")
Back to Journals » Clinical Epidemiology » Volume 15
Risk of Obesity Among Children Aged 2–6 Years Who Had Prolonged Screen Time in Taiwan: A Nationwide Cross-Sectional Study
Authors Chang RY, Chen TL, Yeh CC, Chen CH, Wang QW, Toung T, Liao CC
Received 19 July 2022
Accepted for publication 21 January 2023
Published 13 February 2023 Volume 2023:15 Pages 165—176
DOI https://doi.org/10.2147/CLEP.S382956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Vera Ehrenstein
Rui-Yu Chang,1 Ta-Liang Chen,2– 4,* Chun-Chieh Yeh,5,6 Ching-Hsiang Chen,7 Qiao-Wen Wang,8 Thomas Toung,9 Chien-Chang Liao3,4,10– 13,*
1Department of Sport Promotion, National Taiwan Sport University, Taoyuan, Taiwan; 2Department of Anesthesiology, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 3Department of Anesthesiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan; 4Anesthesiology and Health Policy Research Center, Taipei Medical University Hospital, Taipei, Taiwan; 5Department of Surgery, China Medical University Hospital, Taichung, Taiwan; 6Department of Surgery, University of Illinois, Chicago, IL, USA; 7Physical Education Office, China Medical University, Taichung, Taiwan; 8Doctoral Program of Educational Leadership and Technology Management, Tamkang University, Taipei, Taiwan; 9Department of Anesthesiology and Critical Care Medicine, The Johns Hopkins Hospital, Baltimore, MD, USA; 10Department of Anesthesiology, Taipei Medical University Hospital, Taipei, Taiwan; 11Research Center of Big Data and Meta-Analysis, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 12School of Health Care Administration, Taipei Medical University, Taipei, Taiwan; 13School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Chien-Chang Liao, Department of Anesthesiology, Taipei Medical University Hospital, 252 Wuxing Street, Taipei, 110, Taiwan, Email [email protected]
Objective: To evaluate the risk of obesity in preschool children with prolonged screen time in Taiwan.
Methods: Using a nationwide survey with random sampling, we collected information on 8378 preschool children aged 2– 6 years among 206 preschools in Taiwan from 2016 to 2019. Socioeconomic data, body mass index, and lifestyle of the preschool children and their caregivers were compared among the groups of preschool children who had moderate and prolonged daily screen time. We used multiple log-binomial regression models to calculate the adjusted prevalence ratios (PRs) and 95% confidence intervals (CIs) of obesity associated with prolonged screen time.
Results: The prevalence of obesity in the preschool children was 13.1%, and the average screen time was 104.6 minutes. Children’s age, sleep hours, outdoor play time, sugar intake, snack eating before dinner, sleep disturbance, and obesity, as well as caregiver’s sex, age, education, screen time, exercise time and parent obesity were factors related to high screen time for preschool children. Compared with children with moderate screen time, children with prolonged screen time had a higher risk of obesity (PR, 1.45; 95% CI, 1.18– 1.79). With a 60-minute increase in screen time, the risk of obesity increased, with an PR of 1.10 (95% CI, 1.03– 1.17).
Conclusion: Preschool children with prolonged screen time had an increased risk of obesity in Taiwan. Interventions may be needed for this very susceptible population.
Keywords: digital media, obesity, preschool children, screen time, television
A Letter to the Editor has been published for this article.
Introduction
Prolonged screen time has become a crucial public health problem worldwide that is associated with poor health outcomes in young children, including obesity, sleep disturbance, and aggressive behavior,1–6 as well as a risk of increasing depression,7 exposure to violence and unsafe content and contacts,5 and negative language development.8 It also has immediate correlations with being sedentary.6,9 The reported prevalence of screen time in children has widely varied because of differences in age, gender, socioeconomic status, lifestyle, and home education.4,10–13 In Canada, a recommendation of screen time for young children claimed that no screen time is recommended for children under 2 years of age and that screen time should be limited to less than 1 hour to 2 hours a day for children aged 2 to 4 years; parents should help their children to meet this goal.14 The American Academy of Pediatrics also indicated that 2- to 5-year-old children should not use media over 2 hours per day;3,6 in addition, some research suggests that preschool children should spend less than 2 hours per day engaging in screen time.15,16
However, the average daily screen time among preschool children varies by age and country, ranging from 71.3 minutes in Canada to 125.7 minutes in Switzerland.9,14,17,18 In America, approximately 63.4% of obese preschool children spend over 2 hours per weekday in screen time.10 Australian children aged 3–5 years spent 108.5 minutes per day in screen time.9 In Asia, Japanese preschool children had an average of 118.6 minutes in screen time in 2018.19 Among preschool children aged lower than 5 years in Bangladesh, the average of screen time is 160.9 minutes in 2019.20 Preschool-aged children in Hong Kong had an average of 147 minutes in screen time in 2019–2020.21 Although screen time showed little differences among countries, there still appears to be an increase in screen time in preschool children worldwide,22 particularly during the COVID-19 pandemic period and we need to consider some solutions to seriously reduce and limit screen time.20,23
Because overweight or obesity starting at a young age commonly persists to old age, obesity prevention needs to be focused on the preschool stage.10,24 Parents’ practices and beliefs is one of factors related to children’s lifestyles. It was suggested that making rules for screen time and controlling the home environment may be helpful to maintain children’s health physical status, including normal body mass index.25,26 If parents restricted the screen time of preschool children, they were more likely to achieve the Academy of Pediatrics recommendation of screen time.3,25
Although the problem of prolonged screen time in preschool children with overweight or obesity has been raised in previous studies,10,11,15,26–28 the association between screen time and obesity risk in preschool children remains incompletely understood because of some study limitations, such as small sample sizes,15,26,28 nonrandom sampling,15,26 inadequate control for potential confounding factors,15,26–28 and a lack of detailed information on screen time.10,27
In addition, limited information was available regarding the screen time in preschool children in Taiwan. The purpose of this study was to investigate the association between screen time and obesity status among preschool children in Taiwan using a nationwide survey with random sampling.
Methods
Source of Data
Taiwan is an island nation with a population of approximately 23 million people. This survey was conducted from October 2018 to March 2019 using mailed questionnaire interviews with preschool children’s parents or caregivers. We randomly selected preschools from an official list, and these preschools were legal and regulated by Taiwan’s Ministry of Education. We made telephone calls and queried the possibility of the school participating in this questionnaire-based survey. At the beginning of the telephone call, the interviewer explained the study purpose and asked if the person in charge of the preschool would participate in the interview. We mailed questionnaires to the preschools when obtaining the agreement to participate. We calculated the adequate number of preschools to include according to the populations of each city or county until the number of participating children reached appropriately six thousand per year. This study included three years of data; we collected each year of data from October to December through January to March of the next year. These cities or counties included northern areas (Taipei City, New Taipei City, Keelung City, Taoyuan City, Hsinchu City, Hsinchu County, and Yilan County), central areas (Miaoli County, Taichung City, Changhua County, Nantou County, and Yunlin County), southern areas (Chiayi City, Chiayi County, Tainan City, Kaohsiung City, and Pingtung County) and eastern areas (Hualien County, Taitung County) and outlying islands of Taiwan.
