")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Risk Factors of Birth Asphyxia Among Neonates Born in Public Hospitals of Tigray, Northern Ethiopia
Authors Berhe YZ, Kebedom AG , Gebregziabher L , Assefa NE , Berhe LZ, Mohammednur SA, Wellay T, Berihu G, Welearegay AT, Mitiku M , Teka HG
Received 17 September 2019
Accepted for publication 14 December 2019
Published 8 January 2020 Volume 2020:11 Pages 13—20
DOI https://doi.org/10.2147/PHMT.S231290
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Yodit Zewdie Berhe,1 Abel Gidey Kebedom,2 Letekirstos Gebregziabher,1 Natnael Etsay Assefa,3 Lidya Zewdie Berhe,4 Sumeya Ahmed Mohammednur,1 Tsegay Wellay,1 Gebregziabher Berihu,1 Alemtsehay Tewele Welearegay,1 Mengistu Mitiku,1 Hareya Gebremedhin Teka1
1School of Public Health, College of Health Science, Mekelle University, Tigray, Ethiopia; 2School of Medicine, College of Health Science, Mekelle University, Tigray, Ethiopia; 3Department of Midwifery, College of Medicine and Health Science, Adigrat University, Tigray, Ethiopia; 4School of Medicine, College of Health Science and Medicine, Bahir Dar University, Amhara, Ethiopia
Correspondence: Yodit Zewdie Berhe
School of Public Health, College of Health Science, Mekelle University, PO Box: 1871, Tigray, Ethiopia
Tel +251 910 695771
Fax +251 344416681
Email [email protected]
Introduction: Birth asphyxia is defined by the World Health Organization as not initiating and maintaining default breathing at birth. Approximately 24% of neonatal deaths occurred annually worldwide due to birth asphyxia. About 3% of the 120 million neonates born each year acquire asphyxia in third world countries. Long-term survivors may experience cerebral palsy, delay in growth, vision, hearing and intellectual deficiency, epilepsy, difficulties with communication and behavior. Thus, this study aims to determine the risk factors of birth asphyxia among neonates who were delivered at public hospitals of Tigray, Ethiopia.
Materials and Methods: Hospital-based unmatched case-control study design was implemented on 390 samples from January to February 2018. Data were collected by interviews using a structured questionnaire and checklist. The collected data were coded and entered using EpiData version 3.1 statistical software and transported to statistical package for social science (SPSS) version 20 software for analysis. Cross-tabulation and odds ratio with 95% confidence interval were computed. Bivariate logistic regression and multivariable logistic regression were done. Multicollinearity was checked. Goodness of fit was checked by the Hosmer–Lemeshow test.
Results: A total of 260 controls and 130 cases were enrolled in the study. Multivariable logistic regression showed that Primi-parity [AOR 5.5 (CI: 2.5, 12.3)], pre-eclamcia/pregnancy-induced hypertension [AOR12.4 (CI: 4.17, 37.15)], post-term pregnancy [AOR 2.73 (CI: 1.00, 7.55)] meconium-stained liquor [AOR 29.2 (CI: 12.0, 71.1)], cord entangled [AOR 5.67 (CI: 1.66,19.3)] and non-vertex presentation [AOR 5.49 (CI: 2.20,13.7)] were found to be risk factors for perinatal birth asphyxia.
Conclusion and Recommendations: Intrapartum factors and neonatal factors in the index pregnancy have an association with perinatal birth asphyxia. The research finding suggests effective antenatal care follow-up and follow-up of labor progress using partograph after labor initiation.
Keywords: perinatal asphyxia, neonates, intrapartum, antepartum, Tigray
Introduction
Birth asphyxia is one of the leading causes of newborn death.1,2 Many developing countries have experienced significant declines in deaths below five, though neonatal deaths, with an estimated 3 million annual neonatal deaths, remained stagnant.3,4 According to the Millennium Development Goal (MDG) 4, which has not been met due to the lack of significant reductions in neonatal mortality, neonatal death has gained prominence on the international child survival policy agenda over the past decade. It was projected that a two-thirds reduction in child mortality by 2015, as mandated by the MDG, requires a reduction of at least 50% in neonatal mortality.5
The World Health Organization (WHO) defines birth asphyxia as a failure to trigger and sustain breathing automatically at birth.6 It is a disease that results in hypoxemia (lack of oxygen) and hypercapnia (accumulation of carbon dioxide) when there is a loss of blood-gas exchange.7
High maternal and perinatal mortality occurs in sub-Saharan Africa. Ethiopia is one of the high perinatal mortality countries in Sub-Sahara, accounting for 4% of the world’s perinatal mortality.8 Birth asphyxia in this area is the leading cause of early neonatal death due to poor obstetric care.9 Neonatal mortality rates in Ethiopia were 29 per 1000 live births according to the 2016 Ethiopian Demographic Health Survey (EDHS). Neonatal mortality in Tigray (where this study is conducted) is 34 per 1,000 live births.10 This study was conducted to identify factors that lead to birth asphyxia in the study area. Identification of risk factors and early initiation of therapy thereby can decrease neonatal mortality and morbidity.
