")
Back to Journals » Journal of Asthma and Allergy » Volume 15
Risk Factors of Childhood Asthma Among Patients Attending a Tertiary Care Centre in North-East India
Authors Deka H, Mahanta P , Ahmed SJ, Rajbangshi MC, Konwar R, Basumatari B
Received 18 May 2022
Accepted for publication 31 August 2022
Published 14 September 2022 Volume 2022:15 Pages 1293—1303
DOI https://doi.org/10.2147/JAA.S374007
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Himamoni Deka,1 Putul Mahanta,2 Sultana Jesmin Ahmed,3 Madhab Ch Rajbangshi,4 Ranjumoni Konwar,5 Bharati Basumatari5
1Depatment of Anatomy, Gauhati Medical College, Guwahati, Assam, India; 2Department of Forensic Medicine and Toxicology, Assam Medical College, Dibrugarh, Assam, India; 3Department of Community Medicine, Assam Medical College, Dibrugarh, Assam, India; 4Department of Surgery, Tezpur Medical College and Hospital, Tezpur, Assam, India; 5Department of Radiology, Fakhruddin Ali Ahmed Medical College and Hospital, Barpeta, Assam, India
Correspondence: Putul Mahanta, Department of Forensic Medicine and Toxicology, Assam Medical College and Hospital, Dibrugarh, Assam, 786002, India, Tel +919435017802, Email [email protected]
Introduction: Asthma is a chronic lung illness marked by a reversible airway blockage. Both genetic and environmental factors influence higher asthma rates. The present study aims to assess the various socio-demographic and environmental factors influencing the causation of childhood asthma among patients attending the Paediatric Department of Gauhati Medical College and Hospital (GMCH), Assam.
Materials and Methods: A total of 150 clinically diagnosed asthma patients of 3– 12 years as cases and patients of the same age group free from respiratory diseases with no history of asthma in a 1:1 ratio as controls were selected. A predesigned and pretested proforma was used to collect data, and written informed consent was obtained from all the legal guardians of the participants. Data were analyzed by chi-square test and binary logistic regression using SPSS V20, considering a p-value < 0.05 significant.
Results: Urban and male children were found to be at higher risk of developing asthma. Children belonging to the urban locality (OR= 4.53; 95% CI: 1.57– 13.09; p< 0.05), damp environment (OR= 5.21; 95% CI: 1.23– 22.10; p< 0.05), lower socioeconomic status (OR= 3.48; 95% CI: 1.34– 9.01; p< 0.05), presence of pets (OR= 6.77; 95% CI: 1.76– 25.99; p< 0.05), family history of atopy/ allergy (OR= 43.29; 95% CI: 5.80– 323.15 p< 0.05), smoking/passive smoking (OR=23.54; 95% CI: 1.41– 394.21 p< 0.05) and mixed feeding (OR= 4.47; 95% CI: 1.46– 13.63 p< 0.05) were the significant risk factors of childhood asthma.
Conclusion: Children are vulnerable to environmental-induced asthma. Awareness and preventive measures are necessary to control and reduce the burden of childhood asthma.
Keywords: asthma, environmental factors, children, allergy, atopy
Introduction
Asthma is a chronic lung illness marked by reversible airway blockage caused by inflammation of the lungs’ airways and tightness of the muscles around them. The recent Global Initiative for Asthma (GINA) guidelines defined asthma as “a heterogeneous disease, usually characterized by chronic airway inflammation.” Respiratory symptoms such as wheezing, shortness of breath, chest tightness, and cough, as well as fluctuating expiratory airflow limitation, are the characterizations of asthma.1
In asthmatics, severe symptoms can develop due to several triggers like cigarette and other smoking, moulds, pollen, dust, animal dander, exercise, cold air, domestic and industrial goods, air pollution, and infections.2 Both genetic and environmental factors combine and interact to explain the higher asthma rates in some communities. Often, these other factors may cause a disparity, with race or ethnicity being the factor that is easier to detect between different populations.3
The diagnosis of asthma is a clinical one as there is no standardized definition of the type, severity or frequency of symptoms. Asthma is a common condition producing a significant workload for general medical practice and hospital admissions.4 Although there are many shared features in the diagnosis of asthma in children and adults, the differential diagnosis, the natural history of wheezing illnesses, the ability to perform specific investigations, and their diagnostic value are all influenced by age.
Worldwide more than 300 million people have asthma. Among children, it is one of the top 20 chronic conditions for the global ranking of disability-adjusted life years, with a mortality rate ranging from 0.0–0.7 per 100,000.5 In India, the prevalence of asthma was reported to be ranging from 2% to 23% which may be due to the enormous geographical and environmental variations across the country.6 In a recent study, it was found as 10.4% in Assam.7
Asthma in children causes recurrent respiratory symptoms of wheezing, cough, difficulty breathing and chest tightness and can lead to chronic asthma if not treated adequately. Childhood asthma may increase school absenteeism, decrease active participation in work and thus significantly impair the quality of life of the affected child.
Despite advanced understanding and therapeutic strategies, a dramatic increase in prevalence, morbidity and mortality of childhood asthma has been noted in recent years8,9 necessitating a further understanding of asthma pathogenesis for efficient asthma management. Although many research works are happening in different parts of India, minimal research has been conducted in this underdeveloped region of the north-eastern part of India.
The present study was conducted in the state of Assam, a northeast part of India. The population of Assam constitutes various racial stocks, of which 12.45% belong to the tribal communities like Bodo, Kachari, Karbi, Miri, Mishimi, Rabha, etc. The rural zones are scattered in most of the areas of this region. The state is well known for its biodiversity. Agriculture, primarily rice, tea and pulses, contributes to more than a third of Assam’s income and employs about 69% of the workforce. The state produces 50% of India’s tea production. The other profitable agribusinesses include Pig Farming, Dairy farming, and Fishery businesses involving the rural population. Agriculture, tea, oil and natural gas, coal, and limestone are the major industrial areas. The state’s vast ethnic and geographic variation is significantly attributed to the diverse disease dynamics and pathogenesis factors.
