")
Back to Journals » Infection and Drug Resistance » Volume 15
Risk Factors for Acute Kidney Injury Induced by Intravenous Polymyxin B in Chinese Patients with Severe Infection
Authors Jia X , Guo C, Yin Z, Zhang W, Du S, Zhang X
Received 24 February 2022
Accepted for publication 13 April 2022
Published 19 April 2022 Volume 2022:15 Pages 1957—1965
DOI https://doi.org/10.2147/IDR.S363944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Xuedong Jia,1,2 Cuohui Guo,1 Zhao Yin,1,2 Wan Zhang,1,2 Shuzhang Du,1,2 Xiaojian Zhang1,2
1Department of Pharmacy, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 2The Precision Clinical Pharmacy Key Laboratory of Henan Province, Zhengzhou, People’s Republic of China
Correspondence: Xuedong Jia; Shuzhang Du, Department of Pharmacy, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To analyze the risk factors for acute kidney injury (AKI) induced by intravenous polymyxin B in Chinese patients with severe infection and to provide a reference for clinicians and pharmacists.
Methods: We retrospectively analyzed patients treated with intravenous polymyxin B from August 2018 to August 2020 in a Chinese teaching hospital. Renal function was evaluated during therapy with polymyxin B and at the end of the treatment. Univariate and multivariate analyses were conducted to determine risk factors for the nephrotoxicity of polymyxin B.
Results: A total of 321 patients were included, and the incidence of AKI was 26.2% and 25.1% during polymyxin B therapy and at the end of treatment, respectively. Independent risk factors for AKI during therapy with polymyxin B were septic shock, coadministration of vancomycin or loop diuretics, and advanced age (≥ 60 years), while the incidence of AKI during treatment with polymyxin B was considered to be an independent risk factor for AKI at the end of the treatment.
Conclusion: Septic shock, coadministration of vancomycin or loop diuretics, and advanced age (age ≥ 60 years) were found to be risk factors for AKI induced by intravenous polymyxin B. Clinicians and pharmacists should consider these factors when designing and recommending treatment with polymyxin B.
Keywords: polymyxin B, acute kidney injury, risk factors, anti-infective therapy
Introduction
Polymyxin B was introduced in the 1950s and has been gradually replaced by safer clinical antibiotics due to its high incidence of adverse effects, especially acute kidney injury (AKI, 10–50%),1,2 and the detection of carbapenem-resistant organisms (CROs) has posed great challenges for clinical treatment in recent years.3–5 In 2017, the World Health Organization (WHO) published a catalog of 12 families of bacteria for which new antibiotics are urgently needed, and the first three of them turn out to be CROs,6 making the clinical options extremely limited. Polymyxin B has gained renewed interest because of the high sensitivity of gram-negative bacilli, especially CROs, to this drug.7–9 However, clinicians have many concerns about polymyxin B due to the high incidence of nephrotoxicity, especially as polymyxin is mainly used in patients with critical infections who often have various risk factors, which may further increase the probability of nephrotoxicity.10,11 Therefore, it is necessary to explore the risk factors for AKI induced by polymyxin B.
A meta-analysis based on an observational study in 2018 showed that the incidence of polymyxin B-induced AKI was 29.8% (95% CI 23.8–36.7%), while the criteria for AKI had a significant impact on the results.15 Because most previous studies have inconsistent criteria for AKI, the incidence of polymyxin-induced AKI and its risk factors remain unclear.12–14 Although a meta-analysis in 2021 using uniform RIFLE criteria explored the risk factors for polymyxin B-induced AKI,16 none of the studies included in this meta-analysis were from China. Meta-analyses showed a significant effect of the polymyxin type (colistin or polymyxin B), dose, patient age, number of concomitant nephrotoxins and use of diuretics, glycopeptides or vasopressors on the rate of nephrotoxicity,17 and preliminary studies have shown that active and reciprocal collaboration of pharmacists with physicians can help toward improving the pattern of colistin use.18 Therefore, studying the influencing factors of polymyxin B-induced AKI has important clinical significance for the later development of intervention strategies. Polymyxin B for injection was relaunched in China in September 2017, and its application in Chinese patients is relatively limited. Therefore, there is a lack of reports on the incidence of nephrotoxicity and risk factors for AKI during therapy with intravenous polymyxin B. In this study, we performed a retrospective analysis of patients receiving intravenous polymyxin B in a Chinese hospital to explore the risk factors for AKI.
