")
Back to Journals » Infection and Drug Resistance » Volume 12
Risk Factors And Clinical Outcomes Of Hospital-Acquired MRSA Infections In Chongqing, China
Authors Mao P, Peng P, Liu Z, Xue Z, Yao C
Received 17 July 2019
Accepted for publication 30 October 2019
Published 27 November 2019 Volume 2019:12 Pages 3709—3717
DOI https://doi.org/10.2147/IDR.S223536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eric Nulens
Ping Mao,1,2,* Ping Peng,1,* Zhiyong Liu,3 Zhenrui Xue,1 Chunyan Yao1
1Department of Transfusion Medicine, Southwest Hospital, Third Military Medical University (Army Medical University), Chongqing 400038, People’s Republic of China; 2Department of Clinical Laboratory, Sichuan Provincial Crops Hospital of Chinese People’s Armed Police Forces, Leshan, Sichuan, 614000, People’s Republic of China; 3Department of Laboratory Medicine, Southwest Hospital, Third Military Medical University (Army Medical University), Chongqing 400038, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunyan Yao
Department of Transfusion Medicine, Southwest Hospital, Third Military Medical University (Army Medical University), No. 30 Gaotanyan Street, Chongqing 400038, People’s Republic of China
Tel/Fax +86 23 6876 5475
Email [email protected]
Background: Methicillin-resistant Staphylococcus aureus (MRSA) is a common pathogen of hospital infection with multi-drug resistant characteristics. Its spread and epidemic pose great challenges to nosocomial infection control. This study was aimed to identify risk factors for hospital-acquired MRSA (HA-MRSA) infections and investigate its clinical outcome, developing infection control strategies and improving patient outcomes.
Methods: A retrospective case-case-control study was conducted to compare patients in Southwest Hospital, Chongqing, People’s Republic of China from January 2018 to December 2018 with control patients. In this study, 251 patients with MRSA nosocomial infection, 339 patients with methicillin-sensitive Staphylococcus aureus strains (MSSA) nosocomial infection, and 300 patients with non-Staphylococcus aureus infection were included.
Results: Multivariate analysis showed that presence of central venous catheters (odds ratio [OR], 1.932; 95% confidence interval [CI], 1.074–3.477; P=0.028), sputum suction (OR, 2.887; 95% CI, 1.591–5.240; p<0.001), and total hospital stays more than 30 days (OR, 3.067; 95% CI, 2.063–4.559; P<0.001) were independent risk factors for HA-MRSA. Renal insufficiency (OR, 2.744; 95% CI, 1.089–6.914; P=0.032) and receipt of immunosuppressors (OR, 3.140; 95% CI, 1.284–7.678; P=0.012) were independent predictors of poor prognosis of MRSA nosocomial infection. Moreover, empirical use of antibiotics (OR, 0.514; 95% CI, 0.282–0.935; P=0.029) was a protective factor for poor prognosis of MRSA nosocomial infection. In-hospital mortality in the MRSA group was not statistically significant compared with the other two groups; however, the rate of poor prognosis in the MRSA group was higher than that of the MSSA group (27.5% vs 17.1%, χ2=9.200, P=0.002) and the control group (27.5% vs 16.0%, χ2=19.190, P=0.001).
Conclusion: Our results have shown presence of central venous catheters, sputum suction, and total hospital stays more than 30 days were associated with nosocomial MRSA infection. Patients with renal insufficiency and immunosuppressive therapy were more likely to cause poor prognosis with MRSA infection, and the empirical use of antibiotics can effectively reduce the adverse clinical outcomes caused by MRSA infection. Based on above findings, strategies to control MRSA infection should emphasize more attention to these patients and appropriate empirical use of antibiotics.