Study Population
Before the formal investigation, we conducted a pilot study in 2016 to ensure the validity and reliability of the questionnaire.29 To establish the surface validity and content validity of the questionnaire, we invited five professional experts to participate in the review and revision of the preliminary questionnaire (revising semantics of sentences or uncertain words). Then, a total of twenty-two main caregivers of preschool children who had been asked to complete the same questionnaires twice within two weeks were asked to pretest the questionnaire to detect the test-retest reliability, with a coefficient of 0.891, which reached the acceptable range.
The formal questionnaires were sent to the preschools after a phone invitation to obtain agreement. After the questionnaires were sent to the preschools, teachers or administrative staff helped to give the questionnaires to parents or caregivers. After completing the questionnaire, the parents or caregivers returned them to preschool staff in two weeks; if they did not agree to participate in the survey, they could choose to not return the questionnaire or to return a blank questionnaire. When collection had finished, the preschool staff sent the returned questionnaires back to us. We invited the main caregivers to answer questions and complete the questionnaire including the information of preschool children’s lifestyle habits, health status, height, weight, sleep patterns and other related factors of preschool children’s daily life. In this study, we considered that preschools were registered in the official list of the Bureau of Education were eligible preschools. Children studied in the registered preschools were eligible study subjects.
The Supplementary Figure S1 showed the selection process of study subjects. In the first study year (from October 2016 to January 2017), we randomly selected 122 preschools from the official list of Ministry of Education that included all preschools (6735 preschools) in Taiwan. With the contact by mail and telephone, we received the consent and approval from 75 preschools and 6120 questionnaires were mailed. Then, there were 67 preschools completed and returned 4327 questionnaires. After careful review, checkup, and evaluation of the content of questionnaires (excluding the missing data in age, sex, BMI, and screen time), there were 3075 eligible children were enrolled in this study. In the second study year (from December 2017 to March 2018), we randomly selected 142 preschools from the official list of Ministry of Education that included all preschools (6729 preschools) in Taiwan. With the contact by mail and telephone, we received the consent and approval from 97 preschools and 5789 questionnaires were mailed. Then, there were 70 preschools completed and returned 3409 questionnaires. After careful review, checkup, and evaluation of the content of questionnaires (excluding the missing data in age, sex, BMI, and screen time), there were 2443 eligible children were enrolled in this study. In the third study year (from November 2018 to January 2019), we randomly selected 137 preschools from the official list of Ministry of Education that included all preschools (6721 preschools) in Taiwan. With the contact by mail and telephone, we received the consent and approval from 94 preschools and 5908 questionnaires were mailed. Then, there were 69 preschools completed and returned 3746 questionnaires. After careful review, checkup, and evaluation of the content of questionnaires (excluding the missing data in age, sex, BMI, and screen time), there were 2860 eligible children were enrolled in this study. Finally, we collected adequate information from 8378 preschool children. Overall, the response rate of preschools was 51.3% (206/401) and the participation rate of children was 47% (8378/17817).
Among 8378 preschool children, informed consent was obtained from the main caregivers. Our study complies with the Declaration of Helsinki. This study was evaluated and approved by the Institutional Review Board of Fu-Jen University, Taiwan (C105002 and C105122).
Exposure
Screen time was defined as time spent on screen-based media, such as watching television, DVDs, or videos or playing computer or video games,1 as well as smart phone and tablet usage. Main caregivers (parents) responded to the questionnaire regarding their children’s television time and digital devices time by their observation and memory. We calculated the daily screen time included daily television time plus daily digital devices time. According the international recommendations of screen time,30–32 preschool children in this study were categorized into two groups as moderate screen time (1.0–4.9 years of age: ≤60 minutes per day; 5.0–6.9 years of age ≤120 minutes per day) and prolonged screen time (1.0–4.9 years of age: >60 minutes per day; 5.0–6.9 years of age: >120 minutes per day).
Outcomes
Preschool children’s height and weight were measured by caregivers or preschool teachers. The body mass index of preschool children was calculated according to the latest available growth curve standard of Taiwanese children and adolescents, which was announced by the Ministry of Health and Welfare of Taiwan,33 to classify the body mass index standard of preschool children by age. The categories of body mass index include lean (the growth curve standard is lower than the 5th percentile), normal (the growth curve standard is between the 5th and 85th percentile), overweight (the growth curve standard is higher than the 85th and lower than or equal to the 95th percentile), and obesity (the growth curve standard is >95th percentile).33 Based on the above four growth curve categories, the preschool children in this study were divided into an obesity group (the growth curve > 95th percentile) and a non obesity group (the growth curve ≤ 95th percentile).33
Covariates
The content of the questionnaire included basic characteristics of the preschool children, such as sex, age, height, weight, screen time (including time spent watching television, videos or DVDs and playing with computers, tablets, smartphones or video games),1,8,10,13 sleep hours, sleep disturbance, outdoor play time, and other related lifestyle habits; information was also collected regarding the personal characteristics of the caregiver, such as sex, age, education, and other related lifestyle habits.
Eating snacks were defined as preschool children eating snacks before dinner frequently. Daily intake of sugar was categorized into three groups including seldom, sometimes, and frequently. We also collected the information of outdoor play time and it was divided into three groups included 0–60 minutes/day, 61–120 minutes/day, and >120 minutes/day.
We used the standards of sleep time duration recommendations of the National Sleep Foundation to distinguish sleep hours.34 If the sleep hours of preschool children not meeting age-specific sleep recommendations (1.0–2.9 years: 11.0–14.9 hours/day; 3.0–4.9 years: 10.0–13.9 hours/day; 5.0–13.9 years: 9.0–11.9 hours/day), it meant preschool children had sleep deprivation. Sleep disturbance was defined as sleep problems occurred in the duration of sleep included sleep talking, primary snoring, sleep terrors, nightmares, obstructive sleep apnea, and sleep walking and excluded enuresis and bruxism which often happen at preschool children.
Caregivers are the main person responsible for taking care of the daily routine of preschool children at home, and caregivers are usually the parents of the preschool children. In this study, caregivers included mothers (85.49%), fathers (6.46%), grandmothers (5.74%), grandfathers (1.41%) and other relatives (0.90%). Caregiver education was divided into four groups: high school (caregiver education lower than and equal to high school), college, university, and graduate school (caregiver education higher than and equal to graduate school). According to the criteria from the Ministry of Health and Welfare in Taiwan, caregiver’s obesity was defined as body mass index ≥ 27 kg/m2 in this study.35,36
Statistical Analysis
We used chi-square tests and t tests to compare the distribution of the characteristics among preschool children with low, moderate and high screen times. The characteristics of caregivers were also examined by chi-square tests and t tests among children with low, moderate and high screen times. Multiple log-binomial regression models were used to calculate adjusted prevalence ratios (PRs) and 95% confidence intervals (CIs) of screen time associated with obesity. Stratified analyses by age, sex, and other characteristics were also performed by calculating adjusted PRs and 95% CIs to investigate the association between prolonged screen time and obesity in preschool children. We also calculated the risk of obesity in children with prolonged screen time compared with children had zero screen time (caregivers reported their children had no) in the Supplementary Table S1. All analyses were performed with SAS software, version 9.4 (SAS Institute Inc., Carey, NC).
