")
Back to Journals » Research Reports in Clinical Cardiology » Volume 7
Review of cardiac implantable electronic device related infection
Authors Saliba É, Massie E, Sia YT
Received 18 July 2016
Accepted for publication 9 September 2016
Published 14 November 2016 Volume 2016:7 Pages 137—146
DOI https://doi.org/10.2147/RRCC.S75682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Kones
Émile Saliba,1 Emmanuelle Massie,2 Ying Tung Sia3
1Cardiology Department, Hôtel-Dieu de Montréal, Montréal, QC, Canada; 2Internal Medicine Department, Hôpital Saint Luc, Montréal, QC, Canada; 3Cardiology Department, Hôpital Pierre Boucher, Longueuil, QC, Canada
Abstract: Cardiac implantable electronic devices (CIEDs) are being used more and more often nowadays. Indications have grown, and access to implantation facilities has increased as well. These devices are often lifesaving, and they can be associated with many other benefits. However, as with any medical procedure, complications can occur. In fact, CIED infection is a prevalent complication that can cause high morbidity and can even lead to death. It is important that most clinicians be familiar with signs and symptoms associated with CIED infection as early diagnosis and treatment lead to better outcomes. Nonetheless, the prevention of such infections remains the cornerstone in the management of CIED-related infections. In this paper, we will review in detail the most significant risk factors that can lead to CIED infection. We will also explore the different available tools that can help decrease the incidence of this complication. In addition, we will summarize the different treatment modalities and the major prevention methods.
Keywords: cardiac implantable electronic device, infection, pacemaker, endocarditis
Introduction
Ever since the first pacemaker was implanted in 1960, the use of cardiac implantable electronic devices (CIEDs) has increased exponentially.1 Between 1997 and 2004, the use of permanent pacemaker and implanted cardiac defibrillator (ICD) has increased by 19% and 60%, respectively, in the USA. The arrival of the cardiac resynchronization therapy devices has also led to an increase in the use of CIED.1 As indications for CIED have increased, patients with more comorbidities have also become eligible for these therapies, often requiring long and complex procedures. Although these procedures are safe, complications can occur and can be very morbid. CIED infection is associated with increased mortality and morbidity as well as increased health care-related expenses.2 In fact, patients who develop CIED infection have increased long-term mortality even after successful treatment of the infection.3 Some data have shown a tendency of increased rate of CIED infection, especially in the first few months after installation.
There are multiple CIED on the market nowadays. Pacemakers and defibrillators are the most commonly installed devices and are used in the management of symptomatic bradycardia and prevention or treatment of ventricular tachycardia. These devices are composed of two major components: the pocket (contains the generator) and the leads. The different components of the device can be infected individually or concomitantly. CIED infections can be divided into two main entities: isolated pocket infection or lead infection. Pocket infection is usually limited to the tissue surrounding the generator and is usually not associated with any bacteremia. In contrast, lead infection can be associated with right-sided endocarditis and can cause bacteremia. In some cases, lead infection is not always associated with pocket infection, and it can occur in isolated manner. It is noteworthy to mention that some patients require lead changes and that old leads can remain in the patient if their removal is hard. This abandoned material can also get infected.
This paper reviews CIED infections and mainly focuses on risk factors and prevention of CIED infections. General therapeutic and diagnostic approaches are also outlined.
Epidemiology
The true incidence of CIED infection is difficult to establish due to the lack of national mandatory registries and the lack of reporting. The incidence also varies according to the type of device being installed and depends on other risk factors. In the era of prophylactic antibiotic use before insertion, the incidence of CIED infection can be as high as 6%.4 Implantable cardioverter defibrillator infection rate has recently been reported to be around 1.7%.5 As previously mentioned, the incidence of infection can vary a lot according to registries and studies. However, in a recent systematic review by Persson et al,6 CIED infection ranged between 0.2% and 3.7%, and it was the third leading cause of complication.
Over the last 16 years, ICD implantation increased by a staggering 504% compared to a 45% increase for pacemakers. In addition, the financial burden associated with those infections has also increased.7 According to Sohail et al,2 a CIED infection-related hospital admission could cost as much as $53,349. Infection of complex devices is usually associated with higher costs. Moreover, with the increasing prevalence of heart failure and with the aging of the population, it is expected that CIED implantations keep increasing. Thus, it is probable that CIED infection rate would also increase.
Most CIED infections only involve the pocket, and deeper infection such as endocarditis only occurs in around 10% of cases. However, some studies have reported the prevalence of lead vegetation to be as high as 40%.8,9 In addition, the risk of infection can increase up to tenfold if the patient is undergoing a lead replacement or a device upgrade.10 Early infection refers to cases occurring the first month following the procedure. Late infections occur between 1 and 12 months after implantation, and delayed infections occur after 12 months. In a study by Lekkerkerker et al,11 28% of patients had an early infection, 35% had a late infection, and 37% of patients presented with a delayed infection. Up to 24% of infections occurred 2 years after device installation.
