")
Back to Journals » Patient Preference and Adherence » Volume 13
Risk factors associated with fatigue in chronic hepatitis B patients
Authors Zhong C, Yin J, Zheng Z, Cai S , Gao Y
Received 27 February 2019
Accepted for publication 6 June 2019
Published 4 July 2019 Volume 2019:13 Pages 1065—1072
DOI https://doi.org/10.2147/PPA.S206953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Chunxiu Zhong,1,* Junhua Yin,1,* Zhidan Zheng,2 Shaohang Cai,1,3 Yulin Gao4
1Department Of Infectious Diseases and Hepatology Unit, Nanfang Hospital, Southern Medical University, Guangdong Province, People’s Republic of China; 2Department Of Infectious Diseases, Dongguan People’s Hospital, Guangdong Province, People’s Republic of China; 3Intensive Care Unit, Sun Yat-Sen University Cancer Center, Guangzhou, People’s Republic of China; 4School of Nursing, Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Aim: To evaluate fatigue in chronic hepatitis B patients and its related independent factors, as well as the relationship between fatigue and health-related quality of life (HRQoL).
Materials and methods: The study enrolled 400 patients who met the selection criteria, and their sociodemographic information was collected. The 36-item Short-Form Health Survey (SF-36) and Multidimensional fatigue inventory 20 (MFI-20) were adopted to evaluate HRQoL and fatigue level.
Results: Significant differences between the fatigue group and non-fatigue group were observed for the female proportion (p=0.021), height (p=0.003), and weight (p=0.010), with or without regular exercise (p=0.001). We further determined the dimensions of fatigue that were affected by these factors and found that male patients showed significantly lower results than female patients in terms of physical fatigue (p=0.048), mental fatigue (p=0.017), and reduced motivation (p=0.025). In patients who exercised regularly, the fatigue scores for the three dimensions of general fatigue (p<0.001), physical fatigue (p=0.046), and reduced activity (p=0.008) were significantly better than in those without exercise habits. Multivariate analysis was conducted, which suggested that only height and regular exercise habits were the independent factors affecting the patients’ fatigue levels. We further analyzed the relationship between quality of life and fatigue. With respect to physiological HRQoL, the average fatigue score of patients with high HRQoL was 41.91, which was significantly lower than that of patients with low physiological HRQoL (56.18, p<0.001). Moreover, the average fatigue score in patients with low psychological HRQoL was 55.25, which was significantly higher than that of patients with high psychological HRQoL (41.23, p<0.001). Correlation analysis showed that the physiological HRQoL and psychological HRQoL scores were negatively correlated with fatigue score (r = −0.639, p<0.001 and r= −0.655, p<0.001, respectively).
Conclusions: In this study, we found that the fatigue dimensions of chronic hepatitis B patients differed between various subpopulations. Height and regular exercise habits were the independent factors that affected the patients’ fatigue levels. Moreover, HRQoL was correlated with fatigue level. For patients with risk factors of fatigue, target intervention is advised in order to decrease fatigue and increase HRQoL.
Keywords: chronic hepatitis B, health-related quality of life, fatigue, mental disorder, risk factor
Introduction
Chronic hepatitis B virus (HBV) infection has become a serious global public health burden.1–3 Epidemiological studies have shown that approximately 240 million patients are diagnosed with chronic HBV infection.1,4,5 Anti-HBV treatment is the most basic and important treatment for chronic hepatitis B (CHB).6 Currently, interferon and nucleoside analogs (NAs) are the drugs licensed for anti-HBV treatment.7–10 By inhibiting HBV replication to prevent the progression of liver disease in CHB patients, NAs cannot directly remove HBV covalently closed circular DNA.11 Therefore, most CHB patients need to undergo NAs treatment for a long period.12–15
Long-term disease burden and use of NAs may cause a decline in overall health resulting in fatigue and adverse effects in all aspects of social activities.12,16 Chronic fatigue persists as the disease progresses.17 Currently, the feeling of fatigue does not protect one’s own energy from depletion, but rather aggravates the patient’s disease itself.
