")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Risk factors for delirium: are therapeutic interventions part of it?
Authors Xing J , Yuan Z, Jie Y, Liu Y, Wang M, Sun Y
Received 30 October 2018
Accepted for publication 8 April 2019
Published 17 May 2019 Volume 2019:15 Pages 1321—1327
DOI https://doi.org/10.2147/NDT.S192836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yuping Ning
Jinyan Xing,1 Zhiyong Yuan,1 Yaqi Jie,2 Ying Liu,1 Mingxue Wang,1 Yunbo Sun1
1Department of Critical Care Medicine, the Affiliated Hospital of Qingdao University, Qingdao 266003, People’s Republic of China; 2School of Life Sciences, Qingdao University, Qingdao, 266071, People’s Republic of China
Background: Delirium is associated with increased morbidity and mortality in critically ill patients. Research on risk factors for delirium allows clinicians to identify high-risk patients, which is the basis for early prevention and diagnosis. Besides the risk factors for delirium that are commonly studied, here we more focused on the less-studied therapeutic interventions for critically ill patients which are potentially modifiable.
Materials and methods: A total of 320 non-comatose patients admitted to the ICU for more than 24 hrs during 9 months were eligible for the study. Delirium was screened once daily using the CAM-ICU. Demographics, admission clinical data, and daily interventions were collected.
Results: Ninety-two patients (28.75%) experienced delirium at least once. Delirious patients were more likely to have longer duration of mechanical ventilation, ICU stay, and hospital stay. Most of the less-studied therapeutic interventions were linked to delirium in the univariate analysis, including gastric tube, artificial airway, deep intravenous catheter, arterial line, urinary catheter, use of vasoactive drugs, and sedative medication. After adjusting with age and ICU length of stay, mechanical ventilation (OR: 5.123; 95% CI: 2.501–10.494), Acute Physiology and Chronic Health Evaluation (APACHE) II score≥20 at admission (OR: 1.897; 95% CI: 1.045–3.441), and gastric tube (OR: 1.935, 95% CI: 1.012–3.698) were associated with increased risk of delirium in multivariate analysis.
Conclusion: Delirium was associated with prolonged mechanical ventilation, ICU stay, and hospital stay. Multivariate risk factors were gastric tube, mechanical ventilation, and APACHE II score. Although being a preliminary study, this study suggests the necessity of earliest removal of tubes and catheters when no longer needed.
Keywords: delirium, critical care, intensive care unit, risk factors, prevention
Introduction
Delirium is an acute fluctuating change in mental status with attentional deficits and disorganized behavior. The prevalence of delirium ranges from 20% to 80% in critical ill patients in the intensive care unit (ICU).1,2 Delirium is related with higher mortality, prolonged hospitalization, larger hospital costs, cognitive decline, and potential functional disability.3–8
Effective treatment for delirium is difficult. Thus, preventions of delirium are of great value in the ICU setting.9–11 The study of risk factors for delirium allows clinicians to identify patients at high risk of delirium, thereby enabling clinicians to implement delirium preventions in advance and/or increases delirium screening frequency for earlier diagnosis in this group of patients. Early prevention and diagnosis can also benefit critically ill patients in many ways, such as reducing the incidence of delirium and achieving timely and effective management, which ultimately reduce the risk of delirium, and reduce the burden on patients and the medical system.
The risk factors for delirium can be divided into predisposing factors and precipitating factors. Generally, predisposing factors are defined as baseline vulnerability factors exist prior to admission and are difficult to change. Harmful insults or hospitalization-related factors occurring during the course of illness are defined as precipitating factors, including factors related to therapeutic interventions and other factors related to the critical illness.12 Precipitating factors are potentially modifiable, allowing clinicians to improve local practices and carry out preventive measures. A systematic review of 33 cohort studies or randomized controlled studies has reported only 11 putative risk factors for delirium in critically ill adults.13 Among them, only 3 are potentially modifiable including use of dexmedetomidine, length of mechanical ventilation, and coma.14
Till now, among all the modifiable therapeutic interventions, only the mechanical ventilation and sedative medication are the most widely studied risk factors for delirium.13,15,16 To our knowledge, little is known about the effect of other commonly used therapeutic interventions such as artificial airway, deep intravenous catheter, drainage tube, arterial line, gastric tube, urinary catheter, use of vasoactive drugs, and sedative medication on the development of delirium. Therefore, we conducted a prospective observational study to evaluate less-studied modifiable therapeutic interventions as well as other commonly studied risk factors for delirium in a critical care setting in China.
Methods
Study design and participants
From January 2017 to September 2017, we conducted a prospective observational study in medical and surgical ICU with 24 beds in the Affiliated Hospital of Qingdao University in China. Non-comatose patients aged 15 years or more and admitted for over 24 hrs were included. Patients were excluded if they met the following criteria: 1) RASS score <-3; 2) patients had cognitive dysfunction and were unable to cooperate; 3) patients with severe dementia or abuse of psychoactive drugs. All patients were treated according to ABCDE bundle (Assess, prevent, and manage pain; Both Spontaneous Awakening Trials (SATs) and Spontaneous Breathing Trials (SBTs); Choice of analgesia and sedation; Delirium assess, prevent, and manage; Early mobility and exercise; and Family engagement and empowerment.).17,18 Fentanyl, morphine, midazolam, propofol, dexmedetomidine, or their combination were used for sedation; vasoactive drugs were norepinephrine, dobutamine, and epinephrine. The choice of drugs, dosage, and the duration of administration were determined by the physicians. The study was approved by the Affiliated Hospital of Qingdao University Ethics Committee, and written informed consent was obtained from patients or their guardian, in accordance with the declaration of Helsinki.
