")
Back to Journals » Cancer Management and Research » Volume 13
Role of Chronic Inflammatory Ratios in Predicting Recurrence of Resected Patients with Stage I–III Mucinous Colorectal Adenocarcinoma
Authors Liao YC, Ying HQ , Huang Y, Luo YR, Xiong CF, Nie RW, Li XJ, Cheng XX
Received 25 January 2021
Accepted for publication 12 March 2021
Published 20 April 2021 Volume 2021:13 Pages 3455—3464
DOI https://doi.org/10.2147/CMAR.S303758
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Yu-Cui Liao,1,* Hou-Qun Ying,2,* Ying Huang,3,* Yan-Ran Luo,3 Cui-Fen Xiong,3 Ruo-Wei Nie,3 Xiao-Juan Li,4 Xue-Xin Cheng1
1School of Public Health; Jiangxi Provincial Key Laboratory of Preventive Medicine, Nanchang University, Nanchang, Jiangxi, 330006, People’s Republic of China; 2Department of Nuclear Medicine, Jiangxi Province Key Laboratory of Laboratory Medicine, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330006, People’s Republic of China; 3Jiangxi Medical College, Nanchang University, Nanchang, 330006, People’s Republic of China; 4Department of Clinical Laboratory, Kunming Children’s Hospital, Kunming, Yunnan, 650500, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xue-Xin Cheng
School of Public Health; Jiangxi Provincial Key Laboratory of Preventive Medicine Nanchang University, No. 1 Of Minde Road, Nanchang, People’s Republic of China
Tel/Fax +86 0791-86297662
Email [email protected]
Background: Cancer-related inflammation is the main cause of the progression of mucinous colorectal adenocarcinoma (MCA). Circulating fibrinogen-to-pre-albumin ratio (FPR) is associated with the clinical outcome in colorectal cancer (CRC). However, the prognostic role of FPR and which is the best inflammatory prognostic biomarker within MCA remain unknown.
Methods: We enrolled 157 patients with stage I–III MCA in this study. Kaplan-Meier curve, Cox regression, and time-dependent receiver operation characteristic curve analysis were performed to assess the prognostic value and efficacy of the neutrophil-to-albumin ratio (NAR), neutrophil-to-pre-albumin ratio (NPAR), albumin-to-alkaline phosphatase ratio (AAPR), albumin-to-globulin ratio (AGR), albumin-to-fibrinogen ratio (AFR), and FPR in these patients.
Results:: We found that NAR, NPAR, and FPR were significantly associated with unsatisfactory recurrence-free survival (RFS) in patients with stage I–III MCA, and the predicted efficacy of FPR was superior to that of the other two inflammatory biomarkers. Moreover, patients with a high combined TNM-CA199-FPR score had worse outcomes, with a high predicted efficacy of up to 0.779 (0.703– 0.856). Using FPR, the patient was monitored for the recurrence up to two months earlier than that achieved using the common imaging techniques (4 vs 6 median months) in stage I–III MCA patients undergoing radical resection.
Conclusion: FPR is the preferred inflammatory biomarker and commonly used for predicting and monitoring recurrence in stage I–III MCA patients. The combined TNM-CA199-FPR score is an economical, simple, effective, and independent prognostic factor for localized disease.
Keywords: mucinous colorectal carcinoma, fibrinogen-to-pre-albumin ratio, prognosis, inflammation
Introduction
Mucinous colorectal adenocarcinoma (MCA) is a distinct, rare, and fatal colorectal cancer (CRC) worldwide.1 It is commonly characterized by abundant extracellular mucin, which accounts for more than 50% of the tumor cells. In China, the reported incidence of the disease is only 8.17%,2 and the disease is mostly observed in women and younger patients, with the tumor located on the right side.1 MCA is associated with a poor response to chemotherapy and poor prognosis.3 However, there is no factor that can effectively predict and monitor recurrence.
Cancer-elicited inflammation is an important hallmark of cancer.4 MCA is more commonly diagnosed in patients with inflammatory bowel diseases or Lynch syndrome,5 and emerging epidemiological evidence indicates that non-steroidal anti-inflammatory drugs are potent in preventing CRC.6 Thus, chronic inflammation is a critical characteristic in the onset and progression of MCA,4,7,8 fostering its proliferation, survival, invasion, migration, and metastasis. Moreover, the degree of inflammation is presented as an alternation of inflammatory factors and cells within the cancer microenvironment and circulating peripheral blood, and these changes are possibly linked to clinical recurrence and disease progression. Previous studies have shown that the albumin-to-alkaline phosphatase ratio (AAPR), neutrophil-to-albumin/pre-albumin ratio (NAR/NPAR), and albumin-to-globulin ratio (AGR) are significantly associated with the prognosis of solid malignancies.9–11 In addition, the albumin-to-fibrinogen ratio (AFR), and fibrinogen-to-pre-albumin ratio (FPR) are promising factors for predicting the clinical outcomes of solid malignancies.12–16 However, no study has reported the association between these inflammatory biomarkers and the clinical outcomes of MCA.
The present study aimed to investigate the prognostic roles of AAPR, NAR, NPAR, AGR, AFR, and FPR in localized MCA and assess the monitoring role of FPR in 250 patients. These findings would help clinicians tailor decision-making in MCA treatment.
Materials and Methods
In this study, we enrolled patients diagnosed with MCA at the Second Affiliated Hospital of Nanchang University between November 2010 and April 2017. The study was performed in accordance with the guidelines of the Declaration of Helsinki, and was approved by the Ethics Committees of the Second Affiliated Hospital of Nanchang University. Written informed consent was obtained from each participant before the study.
A flowchart of the protocol for screening and identifying eligible patients in this study is shown in Figure 1. We initially recruited 250 diagnosed stage I–III MCA patients for this study. The eligible patients were identified according to the following inclusion criteria: a) first diagnosed MCA patients were clinically confirmed by histopathological examination of the resected biopsies; b) radical resection was performed in stage I–III patients with tumor-negative resection margins; and c) without any emergency or neoadjuvant chemoradiotherapy, and other malignancies within the patients. In contrast, the following criteria were used to exclude unsuitable participants: a) recent diarrhea, infection, hereditary polyposis, ulcerative colitis, autoimmune or chronic kidney disease, hematopathy, hepatopathy, or cardiovascular and cerebrovascular disease was clinically confirmed in the patients; b) non-steroidal anti-inflammatory drug or intravenous albumin supplement was undertaken in the past three months; and c) clinical characteristics, and baseline information not provided by the participants or lost to follow-up within three months.