CIED infections have been on the rise for the last few years. According to Voigt et al,12 CIED infections in the USA have risen by 12% between 2004 and 2006. As a consequence, hospitalization rates have increased by a staggering 57% and mortality rates doubled. This surge in CIED infection is secondary to increased patient comorbidities and to increased awareness and better diagnosis of this condition.1,12 Mortality associated with CIED varies greatly as it depends on the rapidity of diagnosis and on appropriate management. Mortality can be as high as 36% in patients admitted with a diagnosis of CIED infection.2 According to Sohail et al,2 mortality tends to be higher for many years even after the acute CIED infection was properly managed (absolute risk increase of 15% at 1 year and at 3 years).3
Risk factors
Device related
The risk of infection increases depending on which type of device is being installed and on the amount of leads. According to Durante-Mangoni et al,13 the presence of two leads or more is one of the most important risk factors of CIED infection. Early data did not support the fact that biventricular devices were associated with higher infection rates.11 However, a recent meta-analysis demonstrated that abdominal pockets, epicardial leads, presence of two or more leads, and dual-chamber systems are the main device-related risk factors for infection.14
Patient related
Patients with increased comorbidities are at increased risk of infection. Predisposing factors are immunosuppression, advanced age, cancer therapy, chronic kidney disease, diabetes mellitus, cirrhosis, active infection, and reintervention.13,15 A recent meta-analysis suggested that chronic obstructive pulmonary disease and male sex increased the risk of CIED infection.14 Altered defense mechanisms and increased procedure complexity accounted for this risk increase. In addition, these patients often required more frequent hospitalizations and could undergo invasive investigations, all which increase the risk of CIED infection.12
Chronic kidney disease patients requiring hemodialysis are particularly at increased risk of CIED infection, especially in the presence of a temporary dialysis catheter.16 Heart failure and other cardiac structural anomalies increase the complexity of the implantation procedure, and this is also associated with an increased rate of infection.15 CIED infection in patients requiring dialysis is associated with high short-term mortality and is more often accompanied by endocarditis.17
The use of anticoagulant increases the risk of pocket hematoma. This often leads to extra wound dressing changes and can sometimes require percutaneous drainage. Increased manipulation of the wound can lead to colonization by skin flora and increases healing time.11,13 Accordingly, higher infection rates are observed in anticoagulated patients. In the case of warfarin, its discontinuation is not recommended because bridging therapy with low-molecular-weight heparin increases pocket hematoma formation.18 Most other anticoagulants are stopped prior to the procedure.
Preprocedural fever (24 hours) and local skin disorders have also been associated with increased infection rates. In addition, a history of CIED infection also increases the rate of device infection.14 Withdrawal of indwelling central venous lines 24 hours preprocedure will also decrease the rate of infection.
Procedure related
Postoperative hematoma, reintervention for lead dislodgement, device replacement or revision, lack of temporary antibiotics prophylaxis, temporary pacing, operator inexperience, and procedure length all increase the risk of CIED infection.14 Generator replacement increases the risk of infection by 4% approximately, and lead replacement can increase the risk by around 15%.19 The higher infection rate in reintervention procedures is probably related to the altered defense mechanisms of scar tissue and to the increased healing time.11 In addition, increased tension in the pocket may lead to local tissue ischemia and necrosis, which can compromise the incision line and lead to wound dehiscence.20 These factors can lead to the growth of local bacteria and can increase the risk of infection. The implantation of biventricular resynchronization therapy seems to be the procedure at most risk of infection.21 CIED infection is significantly higher when they were installed by operators with low volume of implants.22
The use of prophylactic intravenous antibiotics should be routine before all CIED procedures. A large double-blinded placebo-controlled study by de Oliveira et al23 demonstrated the superiority of a single intravenous dose of 1 g of cefazolin when compared to placebo. The study was terminated prematurely by the ethics committee due to the benefits of prophylactic antibiotics. In patients at high risk of infection, the use of an antibiotic (minocycline and rifampin)-coated membrane during implantation greatly reduces the risk of infection.24,25 Several observational trials as well as a randomized placebo-controlled trial have shown that the use of various topical antibiotics after the procedure showed no benefit on the rate of CIED infection.26,27
The REPLACE registry, has demonstrated that at 6-month follow-up, hospitals with high CIED infection rates had sicker patients and lower overall procedural volume.19
Clinical manifestations
Most CIED infections usually manifest in the first 6 months after implantation.28 In total, 28% of those patients developed the infection in the first month after implantation, 35% between 1 and 12 months, and 24% of patients developed the infection 24 months after the implantation.11
In general, pocket infections are much more common than lead infection and endocarditis. They typically develop in the first month following implantation, but late infections can also be seen. Early infections are usually associated with local symptoms such as pocket erythema, swelling, pain, and warmth. In contrast, skin erosion is more frequent with late infection, and it can be the only manifestation. When skin erosion is present, infection is certain. Systemic symptoms such as fever and chills can be seen in early and late infections, but they are not a common manifestation. The infection can also extend to the leads, and vegetations can develop on the tricuspid valve.29–31
Even though lead infection is not easily diagnosed based on clinical evidence, it can be seen in up to 40% of patients who present with pocket infection. In general, the intracardiac portion of the lead is more often infected than the transvenous portion.32 Symptoms vary according to the extent of the disease. Fever and chills are usually present, and some patients can present with sepsis and can even be in septic shock.1 Vegetations can also invade the tricuspid valve and cause tricuspid regurgitation. Pulmonary complications such as pneumonia, emboli, and abscesses can be secondary to septic emboli.33 In rare cases, left-sided vegetations can also develop.