Materials and Methods
Study Setting and Period
The study was conducted from March to June, 2018, at four public general and tertiary hospitals of Tigray. Tigray Region is the northernmost of the nine regions of Ethiopia and its capital is Mek’ele. Tigray is bordered by north by Eritrea, west by Sudan, east by the Afar region and south and southwest by the Amhara region. The region is divided administratively into 7 zones including Mekelle, a special zone. It has 52 Woredas (34 rural and 18 urban areas) and 799 Kebelles/Tabias (722 rural and 77 Urban areas). The region has an estimated population of 5.055.999 based on the 2007 census conducted by the Central Statistical Agency of Ethiopia (CSA).
Public health services are provided in Tigray through one specialist hospital, one referral hospital, 15 general hospitals, 22 primary hospitals, 213 health centers and 712 police posts. Through investing in primary health care units or PHCU (health post, health center, and primary hospital) services, the area has demonstrated its focus on disease prevention and health promotion, achieving primary health care coverage of 91.7% on average. More than 500 private health facilities, including two general hospitals, offer additional curative care.
Study Design
Hospital-based unmatched case-control study.
Study Population
All neonates with their mothers who were born at the selected hospitals during the data collection period were study population. Cases were neonates who were diagnosed with birth asphyxia by the attending physician. Diagnostic criteria for asphyxia were no breathing, gasping, cyanosis and Breathing with difficulty APGAR score of <7 at 1 min. Controls were neonates who were born normal (without asphyxia) confirmed by the attending physician who cry, breath without difficulty and no gasping APGAR score ≥7 at 1 min. An exclusion criterion was newborns who were born with congenital malformation incompatible with life.
Sample Size and Sampling Technique
The sample size was calculated using EPI INFO version 3.5.1 StatCalc statistical software using the Double population formula for unmatched case-control study by considering the proportion of non-vertex presentation in control group 82.9% with OR 2.96 from a study done at Pakistan. With assumption of 95% CI, 80% power, control to case ratio 2:1 the sample size will be 371. By adding 5% non-response rate, the total sample size becomes 390 (260 controls and 130 cases). Hospitals were selected randomly and the sample size was allocated proportionally based on a case flow.
Data Quality Control
Structured questionnaire and checklists were used. Data collectors were trained. Data collection was supervised. The questionnaire was written in English and translated into Tigrigna, which is the study area’s local language. Language experts then translated it back to English to see its consistency. Senior researchers updated the questionnaire and suggestions implemented accordingly. The tool has also been tested in the hospital with similar status.
Data Management and Analysis
The collected data were coded, entered and cleaned using EpiData version 3.1 statistical software. Then, it was transported to SPSS version 20 statistical software for analysis. Tables and text were used for descriptive statistics. Frequency and percentage were used for the categorical variable. Median and interquartile range was computed. Cross-tabulation was performed to see the distribution of the independent variables in relation to the dependent variable. Odds ratio with 95% confidence interval was used to measure the strength of association. The bivariate logistic regression model was used to see the association between the independent variables and the dependent variable. Variables with a P< 0.25 at the bivariate regression were exported to the multivariable logistic regression model to control confounding factors and to see the independent predictor of Asphyxia. Statistical significance was declared at P< 0.05. Goodness of fit will be checked by Hosmer–Lemeshowthe test. Multicollinearity was checked.
Ethical Considerations
Ethical approval was received from Mekelle University College of Health Sciences institutional review board. After briefing on the study’s intent and protocol, mothers were asked if they and their newborn were willing to participate and written and signed consent was obtained. Data collectors respected their right not to participate, not to answer any or all of the questions and to withdraw from the interview whenever they wanted. Participants were told that the information obtained from them would be kept confidential.
