")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Risk Factors of Perinatal Asphyxia Among Newborns Delivered at Public Hospitals in Addis Ababa, Ethiopia: Case–Control Study
Authors Mulugeta T , Sebsibe G, Fenta FA, Sibhat M
Received 1 May 2020
Accepted for publication 9 August 2020
Published 25 August 2020 Volume 2020:11 Pages 297—306
DOI https://doi.org/10.2147/PHMT.S260788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Tewodros Mulugeta,1 Girum Sebsibe,2 Fikirtemariam Abebe Fenta,2 Migbar Sibhat1
1Department of Nursing, College of Health Science and Medicine, Dilla University, Dilla, Ethiopia; 2School of Nursing and Midwifery, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Tewodros Mulugeta
Department of Nursing, College of Health Science and Medicine, Dilla University, Dilla, Ethiopia
Email [email protected]
Background: Perinatal asphyxia determines the newborn’s future health status and viability with risk factors yet to be completely understood. It measures the status of the healthcare delivery of an organization including antenatal, intranatal, and postnatal care. In Ethiopia, 31.6% of neonatal mortality was attributed to perinatal asphyxia. This study aimed to assess the risk factors of perinatal asphyxia.
Methods: An unmatched case–control study was conducted on 213 (71 cases selected using lottery method and 142 controls systematically) subjects in Addis Ababa from November 1, 2018 to June 30, 2019. Data were collected using a structured questionnaire through face-to-face interviews, entered to Epi data version 4.4, and exported to SPSS version 25 for analysis. Logistic regression was used for analysis. Variables with p< 0.25 in bivariate analysis were taken to multivariable analysis. Statistical significance was declared at P< 0.05 and findings were presented using texts and tables.
Results: A total of 210 newborns (70 cases and 140 controls) and their mothers were included with an overall response rate of 98.5%. Antepartum hemorrhage [AOR=7.17; 95% CI 1.73– 29.72], low birth weight [AOR=2.87; 95% CI 1.01– 8.13], preterm birth [AOR=3.4; 95% CI 1.04– 11.16], caesarean section delivery [AOR=2.75; 95% CI 1.01– 7.42], instrumental delivery [AOR=4.88; 95% CI 1.35– 17.61], fetal distress [AOR=4.77; 95% CI 1.52– 14.92] and meconium-stained amniotic fluid [AOR=9.02; 95% CI 2.96– 30.24] were significantly associated with perinatal asphyxia. Hence, efforts ought to go to improve the quality of antenatal and intra-natal services.
Keywords: asphyxia, newborn, risk factors, Ethiopia, perinatal
Background
Globally, perinatal asphyxia is still one of the leading causes of neonatal mortality and morbidity,1 especially in the first week of life in low and middle-income countries (LMIC).2 It accounts for 28% of the neonatal deaths each year around the world,2,3 and about 29% of early neonatal deaths.4 In developing countries, the prevalence of birth asphyxia is much higher, ranging from 5.1–30.5% with 40% or higher case fatality rates.5,6 In Sub-Saharan Africa, around 338,000 under-five death occur due to birth asphyxia.2
Perinatal asphyxia is the failure of a newborn to initiate and maintain breathing immediately at birth7 which could result in decreased perfusion, ischemia, and organ failure.8 It can be associated with antenatal, intra-natal, and fetal factors.9 Birth asphyxia is diagnosed with APGAR level less than 7 at 5 minutes by the two levels.10 Worldwide, 5–10% of babies require simple stimulation at birth, 3–6% need a bag and mask ventilation, and <1% breath with endotracheal intubation, chest compression, and drugs each year.11
In low-resource settings access to sufficient intrapartum care is inadequate and mortality and long-term damage from intrapartum related neonatal events are highest.11,12 Perinatal asphyxia leads to numerous short and long term complications13 such as HIE14−16, post-traumatic stress disorders (PTSD),17 low cognitive functions,18,19 multi-organ failure,20 and neurological sequel.19,21,22
The sustainable development goal (SDG) sated a plan to keep NMR to at least as low as 12 deaths per 1000 live births and under-five mortality to at least as low as 25 deaths per 1000 live births by 2030 in all countries.23 This could be achieved through better prevention and treatment of the three leading causes, preterm births, severe infections, and perinatal asphyxia as the key.24 Despite different efforts undertaken including focused antenatal care, neonatal mortality remains unacceptably high.25
In Ethiopia, perinatal asphyxia continued as a major cause of under-five mortality and morbidity. In 2015, 31.6% of neonatal deaths were attributed to perinatal asphyxia26 and the prevalence varied from region to region or in different settings ranging from 3.1–32.9%.27,28 Even though researches conducted in the country, reports from different studies that assess risk factors of perinatal asphyxia were inconsistent and contradicting.29−31 This emphasizes the need for further exploration to put the country figure. Furthermore, we could not found a study conducted in Addis Ababa regarding this topic. Thus, this study intended to identify the determinants of perinatal asphyxia among newborns delivered at public hospitals in Addis Ababa.
Materials and Methods
An unmatched case–control study was carried out in public hospitals of Addis Ababa Ethiopia from November 1, 2018 to June 30, 2019. There are twelve governmental hospitals in Addis Ababa. Among those, the study was conducted in four randomly selected hospitals (Yekatit 12 hospital, Tirunesh Beijing hospital, St. Petros hospital, and Gandhi memorial hospital) which accommodate more than 23,000 deliveries annually.
Study Population
Cases
All asphyxiated newborns with APGAR scores of <7 at 5 minutes delivered after 28 weeks of gestation in selected public hospitals of Addis Ababa during the study period.
