")
Back to Journals » Infection and Drug Resistance » Volume 14
Risk Factors of Death in Bloodstream Infections Caused by AmpC β-Lactamase-Producing Enterobacterales in Patients with Neoplasia
Authors Cunha Ferreira T , Martins IS
Received 6 May 2021
Accepted for publication 3 July 2021
Published 11 August 2021 Volume 2021:14 Pages 3083—3097
DOI https://doi.org/10.2147/IDR.S312920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Tiago da Cunha Ferreira,1– 3 Ianick Souto Martins3,4
1Infection Control Division, Policlínica Piquet Carneiro, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, RJ, Brazil; 2Infectious Diseases Division, Hospital Universitário Pedro Ernesto, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, RJ, Brazil; 3Faculty of Medicine, Fluminense Federal University, Niterói, RJ, Brazil; 4Infection Control Division, Hospital do Câncer I, Instituto Nacional do Câncer, Rio de Janeiro, RJ, Brazil
Correspondence: Ianick Souto Martins
Faculty of Medicine, Universidade Federal Fluminense, Rua Marquês de Paraná, 303, Centro, Niterói, RJ, CEP 240033-900, Brazil
Tel +55 21 2629-9000
Email [email protected]
Purpose: The infections caused by ESCPM Enterobacterales (Enterobacter spp., Serratia spp., Citrobacter spp., Providencia spp. and Morganella spp.) have limited therapeutic options. Patients with neoplastic diseases are particularly vulnerable to bloodstream infections (BSIs).
Objective: To analyze determinant factors of death in patients with neoplasia complicated with BSI caused by ESCPM Enterobacterales.
Patients and Methods: A cohort study of patients aged 18 years or older with neoplasia and BSI due to ESCPM group was conducted at the Cancer Hospital I of the National Cancer Institute, Brazil, from September 2012 to December 2017. The variables associated with death were analyzed using multivariate logistic regression.
Results: Of the 103 patients included in the cohort, 67.0% were male, the median age was 63 years and 67.0% had solid tumors. Of the 107 BSI episodes evaluated, 70.1% were hospital-acquired infections, 54.2% were secondary to extravascular focus of infection, gastrointestinal tract (19.6%), mainly. Enterobacter spp. (n: 49, 45.4%) was the most frequent agent isolated followed by Serratia spp. (n: 34, 31.5%), Morganella morganii (n: 16, 14.9%), Citrobacter freundii. (n: 7, 6.5%) and Providencia spp. (n: 2, 1.8%). Ten (9.3%) BSI episodes were caused by multidrug-resistant ESCPM Enterobacterales (MDR-ESCPM). The 7-day and 30-day mortality were 9.3% and 21.5%, respectively. The BSIs caused by MDR-ESCPM were independently associated with 7-day death (OR = 21.62 95% CI: 1.81– 258.51 P = 0.01). Monotherapy with piperacillin-tazobactam tended to be associated with 7-day death (OR = 10.46 95% CI: 0.97– 112.91 P = 0.05) and 30-day death (OR = 2.73 95% CI: 0.96– 7.70 P = 0.05).
Conclusion: BSIs due to ESCPM group have high mortality and when caused by MDR-ESCPM are independently associated with 7-day death. The possible association of piperacillin-tazobactam monotherapy for BSI-ESCPM with death needs to be better studied.
Keywords: β-lactamases, mortality, cancer, piperacillin-tazobactam
Introduction
Infections caused by multidrug-resistant (MDR) strains have emerged as a major threat to human health. Enterobacterales are among the most common causes of bacterial infections in the community and hospitalized patients. Enterobacterales resistant to third-generation cephalosporins due to the production of AmpC β-lactamase encoded by resident chromosomal genes (eg, Enterobacter spp., Serratia marcescens, Citrobacter freundii, Providencia spp., Morganella morganii – ESCPM group) are frequent agents of infection such as bloodstream infection (BSI).1 In ESCPM group, AmpC β-lactamase is inducible and can be expressed at high levels by mutation. Overexpression confers resistance to broad-spectrum cephalosporins including cefotaxime, ceftazidime, and ceftriaxone and is a problem, especially in infections due to E. aerogenes and E. cloacae, where an isolate initially susceptible to these agents may become resistant upon therapy.2
BSIs can be severe with high mortality,3 and when caused by ESCPM group have limited therapeutic options. Patients with neoplastic diseases are particularly vulnerable to BSI due cellular and humoral immune dysfunction and mucosal barrier damage.4 In this cohort study, mortality and determinant factors of death in patients with neoplastic diseases complicated with BSI due to ESCPM group were analyzed.
Methods
Study Design
A cohort of patients older than 18 years, with neoplastic diseases complicated by BSI caused by ESCPM group was carried on in a referral hospital for cancer in Rio de Janeiro, Brazil, from September 1st, 2012 to December 31st, 2017. All BSI episodes detected in each patient hospitalized to the hospital were included in the analyses; thus, more than one episode of BSI per patient was considered. The main outcomes evaluated were 7-day death and 30-day death after the date that the positive blood culture was collected (defined as the date of the BSI diagnosis). Epidemiological and clinical characteristics of the patients and of the BSI episodes as well as the treatment initiated for each BSI episode were analyzed as possible risk factors for death. Patients who died up to 48 hours from the diagnosis of BSI were excluded. This study was approved by the Board of the Ethics in Research of Instituto Nacional do Cancer (INCA), number 1.786.731. The Ethics Committee of INCA waived the requirement for informed consent for this study, since it was an observational study; data were analyzed anonymously and kept confidential. This study was performed in accordance with the Declaration of Helsinki.
Detection of the BSI Episodes and the Data Collection
The potential episodes of BSI were prospectively detected by daily laboratorial-based surveillance of positive blood cultures. Once a positive blood culture was detected, the diagnosis of BSI was then confirmed in patients with signs and symptoms of infection by bedside physical examination and review of the respective patient’s medical records.5 The following data were: (i) demographic and clinical characteristics of the patients: date of birth, gender, date of hospitalization, type of neoplasia (solid organ tumor and hematological neoplasia), Charlson comorbidity index;6 the oncological disease stages; use of chemotherapy in the last 12 months, radiotherapy in the last six months, and corticosteroid therapy (dose > 60 mg/day prednisone or equivalent) in the last 30 days; (ii) Clinical and microbiological characteristics of the BSI episodes: the date of collection of the positive blood culture, if the BSI episode was the first one or not, the microorganism detected and its antimicrobial sensitivity; the type of BSI acquisition (hospital-acquired infection, community-acquired infection and healthcare-associated infection),7 the focus of the BSI (primary BSI or BSI secondary to an extravascular site of infection),5 the presence of neutropenia (500 neutrophil/mm3) during the BSI episode,8 types of antibiotic initiated for the BSI treatment with date of beginning and finish, other therapeutic approaches such as vascular catheter withdraw, previous colonization by multi-drug resistant (MDR) agent, necessity of life support in the intensive care unit (ICU) during the BSI treatment, date of the clinical outcome (death or discharge) and date.
