")
Back to Journals » Journal of Pain Research » Volume 9
Risks associated with borrowing and sharing of prescription analgesics among patients observed by pain management physicians in Croatia: a qualitative study
Authors Markotic F, Puljak L
Received 4 August 2016
Accepted for publication 6 October 2016
Published 30 November 2016 Volume 2016:9 Pages 1143—1151
DOI https://doi.org/10.2147/JPR.S118945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Filipa Markotic,1 Livia Puljak2
1Centre for Clinical Pharmacology, University Clinical Hospital Mostar, Mostar, Bosnia and Herzegovina; 2Laboratory for Pain Research, University of Split School of Medicine, Split, Croatia
Background: Understanding and improving patient safety is a key issue in medicine. One of the potential threats to patient safety is the sharing of medication among patients, which is a form of self-medication. This study analyzed experiences and attitudes of pain management physicians (PMPs) about sharing prescription analgesics among patients.
Methods: This qualitative study was conducted by semi-structured interviews among PMPs employed in Croatian pain clinics. The study involved two researchers and 15 PMPs.
Results: Among PMPs, 80% have seen patients who share their prescription analgesics with other patients for whom prescription is not intended. Most PMPs consider prescription analgesics sharing a risky and negative behavior. Some of them, however, found certain positive aspects associated to it, such as being a benevolent behavior, helping patients to get medications when they need them, and helping them cope with pain.
Conclusion: The majority of physicians specialized in pain management encountered patients sharing prescription analgesics. Most of them considered this as risky behavior with a number of potential consequences. It has been noted that this problem is neglected and that physicians should inquire about medication sharing. Direct-to-consumers advertising was perceived as a factor contributing to such behavior. Patient education and more involvement of physicians in identifying this behavior were cited as potential remedies for preventing sharing of prescription analgesics.
Keywords: analgesics, sharing, lending, borrowing, risks
Introduction
Patients are prone to self-medication and self-treatment of acute and chronic conditions. Analgesics are particularly often used for self-medication, including nonsteroidal anti-inflammatory drugs (NSAIDs) and strong opioids. Understanding and improving patient safety is a key issue in medicine. One of the potential threats to patient safety is sharing of medication among patients, which is a form of self-medication.1–5 Sharing prescription drugs is defined as giving one’s own medication or taking others’ medications in situations where the recipient of these drugs is not the person for whom the drugs are intended.6 The term “lending” drugs would indicate that it was a temporary transfer of the drug on condition that the amount borrowed be returned; however, a person “borrowing” a drug usually does not give back the drug to the person who is “lending” it.7
It has been shown that analgesics are among the top three medications most often shared among patients.1,2,8,9 In the study of Ward et al, 116 (18%) respondents declared that they borrowed prescription medication from others and 89 of them listed the names of medications received in this way; 42 respondents borrowed opioids and 25 NSAIDs.10 Research among American veterans found that 16% of them shared prescription drugs to treat pain and that this behavior was associated with younger age, more mental health disorders, substance use disorders, more pain seriousness, and higher number of non-pain symptoms.11 A previous study found that nonadherence to pharmacological treatment of chronic nonmalignant pain was associated with sharing analgesics.12
Literature about prescription drug sharing emphasizes negative consequences of such behavior (eg, unexpected side effects, incorrect use of drugs, interactions, delays in the use of professional help, addiction, drug abuse, warped perception of the ineffectiveness of the drug, overdose, and teratogenicity).1,2,6,13 However, there has been no empirical research on the perception of risk among patients and physicians associated with prescription drug sharing.7
Very little is known about the phenomenon of sharing medications among patients, and there is a lack of awareness about this issue.14 A systematic review of Beyene et al, published in April 2014, which analyzed literature published until March 2013, found only 19 published studies about drug sharing and concluded that there is insufficient data about the reasons why drugs are shared, of how patients decide to share drugs, whether patients were aware of the risks of sharing drugs, and the ways in which patients assess the importance of these risk factors.7
Currently, there is insufficient information on whether physicians are aware of the prescription drug sharing problem and whether they perceive this behavior as a problem in their clinical work with patients. This study analyzed experiences and attitudes of pain management physicians (PMPs) about sharing drugs among patients. PMPs were asked to assess the risk and the potential damage (potential negative consequences) that can occur if patients share prescription analgesics.
Materials and methods
Ethics
Based on the submitted research protocol, the Ethics Committee of the University of Split School of Medicine in Split, Croatia approved the study. The study was conducted according to the principles expressed in the Declaration of Helsinki. Informed consent, written and oral, was obtained from the participants.