Controls
All newborns delivered after viability with APGAR scores of ≥7 at 5 minutes in selected public hospitals of Addis Ababa during the study period. In the case of twin or triple newborns, one was taken randomly and babies with congenital malformations were excluded from the study.
Sample Size Determinations and Procedure
The sample size was determined using Epi-Info version 7.2 by using instrumental delivery as a determinant variable from previous study31 which yields the maximum sample size by considering 95% level of confidence, power of 80%, OR 3.5, 9.2% proportion of controls, and 1:2 case to control ratio. Finally, by adding 10% non-response rate the total sample size was 213 with 71 cases and 142 controls that were proportionally allocated to each selected hospital with their respective previous 3 months delivery report (Yekatit 12 hospital= 45, Tirunesh Beijing hospital=48, St. Petros hospital=42 and Gandhi memorial hospital=78). Then cases were selected using simple random sampling technique and controls were selected systematically by including every 15 newborns that were obtained by dividing the total estimated number of non-asphyxiated newborns in previous reports from each hospital to the required number of controls to the study.
Operational Definition
Perinatal asphyxia was diagnosed when a newborn with any of the signs of impaired breathing (not breathing or not crying, gasping, and < 30 breaths per minute) at birth with an APGAR score less than 7 at 5 minutes.9,10 Prolonged labor is the labor exceeding 12 hours in primigravida or 8 hours in multipara mothers after the latent phase of the first stage of labor. Premature rupture of membranes (PROM) is the rupture of the membrane of the amniotic sac and chorion that occur >1 hour before the onset of labor. Low birth weight when birth weight is <2500 gm and normal birth weight if ≥2500.
Data Collection Procedures
The data collection tool was adapted from the previous study done at the Tigray region.29 Data were collected using a structured pretested questionnaire by face-to-face interviews. The questionnaire comprised of maternal socio-demographic, antepartum, intrapartum, and neonatal related factors. Maternal height and MUAC were measured during data collection. The data collection was conducted from March 1 to April 30, 2019.
Data Quality Control
English version questionnaire was prepared, translated to Amharic, and converted back to English for consistency. One week before the data collection, the questionnaire was pre-tested on 5% (12 newborns) of the samples taken from Zewditu memorial hospital (4 Cases and 8 controls). One day training was given for 8 data collectors (BSc midwives) and 2 supervisors (MSc students). Data were evaluated and crosschecked for completeness daily.
Data Processing and Analysis
Data were cleaned, coded, and entered using Epi data version 4.4 and it was exported to SPSS version 25 for analysis. Cross-tabulation was done for the exploration of the data, to clear missing values, and to determine the number of expected events per cell. Binary logistic regression was used for the analysis of the data. Multi-collinearity was checked using variance inflation factor and model fitness was checked using Hosmer and Lemeshow test (p=0.223). Variables with p-values < 0.25 in the bi-variable analysis were identified and fitted to the final model to identify the independent effects of each variable to the outcome variable. An Adjusted Odds Ratio with 95% confidence intervals (CI) was computed to identify the presence and strength of associations, and statistical significance will be declared at p <0.05. Finally, the result was presented in the form of text, table, and graph.
Ethical Consideration
Ethical clearance was obtained from Addis Ababa University, College of Health Science institutional review board. Then officials at different levels of the selected hospitals had been communicated through cooperation letter written from the School of Nursing and Midwifery. The study was conducted per the declaration of Helsinki. The responsible bodies at each postnatal ward and mothers of neonates were informed about the purpose of the study. Written informed consent was obtained from mothers of newborns to confirm willingness. They were notified that they have the right to refuse or terminate the interview at any time. Confidentiality of the information was secured throughout the study process.
Results
Two hundred ten participants (70 cases and 140 controls) who delivered at public hospitals in Addis Ababa with their mothers were included with an overall response rate of 98.59%.
Socio-Demographic Characteristics
The median age of the mothers of newborns was 27 years, 25% of which were below the age of 23 years. Concerning the marital status of the mothers, 65 (92.9%) of cases and 126 (90%) of controls were married. Ten percent of the asphyxiated neonates were born from mothers who reside in rural areas and 50% of newborns from the asphyxiated group were delivered from mothers who had never attended above grade eight. Among those who diagnosed with perinatal asphyxia, 50% were born from unemployed mothers. Regarding the height of the mother, mothers with short stature (<153) were higher in proportion among cases 9 (12.9%) than controls 11 (7.9%). Five (7.1%) of the asphyxiated neonates and 14 (10%) of controls were born from unmarried women (Table 1).