Definitions
The community-acquired BSI (CA-BSI) was defined as those diagnosed or in incubation at the time of the patient’s admission, and not related to healthcare assistance. Then, outpatients in ambulatorial follow-up that were not under medical procedures, such as chemotherapy, radiotherapy, hemodialysis, and use of long-term catheter hospitalized because of BSI, were included in this category. The healthcare-associated BSI (HA-BSI) was defined as that detected in outpatients under healthcare in homecare, day-clinic or hemodialysis clinic, including those patients in chemotherapy, radiotherapy, and use of long-term catheter. The hospital-acquired BSI (H-BSI) was defined as those acquired on or after the 3rd day of hospital stay, manifested during hospital stay or after discharge.7
The definitions of laboratory-confirmed BSI (LC-BSI), central line associated BSI (CLA-BSI), mucosal barrier injury BSI (MBI-BSI), primary BSI (P-BSI) and secondary BSI (S-BSI) were in accordance with The Centers for Disease Control and Prevention (CDC) recommendations.5 P-BSI is defined as an LC-BSI that is not secondary to an infection at another body site and S-BSI as a BSI that is thought to be seeded from a site-specific infection at another body site. Oncological disease stages were defined as:9 (I) disease under treatment with possibility of cure; (II) disease under control if the disease was under control or was cured after a specific treatment; (III) disease without a curative plan if the patient was under palliative-care or end-of-life care. This classification was based on medical records completed by the patient’s treating physician. The ESCPM pathogens were considered MDR according to the following criteria: non-susceptibility to at least one agent in three or more antimicrobial categories, except those with intrinsic resistance.10 Resistance to 1st, 2nd and 3rd-generation cephalosporin, amoxicillin-clavulanate and piperacillin-tazobactam were considered intrinsic due to AmpC cromossomial production by ESCPM group.2 The following criteria were used to define the appropriate antibiotic therapy: (i) the microorganism growth in the blood culture must be susceptible to at least one of the antibiotics used for the treatment and (ii) antibiotic therapy must be initiated in the same day of the blood culture performance and (iii) at least one of the antibiotics used for the treatment must have adequate concentration at the site of infection according to known pharmacological parameters and (iv) antibiotic therapy must be used for at least 48 hours. Otherwise, if any of the previous criteria were not filled out, the antibiotic therapy was considered inappropriate. Life support in the ICU was defined as the beginning of use of vasoactive amines, mechanical ventilation or transfer to the ICU during 48 h before or after the BSI diagnosis.
Microbiological Procedures
Two peripheral blood samples were obtained from at least two different venipuncture sites in each patient, as recommended by the Infection Control Division of the hospital. When a long-term catheter-associated infection was suspected, an additional blood sample was collected from the suspected vascular device at the same time the peripheral blood sample was drawn. Each blood sample was placed into a separate culture bottle (BD BACTEC Lytic/10 Anaerobic/F, BACTEC plus Aerobic/F and BACTEC MYCO/F Lytic; Becton, Dickinson and Company; Maryland USA). Microorganism growth was detected by the BACTEC® 9240 system (Becton Dickinson). The identification of different species was performed by the Vitek2® automated system (BioMérieux), API 20, API Staph and rapid ID 32 Strep (BioMérieux®). Testing for antibiotic susceptibility was performed with Vitek2® and antibiotic gradient tests (BioMérieux) and interpreted in accordance with the Clinical and Laboratory Standards Institute (CLSI) recommendations, applying the versions updated for the year in which the blood culture was performed, from 2012 to 2017. The resistance to cefoxitin is considered a phenotypic marker of the presence of chromosomal AmpC.
Statistical Analysis
Proportions and median values were reported for categorical and continuous variables, respectively. The χ2 or Fisher’s exact tests were used as appropriate for comparison of categorical variables and Student’s t-tests or Mann–Whitney test for comparison of continuous variables, as appropriate. Univariate analysis was performed to evaluate the potential variables associated with death due to the BSI. Those variables presenting P-value ≤0.25 in univariate analysis or considered of clinical relevance were included for multivariate analysis using logistic regression. The backward stepwise strategy was performed, using the likelihood test with P value <0.05 level to determine which covariates remained in the final model. The odds ratio (OR), confidence interval of 95% (IC 95%) and P-value were calculated. P-values less than 0.05 were considered significant. Data were collected using Magpi® Advanced Mobile Data Collection and analyzed using the Stata 11.0 statistical software program (Stata Corp LP, College Station, Texas).
Results
Study Population
A total of 118 patients with 122 BSI episodes were identified during the study period. After excluding 15 patients (15 BSI episodes) due to death within 48 hours of the BSI diagnosis, a cohort of 103 patients with 107 BSI episodes (four patients presented two BSI episodes) remained for further analysis (Figure 1).
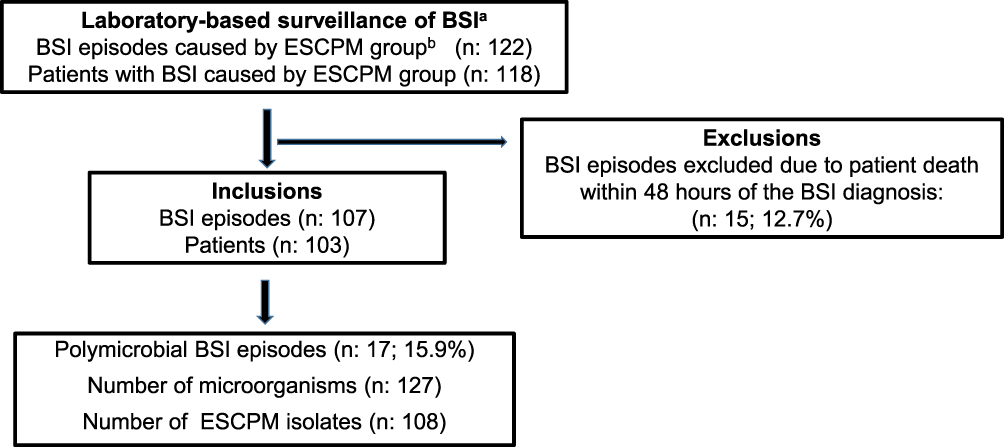 |
Figure 1 Description of the detection of the BSI episodes and patients selected to be included in the study. Abbreviations: aBSI, blood stream infection; bESCPM, Enterobacter spp., Serratia spp., Citrobacter spp., Providencia spp., Morganella spp. |
Of 103 patients, 67% (n: 69) were male; the median age was 63 years (IQR, 18–88), and the median Charlson score was 2 (IQR, 2–9). Most of the patients had solid organ tumors (SOT, 67.0%, n: 69), mainly intra-abdominal cancer (38.8%, n: 40). Hematological neoplasms were found in 33% (n: 34) of the patients with a discrete predominance of lymphomas (14.6%, n: 15). These data are detailed in Table 1.