Delirium screening
Delirium was screened prospectively by a specific trained practitioner for all enrolled patients to ensure standardization. Delirium screening was carried out once daily during 8:00 AM−10:00 AM using the Confusion Assessment Method for the ICU (CAM-ICU). All patients were evaluated for delirium until discharging from ICU or death. Delirious patients were defined as any patient with at least once positive CAM-ICU assessment during our assessment.
Data collection
Demographics and admission clinical data were collected at the enrollment of each patient, including age, sex, education background, medical insurance, APACHE (Acute Physiology and Chronic Health Evaluation) II19 score at enrollment, admission diagnosis, and medical history (diabetes, hypertension, and malignant tumors, and impaired renal function).
We also prospectively collected daily recorded data during ICU stays of each patient, including mechanical ventilation, artificial airway (tracheal intubation or tracheotomy), deep intravenous catheter, drainage tube, arterial line, gastric tube, urinary catheter, use of sedatives medication, use of vasoactive drugs, and private room (environmental factors).
Statistics
Demographic and clinical variables were summarized using descriptive statistics. Non-normal distributed continuous variables were described using median and interquartile range (IQR). The comparison of these continuous variables was done using Wilcoxon rank-sum test for nonparametric data. For categorical variables, descriptions were used frequencies and proportions, and Pearson’s chi-square (X2 test) was used for comparisons between the delirious and non-delirium group. Multivariate logistic regression analysis was used to assess the association of potential covariates with delirium. All analyses were performed using Stata 12.1 (Stata Corporation, College Station, Texas, USA).
Results
Characteristics of study participants
We recruited 320 patients over the study period, with male patients accounted for 58.44%. Characteristics of all patients are shown in Table 1. The median age of patients was 61 years, with interquartile range (IQR) from 46 to 71 years. As high as 30.63% had degree of senior high school or above, and 80.63% had medical insurance. Only 2.81% (n=9) of patients were with alcohol abuse.20 The median of APACHE II scores at enrollment was 20 (IQR, 15 to 23). The median days of ICU length of stay and hospital length of stay were 4 days (IQR, 1 to 9) and 7 days (IQR, 3 to 13), respectively. One hundred and ninety-six patients (61.3%) underwent mechanical ventilation, and the median duration of mechanical ventilation was 1 day (IQR, 1 to 3).
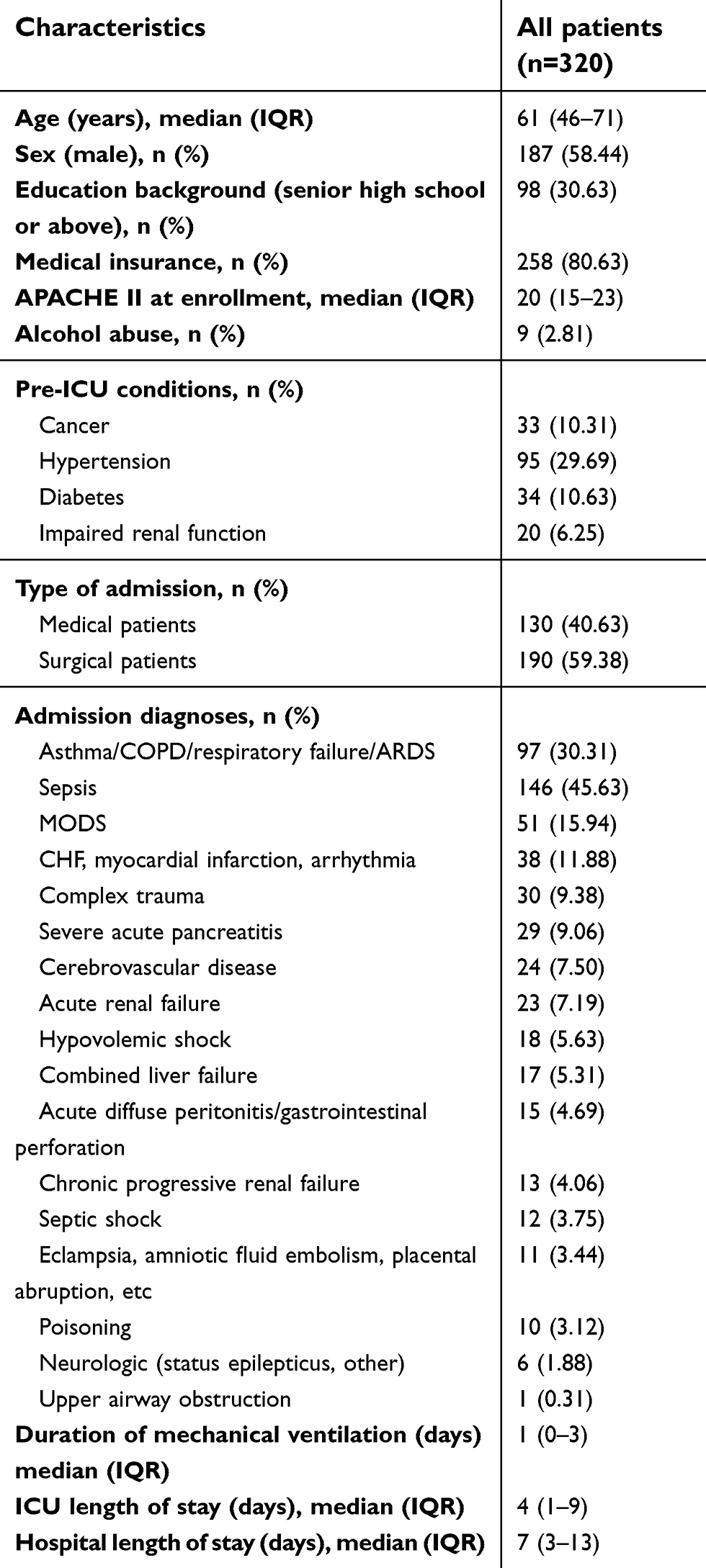 | Table 1 Demographics and characteristics of study participants |
All cases were assessed for delirium daily during the ICU stay, with a median of 2 assessments (IQR, 1–7) per patient. A total of 92 patients (28.75%) experienced delirium at least once during ICU stay. The median duration of delirium was 3 days, with IQR from 1 to 7 days.