Methods
This qualitative study was conducted by semi-structured interviews among PMPs employed in Croatian pain clinics. A pain clinic was defined as a health care facility, an outpatient hospital unit within public tertiary health care, where anesthesiologists specialized for pain management, with or without other physicians and health care workers, focus on diagnosis and management of pain. These clinics do not dispense medications; pain clinic physicians provide treatment recommendation, based on which family physicians write prescriptions.
The study involved two researchers and 15 participants (PMPs). The first interview was conducted on March 31, 2015, and the last on July 15, 2015. The questionnaire had two parts. In the first part of the questionnaire, PMPs answered questions about themselves. The second part of the questionnaire consisted of open-ended semi-structured questions to facilitate discussion about the risks associated with sharing analgesic drugs among patients (Table 1). The physicians were not specifically led to any answer. Consolidated criteria for reporting qualitative studies (COREQ) was used as a support tool for conducting and reporting the study.15
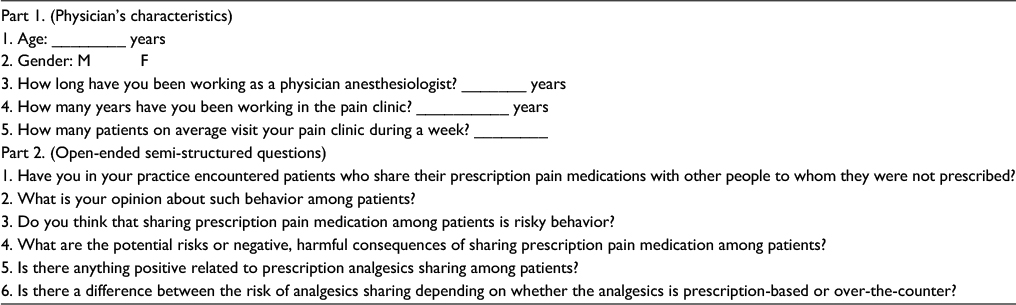 | Table 1 Study questionnaire Abbreviations: M, male; F, female. |
Research team and reflexivity
There were two researchers in the team. Prof LP (MD, PhD) is employed at the University of Split School of Medicine in Split, Croatia as a lecturer at the Department of Histology and Embryology and is a researcher in the Laboratory for Pain Research. She is also a member of the Croatian Society for Pain Treatment (cro. Hrvatsko drustvo za lijecenje boli, HDLB). FM (MD, MSc) is employed in the University Clinical Hospital Mostar, Bosnia and Herzegovina as a specialist of clinical pharmacology and toxicology and as a head of the Centre for Clinical Pharmacology.
LP met some of the participating PMPs via HDLB and had previous research collaborations with them. FM did not know any of the PMPs before the start of the study. Therefore, all potential study participants received an invitation from FM, who also conducted all the interviews.
The participants received detailed information about the study via e-mail. Study data sheet contained information about the research team (titles, positions, and contacts), a description of the research protocol, guarantee of anonymity, and information that the authors intend to publish the study results in a research journal.
Study design
For this qualitative study, semi-structured interviews were conducted with PMPs in order to detect risks recognizable as potential negative consequences of prescription analgesics sharing. Expert interviews are an important instrument for conducting innovative research, taking into consideration the status of the person with whom conversations are carried out, because such research enables the collection of information on subjective experiences and interpretations related to the predefined specialized topic. Semi-structured interview form allows not only a comparison of interviews, but also the inclusion of topics that are not anticipated, but are considered important.16 For the purpose of this study, the physicians were coded with the first 15 English alphabets (A–O).
Inclusion criteria
To be eligible for inclusion in the study, participants had to be a physician currently employed in one of Croatian pain clinics. Most PMPs were contacted electronically and a minority was contacted via phone, when they wished to discuss participation via phone. Some PMPs’ e-mail addresses and phone numbers were found via the HDLB website, and several participants were recommended for inclusion by the other study respondents (snowballing method) or by searching for contacts via the Internet.17 In some cases, official/private e-mail addresses of PMPs were used.
Response rate
Of 35 contacted PMPs, 15 participated in the study. There were 10 PMPs who refused participation via e-mail and one PMP declined participation over phone. Some who refused participation were heads of a pain clinic who declared that the refusal applies to their entire medical team. These PMPs listed four reasons to explain refusal. Some declared that in their pain clinics patients are treated with non-pharmacological methods. Others excused themselves because of their work overload. One PMP was not satisfied with the study design, and another had only children being treated in the clinic. Two heads of pain clinics accepted to participate together with their physician team, but they did not respond to subsequent attempts to schedule the interview. There were nine PMPs who did not respond at all to the e-mail invitation for participation.
