")
Back to Journals » Clinical Ophthalmology » Volume 10
Retinal vascular occlusion: a window to diagnosis of familial and acquired thrombophilia and hypofibrinolysis, with important ramifications for pregnancy outcomes
Authors Dixon S, Bruce C, Glueck C, Sisk R , Hutchins R, Jetty V, Wang P
Received 23 February 2016
Accepted for publication 21 April 2016
Published 9 August 2016 Volume 2016:10 Pages 1479—1486
DOI https://doi.org/10.2147/OPTH.S106969
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Stephan G Dixon,1 Carl T Bruce,1 Charles J Glueck,1 Robert A Sisk,2,3 Robert K Hutchins,2,3 Vybhav Jetty,1 Ping Wang1
1Cholesterol, Metabolism, and Thrombosis Center, Jewish Hospital of Cincinnati, 2Cincinnati Eye Institute, 3Department of Ophthalmology, University of Cincinnati College of Medicine, Cincinnati, OH, USA
Aim: Our specific aim was to document the pathoetiologic importance of thrombophilia among females presenting with severe ischemic retinal vein (RVO) or retinal artery (RAO) occlusion, without typical risk factors, and to emphasize that the ophthalmologists’ diagnosis of thrombophilia has important diagnostic and therapeutic downstream ramifications for nonocular thrombosis, including reproductive outcomes.
Methods: We evaluated familial and acquired thrombophilia in 60 females with RVO (central RVO, n=52; branch RVO, n=8) and 16 with RAO (central RAO, n=11; branch RAO, n=5). They were referred by retinologists, without typical risk factors for RVO/RAO and/or severe ocular ischemic presentation. We focused on extraocular thrombotic events, particularly pregnancy complications, including unexplained spontaneous abortion, pre-eclampsia–eclampsia. Thrombophilia measurements in the 76 females were compared with 62 healthy normal females without ocular vascular occlusions (OVOs).
Results: The 76 females with OVO were more likely than 62 normal female controls to have high homocysteine (24% vs 0%, P<0.0001), high anticardiolipin antibody (immunoglobulin M, 17% vs 3%, P=0.012), high (>150%) factor VIII (42% vs 11%, P<0.0001), and high (>150%) factor XI (22% vs 4%, P=0.004). Of the 76 females, 26 (34%) had ≥1 spontaneous abortion; 17 (22%) had ≥2 spontaneous abortions and/or pre-eclampsia–eclampsia. Compared to 62 healthy female controls, these 17 females with pregnancy complications had high homocysteine (29% vs 0%, P=0.0003), high anticardiolipin antibody immunoglobulin M (24% vs 3%, P=0.02), high factor VIII (38% vs 11%, P=0.02), and were marginally more likely to be heterozygous for the factor V Leiden mutation (19% vs 3%, P=0.058).
Conclusion: In females lacking typical risk factors for retinal vascular occlusion or severely ischemic presentation, by diagnosing thrombophilia as an etiology for OVO, the ophthalmologist opens a window to family screening and preventive therapy, with particular relevance to pregnancy outcomes and venous thromboembolism.
Keywords: thrombophilia, retinal vascular occlusion, retinal vein occlusion, retinal artery occlusion
Introduction
Widely recognized, but neither sensitive nor specific risk factors for ocular vascular occlusion (OVO) include age, history of smoking, hypertension, hyperlipidemia, and diabetes mellitus.1–11 Rare systemic risk factors for OVO include hyperviscosity, myeloproliferative disorders, retro-orbital mass effect, and vasculitis such as Behcet’s.12,13 Open-angle glaucoma decreases venous outflow via increased intraocular pressure, thus creating vascular stasis and increased risk of OVO.2,14–16 In the absence of a cardioembolic etiology for OVO, thrombophilia is a common, major cause of ocular thrombotic events.12,17–25 In particular, thrombophilia should be carefully assessed in younger patients, <65 years old, or in patients with a personal or family history of thrombosis.25
Thrombophilia20 can be heritable – such as hyperhomocysteinemia, factor V Leiden (FVL), prothrombin G20210A (PTG) mutation,18 antithrombin III deficiency, protein C deficiency or protein S deficiency – or acquired, particularly the antiphospholipid syndrome-lupus anticoagulant.26 Of the thrombophilias that are risk factors for OVO,4,8,9,13,17,24,27–37 hyperhomocysteinemia is the most common disorder.8,13,17,24,33–37 Homocysteine is also a risk factor for systemic vascular thrombosis, including ischemic heart disease and deep venous thrombosis.38,39 In addition to hyperhomocysteinemia, FVL and PTG heterozygosity have been shown to be major risk factors for both OVO18 and large vein thrombosis.33,40–43
Thrombophilia is only one of many causes of spontaneous abortion.44–47 Familial and acquired thrombophilia are important risk factors for spontaneous pregnancy loss,48,49 interacting with the physiologic thrombophilia of pregnancy50,51 or the postpartum period52 to promote thrombosis of the spiral arteries of the placenta, facilitating development of placental insufficiency, with resultant spontaneous abortion; pre-eclampsia, eclampsia; and hemolysis, elevated liver enzymes, and low platelet count syndrome.51
Our specific aim was to document the pathoetiologic importance of thrombophilia among females presenting with severe ischemic retinal vein (RVO) or retinal artery (RAO) occlusion, without typical risk factors, and to emphasize that the ophthalmologists’ diagnosis of thrombophilia has important diagnostic and therapeutic downstream ramifications for nonocular thrombosis, including reproductive outcomes.
Methods
The study was approved by the Jewish Hospital Institutional Review Board (ID 12-03), Cincinnati, OH, USA. Written informed consent was obtained from patients after the nature of the study was fully explained. The study was conducted in accordance with the principles of the Declaration of Helsinki.
