")
Back to Journals » Clinical Epidemiology » Volume 12
Risk of Anemia in Patients with Newly Identified Chronic Kidney Disease – A Population-Based Cohort Study
Authors Vestergaard SV , Heide-Jørgensen U , van Haalen H, James G, Hedman K, Birn H, Thomsen RW , Christiansen CF
Received 23 April 2020
Accepted for publication 2 August 2020
Published 11 September 2020 Volume 2020:12 Pages 953—962
DOI https://doi.org/10.2147/CLEP.S259648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Eyal Cohen
Søren Viborg Vestergaard,1 Uffe Heide-Jørgensen,1 Heleen van Haalen,2 Glen James,3 Katarina Hedman,4 Henrik Birn,5,6 Reimar Wernich Thomsen,1 Christian Fynbo Christiansen1
1Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark; 2Health Economics & Payer Evidence, AstraZeneca, Gothenburg, Sweden; 3Epidemiology, AstraZeneca, Cambridge, UK; 4Biometrics, AstraZeneca, Gothenburg, Sweden; 5Department of Renal Medicine, Aarhus University Hospital, Aarhus, Denmark; 6Department of Biomedicine, Aarhus University, Aarhus, Denmark
Correspondence: Søren Viborg Vestergaard
Department of Clinical Epidemiology, Aarhus University Hospital, Olof Palmes Allé 43-45, Aarhus N 8200, Denmark
Tel +45 87168514
Email [email protected]
Purpose: Anemia is prevalent in patients with chronic kidney disease (CKD), but the longitudinal risk of anemia in patients with newly identified CKD is unknown. We therefore examined the risks of experiencing anemia in persons with newly identified CKD.
Patients and Methods: This cohort study included adult patients with newly identified CKD stages 3– 5 defined by an estimated glomerular filtration rate (eGFR) level < 60 mL/min/1.73m2 (at least two measurements ≥ 90 days apart) ascertained from a population-based registry with complete laboratory test results in Northern Denmark (population ∼ 2.2 million) during 2009– 2016. We calculated 1) cumulative incidence (risk) of anemia [hemoglobin < 12/< 13 g/dl in women/men] by CKD stage, and 2) adjusted hazard ratios (HRs) of anemia using Cox regression analyses.
Results: We identified 55,940 distinct individuals with newly identified CKD stages 3– 5 and no prevalent anemia [n=41,958 patients in stage 3a, n=17,875 in stage 3b, n=5182 in stage 4, and n=931 in stage 5]. After one year, 42.3% (95%-confidence interval [CI]: 41.9– 42.7) of patients with CKD stages 3– 5 had newly measured anemia, increasing to 67.7% (95%-CI: 67.2– 68.2) after five years. The absolute and relative anemia risk increased markedly with higher CKD stages. The adjusted HR of any anemia was 5.42 (95%-CI: 5.09– 5.77) in patients with CKD stage 5 compared to patients with CKD stage 3a.
Conclusion: Patients with newly identified CKD stages 3– 5 have a substantial risk of anemia, increasing with higher CKD stages. This study underlines that clinical awareness of anemia risk is important in patients with newly identified or progressed CKD.
Keywords: anemia, chronic kidney disease, CKD, epidemiology, cohort study
Introduction
Anemia is common in patients with chronic kidney disease (CKD),1 increasing the risk of cognitive impairment, sleep disturbances, cardiovascular comorbidities, need for dialysis, and all-cause mortality.2–4
Current knowledge is limited to data from cross-sectional studies reporting a prevalence of anemia ranging from 5% to 51%5,11 in patients with CKD stage 3 (estimated glomerular filtration rate [eGFR] = 30–59 mL/min/1.73 m2) and from 53% to 97%6,11 in patients with stage 5 CKD (eGFR <15 mL/min/1.73 m2). However, anemia prevalence in persons with prevalent CKD depends on duration of CKD and on clinical management of anemia, reducing the utility of the reported prevalence in clinical care.
The exact longitudinal risk of developing anemia in patients with newly identified CKD stages 3–5 (eGFR <60 mL/min/1.73 m2) remains unknown.
We therefore examined the risk of newly measured anemia in patients with newly identified CKD stages 3–5 in a large population-based cohort study conducted in Northern Denmark during 2009–2016.
Patients and Methods
Setting
We conducted a population-based cohort study using data from routine inpatient and outpatient clinical care in Northern Denmark during January 1, 2009 through December 31, 2016 (source population ~2.2 million). The study included all adult patients with newly identified CKD stages 3–5, based on eGFR derived from plasma creatinine values, and followed them for anemia diagnosed on the basis of a low blood hemoglobin (Hb) level.
Data Sources
The Civil Registration System12 contains a personal identification number for every Danish citizen, encoding date of birth and sex of each person. It allows unambiguous linkage between public registries, enabling lifetime follow-up of patients receiving care from the Danish universal health system.
The Laboratory Information System13 is a registry containing laboratory test results from hospital laboratories in Northern Denmark since 1997. These encompass tests ordered during routine clinical care of inpatients and outpatients (at both hospital clinics and general practices in the community). For every test, the registry includes type of test, test result, and exact date of the analysis.
The Danish National Patient Registry14 contains records of hospital inpatient admissions since 1977, and emergency room visits and outpatient clinic contacts since 1995. Data include dates of admission and discharge, hospital and department codes, surgical procedures and major treatments, and primary and secondary discharge diagnoses. Since 1994, diagnoses have been coded according to the Danish version of the International Classification of Diseases, Tenth Revision (ICD-10).
The Danish National Prescription Registry15 contains data on all prescriptions filled at Danish outpatient pharmacies since 1995, including drug type classified according to the Anatomical Therapeutic Chemical (ATC) classification system.
