")
Back to Journals » International Journal of Women's Health » Volume 15
Review of Breast Abscess Cases at a Tertiary Hospital in Addis Ababa, Ethiopia
Authors Suga Y, Kuehn T, W/Ammanuel G, Knfe G , Teklewold B
Received 12 October 2022
Accepted for publication 13 March 2023
Published 24 March 2023 Volume 2023:15 Pages 433—442
DOI https://doi.org/10.2147/IJWH.S391686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Yisihak Suga,1 Thorsten Kuehn,2 Gessesse W/Ammanuel,1 Goytom Knfe,1 Berhanetsehay Teklewold1
1Department of Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Gynecological Oncology and Gynecologic Surgery, Klinikum Esslingen, Esslingen, Germany
Correspondence: Yisihak Suga, Tel +251913470780, Email [email protected]; [email protected]
Background: Breast abscess is a prevalent cause of morbidity in women occurring in 0.4% to 11% of patients after mastitis. The majority are benign, but worrisome etiologies such as inflammatory cancer and concomitant immune-compromising diseases should be addressed when a non-lactating patient presents with a breast abscess. The problem is high among women in developing countries (1). The purpose of this study is to assess the magnitude, clinical presentation, and treatment of breast abscess patients at a tertiary hospital.
Methodology: A descriptive cross-sectional study was conducted on all patients treated for breast abscesses from September 2015 to August 2020. A retrospective review of the clinical records was performed to collect data on sociodemographic, clinical, and management data using a data extraction form. The collected data were then cleaned and entered into SPSS for analysis.
Results: Two hundred and nine patients were included in this study over 5 years and lactational breast abscess (LBA) is more prevalent,182 (87.1%) than non-lactational breast abscess (NLBA), 27 (12.9%). Bilateral breast abscesses occurred in 16 (7.7%) patients. Patients presented at a median duration of 11 days and had been breastfeeding for 2 or more months. A spontaneously ruptured abscess was detected in, 30 (14.4%) of the patients. Comorbidities identified include diabetes mellitus (DM) in, 24 (11.5%), Hypertension in, 7 (3.3%), HIV in, 5 (2.4%) of patients. All women were treated with Incision and Drainage and had a median volume of 60 mL of pus drained. Following surgery, all patients were given ceftriaxone in the immediate post-operative days and either cloxacillin,167 (80.3%), or Augmentin,41 (19.7%) antibiotics p on discharge. Follow-up data were available for 201 (96.1%) patients and the recurrence rate was 5.8%.
Conclusions and Recommendations: Lactational breast abscesses are more common than non-lactational breast abscesses, particularly in primiparas. DM is the most common comorbidity in non-lactational breast abscesses and health-seeking behavior should be improved given the delayed presentation.
Keywords: breast abscess, lactational, non-lactational, magnitude, clinical presentation
Introduction
A breast abscess is a localized collection of pus within the breast. BA can be classified into lactational (LBA) and non-lactational breast abscesses (NLBA).1 LBA occurs in the setting of a young primiparous lactating or expectant mother as a complication of lactational mastitis while non-lactational breast abscess occurs due to multiple factors including DM, smoking, and underlying structural breast lesions like duct ectasia.2,3 The most commonly isolated organism in infectious mastitis is Staphylococcus aureus (S. aureus) although streptococcus and anaerobic flora can also be identified in NLBA.4
The major risk factors reported for LBA are milk stasis and infection and it is likely that bacteria (often originating from the mouth of the infant) gain entry via cracks or fissures in the nipple surface.5–7 NLBA is categorized according to the location into central (sub-areolar) and peripheral. Central or sub-areolar non-lactational breast abscess has a known association with squamous metaplasia of the lactiferous duct epithelium, duct obstruction, duct ectasia, and periductal mastitis Smoking and diabetes mellitus are significant risk factors for periductal mastitis and non-lactational abscesses.4,9 On the other hand, peripheral nonpuerperal breast abscesses are less common and are often associated with an underlying condition such as diabetes, rheumatoid arthritis, steroid treatment, or trauma.8
Treatment of breast abscess entails drainage of the abscess either surgically or with aspiration. Traditionally antibiotics are prescribed for all patients but in LBA this issue is controversial. The current recommendation is aspiration with ultrasound guidance with multiple episodes usually required to achieve resolution of the abscess.10,11 Patients require further workup for co-morbid conditions. Histopathology is done in the case of NLBA and recurrences in LBA.4
The prevalence of mastitis globally was reported as 1–10% with the highest incidence in the first few weeks postpartum, while LBA occurs in 3–11% of those with mastitis with a reported incidence of 0.1–3% in breastfeeding women.4 NLBA is a rare clinical entity accounting for less than 5% of breast abscess cases.8 The underlying predisposing condition: periductal mastitis is said to be responsible for 1–2% of all symptomatic breast conditions.9,12 In a retrospective study conducted at our institution in 2019, breast abscess was found to account for nearly 3% of 3062 emergency admissions placing it as the 9th top general surgical admission.13
Even though breast abscess is one of the most prevalent emergency diagnoses, there is a scarcity of studies describing the clinical characteristics and epidemiology of breast abscess in Ethiopia, and no study was reported from our institution. Hence, this study will address the frequency, clinical presentation, treatment provided, biopsy, and culture findings in breast abscess patients presenting to St. Paul’s Hospital Millennium Medical College.