In a consecutive case series of females referred to vitreoretinal specialists at the Cincinnati Eye Institute with severe ischemia18,53 (OVO without typical risk factors), studies of thrombophilia were carried out in parallel with assessment of other organ systems affected by thrombosis, with special focus on reproductive outcomes, known to be affected by thrombophilia.
The analysis cohort was divided into patients with RVO (low pressure, low velocity), including branch and central RVO (BRVO and CRVO), and those with RAO (high pressure and velocity), including central RAO (CRAO) and branch RAO. Patients were referred and evaluated by vitreoretinal specialists at the Cincinnati Eye Institute. The ocular diagnoses were established by complete ophthalmological evaluations during which the patients’ histories, visual deficits, and fundus abnormalities were ascertained. Patients were referred to our outpatient thrombosis research center between January 1, 2014 and January 1, 2016, for thrombophilia/hypofibrinolysis evaluation based on lack of typical risk factors for OVO, or severely ischemic presentation. The 16 patients referred with RAO had normal carotid ultrasound and cardiac echocardiograms without any evidence for emboli causing RAO.
Patients with RVO showed dilation of retinal veins (all veins if a CRVO, and not all the veins if a BRVO) associated with intraretinal hemorrhages, retinal edema, and cotton wool spots limited in area by the drainage bed of the affected veins.18 Patients with RAO demonstrated retinal arterial narrowing, segmentation of the arterial blood column in some cases, and whitening of the retina due to opacification and thickening of the inner retina.18 In CRAO cases, a cherry-red spot was seen in the macula. Fluorescein angiography and optical coherence tomography were performed to corroborate the diagnosis depending on the preference of the referring ophthalmologist.
During the patients’ initial visit to our center, a detailed history, obstetrical–gynecological history, and physical examination were completed. The number of pregnancies, live births, spontaneous abortions, and elective abortions were recorded. When there was a history of spontaneous abortion, information was systematically obtained on maternal age, gravidity, smoking, alcohol, and cocaine use, in addition to whether there had been prior investigations of risk factors54,55 for spontaneous abortion. Information was gathered regarding any studies for chromosomal abnormalities,44 uterine structural issues (including septate uterus),47 maternal thyroid status, and maternal trauma. Maternal and family histories of previous thrombotic events were obtained. Serologic coagulation assays were done and polymerase chain reaction (PCR) analyses for thrombophilia and hypofibrinolysis were performed. Atherosclerotic risk factors were measured, including age, body mass index (BMI), smoking history, blood pressure, hemoglobin A1c, glucose, homocysteine, and triglyceride and cholesterol levels, including high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol.17
PCR measures56 were used to measure G1691A FVL, PTG, methylene tetrahydrofolate reductase C677T and A1298C mutations, and the plasminogen activator inhibitor-1 4G4G mutation. PCR measures for the thrombomodulin gene mutation were not obtained. In addition, serologic measures of thrombophilia20 were done, including anticardiolipin antibodies (ACLA) IgG and IgM, antigenic protein C, total and free protein S, antithrombin III, lupus anticoagulant, factors VIII and XI, and homocysteine. All PCR and serologic measures were done as previously described.17,18
After signed informed consent was obtained, healthy normal female volunteers (n=62) served as controls. They were documented by interview and physical examination to be free of acute and chronic disease, including any history or evidence of OVO.
Statistical methods
All statistical analyses were performed using SAS V9.4 (SAS institute Inc., Cary, NC, USA). Cases were compared to controls by Fisher’s exact test. Sample size was estimated based on our recent studies of 265 patients, 191 with ocular vein occlusion, and 74 with ocular artery occlusion, with comparison to 110 normal controls,20 where 50% of RVO patients had at least one of seven thrombophilias (FVL, prothrombin gene heterozygosity, low free protein S, high homocysteine, high factor VIII, factor XI, ACLA IgM high) vs 20% in controls. At least 39 subjects were required in each group to detect the difference at significance level alpha =0.05 with power 80%.
Results
As an entire cohort, the 76 females with RVO were more likely than the 62 normal female controls to have high homocysteine (24% vs 0%, P<0.0001), ACLA IgM (17% vs 3%, P=0.012), high factor VIII (>150%) (42% vs 11%, P<0.0001), and high factor XI (>150%) (22% vs 4%, P=0.004) (Figures 1 and 2).