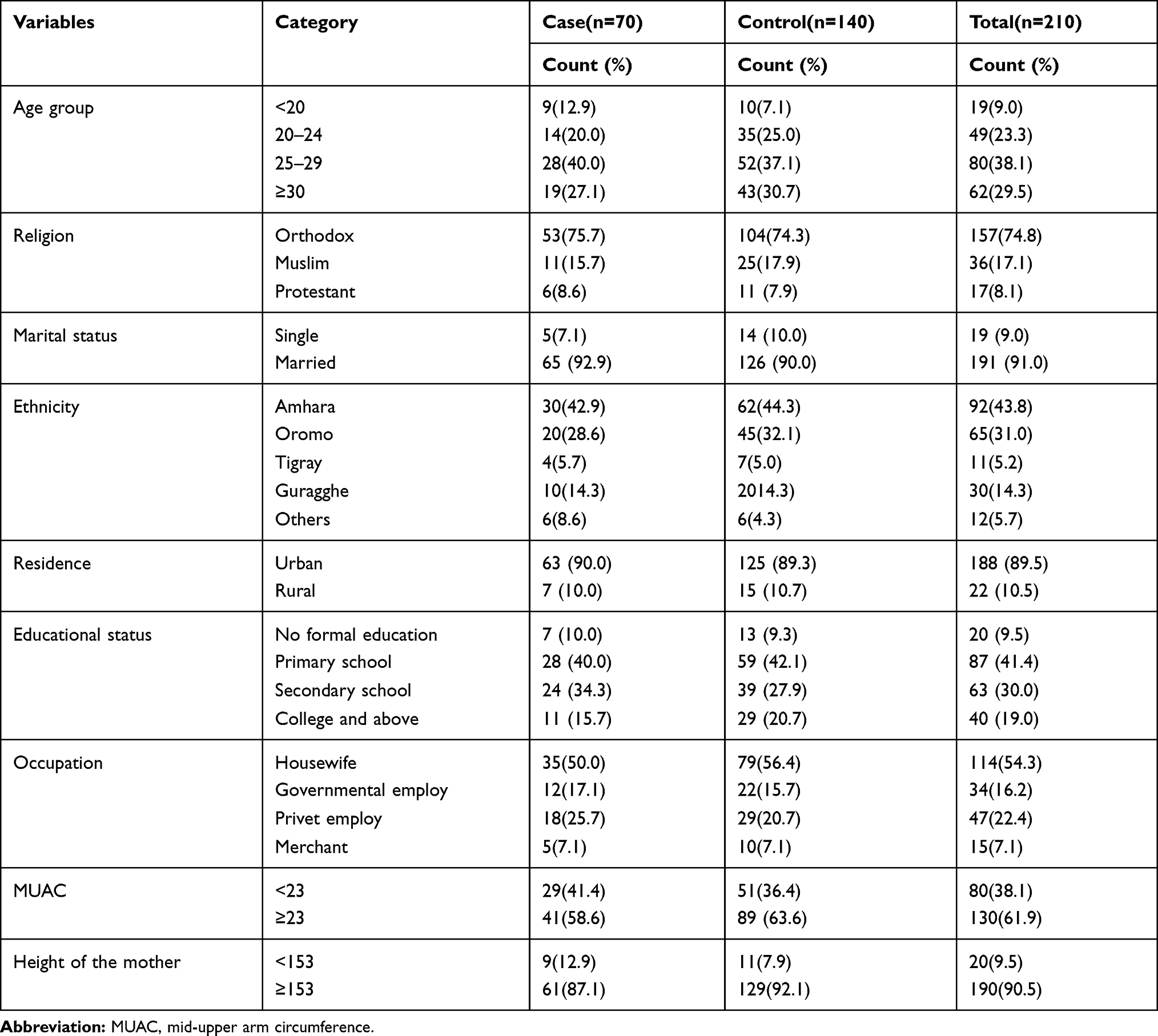 |
Table 1 Distribution of Socio-Demographic Characteristics of the Mothers Among Newborns Delivered at Selected Public Hospitals in Addis Ababa, Ethiopia, 2019 (N = 210) |
Antepartum-Related Characteristics
The finding showed that 20 (28.6%) mothers of cases and 26 (18.6%) of controls did never have ANC service during their pregnancy of the current neonate. Of those having ANC follow-up, only mothers of 16% of the cases and 19.3% of controls followed at hospitals. The proportion of women who got <four ANC visits and with pregnancy-induced hypertension was higher among cases 25 (50%) and 9 (12.9%) than controls 35 (30.7%) and 10 (7.1%) respectively. The proportion of maternal antepartum hemorrhage was also seven times higher among cases 15 (21.4%) than in controls 5 (3.6%). Only two babies (1 asphyxiated and 1 without asphyxia) were born from seropositive mothers (Table 2).
