")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Risk factors for the difficulties in general activities across the day in Chinese children and adolescents with attention-deficit/hyperactivity disorder
Authors Ke X, Du Y, Zheng Y, Su L, Chen Y, Zhang YL, Chen K, Cheng Y, Chen W
Received 17 September 2018
Accepted for publication 4 December 2018
Published 31 December 2018 Volume 2019:15 Pages 157—166
DOI https://doi.org/10.2147/NDT.S187882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Xiaoyan Ke,1 Yasong Du,2 Yi Zheng,3 Linyan Su,4 Yun Chen,5 Yanlei Zhang,5 Kui Chen,5 Yan Cheng,5 Wendong Chen6,7
1Nanjing Brain Hospital, Nanjing, People’s Republic of China; 2Shanghai Mental Health Center, Shanghai, People’s Republic of China; 3Beijing Anding Hospital, Beijing, People’s Republic of China; 4The Second Hospital of Xiangya Medical School, Central South University, Changsha, People’s Republic of China; 5Eli Lilly and Company, Shanghai, People’s Republic of China; 6Changsha Normin Health Technology Ltd., Changsha, People’s Republic of China; 7Normin Health Consulting Ltd., Toronto, ON, Canada
Objectives: To explore the factors significantly associated with the difficulties of general activities during specific time periods across the day in Chinese children and adolescents with attention-deficit/hyperactivity disorder (ADHD).
Methods: A cross-sectional study assessing the validity and reliability of Questionnaire-Children with Difficulties (QCD) for difficulties of general activities during specific time periods of the day in 200 Chinese children and adolescents with ADHD was the data source for this post-hoc analysis. Multivariate linear regression analyses were conducted to identify the factors significantly associated with the total and subscale scores of QCD respectively.
Results: ADHD subtype of inattention (vs combination subtype, coefficient 3.69, P=0.006), parent–child interaction activity (vs no parent–child activity, coefficient 4.30, P=0.002), and any psychiatric comorbidities (vs no mental comorbidities, coefficient -3.68, P=0.010) were independently and significantly associated with the total score of QCD (higher score indicating less difficulties, and vice-versa). These three factors and the other two factors, including mother’s education and parenting style, were independently and significantly associated with at least one subscale score of QCD for the five time domains across the day.
Conclusion: The overall difficulties of the general activities across the day in ADHD patients could be independently affected by ADHD subtype, psychiatric comorbidities, and parent–children interaction activity. However, the factors significantly associated with the difficulties of the general activities during specific time periods of the day in ADHD patients were slightly different.
Keywords: attention-deficit, hyperactivity disorder, Questionnaire-Children with Difficulties QCD, general activities, risk factor
Introduction
Attention deficit/hyperactivity disorder (ADHD) is the most common neurodevelopmental disorder.1 ADHD affects approximately 6.3% of Chinese children and adolescents and the main ADHD subtype in Chinese patients is attention deficit.2 ADHD has a profound impact on the education, career, and social functions in the adulthood of patients.3 Thus, the main goal of ADHD treatment is to improve school performance and social functions of children with ADHD.4 As parents are the direct observer of the symptoms and functional impairment associated with ADHD, many rating scales associated with ADHD have been developed from the perspective of parents.5
With the increasing recognition of the varied symptoms and functional impairment associated with ADHD throughout the day,6 Questionnaire-Children with Difficulties (QCD)7 has been developed to assist parents to assess their child’s daily behaviors during specific time domains such as morning, school, after school, evening, and night time for better ADHD management throughout the day. The validity and reliability of QCD have been validated in Japan and also in our previous cross-sectional study with 200 Chinese children and adolescents with ADHD.8 QCD could be used as an outcome measure to explore the risk factors for the difficulties in general activities during specific QCD time periods across the day in ADHD patients. Because our previous evaluation study for the reliability and validity of QCD in Chinese children and adolescent patients with ADHD had patient level QCD data of 200 patients,8 we leveraged these data to conduct a post-hoc analysis to identify the patient characteristics that could be significantly associated with QCD total score and subscale scores across the day. The identified patient characteristics from our post-hoc analysis could be used to explain the fluctuation of functional impairment associated with ADHD across the day and also guide the management of ADHD across the day.
Methods
This study was a post-hoc data analysis based on the collected data from our previous evaluation study for the reliability and validity of QCD in Chinese children and adolescents with ADHD. This QCD evaluation study has been published and the details and methods for patient enrollment and data collection can be found in our previous publication.8 This post-hoc analysis was conducted under the institutional ethics committee approval from each study center: Beijing Anding Hospital of Capital Medical University, Shanghai Mental Health Center, The Second Xiangya Hospital of Central South University, and Nanjing Brain Hospital Affiliated to Nanjing Medical University. Written informed consents were obtained from the parents of the enrolled adolescents with ADHD.
