")
Back to Journals » Clinical Ophthalmology » Volume 17
Risk of Neurotoxicity with Multiple General Anaesthetics for Examination Under Anaesthesia in Paediatric Ophthalmology – A Cause for Concern?
Authors O'Connell A, Stephenson KAJ, Flitcroft I
Received 4 October 2022
Accepted for publication 20 December 2022
Published 20 January 2023 Volume 2023:17 Pages 291—302
DOI https://doi.org/10.2147/OPTH.S387098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ann O’Connell, Kirk AJ Stephenson, Ian Flitcroft
Ophthalmology Department, Children’s Health Ireland at Temple Street Hospital, Dublin, Ireland
Correspondence: Ann O’Connell, Children’s Health Ireland at Temple Street, Dublin, Ireland, Tel +353 1 8784200, Email [email protected]
Purpose: To evaluate the impact of clinical protocol change via active minimisation on the number of general anaesthetic (GA)/sedation episodes for diagnostic ophthalmic purposes at Children’s Health Ireland at Temple Street (CHI-TS), Dublin, Ireland, from 2016 to 2019, inclusive. Change was implemented following published cautionary principles in 2016 by the FDA regarding the potential neurotoxic risk from multiple GA exposure in children.
Methods: Retrospective analysis of electronic operating theatre records was completed using procedure codes “Ophthalmological examination” and “Examination of fundi”. Available records for patients undergoing multiple examination under anaesthesia (EUA) procedures were assessed for demographics, indication. Comparison was made regarding overall EUA numbers and breakdown for each year, before and after the new departmental approach. From 2018 onward, a patient-centred, departmental strategy of active minimisation of EUA was adopted, using strategies of “training, technology and patience”. A literature review was conducted using online databases.
Results: A total of 450 EUAs were performed over the 4 years investigated. In the former 2 years of the study period, prior to departmental policy change, EUAs represented 32% (304 of 948 total theatre episodes) of the ophthalmic theatre caseload. In the latter 2 years of this study period, this proportion fell to 19% (146 EUAs of 783 theatre episodes). Total theatre case numbers were comparable in both time periods. Eighteen children had multiple EUAs (ie, ≥ 2 EUAs, mean 6.5, SD 2.9) for life/sight threatening indications, totalling 116 EUAs (25.7%).
Conclusion: A significant reduction in diagnostic EUA volume was accomplished resulting in reduced individual patient risk and increased capacity for surgical interventions. A detailed description of this methodology is included for the purposes of replication at comparable units. EUA will continue to play a crucial role in the management of life/sight threatening conditions but the application of a cautionary principle to reduce EUA, where possible, is appropriate to reduce potential for neurotoxicity.
Keywords: paediatric ophthalmology, general anaesthesia, developmental neurotoxicity, ophthalmology, examination under anaesthesia, paediatric anaesthesiology
Introduction
In recent years, there has been growing discussion concerning the potential risk of neurotoxicity in paediatric patients exposed to multiple general anaesthetics (GA). In 2016, the US Food and Drug Administration (FDA) issued an advisory notice on this topic.1 Following this, the Association of Paediatric Anaesthetists of Great Britain and Ireland (APAGBI) produced a guidance document in 2017 regarding a potential association between multiple or prolonged GA and neurotoxicity.2 Their recommendations were to limit exposure (volume and duration) to GA for this population, though specialty-specific guidelines are not universally available. The use of GA in paediatric ophthalmology can be divided into diagnostic examination under anaesthesia (EUA), and therapeutic. A coordinated focus on the considered and judicious use of EUA, which forms a significant proportion of GA volume in the specialty, would reduce overall GA burden.
The safety of single and short (ie, <1 hour) exposure to GA in children, including the under 3 years age group, is supported by the available evidence regarding long-term neurocognitive outcomes.3–5 Ophthalmic procedures in children are usually of limited duration and require a single GA. However, some studies suggest a heightened risk of neurodevelopmental injury with multiple exposures to GA.6
In certain life/sight threatening chronic conditions, multiple EUAs may be unavoidable where detailed conscious examination is often precluded in the paediatric age group.7–10 Examples include cohorts at high risk for familial retinoblastoma (RB), where EUAs to facilitate “intensive” fundus screening may be needed as frequently as every 4 weeks.10 In congenital glaucoma or Coats’ disease, EUA (±treatment) is often required on a two to three monthly basis until the disease is controlled, with continued surveillance potentially required throughout childhood.11–13
In the context of intellectual disability (ID), autism spectrum disorders (ASD), or concurrent illness, necessary elements of assessment like cycloplegic refraction, fundal examination or electrophysiology can be very difficult in the awake patient, necessitating sedation or GA.7,14–16 Ophthalmic manifestations may be an identifying feature of paediatric multisystem disease17–19 with these children often requiring repeated comprehensive assessments.
Is there an identifiable subset of potentially avoidable EUAs, in spite of the challenging clinical context of many paediatric ophthalmic assessments? The establishment of general guidelines regarding indications for, goals of, and recommended intervals for EUA in paediatric ophthalmology would be instrumental in raising awareness amongst physicians of potential neurotoxicity, potentially reducing the GA burden on this vulnerable patient group. Freedom to deviate from such guidelines is essential as life- and sight-threatening conditions do not always obey protocols.
Potential strategies identified at our unit to reduce EUA burden utilise the principles of “technology, training, and patience.” Embracing novel equipment such as the iCare tonometer (Centrevue SPA, Finland) and wide field Optos retinal photography (Optos plc, UK) contribute useful information within the window of cooperation of a small child.20,21 Clinician training in techniques such as Mohindra retinoscopy (ie, non-cycloplegic refraction in a darker environment) may be less overwhelming and more tolerable in certain situations (eg, ASD) thus obviating GA. Education on practice guideline updates was continuous, with a particular emphasis on those that may reduce EUA/GA burden. A trial of awake visual electrodiagnostic testing (EDT) in an abridged paediatric protocol may be appropriate in the first instance. A multi-visit approach, underpinned by patience, persistence, and child-centredness, may allow adequate data gathering without the risks to the patient or the influence of GA on data quality/interpretation.22,23
Using these principles and cognisant of the potential neurodevelopmental toxicity risk of repeated GA, our unit adopted a policy of active minimisation of EUA volume for ophthalmic purposes commencing in 2018. This paper presents an audit of the effect of this clinical policy change, demonstrating significant reductions in overall and individual volume of EUAs. A detailed discussion of the clinical methodology used and a literature review of neurotoxicity risk due to paediatric GA is presented. Herein, we discuss the fundamental concept that GA may not always be required to clinically evaluate the uncooperative child and should be used judiciously to safeguard normal neurodevelopment.
Methods
Retrospective analysis of anonymised operating theatre records at CHI-TS was completed from 2016 to 2019 inclusive. Both the total number of GA/sedation episodes and the proportion carried out for diagnostic ophthalmic purposes under Hospital In-Patient Enquiry system codes “Ophthalmological examination” and “Examination of fundi” were identified. This data set was generated using electronic record programmes Ormis (Dedalus, Italy), the Integrated Patient Management System and with the collaboration of the Information Communications Technology department of CHI-TS.