Results
Socio-Demographic Characteristics
A total of 130 asphyxiated neonates with their mothers and 260 non-asphyxiated neonates with their mothers were included. The median age of the mothers for the case and control was 25 (IQR=8) and 26 (IQR=7) respectively. Slightly more than two-thirds of cases 90 (69.2%) had no formal education as compared to about two-thirds of controls 170 (65.4%) were more than secondary or higher education. Regarding mothers' occupation, 46 (35%) of cases and 123 (47.3%) of controls were housewives. The proportion of participants earning <1000 Ethiopian birr was higher in the cases than controls (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Cases and Controls Attending at Public Hospitals of Tigray, Ethiopia 2017/2018 |
Antepartum Characteristics
Half of the mothers in cases 66 (50.8%) were prim-gravida while about two-thirds of control 159 (61.2%) were prim-gravida. A majority of cases 101 (82.8%) and control 226 (87.9%) had ANC follow-up. Nearly one-fifths of the 25 (19.2%) cases were also found to be pre-eclamptic, while only 8 (3.1%) of controls were pre-eclamptic. Fourteen (10.8%) of cases had multiple births, while only 10 (3.8%) of controls had multiple births. The proportions of history of abortion and previous neonatal death in controls were slightly higher than the cases. Regarding the history of stillbirth, only 4 (3.1%) of cases and 3 (1.2%) of controls experienced stillbirth (Table 2).
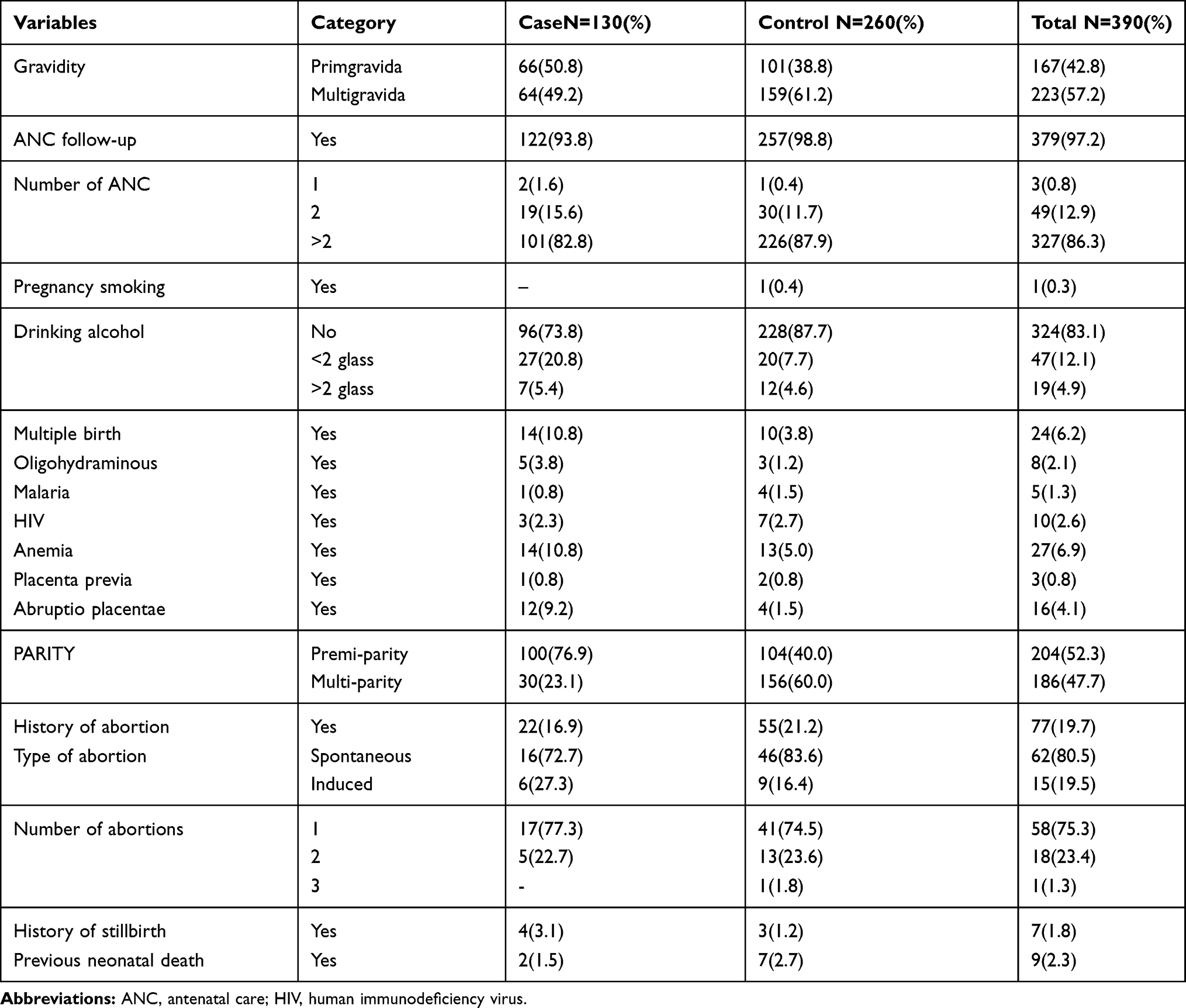 |
Table 2 Antepartum-Related Characteristics of Women Among Cases and Controls Attending at Public Hospitals of Tigray, Ethiopia 2017/2018 |
Intrapartum-Related Characteristics
In majority of cases [113 (86.9%)] and controls [344 (88.2%)], the labor was started spontaneously without medication. Regarding the duration of labor, 48 (36.9%) of cases and 76 (29.2%) of controls had greater than 18 hrs duration of labor. Fifty-nine (45.4%) cases involving mother and 68 (26.2%) cases involving non-cases involving mother birth by caesarian delivery. Sixty-nine (53.1%) of cases and 13 (5%) of control had meconium-stained liquor (Table 3).
