")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Risk Factors of Recurrent Retinal Detachment Following Surgical Treatment for Rhegmatogenous Retinal Detachment: A Retrospective Study
Authors Jia LY, Sun YX , Zhang YP, Ma K
Received 29 October 2020
Accepted for publication 3 December 2020
Published 30 December 2020 Volume 2020:13 Pages 3165—3171
DOI https://doi.org/10.2147/RMHP.S288777
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Li-Yun Jia, Yan-Xia Sun, Yong-Peng Zhang, Kai Ma
Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Kai Ma
Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Ophthalmology and Visual Sciences Key Laboratory, Beijing 100730, People’s Republic of China
Tel/Fax +86 1058269508
Email [email protected]
Objective: To identify potential risk factors for recurrent retinal detachment after surgical treatment for rhegmatogenous retinal detachment with choroidal detachment (RRD-CD) in a Chinese population.
Methods: A total of 1212 patients with RRD-CD admitted to Beijing Tongren Hospital from 2004 to 2018 were reviewed retrospectively. The rate of recurrent retinal detachment was calculated, and risk factors were analyzed by logistic regression analysis.
Results: The average age of the patients was 48.51 years, 760 patients (62.7%) were male, and 630 patients (52.0%) had right eye disease. The recurrence rate in the same eye was 21.3%. The incidence of recurrence retinal detachment was higher in patients who were male, middle age, and with poor preoperative vision, longer axial length, and scleral buckling. Recurrence usually occurred 3 months after surgery.
Conclusion: Male, middle age, longer axial length, and scleral buckling could be risk factors for recurrent retinal detachment following surgical treatment in patients with RRD-CD.
Keywords: rhegmatogenous retinal detachment, choroidal detachment, risk factor
Introduction
Rhegmatogenous retinal detachment associated with choroidal detachment (RRD-CD) is due to ciliary and choroidal body detachment and characterized by quick progression and poor prognosis.1 RRD-CD accounts for 7.6–18.7% of RRD patients in China, significantly higher than the rate in Western countries (2.0–4.5%).2–4 RRD-CD is commonly associated with the breakdown of the blood ocular barrier, the migration of retinal epithelium, the release of inflammatory factors, and the development of proliferative vitreoretinopathy (PVR).5–7
Surgical treatment remains the mainstay for RRD-CD management, but surgical procedures are complex, and CD is considered an unfavorable factor for RRD surgery due to high incidence of postoperative PVR.8 Despite improved surgery strategies for detachment repair for RRD-CD, the recurrence rate of retinal detachment is still high. Therefore, it is important to identify risk factors for the failure of retinal detachment repair to improve the prognosis of RRD-CD.
This study aimed to identify potential risk factors for recurrent retinal detachment after surgical treatment for RRD-CD in a Chinese population. We retrospectively analyzed the clinical characteristics of RRD-CD in our hospital in the past 15 years, especially clinical characteristics of RRD-CD patients with recurrent retinal detachment after the first operation.
Methods
Data Collection
This study was approved by the Ethics Committee of Beijing Tongren Hospital, Capital Medical University in compliance with the principles of the Declaration of Helsinki. All patients provided informed consent. All electronic case records from January 2004 to December 2018 in the Department of Ophthalmology of Beijing Tongren Hospital were integrated to establish a database. The database was searched for all medical records with the first diagnosis of RRD-CD. If the patient had multiple medical records of recurrent RRD or contralateral eye surgery, it was considered a case record. Inclusion criteria: RRD-CD was diagnosed and the first surgery was performed in our hospital. The exclusion criteria were as follows: retinal reattachment was performed more than once in other hospitals; no retinal hole was found in exudative retinal detachment, tractive retinal detachment, or combined retinal detachment. The information on patient demographics, including age, gender, RRD-CD duration, and co-existing diseases such as diabetes and hypertension, and the details on ophthalmic examinations, including intraocular pressure (IOP), best-corrected visual acuity (BCVA), anterior segment evaluation, funduscope examination, ocular ultrasonography, and ultrasonic biomicroscopy, were collected from medical records. Data analysis was based on different age groups: younger than 18 years old, 18–39 years old, and every 20 years for the rest of the age groups.
