")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Risky Sexual Practice and Associated Factors Among Women Living with HIV/AIDS Receiving Antiretroviral Therapy at a PMTCT Clinic in Western Oromia, Ethiopia
Authors Balis B
Received 18 April 2020
Accepted for publication 21 October 2020
Published 16 November 2020 Volume 2020:12 Pages 739—747
DOI https://doi.org/10.2147/HIV.S258740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Bikila Balis
Department of Midwifery, School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Western Oromia, Ethiopia
Correspondence: Bikila Balis
School of Nursing, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Tel +251 921788619
Email [email protected]
Background: Human immunodeficiency virus infection has been one of the top health-related challenges for the past four decades. Ethiopia is extremely infected by HIV pandemic every year, whereby 22,300 people were newly infected and 690,000 were living with HIV at the end of 2018. Sexual behavior of HIV positive individuals visiting treatment clinics is a neglected issue. Nonetheless, it has been a significant way of HIV transmission to serodiscordant partners.
Methods: A facility-based cross-sectional study design was used on a sample of 432 women attending treatment clinics in west Oromia from February 26 to March 26, 2019. Systematic sampling was used to select the study participants. A pretested and structured interviewer-administered questionnaires were used to collect the data. The data were coded, entered, cleaned and exported to SPSS version 20.0 for analysis. Descriptive statistics were used to present frequency distributions. Variables with P-value < 0.25 during bivariate analysis were entered into multiple logistic regression models to control for all possible confounders. Odds ratio along with 95% CI were estimated to measure the strength of the association. Level of statistical significance was declared at a p-value less than 0.05.
Results: Out of total respondents, 240 (56.9%), 95% CI: (52.1– 61.6%) were involved in risky sexual practices in the prior 12 months. Urban residence [AOR: 3.24, (95% CI: (1.52, 6.89)], those with no formal education [AOR: 2.77, (95% CI: (1.18, 6.54)], being on ART for > 2years [AOR: 2.74, (95% CI: (1.13, 6.65)] and CD4 count ≥ 200 cells/mm3 [AOR: 3.20, (95% CI: (1.50, 6.82)] were factors significantly associated with risky sexual practice.
Conclusion: A considerable number of respondents were involved in risky sexual practices 240 (56.9%) due to being rural residence, not attending formal education, being on ART for > 2 years and CD4 count ≥ 200 cells/mm3.
Keywords: women, HIV/AIDS, risky sexual practices, Oromia, Ethiopia
Introduction
Human immunodeficiency virus (HIV) infection has been one of the top health-related challenges for the past four decades.1,2 Accordingly, at the end of 2017, 1.6 million adults (>15 years) were newly infected and 37.9 million people were living with HIV across the world by the end of 2018.2,3 This is especially imperative for sub-Saharan Africa nations which bear 69% of the world’s HIV/AIDS burden. Sub-Saharan Africa remains among the hardest hit regions by the pandemic, over 800 000 people were newly infected and 19.6 million people were living with HIV/AIDS by the end of 2017.3
Ethiopia is one of the sub-Saharan countries which is extremely infected by HIV/AIDS pandemic every year, whereby more than 2700 children (≤ 15 years) and 19,600 adults (> 15 years) were newly infected and 690,000 people were living with HIV/AIDS by the end of 2018.2 The annual number of HIV infected people showed declining trends since 2010 from 0.39% to 0.24% in 2018.2,4 Similarly, the prevalence of PLHIV showed declining trends since 2010 from 1.3% to 1% in 2018.2,4 Risky sexual behaviours contribute to the high HIV prevalence in Ethiopia.5 Risky sexual practices are defined as inconsistent and/or no condom use with partner of HIV negative or unknown sero-status.6,7
The expansion of antiretroviral therapy (ART) services has transformed HIV/AIDS into a controllable chronic illness and has decreased morbidity and mortality from HIV/AIDS.5,8–10 Hence, most of the individuals receiving antiretroviral therapy show good physical improvements and feel healthier.5,8–10 This improvement may increase sexual desire and unprotective sexual behaviors of individuals.6,7 On the other hand, this leads to reinfection with new drug resistant viral strains and transmits the infection to their respective serodiscordant sexual partners, mother to child transmission (MTCT), the transmission of sexually transmitted infections5,11 and unintended pregnancy.5,12,13
Sexual behavior of HIV positive individuals visiting ART and PMTCT clinics is a neglected issue.14–16 Evidence show 20–80% of people living with HIV/AIDS continue to engage in risky sexual behaviors in sub-Saharan countries.16–19 However, there are controverting ideas on the risk of sexual practices of HIV positive individuals who are on ART. Some studies suggest risky sexual practices declined among individuals on HIV treatment because of the detailed counseling they were getting during their ART follow-ups; others claimed that it revealed increases after the initiation of ART because of the physical well-being that followed ART initiation; still, others concluded ART has no effect on it. Factors frequently associated with risky sexual practices were socio-demographics, fertility related, ART related and partner related conditions.16,17,20–22
Many studies show a high incidence of STI during ART treatment14,18,23–26 and continued fertility desire among those living with HIV,27–31 both suggesting the aspiration for and practice of unprotected sex. Ethiopia is primarily focusing on people uninfected with HIV and the sexual risk practices of HIV infected individuals did not receive due attention. Also, little is known about risky sexual practices and studies were confined in a single health facility. Therefore, this study aimed to determine the magnitude of risky sexual practices and associated factors among clients living with HIV/AIDS attending a range of health facility ART and PMTCT clinics in western Oromia, Ethiopia.
