")
Back to Journals » Infection and Drug Resistance » Volume 13
Rifampicin-Resistant Multidrug-Resistant Tuberculosis Cases in Selected Hospitals in Western Oromia, Ethiopia: Cross-Sectional Retrospective Study
Authors Zewdie O, Dabsu R , Kifle E , Befikadu D
Received 4 August 2020
Accepted for publication 8 October 2020
Published 20 October 2020 Volume 2020:13 Pages 3699—3705
DOI https://doi.org/10.2147/IDR.S274589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Olifan Zewdie,1 Regea Dabsu,2 Edosa Kifle,2 Dachasa Befikadu3
1Department of Medical Laboratory Science, College of Medicine and Health Science, Ambo University, Ambo, Ethiopia; 2Department of Medical Laboratory Sciences, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia; 3Department of Medical Laboratory Science, College of Medicine and Health Science, Dambi Dollo University, Dambi Dollo, Ethiopia
Correspondence: Edosa Kifle
Department of Medical Laboratory Sciences, Institute of Health Sciences, Wollega University, P.O. Box: 395, Nekemte, Ethiopia
Tel +251576608212
Fax +251576617980
Email [email protected]
Purpose: With the recommendation of World Health Organization (WHO) and as per the Ethiopian National Implementation Guideline, GeneXpert is used for rapid diagnosis of rifampicin (RIF)-resistant multidrug-resistant tuberculosis (MDR-TB) from the suspected TB patients; however, there were limited findings in Ethiopia particularly in the study area showing the magnitude of RIF-resistant MDR-TB and related factors among suspected TB cases. Hence, we aimed to assess resistance to RIF as a biomarker for the detection of MDR-TB cases from the suspected TB patients in selected hospitals, Western Oromia, Ethiopia.
Patients and Methods: We have conducted a cross-sectional review on 2300 registered GeneXpert data as clinically suspected TB cases in three governmental hospitals, Western Oromia, Ethiopia, between October 2015 and April 2016 to assess resistance to RIF as a biomarker for the detection of MDR-TB cases. Trained data collectors enumerated the data using pre-tested semi-structured questionnaires from the Gene Xpert records found in the registration logbook available at each hospital laboratories. Following checking the data for completeness, we have cleaned and entered our data into SPSS version 20 to compute different analyses. P-value of ≤ 0.05 was taken as statistically significant.
Results: A total of 2300 TB suspected cases were included in the study. The overall prevalence of TB diagnosed by the GeneXpert assay was 21.3% (491/2300). In all TB confirmed cases, RIF-resistant TB accounted for 25.9% (127/491) which expressed rpoB gene mutations. Sex (being male), age (within 16– 30 age group), patient category (relapse, loss to follow-up, treatment failure and had MDR-TB contact) were significantly associated with rifampicin-resistant TB. Relapse patient was 20 times more likely to develop MDR-TB when compared to the new patient (P-value= 0.01, COR = 20.0, 95%C.I = 17.5– 42.5).
Conclusion: The rifampicin-resistant TB is prevalent in all age groups. The strong association and high prevalence of RIF-resistant TB to failure after treatment in this study require more attention towards improving the treatment to minimize evolving of the MDR-TB cases.
Keywords: GeneXpert, M. tuberculosis, RIF-resistant MDR-TB, Oromia, Ethiopia
Introduction
Tuberculosis (TB) remains a major public health problem in causing mortality and morbidity.1 The emergence of drug-resistant isolates/strains has become an area of concern among scientists since it is too difficult to manage and control the disease. Since rifampicin resistance is an important indicator of multidrug-resistant TB detection, they help to know the magnitude of the problem and early management of multidrug-resistant TB.2 GeneXpert MTB/RIF assay (Cepheid, Sunnyvale, CA, USA) is a real-time polymerase chain reaction (RT-PCR) that detects Mycobacterium tuberculosis as well as mutations that confer resistance to RIF in <2 hours.1
Extensive studies on the rpoB gene in rifampicin-resistant M. tuberculosis identified a variety of mutations and short deletion in the gene. More than 95% of the mutations are located in an 81 bp (1294–1375 bp) core region, Rifampicin Resistance Determining Region (RRDR) of the rpoB gene between codons 507–533 with the most common changes in codonsSe531Leu, His526Tyr, and Asp516Val. These changes occur in more than 70% of rifampicin-resistant isolate.3–6 The control of such drug-resistant disease is more difficult especially in endemic settings like Ethiopia due to having sub-standard laboratory services and lack of culture-based drug susceptibility testing at catchment areas, such a delay that results in an adverse effect.