GMCH is a leading tertiary referral centre in this region, and the attending patients belong to the entire North-eastern regions of India, comprising both rural and urban populations. Most patients were from lower socioeconomic status and had low education levels. Childhood asthma is a commonly encountered problem in the paediatric department in the hospital.
The study aims to assess the various socio-demographic and environmental factors influencing the causation of childhood asthma among patients aged 3–12 years attending the paediatric department of GMCH.
Materials and Methods
The retrospective case-control study was conducted in the anatomy department, in collaboration with the department of paediatrics, GMCH, Assam, from April 2013 to March 2017 to investigate childhood asthma’s socio-demographic and environmental factors among paediatric patients aged 3–12 years.
An unmatched case-control study was conducted with 150 cases and 150 controls selected at a 1:1 ratio to study the various factors of childhood asthma. Clinically diagnosed asthma patients of 3–12 years attending outdoor and indoor department of paediatrics were selected as cases, while controls were patients of the same age group preferably residing in a similar environment free from respiratory diseases and having no history of asthma.
The sample size was determined using WinPepi version 11.65. Baseline survey data reveals that childhood asthma ranges from 1 to 4% in India. Therefore, assuming the proportion of childhood asthma as 1% and equal group sizes among cases and controls, the study would require a total sample size of 274 to achieve a power of 80% for detecting a two-way difference in proportions of 4% between the two groups with a 5% level of the significance.
Further assuming about 10% of non-respondent due to following up loss or noncompliance, it was reasonable to draw a sample of 300 constituting 150 cases and 150 controls.
A predesigned and pretested proforma was used to collect data. Written informed consent was obtained from all the legal guardians of the study participants. Data on different socio-demographic and environmental variables were collected. Housing types are defined as
Pucca housing if both walls and roof are made up of bricks, cement, and stones; Katcha housing is made up of wood, mud, straw and dry leaves and Semi pucca housing if the house is made with brick walls and thatched roof or a house with tinned roof mud walls and concrete floor. Socioeconomic status was accessed on a modified Kuppuswamy scale (2014).
Participants’ personal history on the mode of delivery, history of birth asphyxia, type of feeding, history of food allergy, history of mother’s addiction, family history of asthma, atopy or allergy and family history of smoking or passive smoking were also documented. Any family members residing in the same dwelling were considered about family smoking history. Disease severity was classified based on prescribed treatment step as per GINA guidelines for descriptions of participants in epidemiological studies and clinical trials, considering patients prescribed Step 2 treatments as having mild asthma, those prescribed Step 3–4 treatments as having moderate asthma and that prescribed step-5 treatment as having severe asthma.
Inclusion and exclusion criteria: The literature suggests paediatric cases should be included for up to 18 years. Still, in GMCH, most cases attending the Paediatric Department were up to 12 years of age. Furthermore, around puberty, a disease outgrows place for childhood asthma. So, the age group selected for the study was 3–12 years. Clinically diagnosed asthma patients in the age group of 3–12 years who consented to participate in the study during the study period were included as cases. Children of 3–12 years free from respiratory diseases, preferably residing in a similar environment, who gave consent to participate in the study were selected as controls.
Children of 0–3 years were excluded from the study, as a child presenting with wheeze in this age group is not chronic enough to diagnose it as asthma. Also, Children in the relevant age group and their guardians who failed to consent to participate in the study were excluded.
Statistical analysis: Differences in proportions were analyzed using the χ2 test. Binary logistic regression was used to the significant parameters of Univariate analysis, and Wald χ 2 test was used to measure the independent contribution of exposure.
Ethical approval: The ethical clearance was taken from the ethics committee of the institute, viz., Institutional Ethics Committee of GMCH, Guwahati, Assam and India, before collecting the data vide ref: No: 233/2018/215.
Results
Out of the total 112,323 patients attending the paediatric department during the study period, 18.88% were respiratory patients. Among the paediatric patients in the age group 3–12 years, 2.96% were asthmatic. Most childhood asthma cases were reported during the autumn months of September and October (Figure 1).
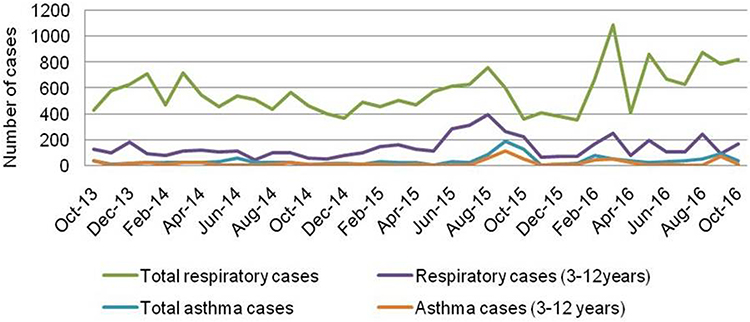 |
Figure 1 Month-wise distribution of patients (OPD+IPD). |
Symptomatic Profile of the Selected Cases
The present case-control study recruited 150 childhood asthma cases and 150 controls. The mean (±standard deviation) age of the study participants was 8.38(±2.69) years. Cough and difficulty in breathing were the most common clinical symptom in the cases. The majority (77.3%) of cases had episodic asthma attacks, and only 8.7% of cases had severe asthma. The preponderance of the cases was reported during the autumn season (30%). Almost 38% of cases reported the occurrence of the symptoms at night-time (Table 1).