Study Design
Definition of Newly Identified CKD
We obtained all recorded plasma creatinine tests in Northern Denmark during 1997–2016 and calculated eGFR from these using the four-variable modification of diet in renal disease (4v MDRD) formula without correction for race, as majority of Danes are Caucasian.16 CKD stage 3–5 was defined as two eGFRs <60 mL/min/1.73 m2 at least 90 days apart, with no eGFR estimate above this threshold between these two tests.17 We considered CKD as newly identified when it was first observed during the study period 2009–2016, ie, criteria were not fulfilled during 1997–2008. The date of the second and qualifying eGFR was defined as the index date for newly identified CKD stage 3–5. The CKD stage at index was defined by the maximal eGFR measurement during the ≥90 day period, classified as stage 3a (eGFR between 45 and 59 mL/min/1.73 m2); stage 3b (eGFR between 30 and 44 mL/min/1.73 m2); stage 4 (eGFR between 15 and 29 mL/min/1.73 m2); and stage 5 (eGFR less than 15 mL/min/1.73 m2).17
Study Cohorts
During 2009–2016 we identified five cohorts of patients at least 18 years old with newly identified or newly progressed to stage 3a, 3b, 4, 5, or any stage 3–5 CKD (first entry to one of the stage 3–5 cohorts) (Figure 1 and Suppl. Figure 1). We allowed patients to enter more advanced CKD stage cohorts if their eGFR declined during the study period. However, patients were not allowed to enter a lower CKD stage cohort if their eGFR increased, as we assumed chronicity of CKD.
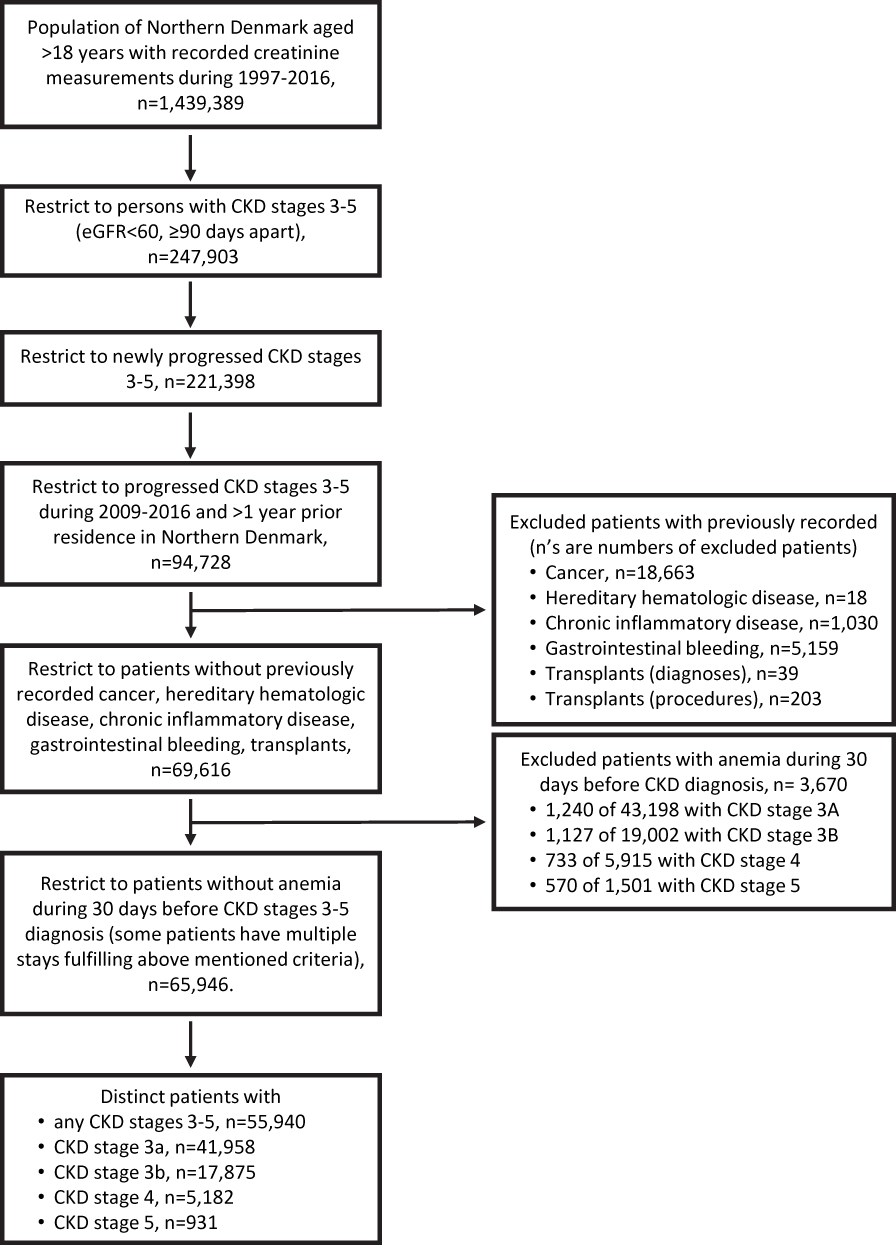 |
Figure 1 Selection of cohort of persons with newly identified CKD stages 3–5 and no prevalent anemia. |
To reduce the risk of recording anemia events stemming from causes other than CKD, we excluded patients with diagnoses of common other causes of anemia (any cancer, hereditary hematologic diseases, chronic inflammatory diseases, gastrointestinal bleeding, or any organ transplant) recorded in the Danish National Patient Registry any time prior to the index date of newly identified CKD (see ICD codes in the Appendix). We excluded patients with known prevalent anemia, ie, a low blood hemoglobin (Hb) level test result within 30 days prior to (not including) the CKD index date. Anemia was considered as an outcome if recorded on the CKD index date, ie, on the same date as the second and CKD stage qualifying eGFR test, or afterwards.