Methods
Study Design
The survey was conducted at St. Paul’s Hospital Millennium Medical College (SPHMMC) in Addis Ababa, which is the second-largest multi-specialty tertiary care teaching hospital in Ethiopia. The hospital has been giving medical services to patients from Addis Ababa and all over the country with a regular catchment of 5 million people for more than 50 years with an emphasis on the underserved population.11 This descriptive cross-sectional survey was conducted from September 1, 2015- to August 31, 2020, and all patients who were treated for breast abscesses in St Paul’s Hospital Millennium Medical College during this period were included. Patients whose charts provided incomplete data were excluded from the study.
Data Collection
From the emergency operation room logbooks, 280 medical record numbers were discovered but only 209 of these records were retrieved from the medical records room because of lost charts. A data extraction format having the specified data variables was prepared and data were collected by medical practitioners after orientation about the study and the form. The data collection format included information on the age, sex, education level, history of trauma, presence of comorbidity, side, and site of breast abscess, duration of symptoms, organism grown in culture and susceptibility, biopsy finding, age of the child, incision type, amount of abscess drained, antibiotics choice, and recurrence.
Data Processing and Analysis
The processing began by checking the gathered data for accuracy and completeness. Each completed questionnaire was assigned a unique code and entered into Epi Info version 3.5.1 (CDC, Atlanta, GA, USA) and exported to SPSS version 26 (IBM, Armonk, NY, USA) for further analysis. Results are presented as frequency distributions and cross-tabulations. Continuous variables are presented as median and interquartile ranges and categorical variables are presented as frequency and percentages.