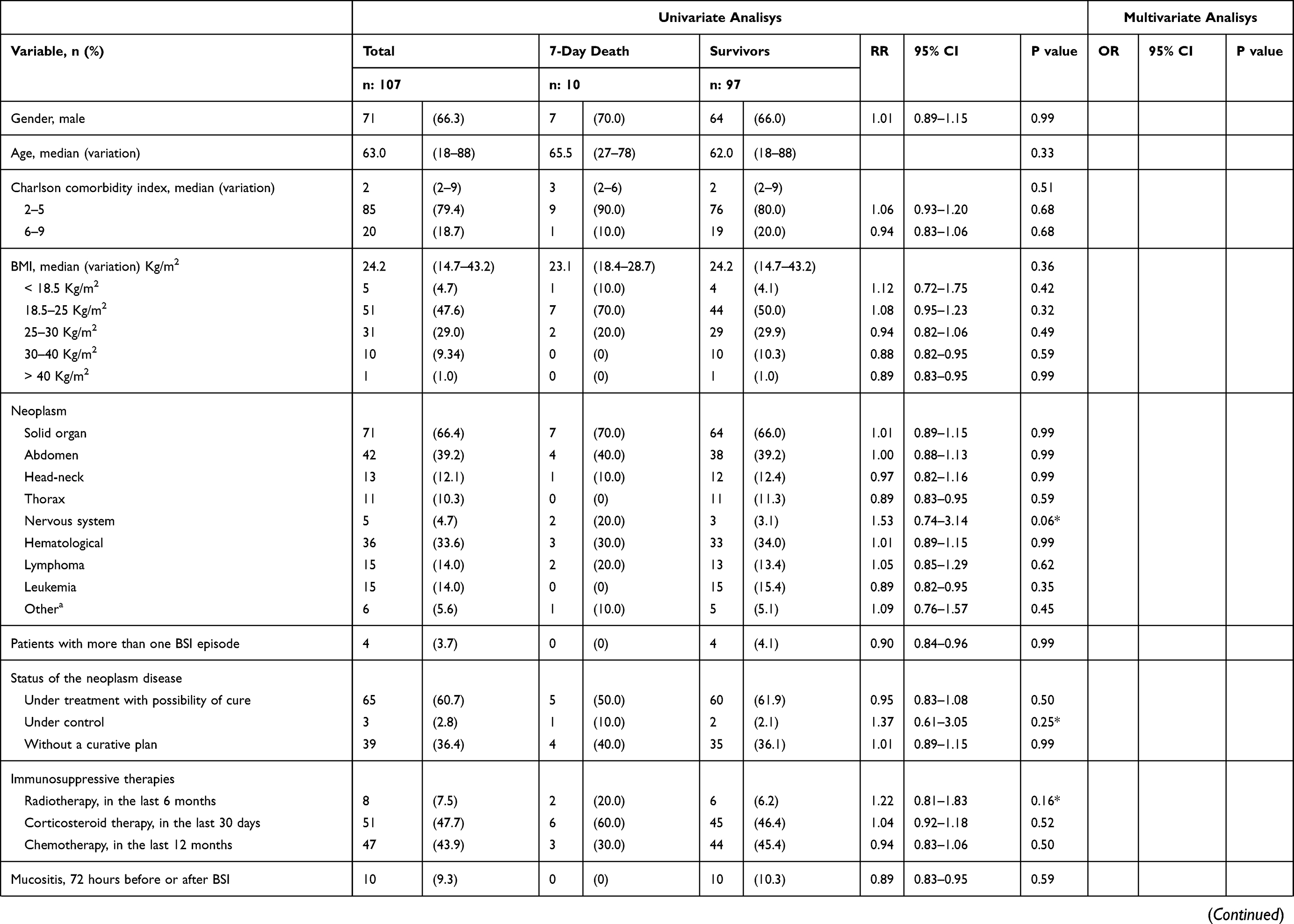 | 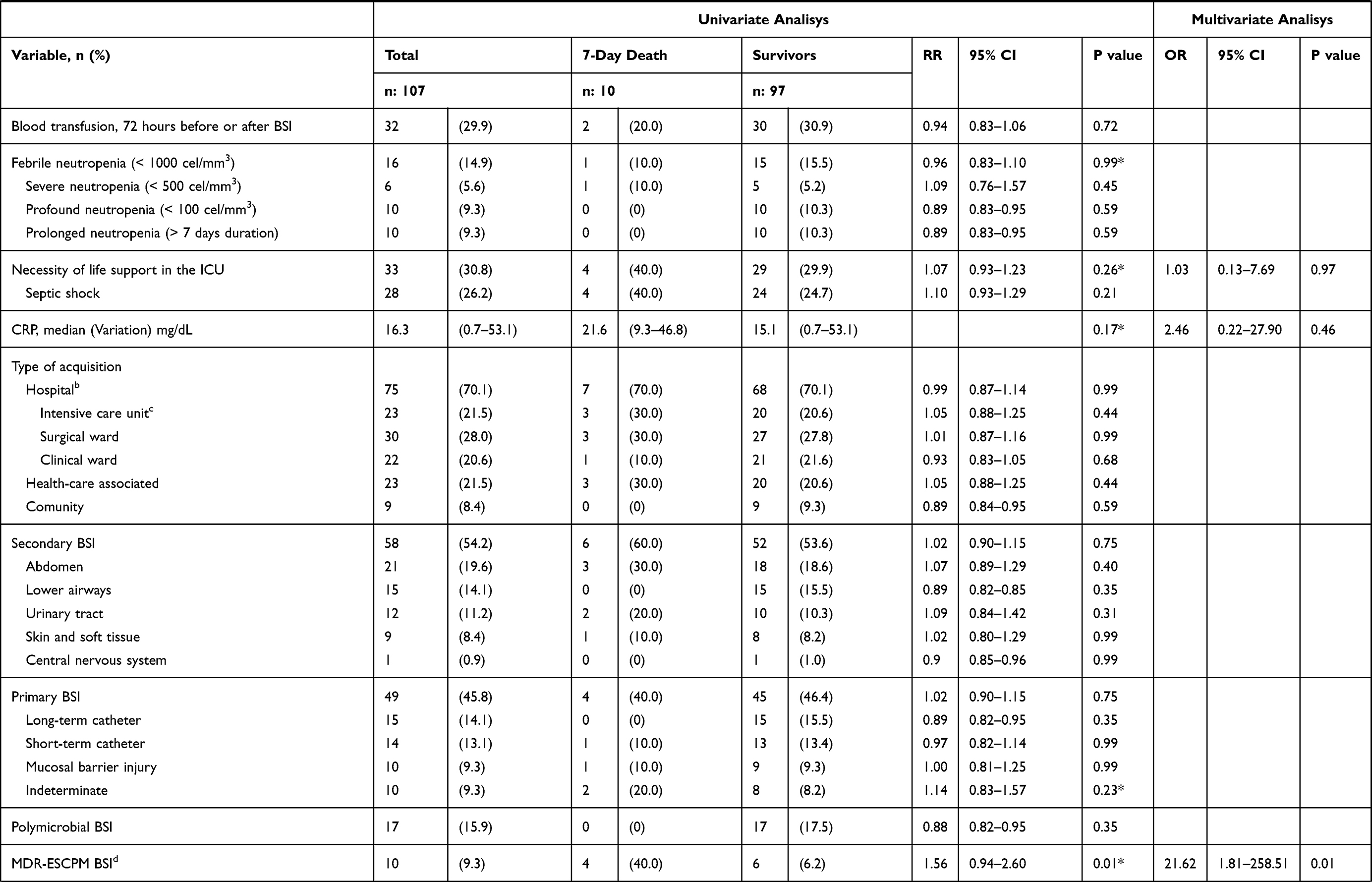 | 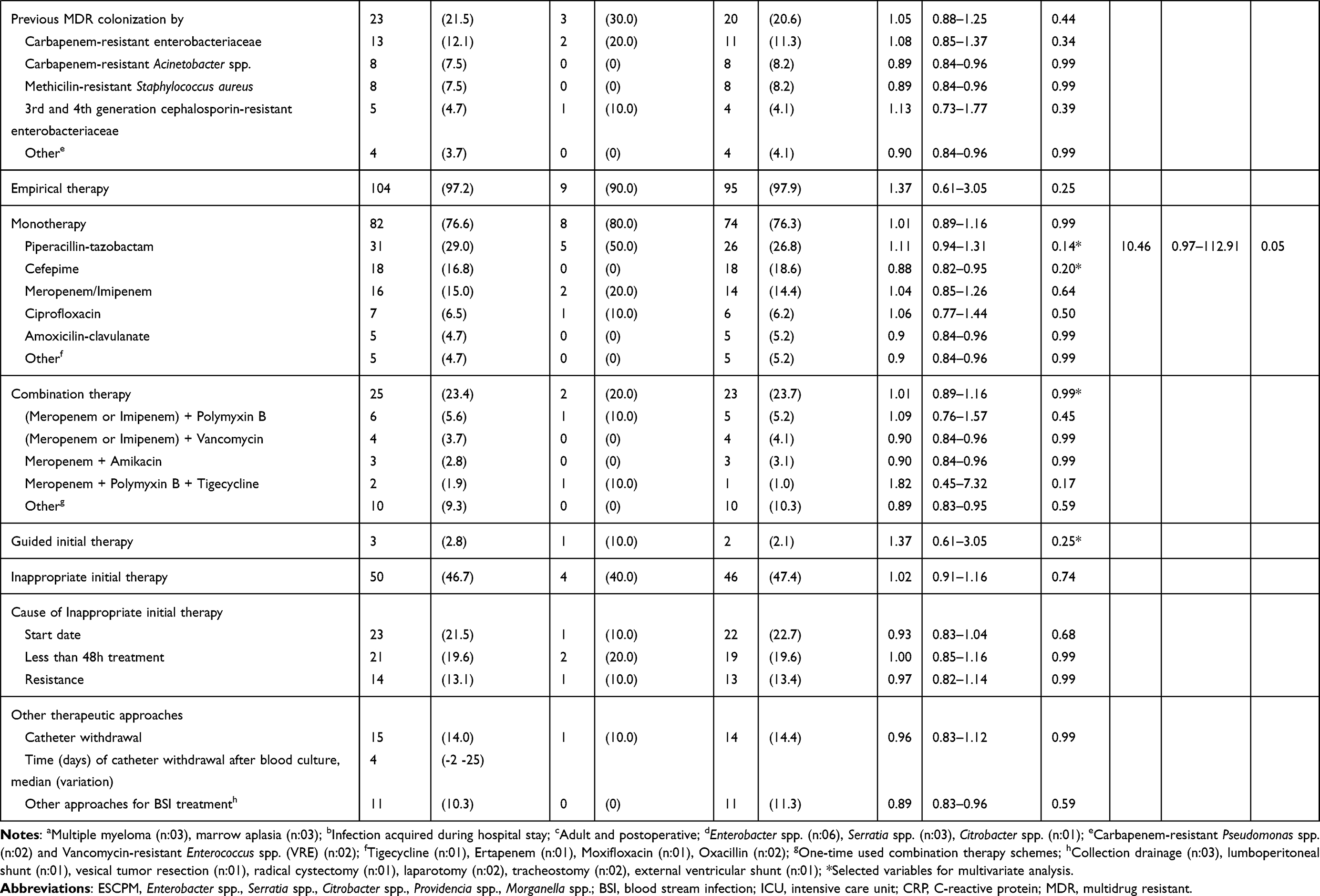 |
Table 1 Univariate and Multivariate Analysis of Risk Factors for 7-Day Death of 107 Episodes of Bloodstream Infection Caused by ESCPM Enterobacteria |
Clinical and Epidemiologic Characteristics of the BSI Episodes
Of the 107 BSI episodes, 60.7% (n: 65) occurred in patients with neoplastic disease under treatment with the possibility of cure. Most of the infections were H-BSI (70.1%, n: 75). BSI episodes secondary to extravascular sites of infection were discreetly predominant (54.2%, n: 58) in comparison to primary BSI, mainly related to intra-abdominal (19.6%, n: 21) and lower airways (14.1%, n: 15) origin. Among primary BSI (45.8%, n: 49), catheter-related infection represented 27.2% (n: 29) of the episodes. Febrile neutropenia was present in 14.9% (n: 16) BSI episodes. The patient’s uses of corticosteroids in the last 30 days and of chemotherapy in the last 12 months were observed in 47.7% (n: 51) and 43.9% (n: 47) of the BSI episodes, respectively. Life support in the ICU was necessary in 30.8% (n: 33) of the BSI episodes, mostly due to septic shock (26.2%, n: 28). Ten (9.3%) BSI episodes were caused by MDR-ESCPM as shown in Table 1.
Treatment