Univariate analysis
To identify the possible risk factors of delirium during the ICU stay, univariate analysis was performed. We first analyzed routine risk factors associated with delirium including the patients’ characteristics, underlying comorbidities and environmental factors, and identified 4 possible risk factors for delirium among our patient population. As shown in Table 2, patients with delirium may more frequently above 65 years of age, and with APACHE II score ≥20. They also more frequently have a history of diabetes and impaired renal function.
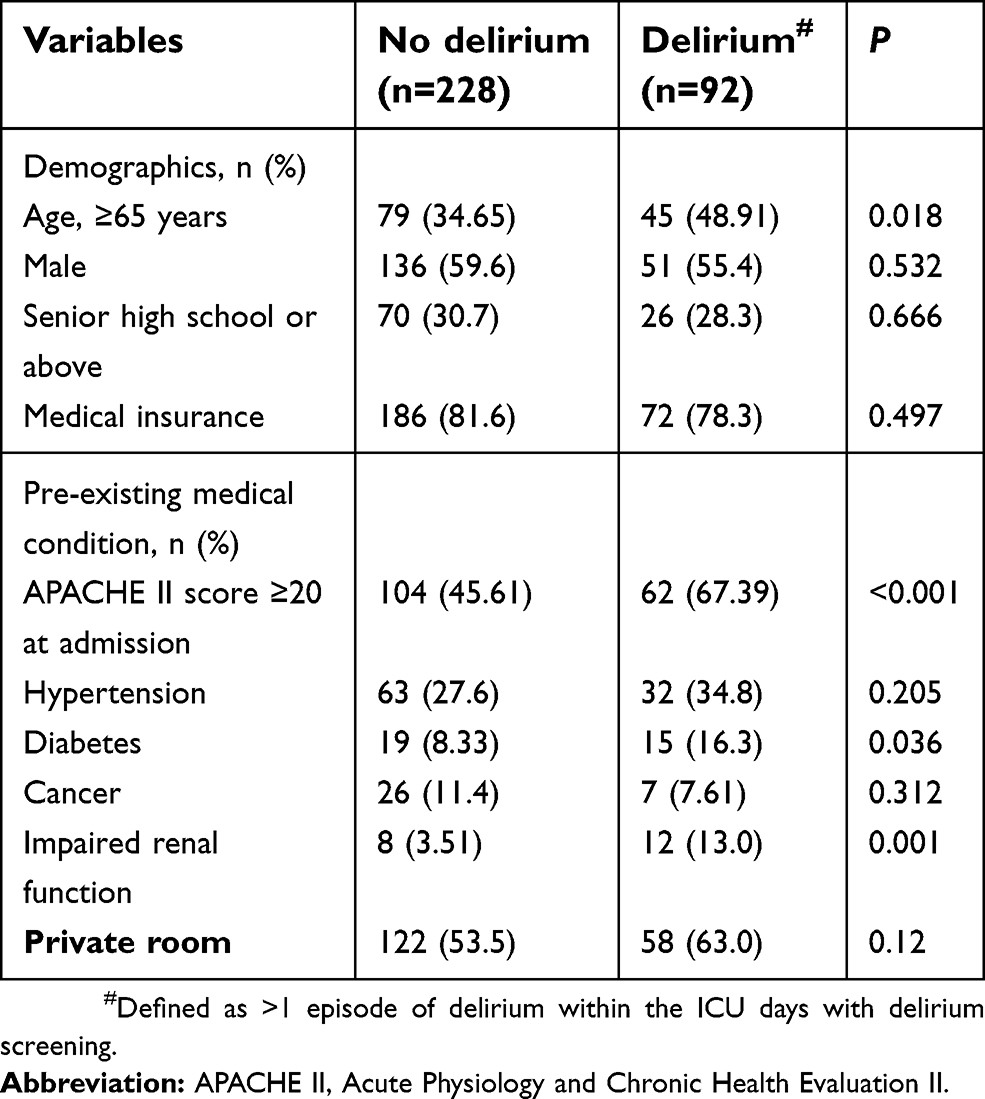 | Table 2 Comparison of routine risk factors associated with delirium |
Besides these routine widely studied risk factors, we also evaluated daily interventions, including mechanical ventilation, artificial airway, deep intravenous catheter, drainage tube, arterial line, gastric tube, urinary catheter, use of vasoactive drugs, and sedative medications (Table 3). Surprisingly, significant differences between the delirium and non-delirium group were observed in most of these interventions, with mechanical ventilation (P<0.001), artificial airway (P<0.001), deep intravenous catheter (P=0.01), arterial line (P=0.007), gastric tube (P<0.001), urinary catheter (P=0.006), use of vasoactive drugs (P=0.003), and sedative medication (P<0.001).