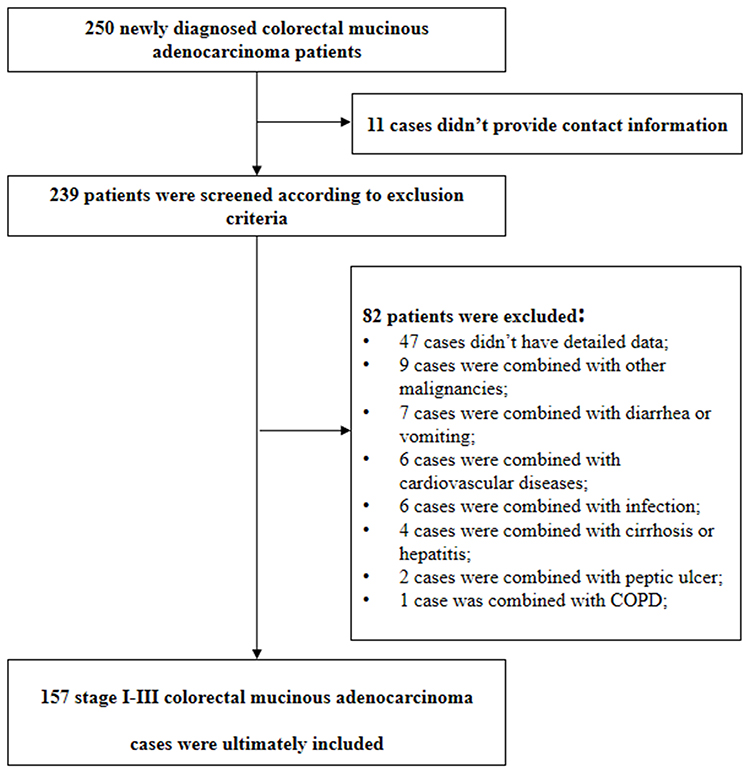 |
Figure 1 The flowchart of screening and identification of eligible patients in the present study. |
We collected the clinical characteristics, baseline information, and pathological results of each eligible patient. Abundant peripheral blood, plasma, and serum samples were collected after admission with one or two days before the surgical operation. Circulating neutrophil count was detected by flow cytometry, laser scattering, and cytochemical staining combined techniques using a Sysmex HST-302 machine (Sysmex, Tokyo, Japan). OLYMPUS AU5400 (Beckman Coulter, Tokyo, Japan) was used to determine the levels of serum alkaline phosphatase (ALP), albumin, and pre-albumin, and the Clauss assay was used to measure plasma fibrinogen level using a SYSMEX CA-7000 machine (Sysmex, Tokyo, Japan). Meanwhile, both carcinoembryonic antigen (CEA) and carbohydrate antigen 19–9 (CA19-9) were quantified through the chemiluminescence immunoassay by a SIEMENS ADVIA Centaur XP machine (Siemens, Erlangen, Germany). The inter- and intra-batch coefficients of these detections were less than 10%. AAPR, NAR, NPAR, AGR, AFR, and FPR were calculated according to the formulas shown in Table 1.
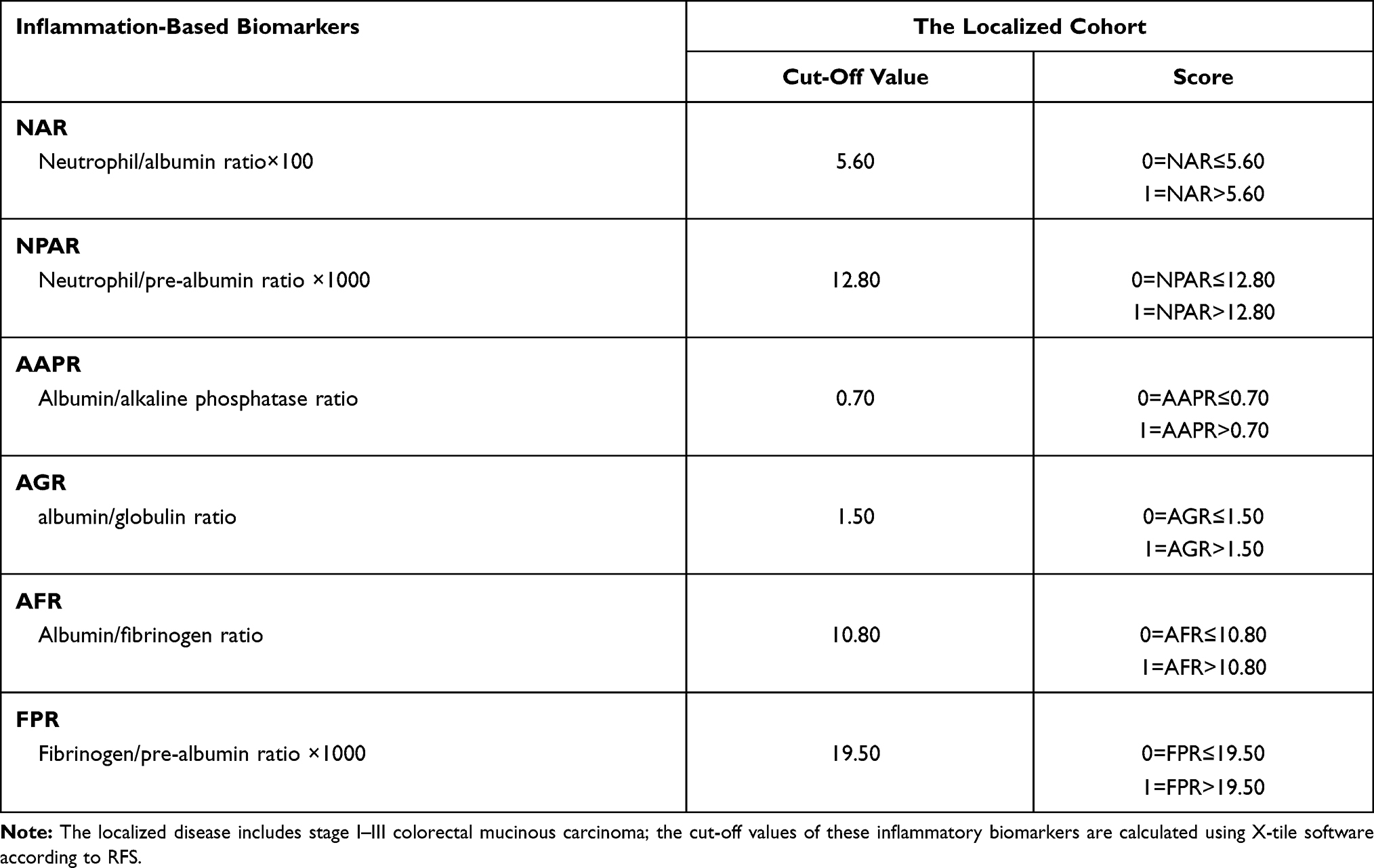 |
Table 1 Definition and Cut-Off Values of the Included Inflammatory Ratio in Predicting Recurrence in the Localized Patients |
The primary survival endpoint in our study was recurrence-free survival (RFS) in the cohort. We performed a three-years follow-up with a frequency of three months in the first two years, and six months subsequently until recurrence or metastasis in the third year or the deadline (April 1st, 2020). The time from resection to recurrence within the localized region or death was considered as RFS. Physical examination, tests for detecting common tumor biomarkers (CEA and CA19-9), and common imaging tests (abdominal computed tomography scan or magnetic resonance imaging) or colonoscopy were performed during follow-up. Contrast-enhanced chest abdominal computed tomography and bone scans were performed to detect lung and bone metastases, respectively. Recurrence or distal metastasis of the disease was diagnosed according to one of the following criteria: a) colonoscopy examination; and b) typical appearances in common imaging detection.