The fatigue in CHB patients is closely related to their own disease and psychological factors. Evon18 surveyed 948 CHB patients and found that fatigue level was associated with demographics and clinical characteristics such as gender, income, advanced fibrosis, and poor mental health. Jang19 conducted a fatigue survey of CHB patients and showed that fatigue had a significant positive correlation with symptoms of anxiety. However, there are no studies evaluating the risk factors of fatigue in CHB patients or the relationship between fatigue and health related quality of life (HRQoL).
Therefore, this study aimed to evaluate the fatigue in CHB patients and its related independent factors. In this study, we analyzed various sociodemographic factors and evaluated the relationship between fatigue and HRQoL, thus providing an evidence-based medical evidence for targeted interventions.
Subjects and methods
Subjects
Our study enrolled 400 patients with CHB.The inclusion criteria were as followed: 1. serum hepatitis B surface antigen (HBsAg) sero-positivity for >6 months; 2. Accompanied by alanine aminotransferase (ALT) levels greater than the upper limit of normal (ULN), documented on two separate occasions, at least 2 weeks apart20 Patients were excluded if they had hepatocellular carcinoma; co-infections with hepatitis C or D virus, or human immunodeficiency virus; any medical evidences of autoimmune hepatitis; heavy alcohol abuse; pregnancy; or were previously treated with interferon. Sociodemographic information was collected for all participating subjects. The definition of “regular exercise” is exercised at least once a week in our study. The Institutional Review Board of Nanfang Hospital have approved the study. All participants provided written informed consent and the study was conducted in accordance with the Declaration of Helsinki.
The flow chart is shown in Figure S1.
Questionnaires
The 36-item Short-Form Health Survey (SF-36) was used to measure HRQoL of CHB patients.16 SF-36 is a brief self-administered HRQoL instrument commonly used in various disease populations. These items with higher scores represent better health conditions. The Chinese versions of the SF-36 questionnaire were available and provided by the developer. The validity and screening ability of this tool have been documented in various samples in China.
The fatigue status of CHB patients was assessed using the Multidimensional fatigue inventory-20 (MFI-20) that consists of 20 items, including general fatigue, physical fatigue, reduced activity, reduced motivation, and mental fatigue. Each content has 4 entries, with each dimension containing 2 fatigue and non-fatigue representation questions each. A high score indicates a high level of fatigue.
Statistical analysis
Continuous variables were expressed as mean and standard deviation, and categorical variables were expressed as percentages. The Chi-square test and student’s t-test were applied as required to determine statistically significant differences. Univariate and multivariate analyses were used to find factors associated with fatigue. The statistical significance of all tests was set as p<0.05 by two-tailed tests. Data analyses and quality control procedures were performed using SPSS for Windows, version 13.0 (SPSS Inc. Chicago, USA).
Results
Demographic data
The questionnaire was completed by 400 patients. Based on the mean fatigue score of 47.17, the patients were divided into two groups of those with fatigue (fatigue group) and those without (non-fatigue group). The differences between the two groups are shown in Table 1. Significant differences were observed for the female proportion (t=5.340, df=398, p=0.021), height (t=3.217, df=398, p=0.003), and weight (t=3.140, df=398, p=0.010), with or without regular exercise (t=10.669, df=398, P=0.001). We have also calculated the BMI and the results shows that BMI was significantly lower in fatigue group with 22.17(SD=3.08), compared with 22.85 (SD=3.06) in non-fatigue group (t=2.214, df=398, p=0.027).