Methods
Study Setting, Design and Period
The study was conducted in western Oromia zone which is one of the 20 zones. Gimbi is the capital city of the zone which is 441 km away from Addis Ababa and located at an altitude of 1885 m above sea level. According to 2007 Statistical Report of the Population and Housing Census of Ethiopia, West Wollega Zone has a total population of 1,350,415, of whom 671,538 are men and 678,877 women; with an area of 10,833.19 square kilometers, West Wollega has a population density of 124.66.32 There were 26 public and one non-governmental health institutions that provide ART and PMTCT in addition to the other health services for the community, six of which were hospitals and the remaining 21 were health centers. A total of 2852 adult clients were on ART in West Oromia. A facility-based, cross-sectional study design was used from February 26 to March 26, 2019.
Study Participants, Sampling Methods and Sample Size Determination
The study participants were all ART and PMTCT attendees who had at least one visit to the selected health facilities during the study period. Women who were post menopausal, term pregnant, postpartum (< 42 days after giving birth) or divorced from their partners were excluded where as all HIV positive women who had at least one visit to the selected health facilities during the study period for the ART and PMTCT services were included.
The health facilities found in the zone were first stratified into hospitals and heath centers. From each strata, three hospitals and five health centers were obtained by simple random sampling. The sample from each hospital and health center were allocated proportionally to the number of clients on ART at each health facility. A systematic random sampling technique was used to select the study participants. The sampling interval was determined based on the number of patients who came for follow up to the ART clinic each month. The average number of patients who came to the ART clinic for follow up during the study period was estimated at 1024. By considering the monthly client flow for follow up, the sampling interval was two. The first participant was chosen by simple random sampling methods which was four. Then the rest of the participants were obtained from each facility by every two interval.
The sample size was determined based on predictors of number of current partner; and using statistical Epi info 7 stat calculator computer software program using 95% CI with Z=1.96, cross-sectional ratio1:1, the proportion of multiple partners about MTCT 56.7% and single partner 34.8% and 80% power, 15% non-response (n=432).33 Therefore a total of 432 clients who were on ART for six months were included in the study.
Data Collection Instrument and Measurement
The questionnaires were adapted from EDHS 2011 and Ethiopian federal ministry of health ART clinic intake and follow up form.5,34 It had three parts; sample characteristics, HIV related knowledge and risky sexual practices. The dependent variable was risky sexual practices (inconsistent and/or no condom use with partner of HIV negative or unknown sero-status or situation such as having multiple sexual partners in the last 12 months preceding the study), and the independent variables included sociodemographic characteristics such as age, marital status, religion, residence (urban/rural), occupational status, duration since ART commencement, duration since HIV diagnosis, partner’s disclosure status and knowledge related to HIV.
A binary scale (yes/no) was employed to measure the general awareness regarding risky sexual practices among HIV clients. The number of “yes” or “no” answers were considered to examine participants’ awareness for specific topics related to risky sexual practices. Participants’ responses as “yes” or “no” for a given statement on the questionnaire were treated separately and a proportion of respondents who said yes or no for a single question were discussed instead of how many questions answered.
Quality Control and Data Collection
Five percent30 of the questionnaires were pre-tested in other health facilities that provide ART services. Then, ambiguous questions were corrected and rephrased before actual data collection. The questionnaire was initially prepared in English and then translated into Afan Oromo (local language of the study area) by those proficient in the language and then back into English to ensure linguistic consistency and to make effective pretest. The data collectors and supervisors were trained for two days about the objectives of the study, contents of tools and technique of interview before data collection started.
After this, clients who consented to participate were pretested and structured interviewer-administered questionnaires were used to collect the data in an isolated, private room found close to the ART clinic. The data were collected by eight trained nurses that work at ART clinics and four supervisors participated in monitoring the whole data collection process closely on a regular basis. After the first participants were obtained by the lottery method, the others were obtained by systematic sampling. The data were collected by eight trained diploma nurses who work at ART clinics and four BSc nurse supervisors were monitoring the whole data collection process closely on a regular basis.
Data Processing and Analysis
The data were coded, double entered into Epi data version 3.1, cleaned and exported to SPSS version 20.0 for analysis. Multi co-linearity test was carried out to see the correlation between independent variables by using standard error and co-linearity statistics. Variables with variance inflation factor >10 and/standard error >2 were dropped. Also, the fitness of the model was tested by the Hosmer-Lemeshow goodness of fit test which was 0.86.
Descriptive statistics were used to present frequency distributions. Bivariate analysis was employed to identify factors associated with risky sexual practices. Variables with P value < 0.25 during bivariate analysis were entered into the multiple logistic regression model to control for all possible confounders to identify factors associated with risky sexual practices. Odds ratio along with 95% CI were estimated to measure the strength of the association. Level of statistical significance was declared at a p-value less than 0.05.
Ethical Considerations
Ethical clearance was obtained from Haramaya University, College of Health and Medical Sciences, Institutional Health Research Ethics Review Committee (HU-IHRERC). A formal letter of permission and support was written to each hospital and health bureau from Haramaya University. Then the health bureau was written a cooperation letter to each health center. Participants were informed of the purposes, procedures, risks and benefits, and the private and confidential nature of the study. More importantly, written informed consent was obtained from each participant and the facility’s head. This study was conducted in accordance with the Declaration of Helsinki.