Available records were assessed for patient demographics, type of GA (ie, EUA vs procedure) and indication. A comparison was made between each year regarding overall GA use and breakdown. This audit was approved by the CHI-TS institutional clinical audit review group (CA2012-05) and adhered to the tenets of the Declaration of Helsinki. Individual patient written consent was not required due to the anonymised nature of the dataset collected. All data was collected and stored in compliance with national General data protection legislation (GDPR).
Active minimisation involved a patient-centred “training, technology and patience” strategy, employed in the outpatient setting. Suitable cases of children with non-emergent, non-life-threatening and non-immediately sight threatening disease were identified at the point of care who may otherwise have proceeded to EUA in the first instance for completion of their ophthalmic assessment. Specific methods under the heading of “training” employed to actively minimise EUAs where possible were 1. Upskilling staff in the use of the Mohindra retinoscopy technique. It was trialled for the assessment of patients with intellectual disability/ASD requiring accurate refraction, 2. Departmental guidelines were updated to reflect the most up-to-date information from the literature (eg, deferral of nasolacrimal duct (NLD) probing/intubation until at least after 1 year of age). 3. Staff training in the utility of newly available investigations (eg, pedigree testing in RB to inform sibling surveillance intervals). Under the heading of “technology”, active minimisation strategies involved the introduction of novel equipment to our department, namely, iCare rebound tonometry, optical coherence tomography (OCT) and Optos wide field colour photography for rapid image acquisition. “Patience” was employed by 1. Gathering information over a multi-visit approach, and 2. Awake EDT was attempted in the first instance, conducted by an experienced senior electrophysiologist. 3. In advance of appointments and when available, children were invited to utilise the new departmental “sensory room”, in order to maximise patient acclimatisation to the clinical environment, promoting comfort and calm. In-depth discussion of the practicalities of implementation of the above methods and the literature providing rationale for their use is found below in the “Discussion” section.
Available literature on GA-associated neurotoxicity in paediatric populations was examined. Literature review was conducted using PubMed, MEDLINE and Cochrane databases and Google Scholar. Combinations of Medical subject headings (MeSH), their synonyms and international spelling equivalents were used (Table 1). Key core search terms were “ophthalmology”, “paediatrics”, “anaesthesia”, “neurotoxicity” and “risk”. Further refined searches were carried out, substituting “ophthalmology” with “dentistry”, “radiology”, “ENT” and their respective alternative international equivalent terms and synonyms. Comparably to ophthalmology, these subspecialties typically carry out EUAs in the paediatric population of our institution.
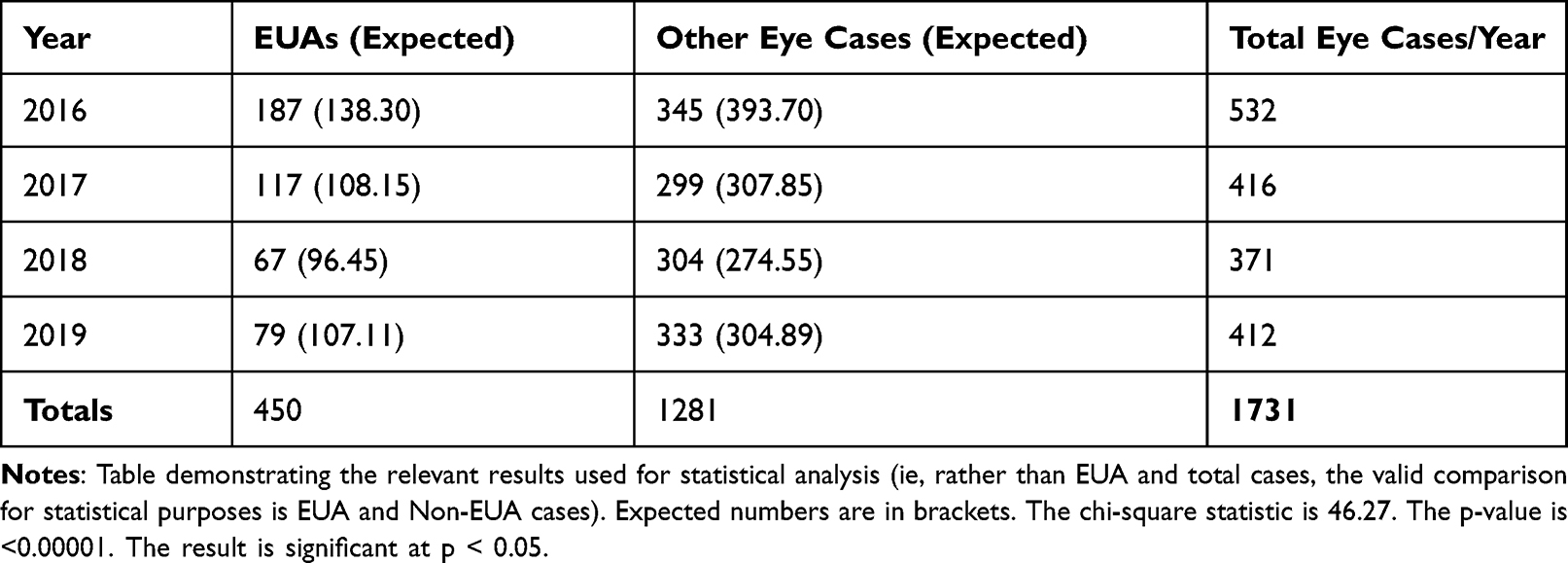 |
Table 1 Results Used for Statistical Analysis |
Results
EUAs constituted 35.2% of ophthalmic theatre episodes (187/532 GAs) in 2016 and 28.1% (117/416 GAs) in 2017. This reduced to 18.1% (67/371 GAs) in 2018 and 19.1% (79/412 GAs) in 2019.
Overall, in the former half of the study period, 2016 to 2017 inclusive, prior to departmental policy change regarding timing/use of EUAs, 304 EUAs represented 32% of the total 948 episodes in the ophthalmic theatre.
In the latter 2 years of this study period (2018 and 2019), EUAs fell to 19% (146 EUAs of 783 theatre episodes). It is noted that total theatre case numbers were comparable in both time periods (Figure 1).