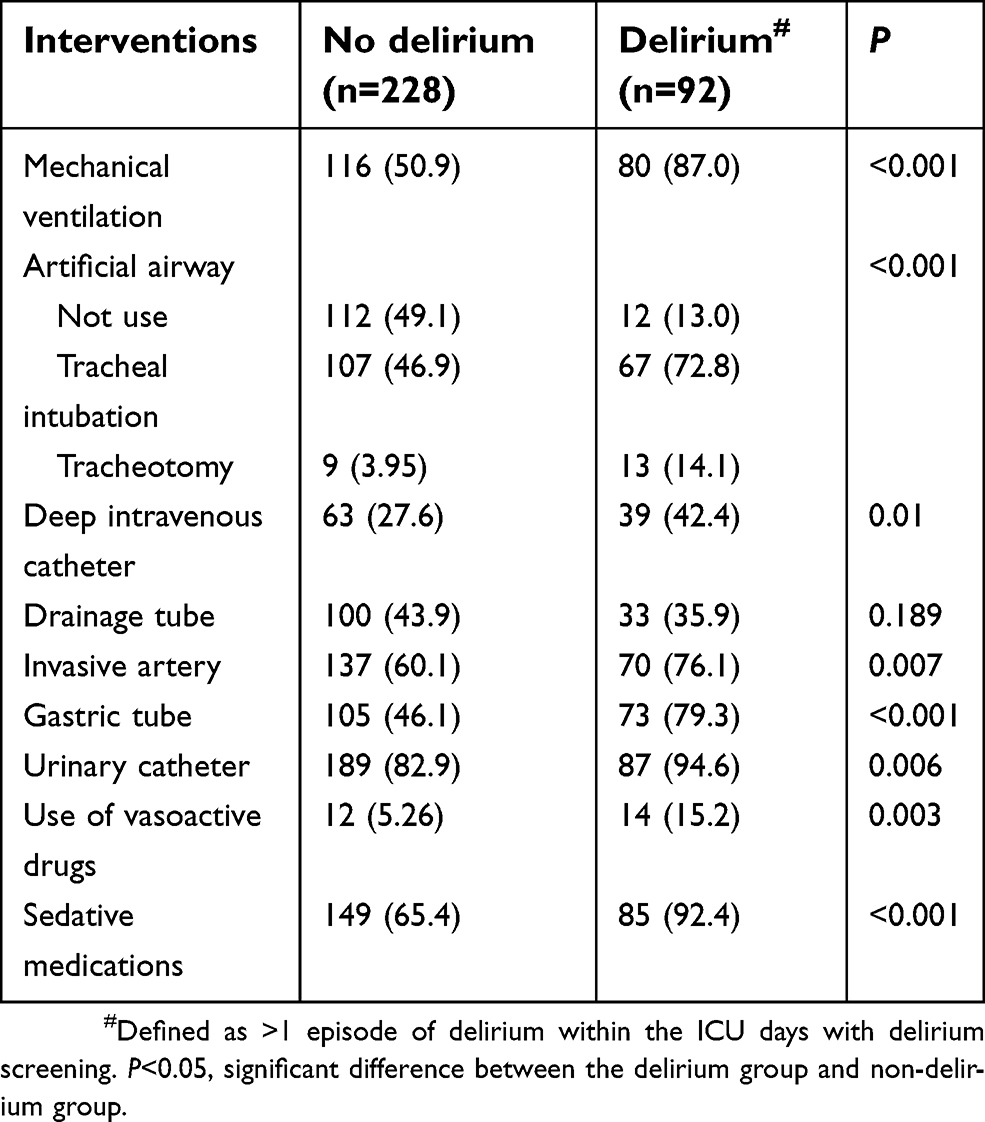 | Table 3 Comparison between delirium group and non-delirium group in terms of interventions |
Taken together, univariate analysis showed that sex, education, medical insurance, hypertension, cancer, drainage tube, and private room were not significantly different between patients with delirium and patients never delirious (Tables 2 and 3).
Multivariate analysis
Multi-logistic regression analysis (Table 4) revealed 3 factors that were retained in the optimized multivariate model after adjustingwith age and ICU length of stay. Mechanical ventilation increased the risk of delirium by odds ratio of 5.123 (95% CI: 2.501–10.494, P<0.001). APACHE II score≥20 at admission is the only predisposing factors that associated with increased risk of delirium (OR 1.897; 95% CI: 1.045–3.441, P=0.035). Gastric tube was the other precipitating risk factor that was associated with delirium (OR 1.935, 95% CI: 1.012–3.698, P=0.046).
