")
Back to Journals » Clinical Ophthalmology » Volume 16
Retinopathy of Prematurity: A Study of Incidence and Risk Factors in a Tertiary Hospital in Vietnam
Authors Nguyen TTB , Bui VT, Pham VPT, Pham TN
Received 19 August 2022
Accepted for publication 30 September 2022
Published 10 October 2022 Volume 2022:16 Pages 3361—3367
DOI https://doi.org/10.2147/OPTH.S386808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Thi Thanh Binh Nguyen,1,* Van Trieu Bui,1,* Vo Phuong Thao Pham,1 Thi Ny Pham2
1Department of Pediatrics, University of Medicine and Pharmacy, Hue University, Hue City, Vietnam; 2Department of Obstetrics and Gynecology, Hue University of Medicine and Pharmacy Hospital, Hue University, Hue City, Vietnam
*These authors contributed equally to this work
Correspondence: Thi Thanh Binh Nguyen, Department of Pediatrics, University of Medicine and Pharmacy, Hue University, 06 Ngo Quyen Street, Hue City, 49000, Vietnam, Email [email protected]; [email protected]
Objective: To determine the incidence and risk factors for the development of retinopathy of prematurity (ROP) in the neonatal intensive care unit (NICU) of Hue Central Hospital, Vietnam.
Methods: A prospective study was performed in 214 preterm infants with gestational age (GA) ≤ 33 weeks and/or ≤ 1800 grams of birth weight (BW) or infants with a GA > 33 weeks and a BW > 1800 grams with an unstable clinical course who were screened for ROP in Hue Central Hospital, Vietnam.
Results: Fifty-eight infants (27.1%) developed ROP; 39.7% cases were stage 1, 34.5% cases were stage 2, and 25.8% cases were stage 3. Gestational age (GA), birth weight, anemia, sepsis, respiratory distress syndrome, total days on oxygen supplementation > 1 week, continuous positive airway pressure (CPAP), mechanical ventilation, blood transfusion, and surfactant had a significant association with ROP in univariate analysis (p< 0.05). Using multivariate analysis, GA less than 32 weeks, sepsis, and CPAP/mechanical ventilation remained independent risk factors for ROP development.
Conclusion: The incidence of ROP in Vietnam was 27.1%. A GA less than 32 weeks, sepsis, and CPAP/mechanical ventilation are important risk factors for developing ROP.
Keywords: retinopathy of prematurity, preterm infants, low birth weight infants
Introduction
Retinopathy of prematurity (ROP) is a disease related to abnormal vasoproliferation of the blood vessels of the retina that led to serious vision impairment or blindness of prematurity infants, especially extremely preterm infants.1 In preterm neonates, the development of the retina and retinal vasculature is incomplete, and the high oxygen level and prolonged oxygen exposure after birth might interrupt the normal retinal vascularization.1 Due to the advances in neonatal intensive care strategies in recent decades, neonatal mortality has been markedly decreased in most countries in the world. However, complications related to preterm birth, including ROP, leave a serious burden on the healthcare system and the infants later in life. Currently, ROP is still a leading cause of potentially preventable blindness around the world. In Vietnam, ROP is one of the major causes of blindness in children under 10 years old, accounting for 32.6% of the cases.2 In a report from 2001, the prevalence of ROP in Vietnam was high at 45.8%.3 After 20 years, the improvement of prenatal and neonatal care programs is increasing the survival chances of preterm infants in Vietnam, and the incidence of ROP might be changed. Therefore, our study aimed to determine the incidence and identify the risk factors for ROP according to our current conditions in the neonatal intensive care unit (NICU).
Patients and Methods
This prospective study was carried out in 214 preterm neonates who were examined for ROP screening in the Pediatric Eye Care Center of the Pediatric Center of Hue Central Hospital from September 2019 to 2021.