Conduct of interviews
Interviews were conducted by phone (N=13) or face-to-face (N=2). All conversations were recorded. The first face-to-face interview was conducted in the outpatient pain treatment clinic. During the interview, one researcher (FM) was alone with a PMP. The interview was conducted in a room with an open door leading to another room where a nurse of a pain clinic was available. The second face-to-face interview also involved one researcher (FM) and one PMP. The conversation was held in the room of the on-duty anesthetist, where no one else was present either in the room or nearby.
Face-to-face interviews were taped via an audio-recorder. The transcripts were prepared after the interviews in the absence of the respondents. Phone interviews lasted between 5 and 25 min. The interview was conducted individually with each PMP after they accepted to participate, at the time they indicated as convenient. The first e-mail invitation for participation in the study was sent on March 27, 2015, while the last invitation was sent on July 24, 2015.
Transcripts and recordings of interviews were not sent to the respondents for checking, commenting, and/or correction.
Data analysis and reporting
In order to ensure uniformity, the whole transcript of a recorded conversation was prepared by one person (FM) and then checked by the other member of the research team (LP). Each participant was assigned a code number, which was used also for the presentation of the study results. The transcripts were then analyzed by using qualitative content analysis, which is an analysis of semi-structured interviews with experts, because it is used to encode the text to a predetermined systematic coding that can be matched and supplemented with new issues that may arise during the interview. A predefined encoding system for this study was based on risk categories that were identified in previously published literature about drug sharing. Coding was done by two independent researchers. Specific risks were divided into appropriate categories. Meaningful units (complete sentences or parts of sentences) were defined as the analysis unit. The results were compared among researchers. Measure of correspondence was calculated between the two researchers who coded the answers. Discrepancies identified between the categorization of individual units of analysis among researchers were discussed among the researchers until reaching consensus. The frequency of risk mentioned in the discussions, as well as spontaneously mentioned risks, was described as descriptive statistics to indicate their relative importance in the individual risk categories. If PMPs mentioned measures for dealing with these risks and/or any additional comments related to the topic of the survey, these responses were also coded, analyzed, and presented.
Results
Participants
The study included 15 PMPs (13 women and two men). The average age of PMPs was 49 years (range 37–61 years). On average, they practiced for 16 years (range 5–25 years) as anesthesiologists and worked in pain treatment clinics for 7.7 years (range 2–15 years).
Observing patients who share their prescription analgesics with other patients for whom prescription is not intended
Until the interview began, 20% of PMPs were not aware whether their patients share analgesics, while 80% of PMPs had patients who admitted to such behavior. Regarding frequency of such behavior, five physicians indicated how often they see such patients; one said “often,” two “not so often,” and two “seldom.” “I noticed that especially women in the waiting room exchange opinions and give recommendations to each other about which analgesics they should take” (A).
Remembering particular instances, physicians mentioned having patients who shared opioid patches (N), tramadol in combination with acetaminophen (N), and seeing drug addicts bringing their parents to the clinic, asking for their parents’ opioid analgesics (L). “Such behavior is more characteristic of patients who do not visit the pain clinic on a regular basis. Such patients consume analgesics that they find at home, belonging to their family members in addition to the prescribed analgesics, and they determine the dose themselves. Then they take old drugs for new painful conditions without consulting a physician” (I).
An opinion was shared that patients with short-term acute pain are better candidates for sharing prescription analgesics than patients with chronic pain. “I believe that physicians rarely ask patients about this issue, but patients themselves sometimes say that they engage in such behavior, usually when I wanted to prescribe a drug with which a patient has already had a bad experience” (O).
Being on friendly terms with a patient may help in receiving such information. “It is not easy for patients to tell their pain physician that they are sharing prescription drugs with others; and to get that information, first you need to make friends with them” (B).
There may be even differences between different types of pain patients. “I probably rarely encounter patients who share prescription analgesics because I work mainly with patients with malignant diseases, where the main problem is patients’ rejecting the use of analgesics, especially opioids, who say that rejecting the use of analgesics is influenced by the family doctor, as patients and family physicians are afraid of addiction” (H).
None of the PMPs encountered a patient who was lending prescription analgesics.