The types of surgical procedures included pars plana vitrectomy (PPV), scleral buckling (SB), PPV with an encircling band, and types of vitreous substitutes.
Statistical Analysis
Statistical analysis was performed using SPSS 17.0 software (SPSS, Chicago, IL, USA). Continuous data were shown as mean and standard deviation (SD), and categorical data were shown as counts and proportions. The comparison was performed by chi-square test. A multivariate analysis with a step-by-step logistic regression was performed to identify risk factors for recurrent retinal detachment after surgery. A 2-tailed P<0.05 indicated significance.
Results
According to inclusion and exclusion criteria, 1212 patients with RRD-CD were collected. All patients had severe choroidal detachment and their average age was 48.51 years, ranging from 2 to 87 years. The 40–59 age group accounted for 42.8% (516 cases; Figure 1). A total of 760 patients were male (62.7%) and 630 patients had right eye disease (52.0%).
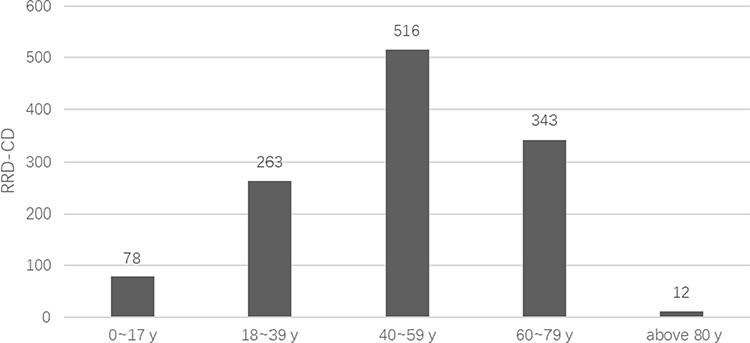 |
Figure 1 Age distribution of RRD-CD patients. RRD-CD, rhegmatogenous retinal detachment with choroidal detachment. |
Table 1 shows patient demographics and clinical parameters. Disease onset varied from 3 days to 2 years, and BCVA varied from no light perception (NLP) to 0.7, and 35.4% was hand movement (HM). IOP values of 0–6 mmHg were found in 513 eyes (42.33%), 7–10 mmHg in 504 eyes (41.58%), 11–15 mmHg in 144 eyes (11.88%), 16–21 mmHg in 40 eyes (3.30%), and over 21 mmHg in 11 eyes (0.91%). Myopia accounted for 92.6% with axial length (AL)>26 mm (Figure 2). Pseudophakic/aphakic accounted for about 28.4% (pseudophakic was 21.0%, aphakic eye was 7.3%), with macular detachment in 94.7%. Preoperative regular fundus examination and postoperative diagnosis showed that 503 eyes (41.5%) had multiple holes (>2), 104 eyes (8.58%) had great retinal tears (GRT), and 205 eyes (16.91%) had macular holes.