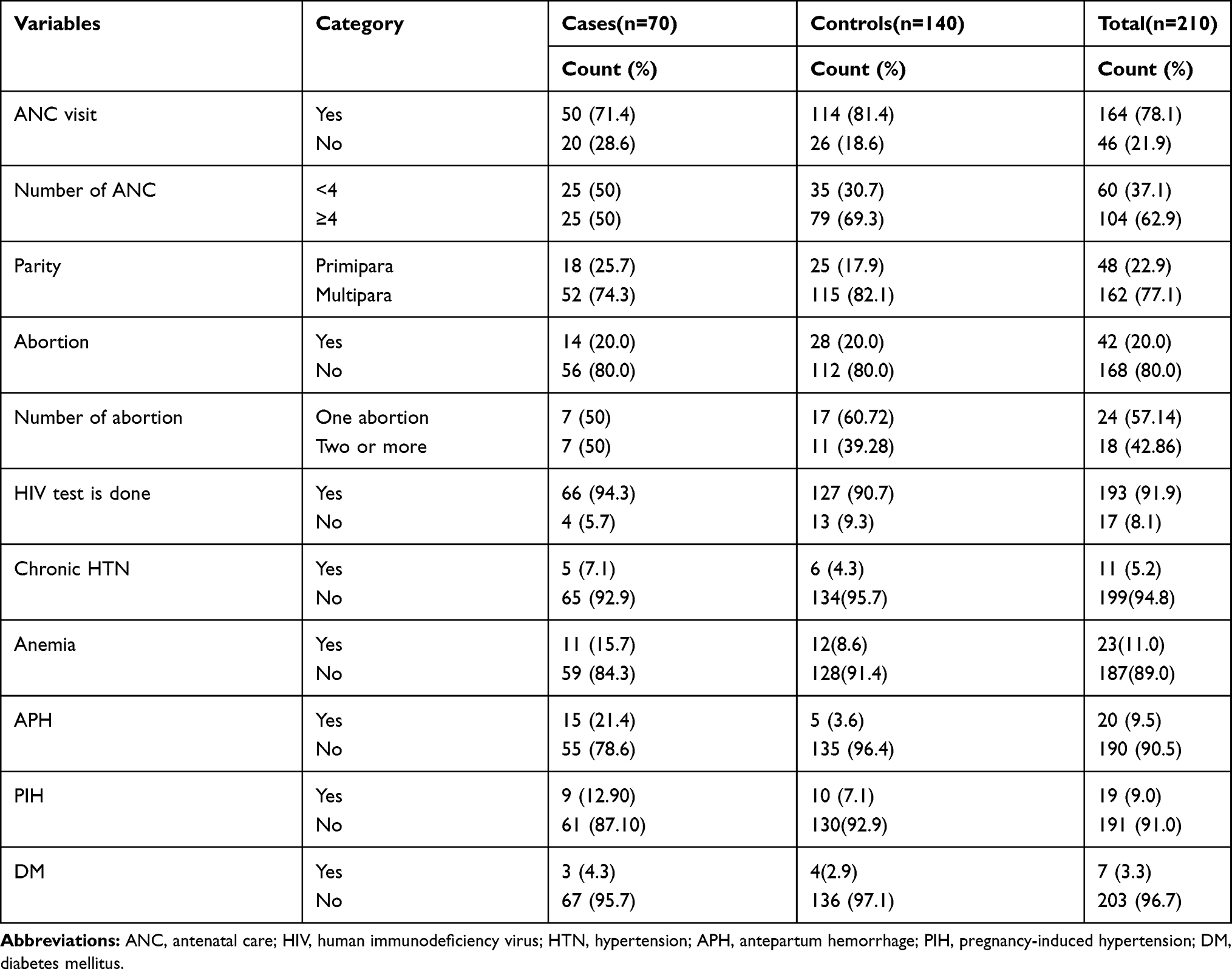 |
Table 2 Antepartum Related Characteristics of Mothers of Newborns Delivered at Selected Public Hospitals in Addis Ababa, Ethiopia, 2019 (N=210) |
Intrapartum Related Risk Factors
The proportion of non-vertex presentation among cases 17 (24.3%) was more than 3 folds to controls 10 (7.1%). General anesthesia was used for 33% of mothers of cases and 13% of controls. Moreover, the proportion of newborns delivered through cesarean section and by instruments was higher in cases 27 (38.6%) and 10 (14.3%) than controls 23 (16.4%) and 8 (5.7%) respectively. Maternal hypotension was recorded among mothers of 24.3% of the cases and 12.9% of the controls. Twenty-five (35.7%) of the cases were delivered after induction and it was applied only for 17.9% among the controls. Only one asphyxiated neonate and 3 non-asphyxiated neonates were born with polyhydramnios (Table 3).
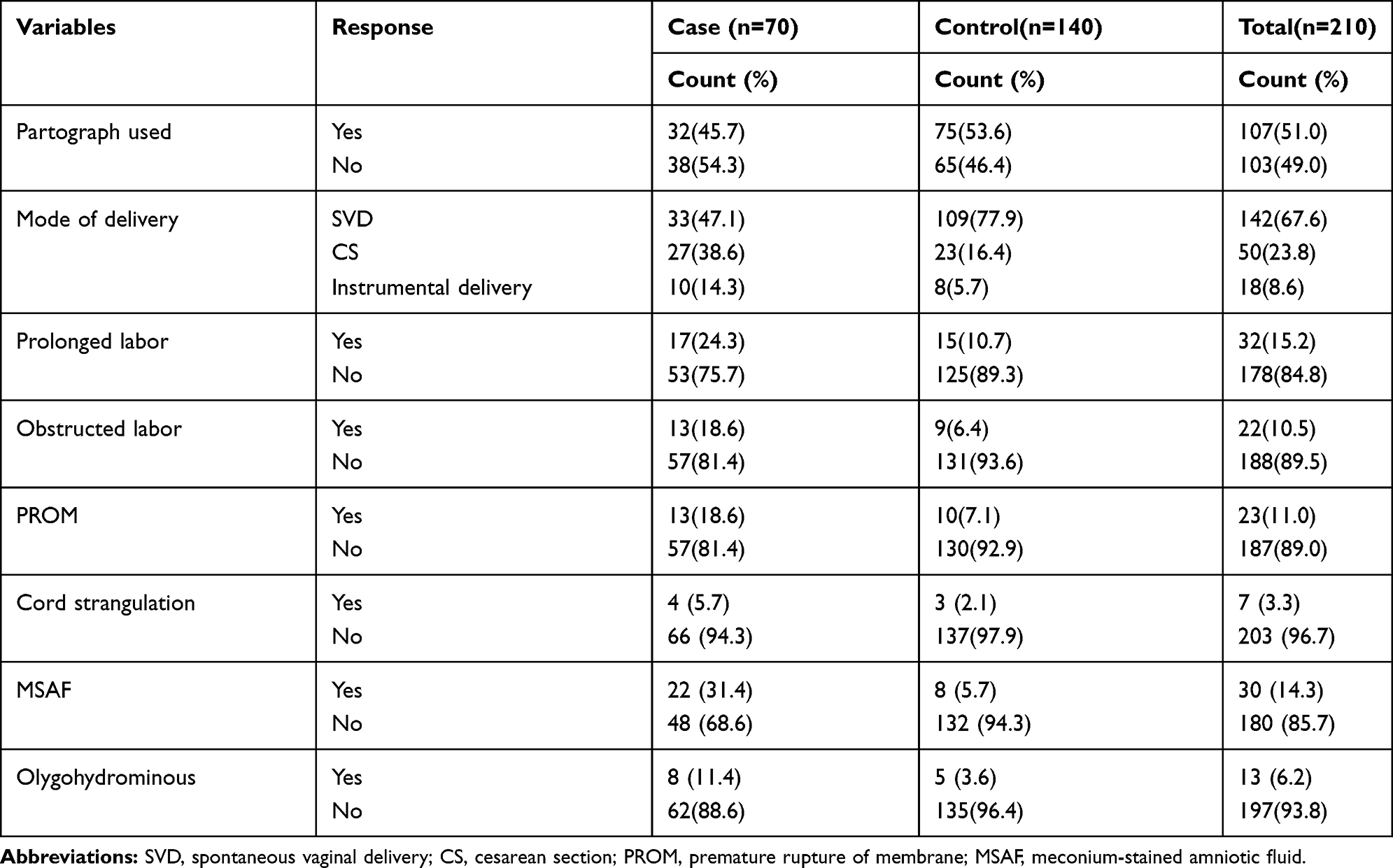 |
Table 3 Distribution of Intrapartum Related Characteristics Among Newborns Delivered at Selected Public Hospitals in Addis Ababa, Ethiopia, 2019 (N = 210) |
Neonatal-Related Factors
More than half (51.4%) of the participants were females. Males were relatively higher in proportion among cases 37 (52.9%) than controls 65 (46.4%). Regarding birth weight, the proportion of low birth weight and prematurity among cases was greater than four times to controls. Additionally, 28.6% of asphyxiated neonates had fetal distress whereas only 5.7% from the control group identified to have fetal distress. Sixty-three (90%) of the case and 137 (97.9%) of the controls who were delivered are singletons.
Risk Factors of Perinatal Asphyxia
Initially we have performed bi-variable analysis. Those variable with p-value <0.25 were transferred to multivariate analysis. Some variables such as ethnicity, maternal DM, cord strangulation, and oligohydrominous were left out of the final model since they have less than 20% expected events per cell. Additionally, obstructed labor was further excluded due to the collinearity effect. Those variables not included in the final model were presented as in Table S1. Afterward, the multivariate analysis showed that antepartum hemorrhage, low birth weight, preterm birth, cesarean section delivery, instrumental delivery, fetal distress, and meconium-stained amniotic fluid were independently associated with perinatal asphyxia (Table 4).
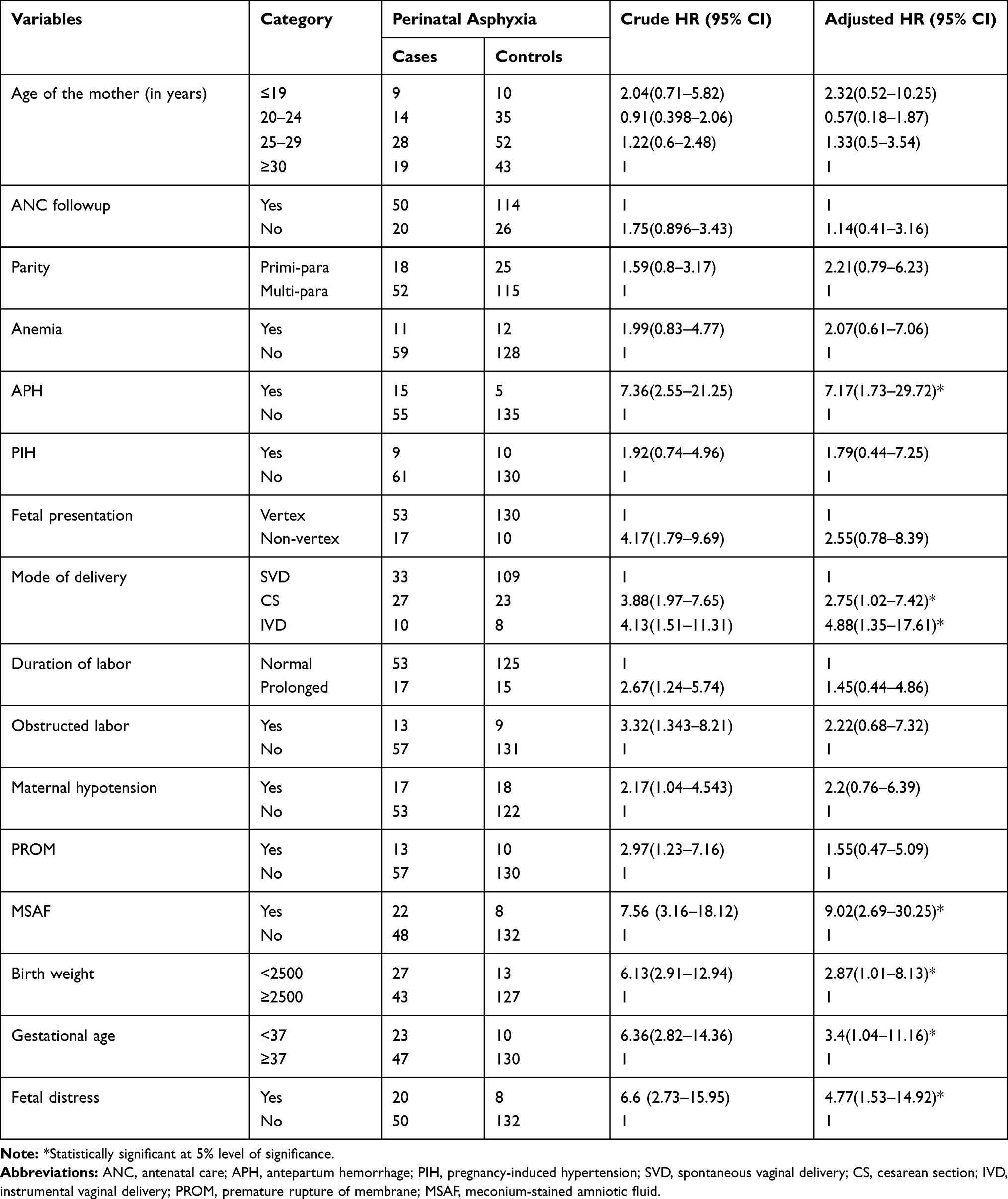 |
Table 4 Bi-Variable and Multivariate Analysis for the Risk Factors of Perinatal Asphyxia Among Newborns Delivered at Public Hospitals in Addis Ababa, Ethiopia, 2019 (N=210) |