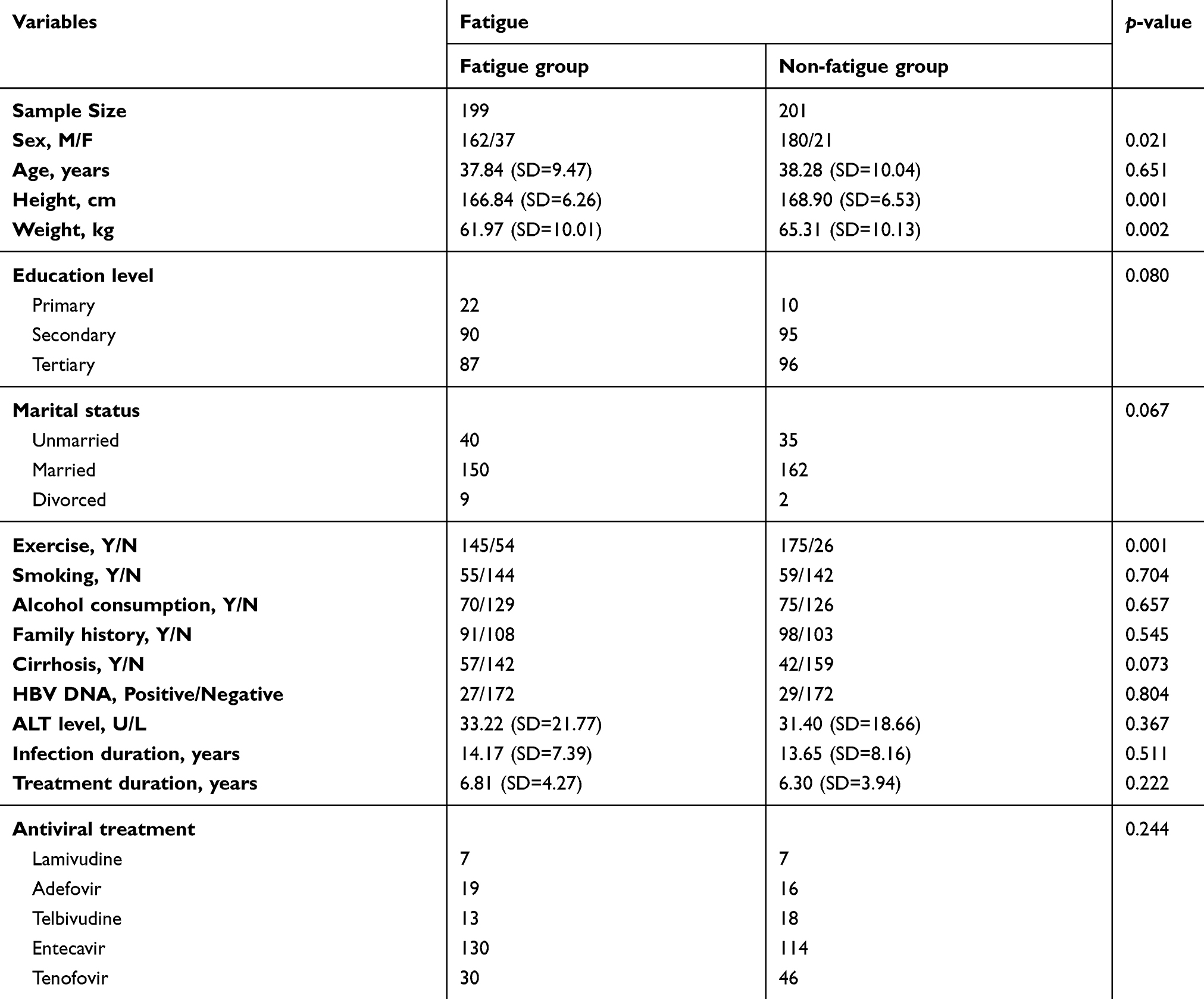 |
Table 1 Factors associated with fatigue among CHB patients |
Dimensions of fatigue caused by different factors
In order to determine the dimensions of fatigue that were decreased by these factors, we analyzed the differences between the two groups for five dimensions of fatigue (Figure 1). The results showed that female patients presented significantly higher values for physical fatigue, mental fatigue, and reduced motivation as compared to male patients. For patients who exercised regularly, the fatigue scores for the three dimensions of general fatigue, physical fatigue, and reduced activity were significantly better than those without exercise habits. However, regular exercise did not affect the fatigue scores for the other two dimensions.