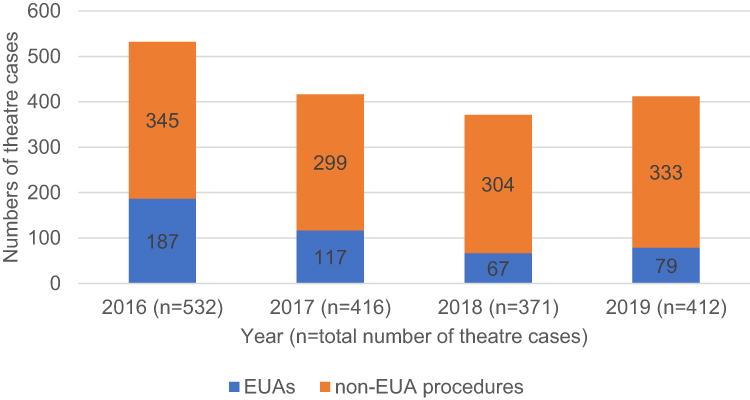 |
Figure 1 Proportion of examination under anaesthesia (EUA) procedures (blue) and non-EUA procedures (Orange) as proportions of total number of paediatric ophthalmology theatre procedures from 2016–2019. Note the decreasing proportion of EUAs across the study period representing active policy change in EUA booking. Abbreviation: EUA, examination under anaesthetic. |
A total of 450 EUAs were performed across the 4-year study period, 68% (304/450) of which were performed in the first half of the study. Of these, 116 EUAs (25.7% of all GAs over 4 years) were accounted for by the 18 children who had ≥2 EUAs (mean 6.5 EUAs, SD 2.9). Regarding individual case breakdown, eight of these children had RB (44%), five had glaucoma including Peters anomaly (28%), four had Coats’ Disease (22%) and one was unknown due to unattainable hard copy clinical records (6%) (Figure 2).
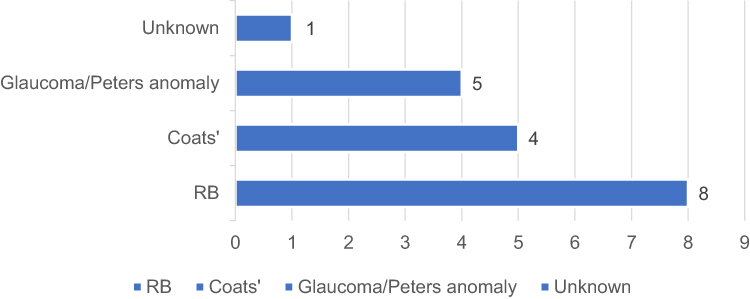 |
Figure 2 Case breakdown of those that underwent multiple (≥2) EUAs, n = 18, during the study period, 2016–2019. Abbreviations: RB, Retinoblastoma; Coats’, Coats’ disease. |
Four children had 8 or more diagnostic procedures (mean 10 procedures, SD 1.6), all of these occurring in the first 2 years of the study period. Two of these were RB cases (50%), one glaucoma (25%) and the other unknown (25%) (Figure 3).
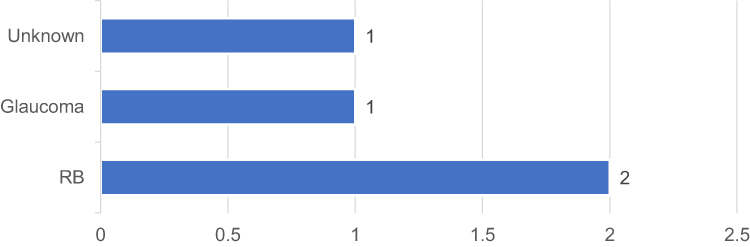 |
Figure 3 Case breakdown of those that underwent 8 or more EUAs (n = 4). Abbreviation: RB, Retinoblastoma. |
The statistical significance of the change in numbers of EUAs over the four-year period was examined using the Chi-square test with the null hypothesis that there was no difference in the number of EUAs vs non-EUA cases over the four-year period (Table 1). This analysis showed that the change in EUA numbers over the four-year period was statistically significant (Chi-squared = 46.27, n = 1731, df = 3, p-value <0.00001).
Literature review search for GA-associated neurotoxicity in paediatric populations yielded a total of 3196 search results. Search terms and combinations are outlined in Table 2. Only published peer-reviewed data were included. Abstracts and non-English language articles were excluded.
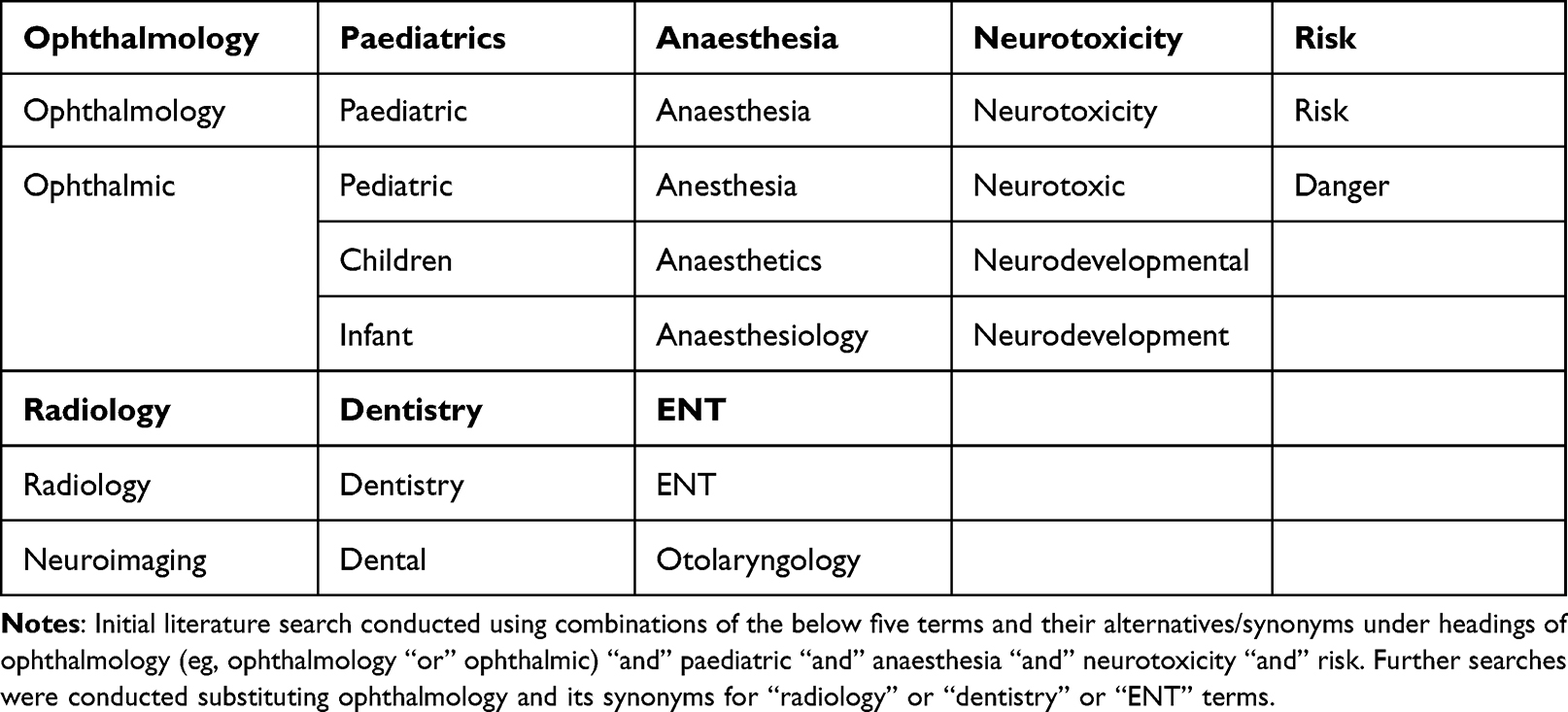 |
Table 2 Literature Search Terms |
On refined search, there were no systematic reviews, meta-analyses, review articles or randomised controlled trials specific to the subspecialties of ophthalmology, radiology, dentistry or ENT identified. On further search, three articles were relevant to the clinical question posed; one randomized controlled trial, and two review articles.3,4,24 Individual trials of relevance and interest were identified from manual analysis of reference lists of the above literature searches.