Occult bacteremia can also be an infrequent presentation of CIED infection. This can occur without any other manifestations around the pocket. For example, in patients with a non-Staphylococcus aureus Gram-positive cocci bacteremia, the CIED infection rate was 30%. Less frequently, patients can present with relapsing bacteremia even when initial investigations showed no signs of pocket or lead infection.34 The use of additional imaging modalities, especially a functional one, can help identify the exact location of infection.
Some authors have tried to create risk scores and to find which factors allow better determination of CIED infection. For example, in the PREDICT-SAB study, the findings suggest that the presence of a permanent pacemaker, more than one device-related procedure, and duration of S. aureus bacteremia ≥4 days are independent predictors of CIED infection in patients presenting with S. aureus bacteremia. In contrast, patients who did not have any of those risk factors and who did not have signs of pocket infection had a low risk of CIED infection.35
Diagnosis
The diagnosis of a CIED infection can be challenging in some cases. Pocket infections are diagnosed based on the clinical presentation, but lead involvement requires additional diagnostic exams to rule out. Given that lead involvement is associated with higher mortality and morbidity, the use of imaging modalities such as echocardiography is essential in the evaluation of those patients.36
Echocardiography is of utmost value to rule out lead infection or endocarditis. Transthoracic echocardiography is a good initial test to screen for lead involvement but is not sensitive enough to rule it out. Thus, most experts recommend the use of transesophageal echocardiography (TEE) as the gold standard exam to detect vegetations.1 Some authors even recommend the use of intracardiac echocardiography, which has a sensitivity of 100% and a specificity of 82%.37 TEE will help better identify masses or vegetations on the leads; however, blood cultures and inflammatory markers should be closely followed to make sure that the nature of such masses is infectious.13
DUKE criteria are sometimes used to diagnose CIED-related endocarditis, but their sensitivity and specificity are relatively low in this context.38 Acute inflammatory markers such as sedimentation rate and C-reactive protein can be elevated, and they can be associated with leukocytosis. If white blood cell count is high, it can be followed to assess appropriateness of therapy.30 Surrogate markers for bacterial infections such as procalcitonin have not been evaluated in the diagnosis of CIED infection.
When doubt persists, nuclear medicine imaging modalities can help increased the diagnostic yield. Radiotraced white blood cell scintigraphy can detect CIED infection and has a sensitivity of 94%.38 Fluorine-18 marked fluorodeoxyglucose positron emission tomography has an even better diagnostic yield, but it is not widely available,39 and its combined use with the DUKE criteria can produce an even higher yield.40 It has also been shown to detect infection related to left ventricular assist devices.41
According to the latest American guidelines, two sets of blood cultures should always be drawn before antibiotics administration.1 If antibiotics have already been started, two to four sets of blood cultures should be drawn after an adequate washout interval. When endocarditis is present, all blood cultures drawn before antibiotic therapy usually show growth of the same pathogen. Although unusual, only one set of blood cultures can be positive, and the use of additional diagnostic exams is essential to distinguish between infection and contaminants. If the device is removed, the generator and the leads should be cultured to confirm the diagnosis.30 Percutaneous aspiration of the infected site is not recommended as colonizing pathogens and skin flora could contaminate this specimen.
In some cases, a definite diagnosis is still hard to obtain. Some authors suggest sonication of the extracted device and of blood cultures. In fact, sonication has been shown to be more sensitive than swab cultures in identifying the culprit pathogen. This usually implies the placement of the extracted device in a Ringer’s solution, which is then vortexed and cultivated. In one study, sonication permitted the identification of significant bacterial growth in 54% of cases compared to 20% for device swabs.42
Microbiology
As shown in Table S1, the majority of CIED infections are caused by S. aureus and Staphylococcus epidermidis infections.43 Methicillin-resistant staphlycocci can also infect CIED, but the prevalence of such infections is quite variable. Up to 20% of patients present with non-staphylococci-related CIED infections such as Corynebacterium, Propionibacterium, Peptococcus, Gram-negative rods (especially Pseudomonas aeruginosa), enterococci, and fungi.43 In addition, 10% of infections can be polymicrobial, and 10% can remain without having a clear pathogen identified.13 Early infections are typically associated with staphylococci species.11
Management
Empirical antibiotic therapy should have an appropriate biofilm penetration rate, a good bactericidal activity, and should be suitable for bacteremia as well. At all times, antibiotics should be tailored according to local bacteria resistance and sensitivity patterns. In general, empirical antibiotics should have adequate coverage of Gram-positive cocci as well as Gram-negative bacteria.43 The duration of appropriate therapy is outlined in Table S1. Antibiotic therapy should always be individualized and should be given according to the latest guidelines. The Infectious Diseases Society of America provide additional information on this topic.1
In most cases, complete device retrieval is necessary in addition to intravenous antibiotics. Most guidelines recommend removal of the generator and all leads even if the infection is only limited to the pocket. This recommendation also includes abandoned leads and all foreign material. In one study, 71.4% of patients with retained material showed recurrence.44 Devices should be removed as soon as possible especially if the patient is displaying signs of sepsis or shock. Attention should be given to patients who are permanently paced to avoid potentially disastrous consequences of removing chronotropic input. Installation of temporary pacemakers should be avoided if possible, since it could get infected, especially if bacteremia is present. However, optimal timing of device removal is quite controversial. It is usually recommended that the patient receives a few days of intravenous antibiotics before removal. This reduces the risk of complications such as septic emboli, and it also reduces the risk of recurrence of infection. Given that some patients might require temporary pacemakers, the administration of antibiotics will reduce the risk of persistent infection.