Keywords: risk factors, clinical outcomes, HA-MRSA, MSSA
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) was first discovered by British Jevons in 1961.1 Since its discovery, MRSA infection has almost spread all over the world. Although the prevalence of MRSA infection has been controlled to some extent in recent years, MRSA is still one of the important pathogens of community and hospital infection.2–4 The main mechanism of MRSA resistance was due to the changes in the properties of penicillin-binding protein (PBPs), which make MRSA resistant to almost all β-lactam antibiotics. Besides, MRSA can also show resistance to various antimicrobial agents such as macrolides antibiotics and aminoglycoside antibiotics by changing the target of antibiotic, reducing membrane permeability, and producing modified enzymes.5,6 It has been reported that MRSA leads to the highest rate of deaths, consumes the most medical resources, and imposes a great economic burden on patients with Staphylococcus aureus infection.7–10
The control and treatment of MRSA infection is one of the clinical challenges all over the world. There have been many reports on risk factors and clinical outcomes of MRSA hospital infection worldwide, but most of them are targeted at specific populations or departments.11–14 In our study, all adult inpatients in the hospital within a certain period were taken as the research objects, which is the special point of this study. In addition, case-control studies are commonly used to identify risk factors for MRSA infection.15–17 However, only analyzing patients infected with methicillin-sensitive Staphylococcus aureus strains (MSSA) as a control group does not represent all control subjects, which would cause bias in the results of the study. Case-case-control studies are superior to case-control studies in analyzing risk factors for drug-resistant pathogen infections.18 Therefore, we used case-case-control study to analyze the risk factors for MRSA infection and predictors of poor prognosis for MRSA infection which will make the conclusion more convincing. Therefore, the research conclusions will be more valuable for guiding the control strategy for MRSA infection prevalence and improve the prognosis of patients in Chongqing, People's Republic of China.
Materials And Methods
Ethics
Our study was approved by the medical ethics committee of the Southwest Hospital of the Third Military Medical University. It was a retrospective study, without direct intervention. All patient data are anonymous. Subjects’ information and privacy are fully protected. Therefore, the institutional review board waived the need for written informed consent provided by participants.
Study Design And Patient Population
The study used a case-case-control study to assess risk factors for HA-MRSA infections and to conduct clinical outcome analysis. The study was carried out in the Southwest Hospital of the Third Military Medical University, in Chongqing, People's Republic of China, with more than 1900 beds and an annual capacity of more than 135,000 patients. The research subjects included adults admitted to the Southwest Hospital between January 2018 and December 2018 (excluding pediatric and neonatal intensive care unit patients). Patients with MRSA and MSSA strains isolated within 48 hrs of admission were excluded. A repeated infection of a patient during a hospitalization was recorded only once.
Three groups were designed. The MRSA group consisted of hospitalized patients infected with MRSA strains during the study period. The MSSA group consisted of hospitalized patients infected with MSSA strains during the study period. The control group was randomly selected from patients infected with organisms other than Staphylococcus aureus. Three groups of patients were hospitalized at the same time, with the same exposure environment.
Microbiologic Methods
All the experiments involved in this study were interpreted with reference to the clinical and laboratory standards (CLSI) documents.19 The Vitek 2 automated system (bioMérieux, Marcy l’Etoile, France) was used for isolate identification and methicillin resistance testing. The quality control strains Staphylococcus aureus ATCC29213 (drug-resistant strain) and Staphylococcus aureus ATCC25923 (sensitive strain) were provided by the National Center for Clinical Laboratories (NCCL).
Data Collection And Definition
The relevant case information was collected from the medical record data management system and supplemented with relevant internal infection control data of the Southwest Hospital. The collected epidemiological and clinical medical record data included demographics (gender and age), underlying diseases (diabetes, malignancy, inflammatory disease, hypertension, renal insufficiency, cardiovascular disease, tuberculosis, hematopathy), unhealthy life styles (alcohol abuse, smoking history), invasive procedures (endoscopic therapy, presence of a Foley catheter, presence of central venous catheter, insertion of gastric tube, tracheotomy, sputum suction), medication (types of antibiotics used, empirical use of antibiotics, use antibiotics based on drug sensitivity test, antibiotic use more than 15 days), laboratory test (serum albumin, white blood cell examination), and receipt of immunosuppressors, radiotherapy, chemotherapy, surgery, admission to the intensive care unit (ICU) and other information.
Culture-positive specimens taken from sterile sites (such as blood, abdominal cavity) were directly defined as infection. According to the US Centers for Disease Control and Prevention (CDC) and the National Health Care Safety Network (NHSN), positive cultures from patients’ respiratory tract, urethra, and surgical wound site were also defined as infection.20 Mixed infection referred to the isolation of more than one pathogen from the same specimen. This study did not include patients with mixed infections. All cases defined as infection were cultured positive 48 hrs after admission.