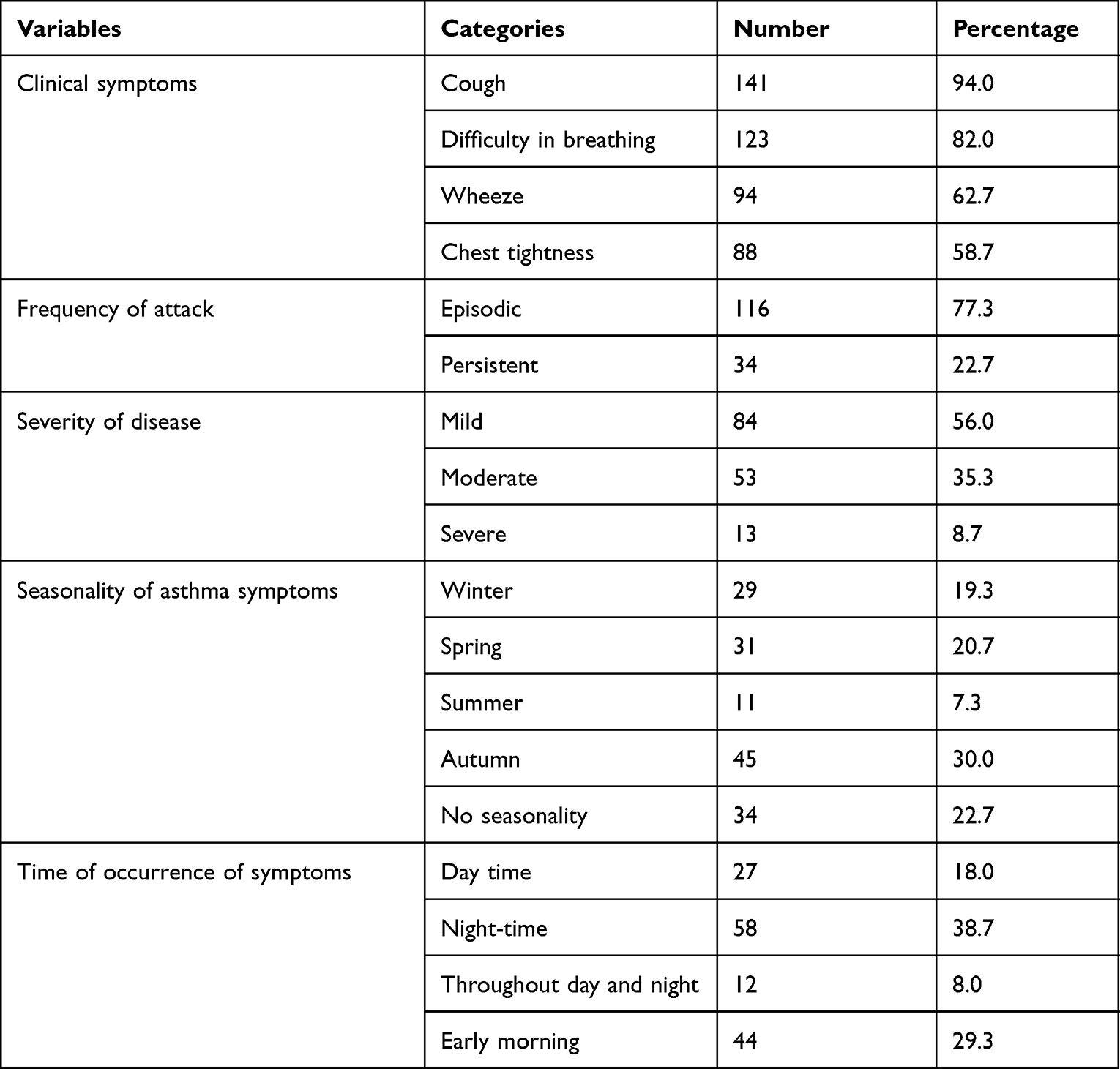 |
Table 1 Symptomatic Analysis of the Selected Asthma Cases (n=150) |
As per the respondents’ perceptions, cold drinks (82.7%), ice cream (71.6%), and exposure to dust (35%) were the common precipitating factors of asthma. Almost 19.3% of the cases reported school absenteeism due to the disease.
Socio-Demographic and Environmental Factors of Childhood Asthma
The participants’ mean age (standard deviation) was 8.34(2.69) years. Most cases belonged to the age group 7–12 years and were males. The study participants were primarily Hindu and non-tribal.
It is observed that children of 7–12 years and the male had higher odds of having the disease, although the association was not statistically significant. Also, childhood asthma was significantly associated with BMI (p-value<0.05). Overweight (OR= 2.22, 95% C.I.:1.17–4.18) and obese (OR=2.72, 95% C.I.:1.46–5.09) had more than two times higher odds of having the disease compared to children with normal weight. Urban children living in joint families, kaccha houses, and damp dwellings with