")
Back to Journals » Vascular Health and Risk Management » Volume 15
Retrospective study of cardiovascular disease risk factors among a cohort of combat veterans with lower limb amputation
Authors Bhatnagar V , Richard E, Melcer T , Walker J, Galarneau M
Received 6 May 2019
Accepted for publication 7 August 2019
Published 19 September 2019 Volume 2019:15 Pages 409—418
DOI https://doi.org/10.2147/VHRM.S212729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Vibha Bhatnagar,1,2 Erin Richard,1,2 Ted Melcer,3 Jay Walker,4 Michael Galarneau3
1Department of Family and Preventive Medicine, University of California San Diego, La Jolla, CA, USA; 2US Department of Veterans Affairs, San Diego Healthcare System, San Diego, CA, USA; 3Medical Modeling, Simulation and Mission Support Department, Naval Health Research Center, San Diego, CA, USA; 4Leidos, San Diego, CA, USA
Correspondence: Vibha Bhatnagar
Department of Family and Preventive Medicine, University of California San Diego 9500 Gilman Drive, MC 0725, La Jolla, CA 92093, USA
Tel +1 858 822 1233
Fax +1 858 534 4642
Email [email protected]
Introduction: Previous studies have shown that veterans with lower limb amputation have a higher risk for cardiovascular disease (CVD) compared with population-based controls. American veterans who have served in Iraq and Afghanistan with lower limb amputation may be at a similarly higher risk.
Patients and methods: The Navel Health Research Center (NHRC) maintains the Expeditionary Medical Encounter Database (EMED) of military personnel who have sustained combat limb amputation or serious limb injury during the conflicts in Iraq and Afghanistan. Department of Veterans Affairs data from 2003 to April 2015 was used to analyze CVD risk factors in this cohort. Veterans with either unilateral (n=442) or bilateral (n=146) lower limb amputation were compared to those with serious lower limb trauma without amputation (n=184). Multivariate regression was used to measure associations between lower limb amputation and CVD risk factors over an average of 8 years of follow-up. Outcomes included mean arterial pressure (MAP), low-density lipoprotein, high-density lipoprotein (HDL), and serum triglycerides (TG).
Results: Compared with the limb injury group, those with unilateral lower limb amputation had significantly lower HDL (p<0.05) and higher TG (p<0.05). Those with bilateral lower limb amputation had significantly higher MAP (p<0.05), lower HDL (p<0.01), and higher TG (p<0.001). The prevalence of metabolic syndrome, defined as type 2 diabetes or a constellation of blood pressure and lipid changes consistent with metabolic syndrome, was 8.7%, 14.9%, and 21.9% for limb injury, unilateral amputation, and bilateral amputation groups, respectively. Veterans with bilateral lower limb amputation had a 2.25-increased odds ratio (95% confidence interval 1.19–5.05) of type 2 diabetes or blood pressure and lipid changes consistent with metabolic syndrome compared to those with limb injury.
Conclusions: Results suggest that veterans with lower limb amputation have a higher risk for metabolic syndrome. Primary care interventions to manage weight, blood pressure, and lipid levels are fundamental in order to reduce cardiac risk in this relatively young cohort.
Keywords: limb amputation, combat injury, blood pressure, cardiovascular disease, dyslipidemia, insulin resistance, expeditionary medical encounter database
Introduction
Thousands of traumatic limb injuries and over 1,000 lower limb amputations have resulted from Operation Enduring Freedom and Operation Iraqi Freedom.1 These veterans with limb amputations are relatively young and have complex comorbidity2 and a high rate of disability,1,3 requiring specialized types of care (eg, rehabilitation, prosthetics, and mental health support), lifelong primary care, and disease prevention.4–8 Studies of World War II veterans documented relatively high rates of obesity, hypertension, and glucose intolerance following combat-related amputations.9,10 As a result of an increased prevalence of these cardiovascular disease (CVD) risk factors, veterans with lower limb amputation have an increased risk of cardiovascular morbidity and mortality compared with population-based controls.7,8,10 However, little previous research has investigated CVD risk factors following combat-related amputations in the Iraq and Afghanistan conflicts.
The present study was designed to describe CVD risk factors in a cohort of young veterans with combat-related injuries resulting in either unilateral or bilateral lower limb amputation while serving in Iran and/or Afghanistan. To partially control for factors related to the physical and emotional stress of combat injury, the control group included veterans with serious combat-related lower limb injury without amputation. All patients were identified in the Naval Health Research Center (NHRC) Expeditionary Medical Encounter Database (EMED)11 and, similar to our prior work, we linked members of the cohort identified in military databases to health data from the Department of Veterans Affairs (VA) national repositories.6,12–14 Compared to veterans with combat-related lower limb injury, we expected a higher prevalence of CVD risk factors, including higher blood pressure and dyslipidemia, among veterans with unilateral or bilateral lower limb amputation.
Patients And Methods
Data Sources
The Human Subjects Review Boards at the NHRC and University of California San Diego approved this study. Details of this cohort and VA data acquisition have been previously described.6,11–14 The EMED contains medical and personnel information for each casualty injured in military operations. Medical record data are obtained from casualty clinical records beginning near the point of injury. The medical data are linked to tactical, operational, and deployment-related data obtained from various other US Department of Defense databases.12 EMED records are reviewed by certified nurse coders at NHRC and assigned codes from the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM), Abbreviated Injury Scale (AIS) 2005 scores, and Injury Severity Score (ISS) coding systems.15,16 Additional patient information was accessed through the VA Informatics and Computing Infrastructure, and included data from the Corporate Data Warehouse (CDW) and Managerial Cost Accounting (MCA) National Data Extracts for the years 2003 through April 2015.17,18
Study Sample
This cohort consisted of US service members with combat-related lower limb amputation(s) and patients without amputation who had a serious lower limb injury with an AIS score ≥3. All patients were identified in the EMED as injured in Iraq or Afghanistan conflicts from 2001 through 2008. The original cohort consisted of 800 patients. Only veterans with at least 1 year in the VA and at least two blood pressure readings were included, resulting in a final cohort of 772 individuals. The final study cohort included 184 veterans with serious limb injury without amputation, 442 veterans with unilateral lower limb amputation, and 146 with bilateral lower limb amputations.
