")
Back to Journals » Clinical Ophthalmology » Volume 15
Revisiting the Robustness of Pentacam HR Indices Against Soft Contact Lens Wear
Authors Elkitkat RS , Badran TA, Ebeid WM
Received 26 February 2021
Accepted for publication 23 March 2021
Published 15 April 2021 Volume 2021:15 Pages 1573—1581
DOI https://doi.org/10.2147/OPTH.S308560
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rania Serag Elkitkat,1– 3 Tamer Abdelfattah Badran,1,4 Weam Mohamed Ebeid1
1Ophthalmology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 2Watany Eye Hospitals, Cairo, Egypt; 3Watany Research and Development Center, Cairo, Egypt; 4Specialized Eye Center, Cairo, Egypt
Correspondence: Rania Serag Elkitkat Email [email protected]
Purpose: To evaluate various selected Pentacam HR indices in a cohort of soft contact lens (SCL) wearers before and after SCL discontinuation.
Methods: Ninety right eyes of 90 SCL wearers (group 1) were compared to healthy controls (group 2). For group 1 eyes, Pentacam HR images were captured within one hour of SCL removal and after one month of discontinuation. The evaluated indices included curvature, elevation, and pachymetric parameters.
Results: Elevation indices and two pachymetric indices (central corneal thickness and thinnest corneal thickness) did not show significant differences, either between the two groups or in group 1 after SCL discontinuation. Some pachymetric indices (average and maximum corneal pachymetry progression indices, and maximum Ambrosio’s relational thickness index) showed statistically significant (P-value < 0.001), yet clinically irrelevant differences. Contrarily, changes in curvature indices were both statistically significant (P-value < 0.001) and clinically relevant.
Conclusion: From a clinical point of view, many elevation and pachymetric indices are robust against SCL wear, and can be relied upon for corneal ectasia screening of SCL wearers, even without abstaining from wearing SCLs.
Keywords: soft contact lens warpage, Pentacam HR indices, soft contact lens wearers, silicone hydrogel contact lenses, contact lens discontinuation
Introduction
Refractive errors are prevalent causes of correctable visual impairment worldwide. Their frequency tends to increase among populations with higher educational levels. Optical correction of these errors should suit the lifestyle, daily activities, and visual requirements of the affected cohorts.1,2
Modalities for refractive error correction include spectacles, soft contact lenses (SCLs), and refractive surgical procedures. Each of these methods has advantages and disadvantages. Although spectacles are a safe and effective way of achieving satisfactory visual function, they are considered cosmetically unpleasant by many people, especially females. Moreover, the narrower visual field, possible alterations of retinal image size with high errors, and undesirable effects of anisometropia are among the disadvantages of spectacles wear.3
SCLs are popular among young adults, especially females, although surgical correction of refractive errors is preferred by those who desire to avoid the continuous expenses and the cumbersome procedures of SCL care, or by people working in particular occupations, including athletes and members of the military services.4 However, there is a growing population of people with refractive errors for whom surgical correction is considered unsafe. These patients are prevented from receiving surgical procedures, especially with the recent advances in preoperative corneal assessment, safety precautions, and guidelines that are meant to avoid the risk of post-surgical ectasia.5,6
SCL wear can be associated with corneal warpage, which results in corneal assessment errors, including possible false diagnoses of corneal ectasia. For this reason, many studies addressed this effect of SCLs on the cornea, to avoid the misinterpretation of topographic/tomographic data.7–9
The possible impact of SCL wear on corneal surface regularity and thickness has been previously reported in the literature. Most studies reported an initial, short-term corneal flattening followed by steepening, which is sometimes irreversible on SCL discontinuation. Corneal thinning, mainly central, has been commonly observed, especially with the newer silicone hydrogel contact lenses, characterized by higher oxygen permeability leading to a remarkable reduction of corneal hypoxia, hence decreasing the incidence of corneal edema in SCL wearers.7,10
To our knowledge, this is the first study evaluating multiple important topographic/tomographic Pentacam HR parameters in a cohort of SCL wearers compared with non-wearers, and also within the SCL wearers cohort after a discontinuation period. The aim of this study was to highlight the overall variability of the Pentacam indices, which should be taken into consideration when evaluating SCL wearers for refractive surgical correction or when screening for ectasia. We aimed to determine which Pentacam indices were robust against the effect of SCL wear on the cornea, thus not showing significant changes when compared with controls, or after an SCL discontinuation period. The Pentacam HR was chosen as a robust and reliable device for detecting small changes in the evaluated indices.