Results
Sample Characteristics
In this study, a total of 422 respondents were interviewed out of 432, with a response rate of 97.7%. Among the respondents, the majority, 260 (61.6%), were women and 180 (42.7%) were their male partners all found between the age of 18–29 years. The mean (±SD) age of women was 29.13 (± 7.48) years, whereas the mean (±SD) age of the male partners was 33.47 (± 9.06) years. Concerning ethnicity, most of the respondents, 315 (74.6%), were Oromo and 199 (47.2%) of the respondents were Protestant by religion. Concerning the duration of HIV diagnosis, two-thirds, 281 (66.6%), of respondents stayed more than two years since HIV diagnosis and 244 (57.8%) were on ART for more than two years (Table 1).
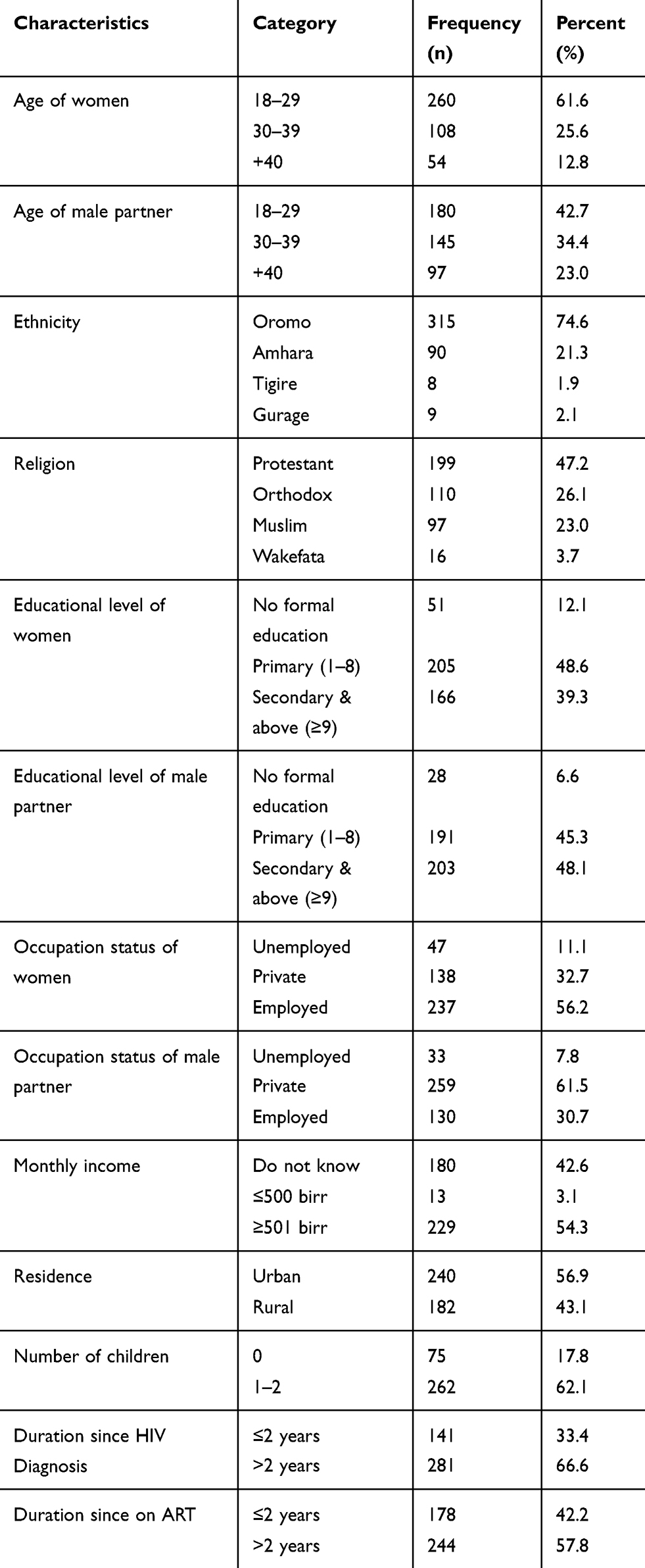 |
Table 1 Sample characteristics of respondents living with HIV/AIDS attending ART and PMTCT services (n=422) in West Oromia, Ethiopia, 2019 |
HIV Related Knowledge
The majority, 397 (94.1%), of respondents were knowledgeable about MTCT. More than three fourths, 348 (82.5%) of respondents had CD4 count ≥200 cells/mm3 and 339 (80.3%) of them reported as their health worker were discussed childbearing and condom use (Table 2).