Results
Among 8378 preschool children with a mean age of 4.91±0.95 years (Table 1), the prevalence of obesity was 13.1%. Preschool children spent an average of 104.6±81.1 minutes per day on screen time, and 46.6% of them had prolonged screen time. A higher proportion of prolonged screen time existed among children with (versus without) the following characteristics: boys, aged 4 years, sleep deprivation, outdoor play time >120 minutes, frequent sugar intake, snack eating before dinner frequently, and obesity.
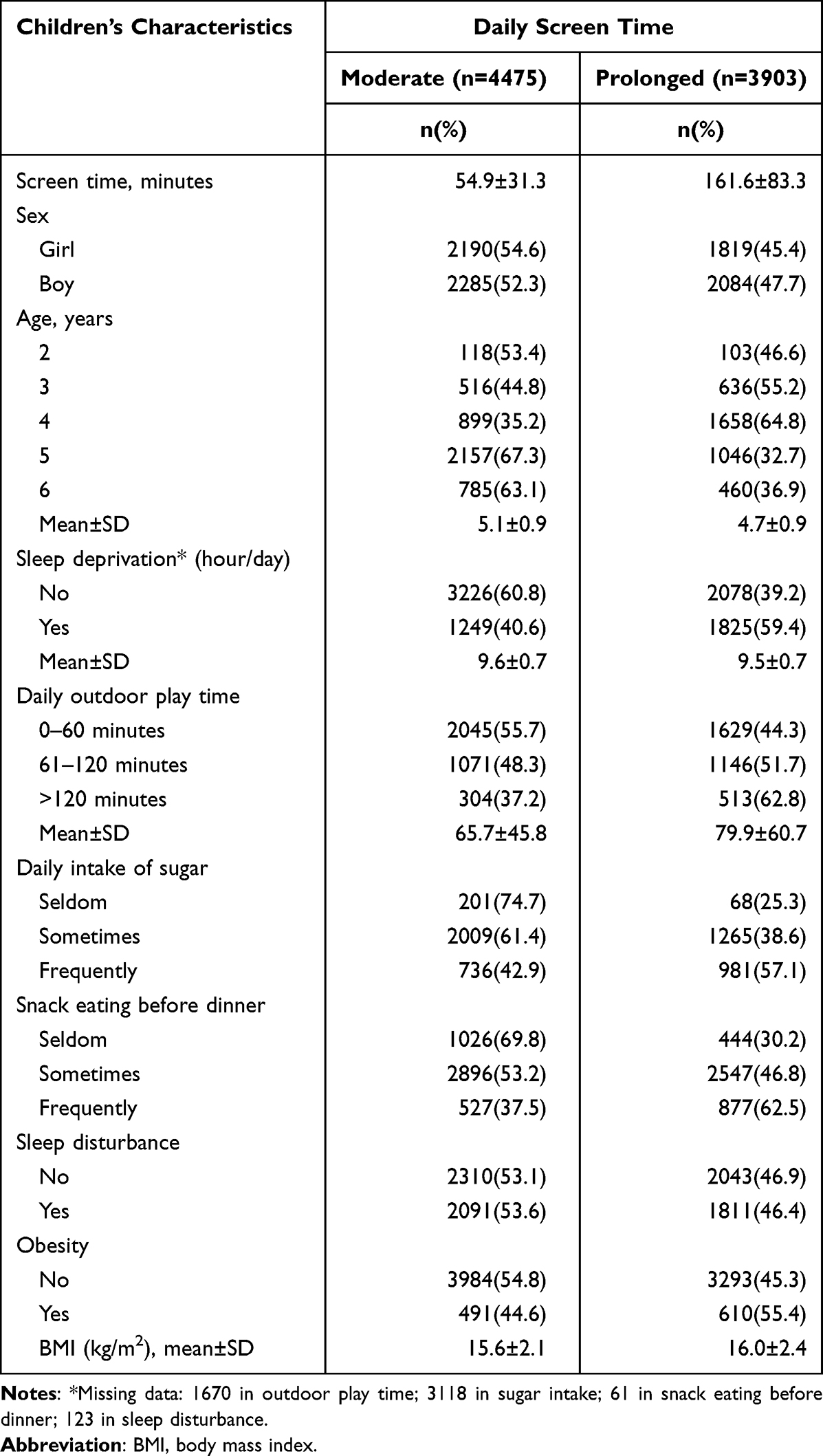 |
Table 1 Characteristics of Preschool Children by Screen Time (N=8378)* |
Table 2 shows that the children whose main caregivers were male, 45–59 years old, with a junior high school level of education, screen time > 240 minutes, exercise time >60 minutes, and obesity had higher proportion of prolonged screen time than those without these characteristics.
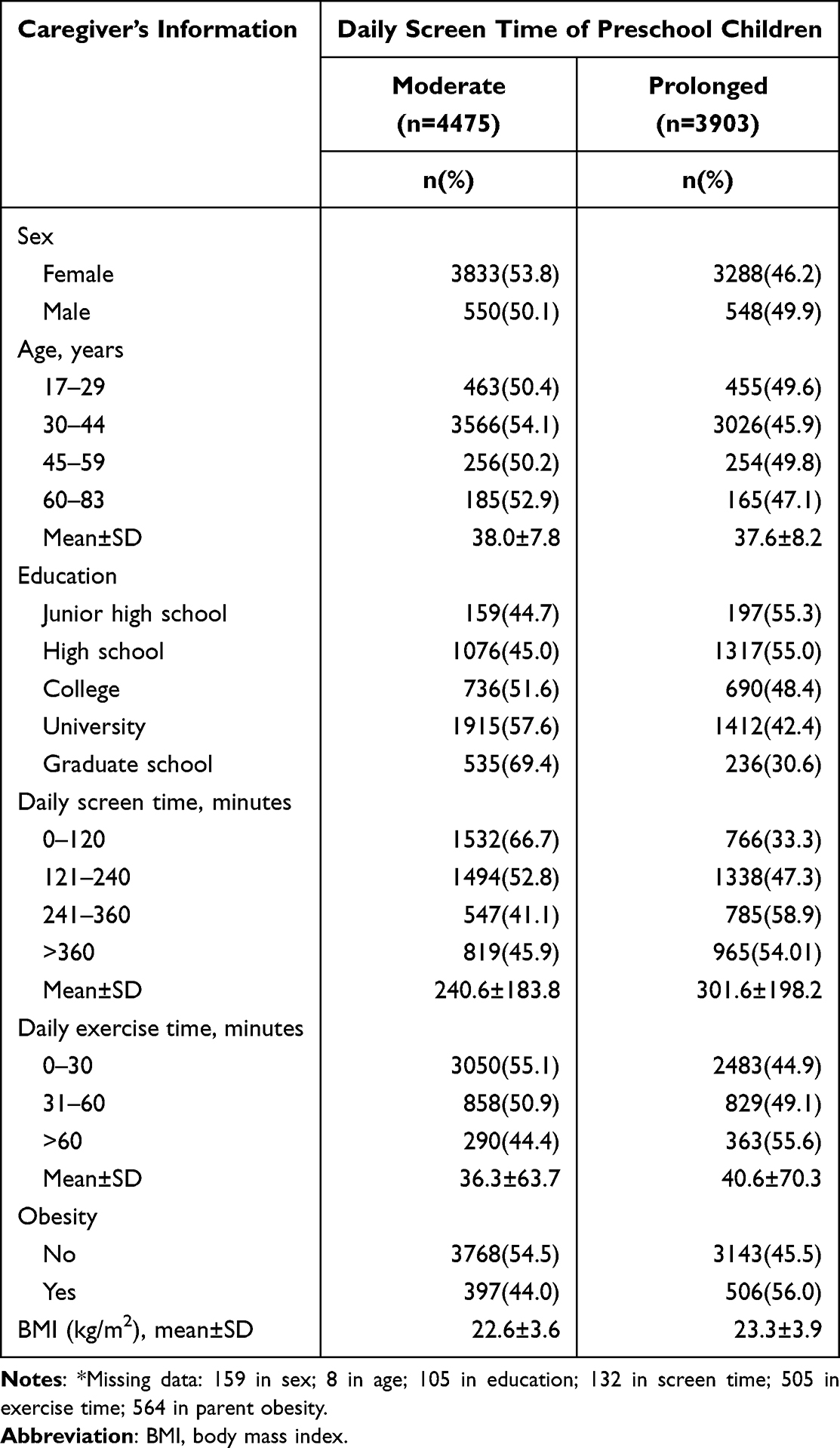 |
Table 2 Baseline Characteristics of Caregiver by Preschool Children’s Screen Time* |
In the multiple log-binomial regression models (Table 3), children with prolonged screen time had an increased risk of obesity compared with children with moderate screen time (PR, 1.45; 95% CI, 1.18–1.79). The adjusted PRs of obesity risk in preschool children with prolonged television time (>120 minutes) was 1.46 (95% CI, 1.18–1.80).