The multivariable analysis result showed that those mothers of newborns who have had antepartum hemorrhage were about 7.17 times to have newborns suffered from perinatal asphyxia compared with their counterparts [AOR=7.17, 95% CI (1.73–29.72)]. The odds of newborns delivered via cesarean section to acquire asphyxia was 2.75 times higher than those neonates delivered via SVD [AOR=2.75, 95% CI (1.02–7.42)] whereas newborn delivered through instrumental delivery were 4.88 times [AOR=4.88, 95% CI (1.35–17.61)] more likely to develop perinatal asphyxia than those delivered via SVD.
Intrapartum fetal distress was also significantly associated with perinatal asphyxia. Neonates with intrapartum fetal distress were 4.77 times more likely to have perinatal asphyxia when compared with their counterparts [AOR=4.77, 95% CI (1.53–14.92)]. Furthermore, the odds of preterm newborns was 3.4 times greater than term neonates did [AOR=3.4, 95% CI (1.04–11.16)]. Neonates delivered with meconium-stained amniotic fluid were 9.02 times [AOR=9.02, 95% CI (2.69–30.25)] more likely to develop perinatal asphyxia compared to their counterparts. Neonates with low birth weight were at three folds increased risk to acquire perinatal asphyxia than normal birth weight newborn did [AOR=2.87, 95% CI (1.01–8.13)] (Table 4).
Discussion
Prevention of perinatal asphyxia and its complications is dependent on the early identification of risk factors during pregnancies along with the appropriate provision of intervention. In this study antepartum hemorrhage, low birth weight, cesarean section delivery, instrumental delivery, fetal distress, preterm birth, and meconium-stained amniotic fluid were identified as risk factors of perinatal asphyxia.
Newborns delivered from the mother with antepartum hemorrhage were approximately seven times more likely to have perinatal asphyxia compared with their counterparts. This finding is consistent with the study conducted at Tigray, Ethiopia,29 and Indonesia.32 This could be due to the decreased placental blood flow secondary to antepartum hemorrhage that will lead to fetal hypoxemia and perinatal asphyxia.
Newborns delivered through instrumental delivery were 4.88 times more at risk for perinatal asphyxia than neonates who were delivered spontaneously. This finding was harmonious with the study conducted at Dessie, Ethiopia,31 and India.33 The possible justification could be that instrumental delivery can cause birth trauma (skull fracture, intracranial hemorrhage, subgaleal hemorrhage) which can further lead to perinatal asphyxia.34 On the contrary, the study done in Hong Kong, China showed that there was a significant decrease in birth asphyxia related to instrumental delivery.35 This could be due to the Hawthorne effect (tendency to improve performance because of awareness of being studied) in that study.
