")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
Ribociclib in the Treatment of Hormone-Receptor Positive/HER2-Negative Advanced and Early Breast Cancer: Overview of Clinical Data and Patients Selection
Authors Parati MC, Pedersini R, Perego G , Reduzzi R, Savio T, Cabiddu M, Borgonovo K, Ghilardi M, Luciani A, Petrelli F
Received 1 March 2022
Accepted for publication 8 April 2022
Published 12 April 2022 Volume 2022:14 Pages 101—111
DOI https://doi.org/10.2147/BCTT.S341857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Maria Chiara Parati,1 Rebecca Pedersini,2 Gianluca Perego,3 Roberto Reduzzi,4 Tommaso Savio,4 Mary Cabiddu,1 Karen Borgonovo,1 Mara Ghilardi,1 Andrea Luciani,1 Fausto Petrelli1
1Oncology Unit, Medical Science Department, ASST Bergamo Ovest, Treviglio, BG, Italy; 2Breast Unit-Medical Oncology, ASST Spedali Civili, Brescia, Italy; 3Pharmacy Unit, IRCCS San Raffaele Hospital, Milan, Italy; 4Breast Unit, ASST Bergamo Ovest, Treviglio, BG, Italy
Correspondence: Fausto Petrelli, Oncology Unit, Medical Sciences Department, ASST Bergamo Ovest, Piazzale Ospedale 1, Treviglio, 24047, BG, Italy, Tel +390363424420, Fax +390363424380, Email [email protected]
Abstract: Among pre- and postmenopausal women with hormone receptor-positive (HR+) breast cancer (BC), combinations of an aromatase inhibitor (AI) or fulvestrant with a CDK 4/6 inhibitor (palbociclib, ribociclib, or abemaciclib) have demonstrated improved progression-free survival (PFS) and overall survival (OS) compared to standard single-agent hormone therapy alone as first-line therapy for de novo metastatic disease or relapse during or after adjuvant therapy and no previous therapies in an advanced setting. We here reviewed clinical data about ribociclib in advanced and early BC. Also, we shed light on patient selection and special settings in which medical oncologists urgently await an advance in treatment. Ribociclib was FDA-approved in combination with letrozole based on a Phase III study in which 668 postmenopausal women with HR+, HER2-negative recurrent or metastatic BC were treated with first-line letrozole with or without ribociclib. For patients with metastatic disease at presentation or after a course of AIs, the results of the MONALEESA-3 trial suggest ribociclib’s efficacy in combination with fulvestrant, and this combination is FDA-approved for initial- and subsequent-line endocrine therapy for postmenopausal women with metastatic hormone receptor-positive, HER2-negative BC. In adjuvant and neoadjuvant settings, the use of CDK 4/6 inhibitors may be useful to boost outcomes in high-risk patients with HR+ BC, but data contrast with those of a phase III study, which produced positive results. New combinations are being explored in upfront disease (neoadjuvant) or in association with other targeted agents in metastatic disease. Compared to other CDK 4/6 available, ribociclib has a higher incidence of liver function test abnormalities than the other agents and can cause QTc prolongation, and therefore may be prudently avoided in patients with cardiac morbidities or other risk factors for QTc prolongation (drugs, interactions). In these cases, different agents (palbociclib or abemaciclib) may be used. In conclusion, ribociclib with letrozole or with fulvestrant is effective for the entire spectrum of patients with HR+ BC in the advanced setting. Ribociclib has all the characteristics of an innovative drug able to change the clinical practice and most BC patients’ prognoses.
Keywords: breast cancer, ribociclib, CDK 4/6 inhibitors, review
Introduction
Among pre-and postmenopausal women with hormone receptor-positive (HR+) breast cancer (BC), combinations of an aromatase inhibitor (AI) and fulvestrant with a CDK 4/6 inhibitor (palbociclib, ribociclib [RIBO], or abemaciclib) have demonstrated improved progression-free survival (PFS) and overall survival (OS) compared to standard single-agent hormone therapy alone as first-line therapy for de novo metastatic disease or relapse during or after adjuvant therapy and no previous therapies in advanced setting. Despite only 1 Phase 3 trials with abemaciclib provided positive results in adjuvant setting, CDK 4/6 inhibitors have not been fully employed in early disease. Ribociclib was FDA-approved in combination with letrozole (LET) based on a phase III study in which 668 postmenopausal women with HR+, HER2-negative recurrent or metastatic BC were treated with first-line L with and without RIBO.1 For patients with metastatic disease at presentation or after a course of AIs, the results of the MONALEESA-32 trial suggest RIBO’s efficacy in combination with fulvestrant, and this combination is FDA-approved for initial- or subsequent-line endocrine therapy (ET) for postmenopausal women with metastatic HR+, HER2-negative BC. In adjuvant and neoadjuvant settings, CDK 4/6 inhibitors may be useful to boost outcomes in high-risk patients with HR+ BC, but data contrast with those from a phase III study, which produced positive results. New combinations are being explored in upfront disease (neoadjuvant) and in association with other targeted agents in metastatic disease. Ribociclib has all the characteristics of an innovative drug that can change the clinical practice and most BC patients’ prognosis. This review highlights patient selection and particular settings in which medical oncologists urgently await advances in treatment.
First-Line Therapy with RIBO in Advanced Disease
In the last few years, the clinical activity and safety of RIBO have been investigated in various settings through the MONALEESA (Mammary Oncology Assessment of LEE011ʹs Efficacy and Safety) clinical trial program, which includes the MONALEESA-2, MONALEESA-3, and MONALEESA-7 trials. The MONALEESA-2 trial is a phase III trial to evaluate the combination of RIBO with LET as first-line therapy in postmenopausal women with advanced BC; the MONALEESA-3 and MONALEESA-7 are more recent trials to investigate new patient populations and CDK 4/6 inhibitor combinations in first-line and second-line settings. The MONALEESA-7 is a phase III trial to study CDK 4/6 inhibition in combination with tamoxifen or a nonsteroidal aromatase inhibitor in a population composed entirely of pre/perimenopausal women, and in the MONALEESA-3 trial, researchers investigated CDK 4/6 inhibition plus fulvestrant in a mixed population (de novo, first-line and second-line treatment for advanced disease in postmenopausal patients).
Combination of RIBO + LET
The MONALEESA-2 and MONALEESA-7 are double-blind, placebo-controlled, randomized phase III trials. In all trials, the initial RIBO dose was 600 mg once daily for 21 days in a 28-day cycle (3 weeks on, 1 week off schedule). In the MONALEESA-2 trial, between January 2014 and March 2015, 668 patients were enrolled, 334 in each arm. The MONALEESA-7 trial included 672 patients between December 2014 and August 2016, with 335 assigned to the experimental arm and 337 in the control arm.