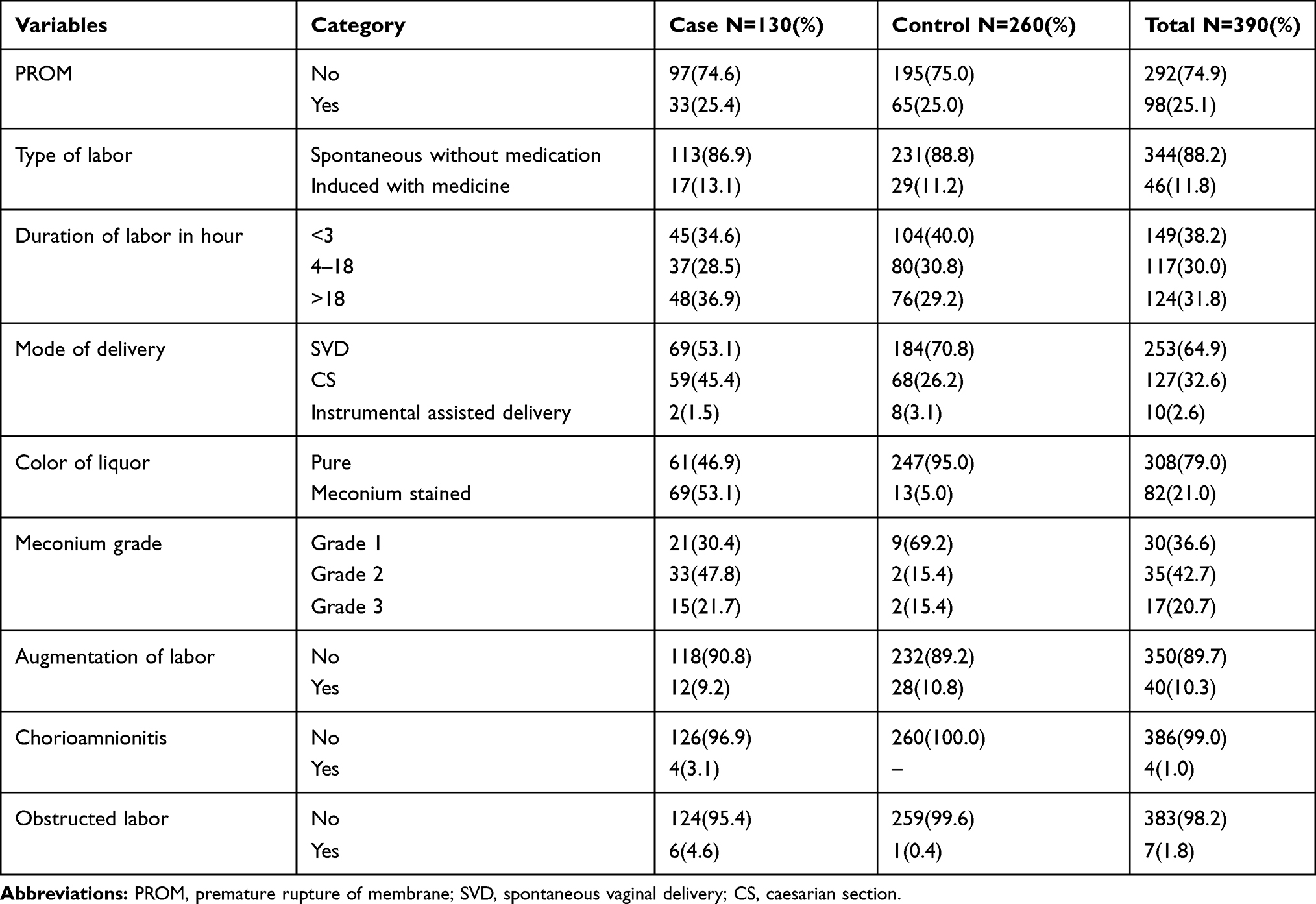 |
Table 3 Intrapartum-Related Characteristics (Risks) of Women Among Cases and Controls Attending at Public Hospitals of Tigray, Ethiopia 2017/2018 |
Neonatal Characteristics
Eighteen (16.1%) of case neonates and around one-quarter of control [57 (24.4%)] neonates were under normal gestational age interval. Almost half of the study participants were preterm. More than three-quarters of 102 (78.5%) cases and more than two-thirds of 80 (30.8%) neonates were not under normal birth weight interval. Regarding nuchal cord, 15 (11.5%) of case neonate and 16 (6.2%) of controls had entangled cord around their neck (Table 4).
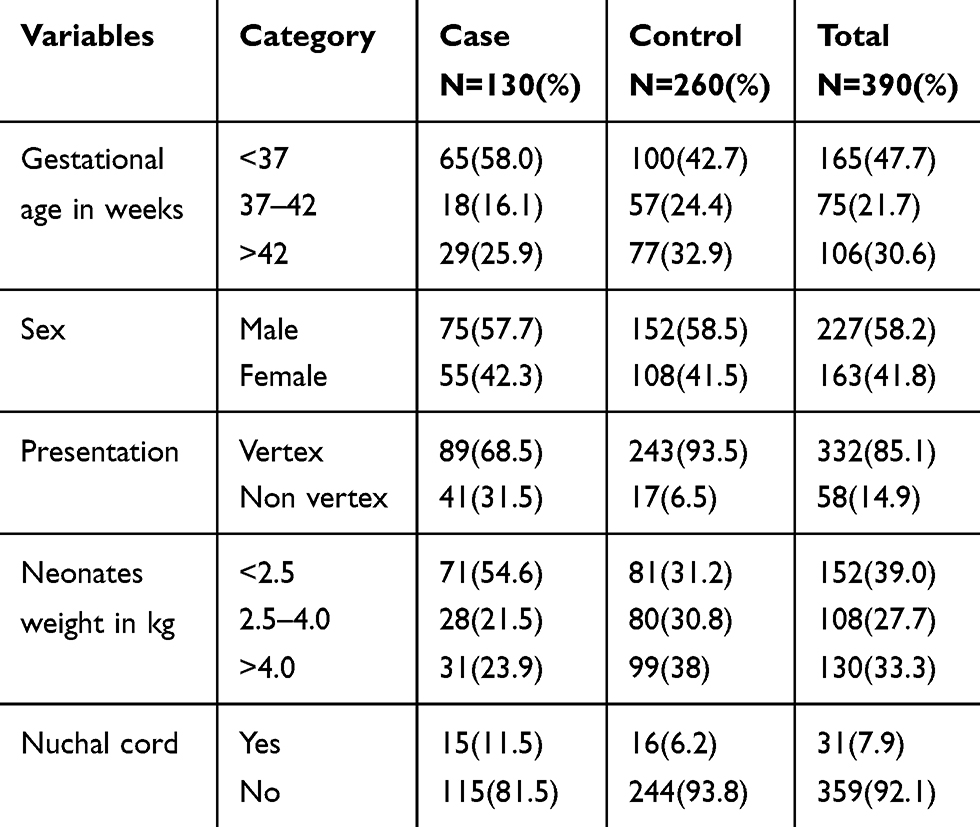 |
Table 4 Neonate-Related Characteristics of Neonates Among Cases and Controls Born in Public Hospitals of Tigray, Ethiopia 2017/2018 |
Risk Factors of Birth Asphyxia (Bivariate and Multivariate Analysis)
The risk of birth asphyxia among neonates born of primiparous mothers was 5.5 times higher [AOR 5.5 (CI: 2.5, 12.3)] relative to neonates born of multi-parous mothers. Post-term neonates were 2.73 times [AOR 2.73 (CI: 1.00, 7.55)] more likely to develop asphyxia than term-born neonates. The odds of developing birth asphyxia for neonates born to mothers with hypertension was 12.4 times higher than neonates born to mothers without hypertension [AOR 12.4 (CI: 4.17, 37.15)]. Neonates born with meconium-stained amniotic fluid were 29.2 times [AOR 29.2 (CI: 12.0, 71.1)] as likely to have asphyxia as those born without meconium-stained amniotic fluid. Neonates entangled in a cord are 5.67 times [AOR 5.67 (CI: 1.66, 19.3)] as likely to be asphyxiated as compared with their counterparts. Neonates with non-vertex presentation had a 5.49-fold higher risk of developing birth asphyxia than those born with normal presentation [AOR 5.49 (CI: 2.20, 13.7)] (Table 5).