Therefore, the implementation of molecular methods like GeneXpert assay for rapid detection of drug-resistant MDR-TB serves as an alternative to culture-based drug susceptibility testing (DST) as per the WHO recommendation in low-income countries like Ethiopia.3 Studies conducted in different geographical locations indicated that the burden of MDR-TB and the mutations responsible for drug resistance vary from country to country and region to region.7
However, there is a scarcity of information concerning the magnitude of MDR-TB cases in the study area, western Oromia. Hence, to fill this gap, we have assessed all of the records of Gene Xpert results between November 2015 and April 2016 to know the magnitude of MDR-TB cases and rifampicin resistance in three hospitals, Western Oromia, Ethiopia.
Patients and Methods
Study Design, Area and Period
A facility-based retrospective cross-sectional study was conducted between November 2015 and April 2016 to assess resistance to RIF as a biomarker for the detection of MDR-TB cases in three general hospitals, namely Nedjo, Gimbi, and Nekemte hospitals, Western Oromia, Ethiopia. These hospitals are governmental hospitals in the west part of Ethiopia, which are 500, 430, and 318 km, respectively, far away from the capital city, Addis Ababa. Besides this, these hospitals were too busy among the hospitals in western Ethiopia in providing referral services including TB diagnosis and treatment.
Study Population and Eligibility Criteria
All TB suspected (patients with clinical signs and symptoms suggestive of tuberculosis) who visited the study area during the study period were the study population. TB suspected patients who have submitted a sputum sample for GeneXpert analysis; whose variables like sex, age, HIV status, and Xpert MTB/RIF results have registered in the laboratory registration book were included in the study whereas, patients who had incomplete data of the mentioned above were excluded from the study.
Sampling Technique and Data Collection
Data were retrieved consecutively from the laboratory registration book of Gene Xpert result during the study period using the data extraction sheet.
Gene Xpert Assay Procedure
As per the standard operating procedure, the GeneXpert assay was performed on sputum specimens to detect MDR-TB cases.8 Sputum samples are treated with sample reagent (SR) containing NaOH and isopropanol. The SR is added using a 2 to 1 ratio of the sputum sample, homogenized and incubated for 15 min at room temperature. The treated sample was then transferred into the GeneXpert cartridge and inserted into the real-time polymerase chain reaction (RT-PCR) machine for DNA extraction and amplification of 192 bp segments of the rpoB gene.8
Ethical Clearance
Ethical approval and clearance were received from the research and ethics review committee (RERC) of Wollega University, Institute of Health Science. A letter of request was officially written to the respective hospital administrator office to facilitate the data collection process. The data were not disclosed to the third body for confidentiality issues during and after data collection.
Data Analysis
Following checking the completeness of the data, we have entered and analyzed our secondary data into SPSS version 20 to see the association between dependent and outcome variables using OR with 95% confidence interval (C.I) and P-value ≤0.05 indicating statistical significance.
Results
Out of 2300 registered Gene Xpert result of RIF-resistant TB suspected cases, 1159 (50.4%) were males and the rest were females. The detection rate of GeneXpert for M. tuberculosis was 21.3% (491/2300) and from the positive TB cases, 25.9% (127/491) showed RIF-resistance by GeneXpert assay. From the MDR-TB identified, 15.7% and 42.5% were new and failed after completed the treatment, respectively (Table 1).