Data sources
The collected data from our previous QCD evaluation study were the data source for this post-hoc analysis. In brief, our QCD evaluation study enrolled 200 consecutive Chinese children and adolescents from four large tertiary care psychiatric clinics in China. The cross-sectional study collected the characteristics of 200 Chinese children and adolescents with ADHD (demographics, school status, family environment, ADHD diagnosis [types and disease duration after the diagnosis], current treatment, and psychiatric comorbidities) and their parents (social economic status [education and employment], lifestyle regarding drinking and smoking, and parenting styles). The scored QCD by the ADHD patients’ parents were included in our data analysis as the outcome measure indicating the degree of difficulty in daily activities during the defined QCD time periods throughout the day. The QCD7 consists of 20 questions assessing the degree of difficulty in activities in the classified time domains of the day (question items 1–4 for early morning/before going to school; question items 5–7 for school time; question items 8–10 for time after school; question items 11–14 for evening time; question items 15–18 for night time; and question items 19 and 20 for overall behavior). Each question can be graded from 0 to 3 to indicate the degree of agreement on the question (0: completely disagree; 1: somewhat (partially) agree; 2: mostly agree; and 3: completely agree), which expresses the difficulty in a specific general activity. Thus, the total score of QCD ranges from 0 to 60 and a higher QCD score indicates less difficulty. Full details of this cross-sectional study can be found in our published cross-sectional study validating QCD in Chinese children and adolescents with ADHD.8
Statistical analysis
The QCD scores of the 20 question items were summed to calculate the QCD total score. The subscale score for each QCD time domain was calculated by summing the scores of the question items in the same time domain. This study conducted univariate linear regression analyses to identify characteristics of the ADHD patients (a binary covariate was created to indicate the status of any psychiatric comorbidities) and their parents that were significantly associated with QCD total score. The identified characteristics with significant association in the univariate linear regression analyses were taken as the independent variables in the multivariate linear regression analyses to confirm