Newly installed leads are easier to remove than older ones due to the lack of endothelialization. In some patients, complete device extraction can be hazardous because of advanced age and increased comorbidities. Risk of device extraction increases with older leads and with complex systems. According to heart rhythm society, vegetations larger than 2 cm indicate surgical removal of the leads, thus it is required to have a TEE before device removal.45 Lead extraction-associated risk decreases when the extraction is performed in a high volume center.46
In select rare cases, such as limited infection and high patient comorbidities, the generator should be removed and replaced as long as the pathogen is of low virulence and aggressive debridement is performed.13 Lopez et al47 reported the case of five patients in whom complete device extraction was not possible, and so conservative therapy was chosen. All patients received a new generator (soaked in a gentamycin and vancomycin solution) and had oral antibiotics on discharge. At 2 years follow-up, none of the patients had recurrence of the infection. Thus, it is possible to consider a conservative approach in some selected patients.
In general, if the infection is limited to the pocket, antibiotics should be given for at least 2 weeks and at least 7 days after device extraction.1 Therapy should be extended for 3 weeks if there is bacteremia and for 6 weeks if endocarditis is present.1 For left-sided endocarditis, treatment should be administered according to local guidelines.
Device reimplantation
Once the CIED is removed, it is always judicious to review the indication for the implantation of a new one since a significant portion of patients might no longer meet the indication for a CIED. As previously mentioned, the administration of antibiotics will reduce the risk of infection of the new device. In all cases, two separate sets of blood cultures have to be negative before implanting the new device. Optimal timing of this reimplantation is controversial. Some authors suggest waiting 7 days in the case of pocket infections and 14 days in the case of bacteremia. However, this depends on many factors, since some patients are pacemaker dependent for example.30 Most experts recommend waiting at least 2 weeks before installing any permanent devices.30
In patients who only need defibrillators and in whom no pacing is needed, the use of a subcutaneous implanted defibrillator should be considered as it reduces the risk of subsequent infection.48 Subcutaneous ICD is effective in treating ventricular tachycardia and has been studied in many trials.49 As a matter of fact, this type of device is associated with very low rates of infection, and if infection was to occur, the extraction of this device is much easier than the extraction of transvenous devices.49 Subcutaneous ICDs have been shown to have lower rates of infection even in patients in whom a previous transvenous CIED was explanted for infection.48 In patients with high risk of infection, the use of epicardial leads can also be considered to reduce the risk of systemic infection.30 Leadless pacemakers could also eventually be one of the options.50
CIED infection prevention
To reduce the incidence of CIED infections, prevention is of utmost importance. CIED installation or upgrade should only be done in patients with a clear indication for it. Ideally, a pacemaker or a defibrillator should be installed once patients are in a stable condition and in those who do not show any signs of local or systemic infection. Elective procedures should be rescheduled if the patient has a central catheter installed.