Antibiotic therapy was empirically started in almost all cases (97.2%, n: 104). Monotherapy was initiated in most of the cases (76.6%, n: 82), mainly with piperacillin-tazobactam (29.0%, n: 31). Antibiotic association was used in 23.4% (n: 25) BSI episodes. Carbapenem plus polymyxin B (5.6%, n: 6) was the most widely used antibiotic combination. Antibiotic therapy was considered inappropriate in 46.7% (n: 50) of the cases. Other therapeutic approaches for BSI treatment were performed, mostly vascular catheter withdrawal (14.0%, n: 15), as shown in Table 1.
Risk Factors of Death
Seven-day and 30-day mortalities were 9.3% (n: 10) and 21.5% (n: 23), respectively. About a quarter (25.2%, n: 27) of the cases remained hospitalized after 30 days of the BSI diagnosis. After univariate analysis, the variables included in multivariate analysis for 7-day death were diagnosis of nervous system neoplasm, neoplasia under control, previous radiotherapy, septic shock during BSI, the median of C-reactive protein, BSI with indeterminate focus, BSI caused by MDR-ESCPM, monotherapy with piperacillin-tazobactam, monotherapy with cefepime and initial antibiotic therapy guided by culture results. Additionally, febrile neutropenia and BSI with the necessity of life support in the ICU were included in multivariate analyses due to their clinical relevance. After univariate analysis, the variables included in the multivariate analyses for 30-day death were BMI from 18.5 to 25.0 kg/m2, other hematological neoplasms, neoplasia under treatment with possibility of