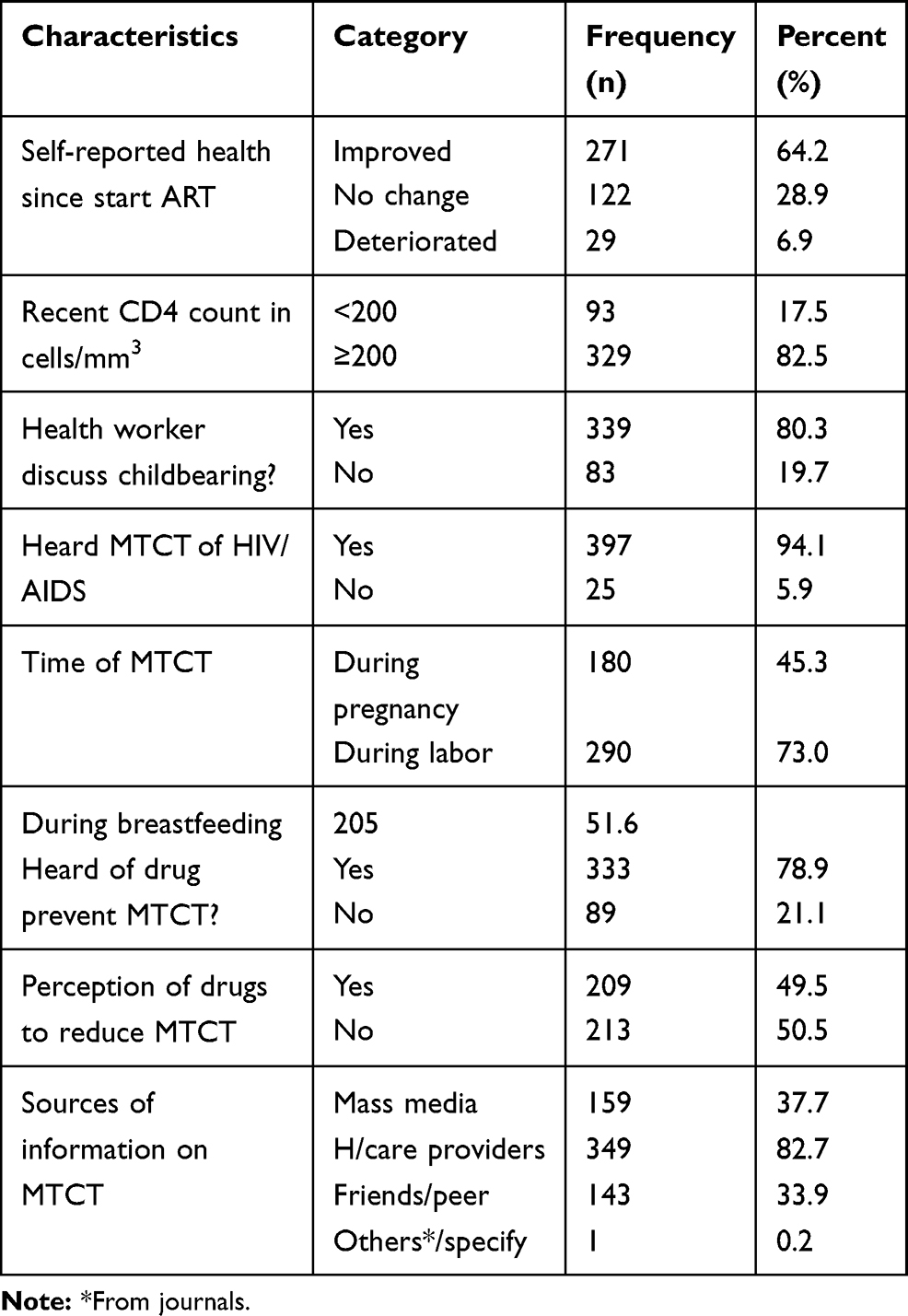 |
Table 2 HIV related knowledge of respondents living with HIV/AIDS attending ART and PMTCT services (n=422) in West Oromia, Ethiopia, 2019 |
Risky Sexual Practices
More than half, 240 (56.9%; 95% CI: 52.1%, 61.6%) of respondents were involved in risky sexual practices (condomless sex). The most common reason for not using a condom during sexual intercourse in the prior 12 months was that respondents were using other contraceptive methods, 96 (40.0%). A total of 377 (89.3%) respondents had disclosed their HIV status to their male partner and 165 (45.5%) respondents reported that their sexual desire was increased since being on treatment (Table 3).
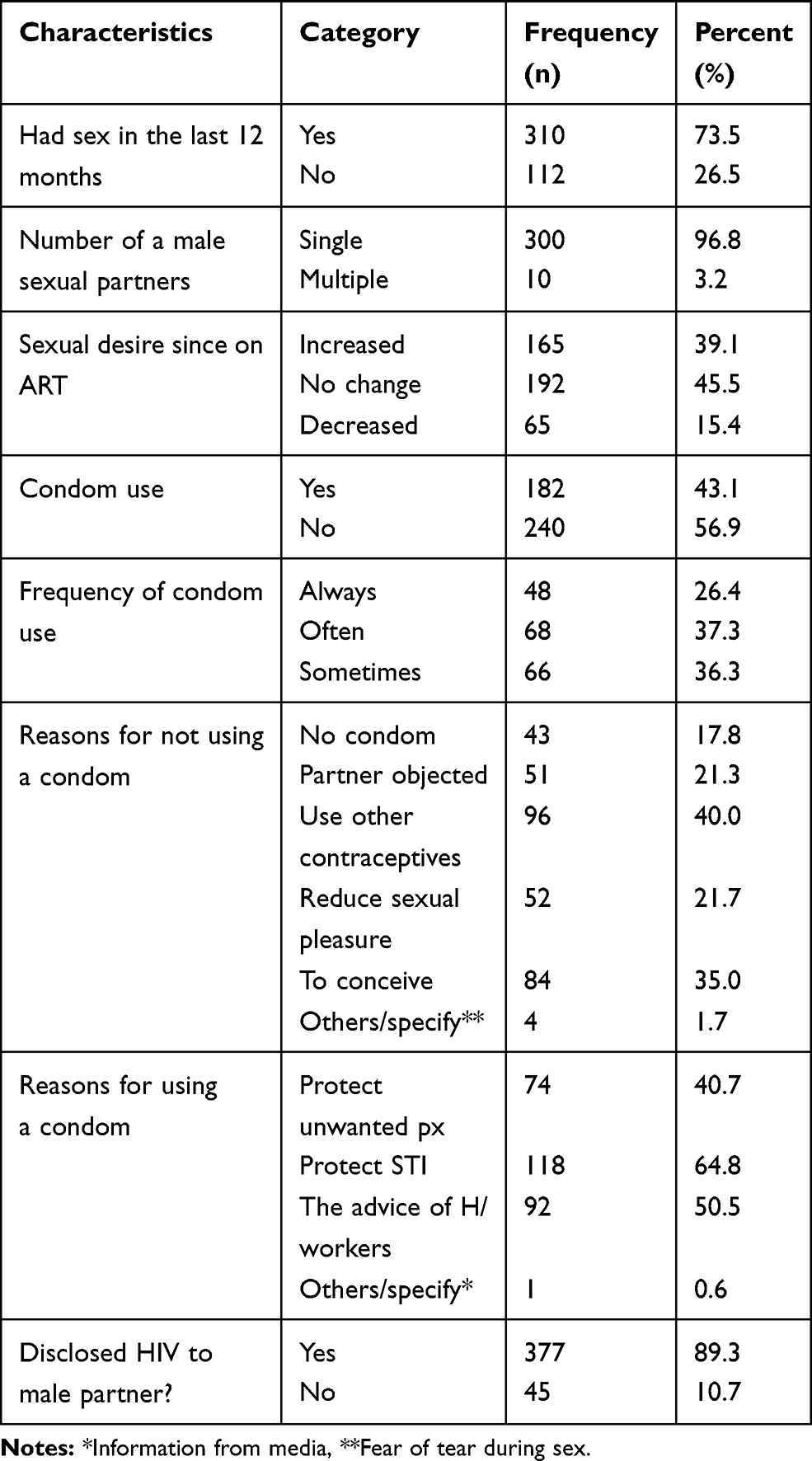 |
Table 3 Risky sexual practices of respondents living with HIV/AIDS attending ART and PMTCT services (n=422) in West Oromia, Ethiopia, 2019 |
Factors Associated with Risky Sexual Practices
In bivariate logistic regression, age of women, age of her male partner, residence, educational level of male partners, occupational status of male partners, number of children, duration since HIV diagnosis, duration on ART, HIV disclosure and CD4 count were factors significantly associated with risky sexual practices of respondents living with HIV/AIDS attending ART services.
However, in multiple logistic regression respondents living in urban areas were nearly three-fold [AOR: 3.24, (95% CI: (1.52, 6.89)] more likely to face risky sexual practices than those who were living in rural areas. Similarly, those with a male partner who had attended primary education were three times more likely to be involved in risky sexual practices [AOR: 2.77, (95% CI: (1.18, 6.54)], women who were on ART for more than two years were three [AOR: 2.74, (95% CI: (1.13, 6.65)] times more likely to engage in risky sexual practices than those who were on ART for less than two years and clients with CD4 count ≥200cells/mm3 were three times [AOR: 3.20, (95% CI: (1.50, 6.82)] more likely to be involved in risky sexual practices than whose with a CD4 count less than 200 cells/mm3(Table 4).
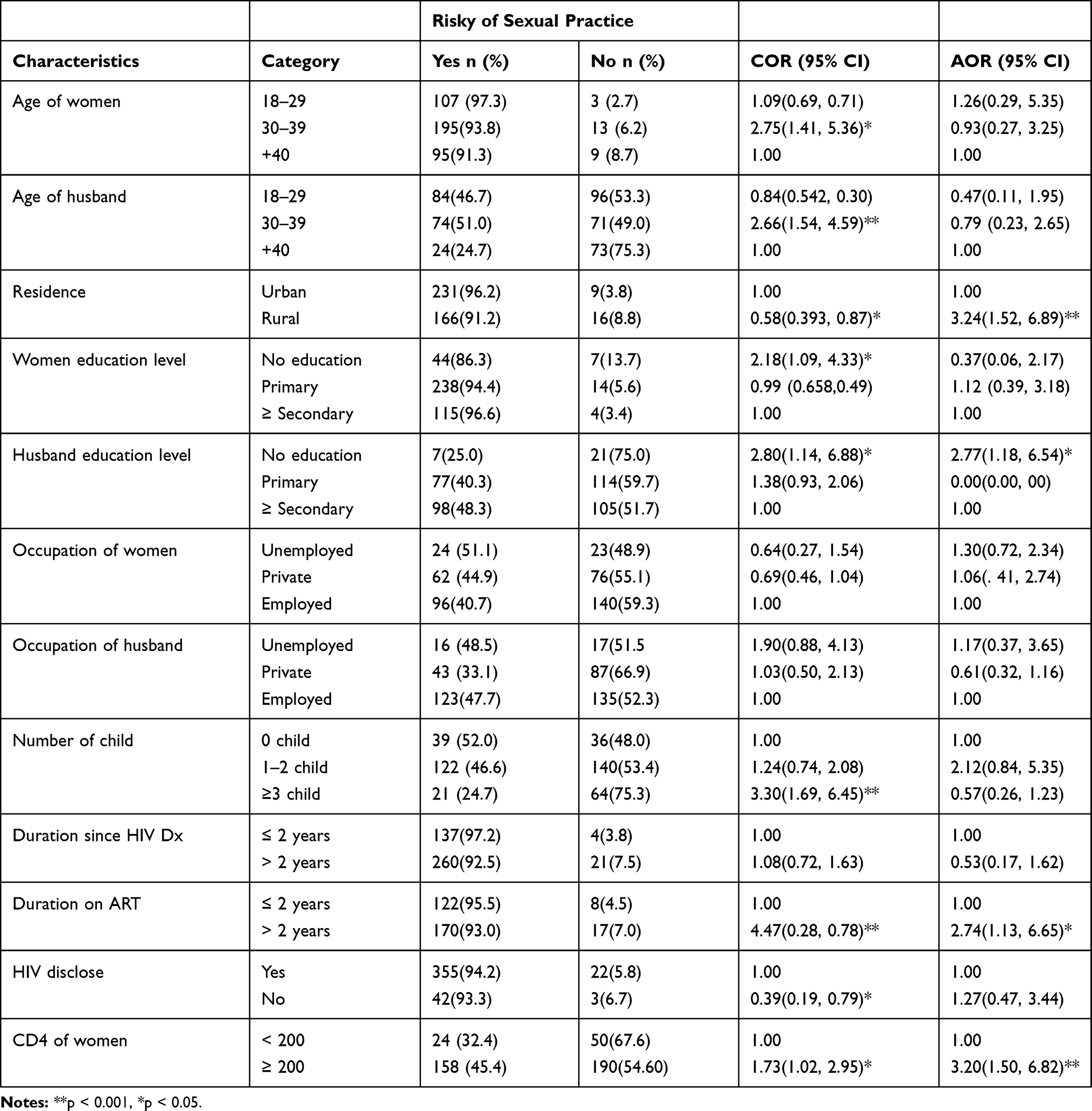 |
Table 4 Factors associated with the risky sexual practices among clients living with HIV/AIDS attending ART service (n=422) in West Oromia, Ethiopia, 2019 |