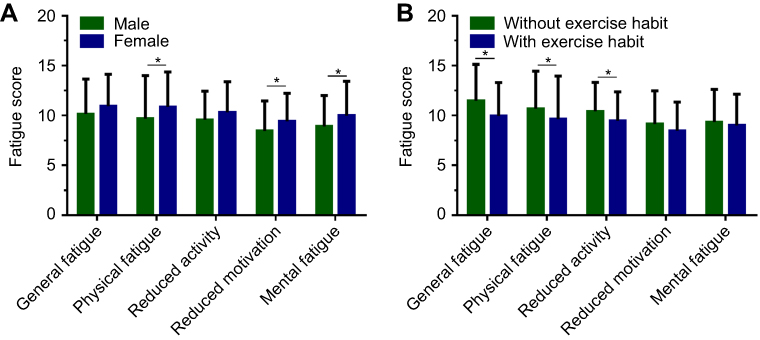 |
Figure 1 Different dimensions of fatigue caused by different factors. (A) Male patients show significantly lower values for physical fatigue (9.67, SD =4.33 vs 10.86, SD =3.51, p=0.048), mental fatigue (8.91±3.09 vs 9.98±3.45, p=0.017), and reduced motivation (8.46±2.99 vs 9.41±2.81, p=0.025) than female patients. (B) In patients exercising regularly, the fatigue scores for the three dimensions of general fatigue (9.94, SD =3.37 vs 11.47, SD =3.65, p<0.001), physical fatigue (9.63, SD =4.33 vs 10.68, SD =3.78, p=0.046), and reduced activity (9.46, SD =2.91 vs 10.41, SD =2.91, p=0.008) were significantly better than in those without exercise habits. *p<0.05. |
Independent factors associated with fatigue
Univariable and multivariable analyses were conducted to explore the independent factors that affected fatigue. Univariable results showed that gender, height, weight, and regular exercise were factors associated with fatigue in patients. However, multivariate analysis suggested that only height and regular exercise habits were the independent factors that affected the patients’ fatigue levels. Patients with shorter heights and irregular exercise habits were more likely to experience fatigue (Table 2).
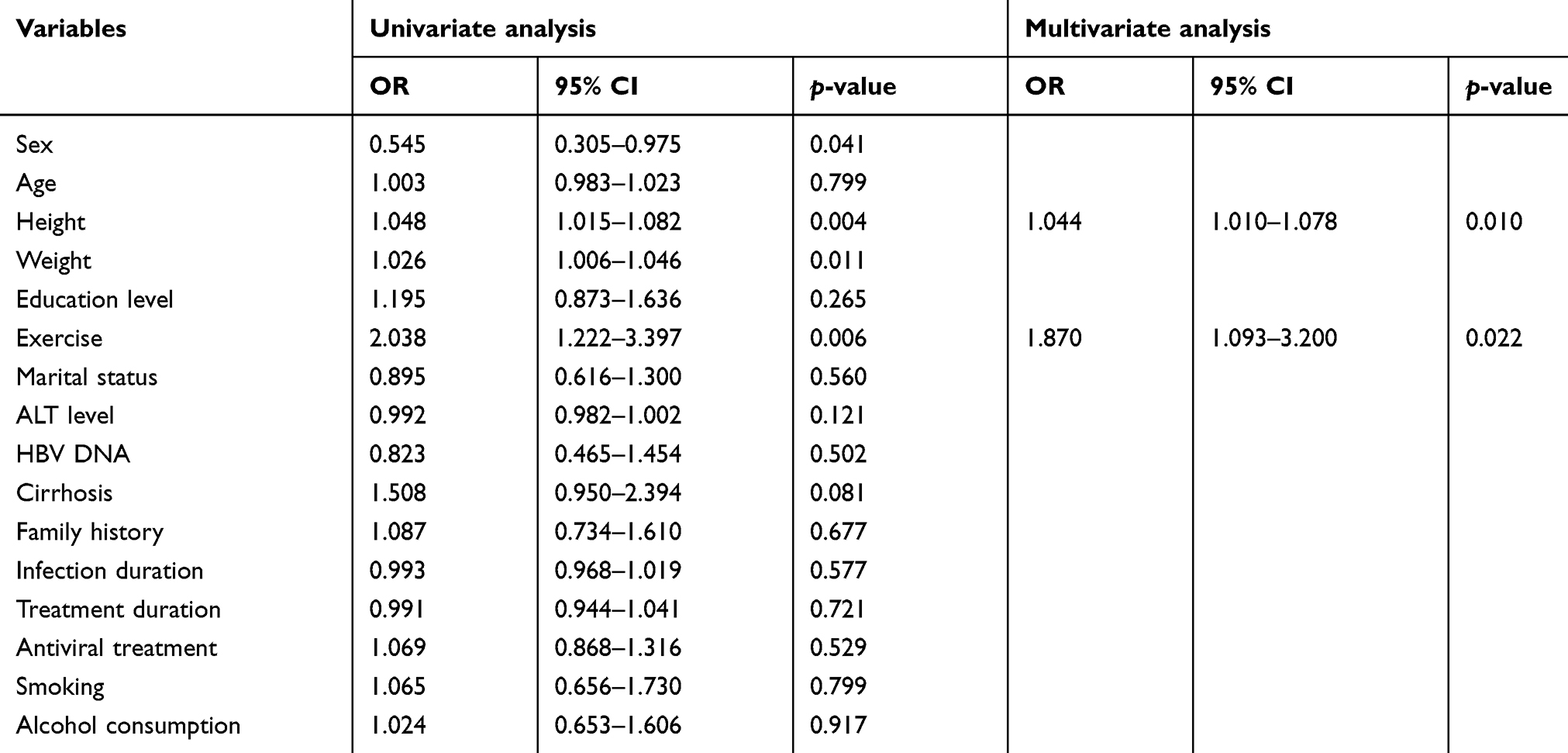 |
Table 2 Univariable and multivariable analysis for fatigue in CHB patients |
Relationship between hrqol and fatigue in CHB patients