inadequate ventilation had substantially higher odds of getting the disease. In attached kitchens, smoke-producing fuels other than LPG, mosquito repellents, Dhuna, etc., are also significantly associated with childhood asthma (p-value<0.05). It has also been observed that children who had pets in their houses had eight times higher risk of Asthma (Table 2).
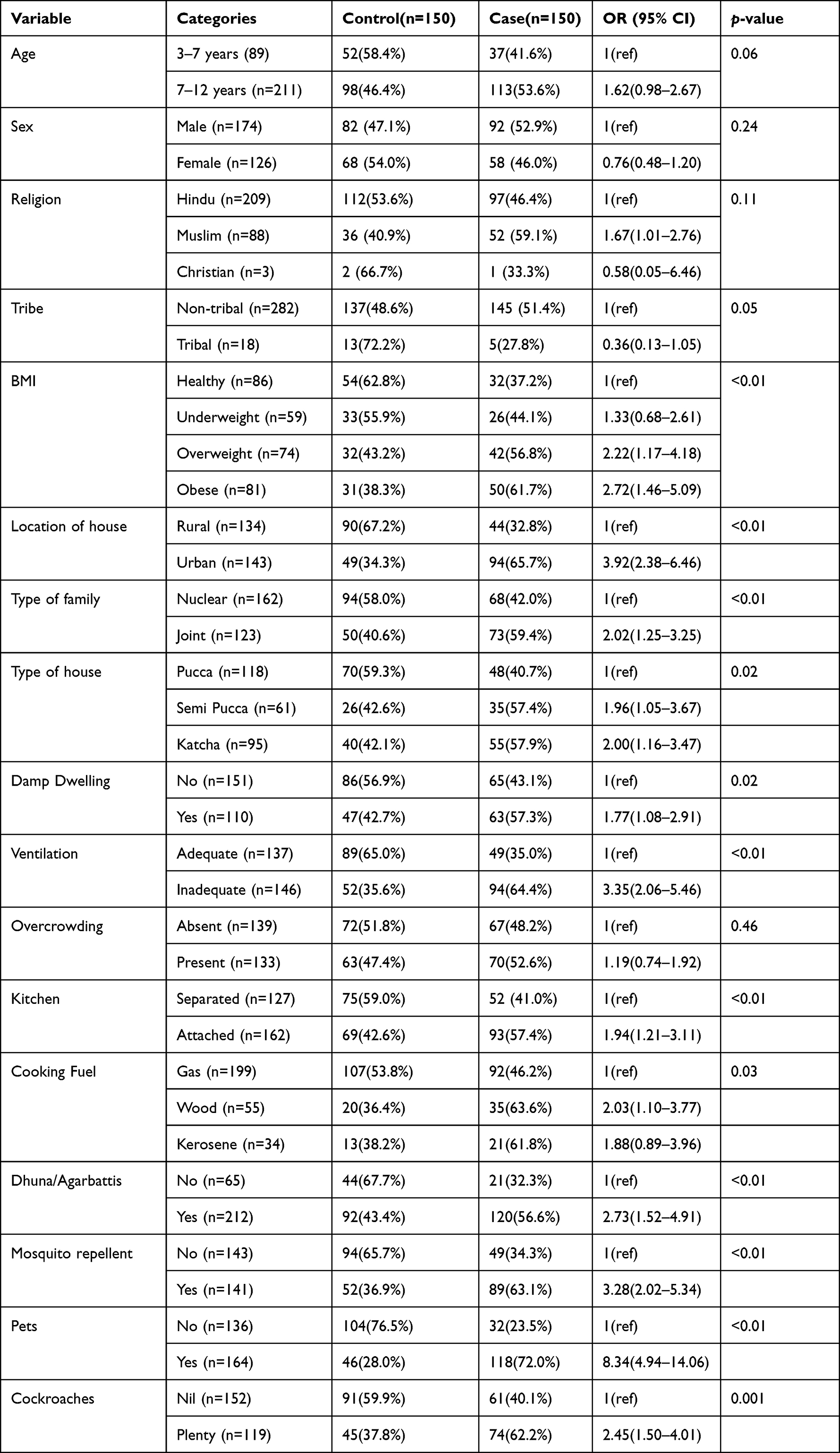 |
Table 2 Socio-Demographic and Environmental Profiles of Cases and Controls |
As seen in Table 3, 46.7% of cases belonged to a lower socioeconomic family. Maternal education was also lower among the cases (p-value<0.05).
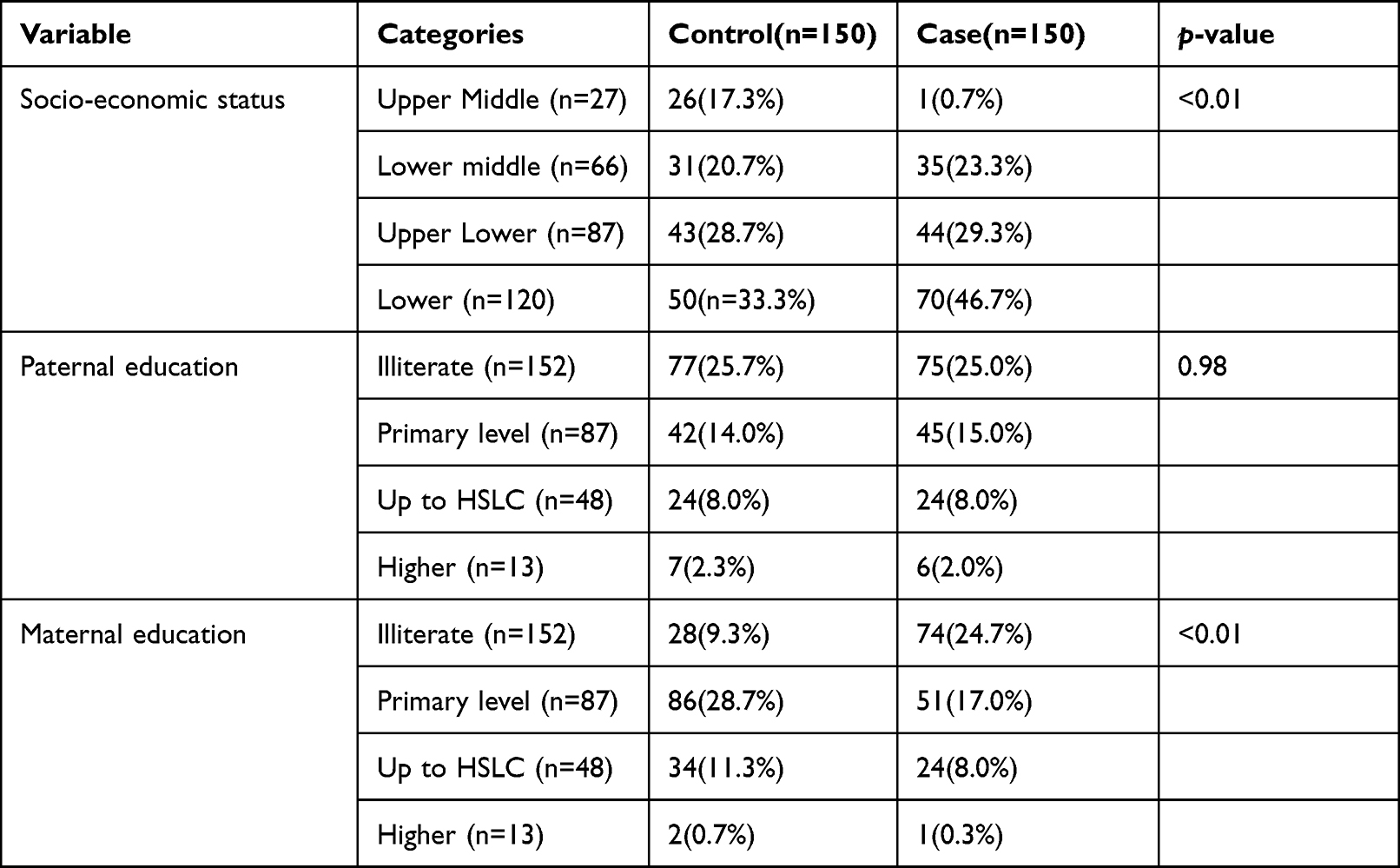 |
Table 3 Socioeconomic and Parental Educational Status Among Cases and Controls |
Birth and Feeding History and Its Relation to Childhood Asthma
Children born by Caesarean Section (CS) or another mode of delivery and children with a history of birth asphyxia had a higher risk of developing the disease. Furthermore, top-fed/mixed-fed children are at almost five times higher risk of the disease than breastfed children (Table 4).