Anemia Outcomes
We defined anemia as a recorded blood Hb level <12 g/dl in women and <13 g/dl in men).18 Anemia was additionally classified into three grades, ie, mild (grade 1): Hb level of 10 to <12 g/dl in women, and 10 to <13 g/dl in men; moderate (grade 2): Hb level of 8 to <10 g/dl; and severe (grade 3): Hb level of <8 g/dl.19
Anemia was further characterized by mean corpuscular hemoglobin (MCH) (hypochromic/normochromic/hyperchromic) and mean corpuscular volume (MCV) (microcytic/normocytic/macrocytic), if this information was available in the laboratory results (see Appendix for specific definitions).20
Covariates
Covariates included age, sex, calendar year of CKD diagnosis, and comorbidity prior to the CKD index date (ie, conditions included in the Charlson Comorbidity Index [CCI] excluding renal disease).21 We calculated CCI scores for every patient based on all their hospital inpatient and outpatient diagnoses during the 10 years prior to the index date (CCI categories: score 0=Low, 1–2=Medium, 3+=High).22 From the Danish National Patient Registry, we collected information on dialysis treatments within 90 days prior to the index date, and on cardiovascular disease, diabetes, chronic pulmonary disease, and liver disease recorded during 10 years before index date. Finally, we obtained information on filled prescriptions during 12 months before index of angiotensin-converting-enzyme inhibitors (ACE-Is), angiotensin II receptor blockers (ARBs), loop diuretics, aspirin, immunosuppressants, glucocorticoids, and vitamin K antagonists from the Danish National Prescription Registry (see codebooks in Appendix).
Statistical Analyses
We tabulated patient characteristics as of the CKD stage index date, and followed patients from their index date until the first of each anemia events of interest, or emigration, death, or 31 December 2016 (the last date that data were available), whichever came first. Anemia events included any anemia and graded anemia (mild, moderate, or severe anemia) on the CKD stage index date or afterwards, and for each anemia event follow-up was stopped only for further anemia events of the same grade. If patients entered a higher CKD stage during follow up, they were not censored from their previous CKD stage cohort. Thus, patients could contribute risk-time to more than one CKD stage cohort at a time. We estimated the incidence rate (IR) per 100 person-years of each anemia outcome, as well as the cumulative incidence proportion (risk) 1, 2, 3, and 5 years after the index date of CKD, considering death as a competing event. We tabulated these risks overall as well as stratified by CKD stage, age, sex, CCI category, diabetes, and any cardiovascular disease. We used Cox regression models to estimate hazard ratios (HRs) for anemia across different CKD stages, with CKD stage 3a serving as the reference group. We used a robust sandwich estimator in the Cox regressions as patients were allowed to belong to several cohorts, introducing dependency between observations.23 Both crude HRs and HRs adjusted for sex, age, calendar year, and CCI category were estimated. We calculated 95% confidence intervals (CIs) for every outcome estimate.
All analyses were performed using SAS version 9.4 (Cary, NC, USA). The study was approved by the Danish Data Protection Agency (record number 2015–57-0002, Aarhus University record number 2016–051-000001/812). According to Danish legislation, no approval from an ethics committee or informed consent from patients are required for registry-based studies.
Results
Patient Characteristics
From 2009 to 2016, we found 55,940 distinct individuals with newly identified CKD stages 3–5 and without recent anemia prior to study inclusion (Figure 1), after the exclusion of 3670 patients with prevalent anemia during the 30 days prior to the index date (5% of the entire CKD cohort; 3%, 6%, 12%, and 38% of patients with CKD stages 3a, 3b, 4, and 5, respectively). As a patient may have belonged to several CKD stage cohorts over the course of follow up, there were a total of 41,958 patients in the CKD 3a cohort, 17,875 in the CKD 3b cohort, 5182 in the CKD 4 cohort, and 931 in the CKD 5 cohort. Table 1 shows baseline patient characteristics in each CKD cohort. Overall, the study population included more women (58%) than men (42%). The median age at index date was 77 years and highest in stages 3b and 4 CKD. Comorbidity levels were high and increased with CKD stage. Among persons with any CKD, 21,462 (38.4%) had cardiovascular disease and 11,931 (21.3%) had diabetes diagnosed up to 10 years before CKD index date. Only a few patients (n=93 [0.2%]) had been treated with dialysis within 90 days preceding their index date of newly identified CKD (Table 1).