In the MONALEESA-2 trial, RIBO (or placebo) was combined with LET (2.5 mg once daily) in post-menopausal women with HR+/HER2 negative advanced BC.5 The primary endpoint was PFS, and the secondary endpoints were OS, overall response rate (ORR), clinical benefit rate, safety, and quality of life assessments.3
In the MONALEESA-7 trial, researchers evaluated pre/perimenopausal patients with HR+, HER2 negative advanced BC who received treatment with either RIBO, a placebo with tamoxifen (20 mg daily), or a nonsteroidal aromatase inhibitor (LET 2.5 mg daily or anastrozole 1 mg daily).4 In addition, all patients in the MONALEESA-7 trial received goserelin (3.6 mg subcutaneously on day 1 of every 28-day cycle) for ovarian suppression. In the MONALEESA-2 trial, patients never received systemic chemotherapy or ET for advanced disease. Patients with inflammatory BC, CNS metastases, impaired gastrointestinal function or history of cardiac disease or dysfunction, or baseline corrected QTc interval >450 ms were excluded. Previous neoadjuvant or adjuvant use of a nonsteroidal aromatase inhibitor was permitted contingent on a disease-free interval of more than 12 months. The MONALEESA-7 trial included pre/perimenopausal women aged 18–58 years, with similar patients enrolled in the MONALEESA-2 trial. The primary endpoint was PFS. The secondary endpoints included OS, ORR, clinical benefit rate, time to response, time to definitive deterioration of ECOG PS, quality of life, safety, and tolerability.4
In the MONALEESA-2 and MONALEESA-7 trials, the primary endpoint was met. PFS was significantly improved in the treatment arm containing RIBO vs the placebo arm. In the MONALEESA-2 trial, after a median follow-up of 36.4 months, the median PFS was 25.3 months in the RIBO arm vs 16 months in the placebo arm (hazard ratio [HR]: 0.568 [95% CI: 0.457–0.704]).
Results from the MONALEESA-7 trial also show a significantly longer duration of PFS in the RIBO group than in the placebo group; the median PFS was 23.8 months (95% CI: 19.2–not reached) in the RIBO arm and 13.0 months (95% CI: 11.0–16.4) in the placebo arm (HR: 0.55 [95% CI: 0.44–0.69]). The median PFS in the subgroup of patients receiving tamoxifen as a combination partner (n = 177) was 22.1 months (95% CI: 16.6–24.7 months) in the RIBO group and 11.0 months (95% CI: 9.1–16.4 months) in the placebo group (HR: 0.59 [95% CI: 0.39–0.88]). In patients receiving a nonsteroidal aromatase inhibitor as a combination partner (n = 495), the median PFS was 27.5 months (95% CI: 19.1 months–not reached) in the RIBO group and 13.8 months (95% CI: 12.6–17.4 months) in the placebo group (HR: 0.57[95% CI: 0.44–0.74]).2 The ORR in the MONALEESA-2 trial was 42.5% versus 28.7% (p < 0.0001) in the RIBO group and the placebo group, and in patients with measurable disease, the ORR was 54.5% versus 38.8% (p < 0.001).5
In the MONALEESA-7 trial, the ORR in all patients was 41% in the RIBO group versus 30% in the placebo group, and among patients with measurable disease, the ORR was 51% and 36%, respectively (p < 0.001 for both comparisons).4 In all MONALEESA trials, the addition of RIBO to ET resulted in measurable tumor reductions, showing an advantage in ORR.
The phase III trials, MONALEESA-2 and MONALEESA-7, both demonstrated a statistically significant OS benefit with the addition of RIBO to ET in pre- and post-menopausal patients.
The MONALEESA-2 trial showed that after 80 months (more than 6.5 years) of follow-up, the median OS was prolonged by more than 12 months, 63.9 months with RIBO plus LET vs 51.4 months with placebo plus LET (HR 0.76; 95% CI: 0.63–0.93), p = 0.0048. Six-year survival rates were 44.2% and 32.0% for RIBO and placebo, respectively. A consistent OS benefit was seen across key subgroups (liver or lung involvement, race, prior chemotherapy or prior hormonal agent, number of metastasis sites, bone-only metastasis, and de novo disease). Ribociclib also delayed time to first chemotherapy by almost 1 year; the median time to first chemotherapy was 50.2 months in the combination group vs 38.9 months in the placebo group (HR 0.74 95% CI: 0.61–0.91).10
In the MONALEESA-7 trial, after a median follow-up of 53.5 months, the median OS was 58.7 vs 48.0 months in the RIBO vs placebo arm (HR 0.76; 95% CI: 0.61–0.96). The survival rate at 4 years was 60% vs 50%, and at 54 months, it was 53% vs 44%.11 Subgroups defined by ET partner were also assessed. In patients receiving a nonsteroidal aromatase inhibitor, the median OS was 58.7 vs 47.7 months in the RIBO vs placebo arm (HR 0.80; 95% CI 0.62–1.04). For patients receiving tamoxifen, the median OS was not estimable vs 49.3 months for RIBO vs placebo (HR 0.71; 95% CI 0.45–1.10).11
Combination of RIBO with Fulvestrant
For patients progressing after a previous course with an AI alone without CDK 4/6, the natural second line is represented by the combination of fulvestrant and RIBO (or palbociclib or abemaciclib). The MONALEESA-31 trial supports the indication of fulvestrant + RIBO. This phase III trial included 726 patients with advanced HR+ BC, with approximately one half receiving first-line endocrine for advanced disease and one half receiving second-line treatment having relapsed at or <12 months from completion of (neo)adjuvant ET with no treatment for advanced or metastatic disease (early relapse), >12 months from completion of (neo)adjuvant ET with subsequent progression after one line of ET for advanced or metastatic disease, and finally those with advanced or metastatic BC at diagnosis who progressed after one line of hormone therapy for advanced disease with no prior (neo)adjuvant treatment for early disease. The median OS in this subgroup was not reached in the combination arm and was 51.8 months (95% CI 40.4–57.6 months) in the fulvestrant/placebo group (HR, 0.64; 95% CI 0.46–0.88). In particular, the endocrine-naive population derived the greatest benefit from the addition of RIBO to fulvestrant (HR = 0.62, 95%0.41–0.95). Patients in the second-line subgroup had a median OS of 39.7 months (95% CI 37.4–46.9 months) in the fulvestrant/RIBO group and 33.7 months (95% CI 27.8–41.3 months) in the fulvestrant/placebo group (HR, 0.78; 95% CI 0.59–1.04).
