")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Risk Assessment of Recurrence and Autoimmune Disorders in Kikuchi Disease
Authors Jung HJ , Lee IJ, Yoon SH
Received 13 July 2020
Accepted for publication 27 August 2020
Published 22 September 2020 Volume 2020:13 Pages 1687—1693
DOI https://doi.org/10.2147/RMHP.S271283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Hyun Joo Jung,1 Il Jae Lee,2 Seung-Hyun Yoon3
1Department of Pediatrics, Ajou University Hospital, Ajou University School of Medicine, Suwon, Gyeonggi-do, South Korea; 2Department of Plastic Surgery, Ajou University Hospital, Ajou University School of Medicine, Suwon, Gyeonggi-do, South Korea; 3Department of Physical Medicine and Rehabilitation, Ajou University Hospital, Ajou University School of Medicine, Suwon, Gyeonggi-do, South Korea
Correspondence: Seung-Hyun Yoon Tel +82 31 219 5279
Fax +82 31 219 5209
Email [email protected]
Purpose: Kikuchi disease (KD) is typically a benign disease. Recent studies reporting recurrence or serious cases suggest a possible association of KD with systemic autoimmune disorders. We performed a long-term analysis of the characteristics of KD in patients of all ages and assessed KD recurrence or progress to systemic autoimmune disorders.
Patients and Methods: Electronic medical records of patients diagnosed with KD between April 1995 and May 2017 were reviewed for clinical and laboratory manifestations.
Results: In total, 480 patients were confirmed to have KD based on histopathology findings. The mean age at KD diagnosis was 24.4 years. Recurrence occurred in 11.3% of patients; 2.7% developed autoimmune diseases after KD diagnosis. Patients who experienced recurrence had more extranodal symptoms, lymphopenia, and a longer lymphopenia-recovery duration. Patients who developed autoimmune diseases after KD were more likely to have extranodal symptoms, KD recurrence, and anti-nuclear antibody positivity.
Conclusion: KD patients with risk factors need to be followed-up for KD recurrence and the development of systemic autoimmune diseases.
Keywords: Kikuchi disease, histiocytic necrotizing lymphadenitis, recurrence, autoimmune disorders
Introduction
Kikuchi disease (KD), also known as histiocytic necrotizing lymphadenitis or Kikuchi-Fujimoto disease, is characterized by fever and lymphadenopathy of unknown etiology and usually affects young Asian women.1–4 Recent reports describe KD as a form of lymphadenitis that can occur in people of all races and in both children and adults of both sexes.2,5–7 The extranodal symptoms of KD are uncommon and diverse, including skin rash, night sweats, weight loss, headache, cough, and abdominal pain.2,6,8,9 Although KD is generally a self-limiting and benign disease, varying rates of recurrence and fatality have been reported.2,6,10–14 Associations between KD and systemic autoimmune disorders, such as systemic lupus erythematosus (SLE), Sjögren’s syndrome, and adult-onset Still’s disease, have been reported.15–20 Studies have also suggested that KD is more likely to develop into systemic autoimmune disorders in patients with KD recurrence, extranodal symptoms, or anti-nuclear antibody (ANA) positivity.9–12,21 However, these studies had limitations such as short study durations and small sample sizes. In this study, we aimed to analyze the clinical characteristics of patients with KD of all ages over a period of more than 20 years and to evaluate the risk factors for KD recurrence or progression to systemic autoimmune disorders.
Patients and Methods
We reviewed the electronic medical records of patients who had been diagnosed with KD between April 1995 and May 2017 at Ajou University Hospital, a tertiary university hospital. KD was diagnosed when all of the following criteria were met: (1) systemic symptoms or physical findings compatible with those for KD; (2) exclusion of any other causes of lymphadenopathy; (3) histological examination of a lymph node biopsy specimen showing typical findings compatible with those for KD. The protocol of this study was approved by the Institutional Review Board of Ajou University Hospital (AJIRB-MED-MDB-20-058). Informed consent from study participants was waived due to the retrospective data collection and patient data de-identification prior to study analyses. The data collected included those of age, sex, presenting symptoms, laboratory test results, histological findings, treatment, and clinical outcome. Recurrence was defined as additional episodes of febrile lymphadenopathy before or after the pathological diagnosis, and these episodes were determined from the patients’ medical records, regardless of whether repeated pathological confirmation had been performed. We excluded cases involving recurrent episodes of lymphadenopathy in which other definite causes were identified. Between-group differences were evaluated using Student’s t- or Pearson χ2-test, as appropriate. Two-sided p-values of less than 0.05 were considered statistically significant. All statistical analyses were performed using the PASW Statistics 13 (SPSS Inc., Chicago, IL, USA) software package.