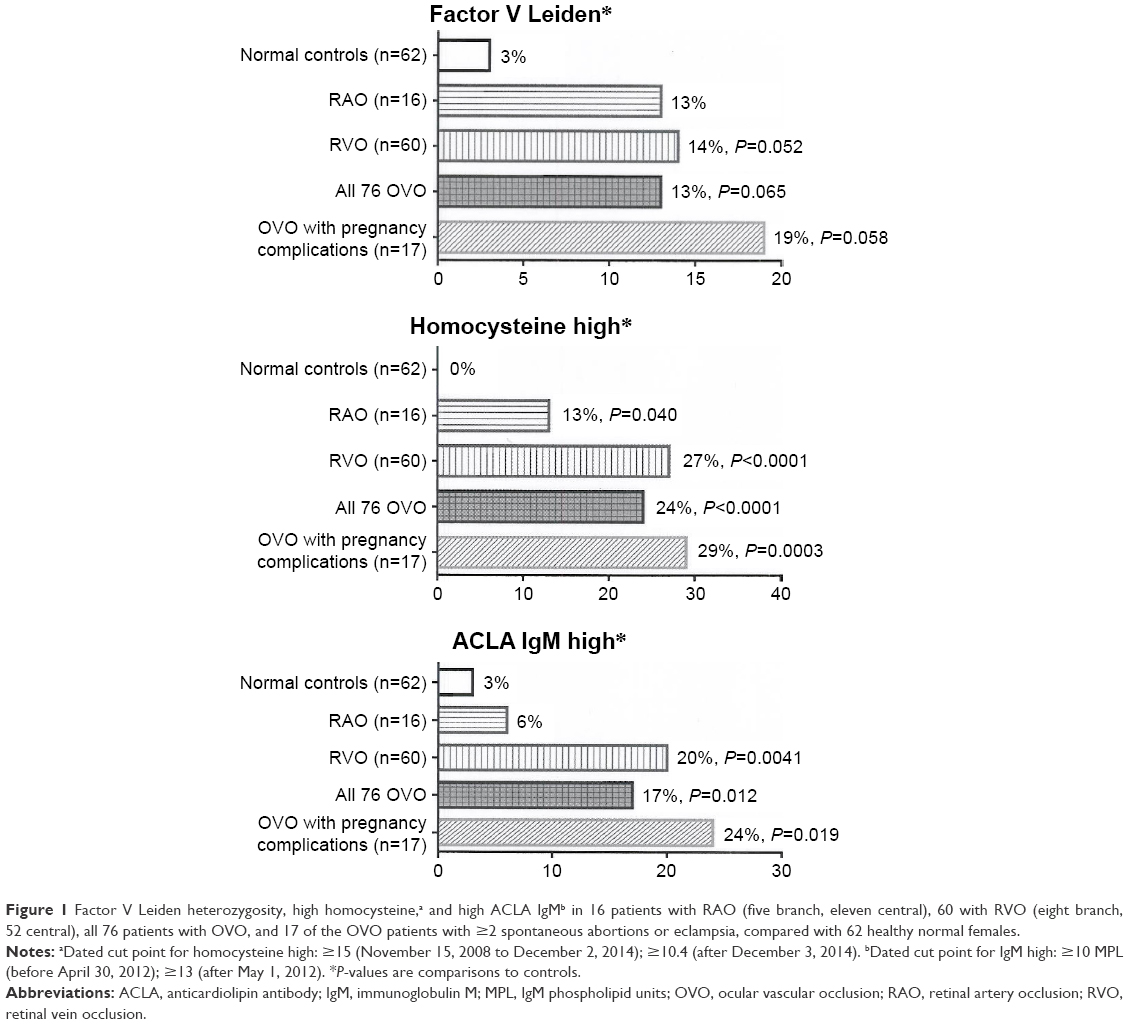 | Figure 1 Factor V Leiden heterozygosity, high homocysteine,a and high ACLA IgMb in 16 patients with RAO (five branch, eleven central), 60 with RVO (eight branch, 52 central), all 76 patients with OVO, and 17 of the OVO patients with ≥2 spontaneous abortions or eclampsia, compared with 62 healthy normal females. |
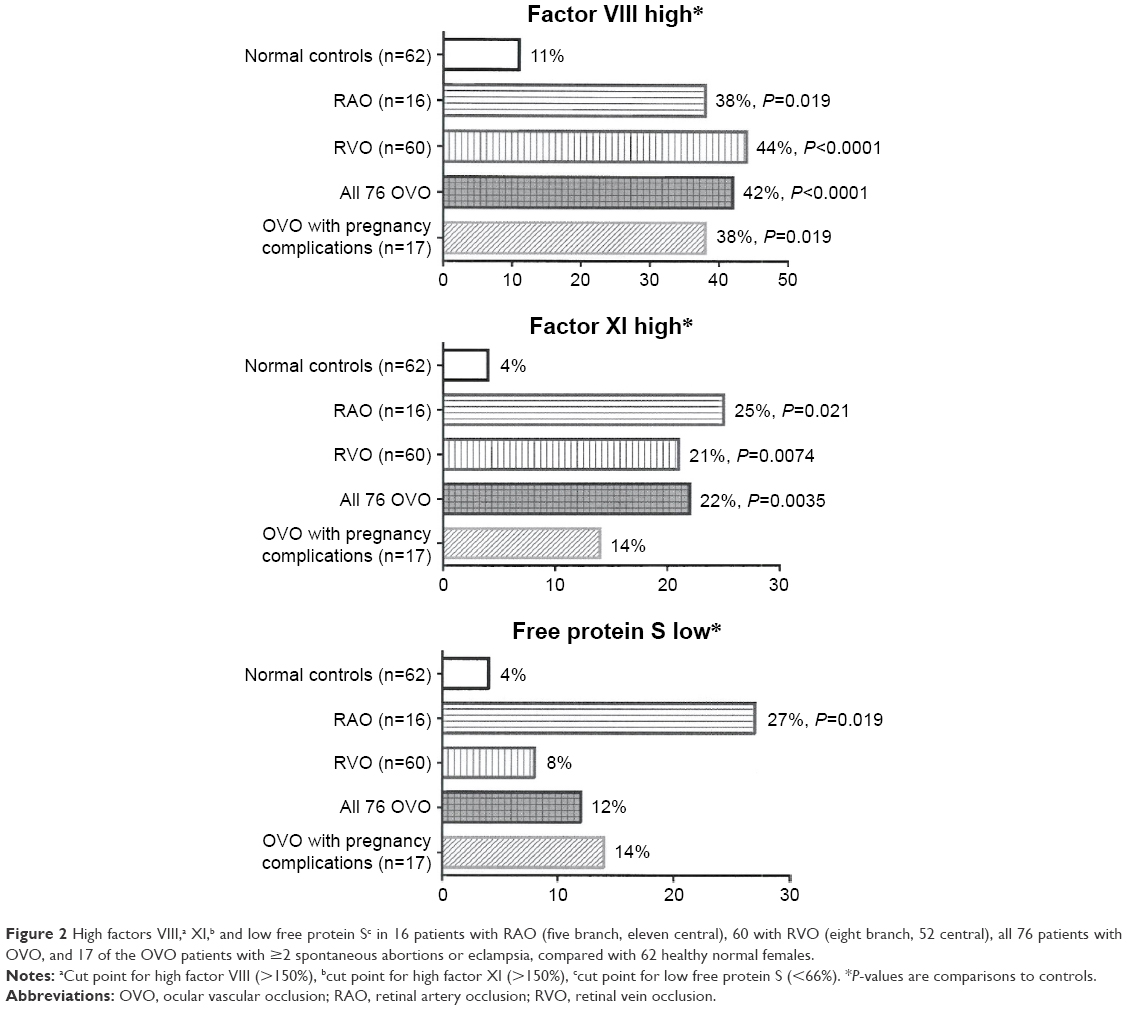 | Figure 2 High factors VIII,a XI,b and low free protein Sc in 16 patients with RAO (five branch, eleven central), 60 with RVO (eight branch, 52 central), all 76 patients with OVO, and 17 of the OVO patients with ≥2 spontaneous abortions or eclampsia, compared with 62 healthy normal females. |
Of the 76 females, 16 presented with RAO (eleven CRAO and five branch RAO), and 60 presented with RVO (52 CRVO and eight BRVO). Of the 76 women, 37 (49%) were ≤60 years of age and 48 (63%) ≤65 years of age. Homocysteine was high in 13% with RAO (P=0.04) and 27% with RVO (P<0.0001) compared to 0% in 62 healthy normal female controls (Figure 1). Factors VIII and XI were higher in 16 females with RAO (38% and 25%, respectively, [P=0.019, 0.021]) and in 60 RVO females (44% and 21%, respectively, [P=<0.0001, 0.0074]) than in normal female controls (11% and 4%, respectively) (Figure 2). The 16 females with RAO were more likely than normal female controls (27% vs 4%, P=0.019) to have low free protein S (<66%) (Figures 1 and 2). The 60 females with RVO were more likely to have high ACLA IgM than normal female controls (20% vs 3%, P=0.0041) (Figures 1 and 2).
Of the 76 females, 73 had a total of 244 pregnancies, 180 live births, and 57 spontaneous abortions. Five females (6.8%) had ≥3 consecutive pregnancy losses before 20 weeks (recurrent pregnancy loss57,58), ten (13.9%) experienced two consecutive pregnancy losses, and 26 (35.6%) had ≥1 pregnancy loss. None of the 57 spontaneous miscarriages in the 73 females could be attributed to alcohol or cocaine use, maternal infection or endocrine abnormalities, uterine structural abnormalities, poorly controlled maternal diabetes, maternal thyroid disorders, or maternal trauma. Cytogenetic studies of the postmiscarriage products of conception samples were done in only three cases, where eight, six, and four spontaneous unexplained abortions had occurred, without demonstration of cytogenetic abnormalities.54,55
Of the 76 females, 17 (23%) had ≥2 spontaneous abortions or eclampsia. Of these 17 females, ten had two spontaneous abortions, three had four, one had six, one had eight spontaneous abortions, and two had eclampsia. Compared to 62 normal female controls, these 17 females had high factor VIII (38% vs 11%, P=0.02), high homocysteine (29% vs 0%, P=0.0003), high ACLA IgM (24% vs 3%, P=0.02), and were marginally more likely to be heterozygous for the FVL mutation (19% vs 3%, P=0.058) (Figures 1 and 2).
Discussion