The clinical outcomes of this study included total hospital stays more than 30 days, admission to the ICU, poor prognosis, and hospital mortality. Hospital mortality was defined as the death of the patient for any reason during hospitalization. Because of the economic and religious customs of Chongqing, some patients give up treatment and choose discharged automatically when their condition deteriorates sharply or there was no hope of cure. Therefore, this study defined hospital mortality and automatic discharge due to hopeless cure as poor prognosis.
Statistical Analysis
Data analysis was performed using SPSS22.0 software (IBM Corporation, Armonk, NY, USA). Categorical variables were presented by frequency and percentage. Continuous variables were summarized using mean±standard deviation or median. We compared MRSA group and MSSA group to the control group using bivariable logistic regression models adjusted for time at risk, respectively. As for the analysis of predictors of poor prognosis in the MRSA group, we used Student’s t-test or Mann–Whitney U-test to evaluate continuous variables and the χ2 test or two-tailed Fisher’s exact test for categorical variables. All variables with a P-value <0.10 in univariable analysis were included in the multivariable logistic regression analysis. Odds ratios (OR) and 95% confidence intervals (CI) were used to evaluate the strength of the associations. All analyses were two-tailed and the significance level was set as P<0.05.
Results
Distribution Of MRSA Isolates
During the study period, a total of 251 cases of MRSA infection were included. The most common types of infection were wound and soft tissue infection (155 cases, 61.8%), followed by respiratory tract infection (51 cases, 20.3%), bloodstream infection (24 cases, 9.6%), and intra-abdominal infection (8 cases, 3.2%). There were no significant differences in the infection types in three groups. The infection types of the three groups are listed in Table 1.
 |
Table 1 Comparison Of Infection Types Among The Three Groups |
Risk Factors
Case-Control Study 1: Comparative Analysis Of MRSA Group And Control Group
As shown in Table 2, there was no statistical difference in the age and gender of the three groups. Univariate statistical analysis showed that there were 5 factors with statistically significant differences between the MRSA group and the control group (P≤0.05): presence of a Foley catheter (OR, 1.588; 95% CI, 1.133–2.226; P=0.007), presence of central venous catheters (OR, 2.612; 95% CI, 1.516–4.502; P=0.001), sputum suction (OR, 3.771; 95% CI, 2.160–6.583; P<0.001), hospital stays before positive culture more than 15 days (OR, 1.829; 95% CI, 1.007–3.320; P=0.047), total hospital stays more than 30 days (OR, 3.626; 95% CI, 2.474–5.313; P<0.001).