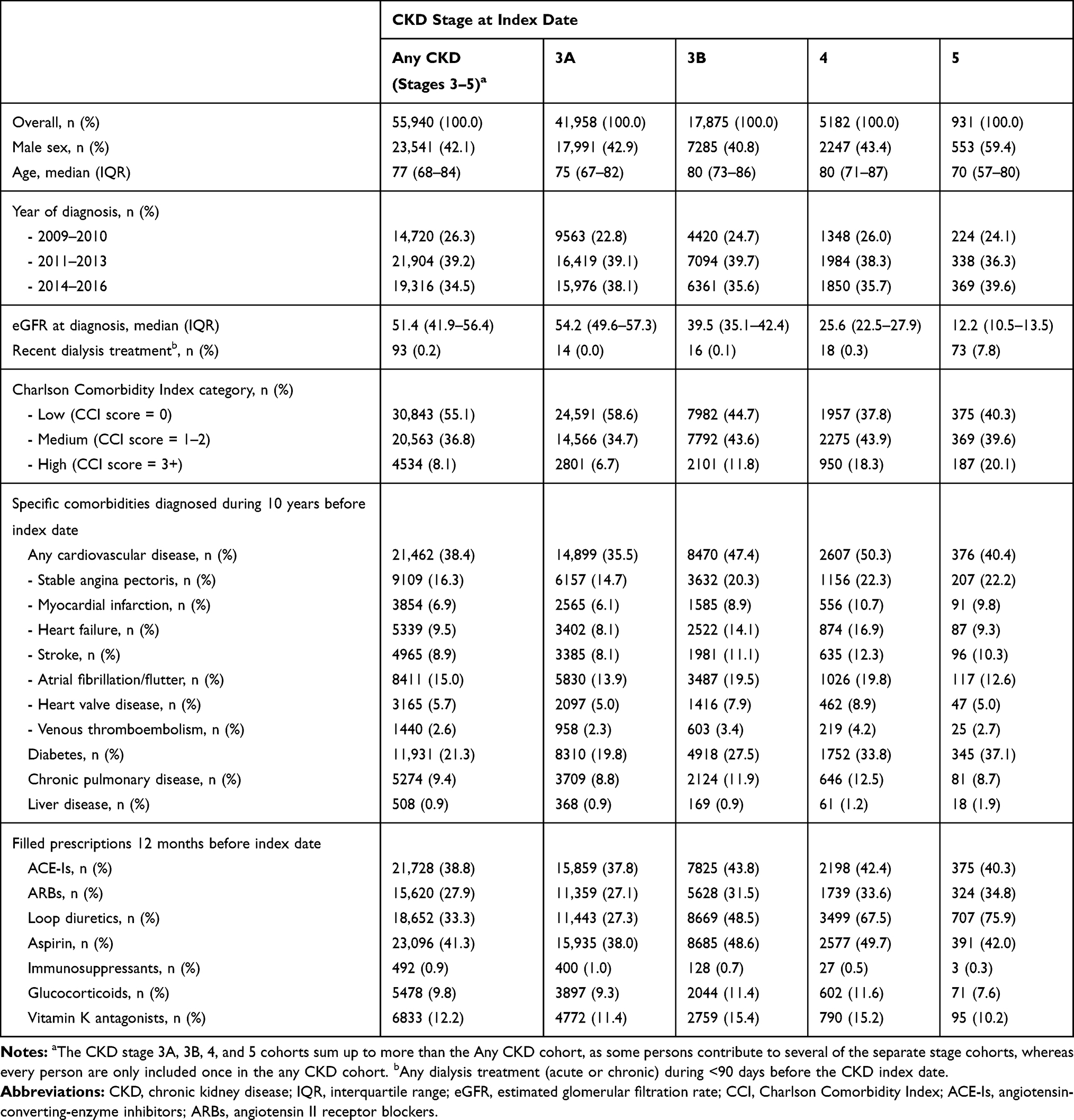 |
Table 1 Characteristics of 55,940 Patients with Newly Identified CKD Stages 3–5, Northern Denmark, 2009–2016 |
Anemia Outcomes
The 55,940 unique CKD patients were followed for a median of 12 months (interquartile range [IQR]: 0.6–34 months). During follow-up we identified a total of 33,614 newly measured anemia events. Within one year, 42.3% (95% CI: 41.9–42.7) of all CKD stage 3–5 patients experienced anemia. The proportion who had anemia increased to 67.7% (95% CI: 67.2–68.2) within five years after study inclusion (Table 2).
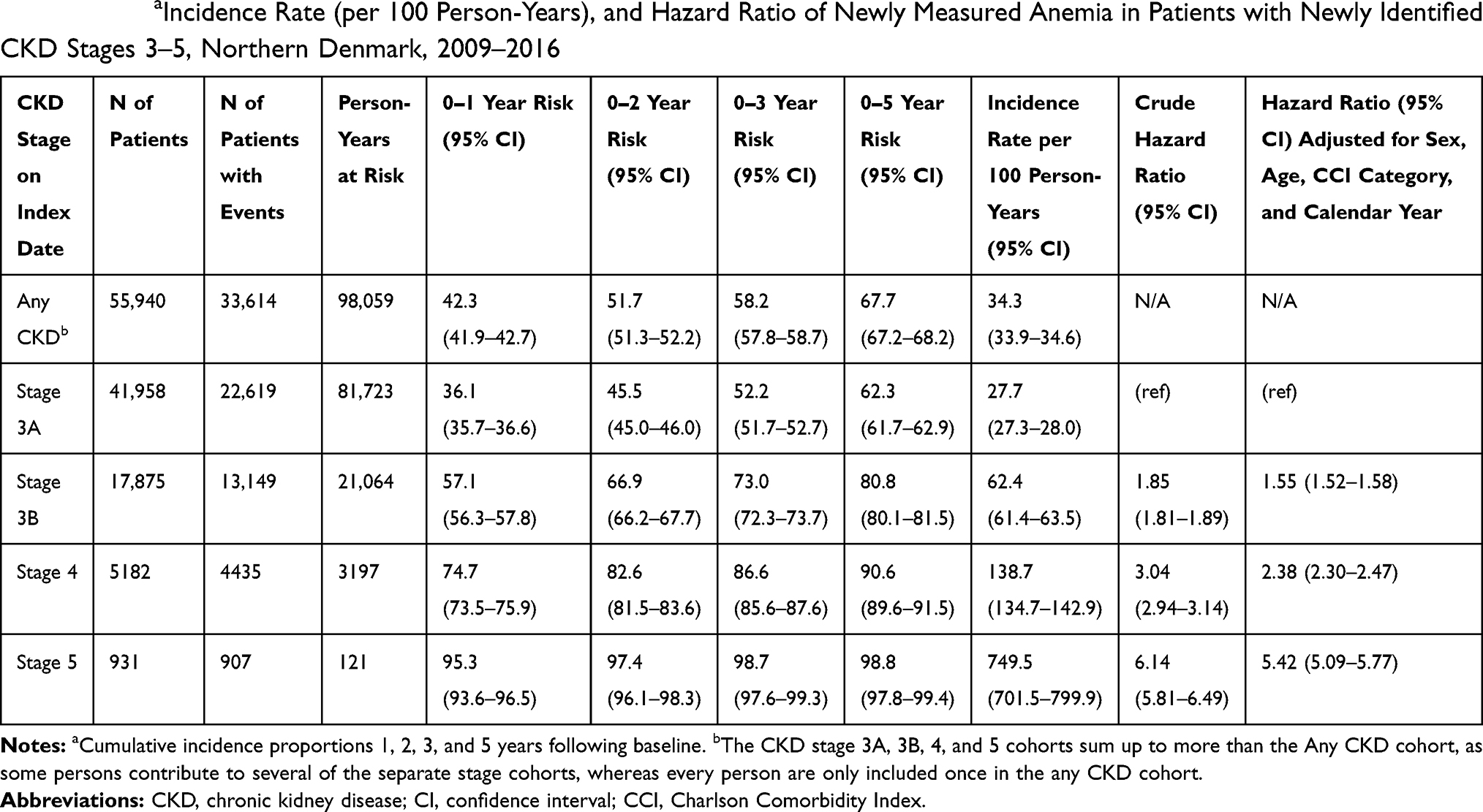 |
Table 2 Risk aIncidence Rate (per 100 Person-Years), and Hazard Ratio of Newly Measured Anemia in Patients with Newly Identified CKD Stages 3–5, Northern Denmark, 2009–2016 |
Patients with CKD stage 3a had the lowest risk: one in three patients experienced anemia during the first year of follow up, increasing to two in three patients after 5 years. Risk increased with higher CKD stages. Among patients in CKD stage 5, nearly every patient experienced an anemia event within one year (Table 2 and Figure 2). Higher CKD stages were also associated with shorter time to an anemia diagnosis, reflected in higher IRs of anemia (Table 2). Cox regression yielded increased anemia hazard ratios for higher CKD stages. After confounder adjustment, estimates decreased somewhat in all CKD stages (Table 2).