Ethical Considerations
An ethical clearance letter was obtained from St. Paul’s Hospital Millennium Medical College Institutional ethics review board and permission from the Department of surgery. The review board checks if any breach of confidentiality before approval of the proposal. There was no patient identifier included in the data collection form. Every precaution was taken to protect the privacy of research subjects and the confidentiality of their personal information in accordance with the declaration Helsinki.
Result
Sociodemographic Characteristics
A total of 280 medical records numbers of patients with breast abscesses were identified out of which 209 were retrieved and included in this study. Table 1 shows the sociodemographic characteristics of the study population. Females made up the whole patient population in this investigation with a median age of 25 years (range of 15–79). The most common site from which patients came seeking treatment were Addis Ababa (49.8%, n = 104) and Oromia regions. Only 129 (61.7%) of the 209 patients had their educational level reported. Nearly 22% had completed elementary school, 24.4% had completed secondary school, and 12.9% had completed higher-level education (Table 1).
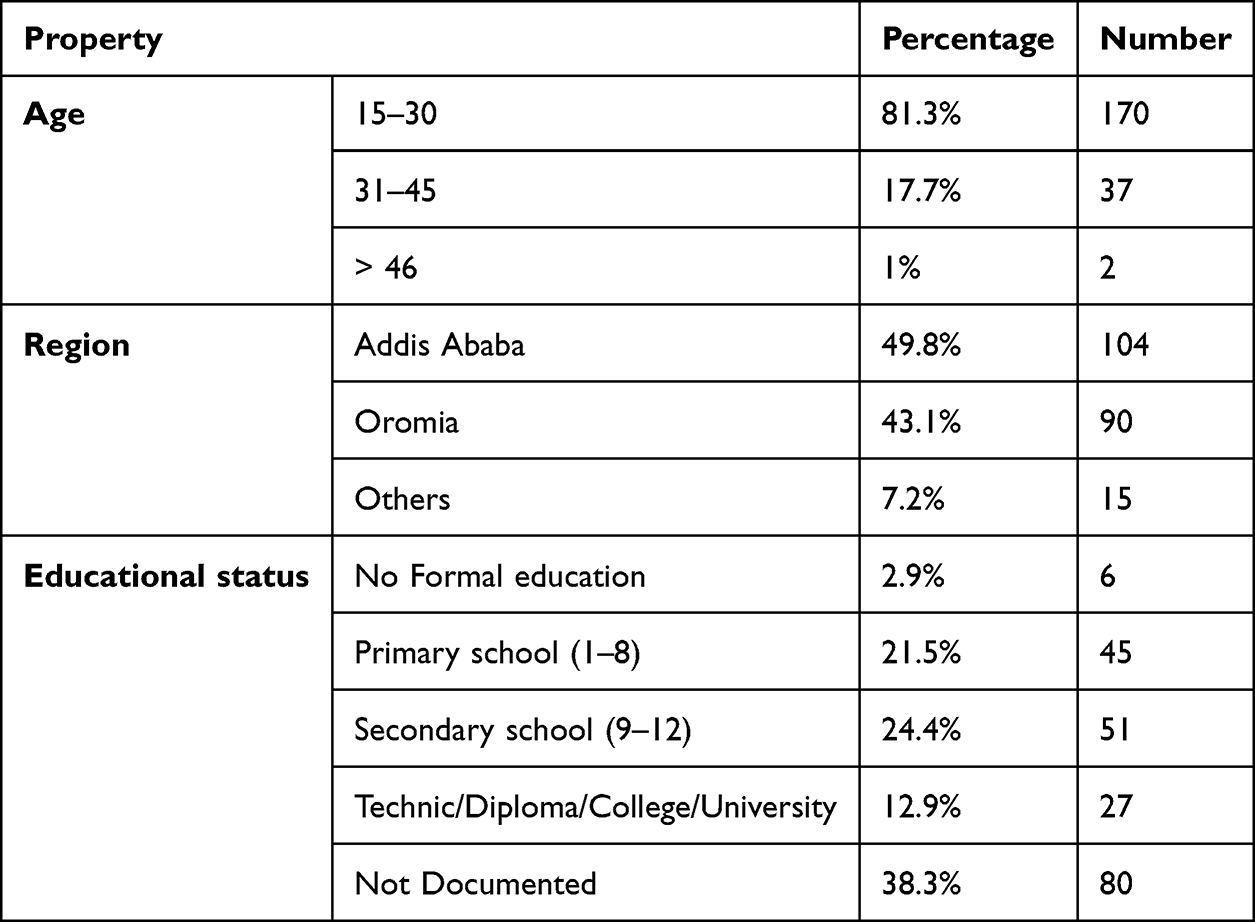 |
Table 1 Sociodemographic Characteristics of Breast Abscess Cases in a Tertiary Hospital in Addis Ababa, Ethiopia, 2020 |
Pattern of Presentation
All of the patients were referred to our facility. Before referral, 147 (70.3%) of patients received prior therapy whereas 24.4% were treatment-naive. Nearly 75% (110) of those who received treatment received antibiotics, while, 26 (17.7%) received antibiotics and antipain. Left, right, and bilateral breast abscesses occurred in, 99 (47.4%), 94 (45.0%), and,16 (7.7%) patients, respectively. The left outer quadrant (LOQ) was the most prevalent quadrant in unilateral abscesses, accounting for, 49 (25.4%) of cases. Most patients presented after a median of 11 days of symptoms.