Patients and Methods
This prospective, case-control, observational study was conducted on refractive surgery candidates who sought medical advice at the Specialized Eye Center, Cairo, Egypt. Detailed SCL wear history was recorded (including SCL type and wear duration). Corrected Distance Visual Acuity (CDVA), refractive spherical equivalent, and slit lamp findings were recorded for all participants. The corneas of the enrolled subjects were evaluated using Pentacam HR, branded as Allegro Oculyzer II (WaveLight GmbH, Erlangen, Germany), software version 120r20, with consecutive inclusion of right eyes conforming with the study design. Images were captured at least thrice, and the most reliable scans were included as per the device manual instructions. All the recruited eyes were imaged in the period from November 2018 to May 2020. The study adhered to the tenets of the Declaration of Helsinki, with informed consents signed by all participants. The Ethical Committee of Ain Shams University approved the study protocol.
Corneas were classified into two groups: group 1 included 90 corneas of SCL wearers, and group 2 was comprised of 90 normal corneas of age- and sex-matched controls. The corneas in group 1 were imaged within one hour of lens removal and re-imaged after one month of SCL discontinuation.
All group 1 participants had been using the same type and brand of SCLs (silicone hydrogel, Johnson and Johnson), for a period of three to five years and on a regular daily basis.
The exclusion criteria were: patients younger than 18 or older than 40 years of age, history of any previous ocular trauma or surgery, hypermetropia or astigmatism of more than one diopter; any clinical symptoms or signs of dry eye, or anterior segment pathology on slit lamp examination. We also excluded corneas with quality specification (QS) suggesting poor data validity for the captured Pentacam HR images, any significant corneal opacity on the Pentacam Scheimpflug display affecting curvature parameters, or any topographic/tomographic evidence of corneal ectasia.
The Investigated Indices Included
Curvature-Based Indices
- Maximum Keratometry reading (K max).
- Mean Keratometry reading (K mean).
- Index of Surface Variance (ISV). (normal value <40)
- Index of Height Decentration (IHD). (normal value <0.016)
Elevation-Based Indices (All Obtained from the 8 mm Diameter)
- Anterior elevation (AE) of the thinnest point from the best fit sphere (BFS). (normal value <+8 um)
- Posterior elevation (PE) of the thinnest point from the BFS. (normal value <+16 um)
- AE from the best fit toric ellipsoid (BFTE). (normal value <+5 um)
- PE from the BFTE. (normal value <+15 um)
Pachymetry Based Indices
- Central Corneal Thickness (CCT).
- Thinnest Corneal Thickness (TCT).
- Average and Maximum Corneal Pachymetry Progression indices (PPI avg (normal value <1.14) and PPI max (normal value <1.6), respectively).
- Maximum Ambrosio’s Relational Thickness index (ART max). (normal value >319 um)
The aforementioned values of some indices have been considered as per the normative values of the Pentacam user manual.
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics for Windows (Version 25.0. Armonk, NY: IBM Corp). Quantitative data were presented as medians and interquartile ranges (IQR). Sex differences were evaluated by the chi-squared test. The one-sample Kolmogorov–Smirnov test was used to test for normality. Comparison between groups was performed using the independent-sample Mann–Whitney U-test. The Wilcoxon signed-rank test was used to compare repeated measurements of the same group. P-values < 0.05 were considered statistically significant.
Results
This study included a cohort of 90 right eyes of 90 SCL wearers (group 1), who had used SCLs for three to five years on a regular daily basis. Their mean age was 27.33 ± 4.08 years. An equal number of normal corneas from age and sex-matched healthy subjects formed the control group (group 2). Demographic data, Corrected Distance Visual Acuity (CDVA), and refractive spherical equivalents of the two groups are shown in Table 1, and no statistically significant difference between the groups in any of these variables was found.