Discussion
There is little data regarding risky sexual practices among HIV positive clients in Ethiopia. This facility-based, cross-sectional study thus provides important information regarding the risky sexual practices among HIV positive clients as well as the associated factors.
More than half, 240 (56.9%), respondents were involved in risky sexual practices (condomless sex). This finding was higher than the study findings in Malawi 75 (37.9%), Western Ethiopia 55 (16.3%) and Northwest Ethiopia 63 (27.0%), 195 (38%).16,21,35,36 This difference might be due to the study being conducted among HIV positive clients with a high fertility desire rate, and respondents who were not exposed to health care counseling about condom use. Ten participants had multiple sexual partners in the past 12 months, which is in line with the study findings in Malawi 11 (5.5), Northwest Ethiopia 25 (9.3), Northern 49 (13.5%) and Western Ethiopia 15 (4.5 %).16,21,35,36
Concerning reasons for condom use, participants revealed that they were using for unwanted pregnancy prevention, following health care providers advice and prevention of sexually transmitted infections. This is compatible with study findings in Northwest, Northern, Western Ethiopia and Addis Ababa.17,21,22,37 Respondent’s reasons for not using condoms were that they were using other contraceptives, they wanted to conceive, partner objection and decreased sexual pleasure. This is congruent with study findings in Northwest, Northern, Western Ethiopia and Addis Ababa.17,21,22,37 Therefore, efforts should be strengthened on sexual health intervention focusing on the partners rather than the individual.
Participants who live in rural areas were three times more likely to engage in risky sexual practices than urban residents. This is inline with studies done in Northwestern Ethiopia,36 Northern Ethiopia16 and Nigeria.18 This is explained by the information gap that would exist between these areas. Rural residents could not access information through media and health facilities like urban residents. Similarly, respondents who did not attend formal education were almost three times more likely to engage in risky sexual practices compared to those without formal education. This was supported by study findings in Malawi,35 Northwestern Ethiopia36 and Addis Ababa.22 This is possibly due to behavioral changes that would not be acquainted by uneducated respondents.