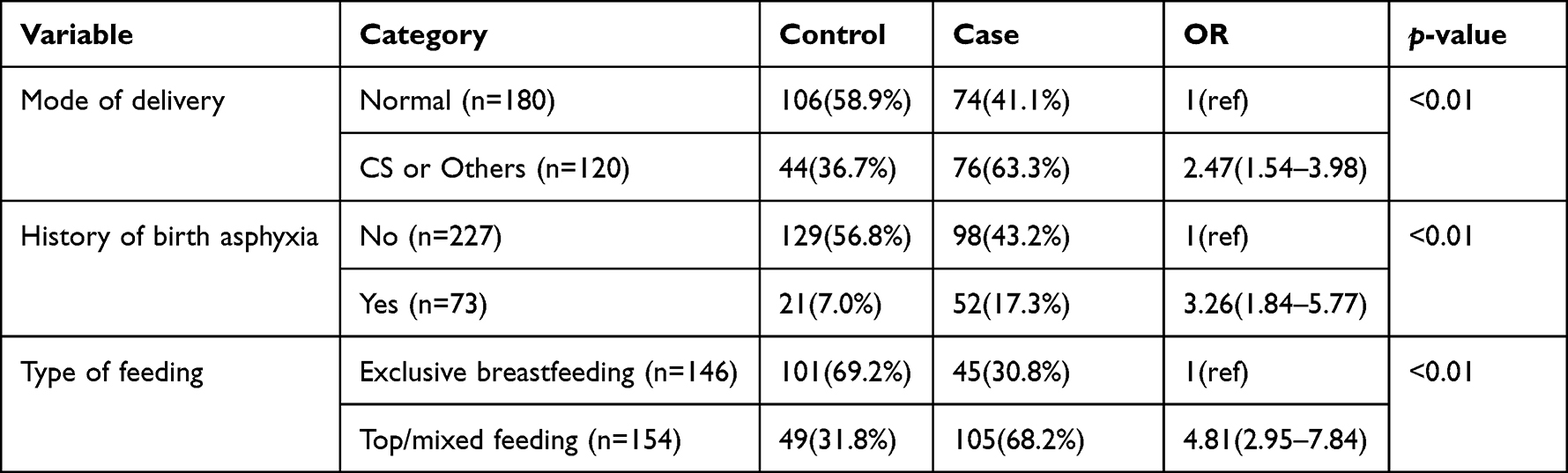 |
Table 4 Birth and Feeding History Among Cases and Controls |
Association of History of Allergy and Substance Use with Childhood Asthma
Children’s history of food allergy and atopy are significantly associated with childhood asthma. Also, children from families with a history of allergy and asthma (p-value<0.05) were highly prone to getting the disease. Passive smoking through other family members also increased almost eight times the risk of asthma among children (p-value<0.05). (Table 5)
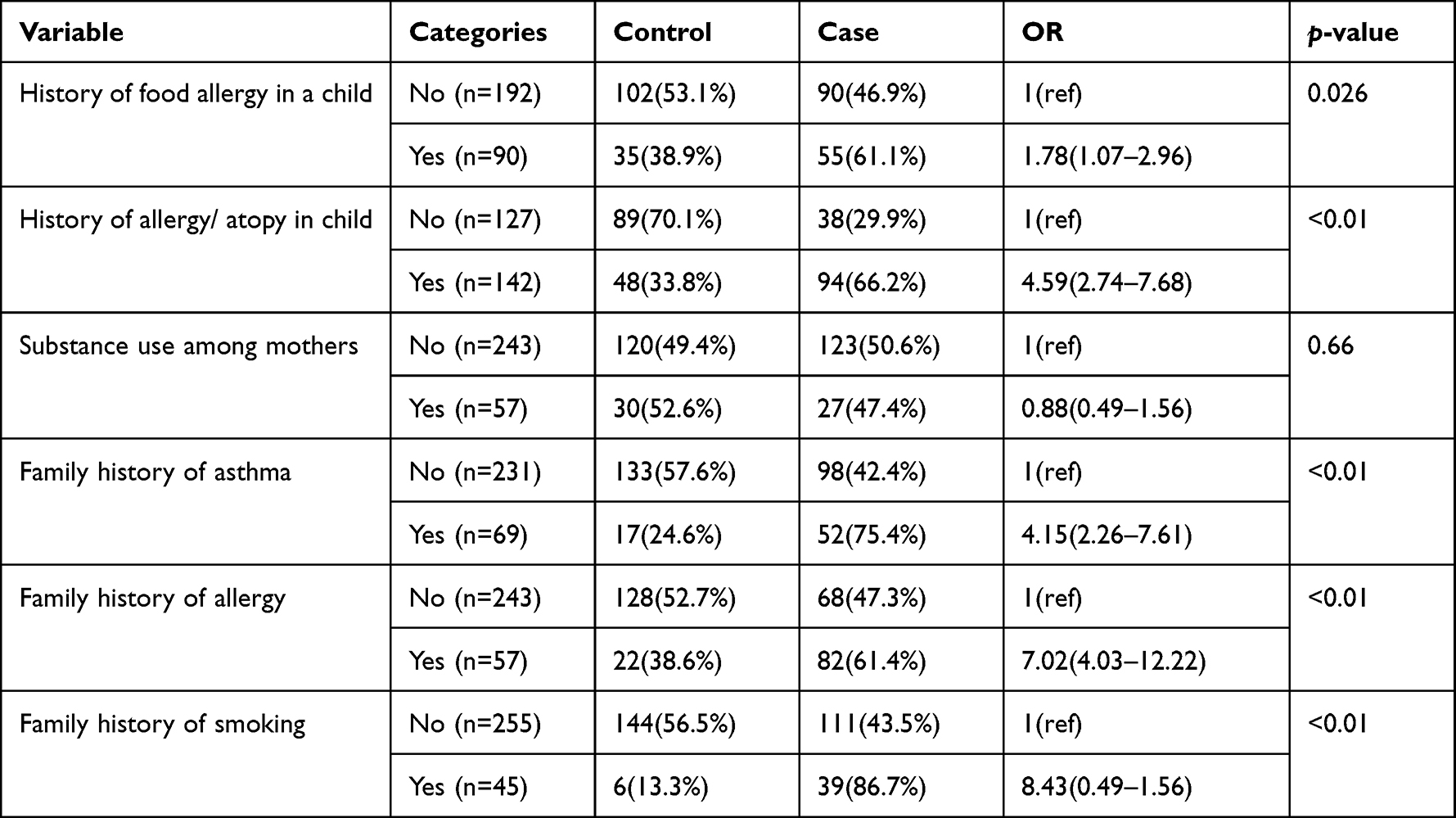 |
Table 5 History of Allergy and Substance Use Among Cases and Controls |
The multivariate binary logistic regression revealed that children belonging to the urban locality, dampness in dwelling environment, lower socioeconomic status, presence of pets in the household, family history of atopy/allergy, family history of smoking/passive smoking and mixed feeding were the significant risk factors of childhood asthma (Table 6).