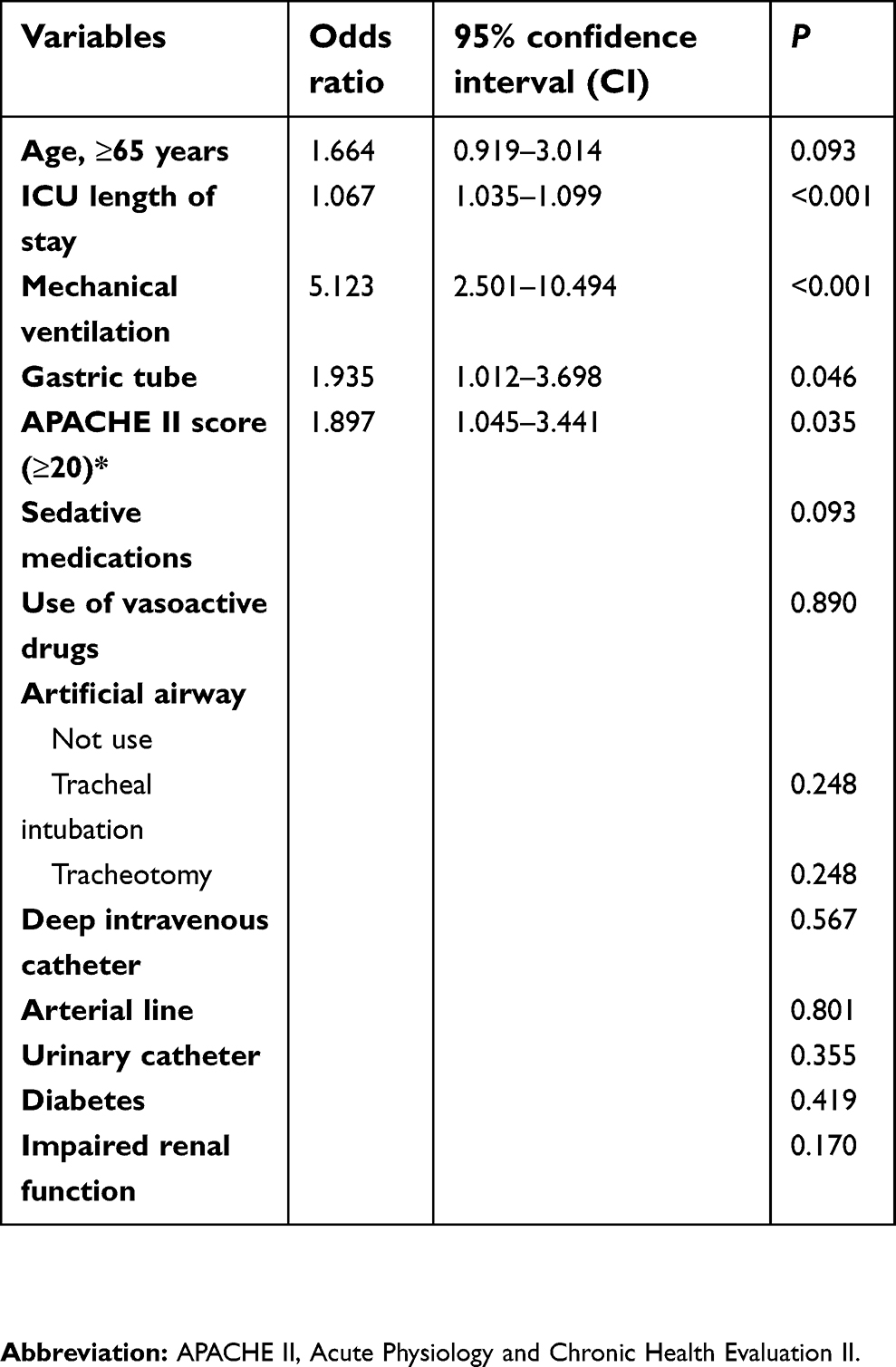 | Table 4 Multivariate analysis |
Consequences of delirium
The median duration of mechanical ventilation of patients who developed delirium was 3.5 (IQR: 1–7.75) days, and those who did not develop delirium was 1 (IQR: 0–2). There was a significant difference (P<0.001) in the duration of mechanical ventilation between the two groups.
The median duration of ICU stay and hospital stay of patients who developed delirium were 10 (IQR: 5–24) days and 12 (IQR: 6.25–27.25) days, respectively. For patients who did not develop delirium, the median duration of ICU stay and hospital stay were 2 (IQR: 1–6) and 5.5 (IQR:2–10) days, respectively. Patients with delirium had significantly longer duration of ICU stay (P<0.001) and hospital stay (P<0.001) (Table 5).