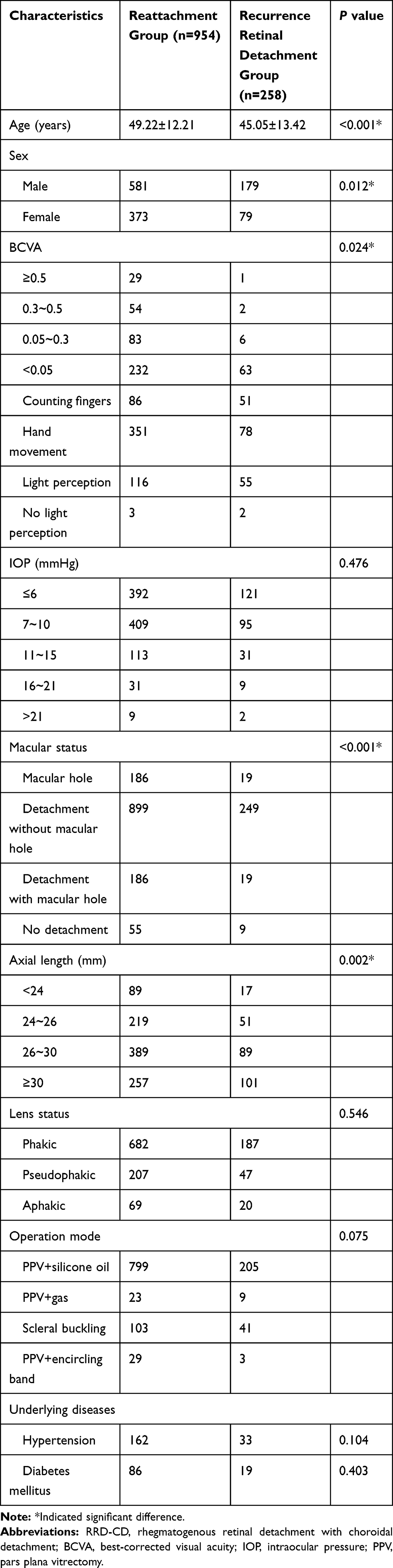 |
Table 1 Characteristics for RRD-CD in the Two Groups |
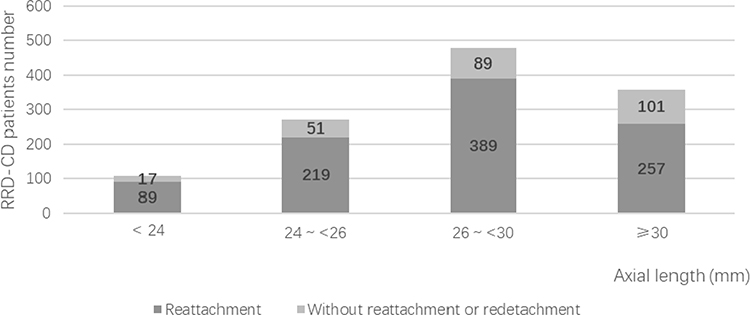 |
Figure 2 Axial length distribution of RRD-CD patients. RRD-CD, rhegmatogenous retinal detachment with choroidal detachment. |
Among RRD-CD patients, 85.5% underwent PPV, filling with either silicone oil (82.8%) or gas (2.6%); 11.9% underwent SB, and 2.6% underwent PPV (silicone oil) combined with encircling band.
Among RRD-CD patients, 258 patients had no total retinal reattachment or retinal redetachment after the first operation, accounting for 21.3% of RRD-CD patients. All RRD-CD patients received oral administration of prednisolone acetate 3 to 7 days before the operation. The average age of those patients was 45.05 years, and the male proportion was 69.3%. We found significant differences in age, gender, BCVA, AL, and macular status between the two groups (Tables 1 and 2).