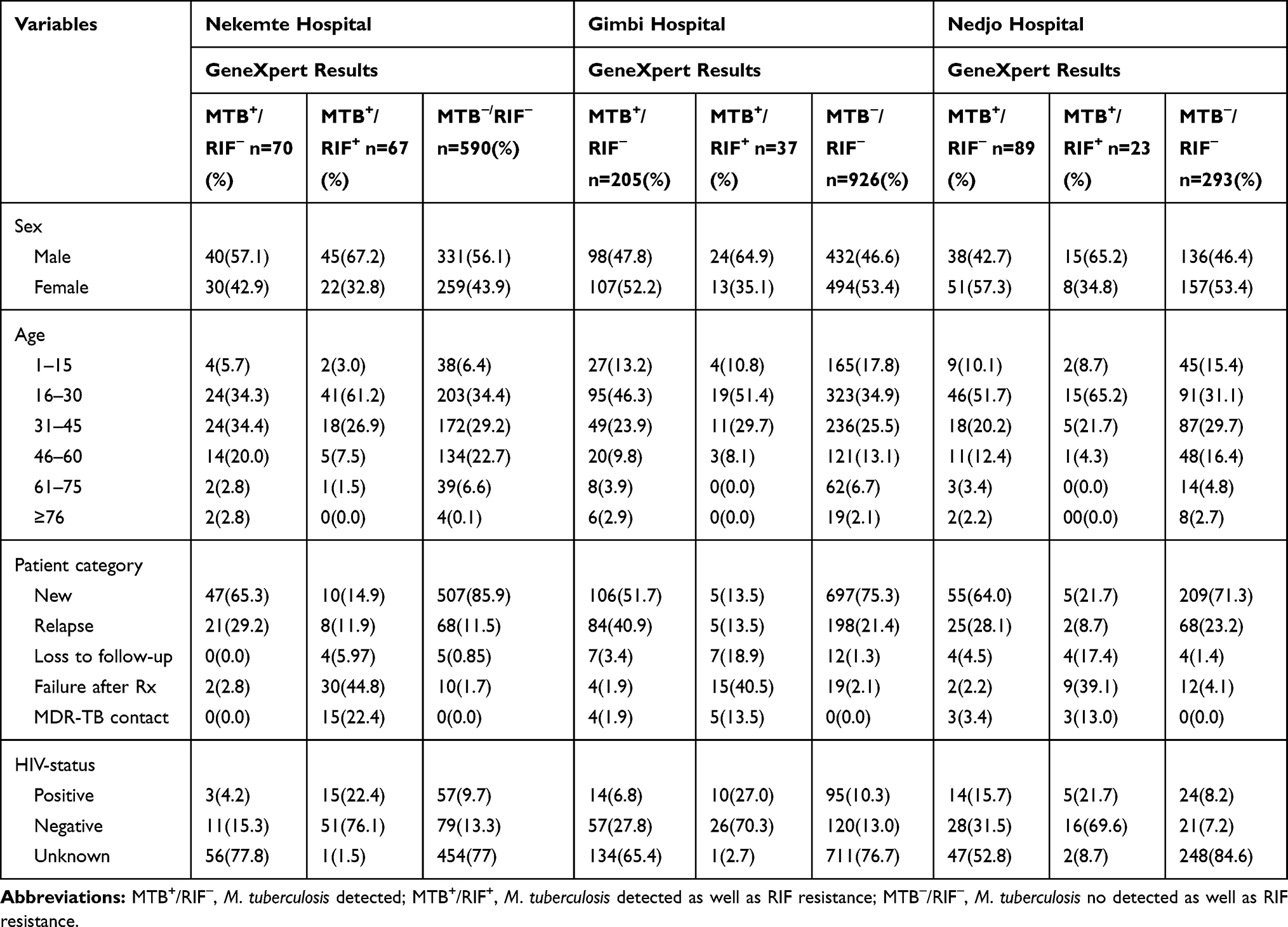 |
Table 1 Distribution of Selected Socio-Demographic Characteristics and Their HIV-Status in Relation to GeneXpert Results Among MDR-TB Suspected Patients in Three Hospitals, West Oromia, Ethiopia, 2016 (n=2300) |
MTB+/RIF+ detection by GeneXpert technique was 2 times more likely to be positive in males when compared to females [COR, 95% CI 2.01 (1.0, 2.9), P= 0.01] and showed statistically significant association in the age group of 16–30 (P-value = 0.001). MTB+/RIF−detection by molecular technique did not vary with the sex of the patients (P-value = 0.2). But it was statistically associated with the age group of 16–30 (P-value =0.01) (Table 2).