The cut-off values for AAPR, NAR, NPAR, AGR, AFR, and FPR were calculated using X-tile software according to RFS. Binary variables are summarized as numbers and frequencies. The chi-square test and Fisher’s exact tests were used to analyze the significant difference in the comparisons. Continuous variables are expressed as the median and quartiles, and were compared using the Kolmogorov–Smirnov and Mann–Whitney U-tests. The Kaplan-Meier curve with a Log rank test was used to assess the difference in RFS between the comparisons. Crude and adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using univariate and multivariate (backward LR method) Cox regression. A time-dependent receiver operating characteristic (ROC) curve was constructed to discriminate and compare the predicted efficacies of these inflammation-based ratios. All statistical analyses were performed using SPSS software 22.0 (IBM Corp, Armonk, NY, USA), R 3.5.1 (Institute for Statistics and Mathematics, Vienna, Austria) with the “rms”, “survival”, “survivalROC”, and “tdROC” packages, and GraphPad Prism 8.2.1 (GraphPad Software Inc., San Diego, USA). All analyses were two-sided, and statistical significance was set at p<0.05.
Results
Baseline Characteristics of Eligible Patients
As shown in Figure 1, 157 patients with stage I–III MCA patients were included in our study according to the inclusion and exclusion criteria. The baseline characteristics and laboratory detection results were described in Table 2. The majority of patients were aged <60 years old (61.78%), and 42.04% of the patients had tumor on the right side. The proportions of patients with stage I, II, and III MCA were 7(4.46%), 71 (45.22%), and 79 (50.32%), respectively. All localized lesions were resected, 77.71% and 11.46% of the included patients received adjuvant chemotherapy and radiotherapy, respectively. The recurrence rate was 38.85% after the follow-up, and the median RFS was 36 months.
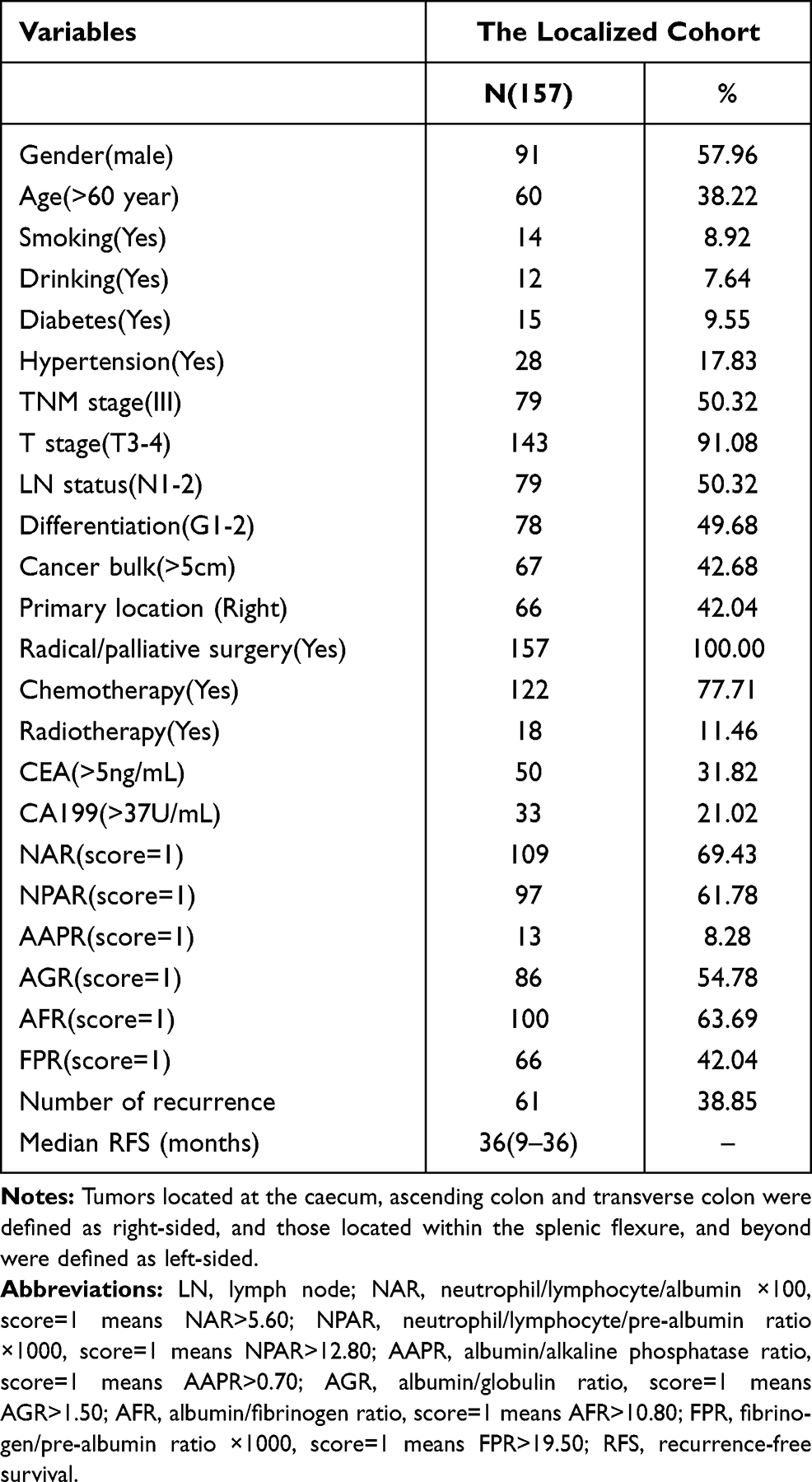 |
Table 2 The Baseline and Clinicopathological Characteristics of Eligible Patients in the Localized Cohort |
Prognosis of Inflammatory Scores
The optimal cut-off values of NAR, NPAR, AAPR, AGR, AFR, and FPR were 5.60, 12.80, 0.70, 1.50, 10.80, and 19.50, respectively (Table 1). The patients were stratified into high- (score 1) and low-score (score 0) subgroups according to the cut-off values of the six inflammatory ratios. However, only TNM stage (p<0.001, adjusted HR=3.664, 95% CI=1.813–7.404), CEA (p=0.018, adjusted HR=2.346, 95% CI=1.161–4.742), CA199 (p<0.005, adjusted HR=2.848, 95% CI=1.377–5.890), NAR (p=0.025, adjusted HR=2.280, 95% CI=1.111–4.678), NPAR (p=0.004, adjusted HR=2.818, 95% CI=1.399–5.674), and FPR (p=0.025, adjusted HR=2.359, 95% CI=1.115–4.990) were found to be significantly associated with poor RFS in the Kaplan-Meier curve, univariate and multivariate Cox regression (Figure 2 and Table 3). Nonetheless, there was no association between AAPR, AGR, or AFR, and the RFS of the patients.