Results
General Characteristics of Patients with Kikuchi Disease
During this 22-year period, a total of 480 patients met the definition of KD. The mean age was 24.4 years (range 4–79 years), and 151 patients (31.5%) were aged <18 years (Figure 1A and B). The ratio of male patients to female patients was 1:1.32 for those under 18 years of age and 1:2.46 for those over 18 years of age (Figure 2). Table 1 shows the general characteristics of patients with KD. Of the 480 patients, 455 (94.8%) had lymphadenopathy and 381 (79.4%) had fever at the time of the initial diagnosis. Overall, 61 (12.7%) patients had systemic symptoms in addition to fever. Among systemic symptoms, rash, myalgia, fatigue, cough, rhinorrhea, abdominal pain, diarrhea, loss of appetite, and headache were predominant. Of the 425 patients whose laboratory findings were available for analysis, 201 (47.3%) had leukopenia (white blood cell count <4000/mm3), 132 (31.1%) had lymphopenia (absolute lymphocyte count <1500/mm3), and 43 (10.1%) had neutropenia (absolute neutrophil count <1500/mm3). Among the 201 patients with leukopenia, 113 (74.8% of 151) were children (under 18 years of age) and 88 (26.7% of 329) were adults (over 18 years of age). Of the 245 patients tested for ANAs, 69 (28.2%) tested positive; of these, 32 patients were younger than 18 years of age (46.4%). Of the 69 patients with ANA positivity, there were 32 (21.2% of 151) children and 37 (11.2% of 329) adults.
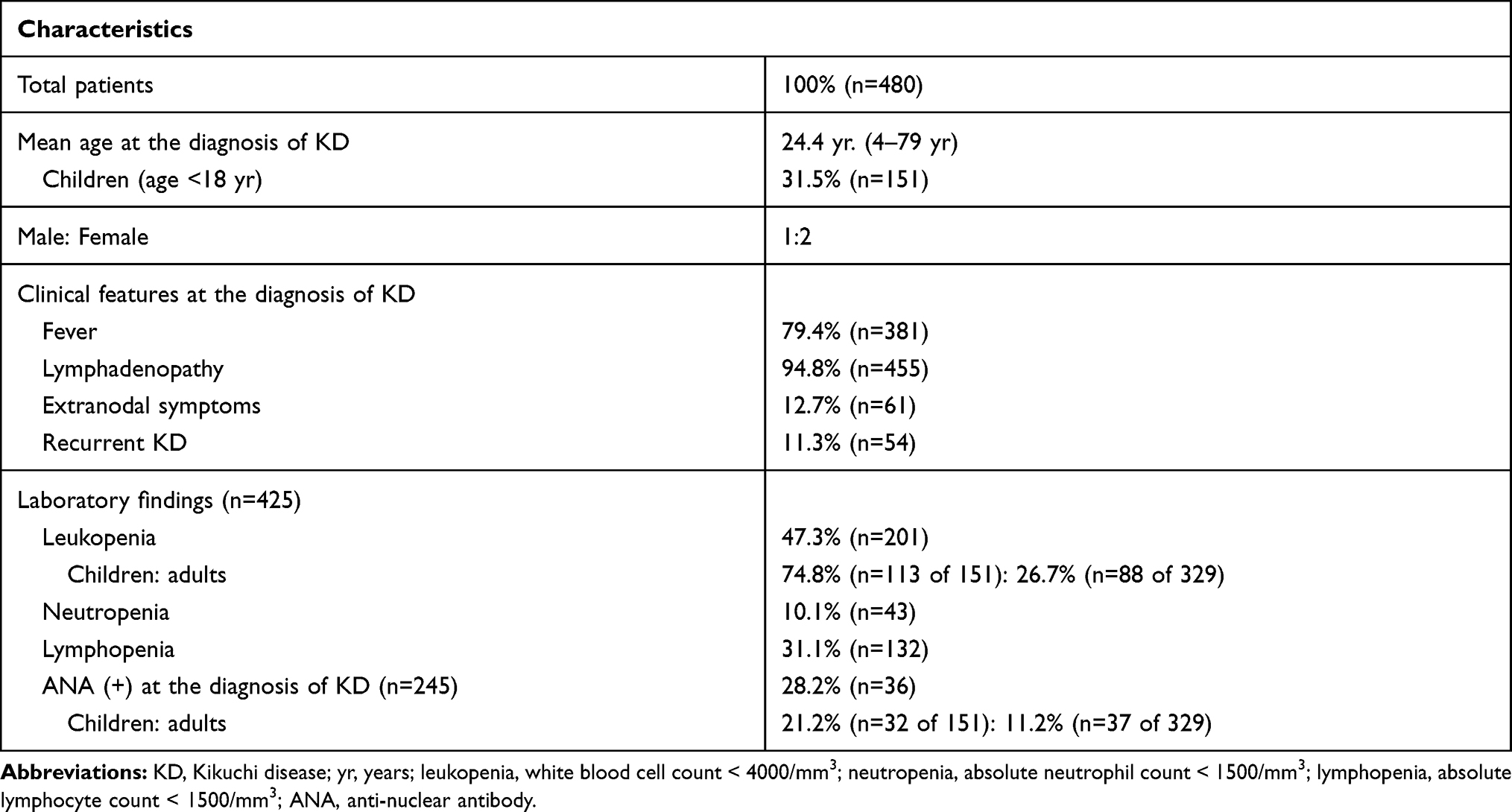 |
Table 1 General Characteristics of Patients with Kikuchi Disease |
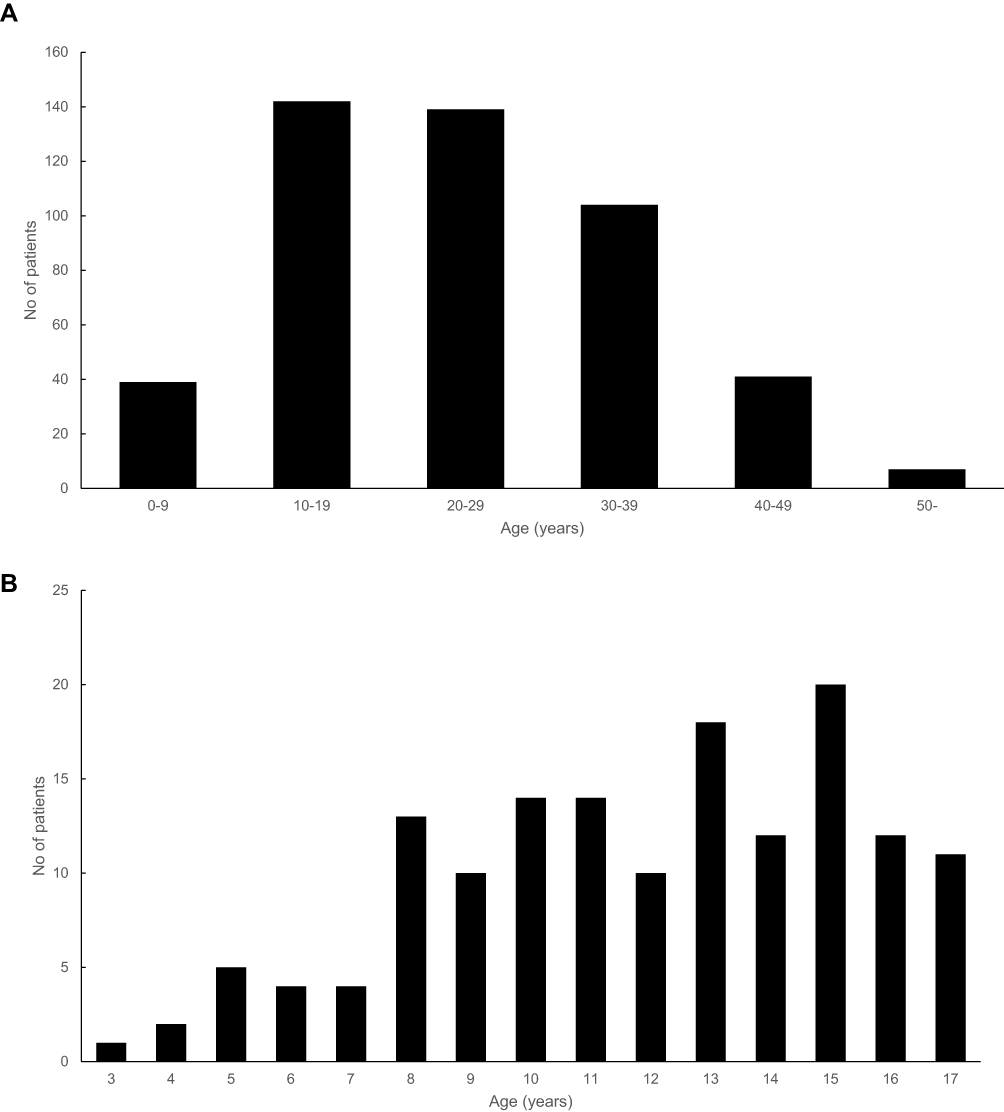 |
Figure 1 Age distribution of Kikuchi disease among (A) all patients and (B) children under 18 years of age. |
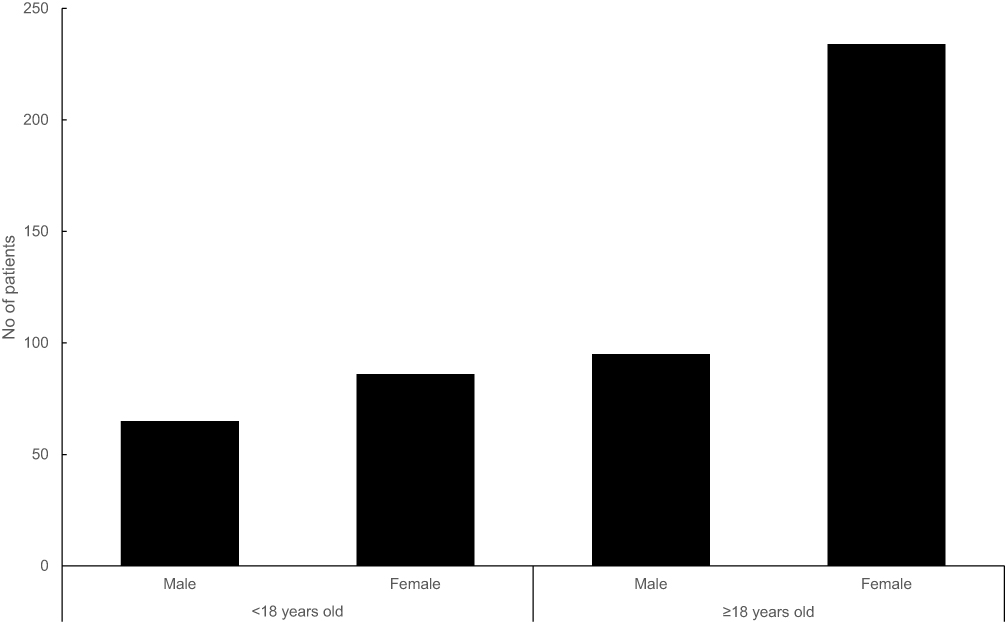 |
Figure 2 The ratio of male patients to female patients with Kikuchi disease. |
Clinical Characteristics of Patients with Recurrent Kikuchi Disease
Fifty-four patients (11.3%) experienced 1–4 recurrent episodes of KD each. The initial recurrence occurred within a mean duration of 6 months (range: 1 month to 6 years). The mean age at the first pathological diagnosis in patients with recurrent KD was 28.5 years (range 8–67 years), and 20 patients (37.0% of 54) were under 18 years of age. The ratio of male patients to female patients was 1:1.57. Table 2 shows the characteristics of patients with recurrent and non-recurrent KD. Of the 54 patients with recurrent KD, 53 (98.1%) patients had lymphadenopathy; 44 (81.5%) had fever; and 18 (33.3%) had extranodal symptoms such as skin rash, myalgia, and headache. Twenty-five patients (46.3%) had leukopenia, 25 (46.3%) had lymphopenia, and 6 (11.1%) had neutropenia. Of the 45 patients with recurrent KD tested for ANAs, 17 (37.8%) tested positive; of these, 8 (47.1%) patients were younger than 18 years of age. In terms of recovery from cytopenia, the mean duration for achieving a normal neutrophil count was 7.1 days (range: 0–10 days) in recurrent cases and 8.4 days (0–32 days) in non-recurrent cases. For recovery from lymphopenia, the mean duration was 14.7 days (range: 0–58 days) in recurrent cases and 6.2 days (range: 0–14 days) in non-recurrent cases. There were no significant differences between recurrent and non-recurrent cases with respect to fever, lymphadenopathy, and ANA positivity. Patients with recurrent KD were more likely to have extranodal symptoms (p=0.000) and lymphopenia (p=0.032) and to require a longer time to achieve a normal lymphocyte count (p=0.002).