Preterm neonates admitted to the NICU in Pediatric Center of Hue Central Hospital who met the criteria for ROP screening (that was evaluated by an attending neonatologist) were sent to Pediatric Eye Care Center. Eye examinations were performed by an experienced ophthalmologist on all preterm neonates who met one of the following criteria: infants with a gestational age (GA) ≤33 weeks and/or birth weight (BW) ≤1800 g or infants with a GA >33 weeks and a BW >1800 g with an unstable clinical course who are believed by attending neonatologist to be at risk for ROP with one of the conditions: respiratory support, severe sepsis, pneumonia, respiratory distress syndrome, ductus arteriosus. In Vietnam, the guideline by the Ministry of Health for ROP screening criteria is modified from American Academy of Pediatrics,4 that is appropriate for our healthcare conditions. The national screening guidelines performing ROP examination to neonates with body weight less than 1800 grams instead of 1500 grams compared to other developed countries.4 Initial screening was performed at 31-week postconceptional age in infants with gestational ages less than 26 6/7 weeks at birth or at 4-week postnatal age in infants with gestational age from 27 weeks at birth.4,5 The ophthalmologist with specialized training in pediatric retina examined the ROP development by using a binocular indirect ophthalmoscope. The infant’s pupils were dilated with 0.5% topical tropicamide and 0.5% phenylephrine 30–60 minutes before examination.4
Characteristics of ROP were defined based on the international classification, including stage and zone.6 All neonates were divided into two groups:
- ROP group: 58 preterm neonates with ROP
- Non-ROP group: 156 preterm neonates without ROP
The screening process is visualized in Figure 1.
 |
Figure 1 Flowchart of the study population. Abbreviation: ROP, retinopathy of prematurity. |
Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences version 20.0. P-values <0.05 were considered statistically significant. Univariate comparison of risk factors was conducted using chi-square test. The multivariate logistic regression model was utilized to determine the predictors of ROP. The odds ratio and 95% confidence interval for each possible risk factor were also calculated.
Ethical Statements
The study was carried out in the conformity to the Declaration of Helsinki and approved by the Institutional Review Board of the University of Medicine and Pharmacy, Hue University (No. H2019/128, dated May 16, 2019). Written informed consent was obtained from the parents of preterm infants before enrollment.
Results