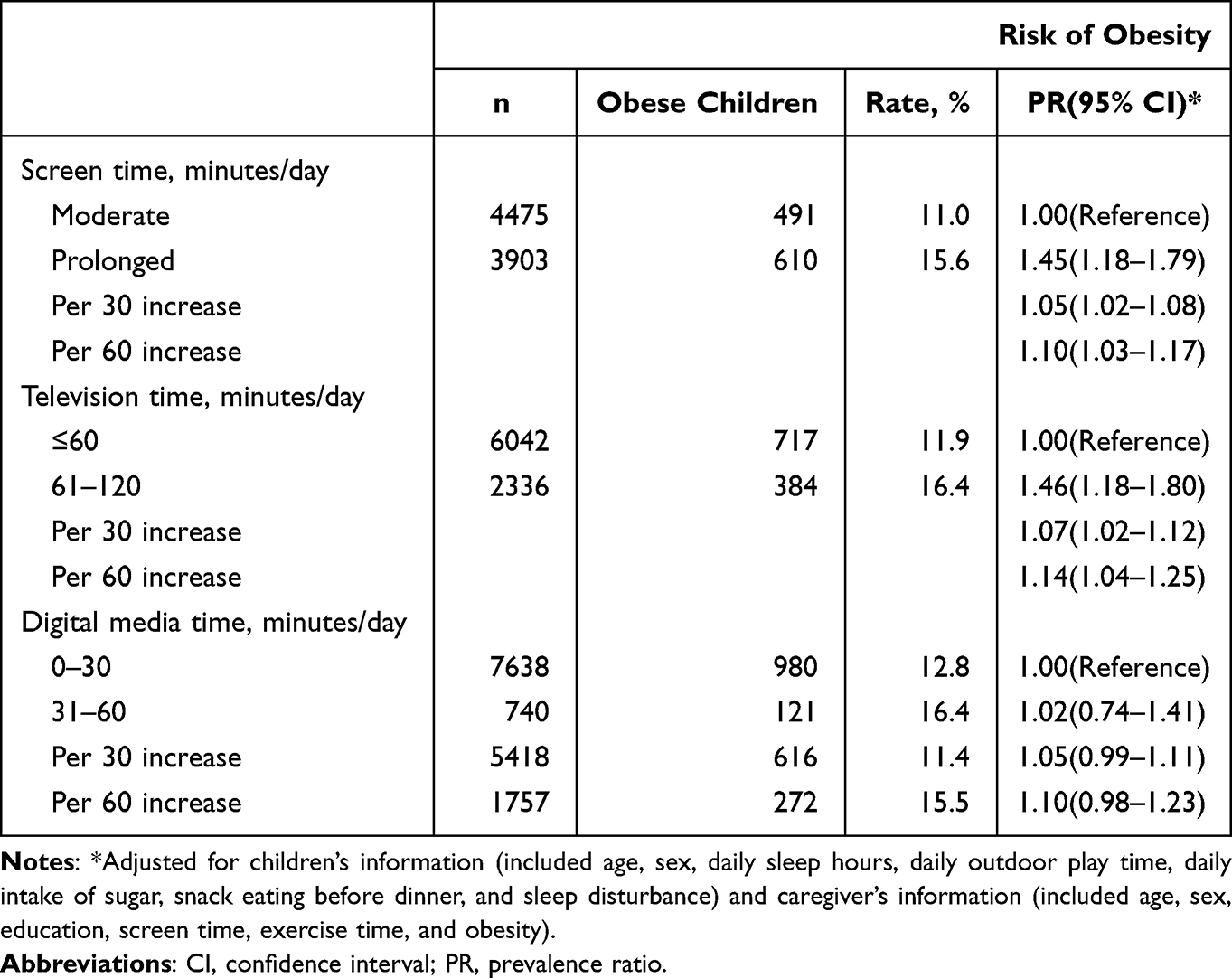 |
Table 3 Adjusted Prevalence Ratios and 95% Confidence Intervals of Obesity Associated with Preschool Children’s Daily Screen Time, Television Time, and Digital Media Time |
In the stratified analysis (Table 4), the association between prolonged screen time (reference group: children without prolonged screen time) and obesity was significant in preschool children who were: girls (PR, 1.72; 95% CI, 1.21–2.45), boys (PR, 1.32; 95% CI, 1.01–1.71), 3 years of age (PR, 1.85; 95% CI, 1.02–3.37), who had no sleep deprivation (PR, 1.72; 95% CI, 1.32–2.23), outdoor play time>120 minutes (PR, 2.26; 95% CI, 1.15–4.46), sometimes sugar intake (PR, 1.55; 95% CI, 1.18–2.02), sometimes eating snacks before dinner (PR, 1.47; 95% CI, 1.13–1.91), and sleep disturbance (PR, 1.60; 95% CI, 1.22–2.09). The risk of obesity in association with high screen time was also significant in children’s caregivers with the following characteristics (Table 5): female sex (PR, 1.46; 95% CI, 1.17–1.82), 30–44 years of age (PR, 1.45; 95% CI, 1.15–1.84), college level of education (PR, 1.84; 95% CI, 1.10–3.11), 241–360 minutes of screen time (PR, 3.20; 95% CI, 1.61–6.35), exercise time 31–60 minutes (PR, 1.56; 95% CI, 1.00–2.45), and obesity (PR, 1.71; 95% CI, 1.03–2.83).