Physicians’ perception of prescription analgesic sharing behavior
When asked about their perception of prescription analgesic sharing behavior, the participating PMPs offered varied opinions. Some physicians indicated that they perceive sharing of prescription analgesics as something negative, calling it irresponsible behavior (B, F, H, K); irresponsible and an indication that patients are not educated (C); irresponsible, but understandable (D, F); very risky (J); wrong and inappropriate (L). Others believed this sharing tendency was something positive (E); reasonable and with good intentions (A, I). Some indicated long-term negative consequences, but also certain positive aspects. “Such behavior is not dangerous in the short-term, but in the long run it is not right” (M). “It is not positive, but helps people to cope with their pain” (N). “It is done with good intentions, but I am not thrilled about this behavior” (O).
Knowing that patients engage in such behavior helps one physician to choose which analgesic will work better for a patient. “Analgesics are very accessible, and previous negative experience of a patient with an analgesic, such as side effects, inefficiency, etc, or positive experience, such as the effectiveness in relieving pain, helps me decide which drug to prescribe to that patient” (E).
Prescription analgesics sharing among patients as a risky behavior
Twelve PMPs considered prescription analgesics sharing “risky behavior”, while the others conferred that such behavior is “potentially risky” or “wrong.” Nearly every physician, 14 of 15, considered sharing analgesics risky, if “wrong” and “potentially risky” are included. One physician believed that such behavior is not risky (I). Physicians who suggested that such behavior is risky pointed out that this is especially true for opioids (E, K) and feared that patients are not aware of the risks: “They do not know the indications, contraindications, and interactions of analgesics” (A, J).
Potential risks of prescription analgesics sharing among the patients
When asked to name potential risks or negative, harmful consequences, two specific problems were indicated: vomiting as a possible adverse reaction while taking tramadol (A) and bleeding as a result of the interaction of warfarin and NSAIDs (A, B, I, L).
The others listed allergies as a potential problem. “Patients who share analgesics do not ask for drug allergies” (A). “Patients who have had an allergic reaction to some medication recognize it only by the brand name while probably its generic name and other brand name are not recognized, and they especially do not recognize if this drug is present in some combination analgesics” (B, D). “The dose of analgesics prescribed for one patient can be inadequate for another patient” (B).
Table 2 lists potential negative consequences of prescription analgesics sharing perceived by the study participants.
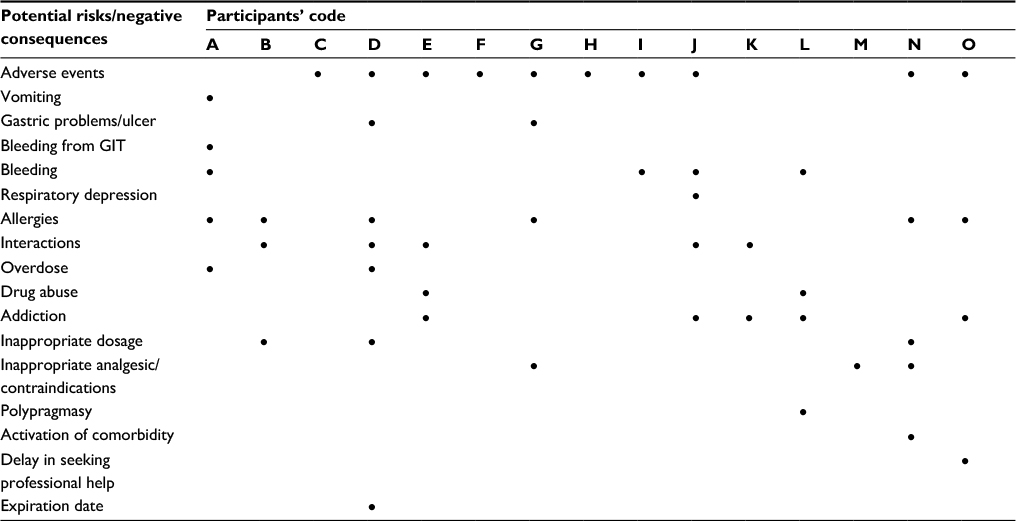 | Table 2 Potential risks associated with prescription analgesics sharing, identified by pain management physicians Abbreviation: GIT, gastrointestinal tract. |
Perception of potential positive side of prescription analgesics sharing among the patients
When asked for the potential positive side of sharing analgesics, five PMPs indicated that there is nothing positive about this behavior (C, F, G, H, M). The remaining PMPs stated that the positive aspects might be: good intentions (A); sharing could be a faster way to obtain analgesics (B); “patients borrow analgesics that are usually prescribed to them, but they ran out of it” (D); gaining experience (E, O); “it is positive if patients encourage each other to use analgesics belonging to the first level of the analgesic ladder according to WHO, such as NSAIDs and paracetamol” (I); “by engaging in sharing analgesics patients can relieve their pain until a visit to the doctor/dentist” (J); “it is positive when someone knows what he is doing” (K); it may be beneficial “when the patient has problems with the availability of primary health care” (N). One physician said that there might be something positive about it, but could not specify anything (L). Four physicians who responded that there is a positive side of analgesics sharing pointed out that they consider the risk more prevalent than benefit (B, E, J, L). Two of those who stated that it is positive that a patient is getting more experience with different medications elaborated that “a patient’s previous experience with analgesic, either positive or negative experience, can help them to make a decision about which analgesics can be recommended for pain treatment” (E, O). Considering potential adverse events, it was suggested that patients would be better-off to share advice about other interventions. “It would be more positive if patients would exchange experiences on non-pharmacological treatment of pain, such as acupuncture, than to engage in sharing analgesics” (L).