We further analyzed the relationship between quality of life and fatigue. With respect to physiological HRQoL, the average fatigue score of patients with high HRQoL was 41.91, which was significantly lower than those with a low physiological HRQoL of 56.18 (t=12.253, df=398, p<0.001). Moreover, the average fatigue score of the patients with low HRQoL was 55.25, which was significantly higher than those with high psychological HRQoL of 41.23 (t=12.326, df=398, p<0.001), as shown in Figure 2.
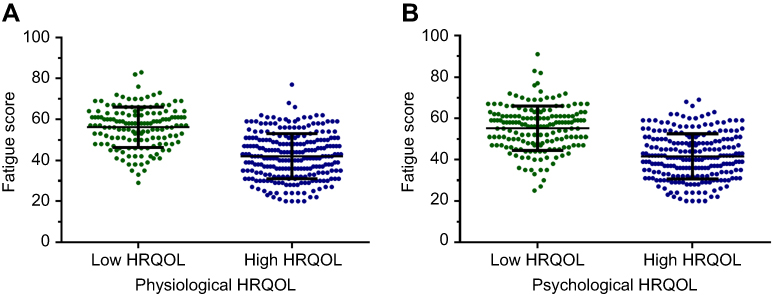 |
Figure 2 Different health related quality of life of patients with fatigue and non-fatigue. (A) Among the physiological HRQoL, the average fatigue score of patients with high HRQoL was 41.91, which was significantly lower than those with low physiological HRQoL of 56.18 (p<0.001). (B) The average fatigue score of patients with low HRQoL was 55.25, which was significantly higher than those with high psychological HRQoL of 41.23 (p<0.001).Abbreviation: HRQoL, health-related quality of life. |
Correlation analysis was conducted to explore the relationship between HRQoL and fatigue, and the results revealed that physiological HRQoL was negatively correlated with fatigue score (r = −0.639, p<0.001). The higher the physiological HRQoL of the patient, lower was the fatigue. In the same way, the psychological HRQoL score was negatively correlated with the fatigue score (r = −0.655, p<0.001). The higher the psychological life quality of the patient, lower was the fatigue, as shown in Figure 3.