their independent associations with QCD total score. The same analysis was also conducted to assess the associations between the QCD subscale scores and the characteristics of the included patients and their parents. The associations in the linear regression analysis were presented with coefficient, standard error, and P-value. All data analyses were conducted using SAS 9.2 (SAS Inc., Cary, NC, USA). The statistical significance in these analyses was defined as a two-sided P-value less than 0.05.
Results
This study generated the following results from the collected data in our previous cross-sectional study assessing the reliability and validity of QCD in 200 children and adolescents with ADHD visiting four Chinese tertiary care psychiatric clinics.
Brief summary of the characteristics of the ADHD patients and their parents
The average age of the included 200 ADHD patients was 10.4 years and 77.5% of these patients were male. The ADHD inattention subtype and the combined inattention and hyperactivity/impulsivity subtype accounted for 45.5% and 49.0% respectively in these ADHD patients. The other collected patient characteristics included disease duration after the diagnosis (62.6±96.6 weeks), proportions of currently on medication for ADHD treatment (63.5%), and psychiatric comorbidities (32.5%). The parents of these ADHD patients were characterized with high proportions of mother with high school or lower education (58.5%) and father with smoking (56.1%) and/or drinking (66.2%) lifestyle. The four parenting styles (authoritarian, authoritative, permissive, and uninvolved) were evenly distributed among the parents of the included ADHD patients. The characteristics of the included 200 ADHD patients and their parents are summarized in Table 1.
 | Table 1 Summary of the characteristics of the included ADHD patients and their parents |
The QCD scores
The mean score associated with each QCD question item ranged from 0.85 for the question item 11 (Can your child do his/her homework at home without difficulties?) to 2.10 for the question item 9 (Does your child have friends of his/her own age?). The average total QCD score associated with the included 200 ADHD patients was 32.0±9.8, indicating the partial agreement on the overall difficulties associated with general activities across the day from the perspective of their parents. The average QCD subscale scores for the classified time domains for early morning/before going to school, school time, time after school, evening time, night time, and overall behavior were 6.0, 5.4, 6.0, 6.6, 5.2, and 2.9, respectively. The QCD scores of the 200 ADHD patients are summarized in Table 2.