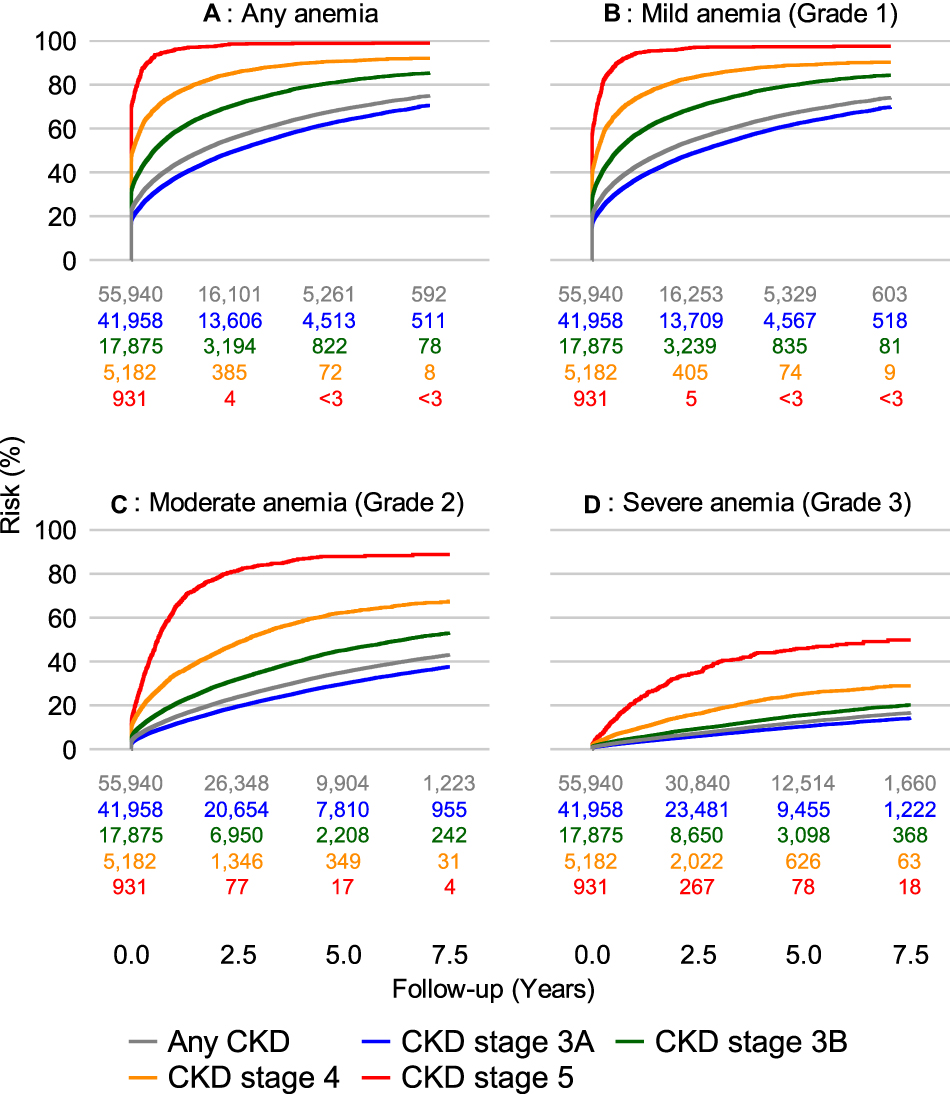 |
Figure 2 Cumulative risk of developing any anemia (Panel (A) and anemia of varying severity (Panels B–D), according to newly identified CKD stage: any CKD (grey curve), stage 3a (blue curve), 3b (green curve), stage 4 (yellow curve), stage 5 (red curve). |
To identify potential effect measure modification, in Table 3, we present the rates of anemia stratified by age, sex, comorbidity level (CCI category), prior cardiovascular disease, and prior diabetes. Compared to patients aged <65 years, higher rates of anemia were observed in patients aged over 65 years (IR = 38.4 [95% CI: 38.0 −38.9] versus IR = 19.8 [95% CI: 19.2–20.4] per 100 person-years). Higher rates of anemia were also observed in male patients compared to female patients (IR = 41.3 [95% CI: 40.7–42.0] versus IR = 30.0 [95% CI: 29.6–30.4] per 100 person-years). In addition, anemia rates were markedly increased in patients with higher CCI scores on their index date, as well as in patients with diabetes or cardiovascular disease (Table 3).
