")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 10
Risky sexual behavior and associated factors among antiretroviral therapy attendees in Nekemte Referral Hospital, Western Ethiopia: a cross-sectional study
Authors Mosisa G , Woldemichael K , Ayalew F
Received 13 December 2017
Accepted for publication 25 April 2018
Published 10 July 2018 Volume 2018:10 Pages 125—131
DOI https://doi.org/10.2147/HIV.S159670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Getu Mosisa,1 Kifle Woldemichael,2 Fantahun Ayalew,3,†
1Department of Nursing and Midwifery, College of Health Sciences, Wollega University, Nekemte, Ethiopia; 2Department of Epidemiology, College of Health Sciences, Jimma University, Jimma, Ethiopia; 3Department of Nursing and Midwifery, College of Health Sciences, Jimma University, Jimma, Ethiopia
†Fantahun Ayalew passed away on August 31, 2017
Background: HIV/AIDS remains a major public health problem. Practice of risky sexual behaviors is the major effective driver of the HIV epidemic among HIV-positive individuals. This behavior exposes their partners to HIV, and for those that are already positive it exposes them to a risk of suprainfection by other strains.
Objective: The aim of this study was to assess the prevalence of risky sexual behavior and associated factors among people living with HIV attending antiretroviral therapy (ART) clinic at Nekemte Referral Hospital.
Methods: An institution-based based cross-sectional study was conducted at the ART clinic of Nekemte Referral Hospital from March to April 2016. A total of 337 people living with HIV on ART for at least 3 months were selected by consecutive sampling technique. Data were collected through face-to-face interview. Data were entered into Epi-data Version 3.1 and analyzed using SPSS version 20. Variables significant on bivariate logistic regression analysis at p<0.25 were considered as candidates for the multivariable logistic regression analysis, and statistical significance was set at p<0.05.
Results: Approximately one third (32.9%) of the study participants were engaged in risky sexual behavior in the past 3 months prior to the study. Having multiple sexual partners (adjusted odds ratio [AOR] =6.38, 95% CI: 1.65, 24.74), being with a positive sero-status partner (AOR =2.68, 95% CI: 1.31, 5.5), not disclosing sero-status (AOR =5.99, 95% CI: 1.36, 26.35), having a desire for a child (AOR =2.6, 95% CI: 1.5, 4.51), having experience of perceived stigma (AOR =2.63, 95% CI: 1.5, 4.62), and lack of education on importance of protecting self from strain (AOR =5.64, 95% CI: 3.19, 9.96) were significantly associated with risky sexual behavior.
Conclusion and recommendation: The prevalence of risky sexual behavior was high, and approximately one third of study participants were engaged in risky sexual behavior. Efforts to increase awareness through health education and counseling are highly recommended.
Keywords: HIV, risky sexual behavior, Nekemte Referral Hospital, Ethiopia
Introduction
HIV/AIDS remains a major public health problem. According to UNAIDS global statistics, about 36.7 million people globally were living with HIV and 1.8 million people became newly infected with HIV in 2016. About 19.5 million people were taking antiretroviral therapy (ART) and an estimated 1 million people died from AIDS-related illnesses in 2016.1 According to a 2014 report, in sub-Saharan Africa there were 25.8 million people living with HIV and 5 out of 7 people on ART live in this region.2
In 2013, in Ethiopia there were an estimated 793,700 people living with HIV and there were ~45,200 AIDS-related deaths.3 Risky sexual behavior is commonly defined as behavior that increases one’s risk of contracting sexually transmitted infections and experiencing unintended pregnancies.4
Risky sexual behavior among people receiving ART is an area of concern; hence, it is the major effective driver of the HIV epidemic. Among people living with HIV (PLHIV), these behaviors are common and potentially expose their partners to risk of disease, and for HIV-positive partners these habits expose them to a real risk of suprainfection by other strains of HIV.5–7 The magnitude of unprotected sexual practice among PLHIV is high in sub-Saharan Africa; about more than 1 in 3 PLHIV were engaged in risky sexual practice.8–10 In Ethiopia, the magnitude of risky sexual behavior among PLHIV is also high, more than one third and nearly one quarter of respondents engage in risky sexual behavior in Addis Ababa and Debrezeit, respectively.11,12
In HIV-related studies, risky sexual behavior has been one of the most documented topics. It has driven most HIV intervention and programs worldwide, and especially in sub-Saharan Africa which is the most affected area.13
However, little is known about risky sexual behavior among PLHIV attending ART in Ethiopia, particularly in the study area. Therefore, the current study aimed to assess the prevalence and associated factors of risky sexual behavior among PLHIV attending ART clinic at Nekemte Referral Hospital.
Methods and materials
Study area
The study was conducted in Nekemte Referral Hospital which is located in East Wollega zone, Nekemte town. Nekemte town is located at a distance of about 331 km to the west of the capital city, Addis Ababa. The town has 1 referral hospital and 2 public health centers. About 2,105 PLHIV were on ART at the time of the study.
Study design and period
An institution-based cross-sectional study was conducted at Nekemte Referral Hospital from March to April 2016.
Study population
The study population included adult clients on ART who were sexually active in the 3 months prior to the study period.