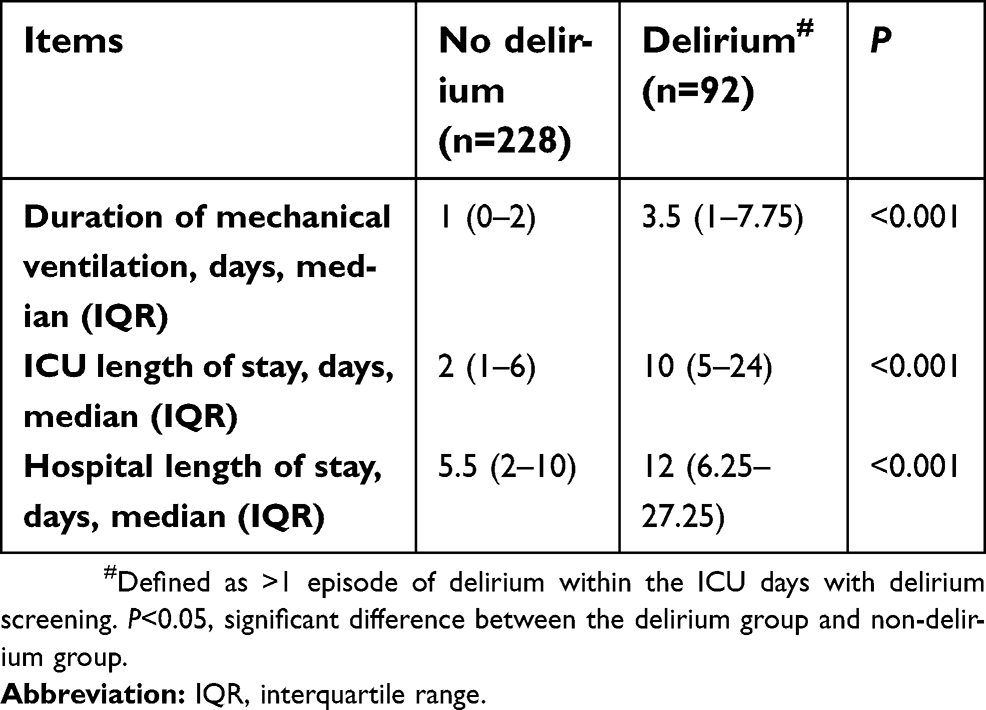 | Table 5 Outcomes of delirium |
Discussion
ICU patients present a high incidence rate of delirium, ranging from 20% to 80%.4,21,22 The relative huge variation is probably associated with many factors, such as patient populations, screening instruments for delirium (CAM-ICU vs ICDSC), and diagnosis and treatment habits. Risk factors for delirium have gradually drawn the clinicians and researchers’ attention in China. Therefore, relative reports increase obviously in recent years.23–26 The prevalence of delirium reported in these publications ranges from 24% to 42%.23–26 In the present study, the incidence of delirium was 28.75% (92 in 320 patients), which is generally consistent with these reports enrolling Chinese populations.23–26
Consistent with previous studies, the patients with delirium may more frequently above 65 years of age, and with APACHE II score ≥20.23,27,28 Moreover, delirious patients are more likely to have worse outcomes with longer duration of mechanical ventilation, ICU stay, and hospital stay.5,29–32
Older age is one of the most basic predisposing risk factors for ICU delirium.33,34 In the univariate analysis, we found that patients with delirium may more frequently above 65 years of age. Although hypertension has been identified as a risk factor of ICU delirium in a systematic review, 5 of the 7 studies included in the meta-analysis did not find association between hypertension and delirium in univariate analysis.13 Hypertension is not associated with delirium even in univariate analysis in our study cohort. Consistently, Yang et al had reported that hypertension is not a risk factor for delirium in univariate analysis in their Chinese patients’ cohort.24 Further studies should carry out to clarify the association of hypertension and delirium in Chinese critically ill patients.
Alcohol abuse is one of the most commonly identified risk factors for delirium in western countries.31,35,36 However, in our study cohort, only 9 of the 320 patients (2.81%) had alcohol abuse habits. Such differences existing in living habits may attribute to the difference of risk factors for ICU delirium between China and Western counties. Similarly, Yang and colleges also did not find that alcohol abuse history affected the development of delirium in sequential sedation critically ill patients.24 Thus, more studies identifying risk factors for the China population are necessary in order to identify Chinese-specific delirium risk factors.
A meta-analysis reported that patients with mechanical ventilation were more likely to develop delirium in the ICU setting than those without mechanical ventilation with an odds ratio of 4.51 (95% CI: 1.41–14.39).37 Our results revealed that mechanical ventilation increased the risk of delirium with an odds ratio of 5.123. Mechanical ventilation is a widely studied risk factor associated with delirium and strong evidences suggesting that minimizing the duration of mechanical ventilation could reduce delirium in critically ill patients.38–43 In addition, our results also showed that patient with delirium had prolonged mechanical ventilation compared with those without delirium. The association between delirium and prolonged mechanical ventilation have also been reported by a meta-analysis.44 Based on current evidence, it is difficult to distinguish the causal relationship between these factors, but we believe that mechanical ventilation and prolonged ventilation in the ICU may interact and aggravate the severity of the disease. Mechanically ventilated ICU patients are susceptible to inhalation, a possible cause of hypoxemia and lung infections, which increase their risk for developing delirium.45 In addition, the prolonged mechanical ventilation may further lead to sleep disorders due to noise, patient care interventions, disease severity, and the use of sedatives.41
Furthermore, many patients in the ICU have a large chance to receive a more invasive treatment, including artificial airway, deep intravenous catheter, drainage tube, arterial line, gastric tube, urinary catheter, use of vasoactive drugs, and sedative medication.36 However, the relationship between these interventions and delirium has been less elucidated. Here, we found that artificial airway, deep intravenous catheter, arterial line, urinary catheter, use of vasoactive drugs, and sedatives medication were linked to delirium in the univariate analysis. Gastric tube was a significant factor associated with delirium both in univariate analysis and multivariate analysis. Although the mentioned factors are related to the severity of the disease and even the necessary treatments, our results still suggest the necessity of earliest removal of tubes and catheters when no longer needed. At the meantime, it is necessary to increase the number of delirium screening in the more severely ill patients or the higher risk patients.