Potential differences between the risks of analgesics sharing depending on whether the analgesic is prescribed or bought over-the-counter (OTC)
OTC analgesics were perceived by some PMPs as less dangerous (C, I, O). Others indicated that OTC drugs may also be hazardous (A, D, J, K, M) or that there is no difference in risk (B, F). “Patients themselves are more afraid to share prescription analgesic than OTC” (B). Some considered that prescription analgesics are associated with a higher risk if shared (E, G, H, L, N) and that opioids are particularly dangerous (G, K). “OTC drugs are more accessible, but there is no significant difference in risk” (L). It was also said that OTC analgesics can be a problem if a patient does not read the instructions (M). “I see no difference in whether someone bought OTC analgesic or borrowed it from neighbors” (E).
Preventing sharing of prescription analgesics
When asked to suggest potential solutions, direct-to-consumers advertising was suggested as a problem by multiple physicians. “Patients are not educated enough to be exposed to direct-to-consumers advertising on television and the Internet because such advertisements provide insufficient information about drugs, especially regarding adverse events” (I, L). “The advertising of OTC analgesics should be completely prohibited because these drugs can cause many serious side effects, such as bleeding, analgesic nephropathy, Reye’s syndrome, and cardiovascular side effects” (J, K).
Some populations and types of drugs were perceived as more problematic. “Especially younger people become prone to indiscriminate use of OTC analgesics. From my experience, in particular OTC analgesics in the form of effervescent tablets are seen by patients as harmless” (J). “The problem is not only availability and liberal consummation of OTC analgesics, but also not reading the instructions that come with the medicine” (M).
Education of patients and an action on behalf of primary care were suggested as the potential remedies. “My pain clinic organized a month-long school for patients where they educate them about the pain and analgesics. Adherence of patients who attended this school was much better than of patients who did not attend such education” (D). “Prescription analgesics should be controlled by primary health care, because I assume that patients have a large stock of medicines in their home pharmacy” (N).
Discussion
This study shows that physicians specialized in pain management perceive sharing of prescription analgesics among patients as a common phenomenon; 80% of those interviewed encountered patients who share prescription analgesics. These data cannot be used for making conclusions about the prevalence of such behavior among patients, but it is certainly an indication that this problem should be addressed more carefully. Most of the participating physicians considered sharing of prescription analgesics a negative behavior with a number of perceived risks, but there were also opinions about potential positive and well-meaning aspects of that behavior. Several potential risks associated with prescription analgesics sharing were identified, related mostly to side effects, drug abuse, and inadequate help for patients.
According to a systematic review by Beyene et al, the prevalence of borrowing medication in different studies was reported to be 5%–52%, and for lending medication 6%–22%.7 Participants of this study stated that physicians should talk with their patients about sharing medications: “patients will tell you about it, if you ask them.” It was also suggested that it is not enough to ask the patient about sharing medications, but that physicians should “befriend” their patients in order to get them to open up about such behavior. In a study of Ward et al, 72% respondents who confessed to engaging in borrowing medications reported that their physicians asked them questions about medications they were taking and 34% of them said that they inform their doctor about their borrowing medications.10
None of the PMPs came across a patient who was lending prescription analgesics, mentioning that patients are prone to borrowing an analgesic from someone when their doctor wants to prescribe them that analgesic. In some previous studies: lending medication appeared to be a rare phenomenon compared to borrowing.1,2,6,9,18 Some doctors indicated that drug sharing can be considered positive because a patient’s experience with an analgesic will facilitate the decision of whether the analgesic should be prescribed to them or not. Some doctors have come across patients who shared opioid patches and tramadol in combination with acetaminophen, which may increase the chances for the development of adverse events, considering that some tramadol formulations already contain paracetamol.