Sample size determination and sampling technique
The sample size of the study was calculated by using single proportion formula, using prevalence of unprotected sex in the past 3 months among ART attendees in Addis Ababa 36.9%,11 margin of sampling error tolerated (d) 5%, CI 95%. Then, the sample size becomes 358. Since the source population was 2,105 clients, which are below 10,000, finite population corrections formula was used to get sample size of 306. Finally, by adding nonresponse rate of 10%, the total sample size was 337. Consecutive sampling technique was used to select study participants. Participants were selected based on inclusion criteria until the required sample size was achieved. People living with HIV/AIDS who were on ART treatment and sexually active in the previous 3 months and 18 years of age and above were included in the study.
Data collection
A structured questionnaire was developed after reviewing relevant literatures8,10,11,14 and modified to the local context based on the study objectives. Prior to data collection, the tool was pretested among 5% (17) of study population at Gimbi Hospital to ensure the clarity and applicability of the tool, and then necessary modifications and correction were undertaken.
The questionnaire was designed to obtain information on sociodemographic characteristics, partner-related factors, clinical-related factors, health-related service, child-related factors, psychosocial related factors, and pattern of condom use.
The outcome variable, risky sexual behavior, was measured by inconsistent use of condoms or no condom-protected sex with HIV-negative, HIV-positive, or unknown-status partners in the previous 3 months.10,11,14
The study was conducted for 1 month; 2 nurses who worked in ART unit were recruited as data collectors and 1 senior BSC nurse was a supervisor. Data collectors and supervisor were trained on interview techniques for 1 day before data collection. Face-to-face exit interview was conducted, and the interview was conducted in an isolated private room.