One hundred eighty-two patients (87.1%) were LBA, whereas 12.9% (27) were NLBA. There were 9 pregnant patients treated for LBA and four of the pregnant patients who acquired LBA were in their second trimester, while five were in their third trimester. There were 48.6% of patients who were primiparous mothers and the median age of the infant among LBA patients was 2 months. On presentation, 38.3% (80) of patients showed fluctuant edema, whereas 78.5% (164) had erythema overlying the swelling. A burst abscess was seen in 14.4% (30) of the patients (Table 2).
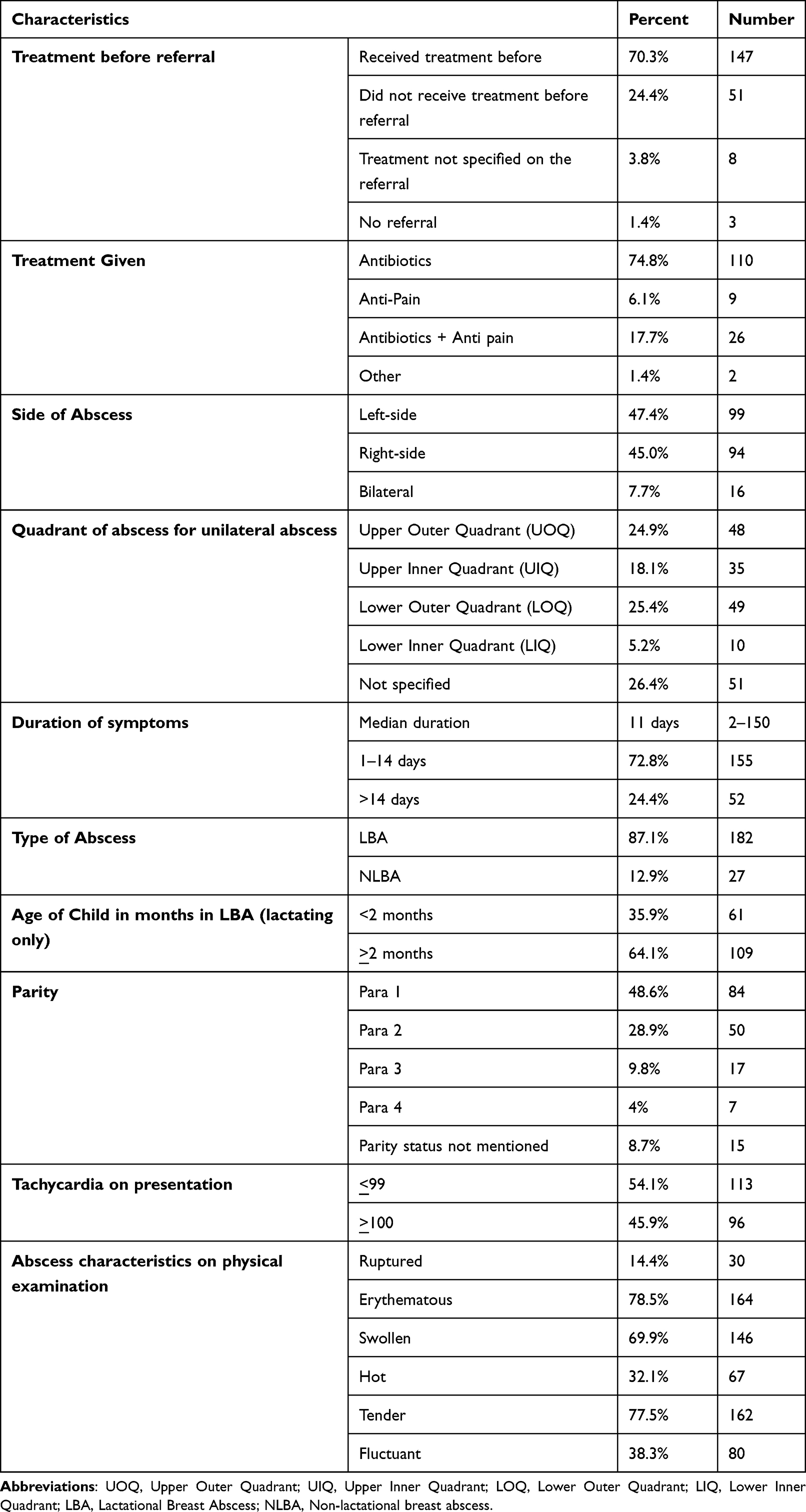 |
Table 2 Clinical Features of Patients on Presentation of Breast Abscess Cases in a Tertiary Hospital in Addis Ababa, Ethiopia, 2020 |
Preoperative Investigation of Patients
Leukocytosis of >10,000 was found in 75.6% (158) of patients with a complete blood profile. Ultrasound was performed on 66% (138) of the patients, with abscesses being reported in 81.9% (113) of them and were managed as breast abscesses based on clinical judgment. Preoperative fine needle aspiration cytology (FNAC) was performed in 13.9% (29) of patients, with abscess being the most prevalent finding at 37.9%11 (Table 3).
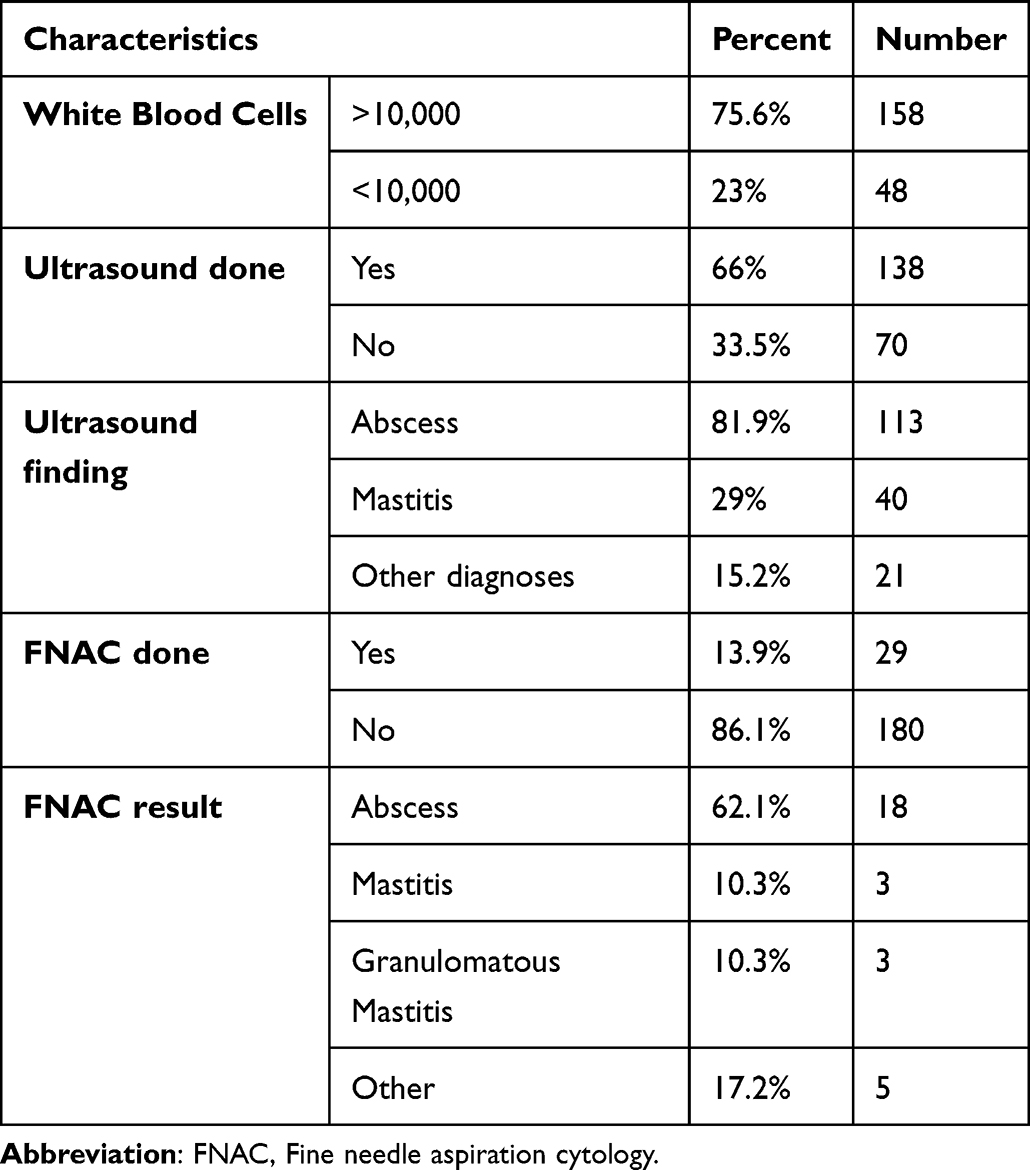 |
Table 3 Results of Investigations Sent for Breast Abscess Cases Who Received Treatment in a Tertiary Hospital in Addis Ababa, Ethiopia |
Risks Present in Patients
History of trauma to the site was reported by 4.8% of patients who presented with Breast abscess and 18.6% (39) had comorbidities. Diabetes Mellitus (DM) was present in 11.5%24 of patients with breast abscesses but in 48.1% of the non-lactational variant. Human immunodeficiency Virus (HIV) was identified in 2.4%5 of patients (Table 4).