A total of 214 preterm neonates who met the criteria for ROP screening were included in this study. The incidence of ROP was 27.1%. The characteristics of study group are shown in Table 1. The average GA and mean BW of the ROP group were significantly lower than those in the non-ROP group (p<0.05). The incidence of ROP increased with decreases in GA and BW. Nutrition classification and type of pregnancy were not found to be significant risk factors for the development of ROP (p>0.05) (Table 1).
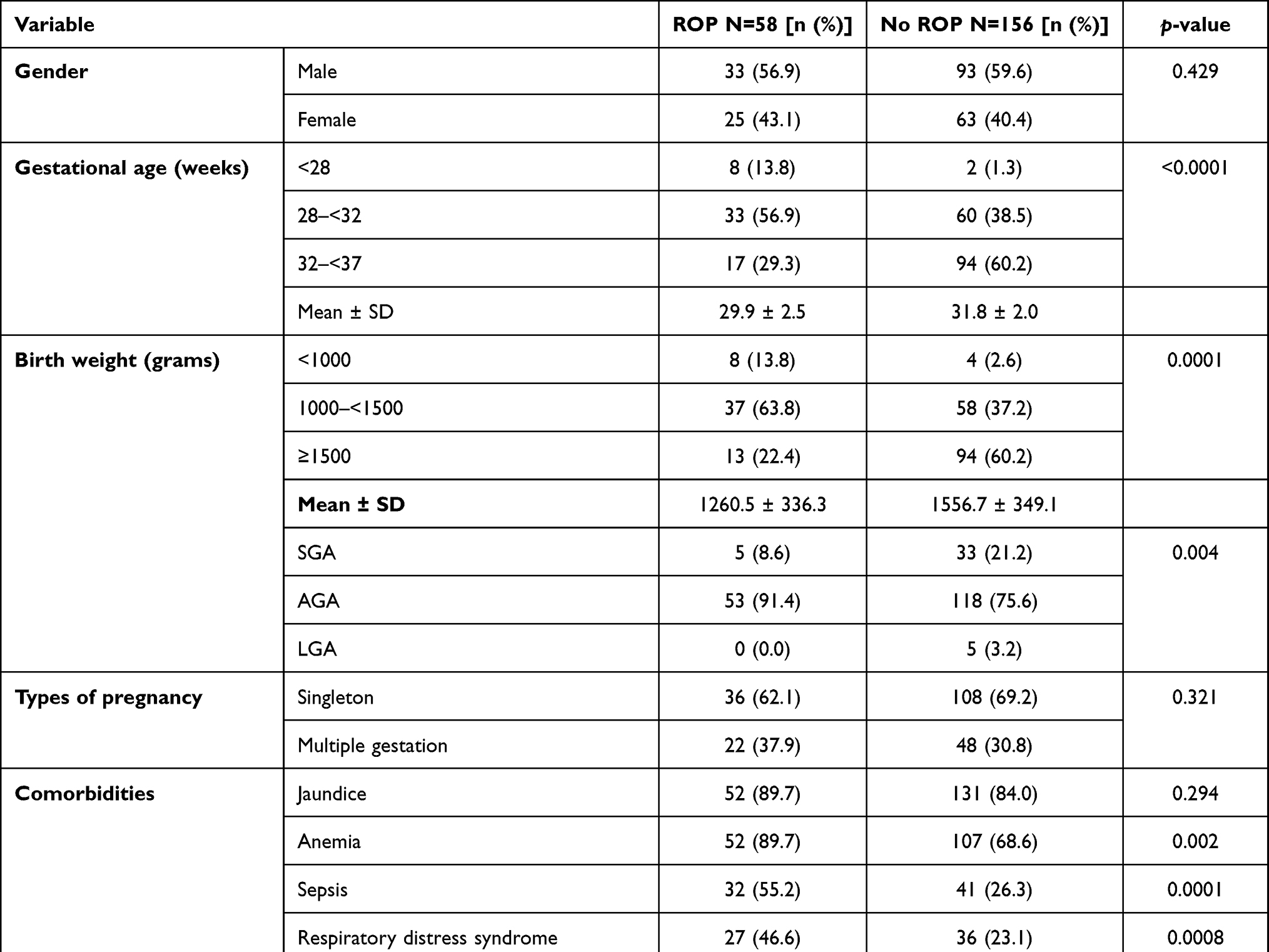 |
Table 1 General Characteristics of Preterm Infants in the Study Population and the Associations with Retinopathy of Prematurity Development |
Characteristics of ROP, including stage of disease and zone affected in all infants who developed ROP, were recorded. Regarding ROP findings, 9/58 (15.5%) infants had ROP only in the right eye, 8/58 (13.8%) infants had ROP only in the left eye, and 41/58 (70.7%) infants had ROP in both eyes. According to the international classification of ROP, 23/58 (39.7%) infants had stage 1, 20/58 (34.5%) infants had stage 2, and 15/58 (25.8%) had stage 3 ROP, while none of the infants had stage 4 or 5 ROP or presented with plus disease. Regarding the retinal zone affected, of 99 affected eyes, 29.3% eyes were in zone 1, 68.7% were in zone 2, and 2% were in zone 3. The incidence of type 1 ROP was 15.5%. Out of the 9 infants (15.5%) requiring treatment, 8 (88.9%) had laser photocoagulation, 1 (11.1%) had intravitreal bevacizumab (anti-VEGF).
We also assessed the association of ROP development with comorbidities and therapeutic interventions of infants in the study group (Table 1). Anemia, respiratory distress syndrome (RDS), and sepsis were significantly associated with ROP (p<0.05). However, other diseases, including jaundice, asphyxia, hypoglycemia, patent ductus arteriosus, and intraventricular hemorrhage, were not associated with an increased risk of ROP development (p>0.05).
Important factors found to have an association with development of ROP included >7 total days on supplemental oxygen, continuous positive airway pressure (CPAP), mechanical ventilation, blood transfusion, and surfactant (all p<0.05). Duration of oxygen exposure was longer in the infants with ROP than in non-ROP infants (25.1 [13.1–43.5] days vs 9.2 [4.0–19.7] days, p<0.05). However, our study also showed that ROP incidence was not statistically significantly different among infants who did or did not receive phototherapy (p>0.05).
According to the multivariate analysis, a GA <32 weeks (OR=2.2, 95% CI 1.0–4.5, p<0.05), sepsis (OR=2.5, 95% CI 1.2–5.1, p<0.05), and CPAP and/or mechanical ventilation (OR=2.9, 95% CI 1.1–7.8, p<0.05) were independently associated with the development of ROP (Table 2).