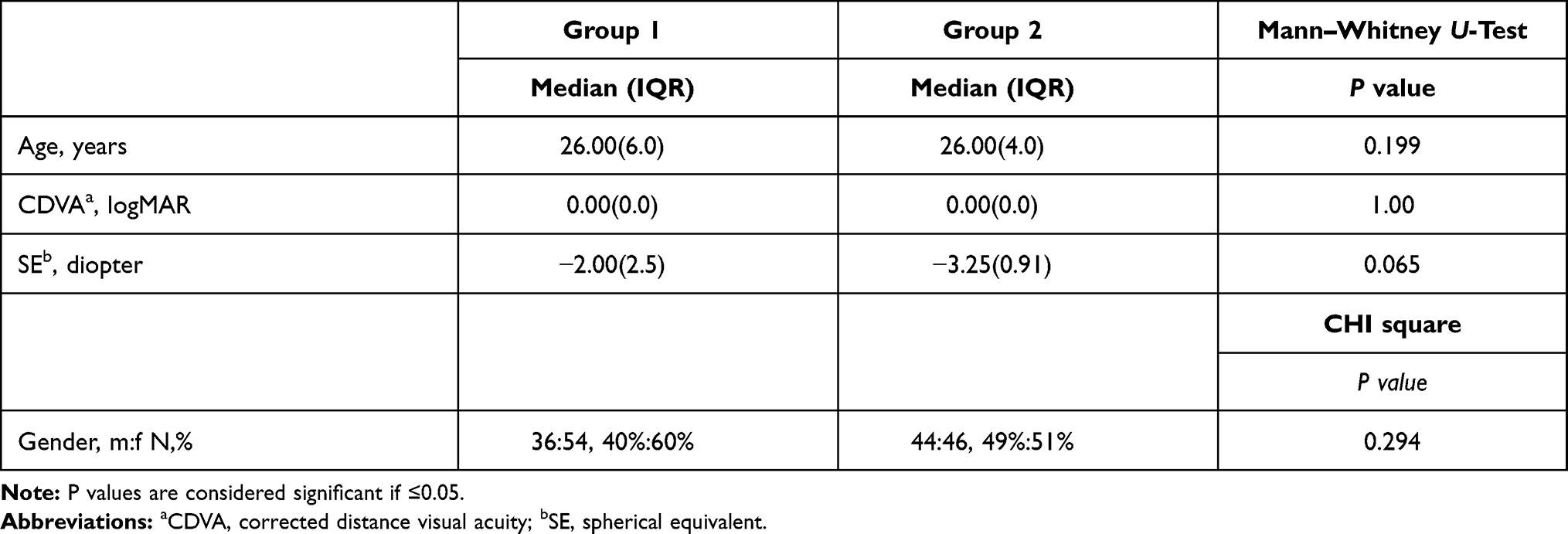 |
Table 1 Demographic Data, Corrected Distance Visual Acuity (CDVA), and Refractive Spherical Equivalent for the 2 Studied Groups |
When we compared the curvature-based Pentacam HR indices between the two groups, without SCL discontinuation in group 1, we detected significantly higher values in group 1 compared to group 2 for all the indices considered (K mean, K max, ISV, and IHD), denoting increased corneal steepening (P-value <0.001 for all indices).
Regarding the elevation-based indices, data analysis revealed statistically non-significant differences between the two groups in AE from BFTE, PE from BFTE, and PE from BFS. The only elevation-based index that showed significantly higher values in group 1 than in group 2 was AE from BFS (P-value = 0.004).
The comparison of pachymetry-based indices between the two groups demonstrated statistically significant differences (yet narrow from a clinical aspect) in PPI avg and PPI max (higher in group 1, both P-values <0.001), and ART max (lower in group 1, P-value <0.001). On the contrary, the CCT and TCT pachymetry indices showed non-significant differences between the two groups.
The descriptive statistics of all investigated Pentacam HR parameters and the differences between the two groups are detailed in Table 2.
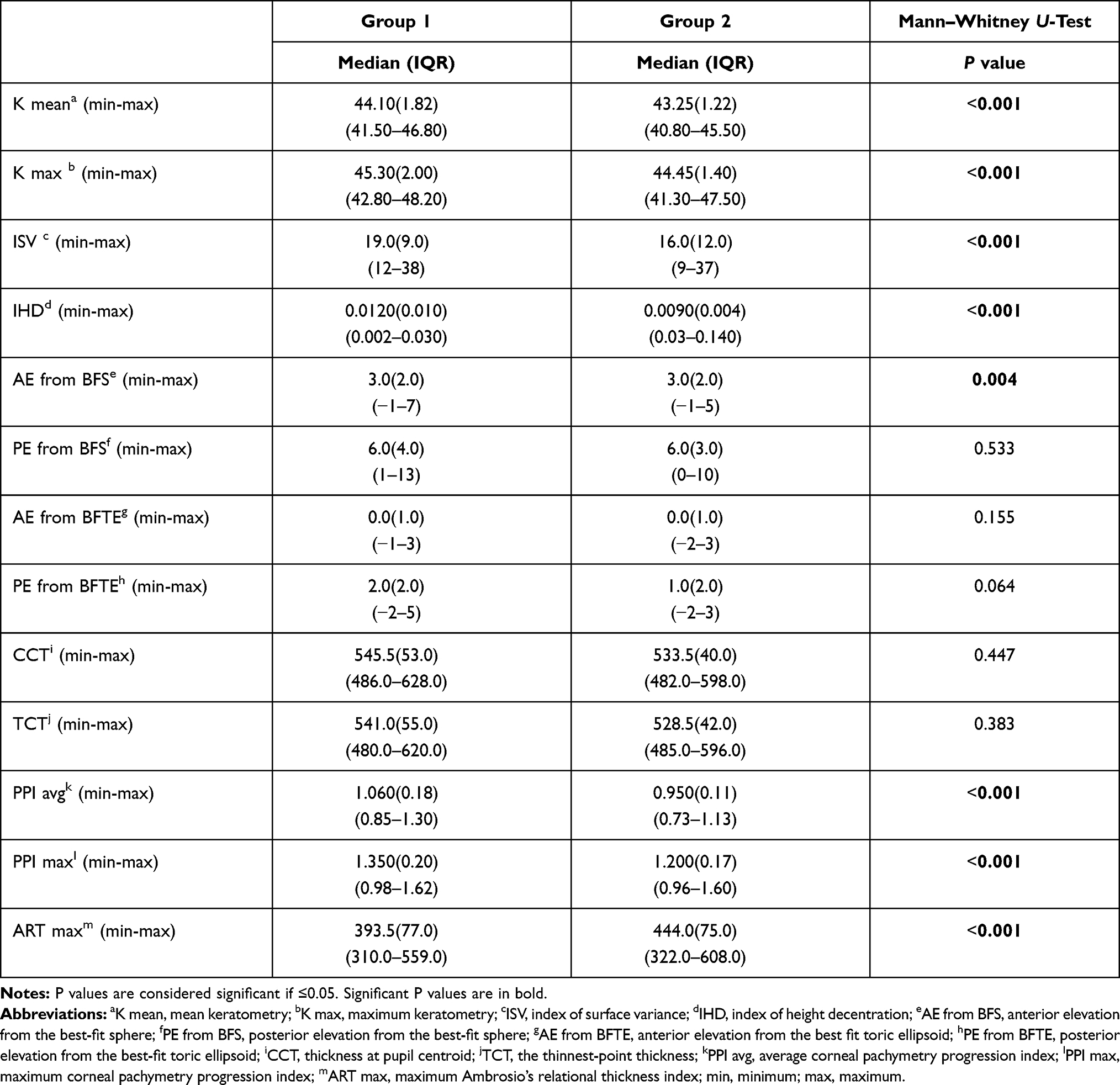 |
Table 2 Medians, Interquartile Ranges (IQR), Minimum (Min) and Maximum (Max) Values of the Various Pentacam HR Indices for the 2 Studied Groups, and P values of Significance Between the 2 Groups |
The corneas in group 1 underwent Pentacam HR imaging again one month after SCL discontinuation. When comparing the two measurements before and after SCL discontinuation, all the curvature indices showed a statistically significant decrease after the discontinuation period (P-value <0.001), while no statistically significant changes were noted in any of the elevation indices. Regarding pachymetric indices, PPI avg, PPI max, and ART max showed statistically significant differences (yet narrow from a clinical aspect) between the two Pentacam captures (P-value <0.001), while the differences in CCT and TCT were not statistically significant.