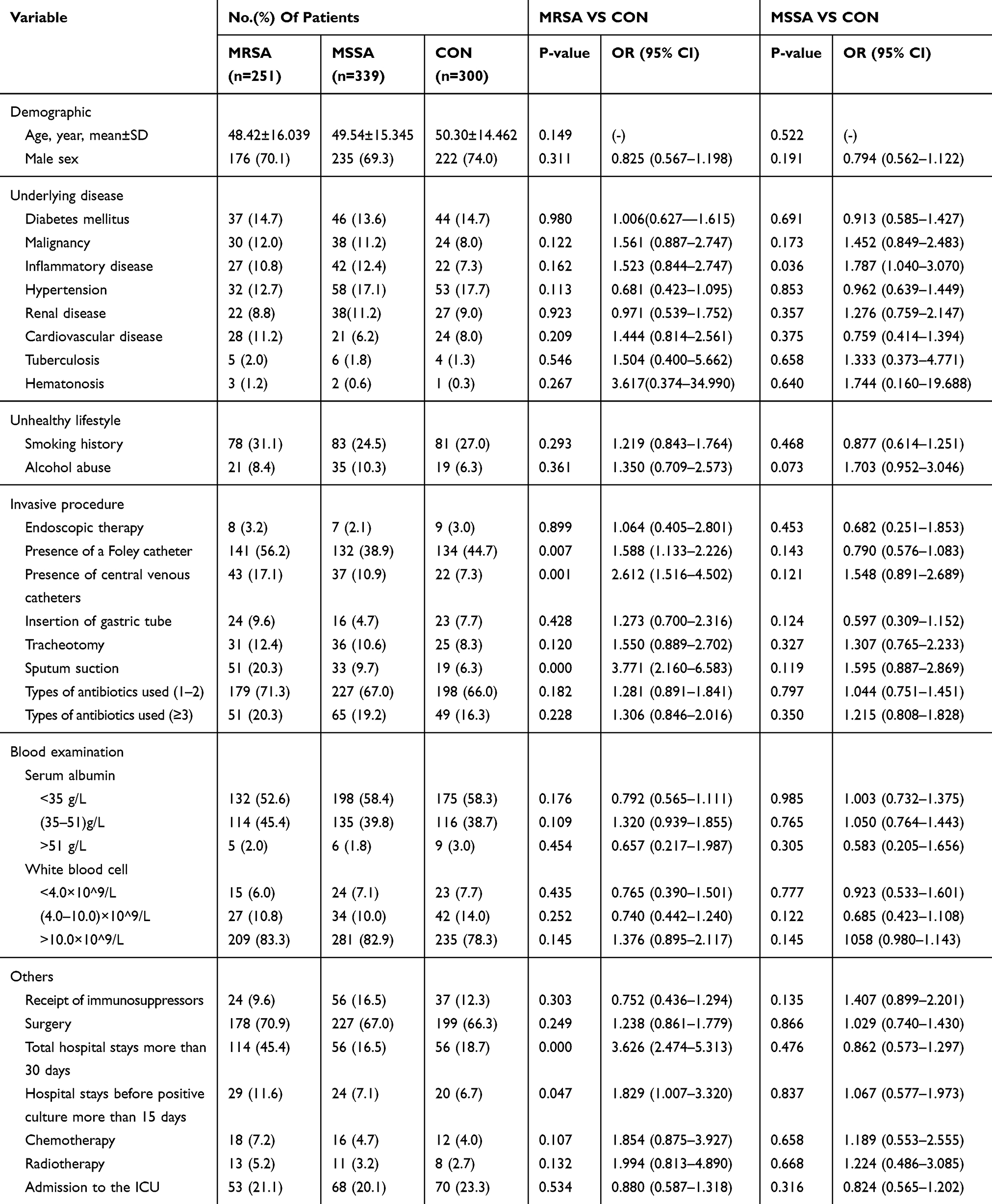 |
Table 2 Univariate Prediction Of Risk Factors For MRSA And MSSA Infection |
Case-Control Study 2: Comparative Analysis Of MSSA Group And Control Group
Univariate analysis showed a greater likelihood of inflammatory disease (OR, 1.787; 95% CI, 1.040–3.070; P=0.036) in the MSSA group compared with the control group. There was no significant difference in demographic characteristics, underlying diseases, and drug treatment between the MSSA group and the control group (Table 2).
Multivariate analysis showed that inflammatory disease was a risk factor for MSSA infection (OR, 1.820; 95% CI, 1.058–3.131; P=0.030) (Table 3).
 |
Table 3 Multivariate Analysis Of Risk Factors For MRSA And MSSA Infection |
Comparison Of Risk Factors Between MRSA Group And MSSA Group
By comparing the risk factors of the MRSA group and the MSSA group, we found that presence of central venous catheters, sputum suction, and total hospital stays more than 30 days were unique risk factors for infection with MRSA (Table 3).
Outcome Study
This study used a univariate analysis to analyze clinical outcomes (Table 4). During the hospitalization of the study patients, 43 (17.1%) patients died in the MRSA group, 45 (13.3%) patients died in the MSSA group, and 38 (12.7%) patients died in the control group. In the clinical poor prognosis analysis, 69 (27.5%) patients, 58 (17.1%) patients, and 48 (16.0%) patients in the MRSA group, MSSA group, and control group had poor prognosis, respectively. After comparing the clinical outcomes of three groups, there was no significant difference in in-hospital mortality between the three groups. However, patients infected with MRSA had longer hospital stay, were more likely to be admitted to ICU, and had poor prognosis.
 |
Table 4 Comparison Of Clinical Outcomes Among The Three Groups |
Univariate analysis showed that renal insufficiency (P=0.013), presence of central venous catheters (P=0.020), insertion of gastric tube (P=0.034), empirical use of antibiotics (P=0.030), and receipt of immunosuppressors (P=0.009) were predictors of poor prognosis in patients with MRSA infection (Table 5).