Data processing and analysis
Data were entered into Epi-data Version 3.1 (The EpiData Association, Odense, Denmark) and exported to SPSS 20 (IBM Corporation, Armonk, NY, USA) for analysis. Descriptive measures like percentages and frequency distributions were used in the form of tables and graphs. Bivariate logistic regression analyses was carried out to assess association between the dependent and all the independent variables and to identify candidates for multivariable analysis. Then, variables with p-values <0.25 were entered in to final multivariable logistic regression model; then, independent variables, which had a statistically significant association with the dependent variable at p<0.05, were entered to the final regression model. Statistical significance was set at p<0.05.
Ethical consideration
Ethical clearance was obtained from Institutional Review Board of Jimma University, College of Health Sciences. A formal letter from the College of Health Sciences of Jimma University was submitted to Nekemte Referral Hospital, then permission and support letter was written to ART clinic of Nekemte Referral Hospital. Oral consent was obtained from each study participant before the interview and confidentiality of the data was ensured. The respondents’ right to refuse or withdraw from the interview was taken into consideration, and confidentiality for collected data was also ensured throughout the study process. Obtained oral consent was approved by the Institutional Review Board of Jimma University, College of Health Sciences.
Results
Sociodemographic characteristics of respondents
A total of 337 respondents were involved in the study, a response rate of 100%. Majority of the respondents 187 (55.5%) were females. The mean age of the study participants was 36.05 (SD ±8.17), and majority of the study participants147 (43.6%) were in the age category of 35–44 years. Regarding educational status, majority (148) (43.9%) of study participants had completed primary school. One hundred sixty-one (47.8%) were Protestants and 282 (83.7%) were of Oromo ethnicity. Concerning marital status, majority of respondents (314) (93.2%) were married and about 312 (92.6%) were from an urban area (Table 1).