Since thrombophilia plays a significant role in the development of OVO,18,20,24,59,60 particularly in younger patients, and in patients without atherosclerosis but with insulin resistance syndrome risk factors, the ophthalmologist is often the first medical diagnostician to initiate steps to diagnose thrombophilia.8,12,20,21,24,30,53,61–69 Although all 76 females in the current study were referred to retinologists because of OVO, subsequent thrombophilia studies revealed not only an enrichment of familial thrombophilia in an OVO cohort but also emphasized the potential diagnostic and therapeutic payoffs obtained when the retinologist looks for thrombophilia in otherwise unexplained OVO. In the current study, congruent with our recent evaluation of 191 patients with RVO and 74 with RAO,20 the group of 76 females (16 with RAO, 60 with RVO) differed from 62 healthy female controls by having high homocysteine, high ACLA IgM, and high factors VIII and XI. RAO and RVO patients both were more likely than healthy normal controls to have high homocysteine, high factor VIII and XI.
Thrombophilia has been reported to play an important pathoetiologic role in RAO and RVO,18 as previously documented in this article, which is congruent with findings in our’s18,21,53 and other’s70–74 studies. Thrombophilia is a known pathoetiology for adverse obstetrical outcomes, including, as in the current study, miscarriage,75–80 recurrent miscarriage,48,49,57,81 pre-eclampsia,82,83 and eclampsia.84,85 Unique to this article is our emphasis on the often central diagnostic role of the ophthalmologist, who, by revealing the pathologic importance of thrombophilia in OVO, opens the gates to primary and secondary prevention and therapy of thrombosis in other vascular beds, including the uterus and placenta, as in this report.
A growing body of evidence highlights thrombophilia as an important cause for spontaneous miscarriage.48,49,75–80,86 Thrombophilia should be assessed in all females with recurrent fetal death,87 but thrombophilia is only one of multiple causes54,55 for spontaneous abortion, including fetal cytogenetic abnormalities,44 congenital abnormalities, illicit drug use, teratogens, maternal trauma, infection, uterine structural issues,45–47 maternal disease, including infection and endocrinopathies. In our cohort, where 73 females had one or more pregnancies with 57 spontaneous abortions, excepting a thrombophilic etiology in 12% to 42% of females, the varied other causes of spontaneous abortion44,54,55 were not identified.
In our cohort, referred solely by OVO, pregnancy loss was much greater than in the general population,57 recurrent pregnancy loss (three or more spontaneous unexplained abortions before 20 weeks’ gestation) occurred in 6.8% vs 0.4% to 1% in general populations, two consecutive losses in 12.3% vs 2% in general population, and 35.6% had ≥1 spontaneous pregnancy loses vs 15% in general population.