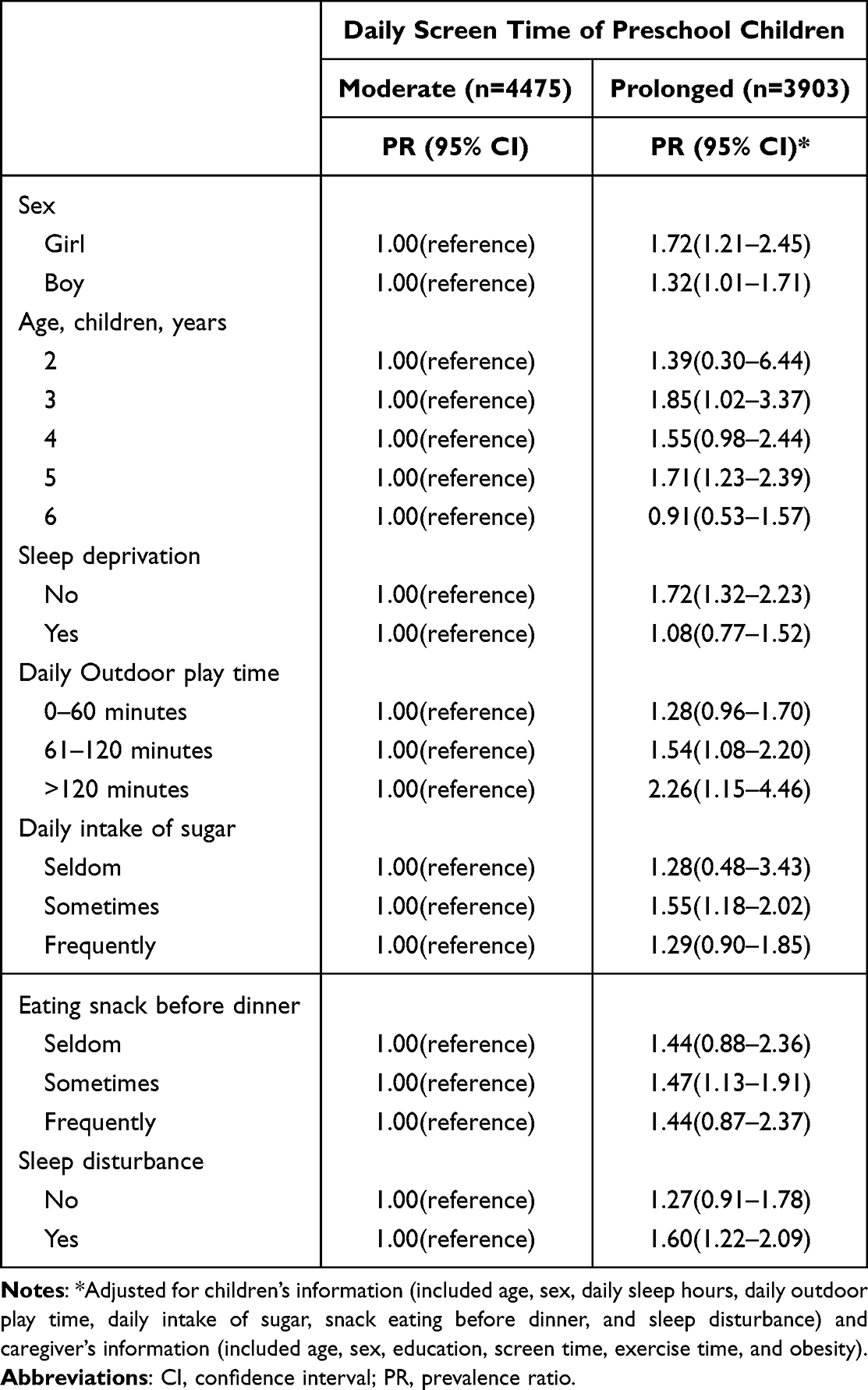 |
Table 4 Stratified Analysis by Preschool Children’s Characteristics for the Risk of Obesity Associated with Daily Screen Time |
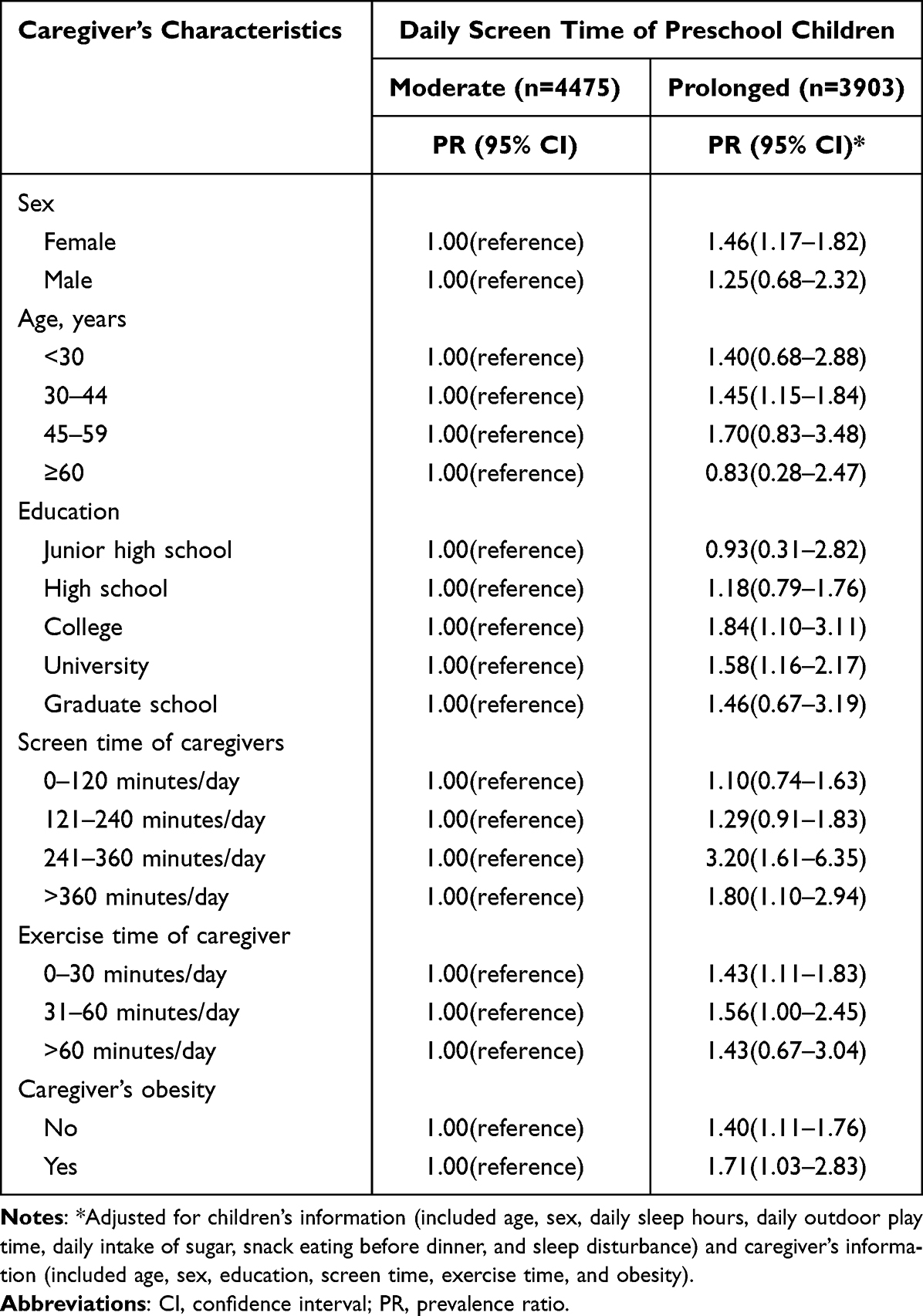 |
Table 5 Stratified Analysis by Caregiver’s Characteristics for the Risk of Obesity Associated with Prolonged Screen Time in Preschool Children |
In the Table S1, compared to children with zero screen time, children with prolonged screen time had increased risk of obesity (PR, 3.36; 95% CI, 1.07–10.6). The characteristics of children (Table S2) and caregivers (Table S3) among children with female caregivers was showed in the Supplementary Files. Among children with female caregivers (Table S4), children’s prolonged screen time was associated with risk of obesity (PR, 1.46; 95% CI, 1.16–1.82).