cure, BSI with necessity of life support in the ICU, median of C-reactive protein, the acquisition of the BSI in the clinical wards, BSI associated with long-term vascular catheter, BSI associated with mucosal barrier injury, BSI secondary to gastrointestinal tract, BSI secondary to lower airways, polymicrobial BSI, BSI caused by MDR-ESCPM, previous colonization by any MDR agent, monotherapy with piperacillin-tazobactam, monotherapy with cefepime, monotherapy with ciprofloxacin and vascular catheter removal. In addition, febrile neutropenia and inappropriate initial therapy were included in multivariate due to their clinical importance. The univariate analysis of risk factor for 7-day death and 30-day death is shown in Tables 1 and 2, respectively.
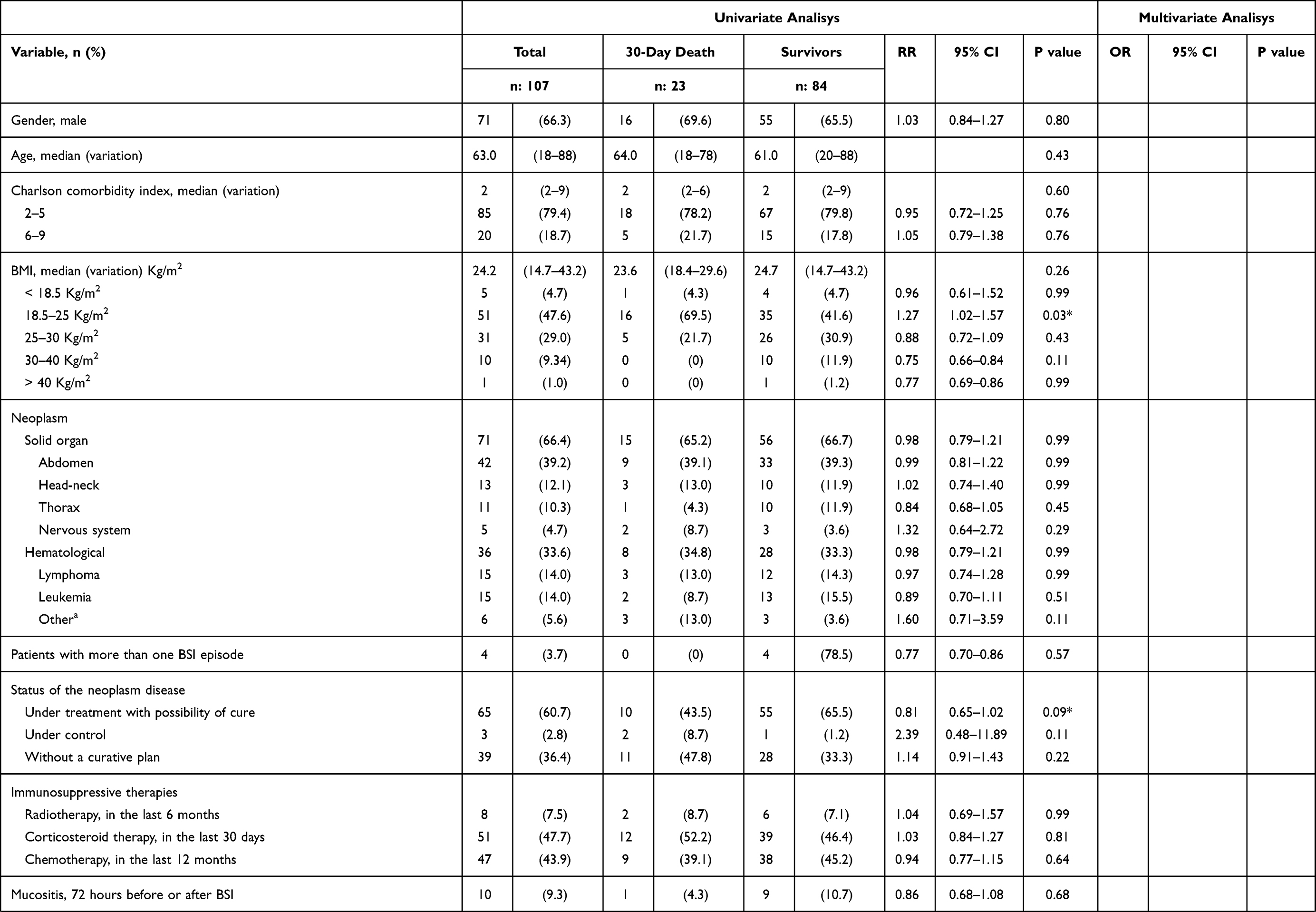 | 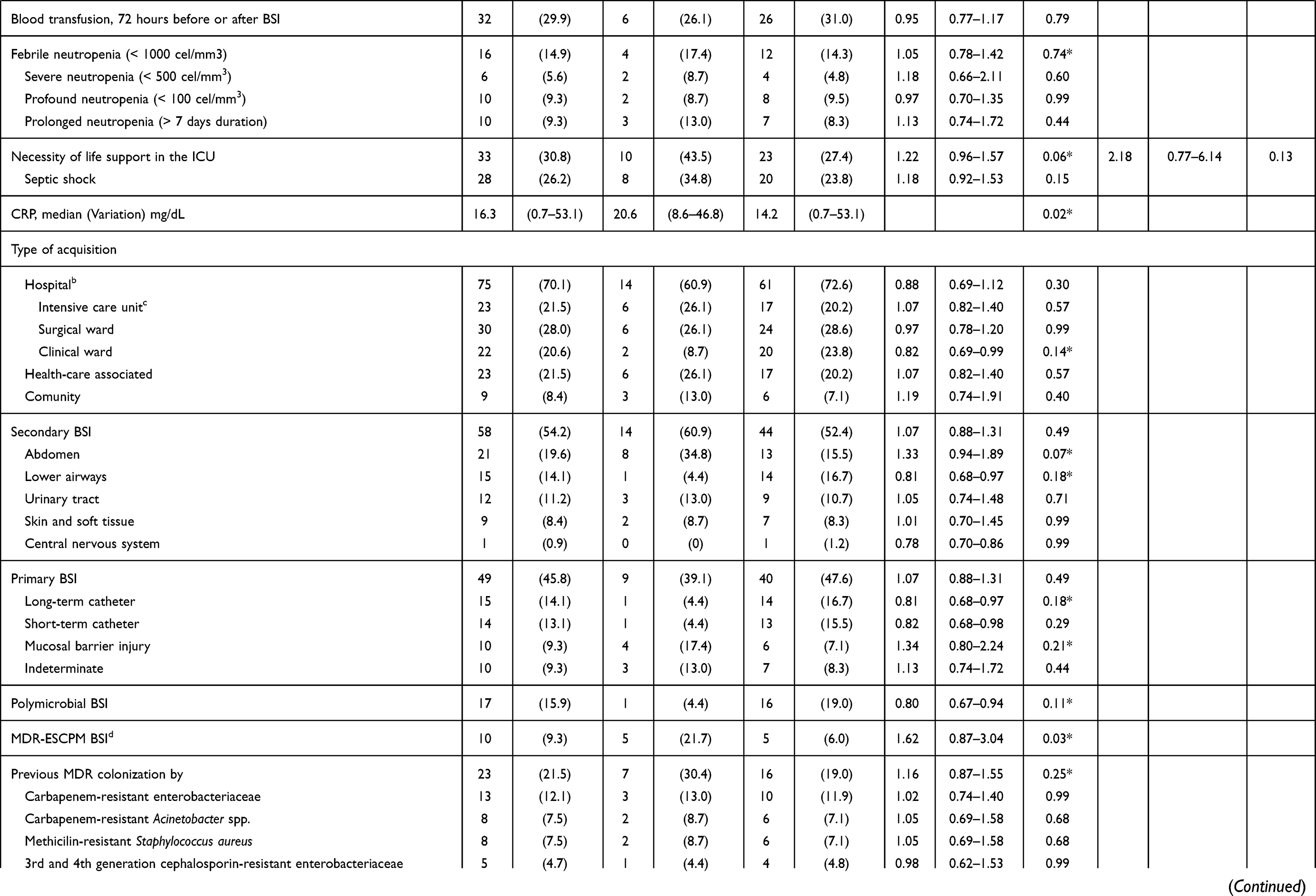 | 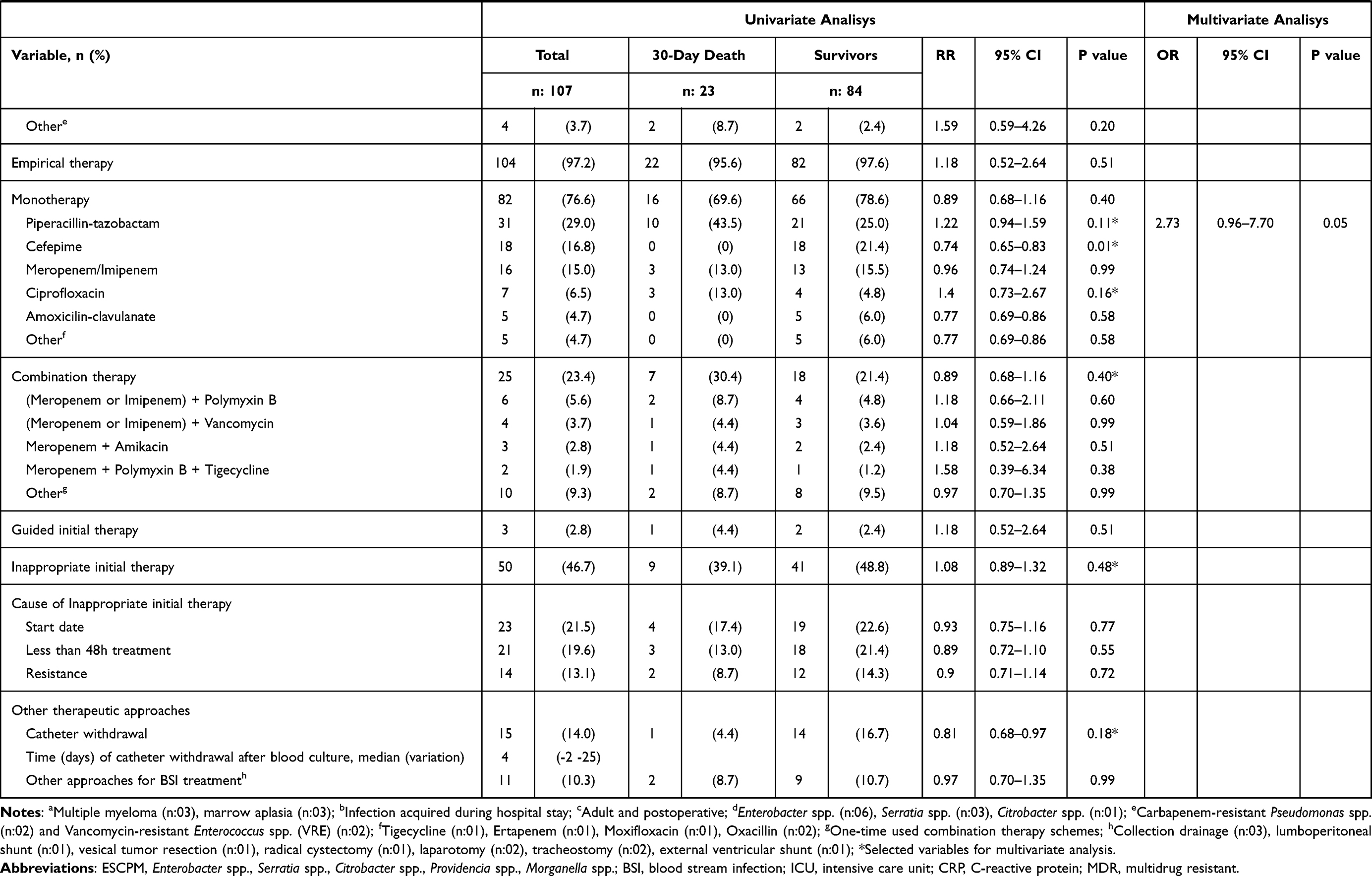 |
Table 2 Univariate and Multivariate Analysis of Risk Factors for 30-Day Death of 107 Episodes of Bloodstream Infection Caused by ESCPM Enterobacteria |
After multivariate analysis, BSI caused by MDR-ESCPM remained independently associated with 7-day death (OR: 21.62; 95% CI: 1.81–258.51, P=0.01). There was a trend towards the association of monotherapy with piperacillin-tazobactam and 7-day death (OR: 10.46; 95% CI: 0.97–112.91, P=0.05) and 30-day death (OR: 2.73; 95% CI 0.96–7.70, P=0.05). These analyses are detailed in Tables 1 and 2.