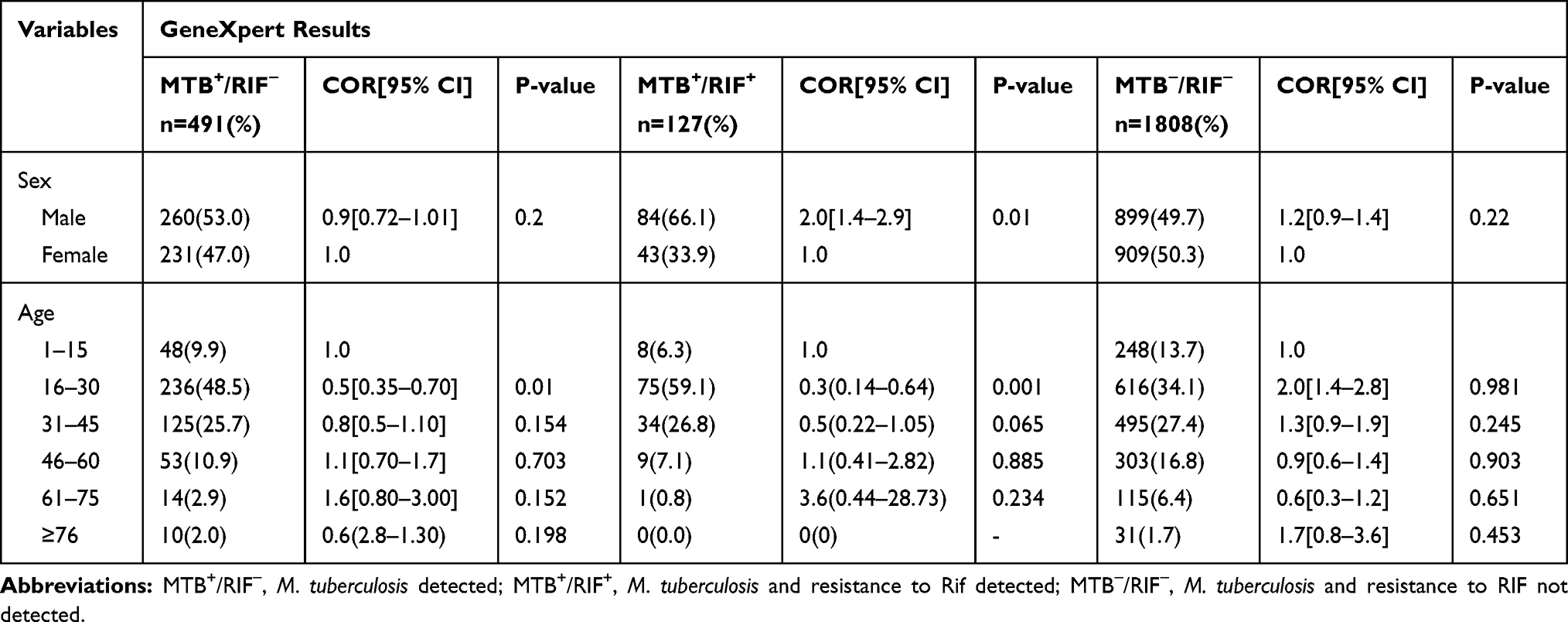 |
Table 2 Diagnostic Characteristics of Study Population by Sex and Age in Three Hospitals, 2016 |
Mycobacterium tuberculosis diagnosis by the GeneXpert was statistically associated with the different patient categories when it was compared with a new patient (P-value ≤0.01). Relapse patient was 20 times more likely to develop MDR-TB by Gene Xpert MTB/RIF-resistance when compared to new patient (P-value ≤0.01, OR = 20.0, 95% CI = 17.5–42.5). Moreover, loss to follow-up and failure after treatment were statistically significant on MDR-TB diagnosed by GeneXpert/RIF-resistance (P-value ≤0.01) (Table 3).