Measures
Primary Outcomes
CVD risk factors were extracted from VA electronic data sources after the time of injury. Systolic blood pressure (SBP; normal <140 mmHg) and diastolic blood pressure (DBP; normal <90 mmHg) were extracted from the CDW vital signs file. Average SBP and DBP were used to estimate mean arterial pressure (MAP) based on this formula: (2DBP + SBP)/3. Serum low-density lipoprotein (LDL; normal <140 mg/dl) cholesterol, high-density lipoprotein (HDL; normal >45 mg/dl in men and >55 mg/dl in women) cholesterol, and triglycerides (TG; normal fasting <150 mg/dl) were extracted from MCA laboratory files. Serum TG (normal <150 mg/dl) were presumed to be fasting. Because TG data were skewed, this parameter was log-transformed [ln(TG)] for analysis. As there is generally variation in these anthropomorphic and biochemical parameters, measures were averaged analyses.
Metabolic syndrome is a constellation of metabolic abnormities that includes SBP ≥130 mmHg, DBP ≥85 mmHg, HDL ≤40 mg/dl (≤50 mg/dl for women), TG ≥150 mg/dl, fasting blood glucose ≥100 mg/dl, and waist circumference ≥40 inches (≥35 inches for women) or a diagnosis of type 2 diabetes.19 Because the majority of the cohort did not have waist circumference or fasting glucose in the data sources, these variables were not used in our case definition for metabolic syndrome. Thus, metabolic syndrome was defined as a diagnosis of type 2 diabetes or as a constellation of blood pressure and lipid changes consistent with metabolic syndrome—specifically, a mean blood pressure over 130/85 mmHg or a prescription for an antihypertensive medication, a mean HDL ≤40 mg/dl (≤50 for women), and mean TG ≥150 mg/dl.19
Covariates
Variables from the EMED included age at injury, number of deployments, and ISS. Veterans with traumatic brain injury (TBI) were identified by ICD-9-CM codes in the following ranges: 800.00–801.99 (fractures of the vault or base of the skull), 803.00–804.99 (other unqualified and multiple fractures of the skull), 850.00–854.10 (intracranial injury, including concussion, contusion, laceration, and hemorrhage), V15.52 (personal history of TBI), 905.0 (late effects of intracranial injury with mention of skull fracture), and 907.0 (late effects of intracranial injury without skull fracture); two ICD-9-CM codes of 309.81 for posttraumatic stress disorder (PTSD) were required in order to be categorized as having PTSD. “Years within the VA” was used as a covariate to adjust for patient complexity. Average weight in kilograms was adjusted for loss of limb; below the knee amputation was assumed to be mid-calf (~3% of body weight) and above the knee was assumed to be mid-thigh (~11% of body weight). Body mass index (BMI) in kg/m2 was calculated based on adjusted weights.20
Data Analysis
Continuous outcomes [MAP, LDL, HDL, and ln(TG)] were modeled separately, adjusting for the covariates described above. Because we were considering several results, models were run using the same set of covariates. The full model included all covariates; the final model included only parameters that appeared to be confounders or independent predictors with a p-value ≤0.10. Age at injury, age at data collection, and years within the VA were highly correlated therefore; therefore, only age at data collection was used as a covariate in the model. Interactions between amputation status and final model parameters were explored and models were stratified by significant effect modifiers (p≤0.05, interaction term). Similarly, logistic regression was used to model metabolic syndrome (defined above). Apart from antihypertensive medication (included in the case definition of metabolic syndrome), the same covariates were included.
Results
Missing Data
Our previous study identified nearly the full population of combat amputees injured in Iraq or Afghanistan between 2001 and 2008, approximately 95% of independent military counts.21 Of the 772 veterans included in this study, 68 (8.8%) had missing lipid data with no significant difference in missing lipid data between the amputation groups. In addition, 29 (3.7%) had missing height documentation for BMI calculation. Among those with bilateral lower limb amputation, 39 (25%) veterans had missing data on whether the amputation was above or below knee for one or both lower limbs. Given that the majority of known amputations were below the knee, BMI was adjusted based on below the knee amputation in cases where amputation level was missing.
Study Population
Most of the cohort was male (98%), median age at time of data collection was 34 years (range 27–59 years), with outcomes at the VA over an average of 8.1 years (standard deviation [SD] 1.8 years; results not shown). At the time of injury, those with unilateral lower limb amputation were significantly older (25.59, SD 5.61 years) than those with limb injury but no amputation (24.27, SD 5.04 years; p<0.01). Age at injury for those with bilateral lower limb amputation (25.09, SD 5.00 years) was not significantly different from those with lower limb injury (results not shown). Other baseline characteristics of this study population by lower limb injury or amputation group are shown in Table 1.