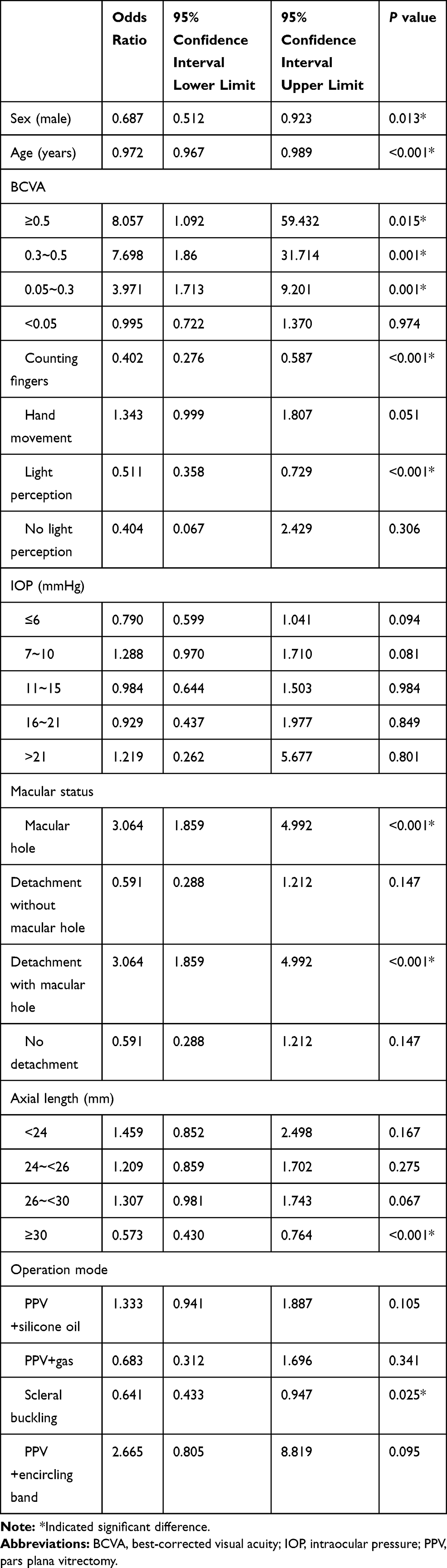 |
Table 2 Univariate Analysis of Risk Factors for Recurrence Retinal Detachment After the First Operation |
Multivariate logistic regression analyses showed significant differences in male, age, BCVA, AL, macular hole with detachment, and scleral buckling (Table 3). The incidence of retinal redetachment was significantly lower (P<0.001) in patients with lower AL (AL<26 mm) than in patients with longer AL (AL≥26 mm), was significantly higher (P=0.011) in patients with poor BCVA (<0.05) than in patients with BCVA, and was significantly lower (P<0.001) in patients with retinal reattachment than in patients with macular hole with detachment. Regarding the first operation mode, the incidence of recurrence retinal redetachment in RRD-CD patients undergoing SB was significantly higher than that in PPV (P=0.031). 74.62% of the patients had recurrent retinal redetachment within 3 months after the first operation, 84.3% of the patients had recurrent retinal redetachment within 6 months after the first operation, and 92.3% of the patients had recurrent retinal redetachment within 12 months after the first operation.
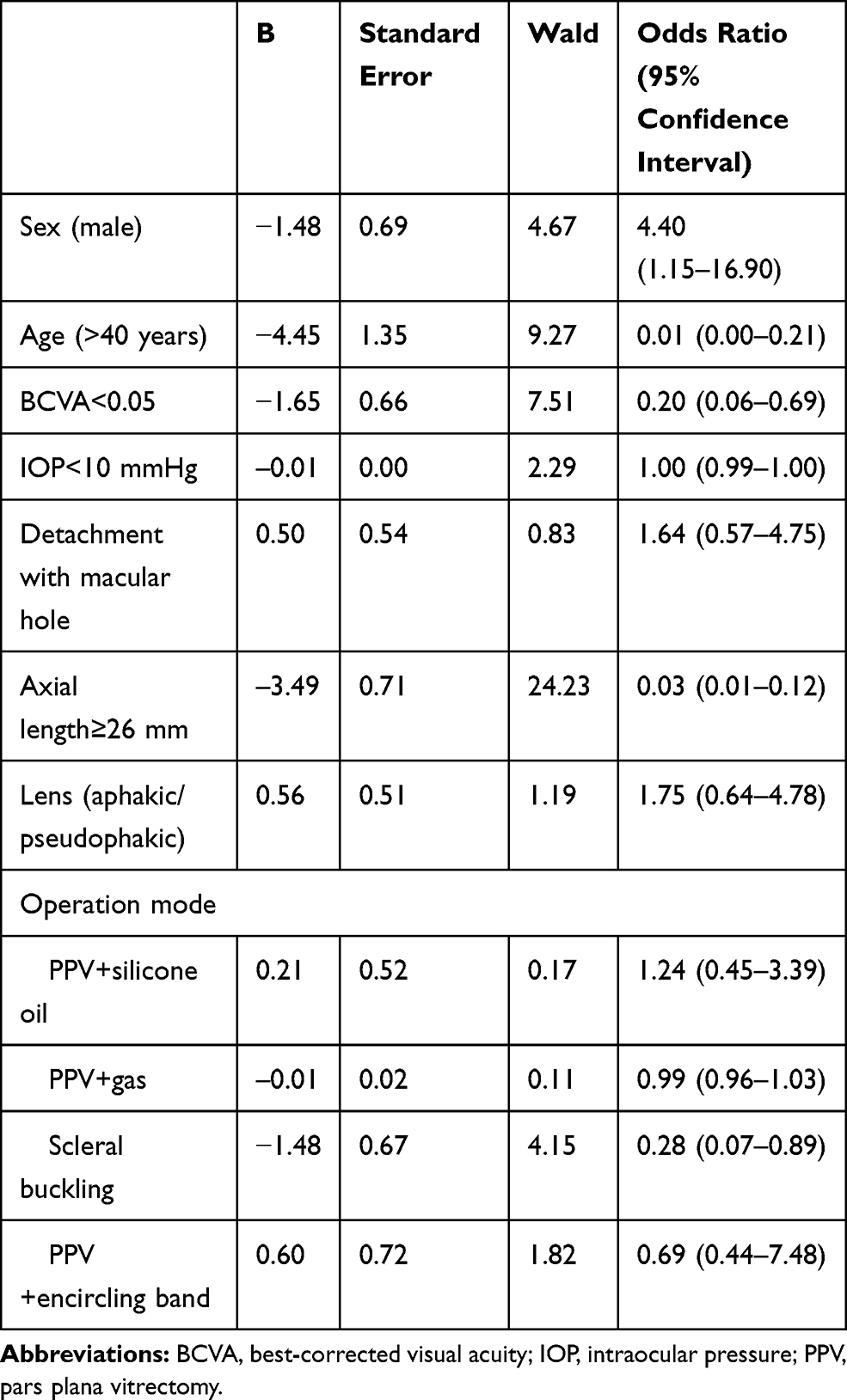 |
Table 3 Multivariate Logistic Regression Analysis of Risk Factors for Recurrence Retinal Detachment |
Discussion
RRD-CD is an unusual severe type of rhegmatogenous retinal detachment, and the prognosis is poor due to rapid onset of massive vitreous and peri-retinal proliferation.1
Up to 10% of RRD cases require additional interventions to repair recurrent detachment, and remain a significant challenge for vitreoretinal surgeons and the patients.9 Despite recent developments in microincision vitrectomy system, perfluorocarbon liquids, and intraocular tamponades for the managing of RRD-CD, we need to identify risk factors for RRD-CD to improve the prognosis of RRD-CD.
In the present study, we analyzed clinical features of RRD-CD patients, and focused on risk factors of recurrent retinal detachment, which is helpful to screen high-risk populations of RRD-CD and reduce the blindness rate of the disease. Based on the analysis of 15-year data, we found that the rate of RRD-CD was higher in males than in females, but was not different between left and right eyes. Yu et al reported that although the proportion of males was higher than that of females, the proportion of males was only 53%, lower than that of males in our study.3 However, in the study by Denwattana et al, the proportion of males was as high as 78%, higher than the rate in our study.10
In the present study, the average age of the patients was 48.51 years. The 40–59 age group accounted for 42.8% (516 cases; Figure 1). It is known that retinal detachment is more common in people over 50 years old, and 66% of RRD-CD patients were older than 50 years and the rate of RRD-CD in the 50–59 year old age group was the highest.11 We think that the differences in the age in different studies were due to geographical and ethnic differences, and different sample size.