Study Design
This study was approved and supervised by the ethics committee of the First Affiliated Hospital of Zhengzhou University (approval No. 2021-KY-0063-002) and was conducted at the First Affiliated Hospital of Zhengzhou University (currently the largest tertiary hospital in China with an authorized bed capacity of 10,000). Since we used secondary data for this study, we did not require the patient’s informed consent. We conducted the study following the Declaration of Helsinki. To ensure the confidentiality of information from the participants’ records, we did not record any personal identifiers on the data collection sheet, and secured data from participant records were not available to anyone except the investigators.
Patients who were hospitalized from August 2018 to August 2020 and received intravenous polymyxin B with severe infection were selected. Severe infections included febrile neutropenia, pneumonia, lung abscess, cellulitis, or sepsis. The inclusion criteria included (1) treatment with intravenous polymyxin B for severe infection; (2) course of treatment ≥ 3 days; (3) and patient age ≥ 18 years; moreover, (4) if patients had more than one hospitalization, only the first course of treatment was included. The exclusion criteria included the following: (1) treatment that was interrupted for various reasons; (2) lack of renal-function indicators and test results before and/or after polymyxin B treatment; (3) kidney transplantation before polymyxin B treatment; and (4) documented underlying kidney disease, including AKI or chronic kidney disease.
Data Collection
The patient data were registered through the Hospital Information Management System, including the basic information of the patients (gender, age, hospitalization time, clinical diagnosis and comorbidities); basic information on the medication (dose, frequency, duration of treatment, coadministration of drugs); the results of bacterial culture and drug-susceptibility tests; and the creatinine values and the results of the treatment course of patients before, during and after the medication. The serum creatinine (SCr) and glomerular filtration rate (GFR) before, during and within one week after the end of the treatment (if there were multiple measurements during the course of drug administration, the maximum level of SCr was recorded; if there were multiple measurements within one week after the end of the treatment, the minimum level of SCr was recorded), and the survival status at the time of discharge. SCr was determined by the picric acid rate method (Jaffe method).
Criteria for Nephrotoxicity
The incidence of nephrotoxicity was determined according to the RIFLE criteria.19 A 1.5-fold increase in SCr or a 25% decrease in GFR was considered to indicate the risk stage of renal function; a 2-fold increase in SCr or a 50% decrease in GFR was considered to indicate renal injury; and a 3.3-fold increase in SCr or a 75% decrease in GFR was considered to indicate renal failure. The incidence of AKI was calculated as the sum of the three filtration rates. A GFR of less than 60 mL/min was used as the criterion for determining baseline renal impairment. The maximum level of SCr (the minimum value of GFR) during the course of drug administration was used to measure the incidence of AKI during the use of polymyxin B, and the minimum level of SCr (the maximum value of GFR) retested within one week after the end of the treatment was used as the criterion for nephrotoxicity after the end of polymyxin B therapy.
Statistical Analysis
All statistical analyses were performed in IBM SPSS 24.0 software (IBM, United States). Normally distributed data are presented as the mean ± SD, and a t-test was used for comparison of means; nonnormally distributed count data are presented as the median (interquartile range [IQR]) and were tested by the Mann–Whitney U-test; count data are expressed as the number of examples and percentages and were tested by Pearson’s chi-square test (χ2) or Fisher’s exact test. Logistic regression analysis was used to investigate the independent factors of polymyxin B-associated AKI, and the variables found to be significantly associated with AKI in univariate analysis were entered into the multivariate logistic regression models to investigate the risk factors associated with AKI during polymyxin B therapy. A P value under 0.05 was considered statistically significant.
Results
A total of 705 patients received polymyxin B for injection from August 2018 to August 2020, and 291 patients were excluded because they did not meet the inclusion criteria. Ninety-three patients were subsequently excluded because they met the exclusion criteria. Ultimately, we enrolled 321 patients (Figure 1 for the screening process). The mean age was 56.93±15.33 years, and there were 249 male patients (77.6%) (Table 1). A total of 220 (68.5%) patients were admitted to the intensive care unit (ICU), and the median number of hospital days was 30 [18.0, 44.5] (Table 1). The daily dose of polymyxin B was 100 [100, 150] mg, and the dose was not adjusted according to the patient’s weight, age or GFR (Table 1). AKI occurred in 84 patients (26.2%) during polymyxin B therapy (33 patients with renal risk, 41 patients with renal injury, and 10 patients with renal failure). Renal function was tested in 195 patients at the end of polymyxin B therapy, and AKI occurred in 49 patients (16 patients with renal risk, 23 patients with renal injury, and 10 patients with renal failure). There was no statistically significant difference between the incidence of AKI during and at the end of polymyxin B therapy, as detailed in Table 2.