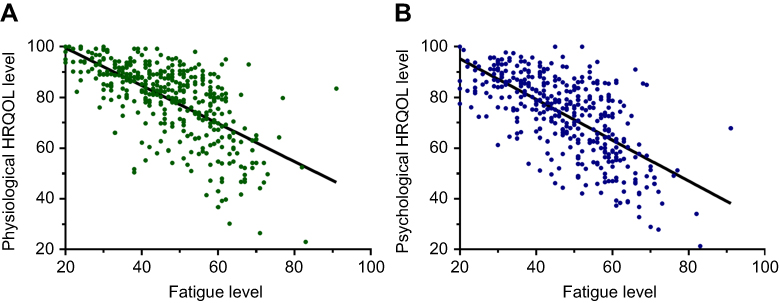 |
Figure 3 Correlation between HRQoL and fatigue in CHB patients (A) Correlation analysis showed that physiological HRQoL was negatively correlated with fatigue score (r = −0.639, p<0.001). (B) Psychological HRQoL score was negatively correlated with the fatigue score (r = −0.655, p<0.001).Abbreviations: HRQoL, health-related quality of life; CHB, chronic hepatitis B. |
Discussion
CHB patients not only suffer from impaired physical health, but also mood disorders and both affect their fatigue levels.21 The fatigue level of patients with CHB is obviously inferior to that of the general population.22,23 Although the impairment of fatigue in CHB patients has been confirmed, the difference in the fatigue dimensions of CHB patients in different subpopulations is unknown. The risk factors and relationship between fatigue and HRQoL is also unclear. This study was the first to observe the different dimensions of fatigue in patients with CHB. Herein, we found that the fatigue dimensions vary among different subpopulations of CHB patients. Female patients show significantly higher values in terms of physical fatigue, mental fatigue, and reduced motivation than male patients. In patients exercising regularly, the fatigue level of general fatigue, physical fatigue, and reduced activity are significantly better than in those without exercise habits. Moreover, height and regular exercise habits were the independent factors that affected the patients’ fatigue levels. Patients with shorter heights and irregular exercise habits were more likely to experience fatigue. For such patients, more attention should be paid to their fatigue and prompt intervention is necessary.
Fatigue is a common symptom in patients with CHB.18,19,24 Some CHB patients may regard fatigue as a symptom that they experienced in the course of CHB. However, fatigue in CHB patients, while affecting the symptoms of the disease itself, may also cause mental illness in patients.24 Hence, early identification of patients with fatigue is important. The results of this study revealed that women, irregular exercise, lower height, and lower body weight were prone to fatigue. For patients with CHB who complained of fatigue, health care providers may recommended that they rest and sleep more. In our study, results showed that regular exercise could reduce the risk of fatigue in these patients. Therefore, for fatigue patients with CHB, it is probably not a good suggestion to recommend more rest. Whether regular exercise can improve the fatigue status in patients with CHB remains to be studied further. However, it is reported that regular exercise in cancer patients relieves fatigue symptoms.25–27 In patients undergoing regular exercise after chemoradiotherapy, the level of fatigue was significantly lower than in the control group.
The data from this study also showed that patients with CHB having lower height and lower body weight were also more prone to fatigue. Clinically, such patients should pay more attention to their fatigue status and undergo timely intervention. However, it is unclear what intervention can alleviate the fatigue status of CHB patients. Previous studies have shown that massage can effectively improve symptoms including fatigue.28–30 Since fatigue is also a kind of emotional symptom, reducing stress and increasing social support can effectively alleviate fatigue. A breast cancer study in Australia evaluated the fatigue intervention in patients that included emotional interventions and social support programs.27 After the intervention, the patients’ fatigue levels decreased significantly. In the future, a prospective multicenter fatigue intervention study for CHB patients is necessary.
Although the decline in HRQoL and fatigue are common symptoms in patients with chronic hepatitis B, the relationship between the two has not been fully clarified. Our study found that the HRQoL of patients with CHB was closely related to fatigue. When fatigue declined, the HRQoL significantly increased. Therefore, clinical help and guidance in reducing fatigue in CHB patients, such as disease knowledge education and social support may improve the HRQoL in them; thus reducing incidence of adverse events caused by poor HRQoL.
There are some limitations in our study. Certain social characteristics were not included in the statistics. Furthermore, because all the patients were from one medical center, a prospective multicenter study is still necessary. In our study, we failed to further explore the reasons why height and weight contribute to the outcomes. We believe that a well-designed controlled study is needed to answer this question. We hope to answer this question in future research.
Conclusions
In this study, the results showed that female patients presented significantlyhigher levels of physical fatigue, mental fatigue, and decreased power than male patients. In patients exercising irregularly, the fatigue level of comprehensive fatigue, physical fatigue, and decreased activity were significantly more severe than in those with exercise habits. Height and regular exercise habits were the independent factors that affected the patients’ fatigue levels. Moreover, HRQoL was correlated with fatigue level. The more the fatigue, the poorer the HRQoL experienced by the patient. For patients with risk factors of fatigue, target intervention was necessary to decrease fatigue and increase HRQoL.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10:1–98.