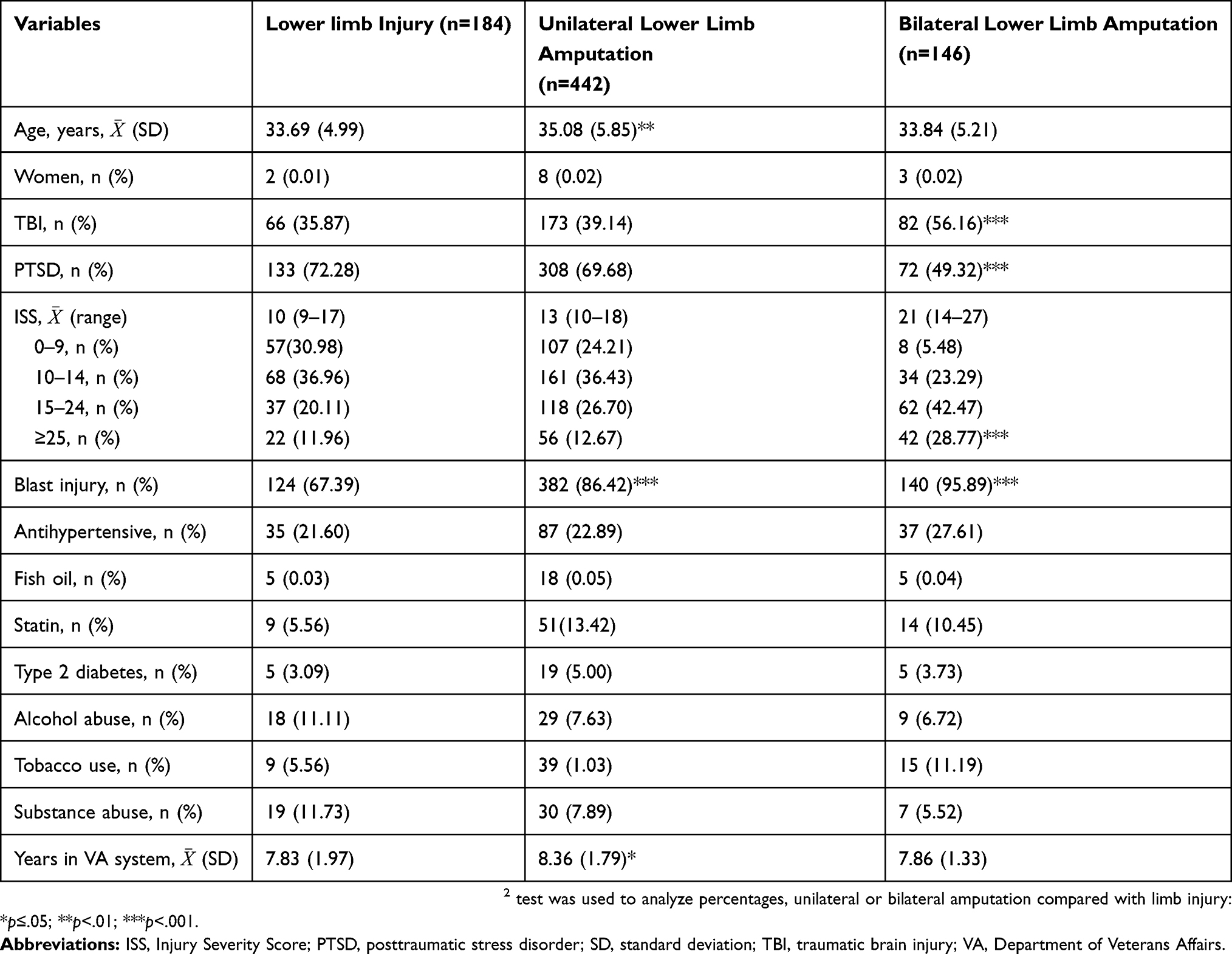 |
Table 1 Baseline Characteristics By Amputation Status |
At the time of data collection, those with unilateral lower limb amputation were significantly older than those with limb injury (p<0.005); average ages were 33.69 years (SD 4.99), 35.08 (SD 5.85), and 33.84 years (SD 5.21) for limb injury, unilateral lower limb amputation, and bilateral lower limb amputation, respectively. In comparison to the limb injury group, veterans with bilateral lower limb amputation had the lowest prevalence of PTSD (p<0.001) but the highest prevalence of TBI (p<0.001) and highest ISS (p=0.001). Veterans with lower limb amputation were much more likely to have sustained a blast injury (p<0.001). Veterans with unilateral lower limb amputation had the longest time in the VA system (p<0.05).
Univariate Results
Unadjusted univariate analyses comparing CVD risk factors between unilateral or bilateral lower limb amputation and lower limb injury are shown in Table 2. Average MAP was higher among veterans with bilateral lower limb amputation (p<0.01). Average HDL cholesterol was highest among patients without an amputation and significantly lower among those with unilateral (p<0.01) and bilateral lower limb amputation (p<0.001). Average TG was lowest among veterans with limb injury and significantly higher among those with unilateral (p<0.01) and bilateral (p<0.001) lower limb amputation. Approximately 8.70% of those without amputation had metabolic syndrome; this is comparable to a prevalence of 14.93% (p<0.05) and 21.92% (p<0.001) with unilateral or bilateral lower limb amputation, respectively.