Likewise, neonates delivered by cesarean section were nearly three times more likely to develop perinatal asphyxia compared with neonates delivered spontaneously per vagina. This finding was congruent with the study conducted in Indonesia,32 Pakistan,13 Nigeria,5 and Iran.36 The possible justification might be unlike vaginal delivery, cesarean section delivery did not involve vaginal squeeze and thus could not cause chest compression and are at greater risk for respiratory distress.37
Additionally, newborns delivered with meconium-stained amniotic fluid were 9 times more likely to have perinatal asphyxia compared with that clear amniotic fluid. This finding is in line with studies from Jimma,28 Thailand,38 Uganda,39 and India.33 The reason for this might be that newborns delivered from mothers with meconium-stained amniotic fluid were prone to aspiration, which can predispose to lung inflammation, obstruction, and limited lung compliance.9,40
The current study revealed that prematurity was significantly associated with perinatal asphyxia (AOR=3.4). This finding was supported by studies conducted at Tigray, Ethiopia,29 Karachi,41 and Jakarta.40,42 This could be explained as the immaturity of organ systems mainly of the pulmonary function especially those who were born before 34 weeks of gestation lack surfactant and may suffer to maintain breathing and tissue perfusion after birth. Preterm neonates are also prone to co-morbidities that will impair normal functioning in the extra-uterine life.40
Again, newborns with low birth weight were three times more at risk to develop perinatal asphyxia than newborns with normal birth weight. This finding was conformable with previous African and Asian studies.29,36,38 This might be due to the possibility that most of the low birth weight babies might be preterm babies that they might not able to produce enough amount of surfactant that further leads to the difficulty of breathing and consequently develop perinatal asphyxia.40
Besides, having intrapartum fetal distress was found to be independently associated with perinatal asphyxia (AOR=4.77). This finding was compatible with studies from Gonder, Ethiopia,30 Karachi,41 and Al-Diwaniya.43 The possible explanation is fetal distress mainly result from insufficient placental perfusion or any factor during labor that will impair fetal oxygenation so that this can further cause difficulty to initiate and sustain breathing after birth end up with asphyxia.