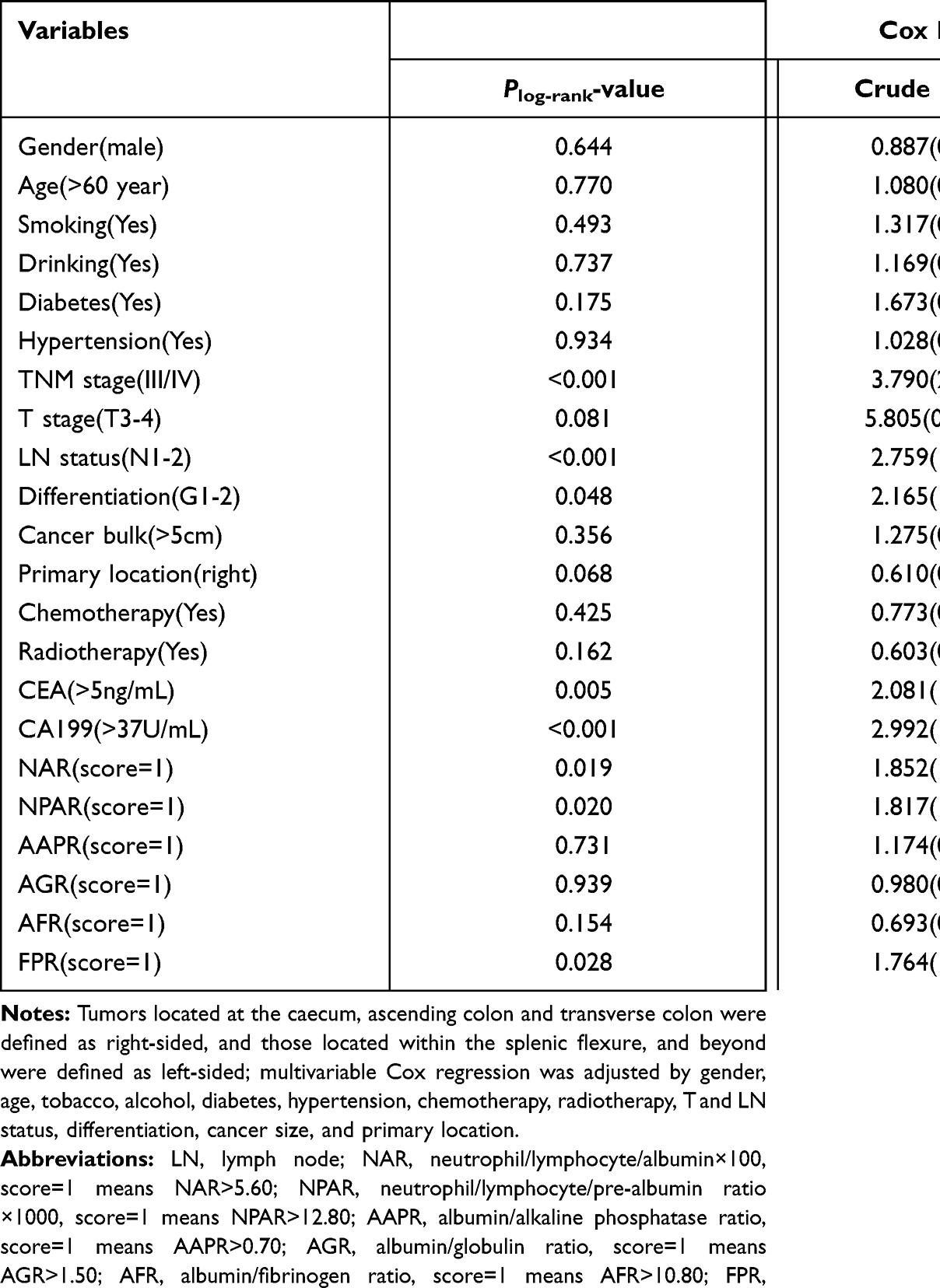 |
Table 3 The Relationship Between the Baseline and Pathological Variables, Inflammatory Ratios and Recurrence-Free Survival in the Localized Cohort |
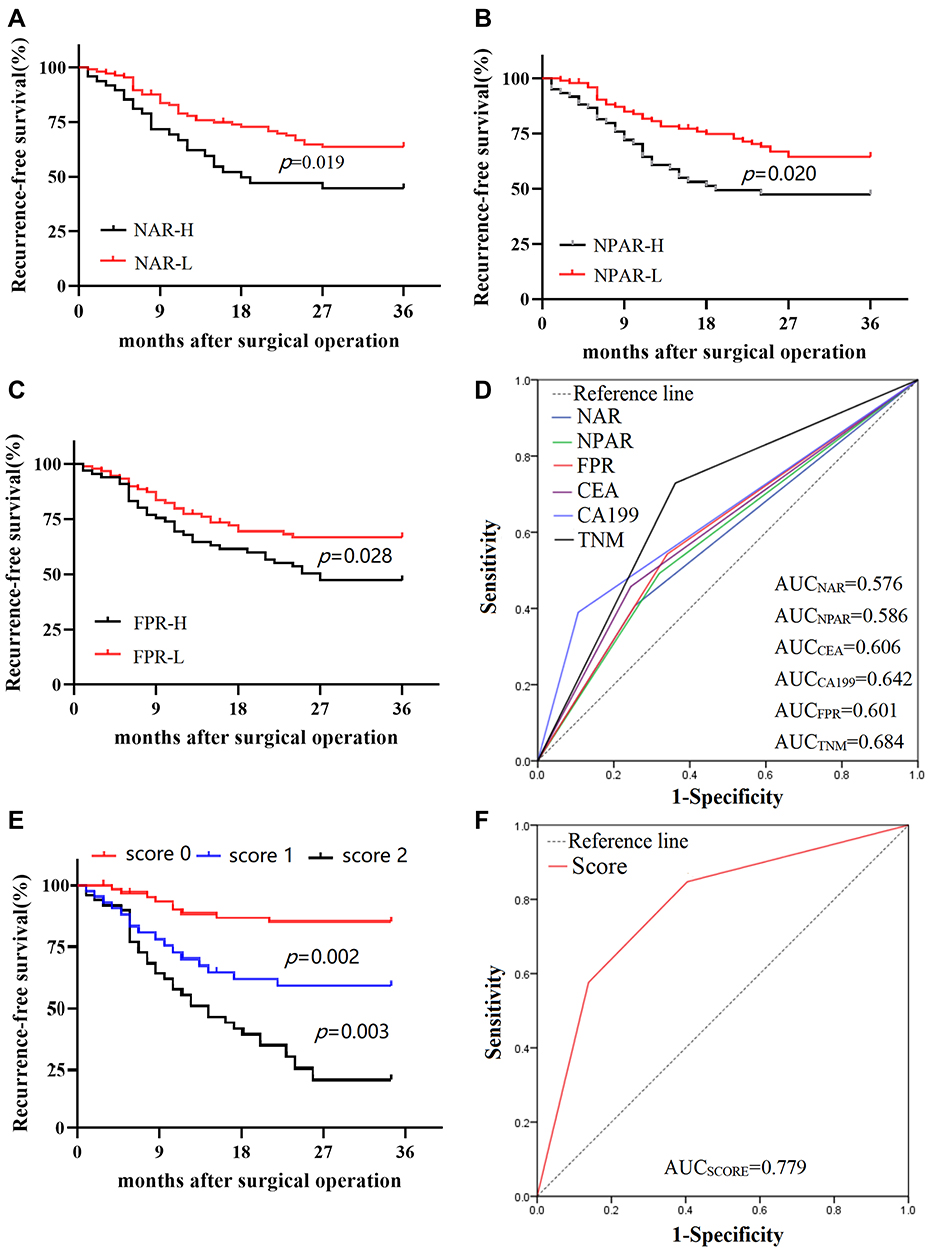 |
Figure 2 Prognostic values of the significant inflammatory biomarkers in the study. (A) Kaplan-Meier (K-M) curve of NAR; (B) K-M curve of NPAR; (C) K-M curve of FPR; (D) time-dependent receiver operating characteristics curve (tdROC) of the independent prognostic factors; (E) K-M curve of TNM-CA199-FPR score; (F) tdROC of TNM-CA199-FPR score. |
We also evaluated the predictive efficacy of the significant inflammatory ratios, CEA, CA199, and TNM in predicting 3-years RFS. Areas under time-dependent receiver operation curves (AUC) were 0.576 (AUC=0.576, 95% CI=0.481–0.670), 0.586 (AUC=0.586, 95% CI= 0.493–0.680), 0.601 (AUC=0.601, 95% CI=0.508–0.694), 0.606 (AUC=0.606, 95% CI= 0.513–0.700), 0.642 (AUC=0.642, 95% CI=0.548–0.735) and 0.684 (AUC=0.684, 95% CI=0.597–0.770) for NAR, NPAR, FPR, CEA, CA19-9, and TNM, respectively. The TNM stage had the highest AUC in predicting RFS. The AUC of FPR was higher than that of the other inflammatory biomarkers. The AUC of CEA was lower than that of CA19-9 (Figure 2D and Table 4).