Box plots were also performed for some selected curvature indices (Figure 1) and other selected elevation and pachymetric indices (Figure 2) for corneas of group 1 to graphically represent these indices before and 1 month after SCL discontinuation, illustrating the same aforementioned results.
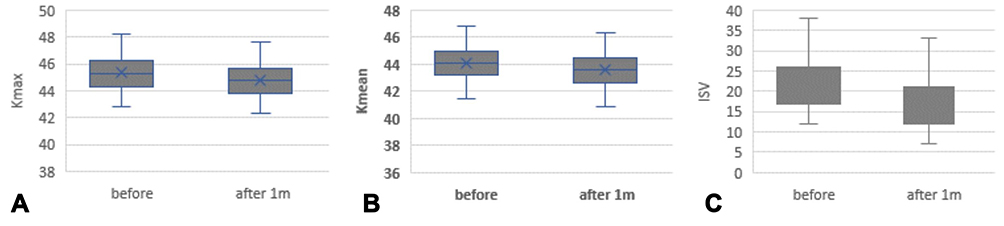 |
Figure 1 Boxplot of some curvature Pentacam-HR indices values in group 1 corneas before and 1month after the Soft Contact Lens (SCL) discontinuation period. (A) K max: Maximum keratometry, (B) K mean: Mean keratometry, (C) ISV: index of surface variance. |
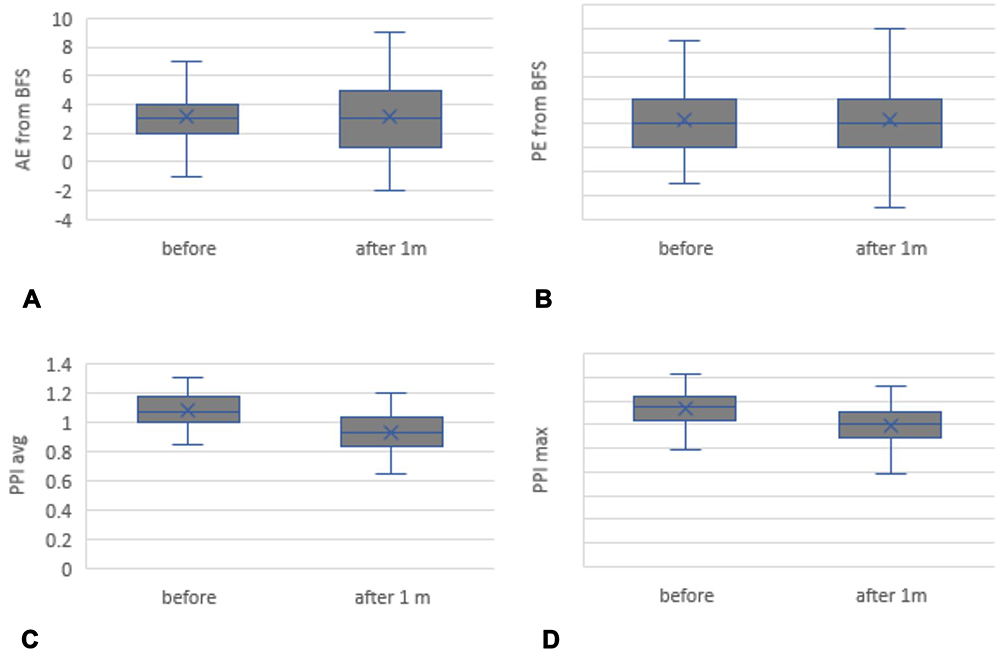 |
Figure 2 Boxplot of some elevation and pachymetric Pentacam-HR indices values in group 1 corneas before and 1month after the Soft Contact Lens (SCL) discontinuation period. (A) AE from BFS: anterior elevation from the best-fit sphere, (B) PE from BFS: posterior elevation from the best-fit sphere, (C) PPI avg: average corneal pachymetry progression index, (D) PPI max: maximum corneal pachymetry progression index. |
The descriptive statistics and the comparison of Pentacam indices values in group 1 corneas before and after the SCL discontinuation period are detailed in Table 3.
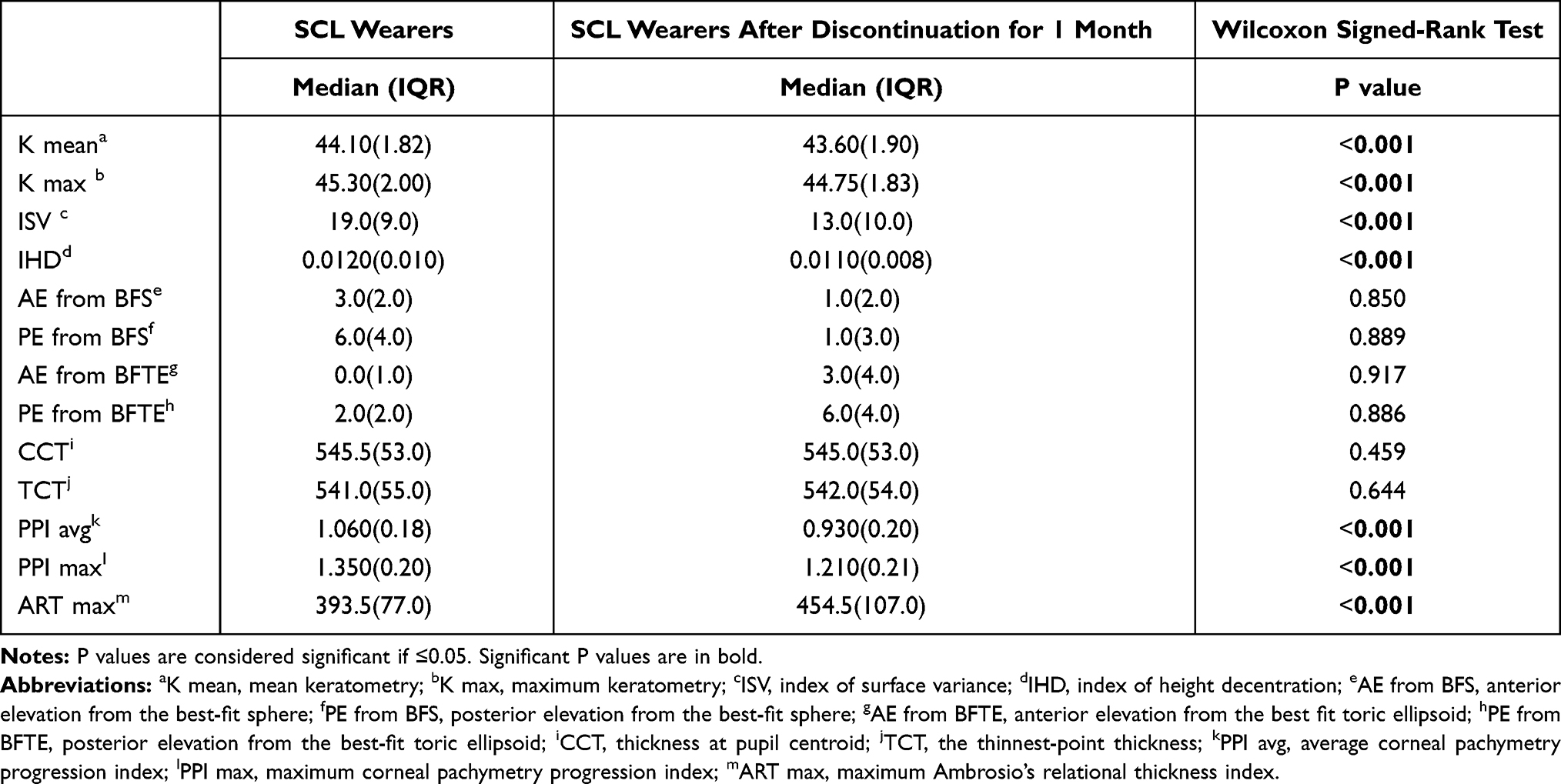 |
Table 3 Medians, Interquartile Ranges (IQR), and Comparisons of Various Pentacam HR Indices in Group 1 Before and After Soft Contact Lens (SCL) Discontinuation |
Discussion
SCL technology is advancing at a rapid pace, with new algorithms for fitting, and new designs and materials that are both safer and more comfortable,10,11 making SCL wear a common and convenient mode for optical correction of refractive errors. Considering that refractive surgical correction has many arising absolute and relative contraindications, SCL wear is still more desirable for people worried about the possible refractive surgery complications that have been described,12,13 or young adults who have not yet reached enough refractive stability to be subjected to refractive procedures.14