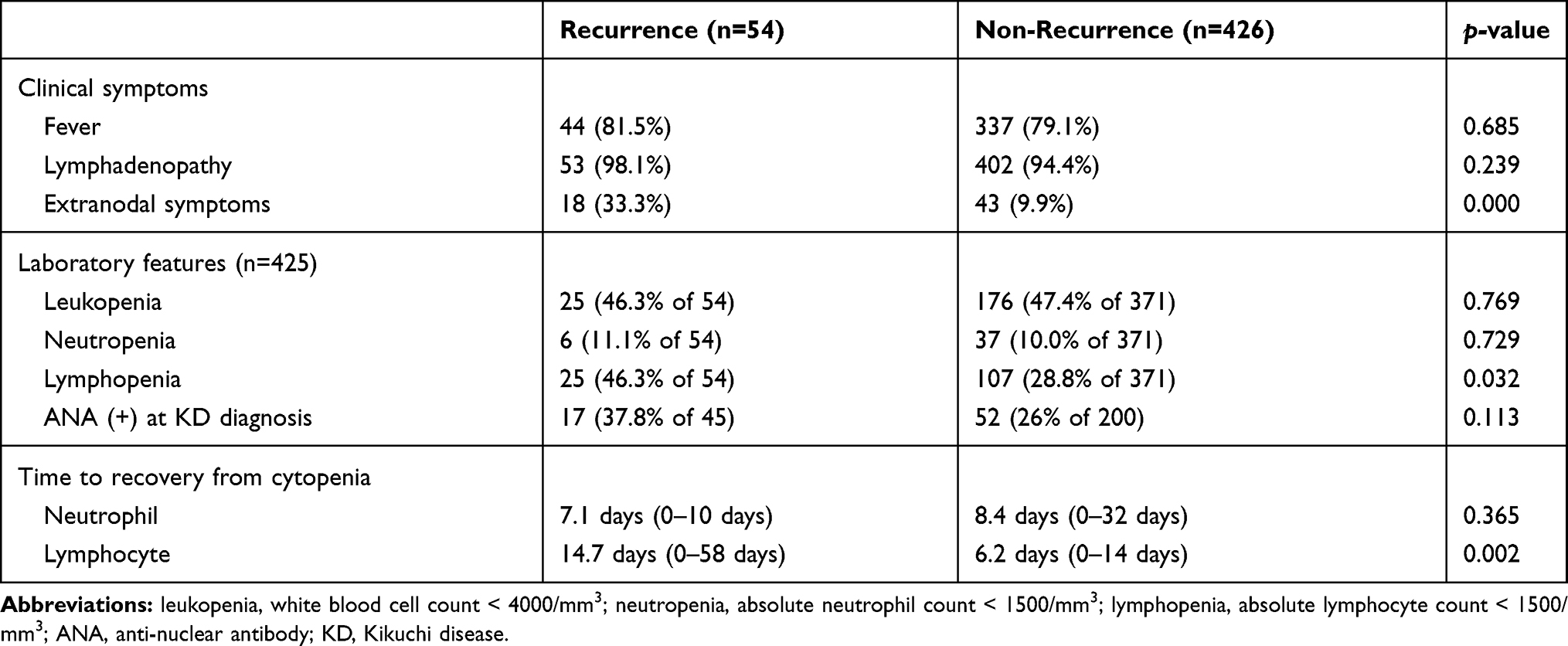 |
Table 2 Clinical Characteristics of Patients with Kikuchi Disease According to Recurrence |
Clinical Characteristics of Kikuchi Disease Patients Who Developed Systemic Autoimmune Diseases
Systemic autoimmune diseases occurred in 13 (2.7% of 480) patients diagnosed with KD during the study period (Table 3). There were 10 patients with SLE, 1 with Sjögren’s syndrome, 1 with rheumatoid arthritis, and 1 with adult-onset Still’s disease. The interval between KD diagnosis and the development of systemic autoimmune diseases ranged from 1 month to 5 years. The mean age at KD diagnosis was 27.9 years (range: 8–67 years). The ratio of male patients to female patients was 1:6. Of these 13 patients, 5 (38.5%) had recurrent KD, and 8 (61.5%) showed ANA positivity at KD diagnosis. All patients in this group had lymphadenopathy, 12 (92.3%) had fever, and 4 (30.8%) had extranodal symptoms including rash, myalgia, fatigue, and abdominal pain. Except for ANA positivity, no other laboratory parameters differed significantly between the patients in this group and those who did not develop systemic autoimmune diseases.