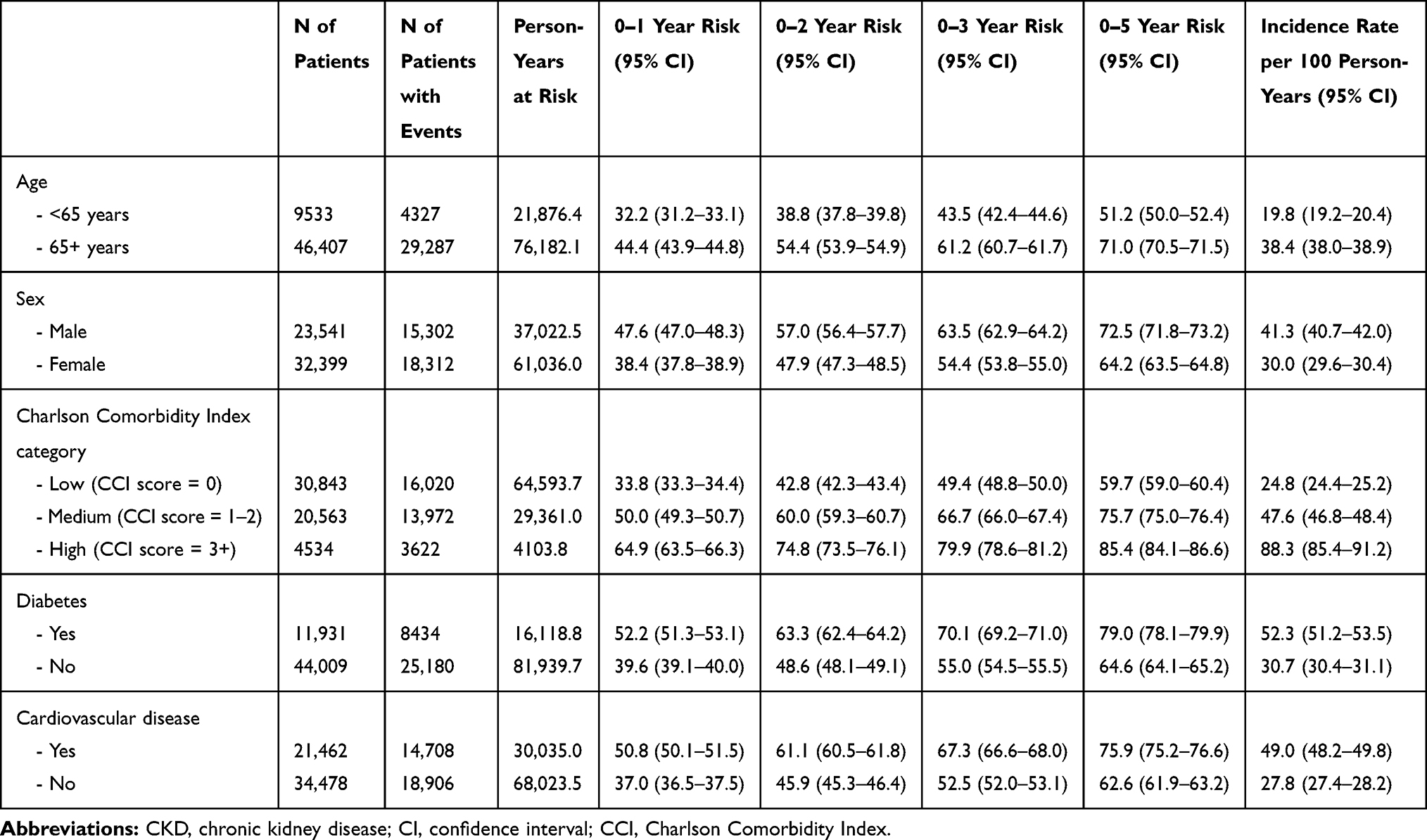 |
Table 3 Risk of Newly Measured Anemia in Patients with Any Newly Identified CKD Stages 3–5, Stratified by Sex, Age, and Comorbidity on the Index Date, Northern Denmark, 2009–2016 |
Across all CKD stages, the risk of experiencing milder anemia was greater than the risk of more severe anemia events. The 1-year risk of moderate (grade 2) anemia ranged between 11.2% (95% CI: 10.9–11.5) in CKD 3a to 63.3% (95% CI: 60.0–66.4) in CKD 5, while 3.1% (95% CI: 3.0–3.3) to 21.8% (95% CI: 19.1–24.6) experienced severe (grade 3) anemia during this timeframe, respectively (Figure 2, Suppl. Table 3). Eight years after newly identified CKD stage 3a, the proportion of patients experiencing severe anemia increased to almost 20% of patients, compared to about 50% of patients with CKD stage 5 (Figure 2). In adjusted analyses using the CKD stage 3a cohort as reference, there was no evidence of a substantial interaction between anemia grade and CKD stage, indicating that progression to higher CKD stages increased the risk of any grade of anemia to similar extent (Suppl. Table 3).
Additional laboratory data on erythrocyte volume or hemoglobin content was available for only few anemia events. Among these, normocytic normochromic anemia was the most common anemia type (Suppl. Table 1 and Suppl. Table 2).