Patients Selection from Subgroup Analysis
Subgroup analyses in the MONALEESA trials showed a consistent treatment benefit across all subgroups evaluated, including participants age ≥65 years as well as those with visceral metastases, bone-only disease, prior (neo)adjuvant chemotherapy or ET, and de novo disease6 (see Table 1). Another subgroup analysis showed that the benefit of PFS was consistent in patients with visceral metastases regardless of the disease burden (>3 visceral metastases); the HR values were 0.60 (95% CI: 0.40–0.90) and 0.50 (95% CI: 0.31–0.82) in the MONALEESA-2 and MONALEESA-7 trials, respectively.7 In the MONALEESA-2 trial, among patients with non de novo advanced BC, the PFS benefit of RIBO plus LET was consistent regardless of treatment-free interval (TFI) duration. In patients with TFI ≤24 months, the HR was 0.455 (95% CI: 0.296–0.701), and in patients with TFI >24 months, the HR was 0.455 (95% CI: 0.287–0.720). In patients with TFI ≤36 months and TFI >36 months, the HR was 0.422 (95% CI: 0.284–0.627) and 0.507 (95% CI: 0.303–0.851), respectively. In patients with TFI ≤48 months and TFI >48 months, the HR was 0.449 (95% CI: 0.310–0.650) and 0.496 (95% CI: 0.274–0.898), respectively.8 Ribociclib plus LET also showed effective tumor reduction versus placebo plus LET in the MONALEESA-2 trial, in which an early response was reported in 37.2% of patients in the RIBO arm versus 23.3% of patients in the placebo arm at 6 months.9
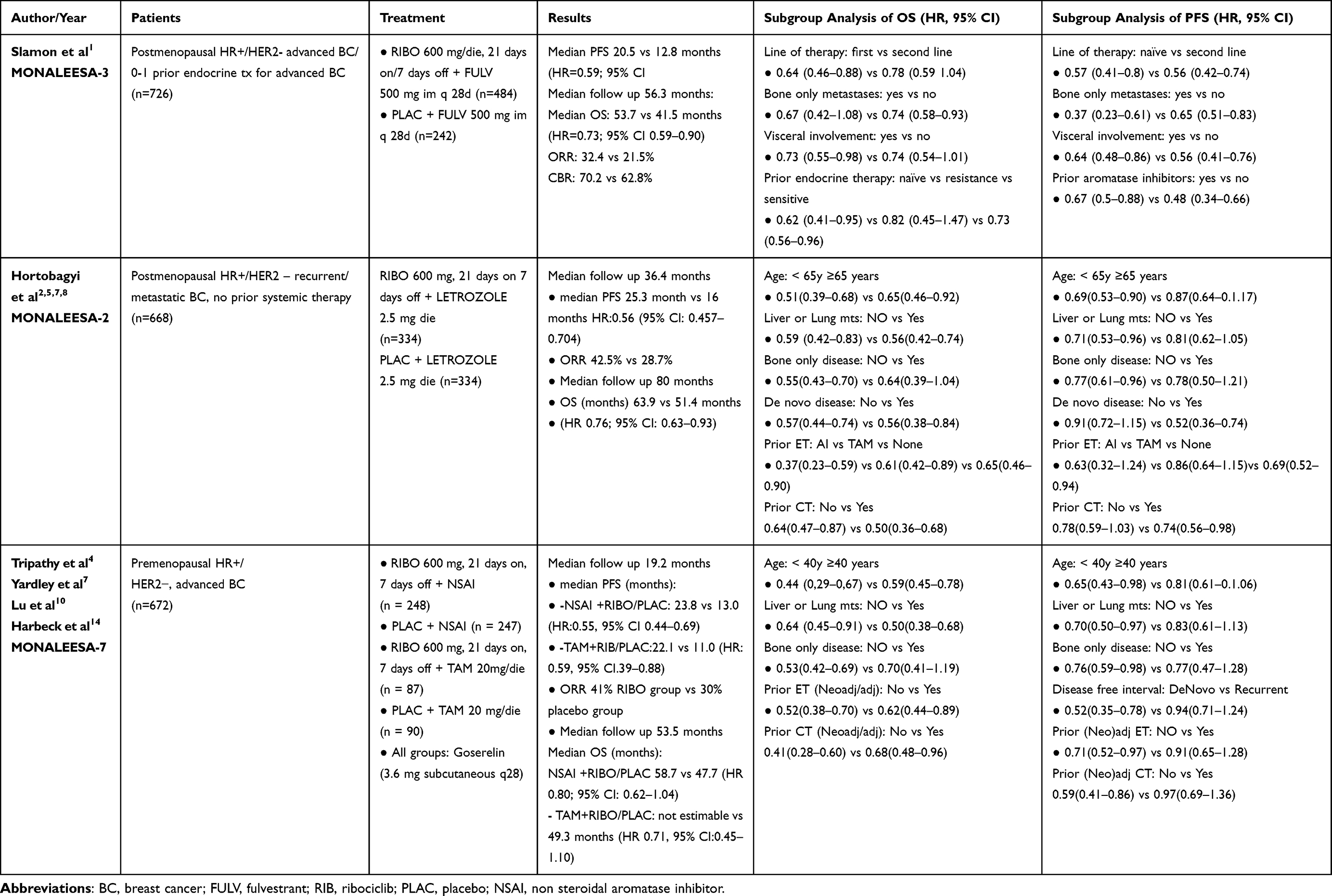 |
Table 1 Phase 3 Ribociclib Studies in Advanced Breast Cancer |
Exploratory subgroups were also assessed for OS; in patients with de novo disease, the median OS was not reached vs 49.6 months with RIBO vs placebo (HR, 0.53; 95% CI, 0.36–0.79). In patients <40 years of age, the median OS was 51.3 vs 40.5 months for RIBO vs placebo (HR, 0.65; 95% CI, 0.43–0.98). In patients ≥40 years of age, the median OS was 58.8 vs 51.7 months for RIBO vs placebo (HR, 0.81; 95% CI, 0.62–1.07).12 Patients who received prior chemotherapy in the advanced setting had a median OS of 47.2 vs 39.0 months (HR, 0.75; 95% CI, 0.44–1.27).