2. Lu JB, Cai SH, Pan YH, Yun JP. Altered epidermal fatty acid-binding protein expression in hepatocellular carcinoma predicts unfavorable outcomes. Cancer Manag Res. 2018;10:6275–6284. doi:10.2147/CMAR.S181555
3. Xiao YB, Cai SH, Liu LL, Yang X, Yun JP. Decreased expression of peroxisome proliferator-activated receptor alpha indicates unfavorable outcomes in hepatocellular carcinoma. Cancer Manag Res. 2018;10:1781–1789. doi:10.2147/CMAR.S166971
4. Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50:661–662. doi:10.1002/hep.23190
5. Cai S, Cao J, Yu T, Xia M, Peng J. Effectiveness of entecavir or telbivudine therapy in patients with chronic hepatitis B virus infection pre-treated with interferon compared with de novo therapy with entecavir and telbivudine. Medicine (Baltimore). 2017;96:e7021. doi:10.1097/MD.0000000000007021
6. European Association for the Study of Liver 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67:370–398. doi:10.1016/j.jhep.2017.03.021
7. Cai S, Li Z, Yu T, Xia M, Peng J. Serum hepatitis B core antibody levels predict HBeAg seroconversion in chronic hepatitis B patients with high viral load treated with nucleos(t)ide analogs. Infect Drug Resist. 2018;11:469–477. doi:10.2147/IDR.S163038
8. Cai S, Ou Z, Liu D, et al. Risk factors associated with liver steatosis and fibrosis in chronic hepatitis B patient with component of metabolic syndrome. United European Gastroenterol J. 2018;6:558–566. doi:10.1177/2050640617751252
9. Cai S, Yu T, Jiang Y, Zhang Y, Lv F, Peng J. Comparison of entecavir monotherapy and de novo lamivudine and adefovir combination therapy in HBeAg-positive chronic hepatitis B with high viral load: 48-week result. Clin Exp Med. 2016;16:429–436. doi:10.1007/s10238-015-0373-2
10. Xue X, Cai S. Comment on “Assessment of liver stiffness in pediatric fontan patients using transient elastography”. Can J Gastroenterol Hepatol. 2016;2016:9343960. doi:10.1155/2016/9343960
11. Cai SH, Lv FF, Zhang YH, Jiang YG, Peng J. Dynamic comparison between Daan real-time PCR and Cobas TaqMan for quantification of HBV DNA levels in patients with CHB. BMC Infect Dis. 2014;14:85. doi:10.1186/1471-2334-14-85
12. Wu X, Cai S, Li Z, et al. Potential effects of telbivudine and entecavir on renal function: a systematic review and meta-analysis. Virol J. 2016;13:64. doi:10.1186/s12985-016-0512-8
13. Ou H, Cai S, Liu Y, Xia M, Peng J. A noninvasive diagnostic model to assess nonalcoholic hepatic steatosis in patients with chronic hepatitis B. Therap Adv Gastroenterol. 2017;10:207–217. doi:10.1177/1756283X16681707
14. Zeng J, Cai S, Liu J, Xue X, Wu X, Zheng C. Dynamic changes in liver stiffness measured by transient elastography predict clinical outcomes among patients with chronic hepatitis B. J Ultrasound Med. 2017;36:261–268. doi:10.7863/ultra.15.12054
15. Cai SH, Lu SX, Liu LL, Zhang CZ, Yun JP. Increased expression of hepatocyte nuclear factor 4 alpha transcribed by promoter 2 indicates a poor prognosis in hepatocellular carcinoma. Therap Adv Gastroenterol. 2017;10:761–771. doi:10.1177/1756283X17725998
16. Xue X, Cai S, Ou H, Zheng C, Wu X. Health-related quality of life in patients with chronic hepatitis B during antiviral treatment and off-treatment. Patient Prefer Adherence. 2017;11:85–93. doi:10.2147/PPA.S127139
17. Lai W, Cai S. Comment on “Prevalence of anxiety and depression in patients with inflammatory bowel disease”. Can J Gastroenterol Hepatol. 2018;2018:6747630. doi:10.1155/2018/6747630
18. Evon DM, Wahed AS, Johnson G, et al. Fatigue in patients with chronic hepatitis B living in North America: results from the Hepatitis B Research Network (HBRN). Dig Dis Sci. 2016;61:1186–1196. doi:10.1007/s10620-015-4006-0
19. Jang Y, Kim JH, Lee K. Validation of the revised piper fatigue scale in Koreans with chronic hepatitis B. PLoS One. 2017;12:e177690. doi:10.1371/journal.pone.0177690
20. European Association for the Study of Liver clinical practical guidelines: management of alcoholic liver disease. J Hepatol. 2012;57:399–420. doi:10.1016/j.jhep.2012.04.004
21. Modabbernia A, Ashrafi M, Malekzadeh R, Poustchi H. A review of psychosocial issues in patients with chronic hepatitis B. Arch Iran Med. 2013;16:114–122. doi:013162/AIM.0013
22. Karaivazoglou K, Iconomou G, Triantos C, et al. Fatigue and depressive symptoms associated with chronic viral hepatitis patients. health-related quality of life (HRQOL). Ann Hepatol. 2010;9:419–427.