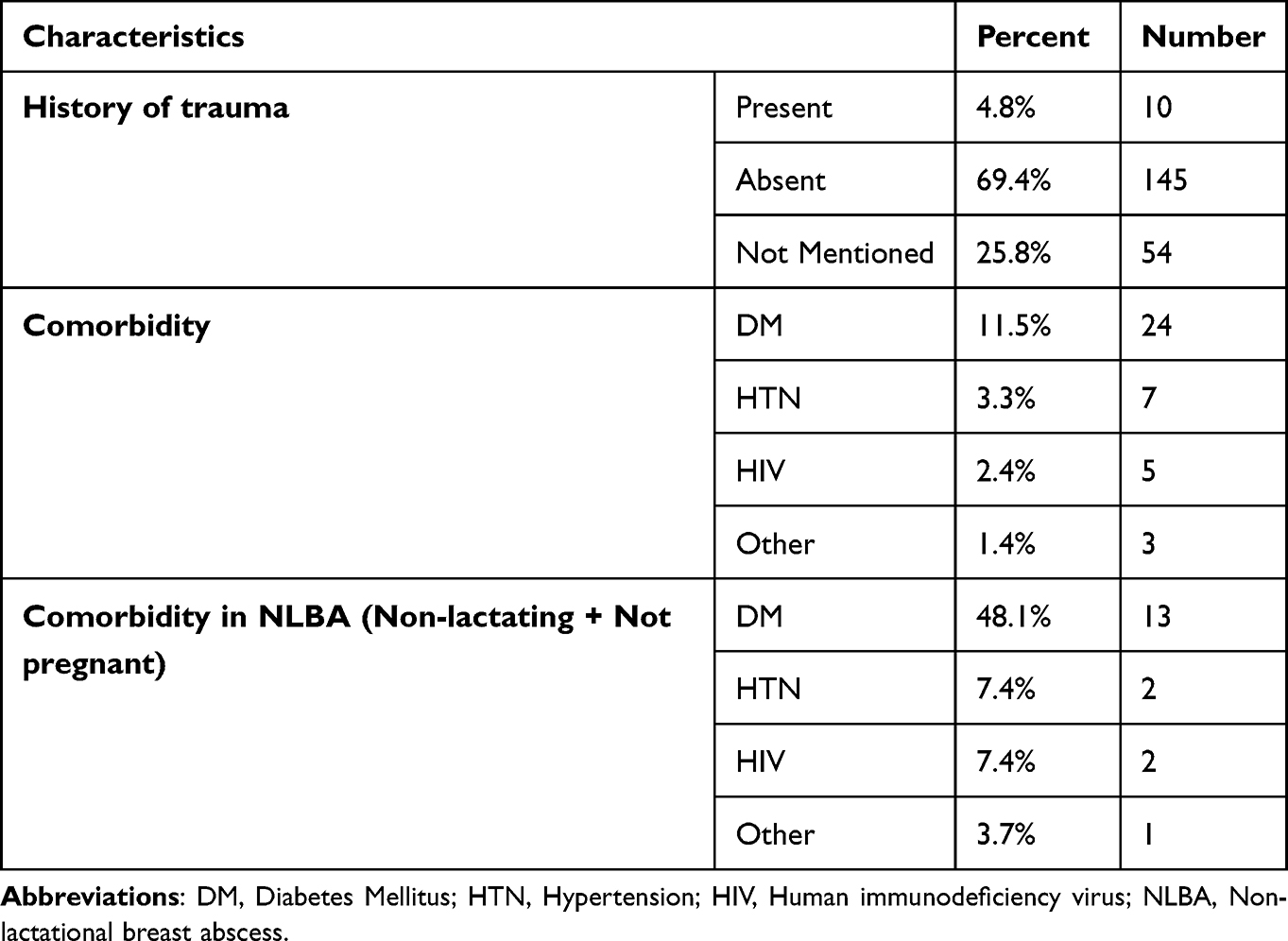 |
Table 4 Risk Factors Identified in Breast Abscess Cases Who Received Treatment in a Tertiary Hospital in Addis Ababa, Ethiopia |
Treatment Given
Incision and drainage were done for all patients. The type of incision most commonly used was peri-areolar (29.7%) incision and the majority were performed under light sedation or general anesthesia. The median volume of the abscess drained was 60 mL for LBA and 50 mL for NLBA. Intravenous antibiotics were prescribed for 98.1% of patients on immediate postoperative days with Ceftriaxone being the most often prescribed antibiotic. Out of the 27 patients treated for NLBA, one patient was given per-oral (PO) cloxacillin with metronidazole, 15 patients cloxacillin alone, and 11 individuals were given Augmentin. The drained pus was submitted for analysis in 19.1% of patients, and a biopsy specimen was sent in 24.9% (52) of patients. Overall, 44.2%23 of patients for whom a biopsy was sent received the results of the biopsy. An abscess was the most prevalent finding in the biopsies taken (60.9%, 14). Out of 27 patients treated for NLBA, 51.9%14 had a biopsy sent, but only 