Discussion
A significant reduction in diagnostic EUA volume was accomplished by the CHI-TS ophthalmology department between 2016 and 2019. The proportion represented by EUAs of total theatre cases decreased from 35.2% and 28.1% in the first two years to 18.1% and 19.1% in the latter two years. There is an increase in total cases between 2018 and 2019 (ie, 371 to 412). Thus, assuming the same proportion of EUAs in both years it would be expected that there would be a small increase in number of EUAs also (Table 1).
This reduction in total number of EUAs and their proportion of total ophthalmic surgical throughput was achieved utilising the minimally invasive and innovative “technology, training and patience” strategies which resulted in a reduced burden of exposure to GA in our patient group. This did not represent reduced productivity, but rather redistribution of resources (ie, maximizing examination options in clinic) and reserving finite operating theatre resources for therapeutic interventions. As total theatre episodes were comparable in both time periods, this represents a greater proportion of interventions per annum. Thus, reduction of EUA volume not only reduces the potential neurotoxic burden, enhancing quality of care for the individual child but could also increase capacity for surgical interventions; we see non-EUA procedures make up a larger proportion of total theatre cases in the latter half of this study. Though not formally evaluated here, we postulate this could indirectly contribute to reduced waiting lists for the whole ophthalmic paediatric population and additionally carry an associated healthcare cost benefit associated with reduction in EUA/GA episodes.25
EUAs and therapeutic surgical interventions are not undertaken for trivial reasons and clinicians generally aim to reduce their number, postpone, or avoid GAs altogether whenever possible. There is growing international interest in the identification of safe and effective alternatives to GA for EUA.26 The initiatives employed in this study may be of relevance and benefit to other comparable paediatric ophthalmology units, similarly endeavoring to reduce the burden of avoidable EUAs in the evaluation of the paediatric patient. To this end, a detailed description is provided herein.
Firstly, this involved embracing the advent of new technologies to provide less invasive evaluation options, where available. iCare rebound tonometry was incorporated at the initial Nurse-led assessment for all clinic patients, following staff education in its use (also demonstrating the second “training” element). Measurement takes place following a brief clinical history, gross ophthalmic inspection, visual acuity measurement and crucially before potentially uncomfortable dilating drops are instilled that risk loss of the child’s cooperation. Valuable IOP measurement is gathered painlessly, at this point of potential maximal cooperation, and before children become unduly fatigued awaiting physician assessment.
Experienced ophthalmic nurses used this opportunity to identify those with previous recorded difficulty with cycloplegic drop instillation or awake refraction. This can be especially relevant in children with ID, chromosomal abnormalities (eg, Children with Trisomy 21, in whom atropine may be contraindicated, though evidence is conflicting27,28) or ASD who have concurrent refractive error. If suitable and with parental input, a trial of Mohindra refraction in the clinic setting can be offered.29,30 In this instance, physician training was required in the use of this technique, which utilises a darkened room with only the retinoscope light to focus on. It is performed at a working distance of 50cm and conventionally involves a corrective subtraction of +1.25D from the final objective spherical result. Advantages include a calm, darkened, less overwhelming environment for children susceptible to overstimulation and distraction. Additionally, it dispenses with the need for cycloplegic pharmacological agents, with their potential for associated ocular discomfort on instillation and other undesired affects.31,32 Anecdotally, this technique, originally described in 1975 by Mohindra,33 has proven useful to obviate the need for refraction under GA/EUA for a number of cases. Engaging the “training and patience” strategies, parents were upskilled in instillation and effects of cycloplegic drops for select cases. When administered as “home dilation” time could elapse for any associated distress to have resolved by the time of examination, while the effects of the drops persist.
Departmental training included dissemination of updated guidelines. These include avoidance of NLD intubation until after 1 year of age in congenital NLD obstruction, which has a high rate of spontaneous resolution by this time.34 Genetic pedigree analysis of siblings with RB informs and potentially lengthens their fundal examination screening intervals, if required at all.35
Technological advances in ophthalmic imaging systems such as the RetCam (Clarity Medical Systems, India) and ultra-widefield retinal imaging [Optos and Zeiss Clarus 500 (Carl Zeiss Meditec AG, Germany)]20,21,36,37 have led to faster acquisition times, in the setting of the potentially narrow window of a child’s cooperation. Exciting advances suggest that integration of artificial intelligence software into RetCam could be utilised in the diagnosis/classification of ROP on site or remotely,38 potentially further reducing EUA burden.
EUA is used as standard for EDT in other international settings,39 or under sedation with quoted rates of 70% requiring pharmacological measures.40 As part of the “patience” strategy, EDT was initially trialled awake, overseen by the senior departmental electrophysiologist. Prior to testing (and indeed before all clinical assessment or investigations, eg, Optos photography/OCT imaging) children were invited to spend time in the departmental sensory room, when time allowed. This is a dedicated, relaxed space incorporating fibre-optics, bubble tubes, tactile objects and soft seating to allow immersion in a comfortable environment. We observed a calming effect for our patients, promoting increased cooperation, mirroring published data.41,42 In the setting of minimal cooperation, prioritising of tests as per clinical indication guided their running order and acquisition speed. Children were allowed time to acclimatise to the dark environment and bottle feeding/cartoon watching on mobile devices were utilised as distraction techniques for electrode placement. All tests were performed according to International society of clinical electrophysiology and vision (ISCEV) guidelines.43 Benefits were observed particularly in children with ID/ASD/sensory processing issues or behavioural challenges. We feel this has contributed to the overall success in obtaining clinically relevant data without the need for EUA, but it is acknowledged that this is a difficult metric to formally measure and further study/audit is required. A conscious drive to reduce EUA/GA burden by promoting alternatives such as chloral hydrate sedation for EDT, among other ophthalmic procedures, is described in literature.26,44 However, this is not a strategy available at our unit to date.
In ophthalmic conditions that were neither life- nor sight-threatening, a new approach by departmental staff was taken to attempt clinical data gathering over several visits, if necessary, rather than defaulting automatically to EUA/GA. This multi-visit approach, underpinned by patience, persistence, and child-centredness, often allowed adequate data gathering without the risks to the patient or the influence of GA on the data quality/interpretation.