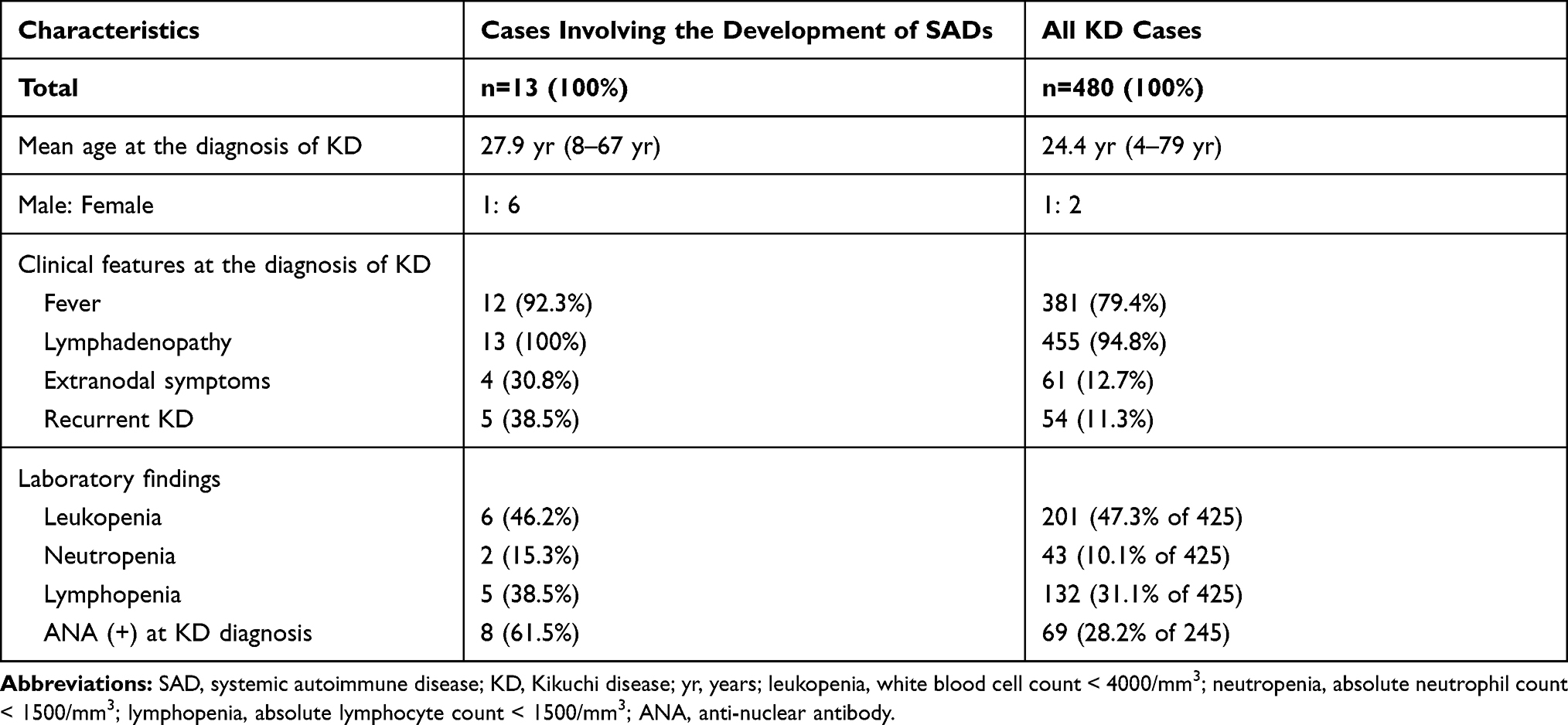 |
Table 3 Manifestations of Kikuchi Disease in Patients Who Developed Systemic Autoimmune Diseases |
Discussion
KD usually affects young women but can occur in any age group.2,5–7 The higher incidence among young women is reflected in the male: female ratio of 1:3–4 in adults; however, this ratio of approximately 1:1 in children.1–3,10,12,21 In our study, the mean age at KD diagnosis was 24.4 years, and 88.3% of the patients were younger than 40 years of age (Figure 1A). Interestingly, KD incidence increased significantly after 8 years of age in children (Figure 1B). The sex distribution of KD varies markedly with age. The proportions of male and female patients with KD are similar at a young age (1:1.32), but the proportion of affected female patients increases rapidly with age (1:2.46) (Figure 2). This study shows that KD occurs mainly in women of childbearing age but can occur in both men and women of all ages. Lymphadenopathy and fever were the predominant symptoms of KD in this study, similar to those in previously reported studies.2,3 WBC counts in patients with KD have been reported to vary across studies. Leukopenia has been reported in many studies1,11,12,22 and was found in 47.3% of our patients. An interesting finding in this study was that children with KD (age <18 years) were more likely to have leukopenia (74.8% vs 26.7%) and ANA positivity (21.2% vs 11.2%) than adults with KD (Table 1).