35.7% percent had collected the result.4 All of the patients returned for follow up and 96.2% (201) of those that returned had completed their follow-up and were discharged. A recurrence of the abscess occurred in 5.8%12 of patients, with all recurrences occurring in LBA at a median time of 1 month and all were managed with repeat incision and drainage (Table 5).
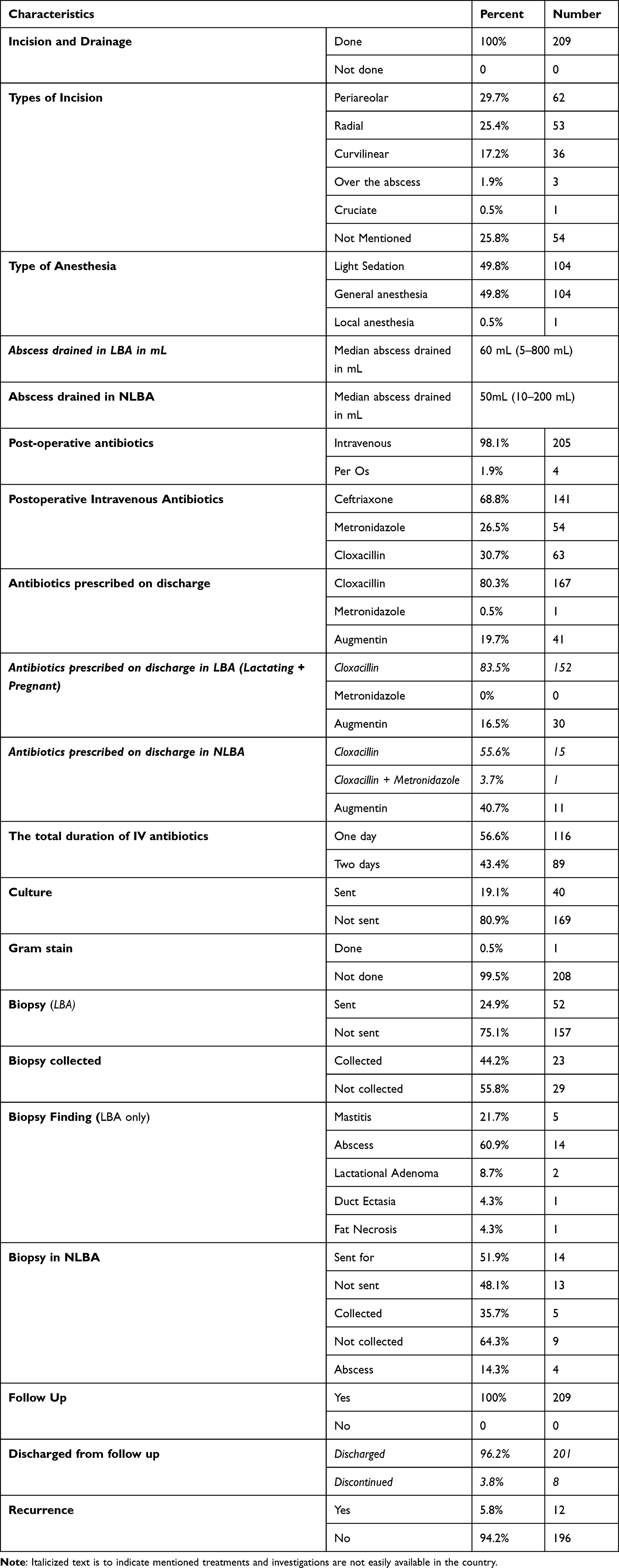 |
Table 5 The Details of the Treatment Provided for Breast Abscess Cases in a Tertiary Hospital in Addis Ababa, Ethiopia |
Discussion
Breast abscesses are a frequent challenge in the general surgical practice in Ethiopia. This study showed that LBA is more common than NLBA similar to a Nigerian study which showed a prevalence of 95%.14 However, a lower proportion of LBA of 50.7%, 76%, and 30% was found in the studies reported from Kenya,15 Saudi Arabia,16 and the United Kingdom (UK),17 respectively. The considerable difference in the ratio of LBA and NLBA between the UK and our study could be attributed to the greater smoking prevalence in the UK while the low number of LBA could be due to correct breastfeeding practices that clients are made aware of.