Microbiological Profile
A total of 108 isolates of ESCPM were detected in 107 BSI episodes; one episode has grown into two bacterial species of the ESCPM group; Enterobacter spp. was the most common (45.4%, n: 49) agent detected followed by Serratia marcescens (31.5%, n: 34), Morganella morganii (14.9%, n: 16), Citrobacter freundii, (6.5%, n: 7) and Providencia spp. (1.8%, n: 2). The higher frequency of resistance was detected to sulfamethoxazole-trimethoprim (21.3%, n: 23), followed by resistance to ciprofloxacin (13.9%, n: 15), cefepime (12.0%, n: 13) and piperacillin-tazobactam (12.0%, n: 13). Enterobacter spp. isolates presented a higher frequency of piperacillin-tazobactam resistance (22.4%, n: 11) than others (Table 3). A total of 17 (15.9%) BSI episodes were polymicrobial, with the growth of other germs (n: 19) in addition to the ESCPM group. These germs were coagulase-negative Staphylococcus (21.0%, n: 4), Enterococcus spp. (15.8%, n: 3), S. aureus (10.5%, n: 2) and Streptococcus spp. (10.5%, n: 2). Pseudomonas aeruginosa (21.0%, n: 4), Acinetobacter baumannii (10.5%, n: 2) and Klebsiella pneumoniae (10.5%, n: 2). None of them was classified as MDR. These data are detailed in Table 3.
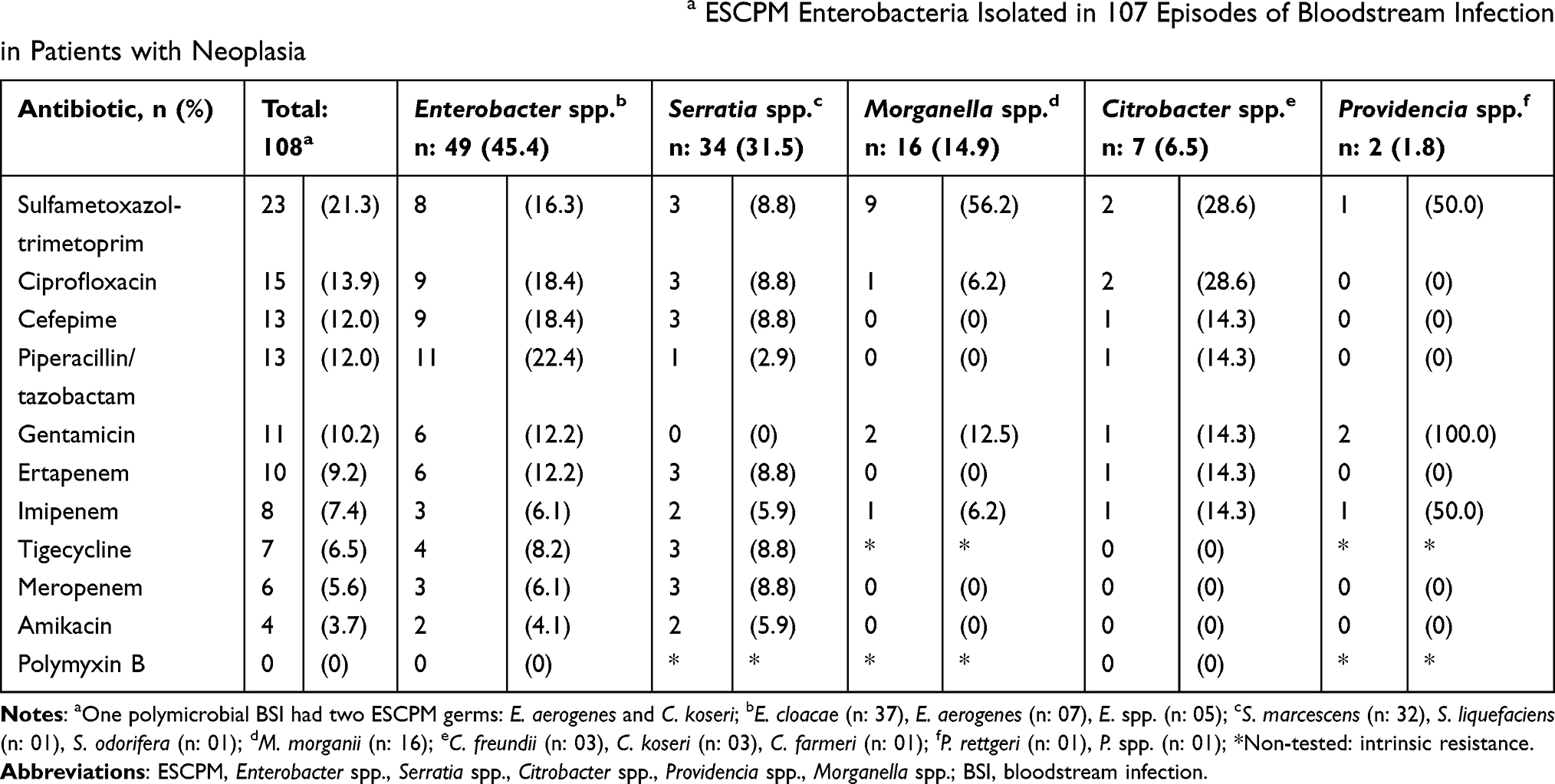 |
Table 3 The Frequency of Antimicrobial Resistance of 108a ESCPM Enterobacteria Isolated in 107 Episodes of Bloodstream Infection in Patients with Neoplasia |
Discussion
In this cohort of BSI caused by the ESCPM group in patients with neoplasia, the 7-day (9.3%) and 30-day (21.5%) mortalities were high. In addition, BSIs caused by MDR-ESCPM were independently associated with 7-day death. A tendency of association between the use of monotherapy with piperacillin-tazobactam and 7-day as well as 30-day deaths was observed.
A relevant proportion of patients with cancer without possibility of cure (36.4%) was present in this study. The frequency of males was higher than females (67.0% vs 33.0%), and the median age was 63 years. Patients with SOTs, mainly intra-abdominal cancer, were more frequent than hematological neoplasms (67.0% vs 33.0%) in this cohort. Likewise, male preponderance (58.5%) was found in another study of BSIs caused by many agents performed in children and adults with cancer, done in the same hospital in 2004.11 In such a study, a greater proportion (59%) of the patients with SOTs was also observed, which could be explained by the higher number of patients with SOT assisted in our hospital. Similarly, in another cohort of BSI in patients with SOTs performed in Greece also published in 2004,12 47% of the episodes occurred in men and the median age was 64 years. Finally, an American cohort of BSI caused by AmpC-producing organisms published in 2018 found male predominance (60.0%) and median age of 57 years.13 These data suggest that the occurrence of BSI caused by ESCPM may prefer elderly males.