The rate of KD recurrence has been reported to be between 3% and 40%, and KD recurrence has been reported to occur more frequently in children.1,11,21,22 In our study, the KD recurrence rate was 11.3% in all patients and 13.2% in children under 18 years of age; this value was not significantly different from that in adults. More extranodal symptoms, lymphopenia, and a longer duration for lymphocyte count recovery were significantly associated with KD recurrence (Table 2). Several previous studies have reported the relation between WBC counts and KD recurrence,9,11 but the time to recovery from cytopenia had not been previously compared between recurrence and non-recurrence groups. In this study, the time to recovery from lymphopenia and lymphocyte counts were evaluated for their association with KD recurrence. KD is mostly self-limiting, but some studies have reported that steroids or hydroxychloroquine may be helpful in shortening the clinical course or reducing the severity of disease, especially in recurrent or severe cases.23–26 Since these studies were mostly case reports, further prospective research is needed to define the role of steroids or hydroxychloroquine in the treatment of KD.
Many studies have described the association of KD with autoimmune conditions such as SLE based on immunological and clinicopathological findings.15–20 Thirteen (2.7% of all patients) patients developed systemic autoimmune diseases after KD during the observation period in this study. The most common type of autoimmune condition was SLE (10 patients). One patient developed Sjögren’s syndrome, one developed rheumatoid arthritis, and one developed adult-onset Still’s disease. There was no difference in the mean age at the initial diagnosis of KD between all patients and those who developed systemic autoimmune diseases. However, the incidence rate of progression to autoimmune diseases after KD diagnosis was significantly higher in female patients with KD (Table 3). Patients showing progression to autoimmune diseases were more likely to have fever (92% vs 79.4%), common extranodal symptoms (30.8% vs 12.7%), a higher recurrence rate (38.5% vs 11.3%), and a higher ANA positivity rate at KD diagnosis (61.5% vs 28.2%) than all patients with KD. However, the group of patients who developed systemic autoimmune diseases after KD diagnosis was too small to yield statistically significant results. Despite this limitation, this study suggests potential predictive risk factors of progression to systemic autoimmune disease after KD diagnosis.
Another limitation of this study was that it was performed at a single center. However, electronic medical records were available for most clinical and laboratory findings of the patients. Further, a strength of this study is the consistent observation of a large number of patients over a long study period.
Conclusion
KD is generally a self-limiting disease; however, some patients have a more severe clinical course, such as recurrence or progression to systemic autoimmune diseases. Patients with extranodal symptoms, prolonged lymphopenia, KD recurrence, or ANA positivity benefit from early diagnosis and proper management of disease progression.
Acknowledgments
This work was supported by the new faculty research fund of Ajou University School of Medicine. We would like to thank Editage for English language editing.
Disclosure
The authors report no conflicts of interest related to this work.
References
1. Perry AM, Choi SM. Kikuchi-Fujimoto disease: a review. Arch Pathol Lab Med. 2018;142(11):1341–1346. doi:10.5858/arpa.2018-0219-RA
2. Bosch X, Guilabert A, Miquel R, Campo E. Enigmatic Kikuchi-Fujimoto disease: a comprehensive review. Am J Clin Pathol. 2004;122(1):141–152. doi:10.1309/YF081L4TKYWVYVPQ
3. Pepe F, Disma S, Teodoro C, Pepe P, Magro G. Kikuchi-Fujimoto disease: a clinicopathologic update. Pathologica. 2016;108(3):120–129.
4. Lee KY, Yeon YH, Lee BC. Kikuchi-Fujimoto disease with prolonged fever in children. Pediatrics. 2004;114(6):e752–756. doi:10.1542/peds.2004-0485
5. Dalton J, Shaw R, Democratis J. Kikuchi-Fujimoto disease. Lancet. 2014;383(9922):1098. doi:10.1016/S0140-6736(14)60262-2
6. Kucukardali Y, Solmazgul E, Kunter E, Oncul O, Yildirim S, Kaplan M. Kikuchi-Fujimoto Disease: analysis of 244 cases. Clin Rheumatol. 2007;26(1):50–54. doi:10.1007/s10067-006-0230-5
7. Lin HC, Su CY, Huang CC, Hwang CF, Chien CY. Kikuchi’s disease: a review and analysis of 61 cases. Otolaryngol Head Neck Surg. 2003;128(5):650–653. doi:10.1016/S0194-5998(02)23291-X
8. Jung IY, Ann HW, Kim JJ, et al. The incidence and clinical characteristics by gender differences in patients with Kikuchi-Fujimoto disease. Medicine (Baltimore). 2017;96(11):e6332. doi:10.1097/MD.0000000000006332
9. Song JY, Lee J, Park DW, et al. Clinical outcome and predictive factors of recurrence among patients with Kikuchi’s disease. Int J Infect Dis. 2009;13(3):322–326. doi:10.1016/j.ijid.2008.06.022
10. Seo JH, Shim HS, Park JJ, et al. A clinical study of histiocytic necrotizing lymphadenitis (Kikuchi’s disease) in children. Int J Pediatr Otorhinolaryngol. 2008;72(11):1637–1642. doi:10.1016/j.ijporl.2008.07.019
11. Yoo IH, Na H, Bae EY, et al. Recurrent lymphadenopathy in children with Kikuchi-Fujimoto disease. Eur J Pediatr. 2014;173(9):1193–1199. doi:10.1007/s00431-014-2306-6
12. Selvanathan SN, Suhumaran S, Sahu VK, Chong CY, Tan NWH, Thoon KC. Kikuchi-Fujimoto disease in children. J Paediatr Child Health. 2020;56(3):389–393. doi:10.1111/jpc.14628
13. Chen JS, Chang KC, Cheng CN, Tsai WH, Su IJ. Childhood hemophagocytic syndrome associated with Kikuchi’s disease. Haematologica. 2000;85(9):998–1000.