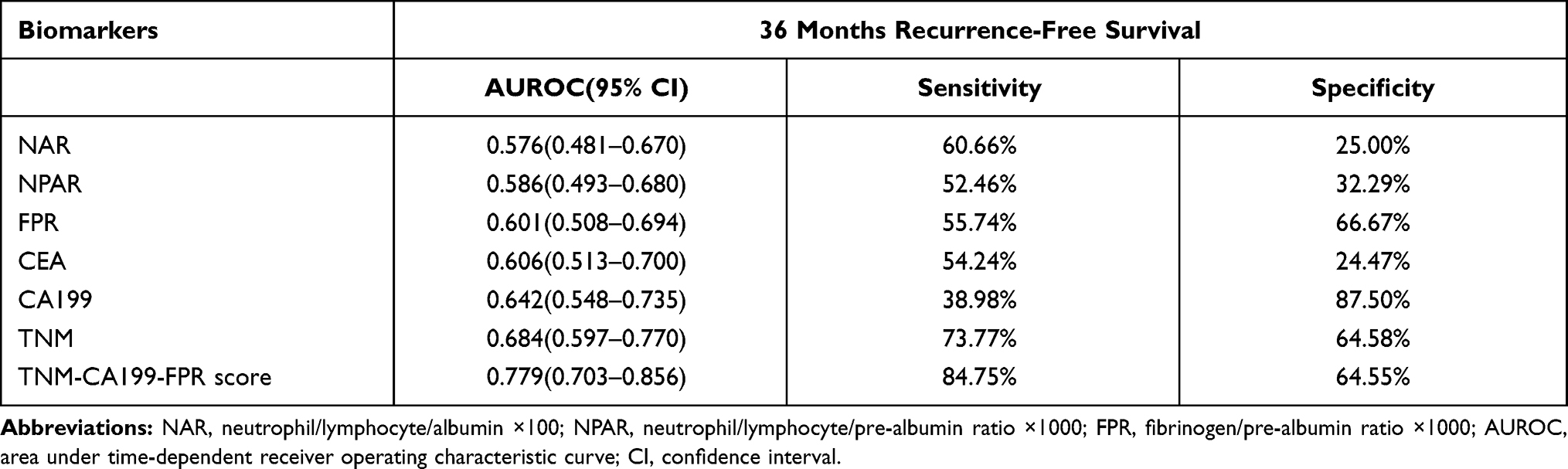 |
Table 4 Comparison of the Performance Discriminative Ability Between the Significant Prognostic Factors |
Prognosis and the Predicted Efficacy of the Combined Score
According to the prognostic roles of TNM (stages I–II and III defined as negative and positive TNM stages, respectively), CA19-9, and FPR in the patients, we constructed a combined score based on the three biomarkers. We considered score 0 for patients with the three low biomarkers or a single positive FPR, score 1 for these with stage III or high CA19-9 and score 2 for those with two or three positive biomarkers. Sixty-five (41.40%), 43 (27.39%), and 49 (31.21%) patients had scores of 0, 1, and 2, respectively. As shown in Figure 2E, the RFS of the patients with a combined score of 1 (plog-rank=0.002, adjusted HR=3.191, 95% CI=0.964–10.599) and 2 (plog-rank=0.003, adjusted HR=4.548, 95% CI=1.671–12.377) was extremely inferior to that of patients with score 0, and their predicted AUC was high (0.779), which was superior to that of the single biomarkers such as TNM, CA19-9, and FPR. Moreover, the sensitivity and specificity of the combined score were 84.75% and 64.55%, respectively, in predicting the 3-year RFS (Figure 2F; Tables 4 and 5).