Considering the setting of immunosuppression, almost half of the cases of BSI we described were related to previous corticosteroid therapy (47.7%), and febrile neutropenia was present in 14.9% of the BSI episodes. Similarly, a prospective Spanish cohort done from January 2006 to July 2012 including 528 episodes of BSI due to several agents in patients with SOTs found neutropenia in 15.0% of the cases and previous corticosteroid therapy in 41.0%.14 The low frequency of patients with neutropenia present in our cohort could be explained by the predominance of patients with SOT. Once, these patients usually have low frequency and duration of neutropenia since their underlying disease does not affect the bone marrow and chemotherapy for SOT tends to have less myelotoxicity. In addition, corticosteroids are often part of the therapeutic regimens for neoplasms, which would explain the high proportion of patients using these medications.
Most of the cases were H-BSI (70.1%). Patients with neoplasia have humoral and cellular immune dysfunction, disruption of cutaneomucosal barriers in addition to the use of intravascular devices, chemotherapy and radiotherapy.4 Consequently, they can require hospitalization several times during the treatment of their underlying disease, which can explain the high frequency of hospital acquired infection by this population. The proportions of primary BSI and BSI secondary to an extravascular site of infection were similar. Among the BSIs secondary to extravascular foci, intra-abdominal source predominated (19.6%). In primary BSI, episodes associated with long-term (14.1%) and short-term (13.1%) vascular catheters were more frequent. Similarly, a retrospective cohort of BSI caused by ESCPM group published in 2020 including patients with several underlying diseases found a high proportion (59.8%) of hospital acquired BSIs.15 In that study, BSIs secondary to an extravascular site of infection also prevailed (63.5%), although the main origin was the urinary tract (22.8%). Noteworthy is the similar frequency of BSIs associated with vascular catheters found in that cohort and ours (22.0% vs 27.2%). Once the ESCPM group bacteria compose the intestinal microbiota and most of the BSI episodes in this cohort occur in patients with SOTs, mainly intra-abdominal, it is not surprising the occurrence of elevated proportion of BSI secondary to intra-abdominal source. In addition, this group of bacteria has been reported causing CLA-BSI,16 which could be explained by a shift in cutaneous microbiota in favor of colonization by these agents.
Microbiological Profile and Susceptibility to Antimicrobials
The frequencies of each ESCPM group bacteria found in the present study were similar to those described in other cohorts15 of BSI caused by these agents, with a predominance of Enterobacter spp. (45.4%) and Serratia spp. (31.5%) followed by Morganella spp. (14.9%), Citrobacter spp. (6.5%) and Providencia spp. (1.8%).
The overall frequency of resistance to sulfamethoxazole-trimethoprim (21.3%), ciprofloxacin (13.9%), cefepime (12%) and piperacillin-tazobactam (12%) was higher than other antibiotics. The highest prevalence of resistance to sulfamethoxazole-trimethoprim (56.2%) was observed in Morganella morganii isolates, while the greatest frequency of resistance to piperacillin-tazobactam (22.4%) and cefepime (18.4%) were detected among Enterobacter spp. isolates. The prevalence of resistance to amikacin was low (3.7%), and all isolates of Morganella morganii, Citrobacter freundii and Providencia spp. were susceptible to this antimicrobial. Differently, in another cohort of BSIs caused by AmpC-producing bacteria, the highest frequency of resistance to sulfamethoxazole-trimethoprim (22%) was observed in isolates of Citrobacter spp. However, the frequency of resistance to piperacillin-tazobactam among Enterobacter spp. was very similar to ours, 20.0%.1 In that cohort, tobramycin was the aminoglycoside tested against Citrobacter spp. (10.0%), Morganella spp. (13%) and Providencia spp. (13%) presenting elevated frequency of resistance and the susceptibility to amikacin was not evaluated.1 This was the only cohort of BSI that evaluated the susceptibilities of AmpC-producing bacteria for different classes of antimicrobials we found and could compare data with ours. Once piperacillin-tazobactam was widely used as empiric therapy for patients with severe serious infections in the present study, the high frequency of resistance detected in this antimicrobial may be associated with an inappropriate therapy and consequently increase the risk of death. According to our data, amikacin would be an excellent option to treat infections caused by ESCPM group bacteria due to the low frequency of resistance to it. It is worth noting that this antimicrobial has reduced activity in acid, and anaerobic environments, therefore, could be an inappropriate choice for abscesses and collections such as BSI secondary to peritonitis. It is not clear if the profile of antimicrobial susceptibility described among ESCPM bacteria in the present study represents a tendency that could be applied to guide antimicrobial therapy in other settings. However, it highlights the necessity of additional studies to better understand the susceptibility profile of ESCPM group bacteria to improve the therapeutic approaches.
The frequency of BSIs caused by MDR-ESCPM found in this study was 9.3%. The definition of MDR we applied was when the bacteria showed resistance to at least one agent in three or more classes of antimicrobials, except for those with intrinsic resistance such as polymyxin, tigecycline, gentamicin and imipenem. Thus, the resistance to aminoglycosides, cefepime, fluoroquinolones, meropenem and sulfamethoxazole-trimethoprim was considered for the definition of MDR. We consider the prevalence of MDR-ESCPM detected was elevated once this group of bacteria already had intrinsic resistance to several antimicrobials considered the last line of therapy for many MDR agents and this level of resistance can impact patients’ prognosis. Thus, easily, ESCPM group can emerge as pan-resistant microorganisms. The present study was the only cohort of BSIs caused by ESCPM bacteria to use this MDR definition that we are aware of. Thereby, it was not possible to compare these results with other studies. Additional studies to investigate the tendency of antimicrobial resistance occurrence among this group of bacteria, considering this classification of MDR agents, are of utmost importance.
The proportion of polymicrobial BSIs in the present study was elevated (15.9%). All isolated pathogens in addition to ESCPM bacteria were susceptible to the tested antibiotics. Consequently, this finding did not influence the adequacy of the empirical antimicrobial therapy. Similarly, an Australian cohort of BSIs caused by ESBL and AmpC-producing bacteria published in 201917 found a frequency of polymicrobial infections of 11.8%. To our knowledge, other cohorts1,13,15 of ESCPM group enterobacteria excluded BSIs caused by more than one germ, which precluded additional comparisons with ours. In fact, infections with source in sites colonized by several microorganisms can be polymicrobial, leading to the growth of more than one germ in blood culture. Thus, by including polymicrobial BSIs, the present study approaches the “true life” found in patients undergoing treatment of BSIs.
Outcomes, Treatment and Risk Factors
In the present study, the 7-day mortality was 9.3%. Differently, an American cohort of BSIs caused by the ESCPM group published in 2018 found a lower 7-day mortality (3.8%) than ours.13 Some differences between the characteristics of the population and BSI episodes included in both studies could explain the higher mortality found in the study we have done. The American cohort was carried out in a general hospital, included only 23.4% of immunosuppressed patients and the median Pitt score was 3 (2–3), denoting less serious infections. Unlike, in the present cohort, the entire population was composed of patients with neoplasia and 30.8% of the BSI cases required life support in the ICU, indicating greater severity of the BSI episodes. Furthermore, in the American cohort, there was a predominance of primary BSIs associated with vascular catheter (37.9%) and BSI secondary to the urinary tract (13.6%), considered low-risk BSIs (51.5%) associated with mortality less than 30%.3 In contrast, in the present cohort, only 38.4% of the BSIs included were of low risk, which corresponded to the primary BSIs associated with vascular catheter (27.2%) added to the BSIs secondary to urinary tract (11.2%). In this cohort, the 30-day mortality was 21.5%, which we considered an elevated value in comparison with a Canadian cohort of BSI caused by AmpC-producing bacteria where a 30-day mortality of 13% was described.1 In this Canadian study, only 18% of the patients presented cancer, which could partially explain the lower mortality found. The severity of the BSI episodes was not stratified, which prevented additional comparisons. These data suggest 7-day and 30-day mortalities in patients with cancer complicated with BSI caused by ESCPM bacteria group are higher than in the general population.