23. Bao ZJ, Qiu DK, Ma X, et al. Assessment of health-related quality of life in Chinese patients with minimal hepatic encephalopathy. World J Gastroenterol. 2007;13:3003–3008. doi:10.3748/wjg.v13.i21.3003
24. Patidar KR, Bajaj JS. Tired of hepatitis B? Dig Dis Sci. 2016;61:953–954. doi:10.1007/s10620-016-4067-8
25. Meeusen R, Piacentini MF. Exercise, fatigue, neurotransmission and the influence of the neuroendocrine axis. Adv Exp Med Biol. 2003;527:521–525.
26. Piper BF, Cella D. Cancer-related fatigue: definitions and clinical subtypes. J Natl Compr Canc Netw. 2010;8:958–966.
27. Yates P, Aranda S, Hargraves M, et al. Randomized controlled trial of an educational intervention for managing fatigue in women receiving adjuvant chemotherapy for early-stage breast cancer. J Clin Oncol. 2005;23:6027–6036. doi:10.1200/JCO.2005.01.271
28. Ahmadidarrehsima S, Mohammadpourhodki R, Ebrahimi H, Keramati M, Dianatinasab M. Effect of foot reflexology and slow stroke back massage on the severity of fatigue in patients undergoing hemodialysis: a semi-experimental study. J Complement Integr Med. 2018;15(4).
29. Wang K, Qi S, Lai H, Zhu X, Fu G. Clinical massage therapy for patients with cancer-related fatigue protocol of a systematic review. Medicine (Baltimore). 2018;97:e13440. doi:10.1097/MD.0000000000013440
30. Lim JH, Kim H, Jeon C, Cho S. The effects on mental fatigue and the cognitive function of mechanical massage and binaural beats (brain massage) provided by massage chairs. Complement Ther Clin Pract. 2018;32:32–38. doi:10.1016/j.ctcp.2018.04.008
Supplementary material
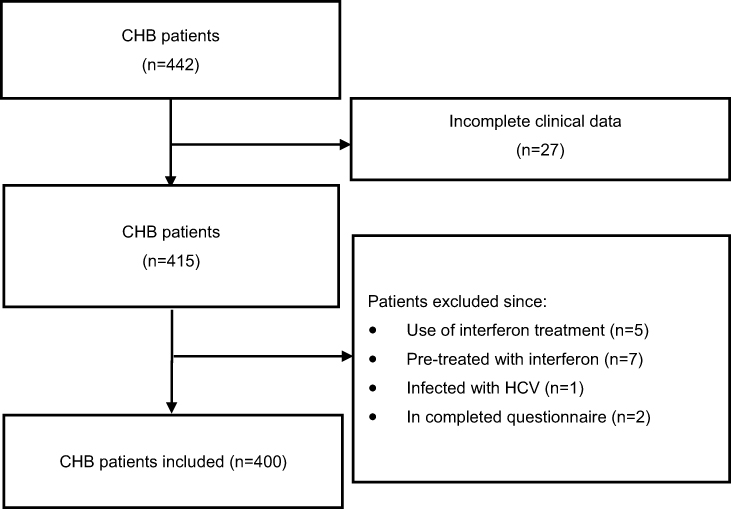 |
Figure S1 Flow chart of the two phases in the study. Abbreviations: CHB, chronic hepatitis B; HCV, hepatitis C virus. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.