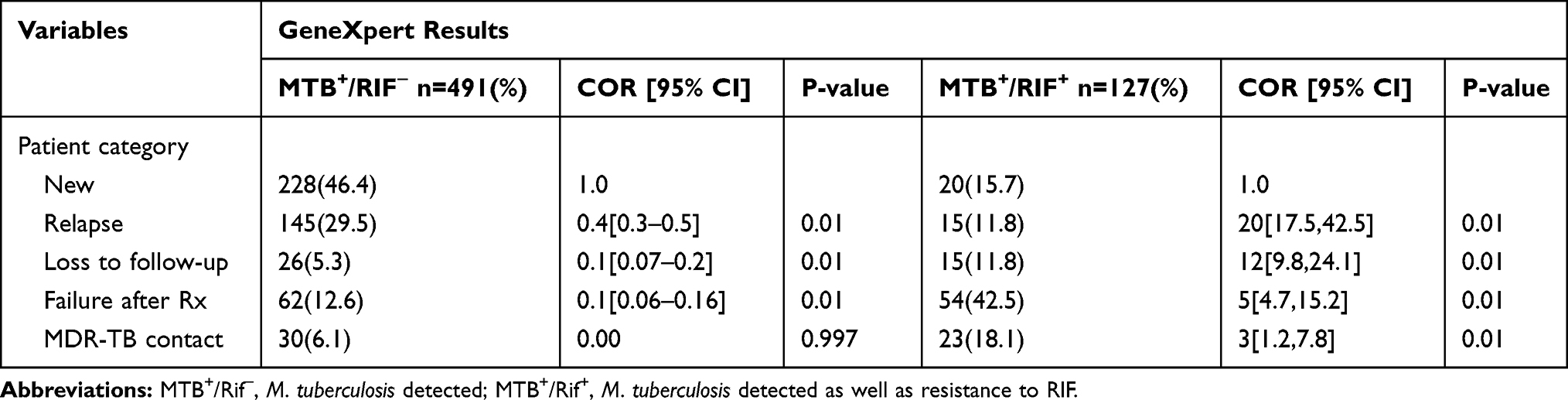 |
Table 3 GeneXpert MTB/RIF Assay in Different Patient Category in Three Hospitals, 2016 |
Discussion
The emergence of the drug-resistance poses a serious threat to global TB control. The rapid detection and identification of drug-resistant Mycobacterium tuberculosis is a challenge in Ethiopia due to limited laboratory facilities and the absence of molecular techniques. This might have indications of incorrect patient management, abusing the use of anti-TB drugs, and finally leading to emerging of drug-resistance strains.9,10 Therefore, this molecular identification using the GeneXpert technique offers an opportunity for early detection and timely management of MDR-TB cases in endemic areas.11–13 Our report indicated that the prevalence of M. tuberculosis diagnosed by GeneXpert was 21.3% (491/2300). From these, the prevalence of RIF-resistant MDR-TB cases detected using GeneXpert was 25.8% (127/491). Our finding was comparable with previous reports from similar findings reported in Ethiopia and elsewhere in the world (19.4–45.3%).14–16 But it was higher than similar findings reported in Southern, Northern Eastern, and Northwest part of Ethiopia with the prevalence of 3.4%, 2.5%, and 1.7%, and 9.317–20 respectively. This difference might be attributed to unorganized patient diagnosis, treatment, and follow-up that may contribute to the higher prevalence of rifampicin resistance in the study area. Besides this, variation in the design of the study, study population, sample-related factors, access to health care facilities, geography, and effectiveness of TB control program might be possible reasons for the differences in GeneXpert test results.