Conclusion
Perinatal asphyxia is one of the worldwide problems of neonates. The current study identified different antepartum, intrapartum, and neonatal factors that were significantly associated with perinatal asphyxia. Antepartum hemorrhage, cesarean section delivery, instrumental delivery, fetal distress, meconium-stained amniotic fluid, low birth weight, and preterm birth were identified as independent risk factors of perinatal asphyxia.
Data Sharing Statement
Extra data that support the findings of this study are available from the corresponding author upon reasonable request and can be shared upon legal request via [email protected]
Ethical Approval and Consent to Participate
Ethical clearance and approval were obtained from Addis Ababa University, College of Health Science institutional review board. Then officials at different levels of the selected hospitals had been communicated through cooperation letter written from the School of Nursing and Midwifery. The study was conducted per the declaration of Helsinki. The purpose of the study was explained to and written informed consent was obtained from mothers of newborns to confirm willingness. They were notified that they have the right to refuse or terminate the interview at any time. Confidentiality of the information was secured throughout the study process.
Acknowledgments
Study participants, data collectors, supervisors, hospital staff, and administrators were appreciated for their unfailing contribution. The authors would also like to thank the funder of this study, Dilla University, and Addis Ababa University to chase this chance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
Girum Sebsibe reports a patent they participated in for this original research. As stated in the ethical approval session, the findings of this study were presented and submitted to Addis Ababa University, collage of health sciences and school of allied health sciences as a postgraduate thesis, and the whole thesis file was just released online in Addis Ababa University (AAU) institutional repository. URL: http://etd.aau.edu.et/handle/123456789/21432. The authors report no other potential conflicts of interest for this work.
References
1. World health organization. Newborns: reducing mortality. Available from: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-mortality.
2. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. The Lancet. 2016;388(10063):3027–3035. doi:10.1016/S0140-6736(16)31593-8
3. Lawn JE, Cousens S, Zupan J, Team LNSS. 4 million neonatal deaths: when? Where? Why? The Lancet. 2005;365(9462):891–900. doi:10.1016/S0140-6736(05)71048-5
4. Lawn JE, Blencowe H, Oza S, et al. Every Newborn: progress, priorities, and potential beyond survival. The Lancet. 2014;384(9938):189–205. doi:10.1016/S0140-6736(14)60496-7
5. Ilah BG, Aminu MS, Musa A, Adelakun MB, Adeniji AO, Kolawole T. Prevalence and risk factors for perinatal asphyxia as seen at a specialist hospital in Gusau, Nigeria. Sub-Saharan Afr J Med. 2015;2(2):64. doi:10.4103/2384-5147.157421
6.. Bhutta ZA. Pediatrics in the Tropics. Manson’s Trop Infect Dis. 2014;1197–1214.e1192. doi:1110.1016/b1978-1190-7020-5101-1192.00081-00089.
7. WHO. Guidelines on basic newborn resuscitation. 2012.
8. Polglase GR, Ong T, Hillman NH. Cardiovascular alterations and multiorgan dysfunction after birth asphyxia. Clin Perinatol. 2016;43(3):469–483. doi:10.1016/j.clp.2016.04.006
9. Federal Ministry of Health of Ethiopia (FMOH). Neonatal Intensive Care Unit (Nicu)training Manual. Addis Ababa; 2015.
10. WHO. ICD-11 for mortality and morbidity statistics. Available from: https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f1875062819.
11. Wall SN, Lee AC, Niermeyer S, et al. Neonatal resuscitation in low‐resource settings: what, who, and how to overcome challenges to scale up? Int J Gynecol Obstetrics. 2009;107(Supplement):S47–S64. doi:10.1016/j.ijgo.2009.07.013
12. Hofmeyr GJ, Haws RA, Bergström S, et al. Obstetric care in low‐resource settings: what, who, and how to overcome challenges to scale up? Int J Gynecol Obstetrics. 2009;107(Supplement):S21–S45. doi:10.1016/j.ijgo.2009.07.017
13. Kiyani AN, Khushdil A, Ehsan A. Perinatal factors leading to birth asphyxia among term newborns in a tertiary care hospital. Iran J Pediatr. 2014;24(5):637.
14. Siva Saranyappa SB, Nair CC, Madhu G, Srinivasa S, Manjunath M. Clinical profile and outcome of perinatal asphyxia in a tertiary care center. Curr Ped Res. 2015;19:1.
15. Ahearne CE, Boylan GB, Murray DM. Short and long term prognosis in perinatal asphyxia: an update. World J Clin Pediatrics. 2016;5(1):67. doi:10.5409/wjcp.v5.i1.67
16. Antonucci R, Porcella A, Pilloni MD. Perinatal asphyxia in the term newborn. J Ped Neonatal Individualized Med. 2014;3(2):e030269.