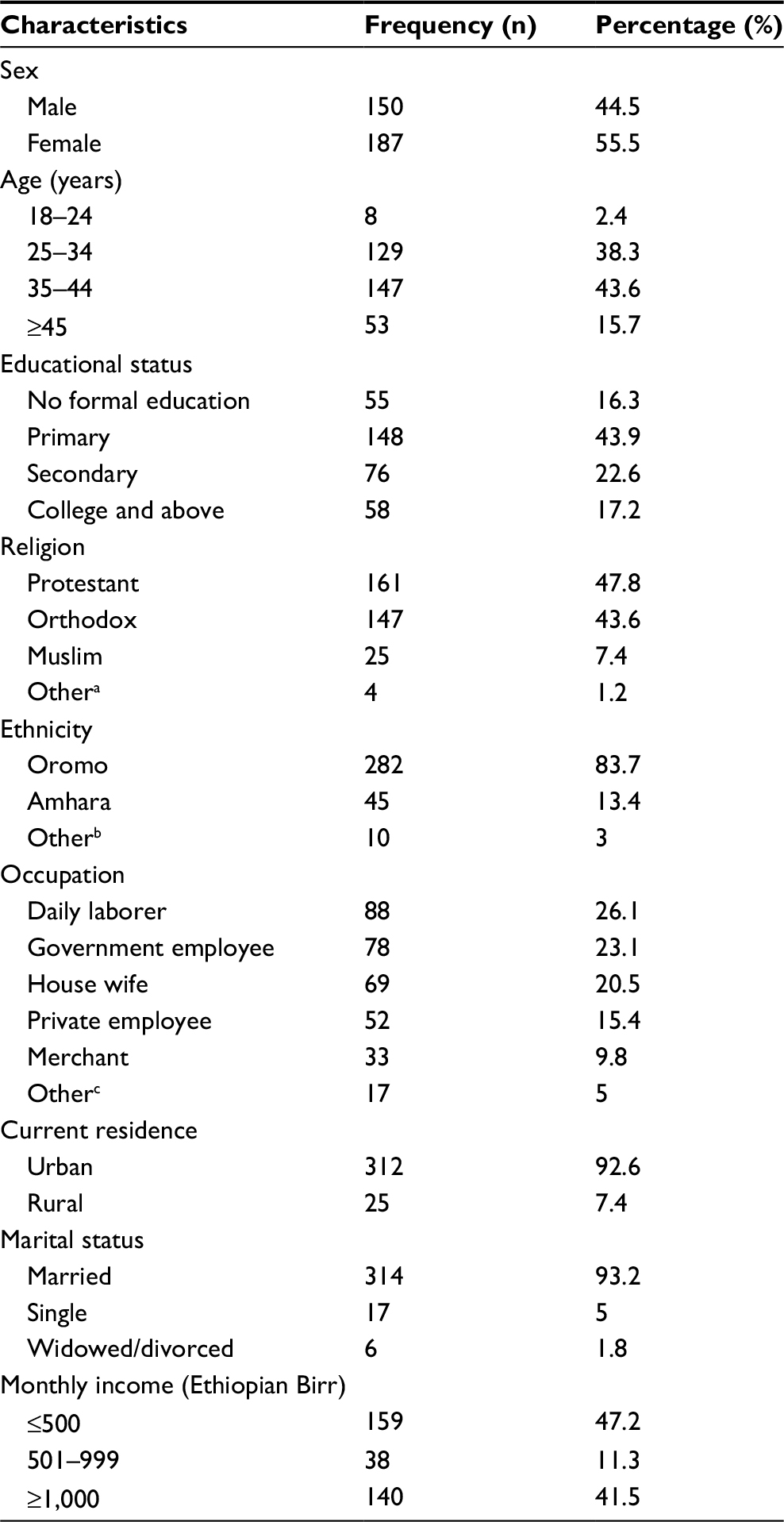 | Table 1 Sociodemographic characteristics of PLHIV attending ART clinic at Nekemte Referral Hospital, East Wollega, Ethiopia, April, 2016 Notes: aAdventist, Catholic, Wakefata and Hawariyat, bTigre, Guraghe, Wolayita and Silte, and cstudent, farmer, commercial sex worker, and house maid. Abbreviations: ART, antiretroviral therapy; PLHIV, people living with HIV. |
Partner-related factors and pattern of condom use
Majority of the study respondents, 322 (95.5%), had a single sexual partner in the past 3 months. Among those who had single partner, majority of them, 317 (98.4%), had a steady partner. More than half (8) (53.3%) of respondents had steady partner among those with multiple sexual partners. Regarding sexual desire after starting ART, about 186 (55.2%) of the study participants stated that their sexual desire had not changed. About 243 (72.1%) respondents’ partners’ sero-status was positive, and 321 (95.3%) disclosed this to their partners (Table 2).
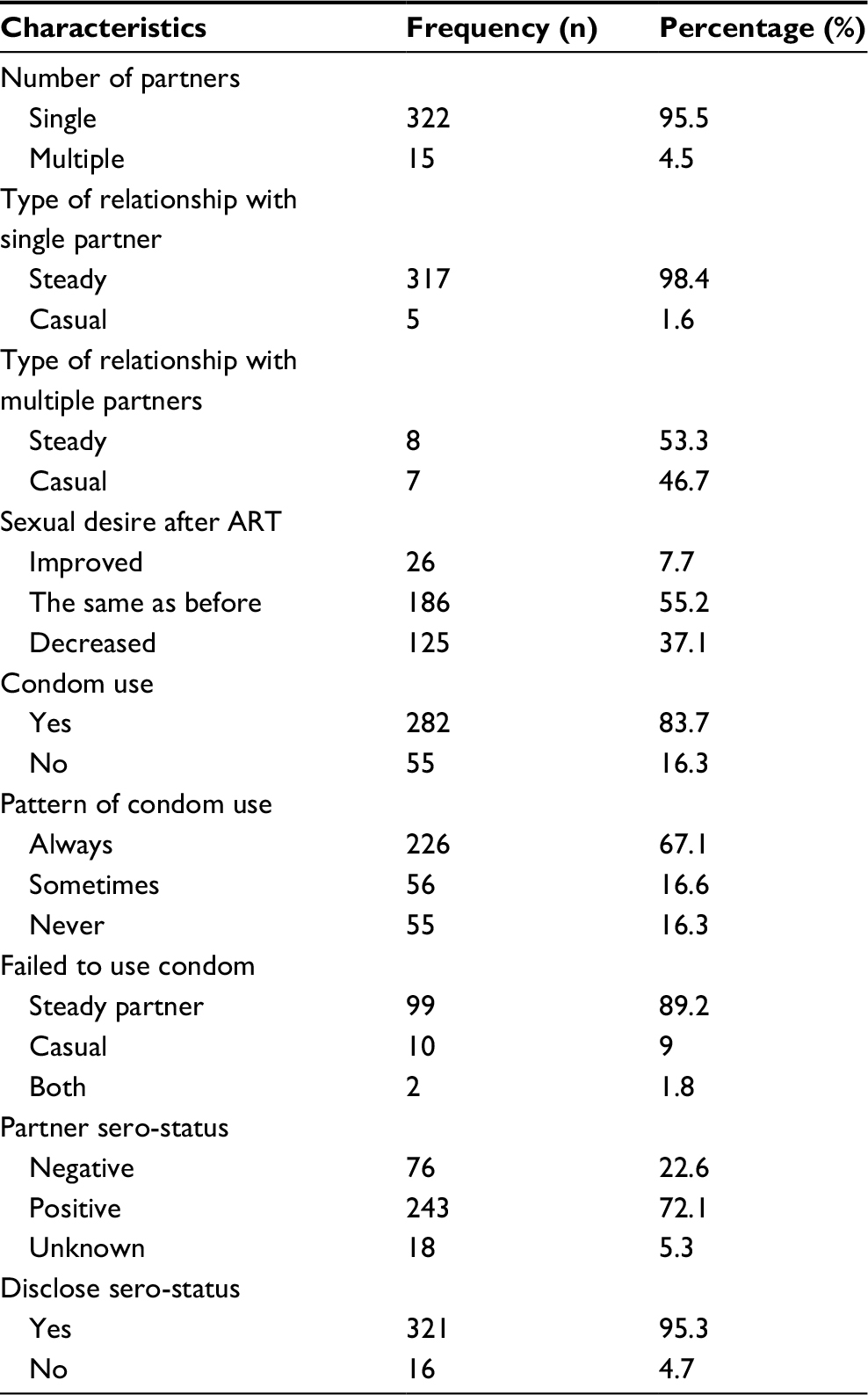 | Table 2 Partner-related characteristics and pattern of condom use among PLHIV attending ART clinic at Nekemte Referral Hospital, East Wollega, Ethiopia, April 2016 Abbreviations: ART, antiretroviral therapy; PLHIV, people living with HIV. |
Regarding condom use, about 226 (67.1%) used condom consistently, 56 (16.6%) used it sometimes, and 55 (16.3%) did not use it at all in the past 3 months prior to the study. From those who did not use condoms consistently or at all, the majority of study participants, 99 (89.2%), failed to use a condom with steady partners. In this study, the prevalence of risky sexual behavior (inconsistent or no use of condom) was 111 (32.9%).