Respondents who were on ART for more than two years were 2.74 times more likely involved in risky sexual practices. This is concurrent with study findings in Cambodia38 and Northwestern Ethiopia.36 This could be due to the effect of more vigorous HIV prevention programs and counseling among ART experienced patients compared with those who were new to ART. It was also found that uptake of condom use increased with time, the longer the follow-up period the higher the prevalence of condom use. This may be a reflection of the fact that continual exposure to secondary prevention messages has a greater impact as time progresses.
Also, respondents with CD4 count ≥ 200cells/mm3 were three times more involved in risky sexual practices than those who had CD4 count less than 200cells/mm3. This is supported by study findings in Northern Ethiopia 16 and Addis Ababa.22 This might be as a result of increased immunity level and feeling healthier, they and their counselors forgot the HIV transmission. Another possible explanation may be ART improves the quality of life and life expectancy of PLHIV by raising the CD4 count and decreasing the viral load. Following this improvement, a significant number of PLHIV started to engage in risky sexual practices.
Conclusion
The magnitude of risky sexual practices (condomless sex) in this study was high, and more than half, 240 (56.9%), of the study participants were engaged in risky sexual practices in the past 12 months prior to study. Rural residence, not attending formal education, being on ART for >2 years and CD4 count ≥ 200 cells/mm3 were factors positively associated with the risky sexual practices of women attending treatment clinics. ART counselors should integrate behavioral change intervention and secondary prevention strategies with the education and counseling session of clients. Interventions must encourage free and explicit discussion among partners about safe sex and enhance positive attitudes toward condom use. Health education and counseling might be provided to these people at ART appointments and in follow-up care.