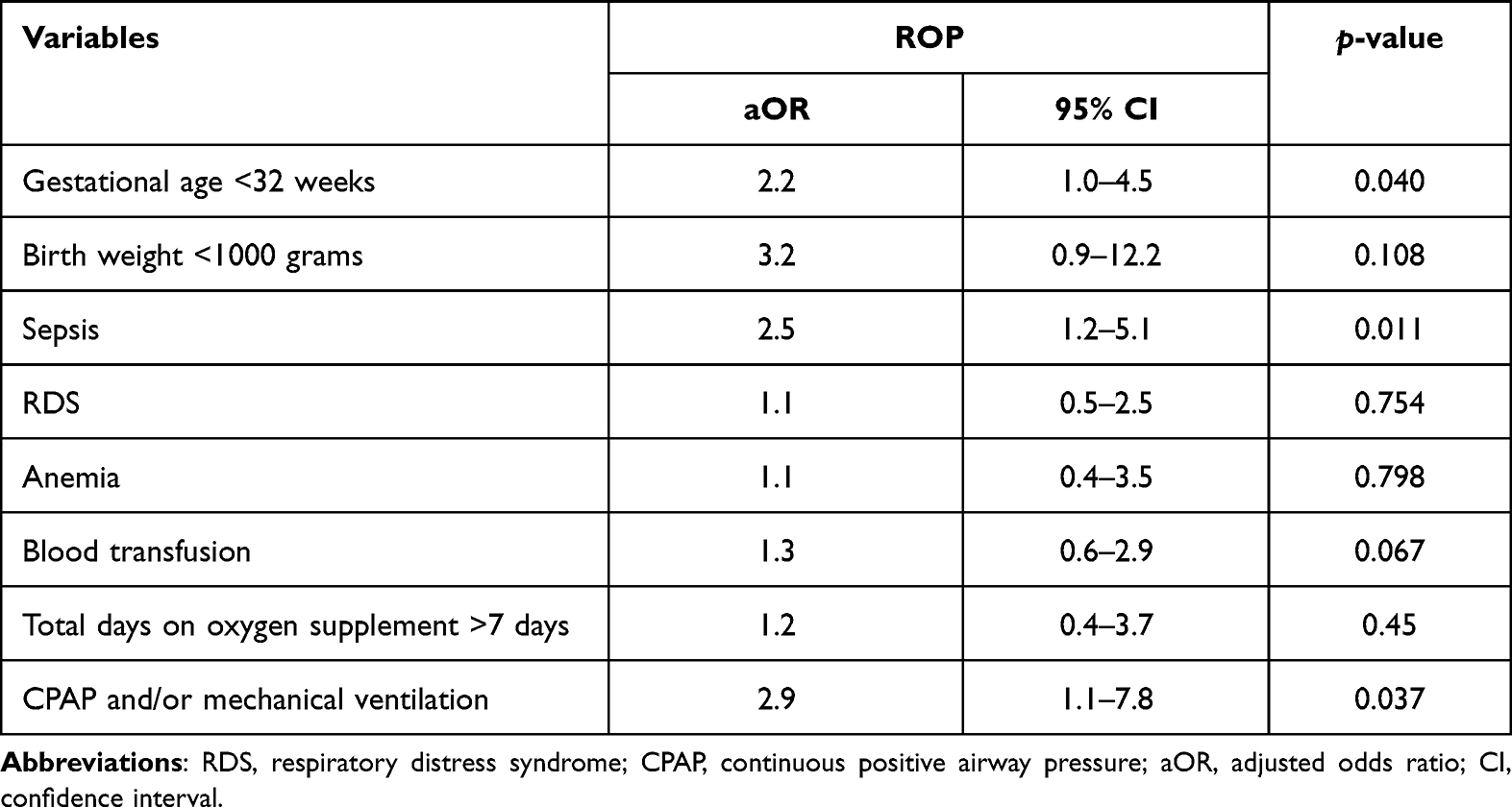 |
Table 2 Multivariate Analysis of Risk Factors for Retinopathy of Prematurity |
Discussion
The incidence of ROP varies among countries and is influenced by improvements in neonatal care, the characteristics of preterm infants, and the available ROP screening program. It should be noted that the prevalence of ROP in Vietnam was listed as 45.8% in a report from 2001.3 In the current study, we found that the incidence of ROP had decreased to 27.1%, which is comparable with the incidence reported in studies conducted in other developing countries.7,8 This result serves as evidence of the improvement in perinatal care in Vietnam in the last two decades. In comparing our results with those of other studies of infants with similar GAs, we found that some studies recorded a higher incidence of ROP—for example, Reyes et al reported an incidence of 40.4% in Oman9—while lower incidence of 18.5% and 19.2%, respectively, were reported in studies by Yau et al in China10 and Abdel et al in Egypt.11
Many studies have revealed that GA and BW are important factors related to the development of ROP in premature infants.9,10,12–15 The results of our study are in agreement with those of previous studies that demonstrated that the incidence of ROP was inversely proportional to GA and BW (Table 1). GA remained significantly associated with ROP even in multivariate analysis (Table 2). Low GA is related to immature vascularization, which increases the susceptibility of the retina to oxidative response and to numerous perinatal factors, including hyperoxic and hypoxic conditions.1,16 In contrast, for BW, the difference was not significant in a multivariate analysis. This finding is similar to those reported in other studies by Akkawi et al in Palestine and Abdel et al in Egypt.8,11 However, some studies have recorded an association between BW and ROP.7,9,10,12
Due to prematurity and comorbidities, the preterm infants received many care and treatment interventions. There was a significant relationship between ROP and a duration of oxygen supplementation >7 days, CPAP, mechanical ventilation, blood transfusion, and surfactant. Significant relationships with ROP were also found for anemia, RDS, and sepsis (Table 1). However, in multivariate analysis, sepsis, CPAP, and/or mechanical ventilation were found to be independent risk factors for ROP development (Table 2). Many neonatal conditions and its association with development of ROP were reported in other studies in developing countries in recent years.7,9–12 Freitas et al found that risk factors associated with ROP at any stage were extremely low BW, pulmonary diseases, intraventricular hemorrhage, and low GA.7 In a study reported by Reyes et al, risk factors including low BW, extremely preterm infants, invasive ventilation, prolonged exposure oxygen, duration of nasal CPAP, late-onset sepsis showed statistically significant association with the development of ROP.9 Bassiouny et al revealed the main risk factors for the development of ROP were GA, BW, oxygen therapy, sepsis, multiple birth, and cesarean section.12 In the current work, we found that sepsis increases the risk of developing ROP 2.7-fold in multivariate analysis (p<0.05). Several possible mechanisms