One physician believed that women are more likely to engage in giving recommendations about drugs and sharing medications. Previous studies have not found gender differences in lending medications, but four studies have found that women are more likely to engage in borrowing of medications, which has not been confirmed in two other studies.1,2,6,9,18,19
It was suggested that patients who do not come on a regular basis to a pain clinic are more inclined to engage in sharing of prescription analgesics. Research about sharing medications among adolescents has indeed found that three-fourths of interviewees borrowed medication to avoid a health service visit.8
One physician opined that patients with short-term pain are more likely to engage in sharing of prescription analgesics than patients with long-term pain. A similar point of view was voiced by another participant, who pointed out that patients who suffer from a malignant disease are less likely to engage in sharing of medications than other patients. However, a study of Sheu et al found that patients with severe chronic pain were more likely to have abused a prescription medication or used an illicit drug to manage their pain than patients without severe chronic pain.20
One physician in this study mentioned having had the experience that drug addicts brought their parents to a pain clinic, claiming that parents suffer from pain for which they need opioids. It is already known that a problem with addiction increases the risk for the borrowing of prescription medications.14,21
Also another participant mentioned that there are problems with patients who refuse using analgesics, especially opioids. The PMP considered that such rejections of opioid analgesics are influenced by their family doctor, as patients and family doctors have concerns about addiction. Fear of addiction and lack of knowledge are the most frequent barriers to effective treatment of pain.22–24
Different levels of risks were perceived by the study participants, with most of them indicating that they consider sharing of prescription analgesics as unwanted behavior with potential negative consequences, while some found certain positive aspects to it, such as being benevolent behavior, helping patients to get drugs when they need them, and helping them cope with pain. One physician even indicated that this is a good way for patients to try different analgesics so that it helps later to make clinical decisions about a prescription analgesic that will be recommended to a patient. When asked to name potential risks associated with such behavior, most of the participants cited adverse reactions as a potential risk. A study of Goldsworthy et al reported there were 37% participants who reported having an adverse event after borrowing prescription medications.8 It is likely that people who share prescription medication have greater risk of accidental overdoses. It has been reported that accidental opioid overdose was commonly due to prescribed and illicit polysubstance use, medication-taking errors, and inadequately treated chronic pain.25
One physician wondered whether patients check the expiry dates when sharing. In a study conducted among female students in Malaysia, it was found that 29% always controlled expiry dates of drugs, 54% sometimes, and only 6.9% did not control it.5
Problems with the access to health care have been cited in previous studies as a factor that contributes to the sharing of medications.19,26 One of the main reasons for borrowing medication in the studies was not having a medication which they normally used.2,26,27 The desire to help someone was one of the identified reasons for engaging in lending medications.2,28 Cultural and legal issues also need to be taken into account. Sharing medications in some cultures can be expressed as care for others when they are ill.29,30 In the USA, this behavior is illegal; a patient cannot lawfully share or borrow prescription pain medication because it is considered pharmaceutical diversion, and a prescriber cannot continue to prescribe when they know that the patient shares the prescribed medication. Such law does not exist in Croatia.
Participating physicians had differing opinion about the relative risk of OTC and prescription analgesics, with some saying that sharing of prescription analgesics was more risky, some indicated that sharing of OTC analgesics is more risky, while there was also an opinion that there is no difference in risk. Particular danger of sharing opioids was identified.
Regarding potential remedies that could prevent patients from engaging in sharing of prescription analgesics, the participating physicians pointed out to dangers of direct-to-consumer marketing of OTC analgesics. Advertising can give a false sense of security of advertised drugs and contribute to the increased request for the prescription of drugs.31 It was mentioned that especially younger people become inclined to indiscriminate use of OTC analgesics and that OTC analgesics, such as those in the form of effervescent tablets, are seen as harmless. This observation is consistent with the results of several studies that have found that younger people are more inclined to share medications than older ones.1,5,21 However, Goldsworthy et al did not find a correlation between age and lending medication.8
Education was mentioned as one potential solution for preventing patients from sharing prescription analgesics, as well as prompting patients to read information about a drug, and encouraging general practitioners to enquire with patients about the contents of their home pharmacy. It was reported that 10% of respondents kept medicine for future use.5 A previous systematic review and meta-analysis, which included 14 studies of patient education interventions in primary care, found that patient education, especially issued by physicians, increases long-term reassurance in patients with acute low back pain.32 Another systematic review and meta-analysis with nine trials reported that therapeutic patient education has an effect for patients with migraine.33 However, one study showed that pain management training of health care professionals is not adequate.34 Fishman et al recommended early education about pain management in order to annul incongruity between students’ opinion and the reality they are facing in their practice.24 Therefore, careful consideration of potential remedies for patient sharing prescription is in order, and future studies on that subject would be welcome.