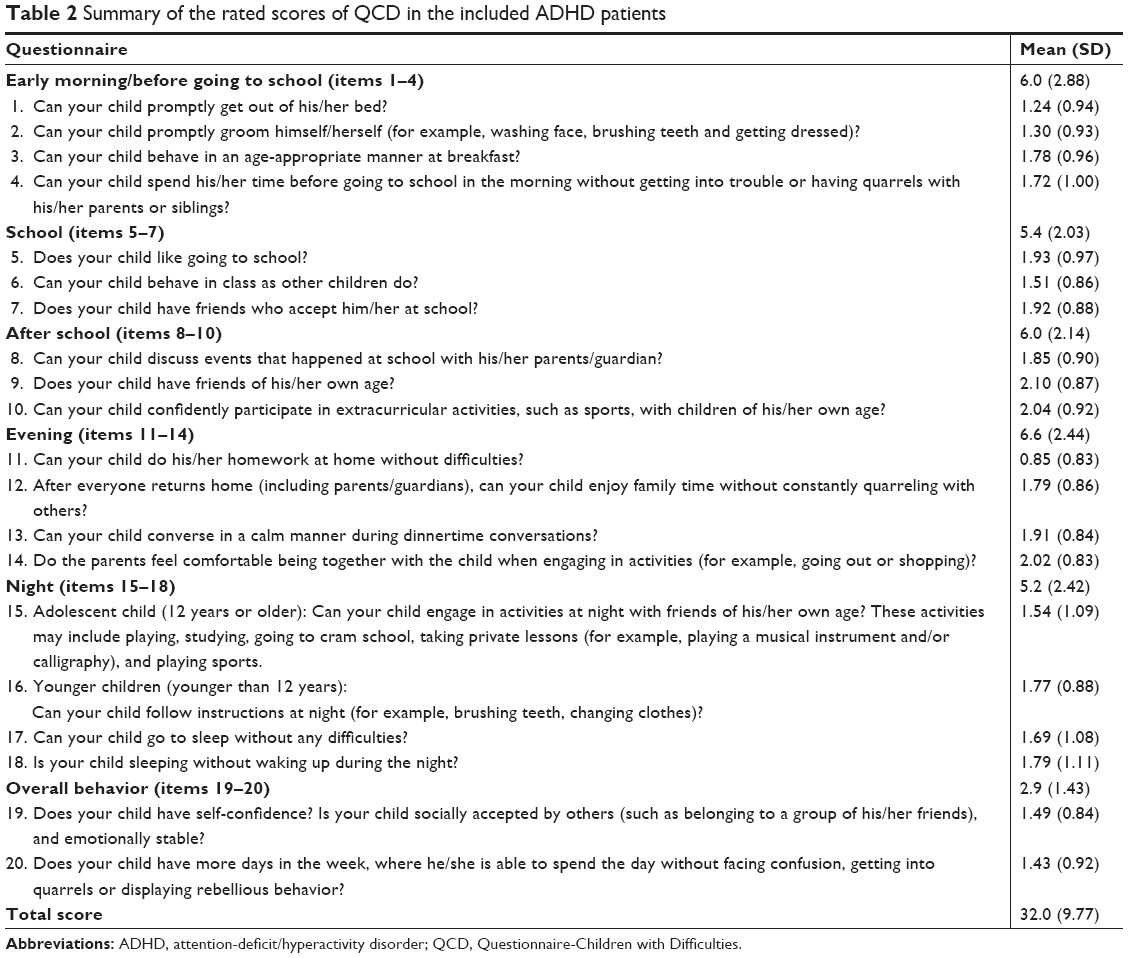 | Table 2 Summary of the rated scores of QCD in the included ADHD patients |
Risk factors associated with the QCD total score
Univariate linear regression analyses identified that QCD total score was significantly associated with any psychiatric comorbidities (patients with at least one psychiatric comorbidity), ADHD inattention subtype, and parent–child interaction activities (Table 3). Multivariate linear regression analysis with adjustment for other patient characteristics, including age, gender, and disease duration after ADHD diagnosis, confirmed the significant and independent association between QCD total score and the three characteristics (any psychiatric comorbidities vs no psychiatric comorbidities: coefficient −3.68, P=0.01; ADHD inattention subtype vs ADHD combination subtype: coefficient 3.69, P=0.006; parent–child interaction activity vs no parent–child interaction activities: coefficient 4.30, P=0.002). The results of multivariate linear regression analyses are illustrated in Figure 1.
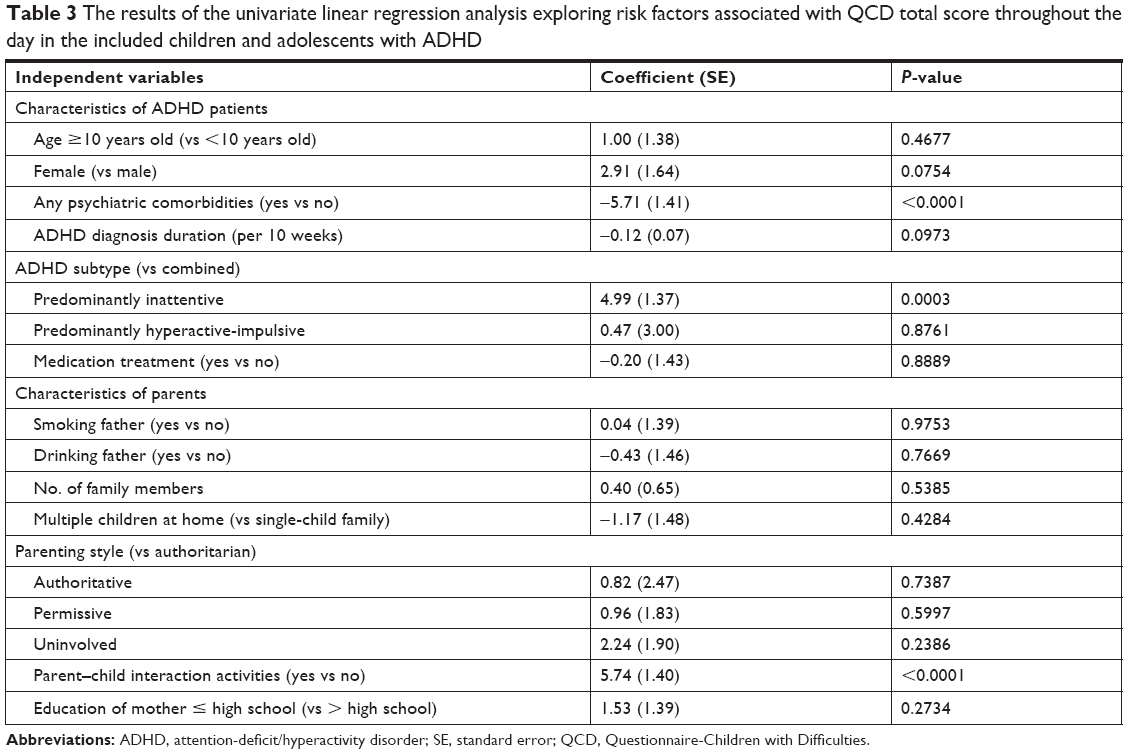 | Table 3 The results of the univariate linear regression analysis exploring risk factors associated with QCD total score throughout the day in the included children and adolescents with ADHD |
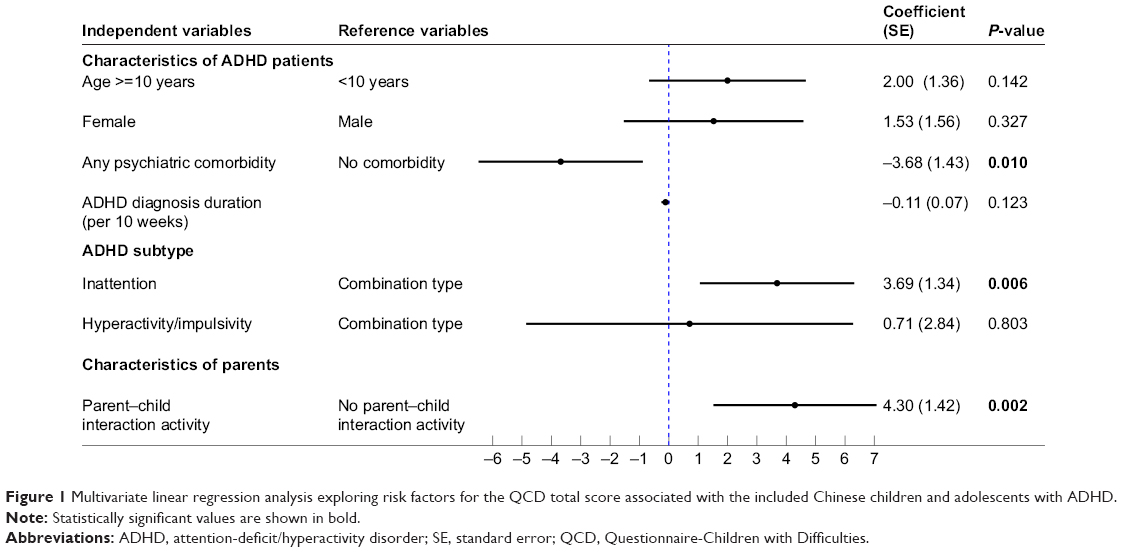 | Figure 1 Multivariate linear regression analysis exploring risk factors for the QCD total score associated with the included Chinese children and adolescents with ADHD. |
Risk factor association with QCD subscale scores
Univariate linear regression analysis observed a slightly different pattern of the associations between the independent variables (the characteristics of ADHD patients and their parents) and the QCD subscale scores associated with the five classified time domains throughout the day. Of the three identified factors significantly and independently associated with the QCD total score, only two factors, any psychiatric comorbidities and parent–child interaction activities, were significantly associated with the QCD subscale scores for all five time domains throughout the day in the univariate linear regression analyses; the other one factor, the ADHD inattention subtype, was significantly associated with QCD subscale scores for three time domains (morning time, school time, and evening time) in the univariate linear regression analyses. Additionally, the lifestyle of the father, parenting style, and education level of the mother were significantly associated with the QCD subscale score for at least one time domain in the univariate linear regression analyses. The results of these univariate linear regression analyses are summarized in Table 4.