Normal pregnancy is characterized by an increase in thrombophilia,88 where a physiologic hyperestrogenic hypercoagulable state appears to be a physiological adaptive mechanism51 to prevent postpartum hemorrhage.50 Thrombophilia,89–94 producing placental insufficiency via thrombosis of the placental spiral arteries, causes spontaneous abortion; pre-eclampsia; eclampsia; and hemolysis, elevated liver enzymes, and low platelet count syndrome.95–100 Within this frame of reference, our current study revealed the 17 females, originally evaluated for RVOs and with two or more unexplained spontaneous pregnancy losses or eclampsia, as a group had high homocysteine, high factor VIII, high ACLA IgM, and increased FVL rates compared with normal female controls. We speculate that thrombophilia associated with RAO and RVO, amplified by the thrombophilia of pregnancy, contributes to placental insufficiency and spontaneous abortion. This finding is congruent with our recent report18 that, of 17 females with FVL or PTG mutations, seven (41%) experienced at least one unexplained spontaneous abortion.
Although prospective with regard to the study of the etiology of OVO, our study is limited by being retrospective with regard to assessment of adverse pregnancy outcomes (spontaneous abortion, eclampsia). A second limitation of the study involves the expensive nature of laboratory assessment of thrombophilia, which often is not fully covered by private health insurance or Medicare or Medicaid.
Conclusion
In females lacking typical risk factors for RVO or severe ischemic presentation, by diagnosing thrombophilia as an etiology for OVO, the ophthalmologist opens a window to family screening and preventive therapy, with particular relevance to pregnancy outcomes and venous thromboembolism. The diagnosis of an underlying thrombophilia is important not only for the management of OVO but also for the success of the pregnancy, allowing timely thromboprophylaxis101–103 to prevent maternal thrombosis and pregnancy loss.
Disclosure
The authors report no conflicts of interest in this work.
References
Mohamed Q, McIntosh RL, Saw SM, Wong TY. Interventions for central retinal vein occlusion: an evidence-based systematic review. Ophthalmology. 2007;114(3):507–519. | ||
Group EDC-CS. Risk factors for central retinal vein occlusion. Arch Ophthalmol. 1996;114(5):545–554. | ||
Stem MS, Talwar N, Comer GM, Stein JD. A longitudinal analysis of risk factors associated with central retinal vein occlusion. Ophthalmology. 2013;120(2):362–370. | ||
Weger M, Renner W, Pinter O, et al. Role of factor V Leiden and prothrombin 20210A in patients with retinal artery occlusion. Eye (Lond). 2003;17(6):731–734. | ||
Hayreh SS, Zimmerman B, McCarthy MJ, Podhajsky P. Systemic diseases associated with various types of retinal vein occlusion. Am J Ophthalmol. 2001;131(1):61–77. | ||
Prisco D, Marcucci R, Bertini L, Gori AM. Cardiovascular and thrombophilic risk factors for central retinal vein occlusion. Eur J Intern Med. 2002;13(3):163–169. | ||
Recchia FM, Brown GC. Systemic disorders associated with retinal vascular occlusion. Curr Opin Ophthalmol. 2000;11(6):462–467. | ||
Backhouse O, Parapia L, Mahomed I, Lee D. Familial thrombophilia and retinal vein occlusion. Eye (Lond). 2000;14(Pt 1):13–17. | ||
Rehak M, Rehak J, Müller M, et al. The prevalence of activated protein C (APC) resistance and factor V Leiden is significantly higher in patients with retinal vein occlusion without general risk factors. Thromb Haemost. 2008;99(5):925–929. | ||
Cheung N, Klein R, Wang J, et al. Traditional and novel cardiovascular risk factors for retinal vein occlusion: the multiethnic study of atherosclerosis. Invest Ophthalmol Vis Sci. 2008;49(10):4297–4302. | ||
O’Mahoney P, Wong T, Ray J. Retinal vein occlusion and traditional risk factors for atherosclerosis. Arch Ophthalmol. 2008;126(5):692–699. | ||
Bick RL, Alfar H, Goedecke C. Thrombophilic causes of retinal vascular thrombosis: etiology and treatment outcomes. Clin Appl Thromb Hemost. 2002;8(4):315–318. | ||
Karia N. Retinal vein occlusion: pathophysiology and treatment options. Clin Ophthalmol. 2010;4:809–816. | ||
Beaumont PE, Kang HK. Clinical characteristics of retinal venous occlusions occurring at different sites. Br J Ophthalmol. 2002;86(5):572–580. | ||
Hitchings RA, Spaeth GL. Chronic retinal vein occlusion in glaucoma. Br J Ophthalmol. 1976;60(10):694–699. | ||
Dryden RM. Central retinal vein occlusions and chronic simple glaucoma. Arch Ophthalmol. 1965;73:659–663. | ||
Glueck CJ, Wang P, Hutchins R, Petersen MR, Golnik K. Ocular vascular thrombotic events: central retinal vein and central retinal artery occlusions. Clin Appl Thromb Hemost. 2008;14(3):286–294. | ||
Schockman S, Glueck CJ, Hutchins RK, Patel J, Shah P, Wang P. Diagnostic ramifications of ocular vascular occlusion as a first thrombotic event associated with factor V Leiden and prothrombin gene heterozygosity. Clin Ophthalmol. 2015;9:591–600. | ||