Limitations
This study had several limitations. There is a possibility of a nonresponse error, that is, risk that those that did not respond have different views from those who did. There may be cross-cultural differences, health and prescription drug delivery systems between different countries and this needs to be taken into account when interpreting the results. The sample size was rather small, with 15 PMPs included. However, based on a survey of pain clinics in Croatia, published in 2015, there were 70 anesthesiologists employed in them.35 If this number is still the same, this sample constitutes 21% of the PMPs who work in pain clinics in Croatia. With larger sample size, the results could be more compelling and statistical comparisons between responses might then be possible. Temporal patterns were not analyzed in this study; physicians could have observed analyzed behavior recently or long time ago, since some of them were practicing for a long time. The study did not separate opioids from non-opioids and OTC analgesics. The risk and safety profile of different analgesics are different; since this qualitative study served for hypothesis generation, future studies can address these issues in a structured manner. This study did not differentiate between practice settings for PMPs in cancer pain vs chronic pain management, because pain clinics are not specialized for different types of pain; observations of the included participants were simply recorded. Physician and patient populations would be expected to have different attitudes regarding sharing medications; therefore, future studies on this topic should analyze such perception of risk among patients.
Conclusion
The majority of physicians specialized in pain management have come across patients sharing prescription analgesics. Most of them considered this as risky behavior with a number of potential consequences. It has been noted that this problem is neglected and that physicians should inquire about drug sharing. Direct-to-consumers advertising was perceived as a factor contributing to such behavior. Patient education and more involvement of physicians in identifying this behavior were cited as potential remedies for preventing sharing of prescription analgesics.
Disclosure
The authors report no conflicts of interest in this work.
References
Petersen EE, Rasmussen SA, Daniel KL, Yazdy MM, Honein MA. Prescription medication borrowing and sharing among women of reproductive age. J Womens Health (Larchmt). 2008;17(7):1073–1080. | ||
Goldsworthy RC, Schwartz NC, Mayhorn CB. Beyond abuse and exposure: framing the impact of prescription-medication sharing. Am J Public Health. 2008;98(6):1115–1121. | ||
Loyola Filho AI, Lima-Costa MF, Uchoa E. Bambui project: a qualitative approach to self-medication. Cadernos de saude publica. 2004;20(6):1661–1669. | ||
Montastruc JL, Bagheri H, Geraud T, Lapeyre-Mestre M. [Pharmacovigilance of self-medication]. Therapie. 1997;52(2):105–110. French. | ||
Ali SE, Ibrahim MI, Palaian S. Medication storage and self-medication behaviour amongst female students in Malaysia. Pharm Pract (Granada). 2010;8(4):226–232. | ||
Daniel KL, Honein MA, Moore CA. Sharing prescription medication among teenage girls: potential danger to unplanned/undiagnosed pregnancies. Pediatrics. 2003;111(5 Pt 2):1167–1170. | ||
Beyene KA, Sheridan J, Aspden T. Prescription medication sharing: a systematic review of the literature. Am J Public Health. 2014;104(4):e15–e26. | ||
Goldsworthy RC, Mayhorn CB. Prescription medication sharing among adolescents: prevalence, risks, and outcomes. J Adolesc Health. 2009;45(6):634–637. | ||
Goulding E, Murphy M, Di Blasi Z. Sharing and borrowing prescription medication: a survey of Irish college students. Ir J Med Sci. 2011;180(3):687–690. | ||
Ward L, Patel NM, Hanlon A, Eldakar-Hein S, Sherlinski K, Ward SH. Prescription medication borrowing among adult patients at an urban medical center. J Urban Health. 2011;88(6):997–1014. | ||
Goebel JR, Compton P, Zubkoff L, et al. Prescription sharing, alcohol use, and street drug use to manage pain among veterans. J Pain Symptom Manage. 2011;41(5):848–858. | ||