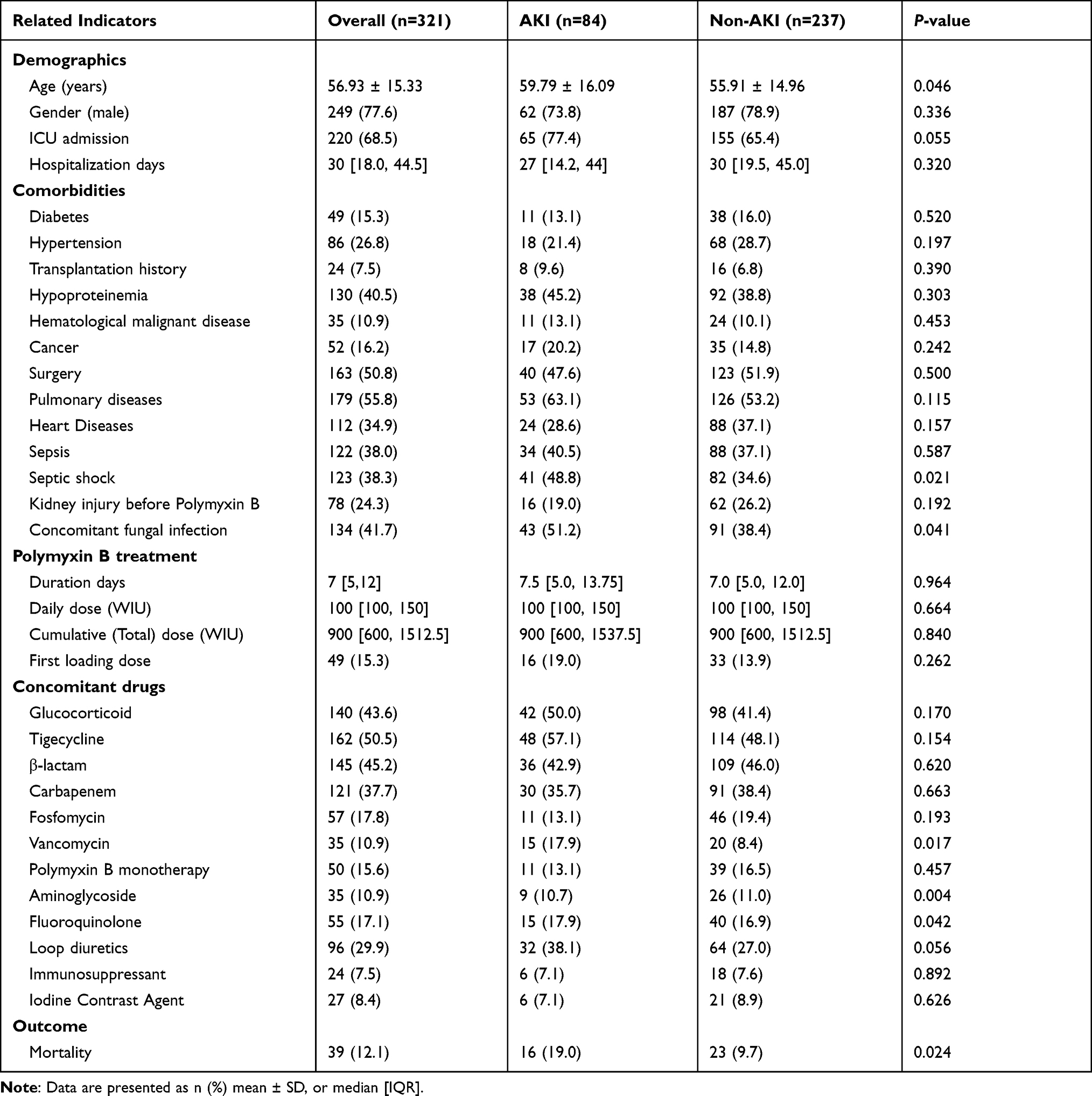 |
Table 1 The Baseline Characteristics of Patients and the Univariate Analysis of AKI- During Treatment Induced by Intravenous Polymyxin B |
 |
Table 2 Comparison Between AKI -During Treatment and AKI -End of Treatment by Intravenous Polymyxin B |
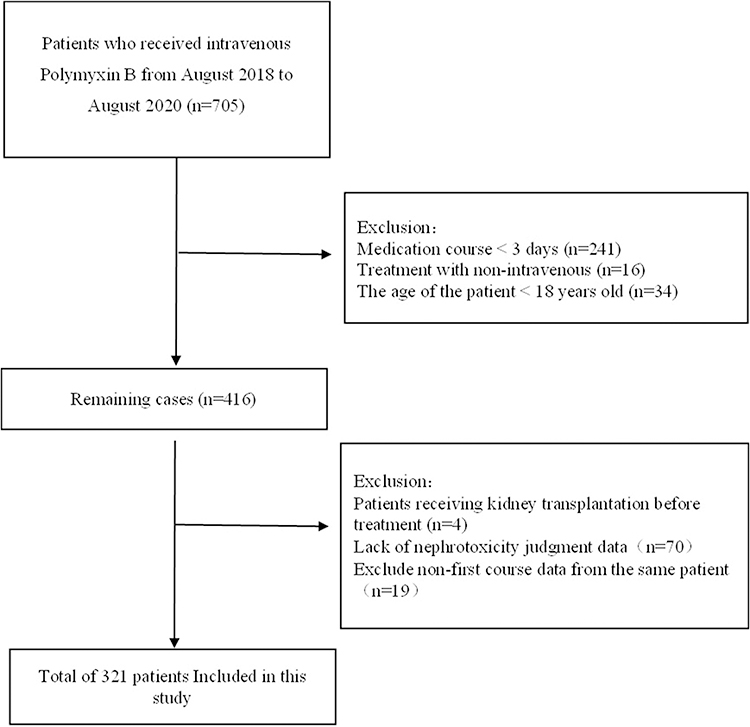 |
Figure 1 Schematic diagram of the case-screening process. |
The Incidence of AKI During Polymyxin B Therapy
The results of the univariate analysis of the incidence of AKI during treatment with polymyxin B showed that patient age, septic shock, fungal coinfection, coadministration of quinolones, coadministration of vancomycin, coadministration of loop diuretics, and coadministration of aminoglycosides were all factors affecting the incidence of AKI, as shown in Table 1. The risk factors screened in the univariate analysis were included in the logistic analysis model for regression analysis, and the results showed that septic shock (OR=1.972, 95% CI: 1.168–3.330, P =0.011), combined use of vancomycin (OR=2.585, 95% CI: 1.221–5.471, P =0.013), combined use of loop diuretics (OR=1.8322, 95% CI: 1.055–3.180, P =0.031) and advanced age (≥60 years) (OR=1.842, 95% CI: 1.091–3.112, P=0.022) were independent risk factors for the incidence of AKI during polymyxin B therapy, as detailed in Table 3.
 |
Table 3 Multi-Factor Analysis of AKI- During Treatment Induced by Intravenous Polymyxin B |
The Incidence of AKI at the End of Polymyxin B Treatment
A univariate analysis of the incidence of AKI at the end of treatment with polymyxin B showed that hypoproteinemia and the incidence of AKI during treatment with polymyxin B were risk factors for the incidence of AKI at the end of the course, as detailed in Table 4. The results of the regression analysis incorporating the risk factors screened in the univariate analysis (P<0.1) into the logistic analysis model showed that the incidence of AKI during polymyxin B therapy was an independent risk factor for the incidence of AKI at the end of the course (OR=20.760, 95% CI: 8.791–49.028, P<0.001), as shown in Table 5.