Choice Among Endocrine Agents in Advanced Disease
Other studies with CDK 4/6 inhibitors (palbociclib and abemaciclib) produced similar OS benefits, even if cross-trial comparison is not feasible due to different patient populations. In a large network meta-analysis, Giuliano et al reported a similar outcome among these agents.15 For those with phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA) mutations and whose cancers have progressed on or after treatment with an AI, another option is the combination of a PI3K inhibitor and fulvestrant. Due to lack of head-to-head comparisons, network meta-analysis may help in clinician choice.12 Compared to pictilisib-/fulvestrant and alpelisib/fulvestrant combinations, RIBO/fulvestrant provided better PFS. Also, everolimus plus fulvestrant was significantly inferior to RIBO plus fulvestrant. Regarding severe hematological toxicities, however, abemaciclib plus fulvestrant was associated with a lower risk of toxicities than RIBO plus fulvestrant (RR, 0.14; 95% CI,0.03–0.63). In conclusion, for early progressors at or <12 months, fulvestrant/RIBO may represent one of the best treatments available according to the MONALEESA-3 trial. Similarly, for patients who had previously received an AI without a CDK 4/6 inhibitor for metastatic disease, fulvestrant plus RIBO is a reasonable option, considering patient’s comorbidities, performance status, and site of disease. Other than delaying start of chemotherapy as a subsequent treatment, patients who received fulvestrant/RIBO as a second-line therapy had a better PFS with the further line of therapy than those who received RIBO alone (26 compared to 20.5 months).1
Open questions remain challenging. First, endocrine resistance may emerge due to mutation in the estrogen-binding domain of the gene that encodes for ER (ESR1). In this case, patients may respond favorably to ER-targeting therapies (eg, ER down-regulators) at higher doses than wild-type cases. Second is the choice of CDK 4/6 agent. In the MONALEESA-3 trial, other than hematological toxicities, other grade 3–4 adverse events were liver toxicity (13.9%) and a prolonged QT interval (3.1%); therefore, RIBO may be less preferable for some patients (eg, those on QTc-prolonging agents). Third, the ideal sequence of combinations after the CDK 4/6 plus LET combination and the current place of AI/everolimus doublet are unknown. In this setting, we suggest fulvestrant alone or with alpelisib in case of PIK3CA mutations or chemotherapy (in the case of rapidly progressing symptomatic and/or visceral metastases). Finally, for the treatment of patients that are undergoing adjuvant tamoxifen therapy, LET plus a CDK 4/6 is the obvious choice. Room for improvement in outcome may become possible in the near future with combinations of RIBO with immunotherapy tested in ongoing trials.
Safety and Quality of Life
The safety profile of RIBO in all trials was similar. The most common adverse events (AEs) of any grade in more than 25% of patients were neutropenia, leukopenia, and nausea. In the MONALEESA-2 trial, the most frequent grade 3/4 AEs were neutropenia and leukopenia.7 In the MONALEESA-7 trial, the most common grade 3/4 AEs were neutropenia, leukopenia, and increased aminotransferase6 (Table 2). Elevated aminotransferase levels were observed in all RIBO trials, and grade 3/4 increases were reported in alanine transferase levels (10 vs 2%) and aspartate aminotransferase levels (7 vs 2%) in the RIBO versus placebo group.2,8 In addition, febrile neutropenia was reported in five patients in the RIBO group (1.5%) in the MONALEESA-2 trial5 and in seven patients (2.1%)2 in the same group in the MONALEESA-7 trial.
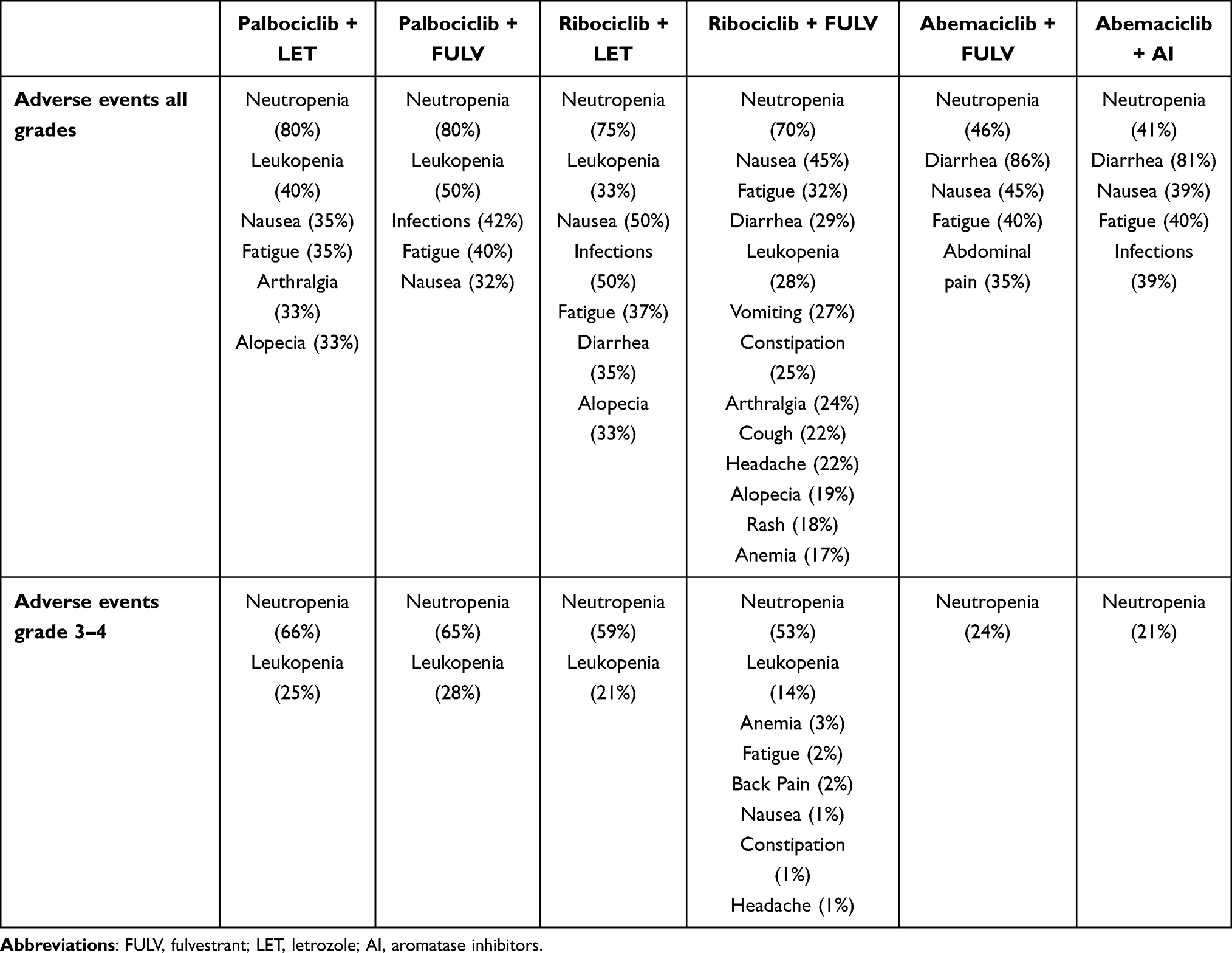 |
Table 2 Cyclin-Dependent Kinases (CDK)4/6 Inhibitors’ Toxicity Profiles |
QTcF prolongation was reported in a small number of patients treated with RIBO in all MONALEESA trials. For example, in the MONALEESA-2 trial, 10 of 334 patients in the RIBO group (3%) showed a >60-ms QTcF prolongation from baseline, and 12 patients (3.6%) had at least one postbaseline QTcF >480 ms versus two of 334 patients (0.6%) in the placebo group.5
In the MONALEESA-7 trial, a postbaseline QTcF >480 ms occurred in 23 patients (6.9%) in the RIBO group and in four patients (1.2%) in the placebo group, and among these patients, postbaseline QTcF >500 ms was reported in five patients (1.5%) and one patient (0.3%), respectively.4
A >60-ms increase in QTcF from baseline occurred in 32 patients (9.6%) in the RIBO group and in six patients (1.8%) in the control group. In the RIBO group, a >60-ms increase from baseline in QTcF was observed in 14 of 87 patients (16%) receiving tamoxifen and in 18 of 245 patients (7%) receiving a nonsteroidal aromatase inhibitor. A >60-ms increase from baseline occurred in the placebo group in six of 90 patients (7%) receiving tamoxifen and in no patients receiving a nonsteroidal aromatase inhibitor.