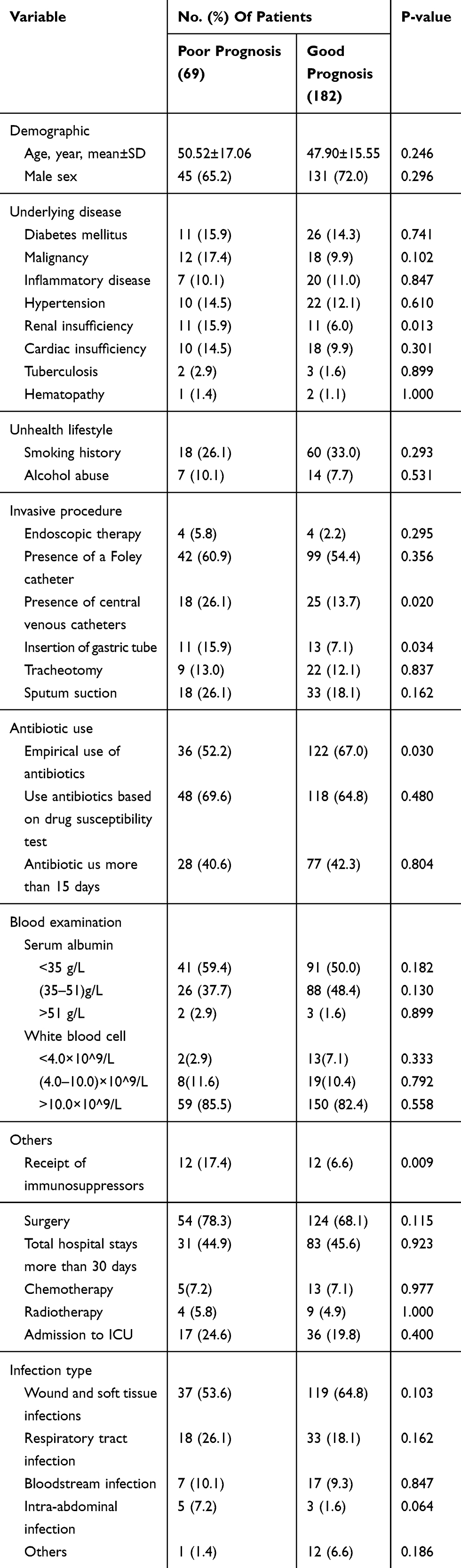 |
Table 5 Univariate Analysis Of Predictors For Poor Prognosis In The MRSA Group |
Multivariate analysis showed that renal insufficiency (OR, 2.744; 95% CI, 1.089–6.914; P=0.032) and receipt of immunosuppressors (OR, 3.140; 95% CI, 1.284–7.678; P=0.012) were independent predictors of poor prognosis of MRSA nosocomial infection. Moreover, empirical use of antibiotics (OR, 0.514; 95% CI, 0.282–0.935; P=0.029) was a protective factor for poor prognosis of MRSA nosocomial infection (Table 6).
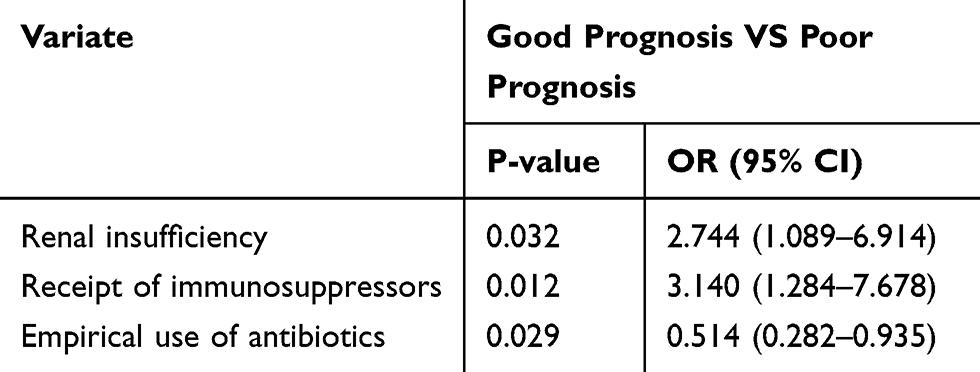 |
Table 6 Multivariate Analysis Of Factors Associated With Poor Prognosis In MRSA Group |
Discussion
MRSA has become one of the important pathogens of hospital infection worldwide, and is no longer limited to ICU, burn department and special medical institutions, which brings great challenges to hospital infection control.21–25 Chongqing, located in the southwest of People's Republic of China, lags behind in economic and medical technology development. Many local hospitals have limited manpower and material resources invested in infection control, leading to lax implementation of infection prevention measures and relative high rate of HA-MRSA infection.26 According to the drug resistance monitoring data of the Southwest Hospital, HA-MRSA infection rates were on the rise in 2016–2018, which reached 5.02% in 2018. In order to effectively control the spread and prevalence of drug-resistant bacteria and reduce the occurrence of adverse prognosis, we carried out a case-case-control study to investigate the risk factors and clinical outcomes of HA-MRSA infection in Chongqing, People's Republic of China.