Given the common use of this refractive correction method, studies have addressed the possible impact of SCL wear on corneal morphology and biomechanics.15 Contact lens warpage commonly causes delays in planned refractive surgical corrections, with follow-up that may extend for long intervals, to elucidate the warpage effect and make sure that the detected corneal changes are not ectatic.7 Discontinuation of SCL wear before refractive procedures should eliminate their warpage effect, with variable discontinuation intervals considered in different studies. A range of two to four weeks is usually sufficient,9,16 although cases of warpage effect persisting for months have been documented.17,18
To the best of our knowledge, this study is the first to analyze various Pentacam HR topographic/tomographic indices in terms of their possible alterations or robustness (unchanged values) in response to SCL wear through a comparison with normal controls, and to validate the results by re-imaging the corneas after discontinuing SCL wear. Moreover, some of the evaluated parameters have not been previously assessed in terms of their possible alterations with regular SCL use (namely elevation values from BFTE, PPI avg, PPI max, and ART max).
This study aimed to identify the indices that can be relied upon for the corneal evaluation of SCL wearers, so as to propose benchmarks that can help reduce delays in planned refractive surgeries, and to provide a reliable way to assess corneal ectasia in SCL wearers, using robust parameters unaffected by SCL regular use. In other words, we identified a set of Pentacam parameters that the topographer can rely upon to screen the corneas of SCL wearers, without the need for an abstinence period from SCLs. Our results regarding the robustness of these indices were validated by the analysis after the discontinuation period.
While designing the study we took into consideration SCL material and wear duration. Interestingly, it has been reported that the duration of SCL wear may not affect the degree of warpage or the discontinuation period needed to abolish the corneal warpage effect.9 However, other studies revealed a relationship between corneal warpage and both duration of wear and