Ribociclib is not indicated in combination with tamoxifen for treating premenopausal women with advanced BC. Ribociclib use should also be avoided with strong cytochrome P4503A inhibitors and other drugs that prolong the QT interval.4,13
Overall health-related quality of life was maintained from baseline in both arms of the MONALEESA-2 trial in all subgroups of patients (visceral disease, bone-only metastases, best overall response of complete or partial response, and ECOG PS score of 0 or 1).1 A clinically meaningful reduction (>5 points) in the pain score in the European Organisation for Research and Treatment of Cancer Quality of Life Core 30 Questionnaire (EORTC QLQ-C30) was observed at week 8 and was maintained up to cycle 11 in the RIBO arm.13 A more significant improvement in pain from baseline was reported in the RIBO arm (26%) than in the placebo arm (15%).9 In the MONALEESA-7 trials, time to definitive deterioration was ≥10% in the RIBO arm versus the placebo arm.14 In the MONALEESA-7 trial, a reduction in pain was observed at week 8 and maintained up to cycle 19 in the RIBO arm.14 Available results from the MONALEESA trials have consistently shown that RIBO is effective in combination partner and has a manageable safety profile. Recent results from the CompLEEment-1 trial (phase 3b trial in an expanded patient population with hormone receptor-positive, human epidermal growth factor receptor-2–negative advanced BC) confirmed that safety and efficacy data in this expanded population were consistent with the data from the MONALEESA-2 and MONALEESA-7 trials and support the use of RIBO plus LET in the first-line setting for patients with HR +, HER2– advanced BC.16
Comparing to other CDK 4/6 available, RIBO has a higher incidence of liver function test abnormalities than the other agents and can cause QTc prolongation, and therefore may be prudently avoided in patients with cardiac morbidities or other risk factors for QTc prolongation (drugs, interactions). In these cases different agents (palbociclib or abemaciclib) may be used.
Emerging Combinations in Metastatic Setting
Inhibitors of CDK4/6 in treating BC have been shown to improve response rates and prolong disease control in combination with ET in HR+, HER2- advanced or metastatic disease either in front- or subsequent-line.17
Ribociclib is now investigated in various BC subtypes, such as HER2-positive and triple-negative disease, as well as in the adjuvant and neoadjuvant treatments of early BC.
Furthermore, with the aim to optimize clinical outcomes, rational combinations with various therapies, such as PI3K inhibitors (eg, alpenlisib), HER2-directed therapies, and immunotherapy, are under investigation.
HER2+ BC patients represent an important group in the BC population. The advent of trastuzumab revolutionized the treatment of patients in various settings, from localized to advanced or metastatic disease. Despite a high disease control rate, many patients eventually recurred, and more effective treatments are under research. The combination of CDK4/6 inhibitors and an anti-HER2 monoclonal antibody (such as trastuzumab in its various formulations) seems to be a valid approach. Preclinical studies have demonstrated the CDK4/6 inhibitors can resensitize HER2+ BC to anti-HER2 therapies. In a phase 1b/2 study, Goel et al investigated the safety and efficacy of combining RIBO with trastuzumab: despite the treatment combination’s good tolerability, only one patient experienced stable disease.18 The combination’s apparent low activity should be a consequence of a cohort of patients being heavily pretreated, and large Phase II trials must be initiated to establish real activity.
Evolution of anti-HER2 therapy has been the immunoconjugate ado-trastuzumab emtansine in patients previously treated with trastuzumab. As a consequence, the next step in the development of a new and effective multidrug approach should be represented by the combination of CDK4/6 inhibitors and ado-trastuzumab emtansine. In a phase 1b trial, the combination of ado-trastuzumab emtansine and RIBO has been investigated in patients with previously treated BC (including anti-HER2 trastuzumab). No dose-limiting toxicities were observed, and the majority of adverse events were graded as 1 or 2, with only grade 3 neutropenia, leukopenia, and anemia, usually reported with CDK4/6 monotherapy.19
Further development of anti HER2-drugs in treating metastatic BC led to the approval of trastuzumab deruxtecan, an antibody-drug conjugate composed of an anti-HER2 antibody, a cleavable tetrapeptide-based linker, and a cytotoxic topoisomerase I inhibitor. In a phase II trial, this new chemotherapeutic agent showed durable antitumor activity in a population of heavily pretreated patients suffering from metastatic BC.20 Currently, no data is available regarding the use of trastuzumab deruxtecan together with RIBO, and no study has been conducted to investigate this eventually very effective combination.