The left breast was affected more frequently and bilateral breast abscesses occurred in about 8% of the cases. Likewise, the left-side predominance of breast abscesses was reported by studies from Turkey and Kenya. Bilaterality is observed less frequently occurring in 3% of the cases.15,18 In terms of classification of the lesion sites, the breast is divided into four quadrants. The most common site for breast abscesses was the LOQ in 25.4% of patients which is in contrast to previous literature supporting the frequent location of breast abscesses in the upper outer quadrant.6 This could be owing to the fact that the quadrant of the abscess was not specified in 26.4% of patients operated on.
Most patients with LBA presented after 2 months of breastfeeding in accordance with existing studies19 but there was delayed presentation of patients after the onset of symptoms with a median duration of symptoms of 11 days as in other developing countries.20 Earlier healthcare-seeking patterns with a mean duration of symptoms of 8.6 days were reported5 and this difference might be explained by the poor health-seeking behavior and the tendency to try different home remedies and herbal medications before coming to healthcare in our setup. These might also be the reason why a considerable percentage of our patients are coming with a ruptured breast abscess.
The clinical presentation of the patients included hot, swollen, tender, erythematous, and fluctuant swelling similar to the previous literature.9,21 History of trauma was elicited in 4.8% of patients, which is similar to an earlier literature by Ekland et al where trauma was elicited in 6% of patients. The cause of trauma could not be determined by our study but this should be looked into and advice and counseling should be given as appropriate.20 Comorbidities detected included DM, HIV, and HTN. In our study, diabetes was identified in 48.1% of patients with NLBA which was higher compared to the study done in Australia where it was identified in 23% of patients with NLBA.10 In a USA study done by Rizzo et al, 72% of patients treated with NLBA had DM, and most had poor glycemic control.9 Hence, patients with diabetes mellitus should be given appropriate health education like treating minor injuries, seeking health care early, achieving good glucose control, and avoiding bad habits like smoking.
Surgical incision and drainage were done for all patients which is in contrast to the recent recommendation to treat breast abscess patients having normal overlying skin with imaging-guided needle aspiration.2,5,10,22 However, this might be because minimal invasive intervention requires patients’ cooperation and understanding for continued follow-up and adequate access to point-of-care ultrasound machines which is difficult to achieve in our patient population. The study conducted by Dixon et al found that only 2–35 mL of the abscess was drained in patients with NLBA.12 However, the median amount of abscess drained in this study was 60 and 50 mL in LBA and NLBA, respectively, which could be owing to the delayed presentation and referral to a hospital with established large-volume abscesses.
In this study, postoperative PO antibiotics were prescribed for all patients and the most commonly prescribed medication was Cloxacillin in 80.3% of patients which was in contrast to other studies where Augmentin was the predominant antibiotic.15,23 Cloxacillin alone was prescribed for more than half of our NLBA patients similar to another study done by Saboo et al where cloxacillin was the preferred antibiotic coverage and was prescribed alone in 44.7% of patients.10 This practice is not supported by literature as anaerobic coverage is required in patients with non-lactational breast abscesses.
Even though a biopsy should be sent for all NLBA cases, it was sent in nearly 50% of patients with NLBA and the biopsy result was not either collected or not seen by the physician before the patient was discharged from follow-up. It is also crucial to send specimens for culture and sensitivity testing in patients treated for a breast abscess to give bacteria-specific treatment and extrapolate the antibiogram data to the community level to change case management. However, only 19% of the patients had their abscess specimens sent for culture and sensitivity tests, and none of their results were collected which is much lower than studies reporting that 80% to 100% of specimens are sent for analysis.24
The recurrence rate of 5.8% in our study is similar to the study done by Mwenda et al where 8% of patients developed recurrence. The recurrence in NLBA in our study was none while in a study done by Mwenda et al it was 13.5%. The recurrence of LBA in our study was 6.6% while lower recurrence rates were reported by other studies ranging from 2.6% to 4%.15,18 The recurrence could be related to inadequate treatment, early closure of the cavity, and inadequate wound care provided by local health centers upon discharge.
Limitations of the Study
The limitations of the study are that it was a retrospective study and relied on the data from medical records with nearly 25% of charts being missed, and was conducted in a single tertiary center where more complicated cases are managed.
Conclusion and Recommendations
A lactational breast abscess is more common than a non-lactational breast abscess and was found to be common in primiparous women. Diabetes Mellitus is the most common comorbidity in NLBA. All patients with breast abscesses were treated with incision and drainage and most did not have culture and sensitivity tests and biopsy results. In addition, there was an improper antibiotic choice, particularly for anaerobic coverage. Hence, an updated institutional management guideline should be implemented to standardize the current practices related to the treatment of breast abscesses not supported by the literature.