Those that underwent multiple EUAs were accounted for in the case breakdown by the life and sight threatening conditions discussed earlier. This underpins the crucial role EUAs will likely always play in this cohort of conditions in paediatric ophthalmology. Of note, some, if not all, of the RB and glaucoma cases who underwent 8 or more EUAs may have had a therapeutic intervention during these encounters. Pre-procedure parental discussion/consent is essential to provide the option to examine and treat concurrently, preventing the need to return for a further, delayed GA. This also confers benefit in affording earlier intervention and better outcomes in time-sensitive or progressive conditions. Many cases of RB requiring radio- or chemotherapy are referred from CHI-TS to a subspecialising UK centre. Thus, the true volume for this vulnerable patient group is not completely captured here. Specialists caring for such malignant or imminently sight-threatening pathology will necessarily carry the disproportionate burden of EUA/GAs and this should be borne in mind when evaluating any similar audit results at comparable centres.
What is Known Regarding Neurocognitive Risk of Individual Anaesthetic Agents or Delivery Methods?
No individual anaesthetic agent, delivery method, or combination of agents to date has conclusively demonstrated neuroprotective or more potent neurotoxic effects over another in the context of multiple GA exposures.2,45,46 “Balanced anaesthesia” is achieved through small and safe doses from 3 categories of drugs (ie, analgesic, anaesthetic and muscle relaxation drugs) during the three key phases of induction, maintenance, and emergence. The underpinning concept is maximizing the beneficial effects of each agent while avoiding potential adverse effects associated with larger doses of any single agent.
Pain itself has a neurotoxic effect47,48 and must be balanced with the increased risk (apnoea, respiratory depression, tolerance, and hypoxia) of intraoperative analgesic agents (eg, opioids including fentanyl). Increased fentanyl concentrations are found in the brain tissue of neonates and young infants due to an immature blood-brain barrier45 through direct causation with neurotoxic injury has not been established.49
Most elective paediatric GA in Ireland are typically managed with inhalational sevoflurane/isoflurane ±nitrous oxide for induction and maintenance50,51 When induction and maintenance of anaesthesia is through IV agents this is referred to as “total intravenous anaesthesia” (TIVA) and is preferentially employed in certain circumstances (eg, history of severe post-operative nausea and vomiting, certain day case procedures, trainee teaching, anticipated difficult airway management, etc.).52 TIVA can involve a combination of agents with synergistic effects, eg, remifentanil potentiates the effects of propofol, reducing required propofol dose by ~50%.53 It has not been established if TIVA can offer a reduced neurotoxic risk over inhalational methods; however, lower required drug doses would imply less risk.
What is Known Regarding Neurocognitive Risk Through Single GA Exposure?
There exists considerable controversy on this question, with conflicting published data.
Animal studies (eg, nematodes, rodents, and primates) have demonstrated histopathological changes in their developing brains following GA exposure. Proposed mechanisms include apoptotic injury, reactive oxygen species damage, neuroinflammation, and variable expression at N-methyl-d-aspartate (NMDA) and γ-amino butyric acid (GABA) receptors. Virtually all anaesthetic agents in common clinical practice are implicated, exerting effects as NMDA antagonists (eg, ketamine, nitrous oxide) and GABA agonists (eg, benzodiazepines, barbiturates, propofol, volatile anaesthetics)54 It is difficult to extrapolate these findings to the developing human brain for several reasons and thankfully these findings have failed to replicate in human studies.2,55
The GA compared to Spinal anaesthesia in infancy (GAS) trial is the only randomised controlled trial evaluating neurotoxicity risk with GA in children. It compared two groups of approximately 350 children randomised to undergo awake-regional anaesthesia or sevoflurane-based GA for elective hernia repair. Supplemental anaesthetic agents were not allowed in the GA group. The surgery duration was <1 hour. It demonstrates that sevoflurane held no additional neurotoxic risk over regional anaesthesia at five-year analysis, using intelligence quotient (IQ) scores as a comparative metric.4
The Paediatric Anaesthesia Neuro Development Assessment (PANDA) study was an ambidirectional, multicentre, sibling-matched cohort study in the United States between 2009 and 2015. Otherwise-healthy children who had one GA exposure for inguinal hernia repair before the age of 3 years were evaluated prospectively for IQ scores, neurocognitive, and neurobehavioral effects. These children, aged 8 to 15 years, were matched to a sibling within 36 months of their age who had no GA exposure. Anaesthetic agents used included volatile agents (eg, sevoflurane, isoflurane), IV agents (eg, propofol, thiopental, ketamine, midazolam, opioids) and adjunct caudal anaesthesia. There was no specific exploration of patient outcome according to the individual or combination of anaesthetic agents used. No statistically significant difference in the global cognitive/IQ scores of the exposed versus unexposed groups was demonstrated. Children who underwent multiple GA were not included.3
A similar Danish age-matched cohort study of 2689 children showed no difference in academic performance by age 15 or 16 years. Again, individual anaesthetic agents used in the exposure group were not analysed for relative risk.54 A recent dentistry publication showed no difference in full-scale IQ scores, the primary outcome, when measured 6 months after awake-local anaesthesia procedures (n = 144) versus sevoflurane-based GA procedures (n = 129) in children under 7 years old.56 This was despite the mean duration of these procedures being longer than 1 hour.
Most available evidence supports the neurodevelopmental safety of a single short (<1 hour) GA exposure in children, with most ophthalmic EUA/procedures falling within this criterion. However, not all studies concur. An Australian observational data linkage study in 2018 specifically aimed to minimise confounders. It found that children exposed to one hospitalisation and/or one GA before the age of 4 demonstrated lower numeracy scores on high school entry testing than those who had no exposure.57 Further publications suggest statistically significant reduction in IQ, language comprehension, and cognition with a single GA exposure.58,59 A limitation of the evidence above is a lack of standardisation between scoring methods and correction for confounders. Establishing direct causation is challenging.
Is There Increased Risk with Multiple GA/EUAs?