Approximately 40% of patients with HR+, HER2-negative BC have activating mutations in the gene PIK3CA, inducing hyperactivation of the alpha isoform (p110α) of phosphatidylinositol 3-kinase (PI3K).21 The inhibition of the PI3K pathway has been intensively evaluated in the treatment of BC, and the most significant results have been obtained in patients with HR+/HER2 disease.22 In this light, in a phase Ib trial, Tolaney et al tried to investigate the safety and efficacy of a triple combination of RIBO-fulvestrant and a PI3K inhibitor, such as alpelisib or buparlisib. Although RIBO plus fulvestrant showed a significant OS benefit over placebo plus fulvestrant in patients with HR+, HER2-negative advanced BC,1 triple combinations with alpelisib or buparlisib plus fulvestrant are not recommended for phase II investigation due to unexpected toxicity. In particular, adverse events of special interest that were most commonly seen were hepatobiliary toxicity, infections, and neutropenia.23 Finally, a potential role for combination therapy with CDK4/6 inhibitors and immunotherapy has been proposed. In vivo models confirm enhanced tumor regression when an immune checkpoint blockade with an anti-PD-L1 antibody is added to CDK4/6 inhibition.24,25 Of interest, researchers are currently recruiting for a multicenter phase II study to evaluate the combination of LET, palbociclib, and pembrolizumab in postmenopausal women with hormone-receptor positive advanced BC.26 In the RIBECCA trial, treatment with RIBO showed favorable effects on the peripheral innate and adaptive immune response in patients with HR+ BC.27
A number of other CDK4/6 inhibitor–immunotherapy combination studies are ongoing in various settings, and the results could radically change oncologists’ approach in the management of BC in various settings, from neo- and adjuvant settings to advanced and/or metastatic disease.28,29 The treatment of BC has radically changed in the last few years, and more drugs have been implemented in oncologists’ armamentaria. Targeted therapy and precision oncology represent the current main road, but novel and more effective treatment options could be available in the next few years. CDK4/6 inhibitors such as palbociclib, abemaciclib, and RIBO have played a central role in treating BC, not only in combination with ET but also with novel agents, to pursue a totally chemotherapy-free approach.
Adjuvant Studies
Although the results of adjuvant CDK 4/6 inhibitors are conflicting (2 published studies demonstrated opposite results), data about RIBO in this setting are lacking. At the 2021 San Antonio Breast Cancer Symposium, data from the Phase 2 LEADER trial were presented.30 For part 1 of the LEADER trial, patients with localized stage I to III ER-positive (≥10%), HER2-negative BC who had completed surgery and started adjuvant ET were randomized to receive either continuous RIBO (400 mg daily on a 28-day cycle) or intermittent RIBO (600 mg daily on days 1–21 of a 28-day cycle) for 1 year. The major finding is that about one-third of patients taking RIBO in the adjuvant setting may need to discontinue RIBO early, and nearly as many require a dose reduction. The most common grade 3 or greater adverse events leading to study discontinuation were neutropenia (44%), alanine aminotransferase (ALT) increase (28%), and aspartate aminotransferase (AST) increase (16%). Rates of serious adverse events were similar for both groups even if no patients discontinued early due to a prolonged QTc interval. Although dose reduction did not influence outcomes in advanced disease,31 confirmatory studies are needed to confirm efficacy and safety in the early stages of disease. The ADAPTcycle is an ongoing phase III trial that will respond to the question about RIBO benefit in patients with early BC previously responders to neoadjuvant ET. Data about palbociclib (negative study) and abemaciclib (positive trial) are opposite in term of benefit, likely to the different mechanism of action of 2 drugs. LEADER study will clarify if any the role of RIBO in this setting. Also, the NATALEE phase 3 multicenter, randomized, open-label trial will evaluate the efficacy and safety of RIBO + ET as adjuvant treatment in patients with HR+, HER2– early BC (NCT03701334).
Neoadjuvant Use of RIBO with ET or Other Agents
Neoadjuvant therapy (NAT) represents a standard treatment option for selected patients with locally advanced BC. Although chemotherapy (CT) is primarily used in NAT, ET has also been explored, particularly in postmenopausal women with luminal clinical stage II/III BC with strong HR expression and a low proliferative index. To date, neoadjuvant endocrine therapy (NET), which rarely leads to pCR,32 is not broadly accepted as an appropriate standard of care in early BC; it is mostly reserved for the elderly or patients with significant comorbidities.
The combination of endocrine therapy and CDK 4/6 inhibitors, the gold standard for treatment of advanced luminal tumors, has also been tested in the neoadjuvant setting in comparison with aromatase inhibitor alone or with chemotherapy (Table 3).
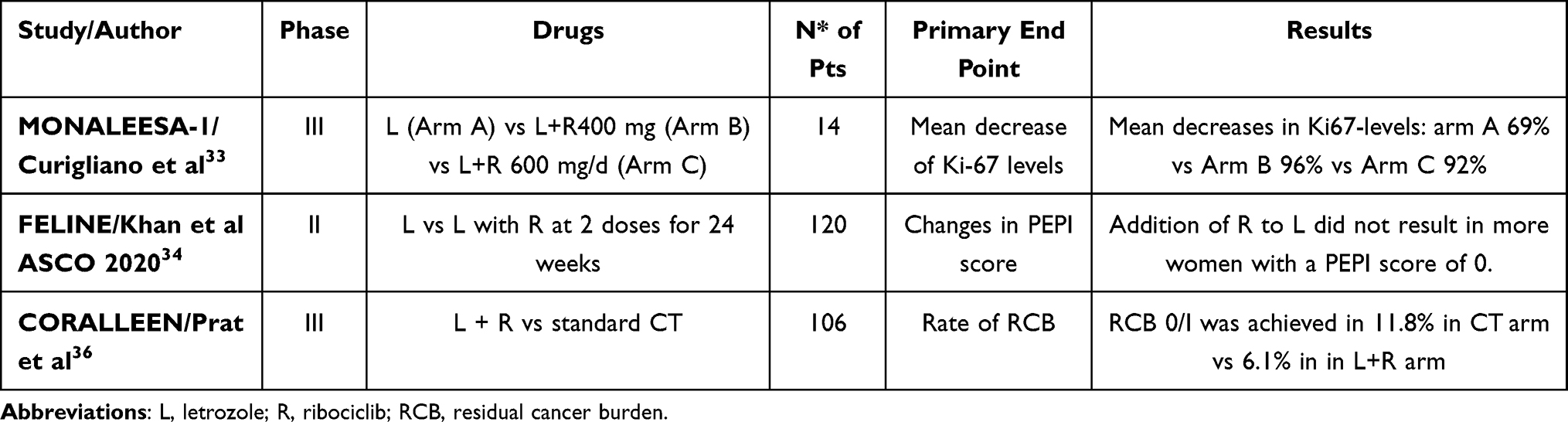 |
Table 3 Neoadjuvant Studies with Ribociclib in ER+ Breast Cancer |
The role of RIBO as a NAT was explored in the MONALEESA-1 trial, a 3-arm study that compared RIBO (at 2 doses: 400 and 600 mg/d) with LET to single-agent L in 14 menopausal women with endocrine-sensitive Her 2 negative BC (HR+HER2- BC), with the primary aim of comparing Ki-67 levels in the 3 study arms.33 Ki-67 levels were reduced in the combination arms compared to L alone (69% decrease in the LET monotherapy arm, 96% for LET with RIBO 400 mg/d, and 92% for LET with RIBO 600 mg/d). Combination therapy was well tolerated, with no reported grade 3/4 adverse events. However, the small number of patients does not allow us to be confident with these results.