Clinical and psychosocial characteristics of respondents
About 269 (79.8%) of the respondents started ART medication more than 2 years ago. Majority of them, 304 (90.2%), had CD4 count >200 cells/mm3. Only 41 (12.2%) respondents consumed alcohol in the past 3 months, of those 27 (65.9%) drank once per week. Regarding substance use, about 14 (4.2%) had history of substance use in the past 3 months, of those 10 (71.4%) used chat, 2 (14.3%) cigarette, and 2 (14.3%) hashish. Regarding stigma, about 96 (28.5%) had experienced enacted stigma and about 139 (41.2%) perceived stigma (Table 3).
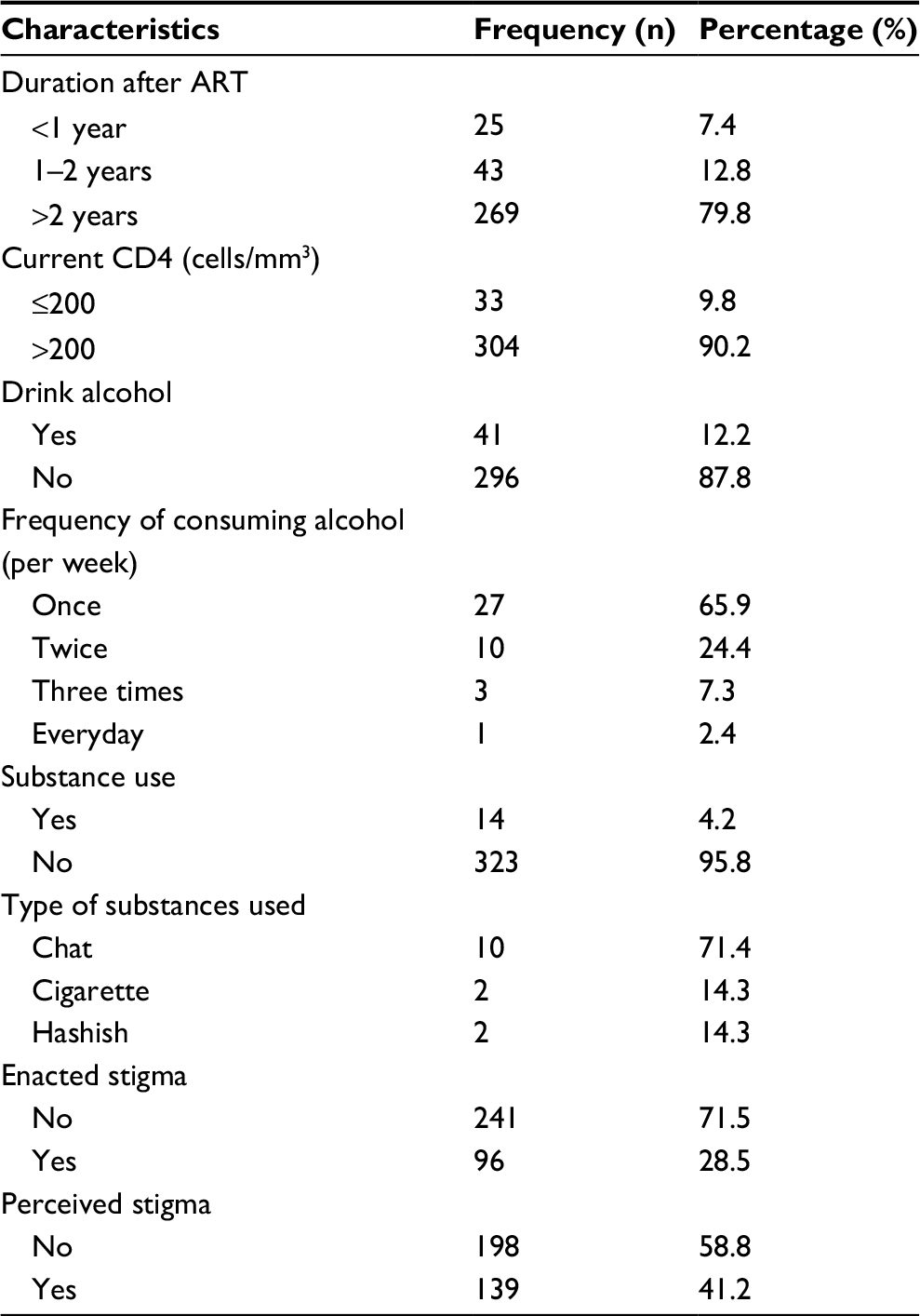 | Table 3 Clinical and psychosocial characteristics of PLHIV attending ART clinic at Nekemte Referral Hospital, East Wollega, Ethiopia, April, 2016 Abbreviations: ART, antiretroviral therapy; PLHIV, people living with HIV. |
Child desire and health-related service characteristics
Majority of respondents (311) (92.3%) had at least 1 child who was currently alive. Regarding fertility desire, 143 (42.4%) desired to have children in the future, of which 75 (52.4%) desired to have 2 children. Concerning health-related service given to the respondents in past 3 months, 231 (68.5%) received education/counseling on the importance of protecting themselves from different strains and 262 (77.7%) were educated on risk reduction strategy (Table 4).
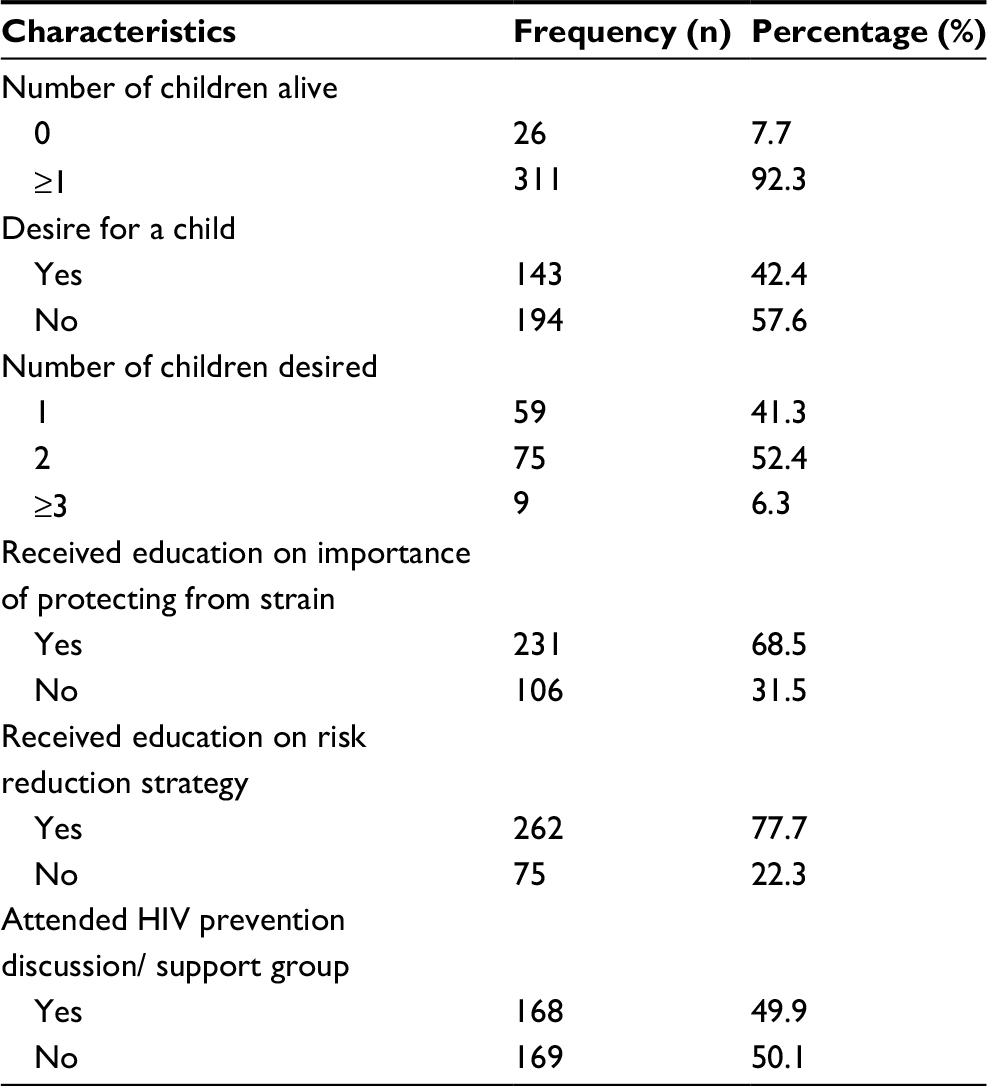 | Table 4 Fertility and health service-related characteristics of PLHIV attending ART clinic at Nekemte Referral Hospital, East Wollega, Ethiopia, April, 2016 Abbreviations: ART, antiretroviral therapy; PLHIV, people living with HIV. |
Association between dependent and independent variables
In multivariable logistic regression analysis, the number of partners, partner sero-status, disclosure status, desire for child, perceived stigma, and education on importance of protection of self from different strains were statistically significantly associated with risky sexual behavior/ unprotected sex.