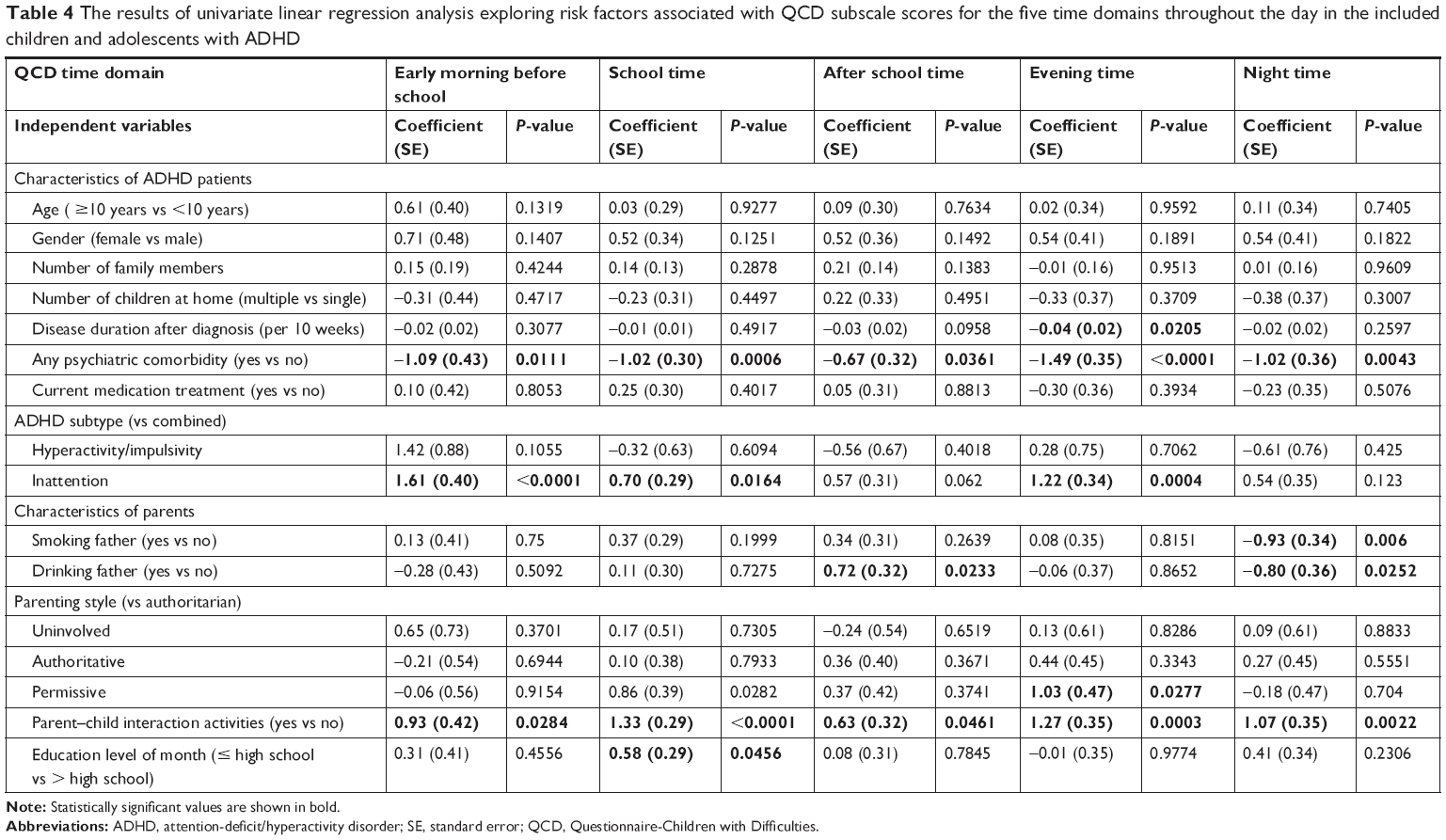 | Table 4 The results of univariate linear regression analysis exploring risk factors associated with QCD subscale scores for the five time domains throughout the day in the included children and adolescents with ADHD |
Multivariate linear regression analyses indicated that the QCD subscale scores for at school and evening time were independently and significantly associated with any psychiatric comorbidities (vs no psychiatric comorbidities) (at school: coefficient −0.64, P=0.028; evening time: coefficient −1.06, P=0.003), ADHD inattention subtype (vs combination type) (at school: coefficient 0.67, P=0.017; evening time: coefficient 1.09, P=0.001), and parent–child interaction activities (vs no parent–child interaction activities) (evening time: coefficient 0.89, P=0.013) and permissive parenting style (vs authoritarian) (at school: coefficient 1.10, P=0.02) or uninvolved parenting style (vs authoritarian) (evening time: coefficient 1.13, P=0.008). The QCD subscale score for at-school domain was also independently and significantly associated with the education of the mother (high school or below vs above high school: coefficient 0.80, P=0.003). The QCD scale score for after school time domain was significantly and independently associated with the duration of ADHD after diagnosis (per 10 weeks) (coefficient −0.03, P=0.047) and father with drinking lifestyle (vs no drinking) (coefficient 0.87, P=0.005). QCD subscale score for the night time domain was significantly and independently associated with parent–child interaction activities (vs no parent–child interaction activities: coefficient 0.96, P=0.009), and father with a smoking lifestyle (vs no smoking father: coefficient −0.72, P=0.038). The QCD subscale score for the morning time domain was only significantly and independently associated with ADHD inattention subtype (vs combination type: coefficient 1.33, P=0.001). Table 5 summarizes the results of the multivariate linear regression analyses for the QCD subscale scores associated with the five classified time domains throughout the day in the included 200 ADHD patients.