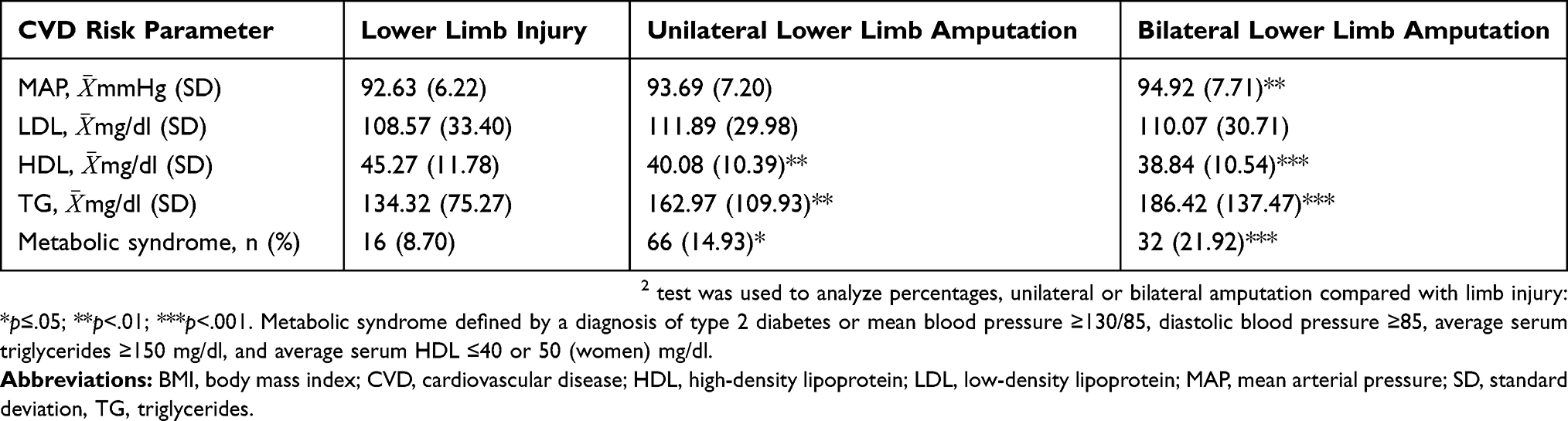 |
Table 2 Univariate Cardiovascular Disease (CVD) Risk Parameters By Amputation Status |
Linear And Logistic Regression Results
Amputation was modeled as an indicator variable with unilateral or bilateral lower limb amputation compared with the limb injury reference group. Adjusted changes, with 95% confidence intervals (CIs) and p-values, are shown in Table 3. Modeling was done using the full set of covariates (described in Methods). A backward elimination was used to determine the final model, which included only covariates with a p-value <0.10. Results from both full and final models are presented in Table 3.
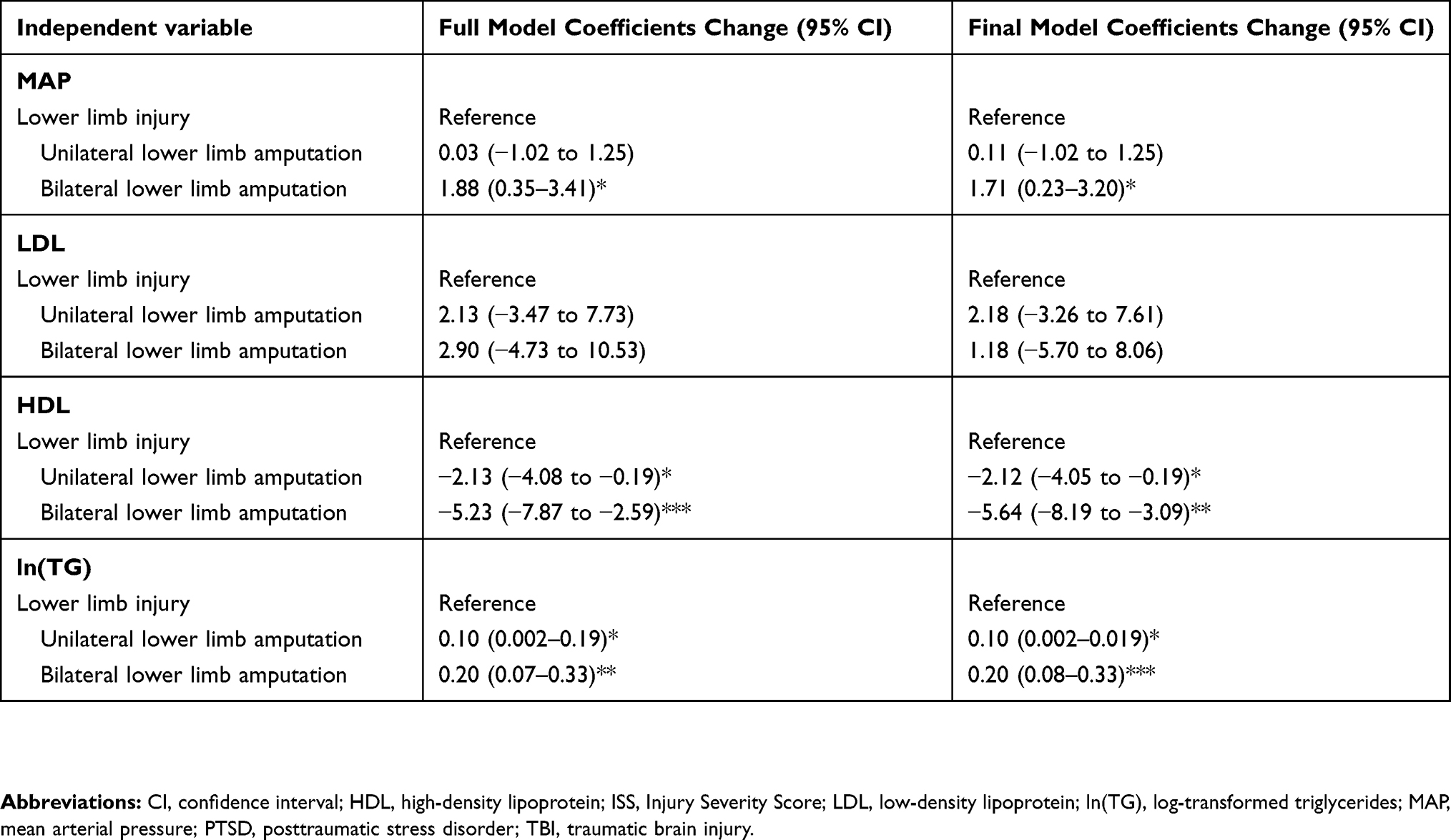 |
Table 3 Multivariable Linear Regression: Change For Cardiovascular Disease Risk Parameters |
Mean Arterial Pressure
Compared with the limb injury group, there was no significant difference in MAP among veterans with unilateral lower limb amputation. However, there was a 1.71 mmHg increase in MAP (95% CI: 0.23–3.20) among veterans with bilateral lower limb amputation. Though not detailed in Table 3, use of an antihypertensive medication (p<0.001), age (p<0.01), male gender (p<0.05), higher BMI (p<0.001), and alcohol use (p<0.05) were all associated with a significantly higher MAP. A diagnosis of TBI was associated with a lower MAP (p<0.001). There was no statistically significant evidence of collinearity or effect of medication (results not shown).