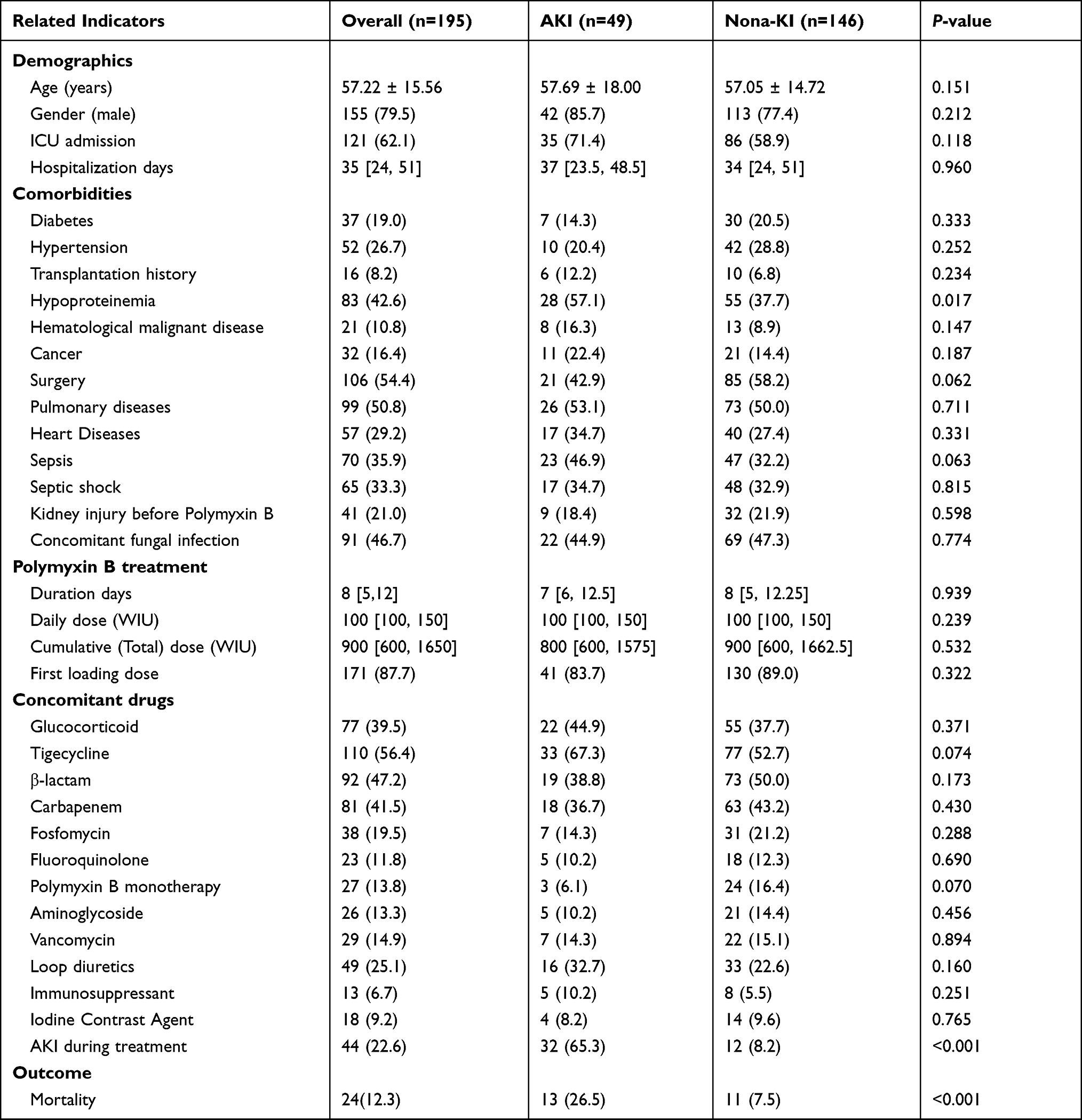 |
Table 4 The Univariate Analysis of AKI- End of Treatment Induced by Intravenous Polymyxin B |
 |
Table 5 Multi-Factor Analysis of AKI- End of Treatment Induced by Intravenous Polymyxin B |
Discussion
In this study, the clinical data of 321 patients who received intravenous polymyxin B were retrospectively analyzed, and the results showed that the incidence of AKI was 26.2% and 25.1% during polymyxin B therapy and the end of polymyxin B treatment, respectively. The difference between the incidence of AKI during polymyxin B therapy and that at the end of the course was not statistically significant, while both incidence rates were significantly associated with patient mortality at discharge compared with that in the non-AKI group. Independent risk factors for the incidence of AKI during polymyxin B therapy were septic shock, coadministration of vancomycin or loop diuretics, and advanced age (≥60 years). The incidence of AKI during treatment was an independent risk factor for AKI at the end of the course of treatment.