14. Lin YW, Horiuchi H, Ueda I, Nambu M. Recurrent hemophagocytic lymphohistiocytosis accompanied by Kikuchi’s disease. Leuk Lymphoma. 2007;48(12):2447–2451. doi:10.1080/10428190701644322
15. Cheng CY, Sheng WH, Lo YC, Chung CS, Chen YC, Chang SC. Clinical presentations, laboratory results and outcomes of patients with Kikuchi’s disease: emphasis on the association between recurrent Kikuchi’s disease and autoimmune diseases. J Microbiol Immunol Infect. 2010;43(5):366–371. doi:10.1016/S1684-1182(10)60058-8
16. Baenas DF, Diehl FA, Haye Salinas MJ, Riva V, Diller A, Lemos PA. Kikuchi-Fujimoto disease and systemic lupus erythematosus. Int Med Case Rep J. 2016;9:163–167. doi:10.2147/IMCRJ.S106396
17. Chen YH, Lan JL. Kikuchi disease in systemic lupus erythematosus: clinical features and literature review. J Microbiol Immunol Infect. 1998;31(3):187–192.
18. Papaioannou G, Speletas M, Kaloutsi V, Pavlitou-Tsiontsi A. Histiocytic necrotizing lymphadenitis (Kikuchi-Fujimoto disease) associated with antiphospholipid syndrome: case report and literature review. Ann Hematol. 2002;81(12):732–735. doi:10.1007/s00277-002-0562-4
19. Al-Allaf AW, Yahia YM. Kikuchi-Fujimoto disease associated with Sjogren’s syndrome: a case report. Eur J Case Rep Intern Med. 2018;5(5):000856.
20. Sondermann W, Hillen U, Reis AC, Schimming T, Schilling B. [Kikuchi-Fujimoto’s disease and adult-onset still’s disease. A rare co-occurence]. Hautarzt. 2015;66(12):940–943. doi:10.1007/s00105-015-3652-7. German.
21. Wang TJ, Yang YH, Lin YT, Chiang BL. Kikuchi-Fujimoto disease in children: clinical features and disease course. J Microbiol Immunol Infect. 2004;37(4):219–224.
22. Kang HM, Kim JY, Choi EH, Lee HJ, Yun KW, Lee H. Clinical characteristics of severe histiocytic necrotizing lymphadenitis (Kikuchi-Fujimoto disease) in children. J Pediatr. 2016;171:208–212 e201. doi:10.1016/j.jpeds.2015.12.064
23. Gerwig U, Weidmann RG, Lindner G. Relapsing Kikuchi-Fujimoto disease requiring prolonged steroid therapy. Case Rep Emerg Med. 2019;2019:6405687.
24. Wong YK, Khan M. Kikuchi-Fujimoto disease: a rare cause of cervical lymphadenopathy and fever. BMJ Case Rep. 2018;2018.
25. Honda F, Tsuboi H, Toko H, et al. Recurrent Kikuchi-Fujimoto disease successfully treated by the concomitant use of hydroxychloroquine and corticosteroids. Intern Med. 2017;56(24):3373–3377. doi:10.2169/internalmedicine.9205-17
26. Lin YC, Huang HH, Nong BR, et al. Pediatric Kikuchi-Fujimoto disease: a clinicopathologic study and the therapeutic effects of hydroxychloroquine. J Microbiol Immunol Infect. 2019;52(3):395–401. doi:10.1016/j.jmii.2017.08.023
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.