Sensitivity Analyses
Finally, in sensitivity analyses, we described the anemia trajectory beyond the first anemia event, as we continued follow-up for subsequent anemia events for all grades of anemia beyond the first event (see detailed methods and results in Additional file 1). The majority of CKD patients with a recorded Hb measurement retained the same anemia grade in the subsequent year, regardless of whether the index date was defined as the date of newly identified CKD or as the date of the first anemia event (Suppl. Table 4 and Suppl. Figure 2).
Discussion
Key Results
In this Danish population-based study of patients with newly identified CKD stages 3–5, the risk of anemia increased with higher CKD stages. One out of three patients with CKD stage 3a and almost every patient with CKD stage 5 experienced anemia within 1 year after entering their respective CKD stage, while more than one out of 10 patients and nearly two-thirds of patients with newly identified CKD stage 3a and 5, respectively, experienced at least moderate (grade 2) anemia within 1 year. After five years, anemia events had occurred in about two-thirds of patients with newly identified CKD stage 3a as well as in most patients with newly identified CKD stages 3b-5. The highest rate of anemia was observed in CKD patients with male sex, older age, higher comorbidity level, diabetes, and cardiovascular disease.
Limitations
We identified patients with CKD based on the definition as specified in the most recent guideline (the 2012 Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease),17 which include a three month duration criteria for CKD. In addition, to minimize the risk of including patients with two incident events of acute kidney injury, we restricted inclusion to patients with no eGFR measurement above the threshold of their respective CKD stage during the ≥90-day period used to define CKD. This conservative approach, combined with the lack of systematic plasma creatinine screening tests, may have resulted in a delay in identifying CKD patients and their progression, as well as potential misclassification of patients to milder stages of CKD because of one falsely high eGFR measurement. Such misclassification could lead to over- or underestimation of anemia risk in individual CKD stage cohorts, but it would not affect overall anemia risk estimates for the study population. Importantly, we reported the prevalence of anemia at study inclusion.
Also, we did not define CKD stage 5 based on the requirement for chronic dialysis. Therefore, any CKD stage could have included patients in dialysis treatment. However, as few patients (0.00.3%) in the CKD stages 3a-4 cohorts received any dialysis treatment during the 90 days before their CKD index date it was unlikely to noticeably affect our results.
We did not censor patients in a specific CKD stage cohort if they progressed to higher CKD stages during the study period. The reasons were twofold. First, we considered it clinically relevant to ascertain risk of anemia regardless of a future decline in kidney function. Second, we wished to avoid informative censoring, as anemia risk in patients with deteriorating kidney function would likely differ from that in patients with stable kidney function.24
Of note, we identified increased risks of anemia with increasing CKD stage, which potentially could be partly explained by closer monitoring of patients with higher CKD stages because of increased detection rate of especially asymptomatic anemia. However, for patients at every CKD stage, we found comparable HRs for mild anemia (ie, possibly asymptomatic) and for moderate or severe anemia (ie, likely symptomatic), so detection bias is unlikely to explain the increased rate of anemia at higher CKD stages (Suppl. Table 3).
Due to lack of information on specific causes of anemia, such as prior iron deficiency, or repeated phlebotomies in hospitalized patients (potentially causing iatrogenic anemia), we were not able to exclude patients from our cohorts on this basis, which may have contributed to the estimated risks of CKD related anemia in our study. We aimed to describe the clinical course of CKD and did therefore not include data on erythropoietin or other anemia treatment, which may have reduced the risk of severe anemia.
Interpretation
In this study we had access to population-based data with complete follow-up, generated by Denmark’s universal health care and administrative systems, making it possible to examine an unselected study population. We identified both CKD and anemia based on laboratory data from blood samples analyzed in all laboratories in Northern Denmark. The blood samples were drawn by general practitioners, by providers at outpatient clinics, and by hospital staff during visits or admissions. We obtained eGFR measurements both before and after the start of the study period, so our results apply to a well-defined CKD cohort including only patients with newly identified CKD stages 3–5, who were followed starting on their diagnosis date. Furthermore, we excluded patients with confirmed anemia up to 30 days prior to the date of confirmed CKD. This allowed us to focus on newly measured anemia rather than known prevalent anemia, in contrast to previous cross-sectional epidemiologic studies.5–11 These previous studies examined prevalent anemia in patients with prevalent CKD, reporting anemia in 551% of patients with CKD stage 3,5–11 5079% in patients with CKD stage 4,5–11 and 5397% in patients with CKD stage 5.6–11 Anemia risk may vary with duration of CKD. By restricting our analysis to patients with newly identified CKD stage 3–5, we were able to compare patients with similar duration of CKD at a given stage. Also, the detection and management of anemia varies between countries and over time, which may affect the prevalence of recorded anemia in previous studies. Thus, previous findings are difficult to compare with each other and with our findings, and we addressed this issue at least in part by focusing on newly measured anemia events.
Conclusions
Our study showed that a substantial proportion of patients with newly identified or progressed CKD experienced anemia during the first year after CKD diagnosis. Anemia risk increased with higher CKD stage, yet the absolute risk of anemia was high across all CKD stages 3–5. This is of interest to clinicians as they inform patients about the risks associated with CKD, and may contribute to the design of algorithms for the follow up of patients with CKD. Anemia is associated with increased risk of potentially severe complications, and this study underlines the importance for timely and continuous Hb monitoring as part of routine clinical care for all patients with newly identified or progressed CKD stages 3–5.
Data Sharing Statement
Data are available as presented in the paper and in the Appendix. Danish legislation does not allow us to distribute or make patient data directly available to other parties. Interested researchers may apply for data access through the Research Service at the Danish Health Data Authority (e-mail: [email protected]). Up-to-date information on data access is available online (http://sundhedsdatastyrelsen.dk/da/forskerservice). Access to data from the Danish Health Data Authority requires approval from the Danish Data Protection Agency (https://www.datatilsynet.dk/english/the-danish-data-protection-agency/introduction-to-the-danish-data-protection-agency/).