In previous studies on the risk factors for HA-MRSA infections, Graffunder and Marshall et al showed that enteral feedings and longer lengths of stay before culture and ICU length of stay were correlated with MRSA infection.27,28 Washio et al showed that hypoalbuminemia may increase the risk of MRSA infection.29 Similar to these studies, the multivariate analysis of our study showed that presence of central venous catheters and total hospital stays more than 30 days before positive culture were independent risk factors of HA-MRSA infections. Karas et al also showed that presence of central venous catheters was a risk factor for MRSA nosocomial infections.30 Unlike these studies, we found that sputum suction was also a risk factor for MRSA infection. Sputum suction is commonly used to dredge the respiratory tract in clinical practice. The relatively frequent operation of sputum suction may increase mechanical stimulation of respiratory tract and mucosal injury, causing damage to the natural barrier of human body, thus MRSA is easy to colonize and infect. However, our study did not find hypoalbuminemia as a risk factor for MRSA infection.
The virulence of Staphylococcus is mainly determined by methicillin resistance, aggregation adhesion, and tetrad formation. There is insufficient evidence to prove that MRSA must be more virulent than MSSA.31 A study by Cosgrove et al showed the highest mortality of MRSA bacteremia caused by Staphylococcus aureus.32,33 However, there were no significant differences in hospital mortality between MRSA group and MSSA group in our study, although patients with MRSA infection had longer hospital stays and were more likely to be admitted to ICU and had a poor prognosis. Pastagia et al showed that organ impairment was independently associated with death from MRSA bacteremia.34 Our study clearly revealed that renal insufficiency was an independent predictor for poor prognosis of MRSA group. We suspect that this may be due to the low immunity of patients with renal insufficiency, which indirectly aggravates the degree of MRSA infection and leads to a poor prognosis. In addition, since the nephrotoxicity of the antibacterial drug itself imposes a great burden on patients with renal insufficiency, the utilization ratio of antibiotics in these patients is also reduced.35,36 We have also found that receipt of immunosuppressors was also a predictor for poor prognosis of MRSA group, which was not found in other studies. Due to individual differences and the complexity of the immune system, as well as the relevant clinical trials carried out less in People's Republic of China, there are no particularly strict pointers on the use of immunosuppressive agents. Off-label use of immunosuppressive agents based on immunotherapy experience is common among clinicians. This inevitably has the problem of improper use of immunosuppressive agents, which may be one of the reasons for the poor prognosis of immunosuppressive agents in patients with MRSA infection. It has been reported that appropriate and timely empirical antibiotic treatment can improve the prognosis of skin and soft tissue infections caused by MRSA.37 Our study also found that early empirical use of antibiotics can effectively reduce the occurrence of adverse clinical outcomes.
There were some limitations in our research. First, the sample size of our research was not large enough, therefore, there were limits on the efficacy of infection risk factors and clinical outcome studies. Secondly, most of the patients in the MRSA group of this study received clinical standard dose antibiotic therapy, and we did not have sufficient conditions to analyze the effect of different antibiotic treatment doses on clinical prognosis, which will be the content of our future study. Finally, our study did not address areas of MRSA outbreaks due to lax infection control measures.
In conclusion, our study showed that presence of central venous catheters and sputum suction as well as total hospital stays more than 30 days were independent risk factors for HA-MRSA infections in Chongqing, People's Republic of China. Renal insufficiency and receipt of immunosuppressors were independent predictors for poor prognosis in HA-MRSA infections. The empirical use of antibiotics can effectively reduce the adverse clinical outcomes caused by MRSA infection.
Data Availability Statement
The raw data required to reproduce these findings cannot be shared at this time due to legal or ethical reasons.