could explain this result, including the pathogenic bacteria’s causing endotoxin-induced retinitis, which can lead to blood vessel inflammation and increased permeability in the retina. Sepsis aggravates the inadequate oxidative stress response, which induces cell degeneration and necrosis, thereby fostering retinal and vascular injuries. Furthermore, inflammatory factors such as interleukin-1β or phospholipase-2 can impact retinal neovascularization.17 Since sepsis is one of the most common diseases in very low BW and extremely preterm neonates, early detection, prevention, and management of infection could be impactful strategies for reducing ROP in preterm infants. Similar results were obtained in other studies; for example, in a meta-analysis, Wang et al demonstrated that sepsis increases the risk of ROP in premature infants, with an OR of 1.57 (95% CI 1.31–1.89, p<0.05),17 and Abdel et al also reported an increased risk, with an OR 1.251 (95% CI 1.082–1.458, p<0.05).11 However, some studies did not find any significant association between ROP development and sepsis.8,12
Some previous studies reported that oxygen supplementation was associated with ROP due to its effect on retinal vessel development: supplemental oxygen can interfere with oxygen tension and a high concentration of oxygen can lead to oxidative stress, which increases retinal ischemia, resulting in ROP.1,9,11,12,18 Factors related to oxygen supplementation, by CPAP and/or mechanical ventilation remained statistically significant on multivariate analysis. Reyes et al and Akkawi et al also found that invasive ventilation, oxygen therapy increase the risk of developing ROP.8,9 In contrast, Freitas et al in Brazil did not find any significant association between ROP development and supplemental oxygen.7
Conclusion
Although the incidence of ROP in Vietnam in the present study is similar to those reported in some other developing countries, it is still high. The results of this study provide constructive information for neonatologists and ophthalmologists for clinical practice regarding the prevention of and screening for ROP in preterm infants. Improving perinatal care to reduce preterm births, optimizing treatment with effective management of sepsis, and monitoring supplemental oxygen by ventilation methods are also important strategies that could reduce the incidence of ROP in developing countries in the coming years.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hartnett ME, Penn JS. Mechanisms and management of retinopathy of prematurity. N Engl J Med. 2012;367(26):2515–2526. doi:10.1056/NEJMra1208129
2. Limburg H, Gilbert C, Hon DN, Dung NC, Hoang TH. Prevalence and causes of blindness in children in Vietnam. Ophthalmology. 2012;119(2):355–361. doi:10.1016/j.ophtha.2011.07.037
3. Phan MH, Nguyen PN, Reynolds JD. Incidence and severity of retinopathy of prematurity in Vietnam, a developing middle-income country. J Pediatr Ophthalmol Strabismus. 2003;40(4):208–212. doi:10.3928/0191-3913-20030701-07
4. Ministry of Health of Vietnam. Decision No. 2582/QĐ-BYT on the Promulgation of “Guidelines for the Care of Premature Infants, Screening, Treatment and Monitoring of Retinopathy of Prematurity”. Hanoi, Vietnam: Vietnam Ministry of Health; 2012:10–24.