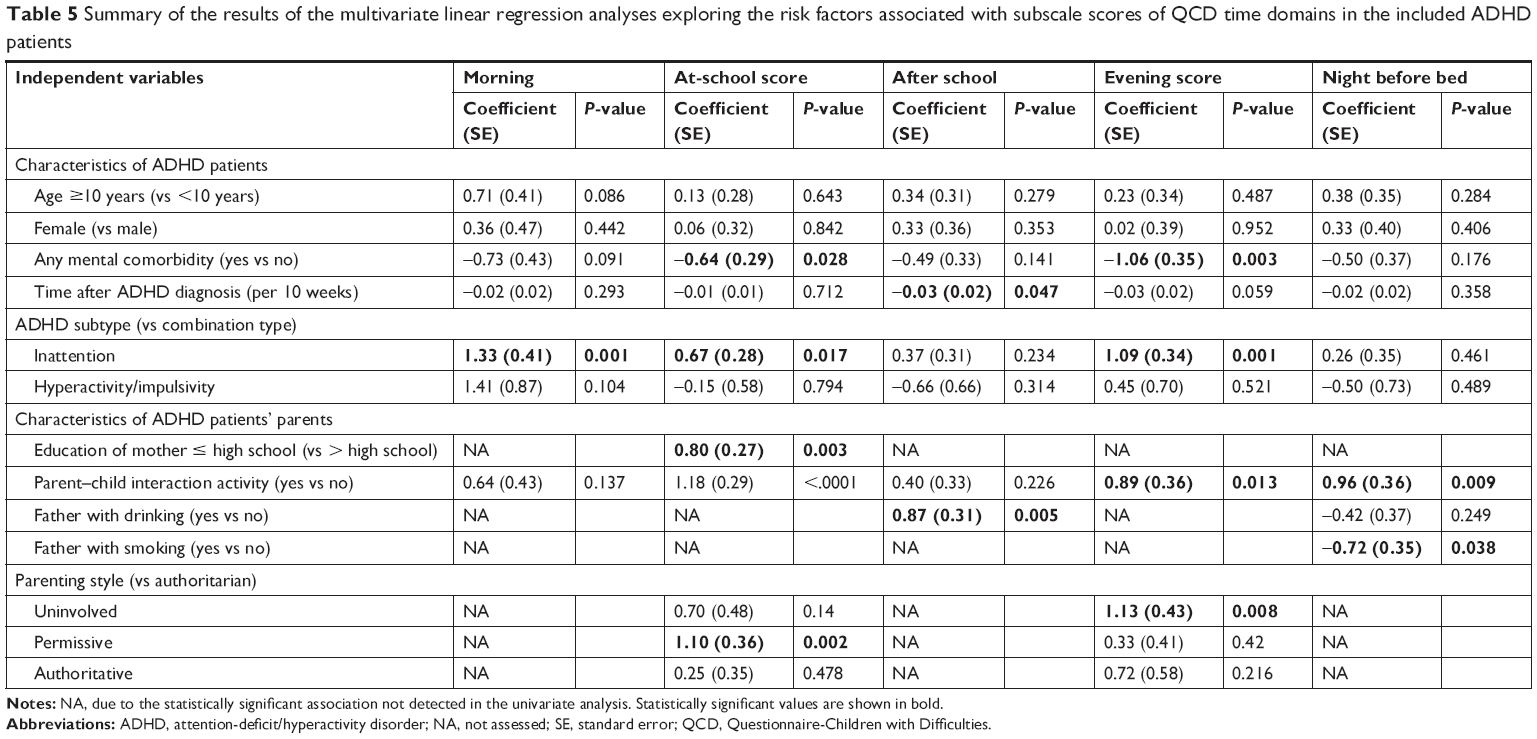 | Table 5 Summary of the results of the multivariate linear regression analyses exploring the risk factors associated with subscale scores of QCD time domains in the included ADHD patients |
Discussion
The recognition of varying functional impairment associated with ADHD throughout the day led to the development of the QCD, which was designed specifically for parents to rate the difficulties of the general activities in the classified five time domains throughout the day. Based on the collected data from our previous study assessing the validity and reliability of QCD in the 200 Chinese children and adolescents with ADHD, this post-hoc analysis observed the varied QCD subscale scores associated with the five time domains throughout the day and a slightly different pattern of the risk factors associated with the QCD total score and subscale scores for the five classified time domains. Thus, this study supports the rationale of managing ADHD by specific time periods throughout the day.4
The observed fluctuations in the QCD subscale scores associated with the five time domains throughout the day were consistent with observed changes of behavioral symptoms and functional impairment across the day in children with ADHD.9 Additionally, the lowest QCD subscale score associated with the morning time domain suggested that our ADHD patients experienced the worst functional impairment in the morning as reported by previous studies. For example, moderate-to-severe ADHD symptoms and functional impairment in the early morning were more frequently observed in the children with ADHD.10 Because the early morning functional impairment associated with ADHD could directly increase the burden on parents, our study added to the evidence which demonstrates the unmet needs regarding the management of ADHD symptoms and functional impairment in the morning.
Our analysis identified that psychiatric morbidities, ADHD inattention subtype, and parent–child interaction activities were independently and significantly associated with the overall difficulties of general activities throughout the day. The observed significant association between psychiatric comorbidities and the QCD total score suggests that psychiatric comorbidities could worsen functional impairment in our ADHD patients. Similar to previously reported prevalence and pattern of psychiatric comorbidities in US ADHD children,11 over one-third of our study subjects had at least one psychiatric comorbidity, which included learning disability, tic disorder, oppositional defiant disorder, personality disorder, and stress. These comorbidities could cause additional functional impairment in ADHD patients. For example, learning disability, the most prevalent comorbidity in our study subjects, significantly increased the severity of executive function impairment.12 Oppositional defiant disorder was associated with a decreased ability to generate strategies or monitor ongoing behavior.13 As reported by Houghton et al,14 identified association between the ADHD inattention subtype and higher QCD total score is aligned with Barkley’s proposed unifying theory of ADHD regarding the lower impact of ADHD inattention subtype on executive function impairment. Additionally, the identified association between parent–child interaction activities and higher QCD total score in our ADHD patients supported the exploration of the clinical utility of parent–child interaction therapy in ADHD patients as it was effective in treating young children with disruptive disorders.15
Our study observed a slightly different pattern of risk factors associated with QCD subscale scores associated with the five classified time domains throughout the day. This finding supports the notion that functional impairments associated with ADHD vary throughout the day and ADHD should be managed by time domains throughout the day. Additionally, our analyses suggest that the functional impairment associated with the specific time periods could be affected by different characteristics of ADHD patients and their parents. Thus, the identified risk factors associated with the QCD subscale scores could help with the explanation for the varied functional impairment and guide future ADHD management by specific time periods throughout the day.