lens material.19,20 Silicone hydrogel lenses were shown to lead to faster resolution of the warpage effect.16 Due to such conflicting study results, we avoided the possible confounding factors related to lens material and wear duration by choosing a cohort that was all using silicone hydrogel lenses, for which higher corneal stability upon long term use has been reported.21 The duration of lens wear for the recruited cohort was also limited to three to five years. We believe that these strict study criteria lend more credibility to the results.
The curvature indices that were evaluated in the present study, namely K mean, K max, ISV, and IHD, had significantly higher values in group 1, namely SCL wearers, reflecting increased corneal topographic steepening. This corneal steepening due to SCL wear has been often described in other studies,7 revealing that the curvature indices are volatile factors influenced by SCL wear. After the discontinuation period, all the curvature indices showed both statistically significant and clinically relevant decreases in group 1 eyes compared to their values before the abstinence period. This clearly implies that these changes are attributed to SCL wear and not to possible corneal ectasia. Curvature indices were previously reported as lacking specificity, being easily affected by many factors, in agreement with our results.22
Regarding the elevation-based indices, they were robust against SCL wear, showing no statistically significant differences compared with controls. Although the AE from BFS was the only elevation index that was significantly different between the two groups, the differences were obviously clinically irrelevant. In agreement with these results, the elevation indices were almost unchanged within the SCL wearers cohort after discontinuing lens wear for one month. This suggests that the elevation indices, which were previously reported as sensitive parameters for early ectasia detection,23 can be relied upon when screening the corneas of SCL wearers. In other words, altered elevation parameters in an SCL wearer should arise suspicion of corneal ectasia rather than warpage.