Acknowledgments
We thank Qinyun Mo for helping to get data from the medical record data management system. This study was supported by grants from the National Natural Science Foundation of China (81672108).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jevons MP. “Celbenin” - resistant Staphylococci. Br Med J. 1961;1(5219):113–114. doi:10.1136/bmj.1.5219.124-a
2. Defres S, Marwick C, Nathwani D. MRSA as a cause of lung infection including airway infection, community-acquired pneumonia and hospital-acquired pneumonia. Eur Respir J. 2009;34(6):1470–1476. doi:10.1183/09031936.00122309
3. Garcia C, Astocondor L, Reyes J, Carvajal LP, Arias CA, Seas C. Community-associated MRSA infection in remote Amazon basin area, Peru. Emerg Infect Dis. 2016;22(5):921–922. doi:10.3201/eid2205.151881
4. Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. 2007;298(15):1763–1771. doi:10.1001/jama.298.15.1763
5. Lee M, Hesek D, Suvorov M, Lee W, Vakulenko S, Mobashery S. A mechanism-based inhibitor targeting the dd-transpeptidase activity of bacterial penicillin-binding proteins. J Am Chem Soc. 2003;125(52):16322–16326. doi:10.1021/ja038445l
6. Vestergaard M, Frees D, Ingmer H. Antibiotic resistance and the MRSA problem. Microbiol Spectr. 2019;7(2):
7. Gould IM, Reilly J, Bunyan D, Walker A. Costs of healthcare-associated methicillin-resistant Staphylococcus aureus and its control. Clin Microbiol Infect. 2010;16(12):1721–1728. doi:10.1111/j.1469-0691.2010.03365.x
8. Claus F, Sachse A, Ried W. On the economic burden of MRSA in Germany. Gesundheitswesen. 2014;76(12):800–806. doi:10.1055/s-0034-1381987
9. Hübner C, Hübner NO, Hopert K, Maletzki S, Flessa S. Analysis of MRSA-attributed costs of hospitalized patients in Germany. Eur J Clin Microbiol Infect Dis. 2014;33(10):1817. doi:10.1007/s10096-014-2131-x
10. Ms SE, Youlin C, Qi M, et al. The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges. Infect Control Hospital Epidemiol. 2005;26(2):166–174. doi:10.1086/502522
11. Yano K, Minoda Y, Sakawa A, et al. Positive nasal culture of methicillin-resistant Staphylococcus aureus (MRSA) is a risk factor for surgical site infection in orthopedics. Acta Orthop. 2009;80(4):486–490. doi:10.3109/17453670903110675
12. Olivo TET, Melo ECD, Rocha C, Fortaleza CMCB. Risk factors for acquisition of methicillin-resistant Staphylococcus aureus among patients from a burn unit in Brazil. Burns. 2009;35(8):1104–1111. doi:10.1016/j.burns.2009.02.008
13. Pujol M, Peña C, Pallares R, Ayats J, Ariza J, Gudiol F. Risk factors for nosocomial bacteremia due to methicillin-resistant Staphylococcus aureus. Eur J Clin Microbiol Infect Dis. 1994;13(1):96–102. doi:10.1007/BF02026134
14. Cowie SE, Ma IS, Smith RM, Hsiang YN. Nosocomial MRSA infection in vascular surgery patients: impact on patient outcome. Vasc Endovascular Surg. 2005;39(4):327–334. doi:10.1177/153857440503900404
15. Salangsang JM, Harrison LH, Brooks MM, Shutt KA, Saul MI, Muto CA. Patient-associated risk factors for acquisition of methicillin-resistant Staphylococcus aureus in a Tertiary Care Hospital. Infect Control Hospital Epidemiol. 2010;31(11):1139–1147. doi:10.1086/656595
16. Arias-Ortiz PM, Calderon LD, Castillo JS, et al. Risk factors for methicillin-resistant Staphylococcus aureus bacteremia: a multicenter matched case-control study. Biomedica. 2016;36(4):612–619. doi:10.7705/biomedica.v36i4.3193
17. Lekkerkerk W, Haenen A, van der Sande M, et al. Newly identified risk factors for MRSA carriage in The Netherlands. PLoS One. 2017;12(11):e188502. doi:10.1371/journal.pone.0188502
18. Kaye KS, Harris AD, Samore M, Carmeli Y. The case-case-control study design: addressing the limitations of risk factor studies for antimicrobial resistance. Infect Control Hosp Epidemiol. 2005;26(4):346–351. doi:10.1086/502550