CIED implantation should always be done in a sterile environment and according to usual surgical sterilization guidelines. New sterilization techniques have been shown to reduce infection rates. For example, the “bundled skin antiseptic preparation” showed superiority compared to standard sterilization techniques, but it requires more time and more resources.51 Good hemostasis throughout the procedure is also beneficial as the risk of hematoma formation will be reduced, and consequently the risk of infection.30 In contrast, other sterilization techniques have been associated with increased risk of infection. In the REPLACE registry, there was some doubt on a possible increased rate of infection associated with povidone iodine compared to chlorhexidine alcohol. The difference between those two substances was especially significant in establishments with high rates of infection.52 However, another study found no statistically significant difference in the rate of CIED infection when either chlorhexidine alcohol or povidone iodine was used.52
The most frequently administered prophylactic antibiotics are second-generation cephalosporins. As previously mentioned, the use of prophylactic antibiotics has been clearly established and should be routinely done. This has been demonstrated in several trials53 including a large randomized one.23 However, the optimal timing of antibiotic use remains controversial. Most surgical references recommend that antibiotics be given 30–60 minutes before the procedure.54 In a recent systematic review, the administration of a prophylactic antibiotic 1 hour before the CIED installation was shown to be effective at reducing surgical site infections.55 It remains unclear if antibiotics effective against methicillin-resistant S. aureus (MRSA) should be administered to everyone, thus antibiotics should be chosen according to local bacterial prevalence.30
The latest advancement in CIED infection prevention is the use of antibiotic envelopes. TYRX™ (Medtronic, Dublin, Republic of Ireland) is a newly developed envelope that releases minocycline and rifampin in the generator pocket after the implantation of the device. This envelope has been shown to reduce the growth of several pathogens.56 In addition, it has been shown to reduce biofilm production and to eliminate staphylococci growth.57 This envelope is easily installed and does not render CIED implantation more difficult or cause more complications. In a study by Bloom et al,25 the use of this antibacterial envelope was associated with an early infection incidence reduction of 0.5%, and these same results were reproduced in other trials.24 The use of such envelopes in patients at high risk of infection seems to be beneficial and cost-effective. Some authors even suggest that the use of such envelopes becomes routine standard care.58 Additional clinical trials are currently underway to evaluate the long-term infection risk reduction associated with antimicrobial envelopes.
Implementation of those recommendations will help reduce the global burden of CIED infections. For example, an infection control protocol was introduced at a tertiary referral central in the UK, and it was associated with a 54% reduction of CIED infection.59 This protocol consisted of thirteen different steps. All patients were screened for MRSA, and if MRSA carriage was detected, topical skin eradication was performed with nasal mupirocin and 4% chlorhexidine. Signs of infection or sepsis 24 hours were an indication for procedure deferral. Intravenous antibiotic prophylaxis was administered to everyone (flucloxacillin 1 g or clarithromycin 500 mg combined with gentamycin 1.5 mg/kg) 30 minutes before the procedure. Operators had a minimum scrubbing time of 2 minutes, and they were required to double glove during draping, and the outer glove was removed prior to skin incision. Sterilization was performed with a solution of 2% chlorhexidine gluconate with 70% isopropyl alcohol. Local hair was removed using an electric razor, and all diabetic patients had their glycemia lowered to <11.0 mmol/L. Cutting diathermy at 40 W was used after incision, and antibacterial-coated sutures were used for the wound. All intravenous accesses were closed systems, and they were installed in a sterile manner. Bair hugger was used to control the temperature in patients undergoing complex procedures. Finally, wound dressings were left intact for 3 days following installation. Implementation of such measures was found to be cost-effective and easy to put in place.59 This strategy for infection control has also been proven to be safe and cost-effective in the context of other interventions.60
Conclusion