Three pachymetry-based indices (PPI avg, PPI max, and ART max) revealed statistically significant differences in SCL wearers compared with controls, and also showed significant changes within the SCL cohort after the discontinuation period. However, such differences can be considered clinically irrelevant, as all values were within the normal acceptable ranges and the changes were very narrow from the clinical aspect. Similar to the elevation indices, these pachymetric indices were previously described as sensitive parameters for corneal ectasia detection.24 However, these small, clinically irrelevant changes in the aforementioned pachymetric parameters could be due to the surface alterations of SCL warpage, evidenced by changes in curvature parameters, which can affect the pachymetric progression at different corneal rings from which the Pentacam device computes PPI avg, PPI max, and ART max.25
In the current study, we excluded all subjects younger than 18 years or older than 40 years, and also all eyes with hypermetropia or astigmatism of more than 1 diopter, since age and hypermetropia are two factors that have been previously reported to cause significant alterations in the Pentacam parameters,26,27 and astigmatism needs correction using toric contact lenses, that were not included in the study.
The strengths of the current study include the strict inclusion and exclusion criteria, the minimization of the effects of confounding factors, and the use of a single eye from each participant, to exclude the effect of inter-eye correlations which could compromise the validity of the statistical analysis.
Future studies should combine the evaluation of the robust indices we identified with the epithelial mapping of anterior segment optical coherence tomography, a recent and promising method for differentiating ectasia from similar conditions affecting the corneal surface.8 Moreover, longitudinal studies including larger cohorts may validate or contradict our study results regarding the detected changes in the indices.
In conclusion, we present an analysis of Pentacam HR indices in regular SCL wearers with three to five years of SCL use, within one hour of lens removal and after a discontinuation period of one month. All the evaluated elevation and pachymetric indices did not show any clinically relevant changes after SCL discontinuation. It is thus plausible to rely upon these indices while screening the SCL wearers for the existence of corneal ectasia without the need for a period of SCL discontinuation. As both elevation and pachymetric (as opposed to curvature) indices stood robust against SCL wear, their alterations in a SCL wearer should arise suspicion of corneal ectasia rather than lens-induced corneal warpage.
Code Availability
Not applicable.
Data Sharing Statement
Available from the corresponding author upon reasonable request.
Ethics Approval
The study adhered to the Tenets of the Declaration of Helsinki and was approved by the Ethical Committee of Ain Shams University.
Consent to Participate
All participants signed informed consents before participation in the study.
Consent for Publication
Not applicable.
Acknowledgment
We would like to thank Editage (www.editage.com) for English language editing.
Funding
There is no funding to report.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Williams KM, Bertelsen G, Cumberland P, et al. Increasing prevalence of myopia in Europe and the impact of education. Ophthalmology. 2015;122(7):1489–1497. doi:10.1016/j.ophtha.2015.03.018
2. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–618. doi:10.1136/bjophthalmol-2011-300539
3. Kanonidou E, Chatziralli IP, Konidaris V, Kanonidou C, Papazisis L. A comparative study of visual function of young myopic adults wearing contact lenses vs. spectacles. Cont Lens Anterior Eye. 2012;35(5):196–198. doi:10.1016/j.clae.2012.07.001
4. Price MO, Price DA, Bucci FA
5. Bohac M, Koncarevic M, Pasalic A, et al. Incidence and clinical characteristics of post lasik ectasia: a review of over 30,000 LASIK cases. Semin Ophthalmol. 2018;33(7–8):869–877. doi:10.1080/08820538.2018.1539183
6. Santhiago MR. Percent tissue altered and corneal ectasia. Curr Opin Ophthalmol. 2016;27(4):311–315. doi:10.1097/ICU.0000000000000276
7. González-Méijome JM, González-Pérez J, Cerviño A, Yebra-Pimentel E, Parafita AM. Changes in corneal structure with continuous wear of high-Dk soft contact lenses: a Pilot Study. Optom Vis Sci. 2003;80(6):440–446. doi:10.1097/00006324-200306000-00010
8. Schallhorn JM, Tang M, Li Y, Louie DJ, Chamberlain W, Huang D. Distinguishing between contact lens warpage and ectasia: usefulness of optical coherence tomography epithelial thickness mapping. J Cataract Refract Surg. 2017;43(1):60–66. doi:10.1016/j.jcrs.2016.10.019
9. Rayess Y, Arej N, Abdel Massih Y, Antoun J, Waked N. Influence of soft contact lens material on corneal warpage: prevalence and time to resolution. Can J Ophthalmol. 2018;53(2):135–138. doi:10.1016/j.jcjo.2017.09.003
10. Alipour F, Letafatnejad M, Beheshtnejad AH, et al. Corneal biomechanical findings in contact lens induced corneal warpage. J Ophthalmol. 2016;2016:5603763. doi:10.1155/2016/5603763
11. Visser ES, Wisse RP, Soeters N, Imhof SM, Van der Lelij A. Objective and subjective evaluation of the performance of medical contact lenses fitted using a contact lens selection algorithm. Cont Lens Anterior Eye. 2016;39(4):298–306. doi:10.1016/j.clae.2016.02.006
12. Caster AI, Friess DW, Schwendeman FJ. Incidence of epithelial ingrowth in primary and retreatment laser in situ keratomileusis. J Cataract Refract Surg. 2010;36(1):97–101. doi:10.1016/j.jcrs.2009.07.039
13. Ambrósio R, Dawson DG, Salomão M, Guerra FP, Caiado AL, Belin MW. Corneal ectasia after LASIK despite low preoperative risk: tomographic and biomechanical findings in the unoperated, stable, fellow eye. J Refract Surg. 2010;26(11):906–911. doi:10.3928/1081597X-20100428-02