Worldwide, the proportion of new cases with MDR-TB is 3.5% higher among people previously treated for TB, at 20.5% in 2013.21 In the present study, of the total resistance cases, 15.7% (20/127) was new patients and 42.5% (54/127) in the failure after treatment cases. The Rif resistance among new and TB treatment failure was high when it was compared with word wide. The high level of drug resistance among new cases in this study might be due to the exposure of patients to anti-TB drugs before they visited health institutions or exposure to drug-resistant M. tuberculosis strain in the community. According to the different sources, the association between TB treatment failure and MDR-TB might be related to unsatisfactory compliance by patients, lack of supervision of treatment, improper drug regimens, and inadequate or irregular drug supply that may potentiate drug resistance.22–26 Also, this may indicate that whether the patients are not strictly following the Directly Observed Therapy; a short course (DOTS) program or the gene of the bacteria may mutate and form resistance to the first lines of anti-TB drugs. Relapse patient was 20 times more likely to develop MDR-TB by GeneXpert MTB/RIF when compared to new patient [P-value ≤0.01, OR = 20.0, 95% CI = 17.5–42.5]. The association between relapse and MDR-TB might be due to poor adherence to patients that may potentiate secondary drug resistance.
The increased incidence of MDR-TB cases affects its management and increases the motility rate in high burden countries like Ethiopia. Culture is a better diagnosis for tuberculosis although it consumes more resources like time and human power.27 Thus, the implementation of molecular methods like GeneXpert for the rapid detection of drug-resistant mycobacterium species is crucial. Recently, WHO and the Ethiopian National Implementation Guideline for GeneXpert strongly recommend the use of GeneXpert for the initial diagnosis of individuals suspected of MDR-TB for rapid screening of MDR-TB.28–30 Moreover, the identification of tubercle bacilli by culture is required for the ultimate proof of Mycobacterial infection. However, due to the unavailability of laboratory equipment and safety procedures, the method is not practiced in resource-poor settings.31,32
Molecular methods in the specific target like GeneXpert employed for rapid identification of mycobacteria from clinical specimens.33 This indicated that the result obtained from a rapid molecular method like the GeneXpert test in our present study has contributed to early management of TB patients, which avoids adverse drug reaction, incorrect use of TB treatments and emerging of drug-resistant strains. In addition to this, the GeneXpert assay helps for early detection of TB cases and prompt treatment that ensures better treatment outcomes and reduced TB transmission to contacts.34
Limitation of the Study
Here are limitations that include the use of the small-scale sampling and retrospective study design to assess RIF-resistant MDR-TB infection status, which may have probably underestimated the finding. We also lacked doing culturing to identify isolates.
Conclusion
Our study indicated the high prevalence of rifampicin-resistant TB was detected in the study area. Sex (being male), age (16–30 age group), patients who lost follow-up, failed treatment and on relapse were significantly associated with MDR-TB cases. Besides this, RT-PCR helps to diagnose both TB and RIF-resistant TB cases simultaneously.
Data Sharing Statement
The data and material set supporting the results of this article are included in the article. In case needed, it can be accessed upon formally requesting the corresponding author.
Ethical Consideration
Prior to conducting the study, we have received ethical approval and clearance from the research and ethics review committee (RERC) of Wollega University. Official letters to the respective hospitals were obtained from the Wollega University. The hospital administrative officers permitted us to collect data. Then after, the questionnaire was given to laboratory professionals based on the informed consent.
Acknowledgments
We would like to thank all the hospitals for granting permission and also the staffs at the study site for their cooperation in data collection.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Kant S, Maurya AK, Kushwaha RA, et al. Multi-drug resistant tuberculosis: an iatrogenic problem. Biosci Trends. 2010;4(2):48–55.
2. World Health Organization. New Technologies for TB Control: A Framework for Their Adoption, Introduction, and Implementation. Geneva: World Health Organization; 2007.