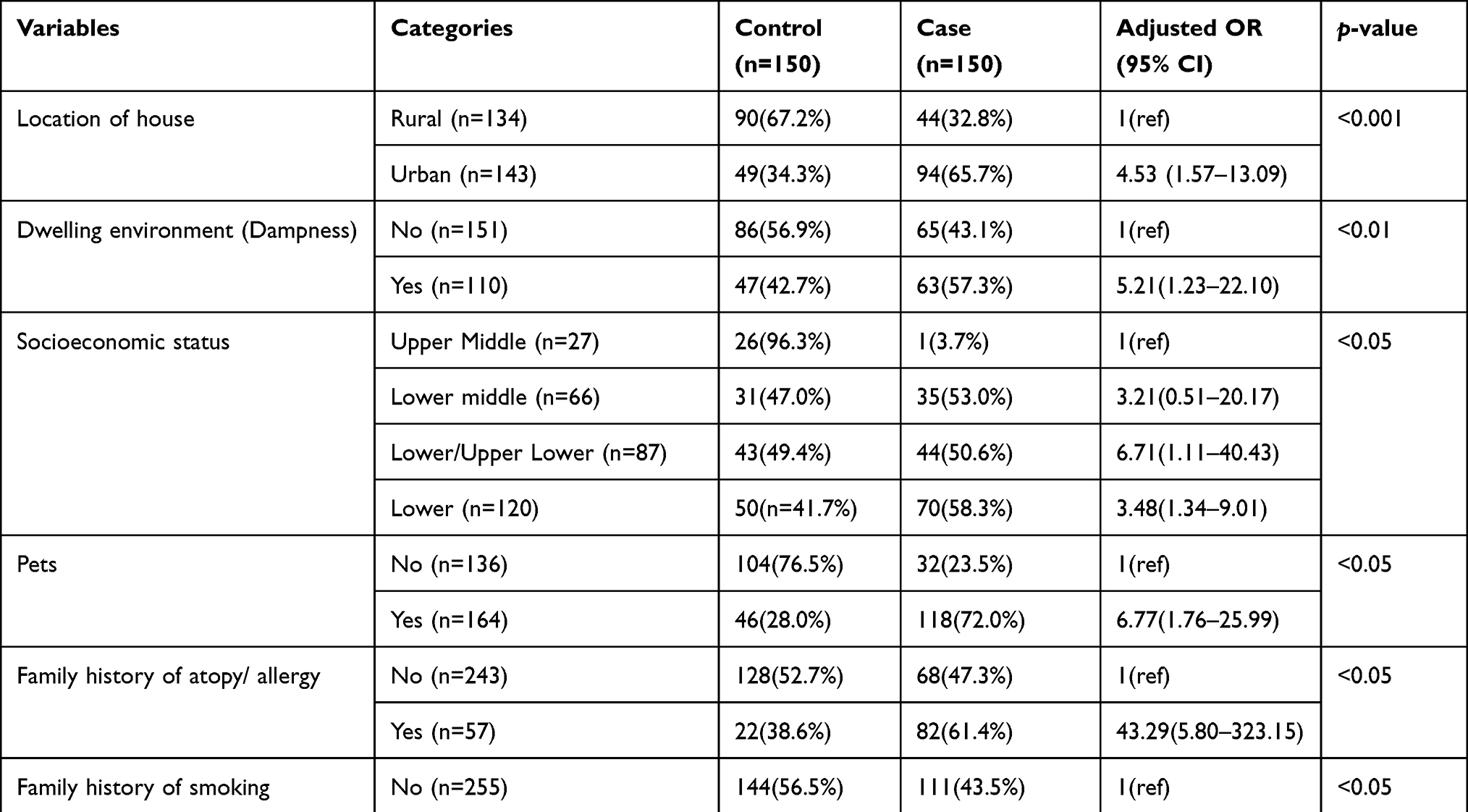 |
Table 6 Multivariate Logistic Regression Analysis to Assess the Significant Factors Affecting Childhood Asthma |
Discussion
Over the past two to three decades, atopic disorders have been rising, prompting much discussion about the changing environment, pollution, and immune responses to infectious pathogens. Environmental exposures and underlying biological and genetic vulnerabilities all have a role in developing asthma.
In the present study, childhood asthma was reported in 2.96% of the patients in the 3–12 years age group. However, some previous studies have reported a varied range of childhood asthma in Indian children.6,10–12 The geographical and environmental disparity across India directly interacts with and interferes with the risk factors associated with the incidence of asthma.6 Therefore, region-specific assessment of the potential factors of childhood asthma is necessary for suitable and timely disease prevention.
Children in the age group 7–12 years, males and those from urban areas, were at higher risk of childhood asthma. Urban and male predominance in asthma prevalence was observed in an Indian study,10 similar to our findings. However, the association was only statistically significant in the case of the house’s location.