The Mayo Anaesthesia Safety in Kids (MASK) study addressed neurodevelopmental outcomes from multiple GA exposure. IQ scores and neuropsychological assessments were taken as primary and secondary outcomes, respectively. An association between GA exposure before age 3 and IQ was not demonstrated. However, those in the multiple exposure group demonstrated neuropsychological testing patterns associated with behavioural and learning difficulties, with modest reductions in cognitive processing speed and fine motor coordination.5
The Mayo Clinic published several large, retrospective, paediatric population-based cohort studies. In summary, those undergoing multiple GA at a young age had a significantly increased risk for the development of learning disability (LD) and/or attention deficit hyperactivity disorder (ADHD) at an older age. Wilder et al state that participants with no or one exposure to GA had no increased risk of LD development. However, 35% of those multiply exposed before 4 years of age developed LD by 19 years versus 20% of the unexposed. Sprung et al quote an incidence of 10.7% of ADHD by the age of 19 in those multiply exposed to GA before the age of 2 years versus 7.3% in the unexposed. Authors acknowledge that patients with LD may be overrepresented in this study due to active/detailed investigation for LD and above average retention of patients in their well-regarded local health services. Though children that require multiple procedures likely have a higher burden of illness, increasing their risk of LD, researchers remained unconvinced that increased risk was fully attributable to these non-GA-associated confounders.60–63
The Avon Longitudinal Study of Parents and Children (ALSPC) was a United Kingdom (UK) cohort study enrolling 13,433 children and compared 46 neurocognitive outcomes after single and multiple exposure to GA. It revealed some important results, namely lower motor and linguistic skills in all those exposed regardless of number of exposures. Additionally, dynamic balance, and behavioural scores were lower in the multiply exposed.64
Study Strengths and Limitations
Strengths of this study are the comparable 2-year period data sets from before and after the implementation of a new departmental strategy, allowing clear comparison of ophthalmic theatre use. Practical, patient centred methods to potentially reduce overall EUA numbers are generalisable and transferrable to most similarly equipped, tertiary paediatric ophthalmology departments. The technologies discussed are widely available at most European/North American centres. Analysis from the perspective of cost benefit was not carried out but would be expected to mirror the literature, demonstrating savings to the healthcare system for reduction of GA for EUA while reducing waiting lists for surgical interventions.25
Limitations of this study include its relatively short follow up. The retrospective observational design means that the ophthalmic diagnosis of children who avoided EUA in the latter half of the study period were not captured here. Surgical theatre records were used to generate the data set, which do not always capture if therapeutic intervention was undertaken during the procedure. Further study including comprehensive chart review of all patients involved, including who underwent EUA and those in which it was deferred or avoided altogether is suggested. Formalised audit of the impact of individual methods used to reduce EUA burden would be helpful, eg, reduction in numbers of EDT events requiring reversion to GA following initial attempt at awake testing. However, due in part to a heavy reliance on hard-copy medical records, this information was not uniformly recorded in clinical notes. Rather, anecdotal comparison through staff interview was relied upon, with the possibility of recall bias, etc. However, overall, the above approaches are potentially useful data that would help identify cases suitable for EUA deferral/avoidance at other units who may wish to adopt a similar approach. Coming from an ophthalmic perspective, comprehensive markers of neurodevelopment/toxicity (eg, sibling-matched IQ) were not assessed and further study would be required to report future incidence/prevalence figures of neurotoxicity among those exposed in this study, acknowledging that causation is difficult to establish in the literature (eg, the effect of underlying medical conditions, multiple exposures to hospitalisation etc).
Summary
The PANDA, GAS and MASK studies demonstrate that single, short (<1 hour) exposure to GA in childhood confers minimal risk of neurodevelopmental injury.3–5 However, the published data does not fully resolve the issue of the risk of neurotoxicity from ≥2 GA in the paediatric population.57–59 All studies to date have been observational, apart from the GAS trial, which itself was limited regarding the neurotoxic risk through multiple exposures.4
Deliberate design of future studies is critical to attempt further clarification of neurodevelopmental risk from the individual factors (ie, patient, medication/pharmacological, surgical intervention) involved in GA. RCTs are difficult to power while maintaining the safety of the populace, and thus endpoints/outcome measures of case control/cohort studies64 must be deliberately designed and validated. A 2019 review article emphasises that delay of elective surgery until after age 3 or 4 is preferable for risk mitigation while further work is carried out to determine the most vulnerable age ranges and if certain anaesthetic agents are less toxic within particular age groups.65 Perhaps, a particular investigation will emerge as an objective and reproducible means of evaluating established neurotoxic damage or, better yet, to identify the most at-risk population before exposure. A small 2019 study by Oba et al suggested visually evoked potential (VEP) responses as an objective, reliable measurement of neurotoxicity in children multiply exposed to GA on at least 15 occasions during treatment for corrosive oesophagitis. VEPs were performed in awake patients at least 3 days post op and compared with those of children with no previous GA exposure exposed to GA.66 A validated pre-EUA checklist may augment the decision-making process in a paediatric ophthalmology setting.
Conclusion: Where to Next? - Application to Clinical Practice
We have demonstrated significant reductions in EUAs through the application of a cautionary principle that repeated GA exposure in children may have deleterious neurocognitive effects over time. Active minimisation was achieved with the use of minimally invasive and innovative strategies for the evaluation of the paediatric patient such as new technology, updated training, and a multi-visit approach, thus leaving GA/EUA for unavoidable, challenging cases where the benefit outweighs potential risk. Reducing EUA/GA when possible, represents a common-sense, multidisciplinary teamwork approach between ophthalmologists and anaesthesiologists. Common goals are to minimise individual patient risk, maintain surgical list efficiency and reduce waiting lists. We believe the methods outlined adopted by our centre can be used to facilitate awake assessment of variably cooperative children in similarly equipped units internationally.
Is it advisable to discuss this potential issue with patients and parents, balancing this with the risk of causing unnecessary stress and fear? Some do advocate for this approach.67 The current consensus of the anaesthesia community of Ireland and the UK is that a discussion on this topic is not mandatory for every preoperative consultation.2
Any potential for harm through clinical intervention will remain an area of great interest to paediatric ophthalmologists, balanced with avoidance of delay for vital diagnostic/therapeutic indications, as echoed in the 2017 amendment to the original FDA advisory.68 Until this important clinical question can be definitively answered, all emerging evidence will be closely debated and scrutinised.
Data Sharing Statement
Anonymised data supporting the results reported in this manuscript are available upon reasonable request from the corresponding author.
Acknowledgments
Gillian O’Mullane - Head orthoptist/senior electrophysiologist and Sabrina Shanahan, Clinical nurse manager at the paediatric ophthalmology department, CHI-TS: data collection assistance and the ongoing, excellent care of study participants. Dr Aoife Doolan, Consultant Anaesthetist, Tallaght University Hospital, Dublin: scholarly discussion contributing to the development of the article.
Ethics Approval and Informed Consent
This study was non-interventional, involving the retrospective analysis of anonymised data, adhering to the tenets of the Declaration of Helsinki.
Disclosure
The authors have no competing interests to declare, financial or non-financial.
References
1. FDA. Drug Safety Communication: FDA review results in new warnings about using general anesthetics and sedation drugs in young children and pregnant women; 2016. Available from: www.fda.gov/Drugs/DrugSafety/ucm532356htm.
2. Association of Paediatric Anaesthetists of Great Britain and Ireland. Joint Professional Guidance on the Use of Anaesthesia in Young Children. APAGBI; 2017.
3. Sun LS, Li G, Miller TLK, et al. Association between a single general anesthesia exposure before age 36 months and neurocognitive outcomes in later childhood. JAMA. 2016;315(21):2312–2320. doi:10.1001/jama.2016.6967
4. McCann ME, de Graaff JC, Dorris L, et al. Neurodevelopmental outcome at 5 years of age after general anaesthesia or awake-regional anaesthesia in infancy (GAS): an international, multicentre, randomised, controlled equivalence trial. Lancet. 2019;393(10172):664–677. doi:10.1016/S0140-6736(18)32485-1
5. Warner DO, Zaccariello MJ, Katusic SK, et al. Neuropsychological and behavioral outcomes after exposure of young children to procedures requiring general anesthesia: the Mayo Anesthesia Safety in Kids (MASK) study. Anesthesiology. 2018;129(1):89–105.