5. Fierson WM, Chiang MF, Good W, et al. Screening examination of premature infants for retinopathy of prematurity. Pediatrics. 2018;142(6). doi:10.1542/peds.2018-3061
6. International Committee for the Classification of Retinopathy of Prematurity. The international classification of retinopathy of prematurity revisited. Arch Ophthalmol. 2005;123(7):991–999. doi:10.1001/archopht.123.7.991
7. Freitas AM, Mörschbächer R, Thorell MR, Rhoden EL. Incidence and risk factors for retinopathy of prematurity: a retrospective cohort study. Int J Retin Vitr. 2018;4(1):1–8. doi:10.1186/s40942-018-0125-z
8. Akkawi MT, Shehadeh MM, Shams AN, et al. Incidence and risk factors of retinopathy of prematurity in three neonatal intensive care units in Palestine. BMC Ophthalmol. 2019;19(1):1–7. doi:10.1186/s12886-019-1180-4
9. Reyes ZS, Al-Mulaabed SW, Bataclan F, et al. Retinopathy of prematurity: revisiting incidence and risk factors from Oman compared to other countries. Oman J Ophthalmol. 2017;10(1):26. doi:10.4103/ojo.OJO_234_2014
10. Yau GS, Lee JW, Tam VT, et al. Incidence and risk factors of retinopathy of prematurity from 2 neonatal intensive care units in a Hong Kong Chinese population. Asia Pac J Ophthalmol. 2016;5(3):185–191. doi:10.1097/APO.0000000000000167
11. Abdel HA, Mohamed GB, Othman MF. Retinopathy of prematurity: a study of incidence and risk factors in NICU of Al-Minya University Hospital in Egypt. J Clin Neonatol. 2012;1(2):76. doi:10.4103/2249-4847.96755
12. Bassiouny RM, Ellakkany RS, Aboelkhair SA, Mohsen TA, Othman IS. Incidence and risk factors of retinopathy of prematurity in neonatal intensive care units: Mansoura, Egypt. J Egypt Ophthalmol Soc. 2017;110(3):71. doi:10.4103/ejos.ejos_25_17
13. Coutinho I, Pedrosa C, Mota M, et al. Retinopathy of prematurity: results from 10 years in a single neonatal intensive care unit. J Pediatr Neonat Individual Med. 2017;6(1):e060122.
14. Azami M, Jaafari Z, Rahmati S, Farahani AD, Badfar G. Prevalence and risk factors of retinopathy of prematurity in Iran: a systematic review and meta-analysis. BMC Ophthalmol. 2018;18(1):1–4. doi:10.1186/s12886-018-0732-3
15. Kim SJ, Port AD, Swan R, Campbell JP, Chan RP, Chiang MF. Retinopathy of prematurity: a review of risk factors and their clinical significance. Surv Ophthalmol. 2018;63(5):618–637. doi:10.1016/j.survophthal.2018.04.002
16. Cavallaro G, Filippi L, Bagnoli P, et al. The pathophysiology of retinopathy of prematurity: an update of previous and recent knowledge. Acta Ophthalmol. 2014;92(1):2–20. doi:10.1111/aos.12049
17. Wang X, Tang K, Chen L, Cheng S, Xu H. Association between sepsis and retinopathy of prematurity: a systematic review and meta-analysis. BMJ Open. 2019;9(5):e025440. doi:10.1136/bmjopen-2018-025440
18. Das PK, Hossain MM, Shirin M, ParvejIbne MS, Halim SP, Hossain AE. Effect of supplemental oxygen on development of retinopathy of prematurity. MedPulse Int J Pediatr. 2020;15(1):11–16. doi:10.26611/10141513
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.