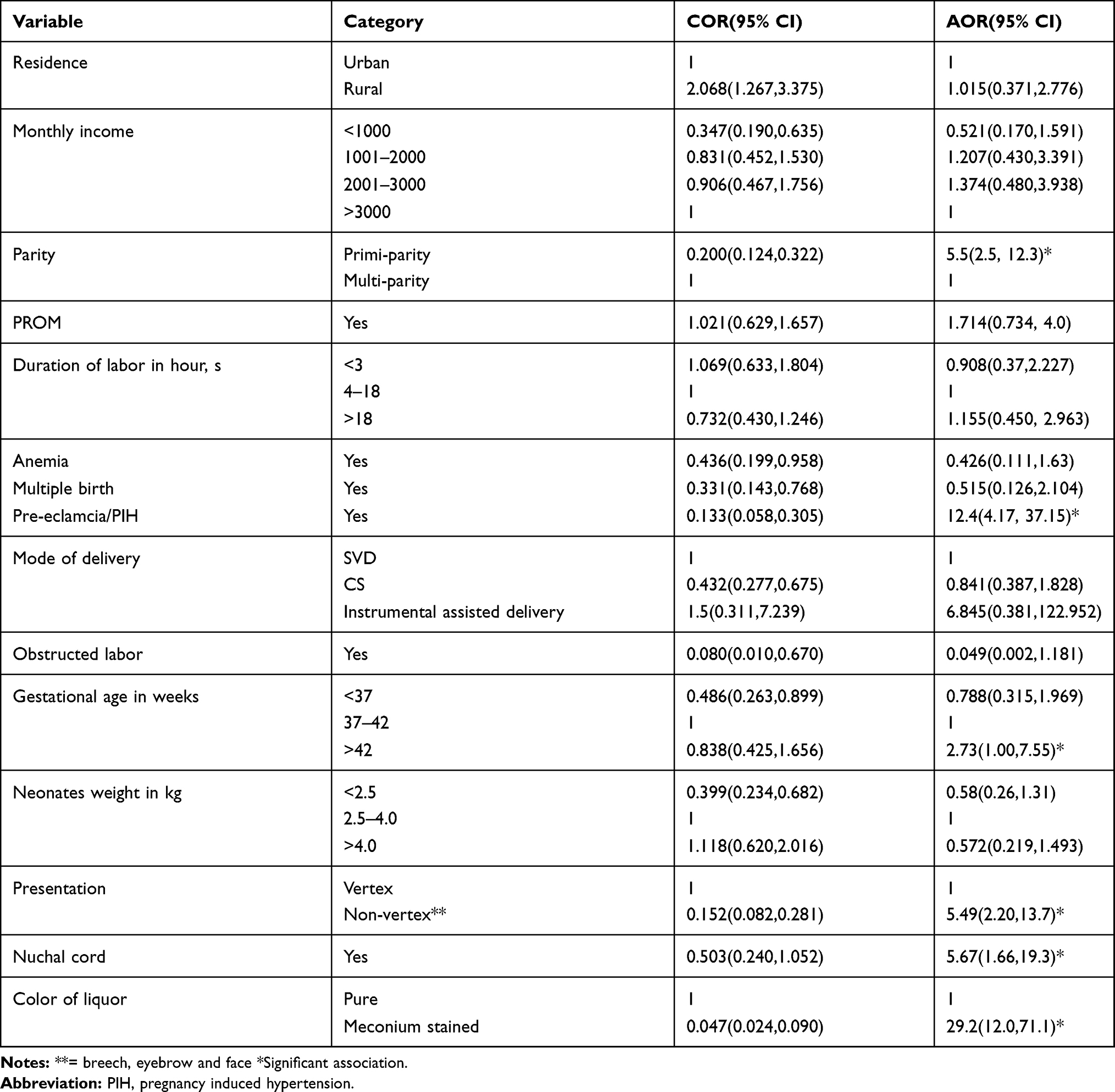 |
Table 5 Final Regression Model of Risk Factors of Birth Asphyxia in Public Hospitals of Tigray, 2017/2018 |
Discussion
Parity had a significant association with birth asphyxia in this study. Those who were primiparous mothers were 5.5 times higher than those who were multiparous mothers. This finding is consistent with the study conducted in Nigeria, India, Pakistan and the central Tigray zone.11–14 This may be due to the fact that prim-parous individuals are often unaware of the demands of pregnancy and often lack routine antenatal care. This may result in complications that lead to asphyxia. The consistency of the results could be attributed to the socio-economic and cultural similarity between the areas of study.