The FELINE trial is a Phase II, 3-arm study that compared R (at 2 doses: 400 or 600 mg/d) with L versus single-agent L as a NAT in 120 menopausal women with ER+ HER2- BC.34 The primary aim of the study was to determine if combination arms compared with L alone for 24 weeks as a NAT increases the proportion of patients with a preoperative endocrine prognostic index (PEPI) score of 0 at surgery. Other endpoints were change in centrally performed Ki-67, complete cell-cycle arrest (CCCA), clinical/imaging response, and difference in response and toxicity between the two R arms (RC and RI).
The addition of R to L as a NET did not result in more women with a PEPI score of 0, and CCCA at surgery was similar between the two groups. The researchers found no difference in clinical, mammographic, US, or MRI response between L alone and the L+R combination.
Continuous and intermittent doses of R have similar efficacy and toxicity.
In the neoadjuvant setting, in ER+HER2- BC, a CDK4/6 inhibitor in combination with ET could represent an alternative to multiagent chemotherapy (CT).
In the CORALLEEN study, researchers randomized 106 postmenopausal patients with stage I–III HR+/HER2- BC classified as luminal B by PAM5035 to receive the combination of L and R or chemotherapy with 4 cycles of AC followed by paclitaxel for 12 weeks.36 The duration of both treatments was 24 weeks. The principal endpoint was the proportion of patients with a low risk of relapse (ROR) score in surgical samples. About 46% of patients in both arms had a low ROR at surgery, showing an activity in downstaging of the tumor. Residual cancer burden (RCB) 0/I was achieved in 11.8% and 6.1% of the participants in the CT and L plus R arm, respectively, and the pCR rate was lower (5.8% vs 0%). The clinical response rate was higher with CT than with L plus R (78.8% vs 57.1%), but the proportion of breast-conserving surgery was similar in both groups (72.2% vs 85.7%).
It is noteworthy that the proportion of low-ROR disease in the no-chemotherapy group was high at 24 weeks (about 47%), as in the chemotherapy group, and this trial’s results suggest that the neoadjuvant approach may be fully explored in the future and allow for better identification of the patients who might have a good outcome without chemotherapy.
Conclusions
The incorporation of RIBO and of other CDK 4/6 inhibitors has revolutionized the treatment of HR+ BC in both early and advanced disease. Studies in adjuvant settings have been recently released, but work is still in progress. The armamentarium for metastatic disease has more solid data.
For most women with HR+ BC who progress in adjuvant therapy or within 12 months of completion and those who progress in first-line treatment with an AI, fulvestrant/RIBO is one of the most appealing combinations. For patients with de novo advanced BC or those relapsing after the end of adjuvant ET, an AI with a CDK 4/6 inhibitor (plus or minus LHRH analogues for women in premenopausal status) is being offered largely for the HR+ population. In particular, the data from the MONALEESA-2 trial included for the first time a median OS exceeding 5 years in a phase 3 trial for advanced HR+ BC with a RIBO/LET combination.
In conclusion, RIBO either with LET or fulvestrant is effective for the entire spectrum of patients with HR+ BC in the advanced setting. If this combination will move into earlier phases of disease, it will be a hot topic for the next few years.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Slamon DJ, Neven P, Chia S, et al. Ribociclib plus fulvestrant for postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the phase III randomized MONALEESA-3 trial: updated overall survival. Ann Oncol. 2021. doi:10.1016/j.annonc.2021.05.353
2. Hortobagyi GN, Stemmer SM, Burris HA, et al. Overall survival results from the phase III MONALEESA-2 trial of postmenopausal patients with HR+/HER2- advanced breast cancer treated with endocrine Therapy ± Ribociclib.
3. Hortobagyi GN, Stemmer SM, Burris HA, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016;375(18):1738–1748. doi:10.1056/NEJMoa1609709
4. Tripathy D, Im SA, Colleoni M, et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised Phase 3 trial. Lancet Oncol. 2018;19(7):904–915. doi:10.1016/S1470-2045(18)30292-4
5. Hortobagyi GN, Stemmer SM, Burris HA, et al. Updated results from MONALEESA-2, a Phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol. 2018;29(7):1541–1547. doi:10.1093/annonc/mdy155
6. Hortobagyi GN. Ribociclib for the first-line treatment of advanced hormone receptor- positive breast cancer: a review of subgroup analyses from the MONALEESA-2 trial. Breast Cancer Res. 2018;20(1):123. doi:10.1186/s13058-018-1050-7
7. Yardley D, Chan A, Nusch A, et al. Ribociclib plus endocrine therapy in patients with hormone receptor-positive, HER2-negative advanced breast cancer presenting with visceral metastases: subgroup analysis of Phase 3 MONALEESA trials.
8. Blackwell KL, Paluch-Shimon S, Campone M, et al. Subsequent treatment for postmenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer who received ribociclib + letrozole vs placebo + letrozole in the Phase III MONALEESA-2 study.
9. Janni W, Alba E, Bachelot T, et al. First-line ribociclib plus letrozole in postmenopausal women with HR+, HER2- advanced breast cancer: tumor response and pain reduction in the Phase 3 MONALEESA-2 trial. Breast Cancer Res Treat. 2018;169(3):469–479.