14. Ambrósio R
15. Alipour F, Letafatnejad M, Beheshtnejad AH, et al. Lens induced corneal warpage. J Ophthalmol. 2016;2016:5603763.
16. Lloyd McKernan A, O’Dwyer V, Simo Mannion L. The influence of soft contact lens wear and two weeks lens cessation on corneal curvature. Cont Lens Anterior Eye. 2014;37(1):31–37. doi:10.1016/j.clae.2013.07.014
17. Tsai PS, Dowidar A, Naseri A, McLeod SD. Predicting time to refractive stability after discontinuation of rigid contact lens wear before refractive surgery. J Cataract Refract Surg. 2004;30(11):2290–2294. doi:10.1016/j.jcrs.2004.05.021
18. Wang X, McCulley JP, Bowman RW, Cavanagh HD. Time to resolution of contact lens-induced corneal warpage prior to refractive surgery. Eye Contact Lens. 2002;28(4):169–171.
19. Hashemi H, Firoozabadi MR, Mehravaran S, Gorouhi F. Corneal stability after discontinued soft contact lens wear. Cont Lens Anterior Eye. 2008;31(3):122–125. doi:10.1016/j.clae.2008.02.001
20. Del Águila-carrasco AJ, Domínguez-Vicent A, Pérez-Vives C, Ferrer-Blasco T, Montés-Micó R. Assessment of modifications in thickness, curvatures, and volume upon the cornea caused by disposable soft contact lens wear. Eur J Ophthalmol. 2015;25(5):385–390. doi:10.5301/ejo.5000592
21. Alba-Bueno F, Beltran-Masgoret A, Sanjuan C, Biarnés M, Marín J. Corneal shape changes induced by first and second generation silicone hydrogel contact lenses in daily wear. Cont Lens Anterior Eye. 2009;32(2):88–92. doi:10.1016/j.clae.2008.11.002
22. Belin MW, Ambrósio R. Corneal ectasia risk score: statistical validity and clinical relevance. J Refract Surg. 2010;26(4):238–240. doi:10.3928/1081597X-20100318-01
23. Muftuoglu O, Ayar O, Ozulken K, Ozyol E, Akıncı A. Posterior corneal elevation and back difference corneal elevation in diagnosing forme fruste keratoconus in the fellow eyes of unilateral keratoconus patients. J Cataract Refract Surg. 2013;39(9):1348–1357. doi:10.1016/j.jcrs.2013.03.023
24. Muftuoglu O, Ayar O, Hurmeric V, Orucoglu F, Kılıc I. Comparison of multimetric D index with keratometric, pachymetric, and posterior elevation parameters in diagnosing subclinical keratoconus in fellow eyes of asymmetric keratoconus patients. J Cataract Refract Surg. 2015;41(3):557–565. doi:10.1016/j.jcrs.2014.05.052
25. Huseynli S, Salgado-Borges J, Alio JL. Comparative evaluation of Scheimpflug tomography parameters between thin non-keratoconic, subclinical keratoconic, and mild keratoconic corneas. Eur J Ophthalmol. 2018;28(5):521–534. doi:10.1177/1120672118760146
26. Hashemi H, Beiranvand A, Khabazkhoob M, et al. Corneal elevation and keratoconus indices in a 40- to 64-year-old population, Shahroud Eye Study. J Curr Ophthalmol. 2015;27(3–4):92–98. doi:10.1016/j.joco.2015.10.007
27. Roshdy MM, Wahba SS, Elkitkat RS, Hakim AM, Fikry RR. Effect of age on pentacam keratoconus indices. J Ophthalmol. 2018;2018:2016564. doi:10.1155/2018/2016564
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.