Studies suggest that sex-specific hormonal changes affect asthma, as boys are more likely to develop asthma in childhood. However, this pattern altered after puberty, with females getting the disease more often than males.13–15 Also, a male child under ten years has a smaller airway size than a female child of the same age and body stature is also considered a factor responsible for childhood asthma among male children.16,17
Kamrup metro, the capital of Assam, has shown rapid urbanization in recent years. Many studies have reported urbanization as a factor affecting asthma incidence agrees with our study.18,19 In the present study, unadjusted logistic regression revealed that overweight and obese children had significantly two times higher chances of having the disease than children with normal BMI, which agrees with a recent review.20 Also, the lower socioeconomic status was a potential risk factor for childhood asthma. Children from low socioeconomic families are at more risk of asthma due to lower immunologic responses and lower health care resources.21–23
Children living in a joint family, kaccha houses, damp dwellings, inadequate ventilation, attached kitchens, smoke-producing fuels, mosquito repellents and Dhuna, etc., were significantly associated with childhood asthma (p-value<0.05). Prior studies have also suggested that the various indoor house environment factors may trigger childhood asthma.24–27 The indoor allergen due to pets and its association with childhood asthma is debatable as few researchers also suggest that early exposure to allergens may help in achieving tolerance.28
Various studies have reported an increased risk of childhood asthma among children born by Caesarian Section delivery compared to those born by normal delivery. This agrees with our findings.29–32 Children with a history of birth asphyxia are also at higher risk of developing asthma. Maternal asthma was a significant factor in pregnancy complications like respiratory distress syndrome and newborns’ asphyxia.33
Similar to other studies, the present findings suggest that a history of food allergy or atopy in children or a family history of allergy and asthma increases the risk of childhood asthma substantially.34,35 In line with our study, an earlier multi-generational study suggested that generation-wise smoking habits may result in heritable alteration of the epigenome, increasing the risk of asthma among future generations.36
Rapid urbanization has been affecting all segments of society in recent days. People often prefer to settle in the city due to different income-generating and occupational sources and are thus exposed to various environmental pollutants. More awareness towards avoiding dampness, smoking, pets in the households of atopic/allergic persons, and avoidance of allergy/ atopy precipitating factors with a child having a family history of allergy/atopy are recommended for family members of the susceptible child. Exclusive breastfeeding awareness should be generated about the benefits of breastfeeding for the prevention of asthma.
Most of the patients coming to Gauhati Medical College belonged to the entire North-eastern region of India, as Gauhati Medical College is a premier tertiary referral centre in this region. Most patients belong to lower socioeconomic status and have low education levels. Childhood asthma is a commonly encountered problem in the Paediatric department in our hospital. Proper preventive strategies in these high-risk patients will help reduce disease and decrease the precipitation of acute attacks.
Despite all the available treatments for controlling asthma, numerous affected people remain insufficiently controlled, but identifying specific patient populations, both phenotypes and endotypes, may optimize their management. Hence, a region-wise study on childhood asthma’s prevalence and risk factors will be instrumental to competently managing these cases.
Limitation
Some patients did not return for further investigations and follow-up in the present study. It may be due to a lack of awareness about the disease’s aetiology and consequences. We were unable to trace all the patients because of poor communication systems.
Conclusion
Children are susceptible to environment-induced asthma, and proper awareness of the environmental triggers of asthma and allergens may help control and reduce the burden of the disease. In families with a history of allergy or asthma, proper care should ensure the susceptible child is free from the triggering factors.
Ethics
All data were treated confidentially, and the study was conducted following the Declaration of Helsinki.
Acknowledgments
Thanks to all the faculty members of the paediatric department who have helped collect the data and evaluate its intellectual content. All departmental colleagues who helped us access the departmental library and settings during the study were also acknowledged.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; they took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report that there are no conflicts of interest in this work.
References
1. Global Strategy for Asthma Management and Prevention. Global initiative for asthma. 2018. Available from: https://ginasthma.org/wp-content/uploads/2019/01/2018-GINA.pdf.
2. Asthma and children fact sheet. American Lung Association. Available from: www.https://www.lung.org/lung-health-diseases/lung-disease-lookup/asthma/learn-about-asthma/asthma-children-facts-sheet.
3. Drake KA, Galanter JM, Burchard EG. Race, ethnicity and social class and the complex etiologies of asthma. Pharmacogenomics. 2008;9(4):453–462. doi:10.2217/14622416.9.4.453
4. Lakhanpaul M, Bird D, Culley L, et al. The use of a collaborative structured methodology for the development of a multifaceted intervention programme for the management of asthma (the MIA project), tailored to the needs of children and families of South Asian origin: a community-based, participatory study. Southampton (UK): NIHR Journals Library; 2014 Sep. (Health Services and Delivery Research, No. 2.28.) Chapter 1, Overview and background of the Management and Interventions for Asthma project. Available from: https://www.ncbi.nlm.nih.gov/books/NBK260072/.
5. Asher I, Pearce N. Global burden of asthma among children. Int J Tuberc Lung Dis. 2014;18(11):1269–1278. doi:10.5588/ijtld.14.0170
6. Bhalla K, Nehra D, Nanda S, Verma R, Gupta A, Mehra S. Prevalence of bronchial Asthma and its associated risk factors in school-going adolescents in Tier-III North Indian City. J Family Med Prim Care. 2018;7(6):1452–1457. doi:10.4103/jfmpc.jfmpc_117_18
7. Sarma J, Sarmah KR Prevalence of Asthma and allergic rhinitis among school-going children (6-14 years) in Kamrup district, Metro, Assam, India. Available from: https://apiassam.com/admin/files/ajim_january_2016.pdf.