Respondents who had multiple sexual partners were 6.38 times more likely to engage in risky sexual behavior than those who had single partner (adjusted odds ratio [AOR] =6.38, 95% CI: 1.65, 24.74).
Study participants with sero-positive partners were 2.68 times more likely to engage in risky sexual behavior than participants with negative sero-status partner (AOR =2.68, 95% CI: 1.31, 5.5).
And those who did not disclose their status to their partner were 5.99 times more likely to engage in risky sexual behavior than those who disclosed (AOR =5.99, 95% CI: 1.36, 26.35).
Those who felt stigma in the past 3 months were 2.63 times more likely to engage in risky sexual behavior than those who did not (AOR =2.63, 95% CI: 1.5, 4.62).
Respondents who did not get education on importance of protecting themselves from different strains were 5.64 times more likely to engage in risky sexual behavior than those who received counseling (AOR =5.64, 95%, CI: 3.19, 9.96). This study also showed that participants with a desire for children were 2.6 times more likely to engage in risky sexual behavior than those who had no desire for child (AOR =2.6, 95% CI: 1.5, 4.51) (Table 5).
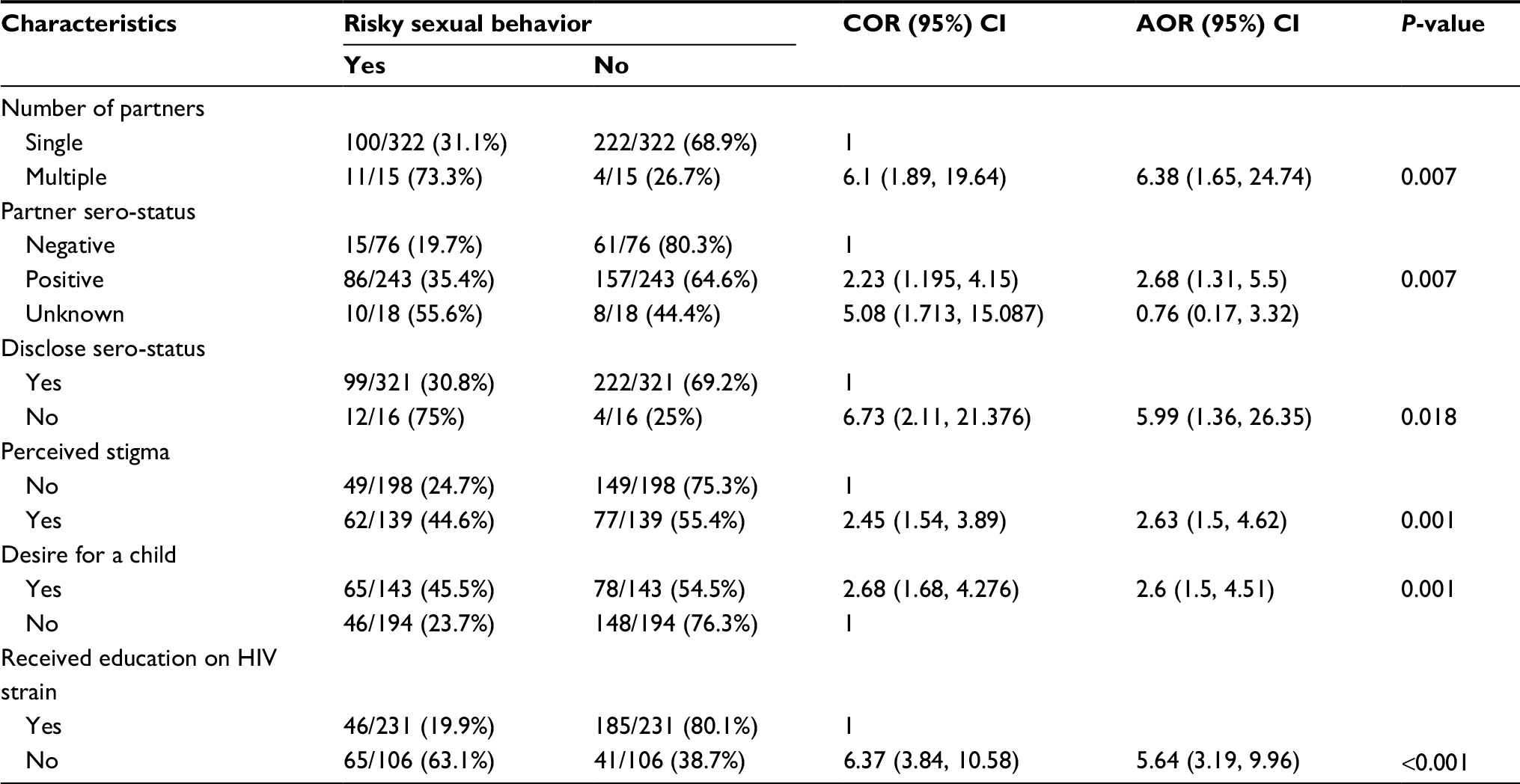 | Table 5 Bivariate and multivariable logistic regression analysis of factors associated with risky sexual behavior among PLHIV attending ART at Nekemte Referral Hospital, April, 2016 Abbreviations: AOR, adjusted odds ratio; ART, antiretroviral therapy; COR, crude odds ratio; PLHIV, people living with HIV. |
Discussion
The study showed that about 32.9% of respondents were engaged in risky sexual behavior (condomless sex) in the past 3 months. This finding is consistent with studies conducted in Kenya (one third of respondents), Togo (34.6%), and Addis Ababa (30.4%).9,10,14 The prevalence rate seems pretty consistent across the various studies. This might be due to similarity in socioeconomic status of the study population. A study from Tanzania showed that about 40% males and 37.5% females engaged in unprotected sex.5 This value is higher than the current study. The difference might be due to variation in study unit, as they considered only young age (<24 years) respondents.
In this study, participants who had multiple sexual partners were 6.38 times more likely to engage in risky sexual behavior than those who had a single partner. This is in line with a study in Addis Ababa in which practicing unprotected sex was higher among those who had multiple sexual partners compared to those who had a single partner.11 The possible explanation might be due to the fact that those who had multiple sexual partners might not disclose their status to their partners, particularly those engaged in commercial sex.
The study result showed that respondents who had positive partners were 2.68 times more likely to be engaged in risky sexual behavior compared to those who have a sero-negative partner. Consistent with the current study, a similar study conducted in western India showed that those with sero-positive partners were 3 times more likely to engage in unsafe sex.15 The possible explanation might be due to false belief that condom is not important if both of them are sero-positive. This might hasten HIV reinfection with different strains and may lead to drug resistance. In contrast with this, a study from Tanzania showed that clients with HIV-positive partners were significantly more likely than those with HIV-negative partners to use condoms consistently.16