The use of CIED is expected to increase in the next few years, and patients with more comorbidity will become eligible for them as well. Thus, precautions should be taken to avoid an increase of infections. To do so, it is very important to recognize the risk factors associated with them and to learn how to prevent them by working on the many factors that can influence the risk of infection.
Disclosure
The authors report no conflicts of interest in this work.
References
Baddour LM, Epstein AE, Erickson CC, et al. Update on cardiovascular implantable electronic device infections and their management: a scientific statement from the American Heart Association. Circulation. 2010;121(3):458–477. | ||
Sohail MR, Henrikson CA, Braid-Forbes MJ, Forbes KF, Lerner DJ. Mortality and cost associated with cardiovascular implantable electronic device infections. Arch Intern Med. 2011;171(20):1821–1828. | ||
Rizwan Sohail M, Henrikson CA, Jo Braid-Forbes M, Forbes KF, Lerner DJ. Increased long-term mortality in patients with cardiovascular implantable electronic device infections. Pacing Clin Electrophysiol. 2015;38(2):231–239. | ||
Eggimann P, Waldvogel F. Pacemaker and defibrillator infections. In: Waldvogel FA, Bisno AL, editors. Infections Associated with Indwelling Medical Devices. 3rd ed. Washington, DC: American Society of Microbiology Press; 2000:247–264. | ||
Prutkin JM, Reynolds MR, Bao H, et al. Rates of and factors associated with infection in 200 909 Medicare implantable cardioverter-defibrillator implants: results from the National Cardiovascular Data Registry. Circulation. 2014;130(13):1037–1043. | ||
Persson R, Earley A, Garlitski AC, Balk EM, Uhlig K. Adverse events following implantable cardioverter defibrillator implantation: a systematic review. J Interv Card Electrophysiol. 2014;40(2):191–205. | ||
Greenspon AJ, Patel JD, Lau E, et al. 16-year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States 1993 to 2008. J Am Coll Cardiol. 2011;58(10):1001–1006. | ||
Arber N, Pras E, Copperman Y, et al. Pacemaker endocarditis. Report of 44 cases and review of the literature. Medicine (Baltimore). 1994;73(6):299–305. | ||
Golzio PG, Fanelli AL, Vinci M, et al. Lead vegetations in patients with local and systemic cardiac device infections: prevalence, risk factors, and therapeutic effects. Europace. 2013;15(1):89–100. | ||
Tarakji KG, Wilkoff BL. Cardiac implantable electronic device infections: facts, current practice, and the unanswered questions. Curr Infect Dis Rep. 2014;16(9):425. | ||
Lekkerkerker JC, van Nieuwkoop C, Trines SA, et al. Risk factors and time delay associated with cardiac device infections: Leiden device registry. Heart. 2009;95(9):715–720. | ||
Voigt A, Shalaby A, Saba S. Continued rise in rates of cardiovascular implantable electronic device infections in the United States: temporal trends and causative insights. Pacing Clin Electrophysiol. 2010;33(4):414–419. | ||
Durante-Mangoni E, Mattucci I, Agrusta F, Tripodi MF, Utili R. Current trends in the management of cardiac implantable electronic device (CIED) infections. Intern Emerg Med. 2013;8(6):465–476. | ||
Polyzos KA, Konstantelias AA, Falagas ME. Risk factors for cardiac implantable electronic device infection: a systematic review and meta-analysis. Europace. 2015;17(5):767–777. | ||
Herce B, Nazeyrollas P, Lesaffre F, et al. Risk factors for infection of implantable cardiac devices: data from a registry of 2496 patients. Europace. 2013;15(1):66–70. | ||
Saad TF, Hentschel DM, Koplan B, et al. Cardiovascular implantable electronic device leads in CKD and ESRD patients: review and recommendations for practice. Semin Dial. 2013;26(1):114–123. | ||
Hickson LJ, Gooden JY, Le KY, et al. Clinical presentation and outcomes of cardiovascular implantable electronic device infections in hemodialysis patients. Am J Kidney Dis. 2014;64(1):104–110. | ||
Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation. N Engl J Med. 2013;368(22):2084–2093. | ||
Uslan DZ, Gleva MJ, Warren DK, et al. Cardiovascular implantable electronic device replacement infections and prevention: results from the REPLACE Registry. Pacing Clin Electrophysiol. 2012;35(1):81–87. | ||
Korantzopoulos P, Sideris S, Dilaveris P, Gatzoulis K, Goudevenos JA. Infection control in implantation of cardiac implantable electronic devices: current evidence, controversial points, and unresolved issues. Europace. 2016;18(4):473–478. | ||
Palmisano P, Accogli M, Zaccaria M, et al. Rate, causes, and impact on patient outcome of implantable device complications requiring surgical revision: large population survey from two centres in Italy. Europace. 2013;15(4):531–540. | ||
Al-Khatib SM, Lucas FL, Jollis JG, Malenka DJ, Wennberg DE. The relation between patients’ outcomes and the volume of cardioverter-defibrillator implantation procedures performed by physicians treating Medicare beneficiaries. J Am Coll Cardiol. 2005;46(8):1536–1540. | ||