In the present study, myopia accounted for 92.6% (high myopia: AL>26 mm about 69.0%) and the incidence of RRD-CD increased with AL, consistent with previous studies.3,4,11 We found that approximately 42.33% of patients with RRD-CD presented with IOP of 0–6 mmHg and more than 83% of patients had IOP lower than 10 mmHg. The current standard for low IOP in RRD-CD patients is 4 mmHg. However, more than 15% of patients had normal IOP. Therefore, hypotension is an important but not necessary indication in RRD-CD diagnosis.
Approximately 28.3% of patients with RRD-CD in our study had cataract surgery history, 20.96% of them had intraocular lens, and 7.34% had aphakia. The proportion of pseudophakic reported by Denwattana et al was higher than that of this study (46.05%), but the proportion of aphakic eyes was similar to our study.10 The proportion of pseudophakic/aphakic reported by Yu et al was lower than that reported in this study (10.95%).4 We presumed that this discrepancy might be due to the differences in the time to visit from the onset of symptoms.
The success rate of surgery for RRD-CD is less than 70%, far less than the rate for RRD patients without CD.11–13 In this study, the rate of RRD-CD patients with total retinal reattachment 3 months after surgery and without retinal redetachment 1 year after surgery was 78.71%, higher than the rate reported previously.11,12 Because this study excluded patients who had a recurrence after the first operation in other hospitals and the success of RRD-CD therapy has been improved with the vitrectomy technique, this may be the reason why the recurrence rate is lower than that of other studies.
In the present study, we found that SB was the preferred operation at the beginning of the study period, but PPV gained more attention later. The majority of retinal redetachment occurred within the first 3 months. Among 1004 patients operated with PPV with oil, 205 cases (20.4%) subsequently underwent redetachment surgery, while among 144 patients operated with SB, 41 cases (28.5%) subsequently underwent redetachment surgery. Therefore, scleral buckling is an important risk factor for recurrence. The retinal reattachment rate of vitreous surgery in RRD-CD patients is high, and the recurrence rate is lower than that of scleral buckling.14 Therefore, we think that SB may lead to complications, which increase the rate of recurrence retinal detachment.
We found that risk factors for recurrence retinal detachment after first surgery included male, middle age, and high myopia. The average age of the recurrence group was 45.05±13.42 years, significantly less than that of the non-recurrence group. In previous studies, most patients were old.3–5 The difference in age may lead to different outcomes. Notably, we found that the rate of recurrence of retinal detachment was significantly higher in males than in females. The differences in the anatomy of the eye and vitreous between males and females may explain the increased risk of recurrence retinal detachment in males. Males have longer axial length while females tend toward early posterior vitreous detachment, which may confer protection for recurrence retinal detachment.15
In the present study, the proportion of aphakic eyes was higher in the recurrent group than in the non-recurrence group, but the difference was not statistically significant, consistent with a previous study showing that macular hole was a risk factor for RRD-CD.16 However, in our study the proportion of RRD-CD patents with macular detachment and hole was significantly lower in the recurrent group than in the non-recurrence group. Any retinal detachment causes the alterations in retinal microstructure.17,18 Therefore, reducing the risk of redetachment helps recover visual acuity of the patients.
This study has several limitations. While we focused on the risk factors of recurrent retinal detachment after first surgery, the redetachment was not operated in a minor part of the patients because they refused the surgery due to financial difficulty or risk management; this may cause a bias for the inclusion of patients for final analysis. Another limitation is that we did not analyze the location, shape, and number of retinal breaks due to the lack of sufficient data from each patient, and could not analyze the classification of PVD.