Discussion
We found that there was a high prevalence of obesity and prolonged screen time among preschool children in Taiwan. Preschool children with prolonged screen time had an increased risk of obesity, and this association existed significantly in many subgroups. High television time and high digital media time were also associated with obesity risk. Our study is a large population-based study that raised the influence of screen time on obesity risk among preschool children in Asian countries.
In this study, the average daily screen time among preschool children in Taiwan was approximately 2 hours, which was lower than that in the United States, Switzerland, Australia, Finland and Japan9–11,17,18 but higher than that in Canada.14 Information regarding screen time in Taiwan’s preschool children was limited. According to the recommendation by the American Academy of Pediatrics, the daily screen time should be less than 2 hours.3,15,16 However, we found that 27% of preschool children in Taiwan had a screen time of more than 2 hours per day in this study.
A high prevalence of obesity was observed in preschool children with prolonged screen time and lower physical activity.11 Some studies reported that age, sex, family background, diet, physical activity, sleep duration and lifestyle habits of preschool children were factors associated with prolonged screen time and the risk of obesity.11,15,37–46 These factors were considered potential confounding factors of obesity and should be controlled for when investigating the association between screen time and obesity, as in the present study. Our results reveal that preschool children who spent more time on screens had an increased obesity risk, which is the same outcome as previous research.6,11,12,38
Age was associated with screen time in preschool children,38 particularly older preschool children who spent a lot of time watching television.38,39 This phenomenon was also found in our study. Moreover, our study showed that the time spent viewing television and digital media were both important predictive factors of childhood obesity, and television time had a more significant association with childhood obesity than digital media time did. Our findings were similar to the results of the National Health and Nutrition Examination Survey (1999–2014), which showed that children aged 2–5 years had a significantly increased risk of obesity if their television time or screen time was over 2 hours/day; especially when television time and screen time exceeded 3 hours/day, children had an increased risk of severe obesity,6 and other studies revealed that television time was more positively associated with adiposity than other forms of screen-based media.12,14
Many studies demonstrated that eating a meal while watching television was positively associated with being overweight.47 Moreover, junk food, such as snacks, fried foods, sweets, and beverages, were often consumed when children watched television;45 therefore, when children used the tablet or smartphone, their fingers were usually less involved in consuming food. In general, a television is often set in a place, eg, a living room or bedroom, and is not easy to move. However, like a smartphone, digital media is usually mobile, which means that the user could have more physical activity and energy consumption.
In the past two decades, our society and research have focused on television, considering how to influence childhood obesity and setting the recommendation that an excessive amount of television hours should be limited. However, recently, numerous screen-based media, eg, smartphones, tablets, and computers, have become common and frequently used devices in our daily home environment. This means that young children have enhanced opportunities to see, touch or use them, so currently, children not only watch television but also interact with various digital media. Although digital media time has a lower predictive power than television time, it is a screen-based medium and still has a negative influence on childhood obesity.
Shorter sleep is also a problem in children with high screen time.15,40,41 Our results revealed that preschool children with high screen time had fewer sleep hours than those with low screen time. It has been suggested that excessive use of television and computers may result in shorter sleep hours and overweight.42 Delayed bedtime and sleep deprivation are risk factors for poor sleep quality in preschool children.40 Deprivation of sleep hours was identified to be associated with a lack of physical activity, weight gain, insulin resistance, and unhealthy dietary patterns.42 High screen time and shorter sleep hours were independent factors contributing to childhood overweight and obesity.11,43 In our results, higher screen time was related to lower sleep hours; thus, limiting preschool children’s screen time might be another way to enhance their sleep health.
It has been reported that high screen time is significantly associated with low physical activity and more sedentary behaviors in children.44 Too much sedentary behavior and screen time increased the risk of obesity.9,11,44 Greater physical activity time was positively associated with decreasing obesity11 because adding outdoor activity time could decrease the sedentary behaviors of preschool children.9,11 Our study showed a lower time of outdoor activity of preschool children who had a higher ratio of screen time. This result might reveal the increased risks faced by preschool children in Taiwan, so reducing screen time and adding active physical activity time for them is required.
A review study suggested that children who spent more time using screen-based media would have more behaviors with food intake or snack consumption.45 Undoubtedly, snack consumption was an important risk factor for childhood obesity.37,45 Overeating snacks in preschool children was associated with high screen time, which was also observed in our findings. To improve preschool children’s health, we suggest that caregivers pay attention to children’s snack consumption during screen time.
Additionally, the family environment and socioeconomic status of caregivers were factors associated with screen time in preschool children.4,25,48 In the current results, we have similar findings that caregivers’ sex, age, education, and physical activity (eg, screen time and exercise time) were associated with preschool children’s screen time. Parenting style and the family environment were important mediators for enhancing the lifestyle and health status of preschool children, such as limiting their screen time or other behaviors and arranging their daily routine schedule.25 Maternal caregivers with lower education or younger age were more likely to allow longer screen time for their preschool children.48 As a result, to effectively reduce the screen time of preschool children, we should consider how to educate caregivers about behaviors in the home environment and how to teach a healthy lifestyle to their children. Another interesting result of this study was that caregivers’ obesity (85% of caregivers were mothers) was also an important factor associated with preschool children’s high screen time. Many studies have shown that parenting is one of the crucial influential factors in child health and obesity.4,10,11,49 Obesity in adults is a multifactorial issue that is frequently caused by lifestyle. In particular, inadequate physical activity increased the risk for adult obesity, and an association was shown between physical inactivity from youth.50 Thus, it can be seen that parenting has a powerful influence on young children’s health and development. A parent’s obesity and unhealthy behaviors might influence a young child in daily routines. To efficiently reduce preschool children’s screen time in Taiwan, caregivers or parents need to stringently limit their television time.