10. Lu YS, Im SA, Colleoni M, et al. Updated overall survival of ribociclib plus endocrine therapy versus endocrine therapy alone in pre- and perimenopausal patients with HR+/HER2- advanced breast cancer in MONALEESA-7: a Phase III Randomized Clinical Trial. Clin Cancer Res. 2021;4:54
11. Yardley DA. MONALEESA clinical program: a review of ribociclib use in different clinical settings. Future Oncol. 2019;15(23):2673–2686. doi:10.2217/fon-2019-0130
12. Leung JH, Leung HWC, Wang SY, Huang SS, Chan ALF. Efficacy and safety of CDK4/6 and PI3K/AKT/mTOR inhibitors as second-line treatment in postmenopausal patients with hormone receptor-positive, HER-2-negative metastatic breast cancer: a network meta-analysis. Expert Opin Drug Saf. 2021;20(8):949–957. PMID: 34047239. doi:10.1080/14740338.2021.1931116
13. Verma S, O’Shaughnessy J, Burris HA, et al. Health-related quality of life of postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer treated with ribociclib + letrozole: results from MONALEESA-2. Breast Cancer Res Treat. 2018;170(3):535–545. doi:10.1007/s10549-018-4769-z
14. Harbeck N, Villanueva Vazquez R, Tripathy D, et al. Ribociclib (RIB) plus tamoxifen (TAM) or a non-steroidal aromatase inhibitor (NSAI) in premenopausal women with hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2−) advanced breast cancer (ABC): additional results from the MONALEESA-7 trial. Eur J Cancer. 2018;92(Suppl3):S1.
15. Giuliano M, Schettini F, Rognoni C, et al. Endocrine treatment versus chemotherapy in postmenopausal women with hormone receptor-positive, HER2-negative, metastatic breast cancer: a systematic review and network meta-analysis. Lancet Oncol. 2019;20(10):1360–1369. PMID: 31494037. doi: 10.1016/S1470-2045(19)30420-6
16. De Laurentiis M, Borstnar S, Campone M, et al. Full population results from the core phase of CompLEEment-1, a phase 3b study of ribociclib plus letrozole as first-line therapy for advanced breast cancer in an expanded population. Breast Cancer Res Treat. 2021;189(3):689–699. doi:10.1007/s10549-021-06334-0
17. Murphy CG. The role of CDK4/6 inhibitors in breast cancer. Curr Treat Options Oncol. 2019;20(6):52. doi:10.1007/s11864-019-0651-4
18. Goel S, Pernas S, Tan-Wasielewski Z, et al. Ribociclib plus trastuzumab in advanced HER2-positive breast cancer: results of a phase 1b/2 trial. Clin Breast Cancer. 2019;19(6):399–404. doi:10.1016/j.clbc.2019.05.010
19. Spring LM, Clark SL, Li T, et al. Phase 1b clinical trial of Ado-Trastuzumab emtansine and ribociclib for HER2-positive metastatic breast cancer. NPJ Breast Cancer. 2021;7(1):103. doi:10.1038/s41523-021-00311-y
20. Modi S, Saura C, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N Engl J Med. 2020;382(7):610–621. doi:10.1056/NEJMoa1914510
21. André F, Ciruelos E, Rubovszky G, et al. Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced breast cancer. N Engl J Med. 2019;380(20):1929–1940. doi:10.1056/NEJMoa1813904
22. Schettini F, Buono G, Trivedi MV, et al. PI3K/mTOR inhibitors in the treatment of luminal breast cancer. Why, When and to Whom? Breast Care. 2017;12(5):290–294. doi:10.1159/000481657
23. Tolaney SM, Im YH, Calvo E, et al. Phase Ib study of ribociclib plus fulvestrant and ribociclib plus fulvestrant plus PI3K inhibitor (Alpelisib or Buparlisib) for HR+ advanced breast cancer. Clin Cancer Res. 2021;27(2):418–428. doi:10.1158/1078-0432.CCR-20-0645
24. Goel S, DeCristo MJ, Watt AC, et al. CDK4/6 inhibition triggers anti-tumour immunity. Nature. 2017;548(7668):471–475. doi:10.1038/nature23465
25. Deng J, Wang ES, Jenkins RW, et al. CDK4/6 inhibition augments antitumor immunity by enhancing T-cell activation. Cancer Discov. 2018;8(2):216–233. doi:10.1158/2159-8290.CD-17-0915
26. Fribbens C, O’Leary B, Kilburn L, et al. Plasma ESR1 mutations and the treatment of estrogen receptor-positive advanced breast cancer. J Clin Oncol. 2016;34(25):2961–2968. PMID: 27269946. doi:10.1200/JCO.2016.67.3061
27. Peuker CA, Yaghobramzi S, Grunert C, et al. Treatment with ribociclib shows favourable immunomodulatory effects in patients with hormone receptor-positive breast cancer-findings from the RIBECCA trial. Eur J Cancer. 2022;162:45–55. doi:10.1016/j.ejca.2021.11.025
28. Pembrolizumab, Letrozole, and Palbociclib in treating postmenopausal patients with newly diagnosed metastatic stage IV estrogen receptor positive breast cancer. Available from: https://clinicaltrials.gov/ct2/show/NCT02778685.
29. Ameratunga M, Kipps E, Okines AFC, et al. To cycle or fight-CDK4/6 inhibitors at the crossroads of anticancer immunity. Clin Cancer Res. 2019;25(1):21–28. doi:10.1158/1078-0432.CCR-18-1999
30. Spring L, Griffin C, Isakoff SJ, et al. Phase II study of adjuvant endocrine therapy with CDK 4/6 inhibitor, ribociclib, for localized ER+/HER2- breast cancer (LEADER). J Clin Oncol. 2020;38:531. doi:10.1200/jco.2020.38.15_suppl.531
31. Burris HA, Chan A, Bardia A, et al. Safety and impact of dose reductions on efficacy in the randomised MONALEESA-2, −3 and −7 trials in hormone receptor-positive, HER2-negative advanced breast cancer. Br J Cancer. 2021;125(5):679–686. doi:10.1038/s41416-021-01415-9
32. Haddad TC, Goetz MP. Landscape of neoadjuvant therapy for breast cancer. Ann Surg Oncol. 2015;22:1408–1415. doi:10.1245/s10434-015-4405-7
33. Curigliano G, Gomez Pardo P, Meric-Bernstam F, et al. Ribociclib plus letrozole in early breast cancer: a presurgical window-of-opportunity study. Breast. 2016;25:191–198. doi:10.1016/j.breast.2016.06.008
34. Khan Q. Letrozole plus ribociclib or placebo as neoadjuvant therapy in ER-positive, HER2-negative. Proc Am Soc. 2020;abs 505.
35. Wallden B, Storhoff J, Nielsen T, et al. Development and verification of the PAM50-based Prosigna breast cancer gene signature assay. BMC Med Genomics. 2015;8:54. doi:10.1186/s12920-015-0129-6
36. Prat A, Saura C, Tomás Pascual C, et al. Ribociclib plus letrozole versus chemotherapy for postmenopausal women with hormone receptor-positive, HER2-negative, luminal B breast cancer, CORALLEEN. Lancet. 2020;21(1):33–43. doi:10.1016/S1470-2045(19)30786-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.