Several studies have examined the effect of the dosage of polymyxin B and the duration of therapy on the incidence of AKI.20–24 Elias et al20 analyzed 235 patients who developed AKI and found that a dosage of ≥200 mg/day polymyxin B was associated with a significantly increased risk of severe renal insufficiency (OR=4.5, 95% CI: 1.6–12.9), while the results of this study show that the dosage of ≥200 mg/day did not significantly increase the incidence of AKI, which may be related to the fact that the daily dosage of polymyxin B and the quartiles of cumulative doses used were closer in the patients in the AKI and non-AKI groups in this study. Colistin had similar findings regarding the effect of cumulative drug doses on AKI. Pogue et al showed that a colistin dose of ≥ 5.0 mg/kg per day was an independent predictor for nephrotoxicity.25 However, the results of two other studies showed that the difference in the median cumulative total dose for patients who developed AKI and those who did not was not significant.26,27 The results of a study conducted by Mostardeiro et al21 showed that there was an independent correlation between the duration of polymyxin B administration and renal damage (OR=1.06, 95% CI 1.00–1.12), while the effect of polymyxin B on the incidence of AKI remained unclear in this study because there was no significant difference in the duration of polymyxin B administration in both the AKI and the non-AKI groups. It is still inconclusive whether the loading dose of polymyxin B and the cumulative dose of polymyxin are associated with the incidence of AKI, and the present study did not find a relationship between these two variables and the incidence of AKI; consequently, further investigation is needed.
The results of the current study generally showed that advanced age was a risk factor for polymyxin B-induced AKI.28–30 However, the effects of advanced age on the incidence of AKI are still inconclusive. The results of this study showed that age ≥60 years was an independent risk factor for the incidence of AKI, and the incidence rate of AKI in patients ≥60 years in age was increased by 1.84 times that in patients under 60 years old. Therefore, the future administration of polymyxin B to elderly patients requires enhanced monitoring of its nephrotoxicity and timely adjustment of the drug dosage.
Severe infections (eg, severe pneumonia or sepsis) can induce renal dysfunction, and partial reversal of renal dysfunction can be achieved by clearing these infections. Therefore, it may be difficult to distinguish polymyxin B-induced AKI from infection-induced AKI without adequate anti-infective therapy.31,32 The results of this study show that the fact that patients had experienced septic shock during drug administration was an important risk factor for the incidence of AKI during polymyxin B therapy, but there was no correlation between septic shock during drug administration and the incidence of AKI at the end of the course of treatment. This suggests that intensifying anti-infective therapy at the beginning of drug-resistant bacterial infection to avoid the occurrence of septic shock in patients may reduce the incidence of AKI during polymyxin B therapy.
Concomitant use of one or more nonspecified nephrotoxic drugs has been considered a risk factor for AKI. Our study shows that coadministration of vancomycin or loop diuretics was an independent risk factor for the incidence of AKI during polymyxin B therapy, consistent with previous studies.14 A systematic review by Tiziana Ciarambino and coworkers33 also showed that piperacillin/tazobactam administered concomitantly with vancomycin appears to be associated with a greater risk of AKI than vancomycin monotherapy, and the true mechanisms behind this additive nephrotoxic effect require further research.
Although we included a relatively large sample size, our study has some limitations: (1) this study was retrospective and excluded many patients with incomplete clinical data, which might have led to selection bias; (2) this was a single-center study that therefore failed to represent the overall incidence of AKI in Chinese patients receiving polymyxin B therapy; and (3) the outcomes of polymyxin B-induced AKI could not be analyzed because the patient outcomes were not followed up after their discharge. (4) The dosage of polymyxin B in this retrospective study was given as a fixed daily dose in accordance with the requirements of the Chinese approval instructions, and the dose was not adjusted according to the age, weight and GFR of the patients. Current guidelines recommend adjusting the dose of polymyxin B based on total body weight.34 Therefore, more large-scale prospective clinical studies are needed in the future to investigate the risk factors for polymyxin B-induced AKI.