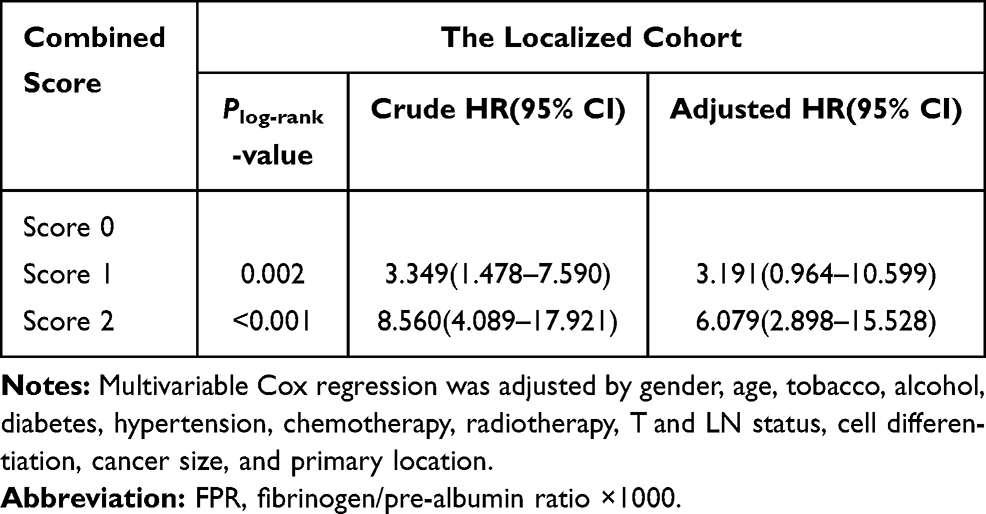 |
Table 5 Cox Analysis of TNM-CA199-FPR Score in the Localized Cohort |
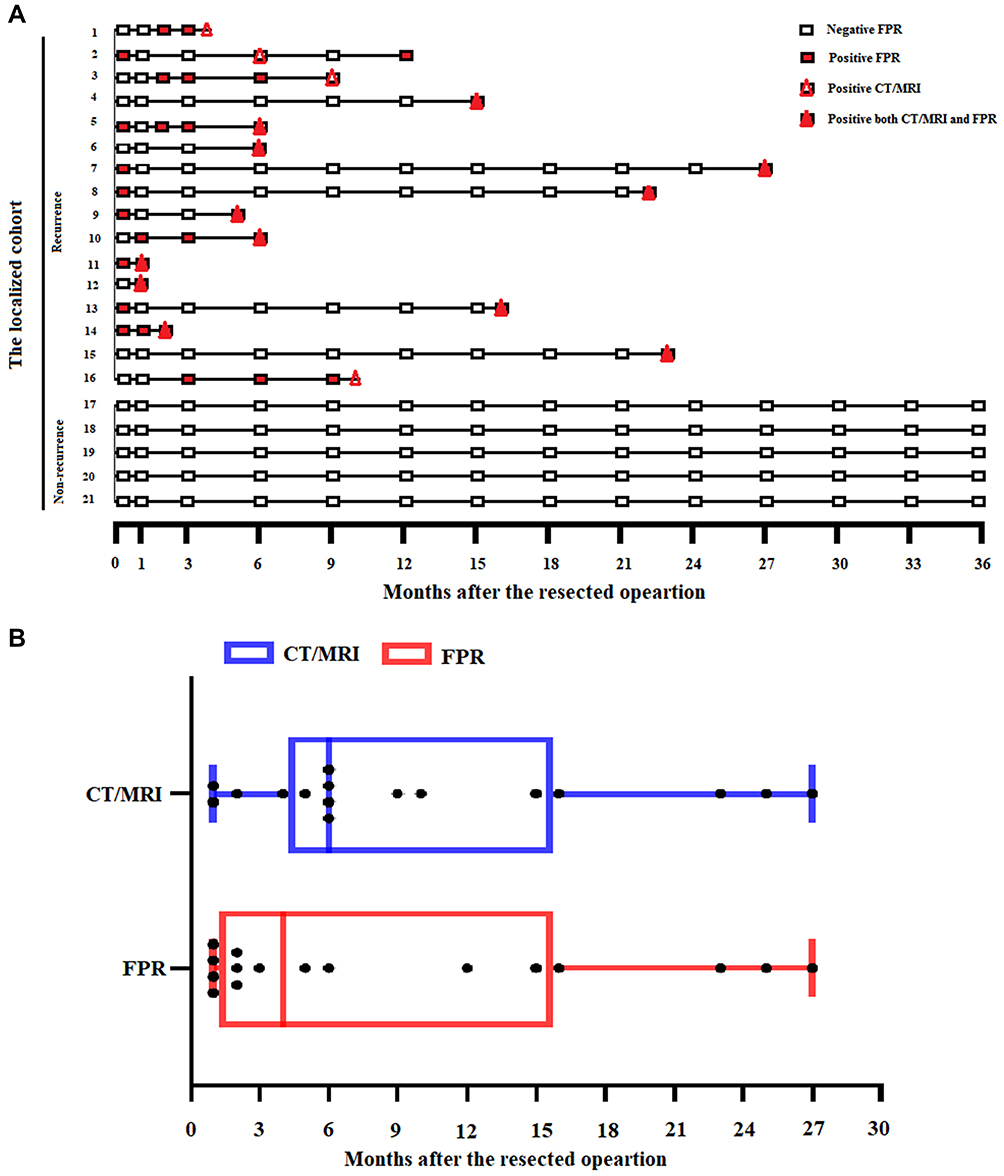 |
Figure 3 FPR monitoring for recurrence in 21 MCA patients. Zero months means the time before the surgical operation in the localized cohort, the other detected points were after the surgical operation. (A) CT/MRI and circulating FPR detection in 21 MCA patients in the follow-up period. (B) comparison of median months between appearance time of positive FPR and CT/MRI detection in monitoring recurrence of MCA patients. |
Predicting the Role of FPR in Monitoring Progression
To investigate the monitor role of FPR in predicting progression, we determined FPR during each follow-up. However, we obtained the complete data from only 21 patients during the follow-up period. Among them, 5 cases did not recur after surgical resection, and negative FPR was examined in each follow-up time. Sixteen patients were found to recurrence, and the first positive FPR detected time within 6 and 9 patients were earlier than or equal to the imaging detection after the operation, respectively. In only one patient, we found that the first positive FPR detection time was later than that in imaging detection (Figure 3).