Our analyses identified that psychiatric comorbidities could increase the functional impairment during school time and evening time, the two time domains when academic and educational activities were most likely. The impact of psychiatric comorbidities on academic performs in ADHD patients has been well investigated. Thus, actively screening and managing psychiatric morbidities should be included in the ADHD management to maximize academic and education outcomes, which are the main goals of ADHD management.16 Our analysis also found that the disease duration after ADHD diagnosis was associated with greater functional impairment for the general activities after school. Because the longer disease duration could indicate more advanced disease, stimulant medications, the current mainstay therapy for ADHD, might not fully control the functional impairment throughout the day due to the poor compliance to two to three administrations throughout the day.17 Because the teachers are unlikely to help the children with treatment administration at school, once daily administration medication for ADHD could be the better solution to address the current challenges associated with using stimulant medications to manage ADHD throughout the day. Additionally, our analyses identified a significant association between father with smoking lifestyle and lower QCD subscale score associated with the night time domain. Because the exposure to tobacco impairs children’s behavioral18 and cognitive function,19 fathers with a smoking lifestyle could spend more time with their children at night and further worsen the functional impairment associated with ADHD.
Our analyses identified that ADHD inattention subtype, parent–child interaction activities, parenting style (uninvolved and permissive), father with drinking lifestyle, and mother with high school education or below were associated with higher QCD subscale scores for some time domains. Because ADHD inattention subtype caused more neuropsychological impairment than the other two ADHD subtypes,20 we highly suspect that the few symptoms associated with inattention subtype could bias parents for their QCD rating. Similar bias was also reported in the low agreement between parents and teachers regarding the diagnosis of ADHD inattention subtype.21 The significant association between parent–child interaction activities and higher QCD subscale scores for evening time and night time might suggest that the parent–child interaction activities were likely to occur in the evening and night time and parent–child interaction activities could help with reducing functional impairment associated with ADHD. The higher QCD subscale score associated with uninvolved and permissive parenting styles at school and in the evening time could be the results of lower anxiety in their children under the two parenting styles.22 The children under the two parenting styles could experience less anxiety, which impacts functional impairment associated with ADHD.23 We did not have sufficient knowledge to explain well the associations between the higher QCD subscale scores associated with the two time domains (at-school time and after school time) and the other two factors, father with drinking lifestyle and mother with high school education level or below. Because drinking and education level are the indicators for poor social economic status, we suspect that the parents with poorer social economic status have limited capacity to appropriately assess the difficulties of general activities related to school.
As a post-hoc analysis, our analyses shared the same limitations as the cross-sectional study assessing the validity and reliability of QCD. For example, the identified risk factors for QCD total score and QCD subscale score were based on cross-sectional association. Future longitudinal study design is still needed to confirm the impact of these risk factors on the functional impairment associated with ADHD throughout the day. Additionally, our analyses were unable to assess the impact of controlling the identified risk factors on the functional impairment associated with ADHD. Thus, future studies are still needed to confirm that the control of the identified risk factors, such as psychiatric comorbidities and reducing the exposure from a smoking father, could reduce functional impairment associated with ADHD. Finally, the identified association between ADHD inattention subtype and QCD total score and subscale scores should be interpreted with caution of the assessment bias associated with the parent rating scales.21
Conclusion
In summary, this post-hoc analysis is the first study using QCD as the outcome measure to explore the risk factors for functional impairment associated with Chinese ADHD patients in specific time domains throughout the day. The observed variance associated with QCD subscale scores confirmed the varied functional impairment associated with ADHD throughout the day and demonstrated the needs of ADHD management by time periods of the day. The observed association between psychiatric comorbidities and lower QCD total score and subscale scores demonstrated that actively screening and managing psychiatric comorbidities could help with reducing the functional impairment associated with ADHD. The observed higher QCD total score and subscale scores associated with parent–patient interaction activities support the potential clinical utility of parent–patient interaction activities in managing ADHD. As our post-hoc analysis only assessed the cross-sectional association between the characteristics of ADHD patients and their parents, future longitudinal studies are needed to confirm the identified associations in our study and guide ADHD management throughout the day.
Acknowledgment
This study was funded by Eli Lilly and Company, Shanghai, China.
Author contributions
Xiaoyan Ke, Yasong Du, Yi Zhen, Linyan Su, Qingqing Liu, Yun Chen, and Yanlei Zhang formulated the research idea and developed the data analysis plan. Xiaoyan Ke, Yasong Du, Yi Zhen, and Linyan Su enrolled the study subjects and conducted the cross-sectional survey to collect study data. Yun Chen performed the data analyses. Yasong Du, Xiaoyan Ke, Yi Zhen, Linyan Su, Yanlei Zhang, Kui Chen, Yan Cheng, and Wendong Chen developed the manuscript. All authors contributed to data analysis, drafting, revising and critically reviewing the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Yasong Du, Xiaoyan Ke, Yi Zhen and Linyan Su have received speaker honoraria from Eli Lilly and Company, Shanghai, China. Wendong Chen is the founder of both Changsha Normin Medical Technology Ltd and Normin Health Consulting Ltd, receiving industry funds for health economics and outcomes research. Yun Chen, Yanlei Zhang, Kui Chen, and Yan Cheng are employees of Eli Lilly and Company, Shanghai, China. The authors report no other conflicts of interest in this work.