Glueck CJ, Goldenberg N, Bell H, Golnik K, Wang P. Amaurosis fugax: associations with heritable thrombophilia. Clin Appl Thromb Hemost. 2005;11(3):235–241. | ||
Glueck CJ, Hutchins RK, Jurantee J, Khan Z, Wang P. Thrombophilia and retinal vascular occlusion. Clin Ophthalmol. 2012;6:1377–1384. | ||
Glueck CJ, Ping W, Hutchins R, Petersen MR, Golnik K. Ocular vascular thrombotic events: central retinal vein and central retinal artery occlusions. Clin Appl Thromb Hemost. 2008;14(3):286–294. | ||
Glueck CJ, Wang P, Bell H, Rangaraj V, Goldenberg N. Nonarteritic anterior ischemic optic neuropathy: associations with homozygosity for the C677T methylenetetrahydrofolate reductase mutation. J Lab Clin Med. 2004;143(3):184–192. | ||
Glueck CJ, Wang P, Bell H, Rangaraj V, Goldenberg N. Associations of thrombophilia, hypofibrinolysis, and retinal vein occlusion. Clin Appl Thromb Hemost. 2005;11(4):375–389. | ||
Sottilotta G, Oriana V, Latella C, et al. Role of hyperhomocystinemia in retinal vascular occlusive disease. Clin Appl Thromb Hemost. 2007;13(1):104–107. | ||
Yau JW, Lee P, Wong TY, Best J, Jenkins A. Retinal vein occlusion: an approach to diagnosis, systemic risk factors and management. Intern Med J. 2008;38(12):904–910. | ||
Bick RL. Antiphospholipid thrombosis syndromes. Clin Appl Thromb Hemost. 2001;7(4):241–258. | ||
Williamson TH, Rumley A, Lowe GD. Blood viscosity, coagulation, and activated protein C resistance in central retinal vein occlusion: a population controlled study. Br J Ophthalmol. 1996;80(3):203–208. | ||
Larsson J, Olafsdottir E, Bauer B. Activated protein C resistance in young adults with central retinal vein occlusion. Br J Ophthalmol. 1996;80(3):200–202. | ||
Ben-Ami R, Zeltser D, Leibowitz I, Berliner SA. Retinal artery occlusion in a patient with factor V Leiden and prothrombin G20210A mutations. Blood Coagul Fibrinolysis. 2002;13(1):57–59. | ||
Aras S, Yilmaz G, Alpas I, Baltaci V, Tayanç E, Aydin P. Retinal vein occlusion and factor V Leiden and prothrombin 20210 G:A mutations. Eur J Ophthalmol. 2001;11(4):351–355. | ||
Demirci FYK, Güney DB, Akarçay K, et al. Prevalence of factor V Leiden in patients with retinal vein occlusion. Acta Ophthalmol Scand. 1999;77(6):631–633. | ||
Larsson J, Hillarp A. The prothrombin gene G20210A mutation and the platelet glycoprotein IIIa polymorphism PIA2 in patients with central retinal vein occlusion. Thromb Res. 1999;96(4):323–327. | ||
Janssen MCH, Heijer MD, Cruysberg JRM, Wollersheim H, Bredie SJH. Retinal vein occlusion: A form of venous thrombosis or a complication of atherosclerosis? J Thromb Haemost. 2005;93(6):1021–1026. | ||
Fegan CD. Central retinal vein occlusion and thrombophilia. Eye (Lond). 2002;16(1):98–106. | ||
Turello M, Pasca S, Daminato R, et al. Retinal vein occlusion: evaluation of “classic” and “emerging” risk factors and treatment. J Thromb Thrombolysis. 2010;29(4):459–464. | ||
Cahill MT, Stinnett SS, Fekrat S. Meta-analysis of plasma homocysteine, serum folate, serum vitamin B(12), and thermolabile MTHFR genotype as risk factors for retinal vascular occlusive disease. Am J Ophthalmol. 2003;136(6):1136–1150. | ||
Biousse V, Newman NJ, Sternberg PJ. Retinal vein occlusion and transient monocular visual loss associated with hyperhomocystinemia. Am J Ophthalmol. 1997;124(2):257–260. | ||
McCully KS. Homocysteine and vascular disease. Nat Med. 1996;2(4):386–389. | ||
Wald DS, Law M, Morris JK. Homocysteine and cardiovascular disease: evidence on causality from a meta-analysis. BMJ. 2002;325(7374):1202. | ||
Simsek E, Yesilyurt A, Pinarli F, Eyerci N, Ulus AT. Combined genetic mutations have remarkable effect on deep venous thrombosis and/or pulmonary embolism occurrence. Gene. 2014;536(1):171–176. | ||
Seligsohn U, Lubetsky A. Genetic susceptibility to venous thrombosis. N Engl J Med. 2001;344(16):1222–1231. | ||
Poort SR, Rosendaal FR, Reitsma PH, Bertina RM. A common genetic variation in the 3′-untranslated region of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase in venous thrombosis. Blood. 1996;88(1):3698–3703. | ||
Koster T, Rosendaal FR, Ronde Hd, Briët E, Vandenbroucke JP, Bertina RM. Venous thrombosis due to poor anticoagulant response to activated protein C: Leiden Thrombophilia Study. Lancet. 1993;342(8886–8887):1503–1506. | ||
Levy B, Sigurjonsson S, Pettersen B, et al. Genomic imbalance in products of conception: single-nucleotide polymorphism chromosomal microarray analysis. Obstet Gynecol. 2014;124(2 Pt 1):202–209. | ||
Mollo A, De Franciscis P, Colacurci N, et al. Hysteroscopic resection of the septum improves the pregnancy rate of women with unexplained infertility: a prospective controlled trial. Fertil Steril. 2009;91(6):2628–2631. | ||