Low-density Lipoprotein, High-density Lipoprotein, And Triglycerides
There were no significant differences in LDL between unilateral or bilateral lower limb amputation groups and patients with limb injury (Table 3). Statin use (p<0.001) and age (p<0.05) were significantly associated with a higher LDL (results not shown).
Compared with the limb injury group, there was a significant 2.12 mg/dl decrease in HDL (95% CI: −4.05 to −0.19) among those with unilateral lower limb amputation and a 5.64 mg/dl decrease in HDL (95% CI: −8.19 to −3.09) among those with bilateral lower limb amputation. Fish oil use (p<0.05), male gender (p<0.01), a diagnosis of PTSD (p<0.05), tobacco use (p<0.05) and BMI (p<0.001) were all associated with lower HDL; alcohol use was associated with a higher HDL (p<0.01; results not shown).
Triglycerides, modeled as ln(TG), were significantly higher among veterans with either unilateral or bilateral lower limb amputation than among the limb injury controls. There was a 0.10 increase in ln(TG) (95% CI: 0.002–0.19) with unilateral and a 0.2 increase (95% CI: 0.08–0.33) with bilateral lower limb amputation. Use of antihypertensive medications, statins, or fish oil and increasing BMI were associated with significantly higher TG levels (p<0.001 for all). There was no evidence of collinearity or effect of medication for LDL, HDL, or TG models (results not shown).
Metabolic Syndrome
Odds ratios for the prevalence of metabolic syndrome defined a diagnosis of type 2 diabetes or a constellation of blood pressure and lipid changes consistent with metabolic syndrome are shown in Table 4. There was a 2.25-fold increase (95% CI: 1.19–5.05) in the odds of metabolic syndrome with bilateral lower limb amputation (Table 4). Age (p<0.001), tobacco use (p<0.05), and BMI (p<0.001) were significantly associated with increased prevalence of metabolic syndrome. There was no evidence of collinearity or effect modification (results not shown).
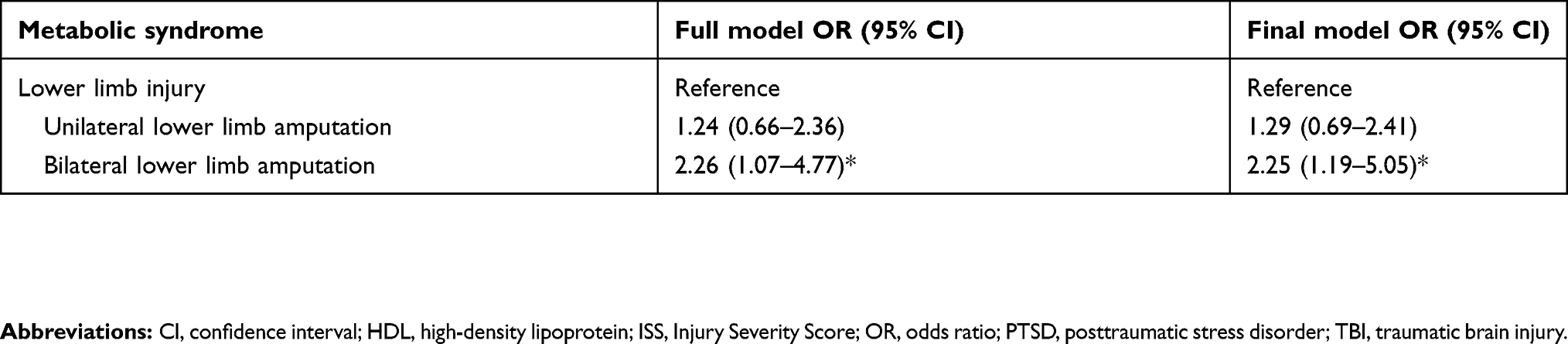 |
Table 4 Multivariate Logistic Regression: Prevalence Of Metabolic Syndrome |
Discussion
The present study is one of the first, to our knowledge, to document an increase in CVD-related risk factors among a contemporary cohort of veterans with combat-related lower limb amputation injured during combat in the recent wars in Iraq and Afghanistan.