Ethics Approval and Informed Consent
The study was approved by the Danish Data Protection Agency (record number 2015-57-0002, Aarhus University record number 2016-051-000001/812). According to Danish legislation, no approval from an ethics committee or informed consent from patients is required for registry-based studies.
Acknowledgment
We owe a great thank to prof. Henrik Toft Sørensen, MD, PhD, DMSc, for excellent editing consultancy during the finalization of the manuscript.
Disclosure
HvH, GJ and KH are employees of AstraZeneca. SVV, UH, HB, RWT and CFC do not report any personal conflicts of interest relevant to this study. The Department of Clinical Epidemiology is, however, involved in studies with funding from various companies as research grants to (and administered by) Aarhus University, and this study was partly funded by a grant from AstraZeneca to Aarhus University. Heleen van Haalen reports personal fees from AstraZeneca, outside the submitted work. Glen James reports holding shares and receiving salary from AstraZeneca, during the conduct of the study. Katarina Hedman reports being an employee and stockholder of AstraZeneca, during the conduct of the study and outside the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Babitt JL, Lin HY. Mechanisms of Anemia in CKD. J Am Soc Nephrol. 2012;23(10):1631–1634. doi:10.1681/ASN.2011111078
2. Tonelli M, Wiebe N, Culleton B, et al. Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol. 2006;17(7):2034–2047. doi:10.1681/ASN.2005101085
3. Thorp ML, Johnson ES, Yang X, Petrik AF, Platt R, Smith DH. Effect of anaemia on mortality, cardiovascular hospitalizations and end-stage renal disease among patients with chronic kidney disease. Nephrology. 2009;14(2):240–246. doi:10.1111/j.1440-1797.2008.01065.x
4. Stevens LA, Viswanathan G, Weiner DE. Chronic kidney disease and end-stage renal disease in the elderly population: current prevalence, future projections, and clinical significance. Adv Chronic Kidney Dis. 2010;17(4):293–301. doi:10.1053/j.ackd.2010.03.010
5. Astor BC, Muntner P, Levin A, Eustace JA, Coresh J. Association of kidney function with anemia: the third national health and nutrition examination survey (19881994). Arch Intern Med. 2002;162(12):1401–1408. doi:10.1001/archinte.162.12.1401
6. Kohagura K, Tomiyama N, Kinjo K, Takishita S, Iseki K. Prevalence of anemia according to stage of chronic kidney disease in a large screening cohort of Japanese. Clin Exp Nephrol. 2009;13(6):614–620. doi:10.1007/s10157-009-0197-z
7. Ryu SR, Park SK, Jung JY, et al. The prevalence and management of anemia in chronic kidney disease patients: result from the korean cohort study for outcomes in patients with chronic kidney disease (KNOW-CKD). J Korean Med Sci. 2017;32(2):249–256. doi:10.3346/jkms.2017.32.2.249
8. McClellan W, Aronoff SL, Bolton WK, et al. The prevalence of anemia in patients with chronic kidney disease. Curr Med Res Opin. 2004;20(9):1501–1510. doi:10.1185/030079904X2763
9. Stauffer ME, Fan T. Prevalence of anemia in chronic kidney disease in the United States. PLoS One. 2014;9(1):e84943. doi:10.1371/journal.pone.0084943
10. St Peter WL, Guo H, Kabadi S, et al. Prevalence, treatment patterns, and healthcare resource utilization in Medicare and commercially insured non-dialysis-dependent chronic kidney disease patients with and without anemia in the United States. BMC Nephrol. 2018;19(1):67. doi:10.1186/s12882-018-0861-1
11. Li Y, Shi H, Wang WM, et al. Prevalence, awareness, and treatment of anemia in Chinese patients with nondialysis chronic kidney disease: first multicenter, cross-sectional study. Medicine. 2016;95(24):e3872. doi:10.1097/MD.0000000000003872
12. Schmidt M, Pedersen L, Sorensen HT. The danish civil registration system as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
13. Grann AF, Erichsen R, Nielsen AG, Froslev T, Thomsen RW. Existing data sources for clinical epidemiology: the clinical laboratory information system (LABKA) research database at Aarhus University, Denmark. Clin Epidemiol. 2011;3:133–138. doi:10.2147/CLEP.S17901
14. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
15. Pottegard A, Schmidt SAJ, Wallach-Kildemoes H, Sorensen HT, Hallas J, Schmidt M. Data resource profile: the danish national prescription registry. Int J Epidemiol. 2017;46(3):798–798f. doi:10.1093/ije/dyw213
16. Levey AS, Greene T, Kusek JW, Beck GJ. A simplified equation to predict glomerular filtration rate from serum creatinine. J Am Soc Nephrol. 2000;11:155A.
17. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Inter Suppl. 2013;(3):1–150.
18. Beutler E, Waalen J. The definition of anemia: what is the lower limit of normal of the blood hemoglobin concentration? Blood. 2006;107(5):1747–1750. doi:10.1182/blood-2005-07-3046
19. National Cancer Institute NIoH. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. 2017;3. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf. Accessed March 1, 2020
20. Rodgers GM
21. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
22. Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sorensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based danish national registry of patients. BMC Med Res Methodol. 2011;11:83. doi:10.1186/1471-2288-11-83
23. Lin DY, Wei LJ. The robust inference for the cox proportional hazards model. J Am Stat Assoc. 1989;84(408):1074–1078. doi:10.1080/01621459.1989.10478874
24. Hernan MA, Hernandez-Diaz S, Robins JM. A structural approach to selection bias. Epidemiology. 2004;15(5):615–625. doi:10.1097/01.ede.0000135174.63482.43
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.