Discussion
MCA accounts for approximately 1.6%~25.4% of all colorectal cancers,17,18 and is associated with a high recurrence rate and unsatisfactory clinical outcome.19 In this study, we found that NAR, NPAR, and FPR were significantly associated with unsatisfactory RFS in the cohort, and the predictive AUC of FPR was superior to that of the other two inflammatory biomarkers. Moreover, the patients with a high combined TNM-CA199-FPR score showed worse outcomes than that of the low score patients, and the predicted efficacy was high up to 0.779, which was significantly improved comparing to that of single biomarkers.In addition, FPR aided in monitoring recurrence up to two months earlier than that achieved using the common imaging techniques in patients with localized lesions.
MCA is a unique subtype of CRC, as it has distinct clinical and histological characteristics and genetic features.1 A previous study showed that MCA was mainly observed in female and younger populations;20 our study showed that 57.96% of the patients were male, and the middle-younger patients accounted for 61.78% of all eligible patients, consistent with findings reported by Song et al.21 Meanwhile, 42.04% of patients with localized lesions had a high FPR. Accumulating evidence showed that a high FPR within the patients indicated a high-degree of chronic inflammation,22 and severe cancer-related inflammation could weaken or lead to chemoradioresistence,16 which leads to unsatisfactory clinical outcomes in CRC patients.8 Thus, the recurrence rate in the cohort was high (38.85%).
Previous studies have shown that the common prognostic factors, such as TNM stage, venous and lymphoid invasion, microsatellite instability (MSI) status, CEA, and CA19-9 are associated with the prognosis of MCA.23–25 However, there was a need for an improved predicted efficacy. In our study, we found that stage III, high CA19-9 and high CEA were related to the worse survival. Recent studies have shown that cancer-elicited inflammatory biomarkers (neutrophil-to-lymphocyte ratio, AFR, and FPR) are promising prognostic biomarkers for the localized and metastatic CRC.8,16,22,26,27 Moreover, circulating FPR was the preferred inflammatory biomarkers in predicting recurrence in patients with stage II–III CRC patients in terms of prognostic ability.22 Furthermore, NAR, NPAR, and FPR were associated with short RFS adjusted by common characteristics and other confounders. This suggests that these variables could be considered as independent prognostic factors to predict disease progression.In addition, the predicted efficacy and sensitivity of the combined TNM-CA199-FPR score were high, up to 0.779 and 84.75%, respectively; these values were significantly higher than those of individual factors. The revealed that the combined score improves the predicted efficacy of the individual factors, and it is economical, simple, and effective in predicting disease recurrence. Moreover, FPR is a better index that aids in monitoring recurrence (up to two months earlier) than the common imaging detection in patients with localized lesions. Thus, FPR detection at each follow-up would possibly help help clinicians to select an effective therapeutic strategy to improve the clinical outcome of these patients.
To the best of our knowledge, this is the first attempt to report the prognostic role of the six inflammatory ratios in MCA, and the combined score can effectively predict the recurrence in patients with localized lesions. Nonetheless, the following shortcomings were encountered in our study. First, this was a retrospective study. Therefore, selection bias might have affected our results. Second, the number of participants in our study was only 157, and all participants were recruited from a single hospital. Thus, the study findings and cut-off values of these inflammatory biomarkers need to be validated by multi-centers designed studies with a large sample size. Thirdly, alterations in the fundamental genes of the MAPK pathway and high microsatellite instability (MSI) status were more likely to be associated with MCA.1,28 However, we did not detect RAS and BRAF mutations or MSI status. Thus, we did not determine the relationship between molecular features and FPR, as well as their predicted efficacies.
Conclusions
In summary, FPR is a preferred parameter in monitoring the recurrence in stage I–III MCA patients after surgery. The combined TNM-CA199-FPR score is an economical, simple, effective, and independent prognostic factor for predicting the recurrence of the patients. Our findings may help surgeons and oncologists to accurately predict and to monitor disease progression, thereby warranting future multicenter prospective studies for verification.