Conclusion
Septic shock during treatment, coadministration of vancomycin or loop diuretics, and advanced age (≥60 years) are independent risk factors for the incidence of AKI during polymyxin B therapy. Prospective large sample studies are needed to further clarify other risk factors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Thomas R, Velaphi S, Ellis S, et al. The use of polymyxins to treat carbapenem resistant infections in neonates and children. Expert Opin Pharmacother. 2019;20(4):415–422. doi:10.1080/14656566.2018.1559817
2. Falagas ME, Kyriakidou M, Voulgaris GL, et al. Clinical use of intravenous polymyxin B for the treatment of patients with multidrug-resistant Gram-negative bacterial infections: an evaluation of the current evidence. J Glob Antimicrob Resist. 2021;24:342–359. doi:10.1016/j.jgar.2020.12.026
3. Nguyen M, Joshi SG. Carbapenem resistance in Acinetobacter baumannii, and their importance in hospital-acquired infections: a scientific review. J Appl Microbiol. 2021;131(6):2715–2738. doi:10.1111/jam.15130
4. Tilahun M, Kassa Y, Gedefie A, et al. Emerging carbapenem-resistant Enterobacteriaceae infection, its epidemiology and novel treatment options: a review. Infect Drug Resist. 2021;14:4363–4374. doi:10.2147/IDR.S337611
5. Livermore DM, Nicolau DP, Hopkins KL, et al. Carbapenem-resistant enterobacterales, carbapenem resistant organisms, carbapenemase-producing enterobacterales, and carbapenemase-producing organisms: terminology past its “sell-by date” in an era of new antibiotics and regional carbapenemase epidemiology. Clin Infect Dis. 2020;71(7):1776–1782. doi:10.1093/cid/ciaa122
6. Willyard C. The drug-resistant bacteria that pose the greatest health threats. Nature. 2017;543(7643):15. doi:10.1038/nature.2017.21550
7. Li J. Reviving polymyxins: achievements, lessons and the road ahead. Adv Exp Med Biol. 2019;1145:1–8. doi:10.1007/978-3-030-16373-0_1
8. Soman R, Bakthavatchalam YD, Nadarajan A, et al. Is it time to move away from polymyxins?: evidence and alternatives. Eur J Clin Microbiol Infect Dis. 2021;40(3):461–475. doi:10.1007/s10096-020-04053-w
9. Nang SC, Azad MAK, Velkov T, et al. Rescuing the last-line polymyxins: achievements and challenges. Pharmacol Rev. 2021;73(2):679–728. doi:10.1124/pharmrev.120.000020
10. Pogue JM, Ortwine JK, Kaye KS. Are there any ways around the exposure-limiting nephrotoxicity of the polymyxins? Int J Antimicrob Agents. 2016;48(6):622–626. doi:10.1016/j.ijantimicag.2016.11.001
11. Sales GTM, Foresto RD. Drug-induced nephrotoxicity. Rev Assoc Med Bras. 2020;66:s82–s90. doi:10.1590/1806-9282.66.S1.82
12. Oliota AF, Penteado ST, Tonin FS, et al. Nephrotoxicity prevalence in patients treated with polymyxins: a systematic review with meta-analysis of observational studies. Diagn Microbiol Infect Dis. 2019;94(1):41–49. doi:10.1016/j.diagmicrobio.2018.11.008
13. Pogue JM, Tam VH. Toxicity in patients. Adv Exp Med Biol. 2019;1145:289–304. doi:10.1007/978-3-030-16373-0_17
14. Nation RL, Rigatto MHP, Falci DR, et al. Polymyxin acute kidney injury: dosing and other strategies to reduce toxicity. Antibiotics. 2019;8(1):24. doi:10.3390/antibiotics8010024
15. Gomes EC, Falci DR, Bergo P, et al. Impact of polymyxin-B-associated acute kidney injury in 1-year mortality and renal function recovery. Int J Antimicrob Agents. 2018;52(1):86–89. doi:10.1016/j.ijantimicag.2018.02.016
16. Sisay M, Hagos B, Edessa D, et al. Polymyxin-induced nephrotoxicity and its predictors: a systematic review and meta-analysis of studies conducted using RIFLE criteria of acute kidney injury. Pharmacol Res. 2021;163:105328. doi:10.1016/j.phrs.2020.105328
17. Wagenlehner F, Lucenteforte E, Pea F, et al. Systematic review on estimated rates of nephrotoxicity and neurotoxicity in patients treated with polymyxins [published online ahead of print]. Clin Microbiol Infect. 2021;27:671–686. doi:10.1016/j.cmi.2020.12.009