Increased CVD-related mortality8 and an increased prevalence of CVD risk factors, including hypertension, dyslipidemia, and insulin resistance have been found in the older cohorts of veterans from World War II with traumatic lower limb amputation.9 Similarly, studies of Iranian10 and Israeli veterans22 with traumatic lower limb amputation have documented higher CVD risk factors, including abdominal adiposity, hyperinsulinemia and hypercoagulability, and excess mortality from CVD compared with population based norms. We observed a significant increase in mean MAP among veterans with bilateral lower limb amputation, and significantly lower HDL and higher TG among veterans with unilateral or bilateral lower limb amputation. Most notably, there was an over 2-fold increase in the prevalence of type 2 diabetes or blood pressure and lipid changes consistent with metabolic syndrome among veterans with bilateral lower limb amputation. Although there are limited data on the age-specific prevalence for metabolic syndrome among young adults, the prevalence among college students has been estimated to vary between 7% and 12%, similar to the prevalence observed here among veterans with lower limb injury without amputation.23,24
We noted higher MAP among veterans with bilateral lower limb amputation, even after controlling for antihypertensive medication use and hypertension risk factors such as age, gender, and BMI. There are also likely to be independent effects from increased peripheral resistance and hemodynamic changes as a direct result of amputation,25 as well as effects related to the level of amputation, with more aberrant vascular changes resulting from more proximal occlusion of the femoral artery.26 In addition to vascular changes, lower limb amputation has also been shown to be associated with increased sympathetic responsiveness and attenuate adrenomedullary secretion in response to a glucose challenge.27 This may result in insulin resistance, a hallmark of metabolic syndrome.19
The prevalence of type 2 diabetes or blood pressure and lipid changes consistent with metabolic syndrome was almost twice as high among veterans with bilateral lower limb amputation compared to the limb injury group, which was similar to the age-adjusted prevalence of 23% in an older US general population.28 Metabolic syndrome is a constellation of changes and includes high blood pressure, altered lipid profile characterized by high TG and low HDL cholesterol, altered glucose metabolism, insulin resistance, and type 2 diabetes.19 It has long been recognized as a significant risk factor for development of CVD,29 and may account for up to 44% of excess cardiovascular risk in the United States.30 Metabolic syndrome is directly mediated by abdominal adiposity, most significantly, visceral adiposity.19,31,32 Moreover, these changes are thought to contribute to a proinflammatory, proatherogenic state, with increases in circulating biomarkers for oxidative stress, including oxidized LDL cholesterol.31,33
A decrease in muscle mass and an increase in weight has been recently observed among veterans within the first year of a lower leg amputation;34 these changes in body composition are likely to result in future metabolic changes and an increased risk of metabolic syndrome. From a primary care perspective, abdominal adiposity and/or BMI are modifiable risk factors. Because physical mobility is limited, specific lifestyle interventions, such as nutritional support22,35,36 and physical conditioning to reduce abdominal and visceral adiposity, will be important.32 However, BMI is not the best indicator for abdominal adiposity and must also be adjusted for the loss of a limb. While we adjusted for below knee or above knee amputation, level of amputation was missing for ~25% of those with bilateral lower limb amputation. Waist circumference is considered a better proxy for abdominal adiposity and a proxy measure for visceral adiposity;32 based on our data, this does not seem to be routinely measured in this patient population. Thus, in addition to clinical guidelines to routinely measure waist circumference, other measures for abdominal adiposity need to be developed.32 It should also be noted that many of the CVD risk factors are also amenable to treatment, including blood pressure control, lipid treatment, and glucose monitoring and management.37
The main strength of the present study is that the majority of the EMED cohort was linked the VA CDW to analyze outcomes for an average of 8.1 years after injury17,18 We also used the EMED to carefully select controls with combat-related serious lower limb injury. This partially controlled for the physical and emotional trauma of combat-related extremity injury. Another strength is approximately 8.1 years of follow-up after injury; this relatively young cohort can now be studied going forward and be expanded to include more recently injured veterans. As this cohort ages, we expect increasing blood pressure and increasing levels of dyslipidemia and type 2 diabetes based on data from previous conflicts.29–33,37 Although PTSD is thought to be a risk factor for CVD,38 this variable had no significant association with any of the CVD risk factors studied here. Given that this is a young cohort, whether an association may be observed as the cohort matures remains to be determined.
Limitations
The EMED consists of veterans injured during combat, so results presented here may not be generalized to civilian cohorts or to patient populations with limb injury or amputation as a result of medical comorbid disease, such as diabetes, or other trauma. Because the CVD outcomes data are somewhat limited at this time, we used average measures instead of a repeated measures analysis. This approach is internally valid for the purpose of this study within the VA system. While veterans with a unilateral lower limb amputation had the longest follow-up period, the number of lipid and blood pressure measurements were not significantly different between the three groups (results not shown). The increase in MAP by amputation status is small (<2 mmHg), corresponding to relatively small changes in SBP or DBP. It has been well-documented that the risk of CVD-related disease and death is directly related to blood pressure in middle-aged populations.39 While this change in MAP may not be clinically relevant, change may increase over time and warrants further study. The definition of metabolic syndrome was based on administrative data sources and not direct measures for insulin resistance, which include fasting insulin levels and formal glucose challenge testing. Several of the parameters used to define metabolic syndrome, including fasting glucose and waist circumference, were not readily available. Whether this underestimated the prevalence of metabolic syndrome is not clear.
Conclusions
Although the results are exploratory at this time, we found an increased prevalence of CVD risk factors, including higher MAP, lower HDL, and higher TG levels among these veterans with lower limb amputations than among veterans with serious lower limb injury but no amputation. The prevalence of type 2 diabetes or blood pressure and lipid changes consistent with metabolic syndrome was also most pronounced among veterans with bilateral lower limb amputation. These results warrant further study and support implementation guidelines, including routine waist circumference measurements; active management of blood pressure, lipids, and obesity; and nutritional, emotional, and lifestyle support to ameliorate CVD risk.