3. Ramaswamy S, Musser JM. Molecular genetic basis of antimicrobial agent resistance in Mycobacterium tuberculosis: 1998 update. Tuber Lung Dis. 1998;79(1):3–29. doi:10.1054/tuld.1998.0002
4. Herrera L, Jiménez S, Valverde A, et al. Molecular analysis of rifampicin-resistant Mycobacterium tuberculosis isolated in Spain (1996–2001). Description of new mutations in the rpoB gene and review of the literature. Int J Antimicrob Agents. 2003;21(5):403–408. doi:10.1016/S0924-8579(03)00036-0
5. Fan XY, Hu ZY, Xu FH, et al. Rapid detection of rpoB gene mutations in rifampin-resistant Mycobacterium tuberculosis isolates in Shanghai by using the amplification refractory mutation system. J Clin Microbiol. 2003;41(3):993–997. doi:10.1128/JCM.41.3.993–997.2003
6. Braunwald E, Fauci AS, Kasper DL, et al. Harrison’s Principles of Internal Medicine. McGraw Hill; 2001.
7. Purwar S, Chaudhari S, Katoch VM, et al. Determination of drug susceptibility patterns and genotypes of Mycobacterium tuberculosis isolates from Kanpur district, North India. Infect Genet Evol. 2011;11(2):469–475. doi:10.1016/j.meegid.2010.12.010
8. Cepheid. GeneXpert diagnosis system GeneXpert MTB/RIF assay manual AND operator manual software version-4. Cepheid. 2012. Available from: https://www.cepheid.com/Package%20Insert%20Files/Xpert-MTB-RIF-ENGLISH-Package-Insert-301-1404-Rev-F.pdf.
9. World Health Organization. Global Tuberculosis Control: A Short Update to the 2009 Report. Geneva: World Health Organization; 2009. Available from: https://apps.who.int/iris/handle/10665/44241.
10. Getahun H, Harrington M, O’Brien R, et al. Diagnosis of smear-negative pulmonary tuberculosis in people with HIV infection or AIDS in resource-constrained settings: informing urgent policy changes. Lancet. 2007;369(9578):2042–2049. doi:10.1016/S0140-6736(07)60284-0
11. Auld SC, Moore BK, Killam WP, et al. Rollout of Xpert® MTB/RIF in Northwest Cambodia for the diagnosis of tuberculosis among PLHA. Public Health Action. 2014;4(4):216–221. doi:10.5588/pha.14.0082
12. Van Kampen SC, Susanto NH, Simon S, et al. Effects of introducing Xpert MTB/RIF on diagnosis and treatment of drug-resistant tuberculosis patients in Indonesia: a pre-post intervention study. PLoS One. 2015;10(6):e0123536. doi:10.1371/journal.pone.0123536
13. Yadav RN, Singh BK, Sharma SK, et al. Correction: comparative evaluatiON of GenotypeMTBDRplus line probe assay with solid culture method in early diagnosis of Multidrug Resistant Tuberculosis (MDR-TB) at a Tertiary Care Centre in India. PLoS One. 2013;8(9):1–6. doi:10.1371/journal.pone.0072036
14. Geleta DA, Megerssa YC, Gudeta AN, et al. Xpert MTB/RIF assay for diagnosis of pulmonary tuberculosis in sputum specimens in remote health care facility. BMC Microbiol. 2015;15(1):220. doi:10.1186/s12866-015-0566-6
15. Iram S, Zeenat A, Hussain S, et al. Rapid diagnosis of tuberculosis using Xpert MTB/RIF assay-report from a developing country. Pak J Med Sci. 2015;31(1):105–110. doi:10.12669/pjms.311.6970
16. Muyoyeta M, Moyo M, Kasese N, et al. Implementation research to inform the use of Xpert MTB/RIF in primary health care facilities in high TB and HIV settings in resource constrained settings. PLoS One. 2015;10(6). doi:10.1371/journal.pone.0126376
17. Hordofa MW, Adela TB. Prevalence of rifampicin mono resistant Mycobacterium tuberculosis among suspected cases attending at Yirgalem hospital. Clin Med Res. 2015;4(3):75–78. doi:10.11648/j.cmr.20150403.13
18. Nigus DM, Lingerew W, Beyene B, et al. Prevalence of multi drug resistant tuberculosis among presumptive multi drug resistant tuberculosis cases in Amhara National Regional State, Ethiopia. J Mycobact Dis. 2014;4(152):2161. doi:10.4172/2161-1068.1000152
19. Seyoum B, Demissie M, Worku A, et al. Prevalence and drug resistance patterns of Mycobacterium tuberculosis among new smear positive pulmonary tuberculosis patients in eastern Ethiopia. Tuberc Res Treat. 2014;2014.