Our study has several limitations. First, we only screened patients once daily due to limited professional personnel, and mild temporary and fluctuated delirium might be missed. Second, we screened all patients during their stay in the ICU. This may inevitably cause time bias. A longer ICU stay could expose patients to a greater exposure to the risk factors, and increasing times of assessment may also increase the chance of delirium diagnosis due to the fluctuating characteristics of delirium. To minimize this time effect, we have adjusted with the duration of ICU stay in multivariate analysis. This problem exists extensively in the studies on risk factors for delirium; further research should focus more on improving the study design in the first step other than use of better statistical methods. Third, we did not evaluate the severity or motor type of delirium which may be another important factor when examining delirium. In addition, we only preliminarily evaluated the effects of specific interventions on delirium, such as vasoactive drugs and sedation. There is no specific drug and dose analysis, partially due to the limited sample size. In the univariate analysis, we found that patients with vasoactive drugs/sedative medications are more likely to develop delirium than patients without vasoactive drugs/sedative medications, respectively. Due to the complexity of medications for patients in the ICU setting, in the future, a well-designed study on specific drugs and doses with larger sample size should be carried out.
Conclusion
Delirium was associated with a longer duration of mechanical ventilation, ICU stay, and hospital stay. Most of the less-studied therapeutic interventions for critically ill patients were associated with delirium in univariate analysis, including gastric tube, artificial airway, deep intravenous catheter, invasive artery, urinary catheter, use of vasoactive drugs, and sedative medication. Mechanical ventilation, APACHE II score≥20 at admission, and gastric tube were multivariate factors associated with increased risk of delirium after adjusting with age and ICU length of stay. Although being a preliminary study, this study suggests the necessity of earliest removal of tubes and catheters when no longer needed. We are currently conducting an in-depth multi-center study on the impact of therapeutic interventions on delirium.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911–922. doi:10.1016/S0140-6736(13)60688-1
2. Xing J, Sun Y, Jie Y, Yuan Z, Liu W. Perceptions, attitudes, and current practices regards delirium in China: A survey of 917 critical care nurses and physicians in China. Medicine (Baltimore). 2017;96(39):e8028. doi:10.1097/MD.0000000000008028
3. Klein Klouwenberg PM, Zaal IJ, Spitoni C, et al. The attributable mortality of delirium in critically ill patients: prospective cohort study. BMJ. 2014;349:g6652.
4. Mehta S, Cook D, Devlin JW, et al. Prevalence, risk factors, and outcomes of delirium in mechanically ventilated adults. Crit Care Med. 2015;43(3):557–566.
5. Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753–1762.
6. Rudolph JL, Inouye SK, Jones RN, et al. Delirium: an independent predictor of functional decline after cardiac surgery. J Am Geriatr Soc. 2010;58(4):643–649.
7. Saczynski JS, Marcantonio ER, Quach L, et al. Cognitive trajectories after postoperative delirium. N Engl J Med. 2012;367(1):30–39.
8. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306–1316.
9. Girard TD, Pandharipande PP, Carson SS, et al. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med. 2010;38(2):428–437.
10. van Eijk MM, Roes KC, Honing ML, et al. Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial. Lancet. 2010;376(9755):1829–1837. doi:10.1016/S0140-6736(10)61855-7
11. Page VJ, Ely EW, Gates S, et al. Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomised, double-blind, placebo-controlled trial. Lancet Respir Med. 2013;1(7):515–523. doi:10.1016/S2213-2600(13)70166-8
12. Inouye SK, Charpentier PA. Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA. 1996;275(11):852–857.
13. Zaal IJ, Devlin JW, Peelen LM, Slooter AJ. A systematic review of risk factors for delirium in the ICU. Crit Care Med. 2015;43(1):40–47. doi:10.1097/CCM.0000000000000625
14. Brown C, Dowdy D. Risk factors for delirium: are systematic reviews enough? Crit Care Med. 2015;43(1):232–233. doi:10.1097/CCM.0000000000000665
15. Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;301(5):489–499. doi:10.1001/jama.2009.56
16. Kim H, Chung S, Joo YH, Lee JS. The major risk factors for delirium in a clinical setting. Neuropsychiatr Dis Treat. 2016;12:1787–1793. doi:10.2147/NDT.S112017
17. Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263–306. doi:10.1097/CCM.0b013e3182783b72
18. Balas MC, Devlin JW, Verceles AC, Morris P, Ely EW. Adapting the ABCDEF bundle to meet the needs of patients requiring prolonged mechanical ventilation in the long-term acute care hospital setting: historical perspectives and practical implications. Semin Respir Crit Care Med. 2016;37(1):119–135. doi:10.1055/s-0035-1570361
19. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829.