Abbreviations
AIS, Abbreviated Injury Scale; BMI, body mass index; CDW, Corporate Data Warehouse; CI, confidence interval; CVD, cardiovascular disease; DBP, diastolic blood pressure; EMED, Expeditionary Medical Encounter Database; HDL, high-density lipoprotein; ISS, Injury Severity Score; LDL, low-density lipoprotein; MAP, mean arterial pressure; NHRC, Naval Health Research Center; PTSD, posttraumatic stress disorder; SBP, systolic blood pressure; TBI, traumatic brain injury; TG, triglycerides; VA, Department of Veterans Affairs.
Ethics statement
The study protocol was approved by the Naval Health Research Center and Department of Veterans Affairs Institutional Review Boards in compliance with all applicable Federal regulations governing the protection of human subjects. Research data were derived from an approved Naval Health Research Center and Department of Veterans Affairs, Institutional Review Board protocol numbers NHRC.2007.0016 and VA H130271.
Disclosure
Vibha Bhatnagar is a military service member or employee of the US Government. This work was prepared as part of my official duties. Title 17, U.S.C. §105 provides that copyright protection under this title is not available for any work of the US Government. Title 17, U.S.C. §101 defines a US Government work as work prepared by a military service member or employee of the US Government as part of that person’s official duties.
This work was supported by the US Navy Bureau of Medicine and Surgery Wounded, Ill, and Injured Program under work unit no. 61110 and the Extremity Trauma and Amputation Center of Excellence. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the US Government. The authors report no other conflicts of interest in this work.
References
1. Cross JD, Ficke JR, Hsu JR, Masini BD, Wenke JC. Battlefield orthopaedic injuries cause the majority of long-term disabilities. J Am Acad Orthop Surg. 2011;19(Suppl1):S1–S7. PMID: 21304041. doi:10.5435/00124635-201102001-00002
2. Pugh MJ, Finley EP, Copeland LA, et al. Complex comorbidity clusters in OEF/OIF veterans: the polytrauma clinical triad and beyond. Med Care. 2014;52(2):172–181. doi:10.1097/MLR.0000000000000059
3. Belisle JG, Wenke JC, Krueger CA. Return-to-duty rates among US military combat-related amputees in the global war on terror: job description matters. J Trauma Acute Care Surg. 2013;75(2):279–286. doi:10.1097/TA.0b013e31829bb777
4. Fitzpatrick KF, Pasquina PF. Overview of the rehabilitation of the combat casualty. Mil Med. 2010;175(Suppl 7):13–17. PMID: 23634473. doi:10.7205/MILMED-D-10-00159
5. Lew HL, Otis JD, Tun C, Kerns RD, Clark ME, Cifu DX. Prevalence of chronic pain, posttraumatic stress disorder, and persistent postconcussive symptoms in OIF/OEF veterans: polytrauma clinical triad. J Rehabil Res Dev. 2009;46(6):697–702. PMID: 20104399. doi:10.1682/JRRD.2009.01.0006
6. Melcer T, Walker J, Bhatnagar V, et al. Glasgow coma scale scores, early opioids, and 4-year psychological outcomes among combat amputees. J Rehabil Res Dev. 2014;51(5):697–710. PMID: 25509056. doi:10.1682/JRRD.2013.06.0143
7. Perkins ZB, De’Ath HD, Sharp G, Tai NR. Factors affecting outcome after traumatic limb amputation. Br J Surg. 2012;99(Suppl 1):75–86. doi:10.1002/bjs.7766
8. Hrubec Z, Ryder RA. Traumatic limb amputations and subsequent mortality from cardiovascular disease and other causes. J Chronic Dis. 1980;33(4):239–250. PMID: 7358826. doi:10.1016/0021-9681(80)90068-5
9. Rose HG, Schweitzer P, Charoenkul V, Schwartz E.Cardiovascular disease risk factors in combat veterans after traumatic leg amputations. Arch Phys Med Rehabil. 1987;68(1):20–23. PMID: 3800619.
10. Shahriar SH, Masumi M, Edjtehadi F, Soroush MR, Soveid M, Mousavi B. Cardiovascular risk factors among males with war-related bilateral lower limb amputation. Mil Med. 2009;174(10):1108–1112. PMID: 19891226. doi:10.7205/milmed-d-00-2309
11. Galarneau MR, Hancock WC, Konoske P, et al. the navy-marine corps combat trauma registry. Mil Med. 2006;171:691–697. PMID: 16933807. doi:10.7205/milmed.171.5.370
12. Melcer T, Sechriest VF, Walker J, Galarneau M. A comparison of health outcomes for combat amputee and limb salvage patients injured in Iraq and Afghanistan wars. J Trauma Acute Care Surg. 2013;75(2 Suppl 2):S247–S254. doi:10.1097/TA.0b013e318299d95e
13. Melcer T, Walker GJ, Galarneau M, Belnap B, Konoske P. Midterm health and personnel outcomes of recent combat amputees. Mil Med.2010;175:147–154. PMID: 20358702. doi:10.7205/MILMED-D-09-00120
14. Bhatnagar V, Richard E, Melcer T, Walker J, Galarneau M. Lower-limb amputation and effect of posttraumatic stress disorder on Department of Veterans Affairs outpatient cost trends. J Rehabil Res Dev. 2015;52(7):827–838. doi:10.1682/JRRD.2014.11.0288
15. Copes WS, Champion HR, Sacco WJ, Lawnick MM, Keast SL, Bain LW. The injury severity score revisited. J Trauma.1988;28:69–77. PMID: 3123707. doi:10.1097/00005373-198801000-00010
16. Tohira H, Jacobs I, Mountain D, Gibson N, Yeo A. Comparisons of the outcome prediction performance of injury severity scoring tools using the Abbreviated Injury Scale 90 Update 98 (AIS 98) and 2005 Update 2008 (AIS 2008). Ann Adv Automot Med. 2011;55:255–265. PMID: 22105401.
