine. Prehosp Emerg Care. 2010;14:334–339. doi:10.3109/10903121003760218
5. Berben SA, Meijs TH, van Dongen RT, et al. Pain prevalence and pain relief in trauma patients in the accident & emergency department. Injury. 2008;39:578–585. doi:10.1016/j.injury.2007.04.013
6. Cordell WH, Keene KK, Giles BK, Jones JB, Jones JH, Brizendine EJ. The high prevalence of pain in emergency medical care. Am J Emerg Med. 2002;20(3):165–169. doi:10.1053/ajem.2002.32643
7. Gueant S, Taleb A, Borel-Kuhner J, et al. Quality of pain management in the emergency department: results of a multicentre prospective study. Eur J Anaesthesiol. 2011;28(2):97–105. doi:10.1097/EJA.0b013e3283418fb0
8. International Association for the Study of Pain. Pain terms: a current list with definitions and notes on usage. Available from: www.iasp-pain.org/files/Content/ContentFolders/Publications2/ClassificationofChronicPain/Part_III-PainTerms.pdf.
9. Ministero della Salute. Relazione sullo Stato Sanitario del Paese: 2009–2010. 2010. Available from: http://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=1655.
10. Parker M, Rodgers A. Management of pain in pre-hospital settings. Emerg Nurse. 2015;23:
11. Marinangeli F, Narducci C, Ursini ML, et al. Acute pain and availability of analgesia in the prehospital emergency setting in Italy: a problem to be solved. Pain Pract. 2009;9(4):282–288. doi:10.1111/j.1533-2500.2009.00277.x
12. Simpson PM, Bendall JC, Tiedemann A, Lord SR, Close JCT, Callaway CW. Provision of out-of-hospital analgesia to older fallers with suspected fractures: above par, but opportunities for improvement exist. Acad Emerg Med. 2013;20(8):761–768. doi:10.1111/acem.12190
13. Walsh B, Cone DC, Meyer EM, Larkin GL. Paramedic attitudes regarding prehospital analgesia. Prehosp Emerg Care. 2013;17:78–87. doi:10.3109/10903127.2012.717167
14. Siriwardena AN, Shaw D, Bouliotis G. Exploratory cross-sectional study of factors associated with pre-hospital management of pain. J Eval Clin Pract. 2010;16:1269–1275. doi:10.1111/j.1365-2753.2009.01312.x
15. Bakkelund KE, Sundland E, Moen S, Vangberg G, Mellesmo S, Klepstad P. Undertreatment of pain in the prehospital setting: a comparison between trauma patients and patients with chest pain. Eur J Emerg Med. 2013;20(6):428–430. doi:10.1097/MEJ.0b013e32835c9fa3
16. Motov SM, Khan AN. Problems and barriers of pain management in the emergency department: are we ever going to get better? J Pain Res. 2009;2:5–11.
17. De Berardinis B, Magrini L, Calcinaro S, et al. Emergency department pain management and its impact on patients’ short term outcome. Open J Emerg Med. 2013;5:1–7. doi:10.2174/1876542420130729001
18. Mills AM, Shofer FS, Chen EH, Hollander JE, Pines JM. The association between emergency department crowding and analgesia administration in acute abdominal pain patients. Acad Emerg Med. 2009;16(7):603–608. doi:10.1111/j.1553-2712.2009.00441.x
19. Karwowski-Soulie F, Lessenot-Tcherny S, Lamarche-Vadel A, et al. Pain in an emergency department: an audit. Eur J Emerg Med. 2006;13:218–224. doi:10.1097/01.mej.0000217975.31342.13
20. Kumar N. WHO normative guidelines on pain management. 2007. Available from: http://www.who.int/medicines/areas/quality_safety/delphi_study_pain_guidelines.pdf.
21. Thomas SH Management of pain in the emergency department. ISRN Emergency Medicine 2013. Article ID 583132.
22. Sills MR, Fairclough DL, Ranade D, Mitchell MS, Kahn MG. Emergency department crowding is associated with decreased quality of analgesia delivery for children with pain related to acute, isolated, long-bone fractures. Acad Emerg Med. 2011;18(12):1330–1338. doi:10.1111/j.1553-2712.2011.01136.x
23. EUSEM guidelines for the management of acute pain in emergency situations 2019. Available from: https://eusem.org/images/EUSEM_EPI_GUIDELINES_MARCH_2020.pdf.
24. Penthrox 99.9% 3mL inhalation vapour, liquid. Summary of product characteristics. Available from: https://www.medicines.org.uk/emc/product/1939/smpc.
25. Tomlin PJ. Methoxyflurane. Br J Anaesth. 1965;37(9):706–709. doi:10.1093/bja/37.9.706
26. Crandell WB, Pappas SG, Macdonald A. Nephrotoxicity associated with methoxyflurane anaesthesia. Anesthesiology. 1966;27:591–607. doi:10.1097/00000542-196609000-00010
27. Mazze RI, Shue GL, Jackson SH. Renal dysfunction associated with methoxyflurane anaesthesia: a randomised, prospective clinical evaluation. JAMA. 1971;216:278–288. doi:10.1001/jama.1971.03180280032006
28. Coffey F, Wright J, Hartshorn S, et al. STOP!: a randomised, double-blind, placebo-controlled study of the efficacy and safety of methoxyflurane for the treatment of acute pain. Emerg Med J. 2014;31(8):613–618. doi:10.1136/emermed-2013-202909
29. Borobia AM, Collado SG, Cardona CC, et al. Inhaled methoxyflurane provides greater analgesia and faster onset of action versus standard analgesia in patients with trauma pain: inMEDIATE: a randomized controlled trial in emergency departments. Ann Emerg Med. 2020;75(3):315–328.
30. Mercadante S, Voza A, Serra S, et al. Analgesic efficacy, practicality and safety of inhaled methoxyflurane versus standard analgesic treatment for acute trauma pain in the emergency setting: a randomised, open-label, active-controlled, multicentre trial in Italy (MEDITA). Adv Ther. 2019;36(11):3030–3046. doi:10.1007/s12325-019-01055-9
31. Ricard-Hibon A, Lecoules N, Jacquin L, et al. Inhaled methoxyflurane for the management of trauma related pain in patients admitted to hospital emergency departments: a randomised, double-blind placebo-controlled trial (PenASAP study). Brit Med J. 2020.
32. Marinangeli F, Reggiardo G, Sblendido A, Soldi A, Farina A; METEORA Group. Prospective, multicentre trial of methoxyflurane for acute trauma-related pain in helicopter emergency medical systems and hostile environments: METEORA protocol. Adv Ther. 2018;35(11):2081–2092. doi:10.1007/s12325-018-0816-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.