The strengths of the study were it investigated a problem that is ignored most of the time by the government and health care workers and it was representative since it covered a broader geographic area. On other hand, the limitations were cross-sectional study design makes it difficult to determine the direction of causality, and a prospective design is recommended to confirm the factors identified. Sampling method did not include clients who received ART for less than six months, and sampling method which includes those clients is recommended. In addition, the study used interviewer administered data collection technique which might result in a social desirability bias because of the sensitive nature of the issue. This might lead to under estimating of the prevalence of risky sexual practices. Finally, recalling past sexual experiences could have caused measurement error.
Abbreviations
AOR, adjusted odds ratio; ART, antiretroviral therapy; MTCT, mother to child transmission; CD4, cluster of differentiation 4; HIV, human immunodeficiency virus; STI, sexually transmitted infection; SPSS, Statistical Package for Social Science; UNAIDS, Joint United Nations Program on HIV/AIDS.
Data Sharing Statement
The datasets used for analysis are available from the corresponding author on reasonable request.
Acknowledgments
I would like to thank our data collectors for their invaluable effort without them this study would not have come to be completed. My deep gratitude also goes to the study subjects who volunteered and took their time to give me all the relevant information for the study.
Author Contributions
The author made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest for this work.
References
1. HAPCO. HIV prevention in ethiopia national road map 2018–2020; 2019. Avaliable from: https://ethiopia.unfpa.org/sites/default/files/pubpdf/HIV%20Prevention%20in%20Ethiopia%20National%20Road%20Map%202018%20-%202020%20FINAL_FINAL.pdf.
2. UNAIDS. UNAIDS data; 2019. Avaliable from: https://www.unaids.org/sites/default/files/media_asset/2019-UNAIDS-data_en.pdf.
3. UNAIDS. UNAIDS data; 2018. Avaliable from: https://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf.
4. UNAIDS. UNAIDS report on the global aids epidemic; 2010. Avaliable from: http://files.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2010/20101123_globalreport_en%5B1%5D.pdf.
5. FMOH. Guidelines for prevention of mother to child transmission of HIV in Ethiopia, Addis Ababa; 2017. Available from: http://www.ilio.org.
6. Tesfaye R, Mesganaw F. Fertility desire and reproductive health care needs of men and women living with HIV/AIDS in Nekemte, East Wollega, Ethiopia. Sci Technol Arts Res J. 2012;1(3):31–38.
7. Adilo MT, Wordofa MH. Prevalence of fertility desire and its associated factors among 15-to 49-year-old people living with HIV/AIDS in Addis Ababa, Ethiopia: a cross-sectional study design. HIV AIDS (Auckl). 2017;9:167.
8. Antelman G, Medley A, Mbatia R, et al. Pregnancy desire and dual method contraceptive use among people living with HIV attending clinical care in Kenya, Namibia and Tanzania. J Fam Plann Reprod Health Care. 2015;41(1):e1. doi:10.1136/jfprhc-2013-100784
9. Hussen M, Fikre E. Effect of antiretroviral therapy on changes in the fertility intentions of human immunodeficiency virus-positive women in Addis Ababa, Ethiopia: a prospective follow-up study. Epidemiol Health. 2017;39:e2017028. doi:10.4178/epih.e2017028
10. Saag MS, Benson CA, Gandhi RT, et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2018 recommendations of the international antiviral society–USA panel. JAMA. 2018;320(4):379–396. doi:10.1001/jama.2018.8431
11. Fifer H, Saunders J, Soni S, Sadiq ST, FitzGerald M. British Association for Sexual Health and HIV National Guideline for the Management of Infection with Neisseria Gonorrhoeae (2019). London: British Association for Sexual Health and HIV; 2019.
12. Kaida A, Matthews LT, Kanters S, et al. Incidence and predictors of pregnancy among a cohort of HIV-positive women initiating antiretroviral therapy in Mbarara, Uganda. PLoS One. 2013;8(5):e63411. doi:10.1371/journal.pone.0063411
13. Kaoje A, Ibrahim M, Njoku C, Gusau G, Saad A, Raji M. Predictors of fertility desire among people living with HIV attending anti-retroviral clinic in a tertiary health facility in Sokoto, Northern Nigeria. Sahel Med J. 2015;18(1):14. doi:10.4103/1118-8561.152153
14. Kalichman SC, Cherry C, Kalichman MO, et al. Sexual behaviors and transmission risks among people living with HIV: beliefs, perceptions, and challenges to using treatments as prevention. Arch Sex Behav. 2016;45(6):1421–1430. doi:10.1007/s10508-015-0559-4
15. Mavhandu-Mudzusi AH, Asgedom T. The prevalence of risky sexual behaviours amongst undergraduate students in Jigjiga University, Ethiopia. Health SA Gesondheid. 2016;21(1):179–186. doi:10.1016/j.hsag.2015.11.002
16. Molla AA, Gelagay AA. Risky sexual practice and associated factors among HIV positive adults attending anti-retroviral treatment clinic at Gondar University Referral Hospital, Northwest Ethiopia. PLoS One. 2017;12(3):e0174267. doi:10.1371/journal.pone.0174267
17. Dessie Y, Gerbaba M, Bedru A, Davey G. Risky sexual practices and related factors among ART attendees in Addis Ababa Public Hospitals, Ethiopia: a cross-sectional study. BMC Public Health. 2011;11(1):422. doi:10.1186/1471-2458-11-422
18. Abiodun O, Sotunsa J, Jagun E. The determinants of sexual risk behavior for HIV/AIDS among university students in Ilishan, Nigeria. Annu Res Rev Biol. 2014;4(24):3980–3992. doi:10.9734/ARRB/2014/11739
19. Yi S, Te V, Pengpid S, Peltzer K. Social and behavioural factors associated with risky sexual behaviours among university students in nine ASEAN countries: a multi-country cross-sectional study. SAHARA J. 2018;15(1):71–79. doi:10.1080/17290376.2018.1503967
20. Mosisa G, Woldemichael K, Ayalew F. Risky sexual behavior and associated factors among antiretroviral therapy attendees in Nekemte Referral Hospital, Western Ethiopia: a cross-sectional study. HIV AIDS (Auckl). 2018;10:125.