The BSIs caused by MDR-ESCPM were independently associated with 7-day mortality in our study. The only other cohort of BSIs caused by this group of bacteria that evaluated 7-day mortality we are aware did not analyze the determinant factors of death.13 Thus, it was not possible to compare our findings with others. We consider 7-day mortality as an outcome related to the BSI if any other causes of death were not detected, and directly influenced by multidrug resistance. This finding is ratified by the fact that the association between MDR-ESCPM BSI and 30-day mortality was not detected. As our acknowledgement, the association between MDR-ESCPM BSI and 7-day mortality was not detected in any other study so far. The association between BSIs caused by MDR Gram-negative bacteria in general and mortality has already been shown in other studies.18,19 Although these studies did not include exclusively BSI caused by ESCPM bacteria and used different MDR definitions, they reinforce our findings.
The overall proportion of inappropriate therapy was high (46.7%), mainly because of the antibiotic beginning after the day of the BSI diagnosis. The frequency of inappropriate therapy was similarly high in dead patients and alive patients, within 7 days and 30 days after the BSI diagnosis, which could explain why it was not found to be a risk factor for death. Nevertheless, the elevated frequency of inappropriate therapy we have found is worrisome, once it could influence the outcome of patients with high-risk BSI as previously described.3
The use of piperacillin-tazobactam for treatment of BSI caused by ESCPM bacteria group was not considered inappropriate when the bacteria isolated was susceptible to this antibiotic in the antibiogram, in spite of the acknowledgment that piperacillin-tazobactam is a poor AmpC inhibitor2 and consequently could be associated with treatment failure. This approach was applied because the reliability of the treatment of ESCPM bacteria BSI with piperacillin-tazobactam remains an open issue20 and we wanted to evaluate this aspect of the treatment of the ESCPM group BSI. A trend of association of piperacillin-tazobactam monotherapy with 7-day and 30-day mortalities was detected, which has biological plausibility, since this antibiotic can be hydrolyzed by AmpC produced by ESCPM group.2 This trend of association can be related to an insufficient sample size to achieve enough power to detect the true effect of piperacillin-tazobactam on death. Thus, additional studies including a larger population are necessary to clarify this issue.
The present study has some limitations. The external validity of the findings may be limited since it is a single-center study. It is not possible to collect data that would allow filling in the PITT score, which is commonly used to measure the severity and prognosis of BSIs. In addition, it was not possible to gather data to fulfill the sepsis criteria. However, to make up those limitations we used the necessity of life support in the ICU as criteria of severity. Another limitation would be that different bacterial species were studied together. Nevertheless, some biological characteristics of these species can vary, their main mechanisms of resistance to antibiotics are similar, allowing us to study them as a group. Maybe, some determinant factors of death could not be detected due to the small sample size. Despite these limitations, all cases of BSIs due to ESCPM group enterobacteria that occurred during the study period were analyzed. Few studies have analyzed risk factors for early (7-day) and late (30-day) deaths in BSI caused by this group of enterobacteria. Finally, this study brings unprecedented data suggesting that MDR-ESCPM group bacteria is an independent risk factor for 7-day mortality of BSI, at least in patients with cancer. This finding needs to be confirmed for this population and for immunocompetent individuals.
Acknowledgments
This work was supported in part by Fundação Carlos Chagas Filho de Amparo à Pesquisa (FAPERJ # E-26/211-554/2019).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chaubey VP, Pitout JDD, Dalton B, Gregson DB, Ross T, Laupland KB. Clinical and microbiological characteristics of bloodstream infections due to AmpC β-lactamase producing Enterobacteriaceae: an active surveillance cohort in a large centralized Canadian region. BMC Infect Dis. 2014;14(1):647. doi:10.1186/s12879-014-0647-4
2. Jacoby GA. AmpC β-lactamases. Clin Microbiol Rev. 2009;22(1):161–182. doi:10.1128/CMR.00036-08
3. Kang CI, Kim SH, Park WB, et al. Bloodstream infections caused by antibiotic-resistant gram-negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome. Antimicrob Agents Chemother. 2005;49(2):760–766. doi:10.1128/AAC.49.2.760-766.2005
4. Gudiol C, Tubau F, Calatayud L, et al. Bacteraemia due to multidrug-resistant Gram-negative bacilli in cancer patients: risk factors, antibiotic therapy and outcomes. J Antimicrob Chemother. 2011;66:657–663. doi:10.1093/jac/dkq494
5. Center for Disease Control and Prevention. Bloodstream infection event (central line-associated bloodstream infection and non-central line-associated bloodstream infection); 2020. Available from: http://www.cdc.gov/nhsn/.
6. Mackenzie CR A new method of classifying prognostic comorbidity in longitudinal studies: development and validation; 1987. Available from: http://appliedresearch.cancer.gov/seermedicare/program/charlson.pdf.
7. Friedman ND, Kaye KS, Stout JE, et al. Health care-associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med. 2002;137(10):791–797. doi:10.7326/0003-4819-137-10-200211190-00007
8. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of America. Clin Infect Dis. 2011;52:e56–e93.
9. Garrido M. Fatores De Risco Para Óbito Relacionado Às Infecções De Corrente Sanguínea Em Pacientes Pediátricos Com Doença Oncológica [Tese De Mestrado] [Risk factors of death related to bloodstream infection in pediatric patients with oncological disease [Master thesis]]. Rio de Janeiro: Instituto Nacional de Câncer José Alencar Gomes da Silva; 2017. Portuguese.
10. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
11. Velasco E, Byington R, Martins CSA, Schirmet M, Dias LCM, Gonçalves VMSC. Bloodstream infection surveillance in a cancer centre: a prospective look at clinical microbiology aspects. Clin Microbiol Infect. 2004;10(6):542–549. doi:10.1111/j.1469-0691.2004.00874.x
12. Anatoliotaki M, Valatas V, Mantadakis E, et al. Bloodstream infections in patients with solid tumors: associated factors, microbial spectrum and outcome. Infection. 2004;32(2):65–71. doi:10.1007/s15010-004-3049-5
13. McKamey L, Venugopalan V, Cherabuddi K, et al. Assessing antimicrobial stewardship initiatives: clinical evaluation of cefepime or piperacillin/tazobactam in patients with bloodstream infections secondary to AmpC-producing organisms. Int J Antimicrob Agents. 2018;52(5):719–723. doi:10.1016/j.ijantimicag.2018.08.007
14. Marín M, Gudiol C, Garcia-Vidal C, Ardanuy C, Carratalà J. Bloodstream infections in patients with solid tumors: epidemiology, antibiotic therapy, and outcomes in 528 episodes in a single cancer center. Medicine. 2014;93(3):143–149. doi:10.1097/MD.0000000000000026
15. Tan SH, Ng TM, Chew KL, et al. Outcomes of treating AmpC-producing Enterobacterales bacteraemia with carbapenems vs. non-carbapenems. Int J Antimicrob Agents. 2020;55(2):105860. doi:10.1016/j.ijantimicag.2019.105860
16. Sievert DM, Ricks P, Edwards JR, et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections summary of data reported to the national healthcare safety network at the centers for disease control and prevention, 2009–2010. Infect Control Hosp Epidemiol. 2013;34(1):1–14. doi:10.1086/668770
17. Lim CL, Spelman D. Mortality impact of empirical antimicrobial therapy in ESBL- and AmpC-producing Enterobacteriaceae bacteremia in an Australian tertiary hospital. Infect Dis Health. 2019;24(3):124–133. doi:10.1016/j.idh.2019.02.001
18. Sostarich AM, Zolldann D, Haefner H, Luetticken R, Schulze-Roebecke R, Lemmen SW. Impact of multiresistance of gram-negative bacteria in bloodstream infection on mortality rates and length of stay. Infection. 2008;36(1):31. doi:10.1007/s15010-007-6316-4
19. Kadri SS, Lai YL, Ricotta EE, et al. External validation of difficult-to-treat resistance prevalence and mortality risk in gram-negative bloodstream infection using electronic health record data from 140 US hospitals. Open Forum Infect Dis. 2019;6(4):ofz110. doi:10.1093/ofid/ofz110
20. Aitken SL, Foolad F, McDaneld PM. Should piperacillin-tazobactam be used as definitive therapy against Enterobacteriaceae harboring inducible AmpC β-lactamases? Antimicrob Agents Chemother. 2017;61(9):e01160–17. doi:10.1128/AAC.01160-17
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.