Markotic F, Cerni Obrdalj E, Zalihic A, et al. Adherence to pharmacological treatment of chronic nonmalignant pain in individuals aged 65 and older. Pain Med. 2013;14(2):247–256. | ||
Ellis J, Mullan J. Prescription medication borrowing and sharing--risk factors and management. Aust Fam Physician. 2009;38(10):816–819. | ||
Morasco BJ, Dobscha SK. Prescription medication misuse and substance use disorder in VA primary care patients with chronic pain. Gen Hosp Psychiatry. 2008;30(2):93–99. | ||
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. | ||
Briner M, Manser T. Clinical risk management in mental health: a qualitative study of main risks and related organizational management practices. BMC Health Serv Res. 2013;13:44. | ||
HDLB. Pain Treatment Clinics; 2015. Available from: http://www.hdlb.org/za-bolesnike/ambulante-za-lijecenje-boli/. | ||
Hogan DJ, Moreland A, Lane P, Lal S. Exchange of prescription medications by dermatology outpatients. J Am Acad Dermatol. 1990;23(5 Pt 1):953. | ||
Jatrana S, Crampton P, Norris P. Ethnic differences in access to prescription medication because of cost in New Zealand. J Epidemiol Commun Health. 2011;65(5):454–460. | ||
Sheu R, Lussier D, Rosenblum A, et al. Prevalence and characteristics of chronic pain in patients admitted to an outpatient drug and alcohol treatment program. Pain Med. 2008;9(7):911–917. | ||
Caviness CM, Anderson BJ, de Dios MA, Kurth M, Stein M. Prescription medication exchange patterns among methadone maintenance patients. Drug Alcohol Depend. 2013;127(1–3):232–238. | ||
Goebel JR, Sherbourne CD, Asch SM, et al. Addressing patients’ concerns about pain management and addiction risks. Pain Manag Nurs. 2010;11(2):92–98. | ||
Vallerand AH, Hasenau SM, Templin T. Barriers to pain management by home care nurses. Home Healthc Nurse. 2004;22(12):831–838; quiz 839–840. | ||
Fishman SM, Young HM, Lucas Arwood E, et al. Core competencies for pain management: results of an interprofessional consensus summit. Pain Med. 2013;14(7):971–981. | ||
Yarborough BJ, Stumbo SP, Janoff SL, et al. Understanding opioid overdose characteristics involving prescription and illicit opioids: a mixed methods analysis. Drug Alcohol Depend. 2016;167:49–56. | ||
Gornick ME, Eggers PW, Reilly TW, et al. Effects of race and income on mortality and use of services among Medicare beneficiaries. N Engl J Med. 1996;335(11):791–799. | ||
Ellis JC, Mullan J, Worsley T. Prescription medication hoarding and borrowing or sharing behaviours in older residents in the Illawarra, New South Wales, Australia. Australas J Ageing. 2011;30(3):119–123. | ||
Daniel KL, Goldman KD, Lachenmayr S, Erickson JD, Moore C. Interpretations of a teratogen warning symbol. Teratology. 2001;64(3):148–153. | ||
Hodgetts D, Nikora LW, Rua M. Māori men and the indirect procurement and sharing of prescription medications. AlterNative. 2011;7(2):152–162. | ||
Kamutingondo S, Groot S, Hodgetts D, Nikora LW. Understandings and social practices of medications for Zimbabwean households in New Zealand. MAI Rev. 2011;3:1–17. | ||
Bell RA, Kravitz RL, Wilkes MS. Direct-to-consumer prescription drug advertising, 1989-1998. A content analysis of conditions, targets, inducements, and appeals. J Fam Pract. 2000;49(4):329–335. | ||
Traeger AC, Hubscher M, Henschke N, Moseley GL, Lee H, McAuley JH. Effect of primary care-based education on reassurance in patients with acute low back pain: systematic review and meta-analysis. JAMA Intern Med. 2015;175(5):733–743. | ||
Kindelan-Calvo P, Gil-Martinez A, Paris-Alemany A, et al. Effectiveness of therapeutic patient education for adults with migraine. A systematic review and meta-analysis of randomized controlled trials. Pain Med. 2014;15(9):1619–1636. | ||
Upshur CC, Luckmann RS, Savageau JA. Primary care provider concerns about management of chronic pain in community clinic populations. J Gen Intern Med. 2006;21(6):652–655. | ||
Fidahic M, Dogan K, Sapunar D, Puljak L. National survey of pain clinics in Croatia: Organization and services. Acta Med Acad. 2015;44(1):18–30. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.