19. Jean B, Mpw P, Eliopoulos GM, Jenkins SG. M100 PerformanceStandards for Antimicrobial Susceptibility Testing.
20. Horan TCM, Andrus MRBC, Dudeck MAM. CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. AJIC. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
21. Klevens RM, Edwards JR, Tenover FC, Mcdonald LC, Horan T, Gaynes R. Changes in the epidemiology of methicillin-resistant Staphylococcus aureus in intensive care units in US hospitals, 1992-2003. Clin Infect Dis. 2006;42(3):389–391. doi:10.1086/499367
22. Nguyen DB, Lessa FC, Belflower R, et al. Invasive methicillin-resistant Staphylococcus aureus infections among patients on chronic dialysis in the United States, 2005-2011. Clin Infect Dis. 2013;57(10):1393–1400. doi:10.1093/cid/cit546
23. Boyce JM. Understanding and controlling methicillin-resistant Staphylococcus aureus infections. Infect Control Hosp Epidemiol. 2002;23(9):485–487. doi:10.1086/502092
24. Boyce JM. Increasing prevalence of methicillin-resistant Staphylococcus aureus in the United States. Infect Control Hosp Epidemiol. 1990;11(12):639–642. doi:10.2307/30146866
25. Boyce JM. Methicillin-resistant Staphylococcus aureus: a continuing infection control challenge. Eur J Clin Microbiol Infect Dis. 1994;13(1):45–49. doi:10.1007/BF02026126
26. Su-Fang G, Jun-Rui W, Yan-Qiu H, et al. Drug resistance and distribution characteristics of Gram-positive bacteria in Western China. Chin J Antibiotics. 2018.
27. Graffunder EM, Venezia RA. Risk factors associated with nosocomial methicillin-resistant Staphylococcus aureus (MRSA) infection including previous use of antimicrobials. J Antimicrob Chemother. 2002;49(6):999–1005. doi:10.1093/jac/dkf009
28. Marshall C, Wolfe R, Kossmann T, Wesselingh S, Harrington G, Spelman D. Risk factors for acquisition of methicillin-resistant Staphylococcus aureus (MRSA) by trauma patients in the intensive care unit. J Hospital Infect. 2004;57(3):245–252. doi:10.1016/j.jhin.2004.03.024
29. Washio M. Risk factors for methicillin-resistant Staphylococcus aureus (MRSA) infection in a Japanese elderly care nursing home. Epidemiol Infect. 1997;119(2):285. doi:10.1017/S0950268897007759
30. Karas JA, Enoch DA, Emery MM. Community-onset healthcare-associated MRSA bacteraemia in a district general hospital. J Hospital Infect. 2006;62(4):480–486. doi:10.1016/j.jhin.2005.10.001
31. Sandulescu O, Bleotu C, Matei L, et al. Comparative evaluation of aggressiveness traits in staphylococcal strains from severe infections versus nasopharyngeal carriage. Microb Pathog. 2017;102:45–53. doi:10.1016/j.micpath.2016.11.006
32. Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis. 2003;36(1):53–59. doi:10.1086/cid.2003.36.issue-1
33. Hassoun A, Linden PK, Friedman B. Incidence, prevalence, and management of MRSA bacteremia across patient populations—a review of recent developments in MRSA management and treatment. Critical Care. 2017;21(1):211. doi:10.1186/s13054-017-1801-3
34. Pastagia M, Kleinman LC, Lacerda De La Cruz EG, Jenkins SG. Predicting risk for death from MRSA bacteremia1. Emerg Infect Dis. 2012;18(7):1072–1080. doi:10.3201/eid1807.101371
35. Hanrahan T, Whitehouse T, Lipman J, et al. Vancomycin-associated nephrotoxicity: a meta-analysis of administration by continuous versus intermittent infusion [J]. Int J Antimicrob Agents. 2015;46(3):249–253. doi:10.1016/j.ijantimicag.2015.04.013
36. Harrison CJ. Innate immunity as a key element in host defense against methicillin resistant Staphylococcus aureus [J]. Minerva Pediatr. 2009;61(5):503–514.
37. Napolitano LM. Early appropriate parenteral antimicrobial treatment of complicated skin and soft tissue infections caused by methicillin-resistant Staphylococcus aureus. Surg Infect (Larchmt). 2008;9(s1):s17–s27. doi:10.1089/sur.2008.063.supp
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.