de Oliveira JC, Martinelli M, Nishioka SA, et al. Efficacy of antibiotic prophylaxis before the implantation of pacemakers and cardioverter-defibrillators: results of a large, prospective, randomized, double-blinded, placebo-controlled trial. Circ Arrhythm Electrophysiol. 2009;2(1):29–34. | ||
Kolek MJ, Dresen WF, Wells QS, Ellis CR. Use of an antibacterial envelope is associated with reduced cardiac implantable electronic device infections in high-risk patients. Pacing Clin Electrophysiol. 2013;36(3):354–361. | ||
Bloom HL, Constantin L, Dan D, et al. Implantation success and infection in cardiovascular implantable electronic device procedures utilizing an antibacterial envelope. Pacing Clin Electrophysiol. 2011;34(2):133–142. | ||
Khalighi K, Aung TT, Elmi F. The role of prophylaxis topical antibiotics in cardiac device implantation. Pacing Clin Electrophysiol. 2014;37(3):304–311. | ||
Da Costa A, Tulane C, Dauphinot V, et al. Preoperative skin antiseptics for prevention of cardiac implantable electronic device infections: a historical-controlled interventional trial comparing aqueous against alcoholic povidone-iodine solutions. Europace. 2015;17(7):1092–1098. | ||
Lin YS, Hung SP, Chen PR, et al. Risk factors influencing complications of cardiac implantable electronic device implantation: infection, pneumothorax and heart perforation: a nationwide population-based cohort study. Medicine. 2014;93(27):e213. | ||
Welch M, Uslan DZ, Greenspon AJ, et al. Variability in clinical features of early versus late cardiovascular implantable electronic device pocket infections. Pacing Clin Electrophysiol. 2014;37(8):955–962. | ||
Nof E, Epstein LM. Complications of cardiac implants: handling device infections. Eur Heart J. 2013;34(3):229–236. | ||
Chua JD, Wilkoff BL, Lee I, Juratli N, Longworth DL, Gordon SM. Diagnosis and management of infections involving implantable electrophysiologic cardiac devices. Ann Intern Med. 2000;133(8):604–608. | ||
Klug D, Lacroix D, Savoye C, et al. Systemic infection related to endocarditis on pacemaker leads: clinical presentation and management. Circulation. 1997;95(8):2098–2107. | ||
Padeletti L, Mascioli G, Perini AP, et al. Critical appraisal of cardiac implantable electronic devices: complications and management. Med Devices (Auckl). 2011;4:157–167. | ||
Madhavan M, Sohail MR, Friedman PA, et al. Outcomes in patients with cardiovascular implantable electronic devices and bacteremia caused by Gram-positive cocci other than Staphylococcus aureus. Circ Arrhythm Electrophysiol. 2010;3(6):639–645. | ||
Sohail MR, Palraj BR, Khalid S, et al. Predicting risk of endovascular device infection in patients with Staphylococcus aureus bacteremia (PREDICT-SAB). Circ Arrhythm Electrophysiol. 2015;8(1):137–144. | ||
Kim DH, Tate J, Dresen WF, et al. Cardiac implanted electronic device-related infective endocarditis: clinical features, management, and outcomes of 80 consecutive patients. Pacing Clin Electrophysiol. 2014;37(8):978–985. | ||
Narducci ML, Pelargonio G, Russo E, et al. Usefulness of intracardiac echocardiography for the diagnosis of cardiovascular implantable electronic device-related endocarditis. J Am Coll Cardiol. 2013;61(13):1398–1405. | ||
Erba PA, Sollini M, Conti U, et al. Radiolabeled WBC scintigraphy in the diagnostic workup of patients with suspected device-related infections. JACC Cardiovasc Imaging. 2013;6(10):1075–1086. | ||
Sarrazin JF, Philippon F, Tessier M, et al. Usefulness of fluorine-18 positron emission tomography/computed tomography for identification of cardiovascular implantable electronic device infections. J Am Coll Cardiol. 2012;59(18):1616–1625. | ||
Pizzi MN, Roque A, Fernandez-Hidalgo N, et al. Improving the diagnosis of infective endocarditis in prosthetic valves and intracardiac devices with 18F-fluordeoxyglucose positron emission tomography/computed tomography angiography: initial results at an infective endocarditis referral center. Circulation. 2015;132(12):1113–1126. | ||
Fujino T, Higo T, Tanoue Y, Ide T. FDG-PET/CT for driveline infection in a patient with implantable left ventricular assist device. Eur Heart J Cardiovasc Imaging. 2016;17(1):23. | ||
Nagpal A, Patel R, Greenwood-Quaintance KE, et al. Usefulness of sonication of cardiovascular implantable electronic devices to enhance microbial detection. Am J Cardiol. 2015;115(7):912–917. | ||
Viola GM, Awan LL, Darouiche RO. Nonstaphylococcal infections of cardiac implantable electronic devices. Circulation. 2010;121(19):2085–2091. | ||
Pichlmaier M, Knigina L, Kutschka I, et al. Complete removal as a routine treatment for any cardiovascular implantable electronic device-associated infection. J Thorac Cardiovasc Surg. 2011;142(6):1482–1490. | ||