In the mothers of cases in the study, pre-eclampsia/pregnancy-induced hypertension (PHI) was also identified as a significant complication of pregnancy. Pre-eclampsia/pregnancy-induced hypertension was also previously reported as a risk factor for birth asphyxia.7,12,13,15–17 Preeclampsia/PIH, if persistent, linked to lower blood supply, nutrients and oxygen to the fetus, results in intrauterine growth restriction. This condition can alone be connected with asphyxia.
Post-term pregnancy results in placental insufficiency which occurs when the placenta does not provide the fetus with enough oxygen and nutrients. The placenta reaches its maximum size after 37 weeks of pregnancy and its functions begin to decline afterward. The longer a fetus goes without adequate nutrition or oxygen, the greater the risk to a range of health complications, including oxygen deprivation, which may also lead to perinatal asphyxia accompanied by cerebral palsy and intellectual problems.18 This study’s result revealed that post-term neonates were 2.73 times more likely than term-born neonates to experience asphyxia.
There was a significant association between meconium-colored liquor and birth asphyxia. Those who had stained meconium were 29.2 times more at risk of asphyxia than those who did not have stained liquor with meconium. This study is consistent with other previous studies conducted in India hospital, Pakistan in Karachi Tertiary Hospital, Phramongkutklao Hospital in Thailand, Nigeria Delta Tertiary Institute, Mulago Hospital in Uganda, Cameron Yaounde Tertiary Hospital, Gondar University Referral Hospital and Tigray Central Zone Public Hospitals in Ethiopia.7,11–15,17,19 The possible explanation could be that meconium-stained AF leads to peripartum inhalation of meconium-stained amniotic fluid, resulting in chemical pneumonitis including inflammation of the pulmonary tissue, mechanical narrowing of the airways and pulmonary air leakage, ending in hypoxia.20
As for the presentation of neonates, those with non-vertex presentation show a significant association with neonatal birth asphyxia. This finding is comparable to studies conducted at Acharya Vinobha Bhave rural hospital in India, Pakistan tertiary hospital in Karachi, Mululago hospital in Uganda, and Phramongkutklao hospital in Thailand.7,13,15,17,21 This might be attributable to the fact that the non-vertex presentation had an increased risk of umbilical cord prolapse, head entrapment and birth injury which result in oxygen deprivation.22
In our research, neonates entangled in the cord are 5.67 times more likely to develop asphyxia than those not entangled in the cord. This result was consistent with the study done in different parts of the world.16,23,24 This is due to the fact that umbilical cord is responsible for providing the fetus with oxygen-rich, nutrient-rich blood and for carrying deoxygenated, nutrient-depleted blood back to the placenta. If the nuchal cord interferes with these processes by compressing the umbilical cord, or blocks the arteries and veins in the fetal neck this can cause a loss of fetal oxygen.25
Conclusion and Recommendations
Birth asphyxia is one of the neonate problems of the world. In this research, intrapartum and neonatal factors in the index pregnancy were associated with birth asphyxia. The study findings suggest proper antenatal care follow-up and using partograph after the initiation of labor is crucial.
Data Sharing Statement
The data and materials of this study are available upon reasonable request from corresponding author.
Acknowledgments
First of all, we would like to thank Mekelle University for financial support. Our deepest gratitude goes to the respective hospitals and health care providers for providing us the necessary information. Last but not least we would like to acknowledge data collectors, supervisor and study participants. Mekelle university funded for data collection, stationery materials and data analysis.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Yodit Zewdie Berhe reports a patent CRPO/CHS/Small/Recurrent/002/2010 issued. The authors report no other conflicts of interest in this work.