6. Lee JH, Zhang J, Wei L, Yu SP. Neurodevelopmental implications of the general anesthesia in neonate and infants. Exp Neurol. 2015;272:50–60.
7. McBride GR, Stephenson KAJ, Comer G, Flanagan O. The use of oral midazolam to facilitate the ophthalmic examination of children with autism and developmental disorders. J Autism Dev Disord. 2021;51(5):1678–1682.
8. Vigoda MM, Latiff A, Murray TG, Tutiven JL, Berrocal AM, Gayer S. Can children undergoing ophthalmologic examinations under anesthesia be safely anesthetized without using an IV line? Clin Ophthalmol. 2011;5:503–508.
9. Yip IYM, Tacea F, Dodeja R, Pendlebury J, Yeo DCM. Ophthalmology examinations under anaesthesia carried out on non-ophthalmology lists in a specialist children’s hospital. Eye. 2021;36:669–670.
10. Fabian ID, Shah V, Kapelushnik N, et al. Number, frequency and time interval of examinations under anesthesia in bilateral retinoblastoma. Graefes Arch Clin Exp Ophthalmol. 2020;258(4):879–886. doi:10.1007/s00417-019-04589-4
11. Yu Chan JY, Choy BN, Ng AL, Shum JW. Review on the management of primary congenital glaucoma. J Curr Glaucoma Pract. 2015;9(3):92–99. doi:10.5005/jp-journals-10008-1192
12. Weinreb RN, Grajewski AL, Papadopoulos M, Grigg J, Freedman S. Childhood Glaucoma. Vol. 9. Kugler Publications; 2013.
13. Adam RS, Kertes PJ, Lam W-C. Observations on the management of Coats’ disease: less is more. Br J Ophthalmol. 2007;91(3):303–306. doi:10.1136/bjo.2006.103382
14. Uribe AA, Mendel E, Peters ZA, Shneker BF, Abdel-Rasoul M, Bergese SD. Comparison of visual evoked potential monitoring during spine surgeries under total intravenous anesthesia versus balanced general anesthesia. Clin Neurophysiol. 2017;128(10):2006–2013. doi:10.1016/j.clinph.2017.07.420
15. Robson AG, Nilsson J, Li S, et al. ISCEV guide to visual electrodiagnostic procedures. Doc Ophthalmol. 2018;136(1):1–26. doi:10.1007/s10633-017-9621-y
16. Meredith SP, Reddy MA, Allen LE, Moore AT, Bradshaw K. Full-field ERG responses recorded with skin electrodes in paediatric patients with retinal dystrophy. Doc Ophthalmol. 2004;109(1):57–66. doi:10.1007/s10633-004-1752-2
17. Pillai GS, Radhakrishnan N. Ocular manifestations of pediatric systemic diseases. Indian J Pediatr. 2018;85(3):217–227. doi:10.1007/s12098-018-2623-2
18. Guretzky TJ, Dyke PC, Whitley HG. Ocular manifestations of cardiac disease. In: Levin AV, Enzenauer RW, editors. The Eye in Pediatric Systemic Disease. Cham: Springer International Publishing; 2017:79–89.
19. Allen LE, Cosgrave EM, Kersey JP, Ramaswami U. Fabry disease in children: correlation between ocular manifestations, genotype and systemic clinical severity. Br J Ophthalmol. 2010;94(12):1602. doi:10.1136/bjo.2009.176651
20. Patel CK, Buckle M. Ultra-widefield imaging for pediatric retinal disease. Asia Pac J Ophthalmol. 2018;7(3):1. doi:10.22608/APO.201857
21. Biswas S, Gray J, Stanga PE. Optos® widefield retinal imaging in a paediatric vitreoretinal service. Invest Ophthalmol Vis Sci. 2012;53(14):1164.
22. McCulloch DL, Garcia-filion P, Matar M, Stewart C, Borchert MS. Repeated measurements of ERGs and VEPs using chloral hydrate sedation and propofol anesthesia in young children. Doc Ophthalmol. 2021;143:141–153. doi:10.1007/s10633-021-09830-2
23. Thompson DA, Fritsch DM, Hardy SE. The changing shape of the ISCEV standard pattern onset VEP. Doc Ophthalmol. 2017;135(1):69–76. doi:10.1007/s10633-017-9596-8
24. Bellinger DC, Calderon J. Neurotoxicity of general anesthetics in children: evidence and uncertainties. Curr Opin Pediatr. 2019;31(2):267–273. doi:10.1097/MOP.0000000000000737
25. Burnett HF, Lambley R, West SK, Ungar WJ, Mireskandari K. Cost-effectiveness analysis of clinic-based chloral hydrate sedation versus general anaesthesia for paediatric ophthalmological procedures. Br J Ophthalmol. 2015;99(11):1565–1570. doi:10.1136/bjophthalmol-2015-306604
26. West SK, Griffiths B, Shariff Y, Stephens D, Mireskandari K. Utilisation of an outpatient sedation unit in paediatric ophthalmology: safety and effectiveness of chloral hydrate in 1509 sedation episodes. Br J Ophthalmol. 2013;97(11):1437–1442. doi:10.1136/bjophthalmol-2013-303818
27. Parsa CF, Adyanthaya R. Why atropine drops should be used in down syndrome. Br J Ophthalmol. 2008;92(2):295–296. doi:10.1136/bjo.2007.122457
28. Harris WS, Goodman RM. Hyper-reactivity to atropine in Down’s syndrome. N Engl J Med. 1968;279(8):407–410. doi:10.1056/NEJM196808222790805
29. Kauser F, Gupta Y, Amitava AK, et al. Do all children need a cycloplegic refraction? A comparison of Mohindra’s versus cycloplegic refraction. Indian J Ophthalmol. 2020;68(11):2458–2461. doi:10.4103/ijo.IJO_229_20
30. Mohindra I, Molinari JF. Near retinoscopy and cycloplegic retinoscopy in early primary grade schoolchildren. Am J Optom Physiol Opt. 1979;56(1):34–38. doi:10.1097/00006324-197901000-00006
31. Major E, Dutson T, Moshirfar M. Cycloplegia in children: an optometrist’s perspective. Clin Optom. 2020;12:129–133. doi:10.2147/OPTO.S217645
32. Farhood QK. Cycloplegic refraction in children with cyclopentolate versus atropine. J Clin Exp Ophthalmol. 2012;3(7):1–6. doi:10.4172/2155-9570.1000239
33. Mohindra I. A technique for infant vision examination. Am J Optom Physiol Opt. 1975;52(12):867–870. doi:10.1097/00006324-197512000-00008
34. Vagge A, Ferro Desideri L, Nucci P, et al. Congenital Nasolacrimal Duct Obstruction (CNLDO): a review. Diseases. 2018;6(4):96. doi:10.3390/diseases6040096
35. Skalet AH, Gombos DS, Gallie BL, et al. Screening children at risk for retinoblastoma: consensus report from the American Association of Ophthalmic Oncologists and Pathologists. Ophthalmology. 2018;125(3):453–458. doi:10.1016/j.ophtha.2017.09.001
36. Salvetat ML, Zeppieri M, Miani F, Tosoni C, Parisi L, Brusini P. Comparison of iCare tonometer and Goldmann applanation tonometry in normal corneas and in eyes with automated lamellar and penetrating keratoplasty. Eye. 2011;25(5):642–650. doi:10.1038/eye.2011.60
37. Chiang MF, Wang L, Busuioc M, et al. Telemedical retinopathy of prematurity diagnosis: accuracy, reliability, and image quality. Arch Ophthalmol. 2007;125(11):1531–1538. doi:10.1001/archopht.125.11.1531
38. Scruggs BA, Chan RVP, Kalpathy-Cramer J, Chiang MF, Campbell JP. Artificial intelligence in retinopathy of prematurity diagnosis. Transl Vis Sci Technol. 2020;9(2):5. doi:10.1167/tvst.9.2.5
39. Lalwani K, Tomlinson M, Koh J, Wheeler D. Office-based deep sedation for pediatric ophthalmologic procedures using a sedation service model. Anesthesiol Res Pract. 2012;2012:598593. doi:10.1155/2012/598593
40. Tan ACS, Chen L, Png R, Chia A. The diagnosis and assessment of visual function in Singaporean children with electrophysiology: 10-year results. Doc Ophthalmol. 2016;132(3):189–199.