Shokeir T, Abdelshaheed M, El-Shafie M, Sherif L, Badawy A. Determinants of fertility and reproductive success after hysteroscopic septoplasty for women with unexplained primary infertility: a prospective analysis of 88 cases. Eur J Obstet Gynecol Reprod Biol. 2011;155(1):54–57. | ||
Tomazevic T, Ban-Frangez H, Virant-Klun I, Verdenik I, Pozlep B, Vrtacnik-Bokal E. Septate, subseptate and arcuate uterus decrease pregnancy and live birth rates in IVF/ICSI. Reprod Biomed Online. 2010;21(5):700–705. | ||
Rey E, Kahn SR, David M, Shrier I. Thrombophilic disorders and fetal loss: a meta-analysis. Lancet. 2003;361(9361):901–908. | ||
Preston FE, Rosendaal FR, Walker ID, et al. Increased fetal loss in women with heritable thrombophilia. Lancet. 1996;348(9032):913–916. | ||
James AH. Thrombosis in pregnancy and maternal outcomes. Birth Defects Res C Embryo Today. 2015;105(3):159–166. | ||
Eldor A. Thrombophilia, thrombosis and pregnancy. Thromb Haemost. 2001;86(1):104–111. | ||
Kamel H, Navi BB, Sriram N, Hovsepian DA, Devereux RB, Elkind MS. Risk of a thrombotic event after the 6-week postpartum period. N Engl J Med. 2014;370(14):1307–1315. | ||
Glueck CJ, Wang P. Ocular vascular thrombotic events: a diagnostic window to familial thrombophilia (compound factor V Leiden and prothrombin gene heterozygosity) and thrombosis. Clin Appl Thromb Hemost. 2009;15(1):12–18. | ||
Risch HA, Weiss NS, Clarke EA, Miller AB. Risk factors for spontaneous abortion and its recurrence. Am J Epidemiol. 1988;128(2):420–430. | ||
Rasch V. Cigarette, alcohol, and caffeine consumption: risk factors for spontaneous abortion. Acta Obstet Gynecol Scand. 2003;82(2):182–188. | ||
Glueck CJ, Freiberg RA, Wang P. Heritable thrombophilia-hypofibrinolysis and osteonecrosis of the femoral head. Clin Orthop Relat Res. 2008;466(5):1034–1040. | ||
Salat-Baroux J. [Recurrent spontaneous abortions]. Reprod Nutr Dev. 1988;28(6B):1555–1568. | ||
Ford HB, Schust DJ. Recurrent pregnancy loss: etiology, diagnosis, and therapy. Rev Obstet Gynecol. 2009;2(2):76–83. | ||
Rehak M, Krcova V, Slavik L, et al. The role of thrombophilia in patients with retinal vein occlusion and no systemic risk factors. Can J Ophthalmol. 2010;45(2):171–175. | ||
Chapin J, Carlson K, Christos PJ, DeSancho MT. Risk factors and treatment strategies in patients with retinal vascular occlusions. Clin Appl Thromb Hemost. 2015;21(7):672–677. | ||
Rehak J, Dusek L, Chrapek O, Fric E, Rehak M. Initial visual acuity is an important prognostic factor in patients with branch retinal vein occlusion. Ophthalmic Res. 2010;45(4):204–209. | ||
Weger M, Stanger O, Deutschmann H, et al. Hyperhomocyst(e)inemia and MTHFR C677T genotypes in patients with central retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol. 2002;240(4):286–290. | ||
Prisco D, Marcucci R. Retinal vein thrombosis: risk factors, pathogenesis and therapeutic approach. Pathophysiol Haemost Thromb. 2002;32(5–6):308–311. | ||
Rehak M, Krcova V, Fric E, et al. [Disturbances of the plasma coagulation defects in retinal venous occlusions]. Cesk Slov Oftalmol. 2008;64(3):108–111. | ||
Demirci FY, Kucukkaya R, Akarcay K, et al. Ocular involvement in primary antiphospholipid syndrome. Ocular involvement in primary APS. Int Ophthalmol. 1998;22(6):323–329. | ||
Larsson J. Central retinal artery occlusion in a patient homozygous for factor V Leiden. Am J Ophthalmol. 2000;129(6):816–817. | ||
Larsson J, Hillarp A, Olafsdottir E, Bauer B. Activated protein C resistance and anticoagulant proteins in young adults with central retinal vein occlusion. Acta Ophthalmol Scand. 1999;77(6):634–637. | ||
Cahill M, Karabatzaki M, Meleady R, et al. Raised plasma homocysteine as a risk factor for retinal vascular occlusive disease. Br J Ophthalmol. 2000;84(2):154–157. | ||
Greiner K, Hafner G, Dick B, Peetz D, Prellwitz W, Pfeiffer N. Retinal vascular occlusion and deficiencies in the protein C pathway. Am J Ophthalmol. 1999;128(1):69–74. | ||
Desai S, Rai N, Kulkarni P, Natarajan S. Combined CRVO with CRAO in a patient with protein C deficiency. Retin Cases Brief Rep. 2014;8(2):145–149. | ||
Kolar P. Risk factors for central and branch retinal vein occlusion: a meta-analysis of published clinical data. J Ophthalmol. 2014;2014:724780. | ||
Jaulim A, Ahmed B, Khanam T, Chatziralli IP. Branch retinal vein occlusion: epidemiology, pathogenesis, risk factors, clinical features, diagnosis, and complications. an update of the literature. Retina. 2013;33(5):901–910. | ||
Incorvaia C, Bandello F, Parmeggiani F, D’Angelo S, Costagliola C, Sebastiani A. Recurrent central retinal vein occlusion in a young thrombophilic patient with factor V Leiden mutation. Eur J Ophthalmol. 2002;12(2):131–134. | ||
Lerche RC, Wilhelm C, Eifrig B, Richard G. [Thrombophilia factors as inducers of retinal vascular occlusion]. Ophthalmologe. 2001;98(6):529–534. | ||
Dizon-Townson D, Miller C, Sibai B, et al. The relationship of the factor V Leiden mutation and pregnancy outcomes for mother and fetus. Obstet Gynecol. 2005;106(3):517–524. | ||