References
1. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367:1747–1757. doi:10.1016/S0140-6736(06)68770-9
2. Lopez AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002–2030. Ann Trop Med Parasitol. 2006;100:481–499. doi:10.1179/136485906X97417
3. UN Inter-Agency Group. Levels & Trends in Child Mortality. UNICEF, WHO, World Bank, UN-DESA Population division; 2013.
4. Lawn J, Blencowe H, Oza S. Every newborn: progress, priorities, and potential beyond survival. Lancet. 2014;384:189–205. doi:10.1016/S0140-6736(14)60496-7
5. Hyder AA, Wali SA, McGuckin J. The burden of disease from neonatal mortality. a review of South Asia and Sub-Saharan Africa. BJOG 2003;10(110):894–901.
6. WHO. Perinatal Mortality: A Listing of Available Information. Geneva: WHO; 1996.
7. Pitsawong C, Panichkul P. Risk factors associated with birth asphyxia in Phramongkutklao Hospital. Thai J Obstet Gynaecol. 2012;19(4):165–171.
8. Gaym A. Maternal mortality. Review Jimma hospital, south west Ethiopia, 1990–1999. Ethiop J Health Dev. 2000;24:3–14.
9. Organization’s WH. Neonatal and Perinatal Mortality, 2004: Country, Regional and Global Estimates. Geneva: World Health Organization; 2007.
10. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, Rockville, Maryland, USA: CSA and ICF; 2016.
11. Gane B, Bhat V, Rao R, et al. Antenatal and intrapartum risk factors for perinatal asphyxia: a case control study. Indea Curr Pediatr Res. 2013;17(2):119–122.
12. Onyearugha CN, Ugboma HAA. Severe birth asphyxia: risk factors as seen in a tertiary institution in the niger delta area of nigeria. Cont J Trop Med. 2010;4:11–19.
13. Aslam HM, Saleem S, Afzal R, et al. Risk factors of birth asphyxia. Ital J Pediatr. 2014;40:94. doi:10.1186/s13052-014-0094-2
14. Tasew H, Zemicheal M, Teklay G, Mariye T, Ayele E. Risk factors of birth asphyxia among newborns in public hospitals of Central Zone, Tigray, Ethiopia. BMC Res Notes. 2018;11:496. doi:10.1186/s13104-018-3611-3
15. Kaye D. Antenatal and intrapartum risk factors for birth asphyxia among emergency obstetric referrals in Mulago Hospital, Kampala, Uganda. East Afr Med J. 2003;80(3):140–143. doi:10.4314/eamj.v80i3.8683
16. Hailu G, Yohannes K, Kassawmar A. Determinants of birth-asphyxia among newborns in Dessie Town Hospitals, North-Central Ethiopia. Int J Sex Health Repro Health. 2018;1(1):1–12.
17. Chiabi A, Nguefack S, Mah E, et al. Risk factors for birth asphyxia in an urban health facility in cameroon. Iran J Child Neurol. 2013;7(3):46–54.
18. Birth Injuriy Guide. 2019. [
19. Wosenu L, Worku AG, Teshome DF, Gelagay AA. Determinants of birth asphyxia among live birth newborns in University of Gondar referral hospital, northwest Ethiopia: a case-control study. PLoS One. 2018;13(9). doi:10.1371/journal.pone.0203763
20. Yurdakök M. Meconium aspiration syndrome: do we know? Turk J Pediatr. 2011;53(2):121–129.
21. Yadav N, Damke S. Study of risk factors in children with birth asphyxia. Int J Contemp Pediatrics. 2017;4(2):518. doi:10.18203/2349-3291.ijcp20170701
22. WHO. Managing complications in pregnancy and childbirth: malpositions and malpresentations India2019 [
23. Tabassum F, Rizvi A, Ariff S, Soofi S, Bhutta ZA. Risk factors associated with birth asphyxia in rural District Matiari, Pakistan: a case control study. Int J Clin Med. 2014;5:1430–1441. doi:10.4236/ijcm.2014.521181
24. Foumane P, Nkomom G, Mboudou ET, Sama JD, Nguefack S, Moifo B. Risk factors of clinical birth asphyxia and subsequent newborn death following nuchal cord in a low-resource setting. Open J Obstet Gynecol. 2013;3:642–647. doi:10.4236/ojog.2013.39117
25. Barhum L Nuchal chord: causes, complications, and management. Medical News Today. MediLexicon International; 2017.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.