41. Unwin KL, Powell G, Jones CR. The use of multi-sensory environments with autistic children: exploring the effect of having control of sensory changes. Autism. 2021;26:13623613211050176.
42. Breslin L, Guerra N, Ganz L, Ervin D. Clinical utility of multisensory environments for people with intellectual and developmental disabilities: a scoping review. Am J Occup Ther. 2020;74(1):7401205060p7401205061–7401205060p7401205012.
43. Constable PA, Bach M, Frishman LJ, Jeffrey BG, Robson AG. ISCEV standard for clinical electro-oculography (2017 update). Doc Ophthalmol. 2017;134(1):1–9.
44. Judisch GF, Anderson S, Bell WE. Chloral hydrate sedation as a substitute for examination under anesthesia in pediatric ophthalmology. Am J Ophthalmol. 1980;89(4):560–563.
45. Verghese ST, Hannallah RS. Acute pain management in children. J Pain Res. 2010;3:105–123.
46. National Library of Medicine. In: Post TW, ed. Neurotoxic Effects of Anesthetics on the Developing Brain UTD 2020. Waltham, MA:National Library of Medicine; 2020.
47. Yang S, Chang MC. Chronic pain: structural and functional changes in brain structures and associated negative affective states. Int J Mol Sci. 2019;20(13):3130.
48. Hashmi JA, Baliki MN, Huang L, et al. Shape shifting pain: chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain. 2013;136(Pt 9):2751–2768.
49. Baldacchino A, Arbuckle K, Petrie DJ, McCowan C. Neurobehavioral consequences of chronic intrauterine opioid exposure in infants and preschool children: a systematic review and meta-analysis. BMC Psychiatry. 2014;14(1):104.
50. Gaynor J, Ansermino JM. Paediatric total intravenous anaesthesia. BJA Educ. 2016;16(11):369–373.
51. James I. Anaesthesia for paediatric eye surgery. Contin Educ Anaesth Crit Care Pain. 2008;8(1):5–10.
52. Al-Rifai Z, Mulvey D. Principles of total intravenous anaesthesia: practical aspects of using total intravenous anaesthesia. BJA Educ. 2016;16(8):276–280.
53. Nimmo AF, Absalom AR, Bagshaw O, et al. Guidelines for the safe practice of total intravenous anaesthesia (TIVA). Anaesthesia. 2019;74(2):211–224.
54. Hansen TG, Pedersen JK, Henneberg SW, et al. Academic performance in adolescence after inguinal hernia repair in infancy: a nationwide cohort study. Anesthesiology. 2011;114(5):1076–1085.
55. Shao L-J-Z, Zou Y, Xue F-S. Anesthesia-induced developmental neurotoxicity in children: past, present, and future. Chin Med J. 2019;132(16):1990–1992.
56. Zhou P, Zhang C, Huang G, Hu Y, Ma W, Yu C. The effect of sevoflurane anesthesia for dental procedure on neurocognition in children: a prospective, equivalence, controlled trial. BMC Pediatr. 2021;21(1):177.
57. Schneuer FJ, Bentley JP, Davidson AJ, et al. The impact of general anesthesia on child development and school performance: a population-based study. Paediatr Anaesth. 2018;28(6):528–536.
58. Backeljauw B, Holland SK, Altaye M, Loepke AW. Cognition and brain structure following early childhood surgery with anesthesia. Pediatrics. 2015;136(1):e1–12.
59. Ing C, DiMaggio C, Whitehouse A, et al. Long-term differences in language and cognitive function after childhood exposure to anesthesia. Pediatrics. 2012;130(3):e476–485.
60. Flick RP, Katusic SK, Colligan RC, et al. Cognitive and behavioral outcomes after early exposure to anesthesia and surgery. Pediatrics. 2011;128(5):e1053–1061.
61. Hu D, Flick RP, Zaccariello MJ, et al. Association between exposure of young children to procedures requiring general anesthesia and learning and behavioral outcomes in a population-based birth cohort. Anesthesiology. 2017;127(2):227–240.
62. Sprung J, Flick RP, Katusic SK, et al. Attention-deficit/hyperactivity disorder after early exposure to procedures requiring general anesthesia. Mayo Clin Proc. 2012;87(2):120–129.
63. Wilder Robert T, Flick Randall P, Sprung J, et al. Early exposure to anesthesia and learning disabilities in a population-based birth cohort. Anesthesiology. 2009;110(4):796–804.
64. Walkden GJ, Gill H, Davies NM, Peters AE, Wright I, Pickering AE. Early childhood general anesthesia and neurodevelopmental outcomes in the Avon longitudinal study of parents and children birth cohort. Anesthesiology. 2020;133(5):1007–1020.
65. McCann ME, Soriano SG. Does general anesthesia affect neurodevelopment in infants and children? BMJ. 2019;367:l6459.
66. Oba S, Işıl CT, Türk HŞ, et al. Evaluation of neurotoxicity of multiple anesthesia in children using visual evoked potentials. Sisli Etfal Hastan Tip Bul. 2019;53(3):284–289.
67. Andropoulos DB, Greene MF. Anesthesia and developing brains — implications of the FDA warning. N Eng J Med. 2017;376(10):905–907.
68. FDA. Food and Drug Administration: drug safety communication; 2017. Available from: https://www.fda.gov/Drugs/DrugSafety/ucm554634.htm.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.