In the subgroup analysis of this study, high screen time was not significantly associated with obesity risk in some subgroups. This phenomenon revealed that the association between screen time and obesity was mediated by sociodemographic and lifestyle factors. More comprehensively designed studies are needed to prove this relationship.
Interpretations of the current findings should be made with caution because some limitations existed in this study. First, recall bias may occur in surveys, and all data were based on main caregivers’ reports by observation. Second, the unavailable information on body mass index and detailed lifestyle habits of the main caregivers may confound the findings of this study. Third, inadequate physical activity was associated with sedentary behavior and obesity, but we have no corresponding data in preschool children. Fourth, caregiver sex as an important limitation of this study because fathers are very underrepresented (less than 7%). In addition, some confounding factors potentially affected our study, although we adjusted for all available information. Finally, our study was a cross-sectional survey that could not demonstrate a causal relationship between screen time and obesity. We could not exclude the possibility of the potential reverse causation that obesity may be a risk factor for prolonged screen time among preschool children.
Conclusion
We observed a high prevalence of obesity and prolonged screen time among preschool children in Taiwan. Preschool children with prolonged screen time may have increased risk of obesity, and this association was mediated by sociodemographic and lifestyle factors. Our observations are of considerable public health interest, and future high-quality studies, such as randomized controlled trials, are needed to demonstrate causality.
Abbreviations
SD, standard deviation; CI, confidence interval; PR, prevalence ratio.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported in part by the Ministry of Science and Technology, Taiwan (MOST111-2320-B-532 -001-MY3; MOST110-2314-B-038-108-MY2; MOST108-2320-B-038-070-MY3).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yilmaz G, Caylan ND, Karacan CD. An intervention to preschool children for reducing screen time: a randomized controlled trial. Child Care Health Dev. 2014;41(3):443–449. doi:10.1111/cch.12133
2. Hancox RJ, Milne BJ, Poulton R. Association of television viewing during childhood with poor educational achievement. Arch Pediatr Adolesc Med. 2005;159(7):614–618. doi:10.1001/archpedi.159.7.614
3. American Academy of Pediatrics, Council on Communications and Media. Media and young minds. Pediatrics. 2016;138(5):e20162591. doi:10.1542/peds.2016-2591
4. De Decker E, De Craemer M, De Bourdeaudhuij I, et al. Influencing factors of screen time in preschool children: an exploration of parents’ perceptions through focus groups in six European countries. Obes Rev. 2012;13(Suppl. 1):75–84. doi:10.1111/j.1467-789X.2011.00961.x
5. Robinson TN, Wilde ML, Navracruz LC, et al. Effects of reducing children’s television and video game use on aggressive behavior: a randomized controlled trial. Arch Pediatr Adolesc Med. 2001;155(1):17–23. doi:10.1001/archpedi.155.1.17
6. Tester JM, Phan TLT, Tucker JM, et al. Characteristics of children 2 to 5 years of age with severe obesity. Pediatrics. 2018;141(3):e20173228. doi:10.1542/peds.2017-3228
7. Djalalinia S, Qorbani M, Rezaei N, et al. Joint association of screen time and physical activity on self-rated health and life satisfaction in children and adolescents: the CASPIAN-IV study. Int Health. 2017;9:58–68. doi:10.1093/inthealth/ihw044
8. Duch H, Fisher EM, Ensari I, et al. Association of screen time use and language development in Hispanic toddlers: a cross-sectional and longitudinal study. Clin Pediatr. 2013;52(9):857–865. doi:10.1177/0009922813492881
9. Downing K, Hinkley T, Salmon J, et al. Do the correlates of screen time and sedentary time differ in preschool children? BMC Public Health. 2017;17(1):285. doi:10.1186/s12889-017-4195-x
10. Anderson SE, Whitaker RC. Household routines and obesity in us preschool-aged children. Pediatrics. 2010;125(3):420–428. doi:10.1542/peds.2009-0417
11. Watanabe E, Lee JS, Mori K, et al. Clustering patterns of obesity-related multiple lifestyle behaviours and their associations with overweight and family environments: a cross-sectional study in Japanese preschool children. BMJ Open. 2016;6(11):e012773. doi:10.1136/bmjopen-2016-012773
12. Stamatakis E, Coombs N, Jago R, et al. Associations between indicators of screen time and adiposity indices in Portuguese children. Prev Med. 2013;56(5):299–303. doi:10.1016/j.ypmed.2013.02.006
13. Sorrie MB, Yesuf ME, GebreMichael TG, Jadhao SB. Overweight/obesity and association factors among preschool children in Gondar city, Northwest Ethiopia: a cross-sectional study. PLoS One. 2017;12(8):e0182511. doi:10.1371/journal.pone.0182511
14. Carson V, Tremblay MS, Spence JC, et al. The Canadian sedentary behaviour guidelines for the early years (zero to four years of age) and screen time among children from Kingston, Ontario. Paediatr Child Health. 2013;18(1):25–28. doi:10.1093/pch/18.1.25
15. Khalsaa AS, Kharofaa R, Ollberdingb NJ, et al. Attainment of ‘5-2-1-0’ obesity recommendations in preschool-aged children. Prev Med Rep. 2017;8:79–87. doi:10.1016/j.pmedr.2017.08.003
16. American Academy of Pediatrics Committee on Public Education. American Academy of Pediatrics: children, adolescents, and television. Pediatrics. 2001;107(2):423–426. doi:10.1542/peds.107.2.423
17. Berglind D, Tynelius P. Objectively measured physical activity patterns, sedentary time and parent-reported screen-time across the day in four-year-old Swedish children. BMC Public Health. 2018;18(1):69. doi:10.1186/s12889-017-4600-5
18. Määttä S, Kaukonen R, Vepsäläinen H, et al. The mediating role of the home environment in relation to parental educational level and preschool children’s screen time: a cross-sectional study. BMC Public Health. 2017;17(1):688. doi:10.1186/s12889-017-4694-9
19. Kim H, Ma J, Harada K, Lee S, Gu Y. Associations between adherence to combinations of 24-h movement guidelines and overweight and obesity in Japanese preschool children. Int J Environ Res Public Health. 2020;17(24):9320. doi:10.3390/ijerph17249320
20. Hossain MS, Deeba IM, Hasan M, et al. International study of 24-h movement behaviors of early years (SUNRISE): a pilot study from Bangladesh. Pilot Feasibility Stud. 2021;7:176. doi:10.1186/s40814-021-00912-1
21. Ng JYY, He Q, Chong KH, Okely AD, Chan CHS, Ha AS. The impact of COVID-19 on preschool-aged children’s movement behaviors in Hong Kong: a longitudinal analysis of accelerometer-measured data. Int J Environ Res Public Health. 2021;18:11907. doi:10.3390/ijerph182211907
22. Ponti M, Bélanger S, Grimes R; Canadian Paediatric Society, Digital Health Task Force, Ottawa, Ontario. Screen time and young children: promoting health and development in a digital world. Paediatr Child Health. 2017;22:461–477. doi:10.1093/pch/pxx123
23. Bergmann C, Dimitrova N, Alaslani K, et al. Young children’s screen time during the first COVID‑19 lockdown in 12 countries. Sci Rep. 2022;12:2015. doi:10.1038/s41598-022-05840-5
24. Birken CS, Maguire J, Mekky M, et al. Office-based randomized controlled trial to reduce screen time in preschool children. Pediatrics. 2012;130(6):1110–1115. doi:10.1542/peds.2011-3088
25. Veldhuis L, van Grieken A, Renders CM, et al. Parenting style, the home environment, and screen time of 5-year-old children; the ‘be active, eat right’ study. PLoS One. 2014;9(2):e88486. doi:10.1371/journal.pone.0088486
26. Jones BL, Fiese BH. Parent routines, child routines, and family demographics associated with obesity in parents and preschool-aged children. Front Psychol. 2014;5:374. doi:10.3389/fpsyg.2014.00374
27. Androutsos O, Moschonis G, Ierodiakonou D, et al. Perinatal and lifestyle factors mediate the association between maternal education and preschool children’s weight status: the ToyBox study. Nutrition. 2018;48:6–12. doi:10.1016/j.nut.2017.11.006
28. Chaput JP, Colley RC, Aubert S, et al. Proportion of preschool-aged children meeting the Canadian 24-hour movement guidelines and associations with adiposity: results from the Canadian health measures survey. BMC Public Health. 2017;17(Suppl 5):829. doi:10.1186/s12889-017-4854-y
29. Chang FC, Chen CH, Haung YK, et al. The influence of time of television viewing on obesity and associated factors among preschool children in Taiwan: a cross-sectional study. Taiwan J Public Health. 2017;36:54–63.