References
Mittal VA, Walker EF. Diagnostic and statistical manual of mental disorders (Letter). Psychiatr Res. 2011;189(1):158–159. | ||
Wang T, Liu K, Li Z, et al. Prevalence of attention deficit/hyperactivity disorder among children and adolescents in China: a systematic review and meta-analysis. BMC Psychiatry. 2017;17(1):32. | ||
Spira EG, Fischel JE. The impact of preschool inattention, hyperactivity, and impulsivity on social and academic development: a review. J Child Psychol Psychiatry. 2005;46(7):755–773. | ||
Wolraich M, Brown L, Brown RT, et al. ADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics. 2011;128(5):1007–1022. | ||
Collett BR, Ohan JL, Myers KM. Ten-year review of rating scales. V: scales assessing attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2003;42(9):1015–1037. | ||
Usami M, Iwadare Y, Watanabe K, et al. A case-control study of the difficulties in daily functioning experienced by children with depressive disorder. J Affect Disord. 2015;179:167–174. | ||
Usami M, Sasayama D, Sugiyama N, et al. The reliability and validity of the Questionnaire-Children with Difficulties (QCD). Child Adolesc Psychiatry Ment Health. 2013;7(1):11. | ||
Zheng Y, du Y, Su LY, et al. Reliability and validity of the Chinese version of Questionnaire-Children with Difficulties for Chinese children or adolescents with attention-deficit/hyperactivity disorder: a cross-sectional survey. Neuropsychiatr Dis Treat. 2018;14:2181–2190. | ||
Antrop I, Roeyers H, De Baecke L. Effects of time of day on classroom behaviour in children with ADHD. Sch Psychol Int. 2005;26(1):29–43. | ||
Sallee FR. Early morning functioning in stimulant-treated children and adolescents with attention-deficit/hyperactivity disorder, and its impact on caregivers. J Child Adolesc Psychopharmacol. 2015;25(7):558–565. | ||
Larson K, Russ SA, Kahn RS, Halfon N. Patterns of comorbidity, functioning, and service use for US children with ADHD, 2007. Pediatrics. 2011;127(3):462–470. | ||
Seidman LJ, Biederman J, Monuteaux MC, Doyle AE, Faraone SV. Learning disabilities and executive dysfunction in boys with attention-deficit/hyperactivity disorder. Neuropsychology. 2001;15(4):544–556. | ||
Clark C, Prior M, Kinsella GJ. Do executive function deficits differentiate between adolescents with ADHD and oppositional defiant/conduct disorder? A neuropsychological study using the Six Elements Test and Hayling Sentence Completion Test. J Abnorm Child Psychol. 2000;28(5):403–414. | ||
Houghton S, Douglas G, West J, et al. Differential patterns of executive function in children with attention-deficit hyperactivity disorder according to gender and subtype. J Child Neurol. 1999;14(12):801–805. | ||
Wagner SM, McNeil CB. Parent-child interaction therapy for ADHD: a conceptual overview and critical literature review. Child Fam Behav Ther. 2008;30(3):231–256. | ||
Loe IM, Feldman HM. Academic and educational outcomes of children with ADHD. J Pediatr Psychol. 2007;32(6):643–654. | ||
Swanson J. Compliance with stimulants for attention-deficit/hyperactivity disorder. CNS Drugs. 2003;17(2):117–131. | ||
Weitzman M, Byrd RS, Aligne CA, Moss M. The effects of tobacco exposure on children’s behavioral and cognitive functioning: implications for clinical and public health policy and future research. Neurotoxicol Teratol. 2002;24(3):397–406. | ||
Braun JM, Kahn RS, Froehlich T, Auinger P, Lanphear BP. Exposures to environmental toxicants and attention deficit hyperactivity disorder in US children. Environ Health Perspect. 2006;114(12):1904–1909. | ||
Chhabildas N, Pennington BF, Willcutt EG. A comparison of the neuropsychological profiles of the DSM-IV subtypes of ADHD. J Abnorm Child Psychol. 2001;29(6):529–540. | ||
Wolraich ML, Lambert EW, Bickman L, Simmons T, Doffing MA, Worley KA. Assessing the impact of parent and teacher agreement on diagnosing attention-deficit hyperactivity disorder. J Dev Behav Pediatr. 2004;25(1):41–47. | ||
Wood JJ, McLeod BD, Sigman M, Hwang WC, Chu BC. Parenting and childhood anxiety: theory, empirical findings, and future directions. J Child Psychol Psychiatry. 2003;44(1):134–151. | ||
Reid AM, Graziano P, McNamara J, Paneto A, Geffken G. Functional impairment differences among youth with ADHD: the role of comorbid anxiety and mood disorders. J Nat Sci. 2015;1(1):31. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.