20. Derbie A, Worku S, Mekonnen D, et al. Xpert MTB/RIF assay for the diagnosis of Mycobacterium tuberculosis and its Rifampicin resistance at FelegeHiwot and Debre Tabor Hospitals, Northwest Ethiopia: a preliminary implementation research. Ethiop J Health Dev. 2016;30(2):60–66.
21. World Health Organization. World Health Organization Global Tuberculosis Report 2013. Geneva, Switzerland: World Health Organization. Available from: https://apps.who.int/iris/bitstream/handle/10665/91355/9789241564656_eng.pdf.
22. Zhang Y, Yew WW. Mechanisms of drug resistance in Mycobacterium tuberculosis [State of the art series. Drug-resistant tuberculosis. Edited by CY. Chiang. Number 1 in the series]. Int J Tuberc Lung Dis. 2009;13(11):1320–1330.
23. Torres M, Criado A, Gónzalez N, et al. Rifampin and isoniazid resistance associated mutations in Mycobacterium tuberculosis clinical isolates in Seville, Spain. Int J Tuberc Lung Dis. 2002;6(2):160–163.
24. Hillemann D, Kubica T, Rüsch-Gerdes S, et al. Disequilibrium in distribution of resistance mutations among Mycobacterium tuberculosis Beijing and non-Beijing strains isolated from patients in Germany. Antimicrob Agents Chemother. 2005;49(3):1229–1231. doi:10.1128/AAC.49.3.1229-1231.2005
25. Lee AS, Lim IH, Tang LL, et al. High frequency of mutations in the rpoB gene in rifampin-resistant clinical isolates of Mycobacterium tuberculosis from Singapore. J Clin Microbiol. 2005;43(4):2026–2027. doi:10.1128/JCM.43.4.2026-2027.2005
26. Barnard M, Albert H, Coetzee G, et al. Rapid molecular screening for multidrug-resistant tuberculosis in a high-volume public health laboratory in South Africa. Am J Respir Crit Care Med. 2008;177(7):787–792.
27. Ani AE. Advances in the laboratory diagnosis of Mycobacterium tuberculosis. Ann Afr Med. 2008;7(2):57–61. doi:10.4103/1596-3519.55680
28. Helb D, Jones M, Story E, et al. Rapid detection of Mycobacterium tuberculosis and rifampin resistance by use of on-demand, near-patient technology. J Clin Microbiol. 2010;48(1):229–237. doi:10.1128/JCM.01463-09
29. World Health Organization (WHO). Molecular Line Probe Assays for Rapid Screening of Patients at Risk of Multidrug Resistant Tuberculosis (MDR-TB): Policy Statement. Geneva: World Health Organization; 2008. Available from: https://www.who.int/tb/laboratory/line_probe_assays/en/.
30. World Health Organization. Automated Real-Time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB. No. WHO/HTM/TB/2013.16. World Health Organization; 2013. Available from: https://apps.who.int/iris/handle/10665/112472.
31. Huang J, Shen M, Sun Y. Epidemiological analysis of extrapulmonary tuberculosis in Shanghai. Zhonghua Jie He He Hu Xi Za Zhi. 2000;23(10):606–608.
32. Bass JB
33. Eisenach KD, Donald Cave M, Bates JH, et al. Polymerase chain reaction amplification of a repetitive DNA sequence specific for Mycobacterium tuberculosis. J Infect Dis. 1990;161(5):977–981. doi:10.1093/infdis/161.5.977
34. Federal Democratic Republic of Ethiopia Ministry of Health/Ethiopian Public Health Institute. Implementation Guideline for GeneXpert MTB/RIF Assay in Ethiopia. Addis Ababa; 2014. Available from: https://www.ephi.gov.et/images/pictures/Implementation%20Guideline%20for%20%20GeneXpert%20MTBRIF%20Assay%20in%20%20Ethiopia%20Nov%2003%202 ....pdf.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.