30. Tremblay MS, Chaput JP, Adamo KB, et al. Canadian 24-hour movement guidelines for the early years (0–4 years): an integration of physical activity, sedentary behaviour, and sleep. BMC Public Health. 2017;17(Suppl 5):87. doi:10.1186/s12889-017-4859-6
31. Tremblay MS, Carson V, Chaput JP, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2016;41(6 Suppl 3):S311–S327. doi:10.1139/apnm-2016-0151
32. World Health Organization. Guidelines on physical activity, sedentary behaviour and sleep for children under 5 years of age; 2019. Available from: https://www.who.int/publications/i/item/9789241550536.
33. Chen W, Chang MH. New growth charts for Taiwanese children and adolescents based on World Health Organization standards and health-related physical fitness. Pediatr Neonatol. 2010;51:69–79. doi:10.1016/S1875-9572(10)60014-9
34. Hirshkowitz M, Whiton K, Albert SM, et al. National sleep foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1(1):40–43. doi:10.1016/j.sleh.2014.12.010
35. Hwang LC, Bai CH, Chen CJ. Prevalence of obesity and metabolic syndrome in Taiwan. J Formos Med Assoc. 2006;105:626–635. doi:10.1016/S0929-6646(09)60161-3
36. Health Promotion Administration, Ministry of Health and Welfare. Evidences-Based Guideline on Adult Obesity Prevention and Management. Taiwan, Taipei: Health Promotion Administration, Ministry of Health and Welfare; 2018.
37. Do LM, Tran TK, Eriksson B, Petzold M, Nguyen CTK, Ascher H. Preschool overweight and obesity in urban and rural Vietnam: differences in prevalence and associated factors. Glob Health Action. 2015;8:28615. doi:10.3402/gha.v8.28615
38. Jago R, Baranowski T, Baranowski JC, Thompson D, Greaves KA. BMI from 3–6y of age is predicted by TV viewing and physical activity, not diet. Int J Obes. 2005;29:557–564. doi:10.1038/sj.ijo.0802969
39. Lin LY, Cherng RJ, Chen YJ, Chen YJ. Effects of television exposure on developmental skills among young children. Infant Behav Dev. 2015;38:20–26. doi:10.1016/j.infbeh.2014.12.005
40. Cespedes EM, Gillman MW, Kleinman K, Rifas-Shiman SL, Redline S, Taveras EM. Television viewing, bedroom television, and sleep duration from infancy to mid-childhood. Pediatrics. 2014;133:e1163–e1171. doi:10.1542/peds.2013-3998
41. Xu H, Wen LM, Hardy LL, Rissel C. Associations of outdoor play and screen time with nocturnal sleep duration and pattern among young children. Acta Paediatr. 2016;105(3):297–303. doi:10.1111/apa.13285
42. Garmy P, Clausson EK, Nyberg P, Jakobsson U. Insufficient sleep is associated with obesity and excessive screen time amongst ten-year-old children in Sweden. J Pediatr Nurs. 2018;39:e1–e5. doi:10.1016/j.pedn.2017.11.009
43. Shang L, Wang J, O’Loughlin J, et al. Screen time is association with dietary intake in overweight Canadian children. Prev Med Rep. 2015;2:265–269. doi:10.1016/j.pmedr.2015.04.003
44. Tanaka C, Tanaka M, Okuda M, Inoue S, Aoyama T, Tanaka S. Association between objectively evaluated physical activity and sedentary behavior and screen time in primary school children. BMC Res Notes. 2017;10(1):175. doi:10.1186/s13104-017-2495-y
45. Avery A, Anderson C, McCullough F. Associations between children’s diet quality and watching television during meal or snack consumption: a systematic review. Matern Child Nutr. 2017;13(4):e12428. doi:10.1111/mcn.12428
46. Skinner AC, Skelton JA. Prevalence and trends in obesity and severe obesity among children in the United States, 1999–2012. JAMA Pediatr. 2014;168(6):561–566. doi:10.1001/jamapediatrics.2014.21
47. Ghobadi S, Hassanzadeh-Rostami Z, Salehi-Marzijarani M, et al. Association of eating while television viewing and overweight/obesity among children and adolescents: a systematic review and meta-analysis of observational studies. Obes Rev. 2018;19(3):313–320. doi:10.1111/obr.12637
48. Lloyd AB, Lubans DR, Plotnikoff RC, et al. Maternal and paternal parenting practices and their influence on children’s adiposity, screen-time, diet and physical activity. Appetite. 2014;79:149–157. doi:10.1016/j.appet.2014.04.010
49. Matłosz P, Wyszyńska J, Asif M, et al. Prevalence of overweight, obesity, abdominal obesity, and obesity-related risk factors in Polish preschool children: a cross-sectional study. J Clin Med. 2021;10(4):790. doi:10.3390/jcm10040790
50. Kallio P, Pahkala K, Heinonen OJ, et al. Physical inactivity from youth to adulthood and adult cardiometabolic risk profile. Prev Med. 2021;145:10643. doi:10.1016/j.ypmed.2021.106433
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.