Ethical Approval
Ethical approval was obtained from the review board of the college. The patient’s records were kept confidential.
Acknowledgments
We acknowledge the Health Care Workers and support staff of SPHMMC for helping us during the data collection of this survey.
Funding
No funds were received for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bharat A, Gao F, Aft RL, Gillanders WE, Eberlein TJ, Margenthaler JA. Predictors of primary breast abscesses and recurrence. World J Surg. 2009;33(12):2582–2586. doi:10.1007/s00268-009-0170-8
2. Trop I, Dugas A, David J, et al. Breast abscesses: evidence-based algorithms for diagnosis, management, and follow-up. Radiographics. 2011;31(6):1683–1699. doi:10.1148/rg.316115521
3. Tabe-Tanyi AC, Ngoin M. An assessment of the rate and predisposing factors to the development of breast abscess among lactating mothers in the Batibo health district, northwest region, Cameroon: a case study. S Am J Med. 2014;2:1.
4. Boakes E, Woods A, Johnson N, Kadoglou N. Breast infection: a review of diagnosis and management practices. Eur J Breast Health. 2018;14(3):136–143. doi:10.5152/ejbh.2018.3871
5. Dener C, Inan A. Breast abscesses in lactating women. World J Surg. 2003;27(2):130–133. doi:10.1007/s00268-002-6563-6
6. Marchant DJ. Inflammation of the breast. Obstet Gynecol Clin North Am. 2002;19(1):90–102.
7. Inch S, von Xylander S, Savage F. Mastitis Causes and Management. World Health Organzation; 2000.
8. Akhator A. Nonpuerperal breast abscesses [Internet]. Available from: https://www.researchgate.net/publication/341441585.
9. Rizzo M, Peng L, Frisch A, Jurado M, Umpierrez G. Breast abscesses in nonlactating women with diabetes: clinical features and outcome. Am J Med Sci. 2009;338(2):123–126. doi:10.1097/MAJ.0b013e3181a9d0d3
10. Saboo A, Bennett I. Trends in non-lactation breast abscesses in a tertiary hospital setting. ANZ J Surg. 2018;88(7–8):739–744. doi:10.1111/ans.14146
11. Rao R, Ludwig K, Bailey L, et al. Select choices in benign breast disease: an initiative of the American Society of Breast Surgeons for the American Board of Internal Medicine choosing Wisely® Campaign. Ann Surg Oncol. 2018;25(10):2795–2800. doi:10.1245/s10434-018-6584-5
12. Dixon JM, Khan LR. Treatment of breast infection. BMJ. 2011;342(7795):484–489. doi:10.1136/bmj.d396
13. Argaw F, Bekele Muleta M, Tsehay A, et al. Pattern of general surgical and urologic admissions at St. Paul’s hospital millennium medical college. Ethiop Med J. 2019;57(1):19.
14. Efem SE. Breast abscesses in Nigeria: lactational versus non-lactational. J R Coll Surg Edinb. 1995;40(1):25–27.
15. Mwenda AS, Wasike R. Breast abscess management and the role of post incisional antibiotics. Ann Afr Surg. 2016;13(2):63–66. doi:10.4314/aas.v13i2.7
16. Abdelhadi MSA, Facs HA, Bukharie A. Breast infections in nonlactating women. J Family Community Med. 2022;12(3):133.
17. Bundred NJ, Dover MS, Coley S, et al. Breast abscesses and cigarette smoking. Br J Surg. 1992;79(1):58–59. doi:10.1002/bjs.1800790121
18. Eryilmaz R, Sahin M, Tekelioglu MH, Daldal E. Management of lactational breast abscesses. Breast. 2005;14(5):375–379. doi:10.1016/j.breast.2004.12.001
19. Lukassek J, Ignatov A, Faerber J, Costa SD, Eggemann H. Puerperal mastitis in the past decade: results of a single institution analysis. Arch Gynecol Obstet. 2019;300(6):1637–1644. doi:10.1007/s00404-019-05333-3
20. Elagili F, Abdullah N, Fong L, Pei T. Aspiration of breast abscess under ultrasound guidance: outcome obtained and factors affecting success. Asian J Surg. 2007;30(1):40–44. doi:10.1016/S1015-9584(09)60126-3
21. David Ekland MA, Michael Zeigler LG, Sam houston F. Abscess in the nonlactating breast. Arch Surg. 1973;107:398–401. doi:10.1001/archsurg.1973.01350210034011
22. Chandika AB, Gakwaya AM, Kiguli-Malwadde E, Chalya PL. Ultrasound guided needle aspiration versus surgical drainage in the management of breast abscesses: a Ugandan experience. BMC Res Notes. 2012;5. doi:10.1186/1756-0500-5-12
23. Fahrni M, Schwarz EI, Stadlmann S, Singer G, Hauser N, Kubik-Huch RA. Breast abscesses: diagnosis, treatment and outcome. Breast Care. 2012;7(1):32–38. doi:10.1159/000336547
24. Munj DS. Role of diagnostics in management of breast infection – a retrospective study from North Goa District Hospital. J Med Sci Clin Res. 2021;9(01). doi:10.18535/jmscr/v9i1.36
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.