20. O‘Connor PG, Schottenfeld RS. Patients with alcohol problems. N Engl J Med. 1998;338(9):592–602. doi:10.1056/NEJM199802263380907
21. McPherson JA, Wagner CE, Boehm LM, et al. Delirium in the cardiovascular ICU: exploring modifiable risk factors. Crit Care Med. 2013;41(2):405–413.
22. Weaver CB, Kane-Gill SL, Gunn SR, Kirisci L, Smithburger PL. A retrospective analysis of the effectiveness of antipsychotics in the treatment of ICU delirium. J Crit Care. 2017;41:234–239.
23. Zhang Z, Pan L, Deng H, Ni H, Xu X. Prediction of delirium in critically ill patients with elevated C-reactive protein. J Crit Care. 2014;29(1):88–92.
24. Yang J, Zhou Y, Kang Y, et al. Risk Factors of Delirium in Sequential Sedation Patients in Intensive Care Units. Biomed Res Int. 2017;2017:3539872.
25. Li G, Lei X, Ai C, Li T, Chen Z. Low plasma leptin level at admission predicts delirium in critically ill patients: A prospective cohort study. Peptides. 2017;93:27–32.
26. Wang J, Ji Y, Wang N, et al. Risk factors for the incidence of delirium in cerebrovascular patients in a Neurosurgery Intensive Care Unit: A prospective study. J Clin Nurs. 2018;27(1–2):407–415.
27. McNicoll L, Pisani MA, Zhang Y, Ely EW, Siegel MD, Inouye SK. Delirium in the intensive care unit: occurrence and clinical course in older patients. J Am Geriatr Soc. 2003;51(5):591–598.
28. Kanova M, Sklienka P, Roman K, Burda M, Janoutova J. Incidence and risk factors for delirium development in ICU patients - a prospective observational study. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2017;161(2):187–196.
29. Witlox J, Eurelings LS, de Jonghe JF, Kalisvaart KJ, Eikelenboom P, van Gool WA. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA. 2010;304(4):443–451.
30. Lin SM, Huang CD, Liu CY, et al. Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients. J Crit Care. 2008;23(3):372–379.
31. Ouimet S, Kavanagh BP, Gottfried SB, Skrobik Y. Incidence, risk factors and consequences of ICU delirium. Intensive Care Med. 2007;33(1):66–73.
32. Shehabi Y, Riker RR, Bokesch PM, Wisemandle W, Shintani A, Ely EW. Delirium duration and mortality in lightly sedated, mechanically ventilated intensive care patients. Crit Care Med. 2010;38(12):2311–2318.
33. Arumugam S, El-Menyar A, Al-Hassani A, et al. Delirium in the intensive care unit. J Emerg Trauma Shock. 2017;10(1):37–46.
34. Pandharipande P, Shintani A, Peterson J, et al. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology. 2006;104(1):21–26.
35. Heymann A, Sander M, Krahne D, et al. Hyperactive delirium and blood glucose control in critically ill patients. J Int Med Res. 2007;35(5):666–677.
36. Van Rompaey B, Elseviers MM, Schuurmans MJ, Shortridge-Baggett LM, Truijen S, Bossaert L. Risk factors for delirium in intensive care patients: a prospective cohort study. Crit Care. 2009;13(3):R77.
37. Huai J, Ye X. A meta-analysis of critically ill patients reveals several potential risk factors for delirium. Gen Hosp Psychiatry. 2014;36(5):488–496.
38. Sharma A, Malhotra S, Grover S, Jindal SK. Incidence, prevalence, risk factor and outcome of delirium in intensive care unit: a study from India. Gen Hosp Psychiatry. 2012;34(6):639–646.
39. Ranhoff AH, Rozzini R, Sabatini T, Cassinadri A, Boffelli S, Trabucchi M. Delirium in a sub-intensive care unit for the elderly: occurrence and risk factors. Aging Clin Exp Res. 2006;18(5):440–445.
40. Peterson JF, Pun BT, Dittus RS, et al. Delirium and its motoric subtypes: a study of 614 critically ill patients. J Am Geriatr Soc. 2006;54(3):479–484.
41. Tsuruta R, Nakahara T, Miyauchi T, et al. Prevalence and associated factors for delirium in critically ill patients at a Japanese intensive care unit. Gen Hosp Psychiatry. 2010;32(6):607–611.
42. Shi CM, Wang DX, Chen KS, Gu XE. Incidence and risk factors of delirium in critically ill patients after non-cardiac surgery. Chin Med J. 2010;123(8):993–999.
43. Cebula TA, Payne WL, Feng P. Simultaneous identification of strains of Escherichia coli serotype O157: h7and their Shiga-like toxin type by mismatch amplification mutation assay-multiplex PCR. J Clin Microbiol. 1995;33(1):248–250.
44. Zhang Z, Pan L, Ni H. Impact of delirium on clinical outcome in critically ill patients: a meta-analysis. Gen Hosp Psychiatry. 2013;35(2):105–111.
45. Elpern EH, Scott MG, Petro L, Ries MH. Pulmonary aspiration in mechanically ventilated patients with tracheostomies. Chest. 1994;105(2):563–566.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.