18. Vazin A, Karimzadeh I, Zand A, et al. Evaluating adherence of health-care team to standard guideline of colistin use at intensive care units of a referral hospital in Shiraz, Southwest of Iran. Adv Pharm Bull. 2017;7(3):391–397. doi:10.15171/apb.2017.047
19. Venkataraman R, Kellum JA. Defining acute renal failure: the RIFLE criteria. J Intensive Care Med. 2007;22(4):187–193. doi:10.1177/0885066607299510
20. Elias LS, Konzen D, Krebs JM, et al. The impact of polymyxin B dosage on in-hospital mortality of patients treated with this antibiotic. J Antimicrob Chemother. 2010;65(10):2231–2237. doi:10.1093/jac/dkq285
21. Mostardeiro MM, Pereira CA, Marra AR, et al. Nephrotoxicity and efficacy assessment of polymyxin use in 92 transplant patients. Antimicrob Agents Chemother. 2013;57(3):1442–1446. doi:10.1128/AAC.01329-12
22. Rigatto MH, Behle TF, Falci DR, et al. Risk factors for acute kidney injury (AKI) in patients treated with polymyxin B and influence of AKI on mortality: a multicentre prospective cohort study. J Antimicrob Chemother. 2015;70(5):1552–1557. doi:10.1093/jac/dku561
23. Dubrovskaya Y, Prasad N, Lee Y, et al. Risk factors for nephrotoxicity onset associated with polymyxin B therapy. J Antimicrob Chemother. 2015;70(6):1903–1907. doi:10.1093/jac/dkv014
24. Tuon FF, Rigatto MH, Lopes CK, et al. Risk factors for acute kidney injury in patients treated with polymyxin B or colistin methanesulfonate sodium. Int J Antimicrob Agents. 2014;43(4):349–352. doi:10.1016/j.ijantimicag.2013.12.002
25. Pogue JM, Lee J, Marchaim D, et al. Incidence of and risk factors for colistin-associated nephrotoxicity in a large academic health system. Clin Infect Dis. 2011;53:879–884. doi:10.1093/cid/cir611
26. Doshi NM, Mount KL, Murphy CV. Nephrotoxicity associated with intravenous colistin in critically ill patients. Hum Gene Ther Clin Dev. 2011;31:1257–1264. doi:10.1592/phco.31.12.1257
27. Vazin A, Malek M, Karimzadeh I. Evaluation of colistin nephrotoxicity and urinary level of kidney injury molecule-1 in hospitalized adult ICU patients. J Renal Inj Prev. 2020;9(2):e13. doi:10.34172/jrip.2020.13
28. Akajagbor DS, Wilson SL, Shere-Wolfe KD, et al. Higher incidence of acute kidney injury with intravenous colistimethate sodium compared with polymyxin B in critically ill patients at a tertiary care medical center. Clin Infect Dis. 2013;57(9):1300–1303. doi:10.1093/cid/cit453
29. Phe K, Lee Y, McDaneld PM, et al. In vitro assessment and multicenter cohort study of comparative nephrotoxicity rates associated with colistimethate versus polymyxin B therapy. Antimicrob Agents Chemother. 2014;58(5):2740–2746. doi:10.1128/AAC.02476-13
30. Maniara BP, Healy LE, Doan TL. Risk of nephrotoxicity associated with nonrenally adjusted intravenous polymyxin b compared to traditional dosing. J Pharm Pract. 2020;33(3):287–292. doi:10.1177/0897190018799261
31. Rello J, van Engelen TSR, Alp E, et al. Towards precision medicine in sepsis: a position paper from the European Society of Clinical Microbiology and Infectious Diseases. Clin Microbiol Infect. 2018;24(12):1264–1272. doi:10.1016/j.cmi.2018.03.011
32. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–e111. doi:10.1093/cid/ciw353
33. Ciarambino T, Giannico OV, Campanile A, et al. Acute kidney injury and vancomycin/ piperacillin/tazobactam in adult patients: a systematic review. Intern Emerg Med. 2020;15(2):327–331. doi:10.1007/s11739-020-02287-2
34. Tsuji BT, Pogue JM, Zavascki AP, et al. International consensus guidelines for the optimal use of the polymyxins: endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy. 2019;39(1):10–39. doi:10.1002/phar.2209
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.