Disclosing sero-status to partner showed a significant association with risky sexual behavior in this study. Participants who did not disclose their sero-status to their partners were 5.99 times more likely to engage in risky sexual practice than those who disclosed. This is consistent with a study from South Africa (Cape Town) where sexual transmission risk behaviors were reported mostly in people who had not disclosed their HIV status to sex partners, and the result is also similar to a study conducted among HIV-infected women in Cameroon where disclosure of HIV sero-status to the main partner has been associated with safer sexual practices.17,18 Another study conducted in Johannesburg, South Africa, also indicated that participants who were aware of their partner’s HIV status were 4 times more likely to use condoms in a consistent manner than those who were not.19 This might be due to the possibility that PLHIV who did not know their partners’ status might not push to use condom during sex.
In this study, individuals who felt stigmatized in the last 3 months were 2.63 times more likely to engage in risky sexual behavior than those who did not. This is in line with studies from Addis Ababa and western India.11,15 This might indicate that individuals who felt stigmatized were afraid to disclose their status to their partner.
Desire for child showed strong association with risky sexual behavior. Participants who desired to have child/children were 2.6 times more likely to engage in risky sexual practice than those who did not desire a child.
This was supported by study conducted in South India that showed desire for children as being associated with unprotected sex.20 Similarly, in study conducted in Kampala, Uganda, desire for more children was a strong independent predictor of engaging in high-risk sex.21 This was also consistent with a study conducted in Southern Nations and Nationalities Peoples Region which showed risky sexual behavior was associated with desire for a child.22
Education on HIV prevention measures is an important strategy to reduce risky sexual behavior. The study result showed that respondents who did not receive education on importance of protecting themselves from different strains were 5.64 times more likely to engage in risky sexual behavior than those who were educated. This finding is consistent with studies from Uganda and Western India.8,15 The reason might be due to the fact that progressive education and or counseling given on the importance of protecting oneself from strain could change their behavior to one of practicing safe sex.
Conclusion and recommendations
The prevalence of risky sexual behavior in this study was high, and about one third of the study participants were engaged in risky sexual behavior in the past 3 months prior to study.
Having multiple sexual partner, being with positive sero-status partner, not disclosing sero-status, having desire for child, having experience of perceived stigma, and lack of education on importance of protecting oneself from strain were significantly associated with risky sexual behavior. ART counselors should integrate behavioral change intervention and secondary prevention strategies with the education and counseling session of clients.