17. VA Information Resource Center. VIReC resource guide: VA Corporate Data Warehouse. U.S. Department of Veterans Affairs, Health Services Research & Development. Available from: https://www.virec.research.va.gov/.
18. Health Services Research & Development. VA Informatics and Computing Infrastructure (VINCI). U.S. Department of Veterans Affairs. Available from: http://www.hsrd.research.va.gov/for_researchers/vinci.
19. Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9:48. doi:10.1186/1741-7015-9-4
20. Amputee Coalition. Available from: https://www.amputee-coalition.org/limb-loss-resource-center/resources-filtered/resources-by-topic/healthy-living/about-bmi/.
21. Deployment related conditions of special surveillance interests, U.S. Armed Forces, by month and service, January 2003–october 2012. MSMR. 2013;20(1):19.
22. Modan M, Peles E, Halkin H, et al. Increased cardiovascular disease mortality rates in traumatic lower limb amputees. Am J Cardiol. 1998;82(10):1242–1247. PMID: 9832102. doi:10.1016/s0002-9149(98)00287-2
23. Morrell JS, Byrd-Bredbenner C, Quick V, Olfert M, Dent A, GB C. Metabolic syndrome: comparison of prevalence in young adults at 3 land-grant universities. J Am Coll Health. 2014;62(1):1–9. doi:10.1080/07448481.2013.841703
24. Dalleck LC, Kjelland EM. The prevalence of metabolic syndrome and metabolic syndrome risk factors in college-aged students. Am J Health Promot. 2012;27(1):37–42. doi:10.4278/ajhp.100415-QUAN-116
25. Paula-Ribeiro M, Garcia MMN, Martinez DG, Lima JRP, Laterza MC. Increased peripheral vascular resistance in male patients with traumatic lower limb amputation: one piece of the cardiovascular risk puzzle. Blood Press Monit. 2015;20(6):341–345. doi:10.1097/MBP.0000000000000148
26. Naschitz JE, Lenger R. Why traumatic leg amputees are at increased risk for cardiovascular diseases. QJM. 2008;101(4):251–259. doi:10.1093/qjmed/hcn067
27. Peles E, Akselrod S, Goldstein DS, et al. Insulin resistance and autonomic function in traumatic lower limb amputees. Clin Auton Res. 1995;5(5):279–288. doi:10.1007/BF01818893
28. Beltran-Sanchez H, Harhay MO, Harhay MM, McElligott S. Prevalence and trends of metabolic syndrome in the adult U.S. population, 1999–2010. J Am Coll Cardiol. 2013;62(8):697–703. doi:10.1016/j.jacc.2013.05.064
29. Cao HL, Chen XB, Lu JG, et al. Metabolic syndrome and coronary artery calcification: a community-based natural population study. Chin Med J (Engl). 2013;126:4618–4623. PMID: 24342299.
30. Liu L, Miura K, Fujiyoshi A, et al. Impact of metabolic syndrome on the risk of cardiovascular disease mortality in the United States and in Japan. Am J Cardiol. 2014;113(1):84–89. doi:10.1016/j.amjcard.2013.08.042
31. Jialal I, Devaraj S, Adams-Huet B, Chen X, Kaur H. Increased cellular and circulating biomarkers of oxidative stress in nascent metabolic syndrome. J Clin Endocrinol Metab. 2012;97(10):E1844–E1850. doi:10.1210/jc.2012-2498
32. Schuster J, Vogel P, Eckhardt C, Morelo SD. Applicability of the Visceral Adiposity Index (VAI) in predicting components of metabolic syndrome in young adults. Nutr Hosp. 2014;30(4):806–812. doi:10.3305/nh.2014.30.4.7644
33. Aroor AR, McKarns S, Demarco VG, Jia G, Sowers JR. Maladaptive immune and inflammatory pathways lead to cardiovascular insulin resistance. Metabolism. 2013;62(11):1543–1552. doi:10.1016/j.metabol.2013.07.001
34. Eckard CS, Pruziner AL, Sanchez AD, Andrews AM. Metabolic and body composition changes in first year following traumatic amputation. J Rehabil Res Dev. 2015;52(5):553–562. doi:10.1682/JRRD.2014.02.0044
35. Kesse-Guyot E, Ahluwalia N, Lassale C, Hercberg S, Fezeu L, Lairon D. Adherence to Mediterranean diet reduces the risk of metabolic syndrome: a 6-year prospective study. Nutr Metab Cardiovasc Dis. 2013;23(7):677–683. doi:10.1016/j.numecd.2012.02.005
36. Ahluwalia N, Andreeva VA, Kesse-Guyot E, Hercberg S. Dietary patterns, inflammation and the metabolic syndrome. Diabetes Metab. 2013;39(2):99–110. doi:10.1016/j.diabet.2012.08.007
37. Takahara M, Shimomura I. Metabolic syndrome and lifestyle modification. Rev Endocr Metab Disord. 2014;15(4):317–327. doi:10.1007/s11154-014-9294-8
38. Brudey C, Park J, Wiarderkiewicz J, Kobayashi I, Mellman T, Marvar P. Autonomic and inflammatory consequences of posttraumatic stress disorder and the link to cardiovascular disease. Am J Physiol Regul Integr Comp Physiol. 2015;309(4):R315–R321. doi:10.1152/ajpregu.00343.2014
39. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi:10.1016/S0140-6736(02)11911-8
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.