Wilkoff BL, Love CJ, Byrd CL, et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: this document was endorsed by the American Heart Association (AHA). Heart Rhythm. 2009;6(7):1085–1104. | ||
Di Monaco A, Pelargonio G, Narducci ML, et al. Safety of transvenous lead extraction according to centre volume: a systematic review and meta-analysis. Europace. 2014;16(10):1496–1507. | ||
Lopez JA. Conservative management of infected pacemaker and implantable defibrillator sites with a closed antimicrobial irrigation system. Europace. 2013;15(4):541–545. | ||
Boersma L, Burke MC, Neuzil P, et al. Infection and mortality after implantation of a subcutaneous ICD after transvenous ICD extraction. Heart Rhythm. 2015;13(1):157–164. | ||
Bongiorni MG, Viani S, Zucchelli G, et al. Subcutaneous implantable cardiac defibrillators: indications and limitations. Curr Heart Fail Rep. 2015;12(1):79–86. | ||
Arkles J, Cooper J. The emerging roles of leadless devices. Curr Treat Options Cardiovasc Med. 2016;18(2):14. | ||
Chen HC, Chen MC, Chen YL, Tsai TH, Pan KL, Lin YS. Bundled preparation of skin antisepsis decreases the risk of cardiac implantable electronic device-related infection. Europace. 2016;18(6):858–867. | ||
Qintar M, Zardkoohi O, Hammadah M, et al. The impact of changing antiseptic skin preparation agent used for cardiac implantable electronic device (CIED) procedures on the risk of infection. Pacing Clin Electrophysiol. 2015;38(2):240–246. | ||
Da Costa A, Kirkorian G, Cucherat M, et al. Antibiotic prophylaxis for permanent pacemaker implantation: a meta-analysis. Circulation. 1998;97(18):1796–1801. | ||
Weber WP, Marti WR, Zwahlen M, et al. The timing of surgical antimicrobial prophylaxis. Ann Surg. 2008;247:918–926. | ||
Darouiche R, Mosier M, Voigt J. Antibiotics and antiseptics to prevent infection in cardiac rhythm management device implantation surgery. Pacing Clin Electrophysiol. 2012;35(11):1348–1360. | ||
Hansen LK, Brown M, Johnson D, Palme li DF, Love C, Darouiche R. In vivo model of human pathogen infection and demonstration of efficacy by an antimicrobial pouch for pacing devices. Pacing Clin Electrophysiol. 2009;32(7):898–907. | ||
Kolek MJ, Patel NJ, Clair WK, et al. Efficacy of a bio-absorbable antibacterial envelope to prevent cardiac implantable electronic device infections in high-risk subjects. J Cardiovasc Electrophysiol. 2015;26(10):1111–1116. | ||
Shariff N, Eby E, Adelstein E, et al. Health and economic outcomes associated with use of an antimicrobial envelope as a standard of care for cardiac implantable electronic device implantation. J Cardiovasc Electrophysiol. 2015;26(7):783–789. | ||
Ahsan SY, Saberwal B, Lambiase PD, et al. A simple infection-control protocol to reduce serious cardiac device infections. Europace. 2014;16(10):1482–1489. | ||
Forbes SS, Stephen WJ, Harper WL, et al. Implementation of evidence-based practices for surgical site infection prophylaxis: results of a pre- and postintervention study. J Am Coll Surg. 2008;207(3):336–341. |
Supplementary material
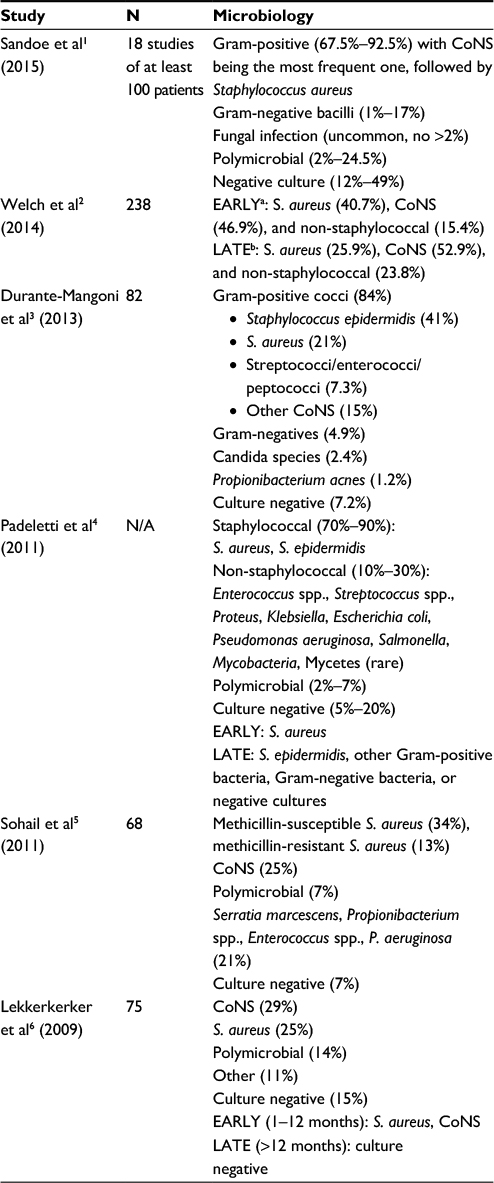 | Table S1 Pathogens associated with CIED infections Notes: a0–12 months after implantation; b>12 months after implantation. Abbreviations: CIED, cardiac implantable electronic device; CoNS, coagulase-negative Staphylococcus; N/A, not available. |
References
Sandoe JA, Barlow G, Chambers JB, et al. Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Report of a joint Working Party project on behalf of the British Society for Antimicrobial Chemotherapy (BSAC, host organization), British Heart Rhythm Society (BHRS), British Cardiovascular Society (BCS), British Heart Valve Society (BHVS) and British Society for Echocardiography (BSE). J Antimicrob Chemother. 2015;70(2):325–359. | ||
Welch M, Uslan DZ, Greenspon AJ, et al. Variability in clinical features of early versus late cardiovascular implantable electronic device pocket infections. Pacing Clin Electrophysiol. 2014;37(8):955–962. | ||
Durante-Mangoni E, Mattucci I, Agrusta F, Tripodi MF, Utili R. Current trends in the management of cardiac implantable electronic device (CIED) infections. Intern Emerg Med. 2013;8(6):465–476. | ||
Padeletti L, Mascioli G, Perini AP, et al. Critical appraisal of cardiac implantable electronic devices: complications and management. Med Devices (Auckl). 2011;4:157–167. | ||
Sohail MR, Henrikson CA, Braid-Forbes MJ, Forbes KF, Lerner DJ. Mortality and cost associated with cardiovascular implantable electronic device infections. Arch Intern Med. 2011;171(20):1821–1828. | ||
Lekkerkerker JC, van Nieuwkoop C, Trines SA, et al. Risk factors and time delay associated with cardiac device infections: Leiden device registry. Heart. 2009;95(9):715–720. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.