In conclusion, this retrospective study showed that the risk factors of recurrent retinal detachment after first surgery for patients with RRD-CD were male, middle age, poor preoperative vision, and longer axial length patients with RRD-CD. Scleral buckling was an independent risk factor for retinal redetachment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Seelenfreund MH, Kraushar MF, Schepens CL, Freilich DB. Choroidal detachment associated with primary retinal detachment. Arch Ophthalmol. 1974;91:254–258.
2. Li Z, Li Y, Huang X, et al. Quantitative analysis of rhegmatogenous retinal detachment associated with choroidal detachment in Chinese using UBM. Retina. 2012;32(10):2020–2025.
3. Yu Y, An M, Mo B, Yang Z, Liu W. Risk factors for choroidal detachment following rhegmatogenous retinal detachment in a Chinese population. BMC Ophthalmol. 2016;16:140.
4. Gottlieb F. Combined choroidal and retinal detachment. Arch Ophthalmol. 1972;88:481–486.
5. Sharma T, Challa JK, Ravishankar KV, Murugesan R. Scleral buckling for retinal detachment. Predictors for anatomic failure. Retina. 1994;14(4):338–343.
6. Campochiaro PA, Jerdan JA, Glaser BM. Serum contains chemoattractants for human retinal pigment epithelial cells. Arch Ophthalmol. 1984;102:1830–1833.
7. Dai Y, Wu Z, Sheng H, Zhang Z, Yu M, Zhang Q. Identification of inflammatory mediators in patients with rhegmatogenous retinal detachment associated with choroidal detachment. Mol Vis. 2015;21:417–427.
8. Adelman RA, Parnes AJ, Michalewska Z, Ducournau D. European Vitreo-Retinal Society Retinal Detachment Study G. Clinical variables associated with failure of retinal detachment repair: the European vitreo-retinal society retinal detachment study report number 4. Ophthalmology. 2014;121:1715–1719.
9. Nagpal M, Chaudhary P, Wachasundar S, Eltayib A, Raihan A. Management of recurrent rhegmatogenous retinal detachment. Indian J Ophthalmol. 2018;66:1763–1771.
10. Denwattana A, Prakhunhungsit S, Thoongsuwan S, et al. Surgical outcomes of preoperative steroid for rhegmatogenous retinal detachment with associated choroidal detachment. Eye. 32:602–607.
11. Jarrett WH. Rhegmatogenous retinal detachment complicated by server intraocular inflammation, hypotony, and choroidal detachment. Trans Am Ophthalmol Soc. 1981;79:664–683.
12. Ghoraba HH. Primary vitrectomy for the management of rhegmatogenous retinal detachment associated with choroidal detachment. Graefes Arch Clin Exp Ophthalmol. 2001;239:733–736.
13. Gui JM, Jia L, Liu L, Liu JD. Vitrectomy, lensectomy and silicone oil tamponade in the management of retinal detachment associated with choroidal detachment. Int J Ophthalmol. 2013;6(3):337–341.
14. Sari S, Raimo T, Jari H, et al. A retrospective study comparing outcomes of primary rhegmatogenous retinal detachment repair by scleral buckling and pars plana vitrectomy in Finland. Clin Ophthalmol. 2017;11:503–509.
15. Fotedar R, Wang JJ, Burlutsky G, et al. Distribution of axial length and ocular biometry measured using partial coherence laser interferometry (IOL Master) in an older white population. Ophthalmology. 2010;117(3):417–423.
16. Kang JH, Park KA, Shin WJ, Kang SW. Macular hole as a risk factor of choroidal detachment in rhegmatogenous retinal detachment. Korean J Ophthalmol. 2008;22(2):100–103.
17. Ghazi NG, Green WR. Pathology and pathogenesis of retinal detachment. Eye. 2002;16(4):411–421.
18. Abouzeid H, Wolfensberger TJ. Macular recovery after retinal detachment. Acta Ophthalmol Scand. 2009;84(5):597–605.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.