Acknowledgments
We would like to express our deepest gratitude to Jimma and Wollega University for financially supporting the research. Our appreciation also goes to the data collectors, supervisors, Nekemte Referral Hospital, and study participants for their valuable contribution in the realization of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
UNAIDS. Fact Sheet-Latest Statistics on the Status of the AIDS Epidemic, Global HIV Statistics. Geneva: UNAIDS; 2017. | ||
UNAIDS. Fact Sheet On Global Statistics, 2015. Geneva: UNAIDS. Available from: http://www.unaids.org/en/resources/campaigns/HowAIDSchangedeverything/factsheet. Accessed May 19, 2018. | ||
Federal Democratic Republic of Ethiopia. Country Progress Report on HIV Response. 2014. Available from: http://www.unaids.org/sites/default/files/country/documents/ETH_narrative_report_2014.pdf. | ||
Centers for Disease Control and Prevention. Youth risk behavior surveillance-United Sates, 2009. MMWR. 2010;59(SS05):1–142. | ||
Mhalu A, Leyna GH, Mmbaga EJ. Risky behaviors among young people living with HIV attending care and treatment clinics in Dar Es Salaam, Tanzania: implications for prevention with a positive approach. J Int AIDS Soc. 2013;16:17342. | ||
Peretti-Watel P, Spire B, Schiltz MA, et al; VESPA Group. Vulnerability, unsafe sex and non-adherence to HAART: evidence from a large sample of French HIV/AIDS outpatients. Soc Sci Med. 2006;62(10):2420–2433. | ||
Essomba N, Kollo B, Fouda AB, et al. Sexual risk behaviours among patients living with HIV/AIDS in Douala in 2012. J Med Health Sci. 2013;14(1):36–43. | ||
Musinguzi G, Bwayo D, Kiwanuka N, et al. Sexual behavior among persons living with HIV in Uganda : implications for policy and practice. PLoS One. 2014;9(1):1–10. | ||
Ragnarsson A, Ekström AM, Carter J, et al. Sexual risk taking among patients on antiretroviral therapy in an urban informal settlement in Kenya : a cross-sectional survey. J Int AIDS Soc. 2011;14(1):20. | ||
Yaya I, Saka B, Landoh DE, et al. Sexual risk behavior among people living with HIV and AIDS on antiretroviral therapy at the regional hospital of Sokodé, Togo. BMC Public Health. 2014;14:636. | ||
Dessie Y, Gerbaba M, Bedru A, Davey G. Risky sexual practices and related factors among ART attendees in Addis Ababa Public Hospitals, Ethiopia : a cross-sectional study. BMC Public Health. 2011;11(1):422. | ||
Engedashet E, Worku A, Tesfaye G. Unprotected sexual practice and associated factors among people living with HIV at ante retroviral therapy clinics in Debrezeit Town, Ethiopia : a cross sectional study. Reprod Health. 2014;11(1):1–9. | ||
Dimbuene ZT, Emina JB, Sankoh O. UNAIDS “multiple sexual partners” core indicator: promoting sexual networks to reduce potential biases. Glob Health Action. 2014;7:23103. | ||
Demissie K, Asfaw S, Abebe L, Kiros G. Sexual behaviors and associated factors among antiretroviral treatment attendees in Ethiopia. HIV AIDS (Auckl). 2015:7 183–190. | ||
Mehta KG, Baxi R, Chavda P, Patel S, Mazumdar V. Predictors of unsafe sexual behavior among people living with human immunodeficiency virus/AIDS attending antiretroviral therapy center in Western India. Indian J Sex Transm Dis. 2016;37(1):21–27. | ||
Conserve D, Sevilla L, Younge S, Mbwambo J, King G. Condom use among HIV-positive sexually active adults and partner’s HIV status in Dares Salaam, Tanzania. J Health Care Poor Underserved. 2012;23(1):191–203. | ||
Simbayi LC, Kalichman SC, Strebel A, Cloete A, Henda N, Mqeketo A. Disclosure of HIV status to sex partners and sexual risk practices among HIV-positive men and women, Cape Town, South Africa. Sex Transm Infect. 2007;83(1):29–34. | ||
Loubiere S, Peretti-Watel P, Boyer S, Blanche J, Abega SC, Spire B. HIV disclosure and unsafe sex among HIV-infected women in Cameroon: results from the ANRS-EVAL study. Soc Sci Med. 2009;69(6):885–891. | ||
Madiba S, Letsoalo B. Disclosure, multiple sex partners, and consistent condom use among HIV positive adults on antiretroviral therapy in Johannesburg, South Africa. World J AIDS. 2014;4(1):62–73. | ||
Venkatesh KK, Srikrishnan A, Safren SA, et al. Sexual risk behaviors among HIV-infected South Indian couples in the HAART era implications for reproductive health and HIV care delivery. AIDS Care. 2011;23(6):722–733. | ||
Tumukunde D, Nuwaha F, Ekirapa E, Kityo C, Ssali F, Mugyenyi P. Sexual behavior among persons living with HIV/AIDS in Kampala, Uganda. East Afr Med J. 2010;87(3):91–99. | ||
Debeko K. Sexual and Reproductive Health Needs and Preferences of People Living with HIV/AIDS in Southern Nations Nationalities and Peoples Region [MPH thesis]. Addis Ababa: Addis Ababa University; 2007. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.