17. Horsch A, Jacobs I, Gilbert L, et al. Impact of perinatal asphyxia on parental mental health and bonding with the infant: a questionnaire survey of Swiss parents. BMJ Pediatrics Open. 2017;1:1. doi:10.1136/bmjpo-2017-000059
18. Ehrenstein V, Pedersen L, Grijota M, Nielsen GL, Rothman KJ, Sørensen HT. Association of Apgar scores at five minutes with a long-term neurologic disability and cognitive function in a prevalence study of Danish conscripts. BMC Pregnancy Childbirth. 2009;9(1):14. doi:10.1186/1471-2393-9-14
19. Herrera MI, Otero-Losada M, Udovin LD, et al. Could perinatal asphyxia induce a synaptopathy? new highlights from an experimental model. Neural Plast. 2017;2017.
20. Pattar RS, Raj A, Yelamali BC. Incidence of multiorgan dysfunction in perinatal asphyxia. Int J Contemp Pediatrics. 2017;2(4):428–432.
21. Ehrenstein V. Association of Apgar scores with death and neurologic disability. Clin Epidemiol. 2009;1:45. doi:10.2147/CLEP.S4782
22. Shireen N, Nahar N, Mollah A. Risk factors and short-term outcome of birth asphyxiated babies in Dhaka Medical College Hospital. Bangladesh J Child Health. 2009;33(3):83–89. doi:10.3329/bjch.v33i3.5688
23. WHO. World Health Statistics: Monitoring Health for Sustainable Development Goals (Sdgs). WHO Library Cataloguing-in-Publication Data; 2016: 1–136.
24. FMOH. Health Sector Transformation Plan-I; 2016.
25. Alkema L, Chou D, Hogan D, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. The Lancet. 2016;387(10017):462–474. doi:10.1016/S0140-6736(15)00838-7
26. UNICEF. Maternal and Newborn Health Disparities. Ethiopia; 2015.
27. Ibrahim N, Muhye A, Abdulie S. Prevalence of birth asphyxia and associated factors among neonates delivered in Dilchora Referral Hospital. Dire Dawa, Eastern Ethiopia Clin Mother Child Health. 2017;14:4.
28. Belachew T, Joseph J. Birth asphyxia and associated factors among newborns delivered in Jimma zone public hospitals, Southwest Ethiopia: a cross-sectional study. J Midwif Reprod Health. 2018;6(2):1289–1295.
29. Tasew H, Zemicheal M, Teklay G, Mariye T, Ayele E. Risk factors of birth asphyxia among newborns in public hospitals of Central Zone, Tigray, Ethiopia 2018. BMC Res Notes. 2018;11(1):496. doi:10.1186/s13104-018-3611-3
30. Wosenu L, Worku AG, Teshome DF, Gelagay AA. Determinants of birth asphyxia among live birth newborns in University of Gondar referral hospital, northwest Ethiopia: a case-control study. PLoS One. 2018;13(9):e0203763. doi:10.1371/journal.pone.0203763
31. Hailu G, Yohannes K, Kassawmar A. Determinants of birth-asphyxia among newborns in Dessie Town Hospitals, North-Central Ethiopia,2018. Int J Sex Health Repro Health. 2018;1(1):1–12.
32. Utomo MT. Risk factors for birth asphyxia. Folia Medica Indonesiana. 2011;47(4):211.
33. Gane B, Bhat V, Adhisivam B, Joy R, Prasad P, Shruti S. Antenatal, and intrapartum risk factors for perinatal asphyxia: a case-control study. Curr Ped Res. 2013;17:2.
34. Towner DR, Ciotti MC. Operative vaginal delivery: a cause of birth injury or is it? Clin Obstet Gynecol. 2007;50(3):563–581. doi:10.1097/GRF.0b013e31811eaa39
35. Leung W, Chan B, Ma G, et al. Continued reduction in the incidence of birth trauma and birth asphyxia related to instrumental deliveries after the study period: was this the Hawthorne effect? Eur J Obstetrics Gynecol Reprod Biol. 2007;130(2):165–168. doi:10.1016/j.ejogrb.2006.02.013
36. Nayeri F, Shariat M, Dalili H, Adam LB, Mehrjerdi FZ, Shakeri A. Perinatal risk factors for neonatal asphyxia in Vali-e-Asr hospital, Tehran-Iran. Iran J Reprod Med. 2012;10(2):137.
37. Champlain Maternal Newborn Regional Program (CMNRP). Newborn Adaptation to Extrauterine Life: A Self-Learning Module. 2013:7–11
38. Pitsawong C, Panichkul P. Risk factors associated with birth asphyxia in Phramongkutklao Hospital. Thai J Obstetrics Gynaecol. 2012;19(4):165–171.
39. Kaye D. Antenatal and intrapartum risk factors for birth asphyxia among emergency obstetric referrals in Mulago Hospital, Kampala, Uganda. East Afr Med J. 2003;80(3):140–143. doi:10.4314/eamj.v80i3.8683
40. UNICEF. Neonatal Care Pocket Guide for Hospital Physicians; 2010.
41. Aslam HM, Saleem S, Afzal R, et al. Risk factors of birth asphyxia. Ital J Pediatr. 2014;40(1):94. doi:10.1186/s13052-014-0094-2
42. Opitasari C, Andayasari L. Maternal education, prematurity, and the risk of birth asphyxia in selected hospitals in Jakarta. Health Sci J Indonesia. 2015;6(2):111–115.
43. Sahib HS. Risk factors of perinatal asphyxia: a study at Al-Diwaniya maternity and children teaching hospital. Risk. 2015;2(2):50–57.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.