Acknowledgment
We would like to thank Editage for English language editing.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Luo C, Cen S, Ding G, Wu W. Mucinous colorectal adenocarcinoma: clinical pathology and treatment options. Cancer Commun. 2019;39(1):13. doi:10.1186/s40880-019-0361-0
2. Gao P, Song YX, Xu YY, et al. Does the prognosis of colorectal mucinous carcinoma depend upon the primary tumour site? Results from two independent databases. Histopathology. 2013;63(5):603–615. doi:10.1111/his.12190
3. Kim SH, Shin SJ, Lee KY, et al. Prognostic value of mucinous histology depends on microsatellite instability status in patients with stage III colon cancer treated with adjuvant FOLFOX chemotherapy: a retrospective cohort study. Ann Surg Oncol. 2013;20(11):3407–3413. doi:10.1245/s10434-013-3169-1
4. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. doi:10.1038/nature01322
5. Hugen N, van Beek JJ, de Wilt JH, Nagtegaal ID. Insight into mucinous colorectal carcinoma: clues from etiology. Ann Surg Oncol. 2014;21(9):2963–2970. doi:10.1245/s10434-014-3706-6
6. Drew DA, Cao Y, Chan AT. Aspirin and colorectal cancer: the promise of precision chemoprevention. Nat Rev Cancer. 2016;16(3):173–186. doi:10.1038/nrc.2016.4
7. Sun F, Tan YA, Gao QF, et al. Circulating fibrinogen to pre-albumin ratio is a promising biomarker for diagnosis of colorectal cancer. J Clin Lab Anal. 2019;33(1):e22635. doi:10.1002/jcla.22635
8. Sun F, Peng HX, Gao QF, et al. Preoperative circulating FPR and CCF score are promising biomarkers for predicting clinical outcome of stage II-III colorectal cancer patients. Cancer Manag Res. 2018;10:2151–2161. doi:10.2147/CMAR.S167398
9. Guo X, Zou Q, Yan J, Zhen X, Gu H. Prognostic effect of pretreatment albumin-to-alkaline phosphatase ratio in human cancers: a meta-analysis. PLoS One. 2020;15(8):e0237793. doi:10.1371/journal.pone.0237793
10. Tingle SJ, Severs GR, Goodfellow M, Moir JA, White SA. NARCA: a novel prognostic scoring system using neutrophil-albumin ratio and Ca19-9 to predict overall survival in palliative pancreatic cancer. J Surg Oncol. 2018;118(4):680–686. doi:10.1002/jso.25209
11. Chi J, Xie Q, Jia J, et al. Prognostic Value of Albumin/Globulin Ratio in Survival and Lymph Node Metastasis in Patients with Cancer: a Systematic Review and Meta-analysis. J Cancer. 2018;9(13):2341–2348. doi:10.7150/jca.24889
12. Li SQ, You XH, Sun F, et al. Albumin to fibrinogen ratio and fibrinogen to pre-albumin ratio are economical, simple and promising prognostic factors for solid malignancy. J Thorac Dis. 2019;11(Suppl15):S2036–S2038. doi:10.21037/jtd.2019.08.96
13. Zhang J, Li SQ, Liao ZH, et al. Prognostic value of a novel FPR biomarker in patients with surgical stage II and III gastric cancer. Oncotarget. 2017;8(43):75195–75205. doi:10.18632/oncotarget.20661
14. Li SQ, Jiang YH, Lin J, et al. Albumin-to-fibrinogen ratio as a promising biomarker to predict clinical outcome of non-small cell lung cancer individuals. Cancer Med. 2018;7(4):1221–1231. doi:10.1002/cam4.1428
15. Gao QF, Qiu JC, Huang XH, et al. The predictive and prognostic role of a novel ADS score in esophageal squamous cell carcinoma patients undergoing esophagectomy. Cancer Cell Int. 2018;18:153. doi:10.1186/s12935-018-0648-2
16. Chen QG, Zhang L, Sun F, et al. Elevated FPR confers to radiochemoresistance and predicts clinical efficacy and outcome of metastatic colorectal cancer patients. Aging. 2019;11(6):1716–1732. doi:10.18632/aging.101864
17. Pande R, Sunga A, Levea C, et al. Significance of signet-ring cells in patients with colorectal cancer. Dis Colon Rectum. 2008;51(1):50–55. doi:10.1007/s10350-007-9073-7
18. Papadopoulos VN, Michalopoulos A, Netta S, et al. Prognostic significance of mucinous component in colorectal carcinoma. Tech Coloproctol. 2004;8(Suppl 1):s123–5. doi:10.1007/s10151-004-0131-z
19. Yu F, Huang L, Shen F, Wu S, Chen J. Prognostic implications of mucinous histology in stage III colon cancer with the receipt of adjuvant chemotherapy. J Gastrointest Oncol. 2020;11(5):858–869. doi:10.21037/jgo-20-160
20. Ahnen DJ, Wade SW, Jones WF, et al. The increasing incidence of young-onset colorectal cancer: a call to action. Mayo Clin Proc. 2014;89(2):216–224. doi:10.1016/j.mayocp.2013.09.006
21. Song W, He YL, Cai SR, et al. [Clinical features of colorectal mucinous adenocarcinoma]. Zhonghua Wei Chang Wai Ke Za Zhi. 2009;12(5):487–490. Chinese.
22. Liao YC, Ying HQ, Sun F, Peng HX. The role of cancer-elicited inflammatory biomarkers in predicting early recurrence within stage II-III colorectal cancer patients after curable resection. J Inflamm Res. 2021;14:115–129.
23. Triki M, Kallel R, Feki J, et al. Prognostic significance of E-cadherin and Cox 2 expression in Tunisian patients with colorectal mucinous adenocarcinoma. Ann Diagn Pathol. 2020;49:151624. doi:10.1016/j.anndiagpath.2020.151624
24. Li ZP, Liu XY, Kao XM, et al. Clinicopathological characteristics and prognosis of colorectal mucinous adenocarcinoma and nonmucinous adenocarcinoma: a surveillance, epidemiology, and end results (SEER) population-based study. Ann Transl Med. 2020;8(5):205. doi:10.21037/atm.2020.01.52
25. Huang Q, Zou MH, Jiang Y, et al. Outcomes of Laparoscopic Surgery for Mucinous Colorectal Adenocarcinoma. J Laparoendosc Adv Surg Tech A. 2020. doi:10.1089/lap.2020.0588
26. Malietzis G, Giacometti M, Askari A, et al. A preoperative neutrophil to lymphocyte ratio of 3 predicts disease-free survival after curative elective colorectal cancer surgery. Ann Surg. 2014;260(2):287–292. doi:10.1097/SLA.0000000000000216
27. Ying HQ, Deng QW, He BS, et al. The prognostic value of preoperative NLR, d-NLR, PLR and LMR for predicting clinical outcome in surgical colorectal cancer patients. Med Oncol. 2014;31(12):305. doi:10.1007/s12032-014-0305-0
28. Reynolds IS, Thomas V, O’Connell E, et al. Mucinous Adenocarcinoma of the Rectum: a Whole Genome Sequencing Study. Front Oncol. 2020;10:1682. doi:10.3389/fonc.2020.01682
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.