8. Braman SS. The global burden of asthma. Chest. 2006;130(1 Suppl):4S–12S. doi:10.1378/chest.130.1_suppl.4S
9. Serebrisky D, Wiznia A. Pediatric Asthma: a Global Epidemic. Ann Glob Health. 2019;85(1):6. doi:10.5334/aogh.2416
10. Pal R, Dahal S, Pal S. Prevalence of bronchial asthma in Indian children. Indian J Community Med. 2009;34(4):310–316. doi:10.4103/0970-0218.58389
11. Sharma BS, Kumar MG, Chandel R. Prevalence of Asthma in urban school children in Jaipur, Rajasthan. Indian Pediatr. 2012;49(10):835–836. doi:10.1007/s13312-012-0188-0
12. Kumar GS, Roy G, Subitha L, Sahu SK. Prevalence of bronchial Asthma and its associated factors among school children in urban Puducherry, India. J Nat Sci Biol Med. 2014;5(1):59–62. doi:10.4103/0976-9668.127289
13. Osman M. Therapeutic implications of sex differences in asthma and atopy. Arch Dis Child. 2003;88(7):587–590. doi:10.1136/adc.88.7.587
14. Almqvist C, Worm M, Leynaert B. working group of GA2LEN WP 2.5 Gender. Impact of gender on asthma in childhood and adolescence: a GA2LEN review. Allergy. 2008;63(1):47–57. doi:10.1111/j.1398-9995.2007.01524.x
15. Naeem A, Silveyra P. Sex Differences in Paediatric and Adult Asthma. Eur Med J. 2019;4(2):27–35.
16. Becklake MR, Kauffmann F. Gender differences in airway behaviour over the human life span. Thorax. 1999;54(12):1119–1138. doi:10.1136/thx.54.12.1119
17. Trivedi M, Denton E. Asthma in children and adults-what are the differences and what can they tell us about asthma? Front Pediatr. 2019;7:256. doi:10.3389/fped.2019.00256
18. Robinson CL, Baumann LM, Romero K, et al. Effect of urbanization on asthma, allergy and airways inflammation in a developing country setting. Thorax. 2011;66(12):1051–1057. doi:10.1136/thx.2011.158956
19. Rodriguez A, Brickley E, Rodrigues L, Normansell RA, Barreto M, Cooper PJ. Urbanization and asthma in low-income and middle-income countries: a systematic review of the urban-rural differences in asthma prevalence. Thorax. 2019;74(11):1020–1030. doi:10.1136/thoraxjnl-2018-211793
20. Azizpour Y, Delpisheh A, Montazeri Z, Sayehmiri K, Darabi B. Effect of childhood BMI on Asthma: a systematic review and meta-analysis of case-control studies. BMC Pediatr. 2018;18(1):143. doi:10.1186/s12887-018-1093-z
21. Hedlund U, Eriksson K, Rönmark E. Socioeconomic status is related to incidence of asthma and respiratory symptoms in adults. Eur Respir J. 2006;28(2):303–310. doi:10.1183/09031936.06.00108105
22. Kozyrskyj AL, Kendall GE, Jacoby P, Sly PD, Zubrick SR. Association between socioeconomic status and the development of asthma: analyses of income trajectories. Am J Public Health. 2010;100(3):540–546. doi:10.2105/AJPH.2008.150771
23. Chen E, Shalowitz MU, Story RE, et al. Dimensions of Socioeconomic Status and Childhood Asthma Outcomes: evidence for Distinct Behavioral and Biological Associations. Psychosom Med. 2016;78(9):1043–1052. doi:10.1097/PSY.0000000000000392
24. Richardson G, Eick S, Jones R. How is the indoor environment related to asthma?: literature review. J Adv Nurs. 2005;52(3):328–339. doi:10.1111/j.1365-2648.2005.03591.x
25. Phipatanakul W. Environmental factors and childhood asthma. Pediatr Ann. 2006;35(9):646–656. doi:10.3928/0090-4481-20060901-08
26. Rao D, Phipatanakul W. Impact of environmental controls on childhood asthma. Curr Allergy Asthma Rep. 2011;11(5):414–420. doi:10.1007/s11882-011-0206-7
27. Wang T, Zhao Z, Yao H, et al. Housing characteristics and indoor environment in relation to children’s asthma, allergic diseases and pneumonia in Urumqi, China. Chin Sci Bull. 2013;58:4237–4244. doi:10.1007/s11434-013-5727-0
28. Dharmage SC, Perret JL, Custovic A. Epidemiology of Asthma in Children and Adults. Front Pediatr. 2019;7:246. doi:10.3389/fped.2019.00246
29. Kero J, Gissler M, Grönlund MM, et al. Mode of delivery and asthma – is there a connection? Pediatr Res. 2002;52(1):6–11. doi:10.1203/00006450-200207000-00004
30. Almqvist C, Cnattingius S, Lichtenstein P, Lundholm C. The impact of birth mode of delivery on childhood asthma and allergic diseases-A sibling study. Clin Exp Allergy. 2012;42(9):1369–1376. doi:10.1111/j.1365-2222.2012.04021.x
31. Darabi B, Rahmati S, HafeziAhmadi MR, Badfar G, Azami M. The association between caesarean section and childhood asthma: an updated systematic review and meta-analysis. Allergy Asthma Clin Immunol. 2019;15:62. doi:10.1186/s13223-019-0367-9
32. Rusconi F, Zugna D, Annesi-Maesano I, et al. Mode of Delivery and Asthma at School Age in 9 European Birth Cohorts. Am J Epidemiol. 2017;185(6):465–473. doi:10.1093/aje/kwx021
33. Mendola P, Männistö TI, Leishear K, Reddy UM, Chen Z, Laughon SK. Neonatal health of infants born to mothers with asthma. J Allergy Clin Immunol. 2014;133(1):85–90.e904. doi:10.1016/j.jaci.2013.06.012
34. Liu T, Valdez R, Yoon PW, Crocker D, Moonesinghe R, Khoury MJ. The association between family history of asthma and the prevalence of Asthma among US adults: national Health and Nutrition Examination Survey, 1999-2004. Genet Med. 2009;11(5):323–328. doi:10.1097/GIM.0b013e31819d3015
35. Paaso EM, Jaakkola MS, Rantala AK, Hugg TT, Jaakkola JJ. Allergic diseases and asthma in the family predict the persistence and onset-age of asthma: a prospective cohort study. Respir Res. 2014;15(1):152. doi:10.1186/s12931-014-0152-8
36. Accordini S, Calciano L, Johannessen A, et al. A three-generation study on the association of tobacco smoking with asthma. Int J Epidemiol. 2018;47(4):1106–1117. doi:10.1093/ije/dyy031
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.