21. Ali MS, Tesfaye Tegegne E, Kassa Tesemma M, Tesfaye Tegegne K. Consistent condom use and associated factors among HIV-positive clients on antiretroviral therapy in North West Ethiopian Health Center, 2016 GC. AIDS Res Treat. 2019;2019.
22. Tadesse WB, Gelagay AA. Risky sexual practice and associated factors among HIV positive adults visiting ART clinics in public hospitals in Addis Ababa city, Ethiopia: a cross sectional study. BMC Public Health. 2019;19(1):113. doi:10.1186/s12889-019-6438-5
23. Blumenthal J, Haubrich R, Jain S, et al. Factors associated with high transmission risk and detectable plasma HIV RNA in HIV-infected MSM on ART. Int J STD AIDS. 2014;25(10):734–741. doi:10.1177/0956462413518500
24. Belayneh F. Prevalence of hepatitis B virus infection and associated factors among HIV positive adults attending ART Clinic at Hawassa referral hospital, SNNPR, Ethiopia. Open Access Lib J. 2015;2(05):1.
25. Archibong MA. Perceptions About Sexually Transmitted Diseases in Akwa Ibom State of Nigeria: A Qualitative Study of Young Adults Age 18–24. 2016.
26. Derbie A, Assefa M, Mekonnen D, Biadglegne F. Risky sexual behaviour and associated factors among students of Debre Tabor University, Northwest Ethiopia: a cross-sectional study. Ethiop J Health Dev. 2016;30(1):11–18.
27. Fassika A, Worku A, Yayehirad A. Fertility desire and associated factors among clients on highly active antiretroviral treatment at finoteselam hospital Northwest Ethiopia: a cross sectional study. Reprod Health. 2015;12(1):69. doi:10.1186/s12978-015-0063-2
28. Ayieko J, Ti A, Hagey J, et al. HIV status and treatment influence on fertility desires among women newly becoming eligible for antiretroviral therapy in western Kenya: insights from a qualitative study. Reprod Health. 2017;14(1):93. doi:10.1186/s12978-017-0355-9
29. Burgess A, Purssell E. What is the relationship between increased access to HAART, relationship status and fertility decisions amongst HIV-positive women? A literature review and meta-analysis. J Clin Nurs. 2017;26(23–24):3800–3810. doi:10.1111/jocn.13731
30. Remera E, Boer K, Umuhoza SM, et al. Fertility and HIV following universal access to ART in Rwanda: a cross-sectional analysis of demographic and health survey data. Reprod Health. 2017;14(1):40. doi:10.1186/s12978-017-0301-x
31. Krashin JW, Haddad LB, Tweya H, et al. Factors associated with desired fertility among HIV-positive women and men attending two urban clinics in Lilongwe, Malawi. PLoS One. 2018;13(6):e0198798. doi:10.1371/journal.pone.0198798
32. CSA. Statistical report of the population and housing census of West Wollega, Ethiopia; 2007. Avaliable from: https://wwwrevolvy.com/page/WestWelegaZone.
33. Menberu G, Fessehaye A, Mulumebet A, Deribew A. Factors affecting fertility decisions of married men and women living with HIV in South Wollo Zone, Northeast Ethiopia. Ethiop J Health Dev. 2010;24(3):214–220.
34. EDHS. Central statistical agency Addis Ababa, Ethiopia: ICF international Calverton, Maryland, USA; March 2012. Available from: hhtps://www.uniceforg/ethiopia/ET2011.
35. Haddad LB, Feldacker C, Jamieson DJ, et al. Pregnancy prevention and condom use practices among HIV-infected women on antiretroviral therapy seeking family planning in Lilongwe, Malawi. PLoS One. 2015;10(3):e0121039. doi:10.1371/journal.pone.0121039
36. Shewamene Z, Legesse B, Tsega B, Bhagavathula AS, Endale A. Consistent condom use in HIV/AIDS patients receiving antiretroviral therapy in northwestern Ethiopia: implication to reduce transmission and multiple infections. HIV AIDS (Auckl). 2015;7:119.
37. Yalew E, Zegeye DT, Meseret S. Patterns of condom use and associated factors among adult HIV positive clients in North Western Ethiopia: a comparative cross sectional study. BMC Public Health. 2012;12(1):308. doi:10.1186/1471-2458-12-308
38. Tuot S, Pal K, Thin K, et al. Determinants of Inconsistent Condom Use Among HIV Serodiscordant Couples in Cambodia. 2016.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.