Said JM, Higgins JR, Moses EK, et al. Inherited thrombophilia polymorphisms and pregnancy outcomes in nulliparous women. Obstet Gynecol. 2010;115(1):5–13. | ||
Murphy RP, Donoghue C, Nallen RJ, et al. Prospective evaluation of the risk conferred by factor V Leiden and thermolabile methylenetetrahydrofolate reductase polymorphisms in pregnancy. Arterioscler Thromb Vasc Biol. 2000;20(1):266–270. | ||
Clark P, Walker ID, Govan L, Wu O, Greer IA. The GOAL study: a prospective examination of the impact of factor V Leiden and ABO(H) blood groups on haemorrhagic and thrombotic pregnancy outcomes. Br J Haematol. 2008;140(2):236–240. | ||
Lindqvist PG, Svensson PJ, Marsaal K, Grennert L, Luterkort M, Dahlback B. Activated protein C resistance (FV:Q506) and pregnancy. Thromb Haemost. 1999;81(4):532–537. | ||
Silver RM, Zhao Y, Spong CY, et al. Prothrombin gene G20210A mutation and obstetric complications. Obstet Gynecol. 2010;115(1):14–20. | ||
Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA. 2002;287(3):356–359. | ||
Berks D, Duvekot JJ, Basalan H, De Maat MP, Steegers EA, Visser W. Associations between phenotypes of preeclampsia and thrombophilia. Eur J Obstet Gynecol Reprod Biol. 2015;194:199–205. | ||
Simcox LE, Ormesher L, Tower C, Greer IA. Thrombophilia and pregnancy complications. Int J Mol Sci. 2015;16(12):28418–28428. | ||
Dehkordi MA, Soleimani A, Haji-Gholami A, Vardanjani AK, Dehkordi SA. Association of deficiency of coagulation factors (Prs, Prc, ATIII) and FVL positivity with preeclampsia and/or eclampsia in pregnant women. Int J Hematol Oncol Stem Cell Res. 2014;8(4):5–11. | ||
Wang X, Bai T, Liu S, Pan H, Wang B. Association between thrombophilia gene polymorphisms and preeclampsia: a meta-analysis. PLoS One. 2014;9(6):e100789. | ||
Kjellberg U, van Rooijen M, Bremme K, Hellgren M. Factor V Leiden mutation and pregnancy-related complications. Am J Obstet Gynecol. 2010;203(5):469, e1–e8. | ||
Barros VI, Igai AM, Andres Mde P, Francisco RP, Zugaib M. [Pregnancy outcome and thrombophilia of women with recurrent fetal death]. Rev Bras Ginecol Obstet. 2014;36(2):50–55. | ||
Cerneca F, Ricci G, Simeone R, Malisano M, Alberico S, Guaschino S. Coagulation and fibrinolysis changes in normal pregnancy. Increased levels of procoagulants and reduced levels of inhibitors during pregnancy induce a hypercoagulable state, combined with a reactive fibrinolysis. Eur J Obstet Gynecol Reprod Biol. 1997;73(1):31–36. | ||
Glueck CJ, Awadalla SG, Phillips H, Cameron D, Wang P, Fontaine RN. Polycystic ovary syndrome, infertility, familial thrombophilia, familial hypofibrinolysis, recurrent loss of in vitro fertilized embryos, and miscarriage. Fertil Steril. 2000;74(2):394–397. | ||
Mekaj Y, Lulaj S, Daci F, et al. Prevalence and role of antithrombin III, protein C and protein S deficiencies and activated protein C resistance in Kosovo women with recurrent pregnancy loss during the first trimester of pregnancy. J Hum Reprod Sci. 2015;8(4):224–229. | ||
Wang Y, Lin X, Wu Q, et al. Thrombophilia markers in patients with recurrent early miscarriage. Clin Lab. 2015;61(11):1787–1794. | ||
Glueck CJ, Gogenini S, Munjal J, Tracy T, Pranikoff J, Wang P. Factor V Leiden mutation: a treatable etiology for sporadic and recurrent pregnancy loss. Fertil Steril. 2008;89(2):410–416. | ||
Glueck CJ, Pranikoff J, Aregawi D, et al. The factor V Leiden mutation, high factor VIII, and high plasminogen activator inhibitor activity: etiologies for sporadic miscarriage. Metabolism. 2005;54(10):1345–1349. | ||
O’Donnell CI, Glueck CJ, Fingerlin TE, Glueck DH. A likelihood model that accounts for censoring due to fetal loss can accurately test the effects of maternal and fetal genotype on the probability of miscarriage. Hum Hered. 2009;67(1):57–65. | ||
Besharat M, Tabandeh A, Keshtkar A, Mobasheri E, Besharat S, Joshaghani H. Evaluation of some plasma coagulation factors in women with spontaneous miscarriage. Int J Fertil Steril. 2015;9(3):309–312. | ||
Bouvier S, Cochery-Nouvellon E, Lavigne-Lissalde G, et al. Comparative incidence of pregnancy outcomes in thrombophilia-positive women from the NOH-APS observational study. Blood. 2014;123(3):414–421. | ||
de Jong PG, Goddijn M, Middeldorp S. Antithrombotic therapy for pregnancy loss. Hum Reprod Update. 2013;19(6):656–673. | ||
Glueck CJ, Wang P, Goldenberg N, Sieve L. Pregnancy loss, polycystic ovary syndrome, thrombophilia, hypofibrinolysis, enoxaparin, metformin. Clin Appl Thromb Hemost. 2004;10(4):323–334. | ||
Lino FL, Traina E, Barreto JA, Moron AF, Mattar R. Thrombophilic mutations and polymorphisms, alone or in combination, and recurrent spontaneous abortion. Clin Appl Thromb Hemost. 2015;21(4):365–372. | ||
Mazzucconi MG, De Sanctis V, Alfo M, et al. Maternal thrombophilia and adverse pregnancy outcome: a case-control study. Acta Haematol. 2015;133(2):242–248. | ||
Grandone E, De Stefano V, Rossi E, Cappucci F, Colaizzo D, Margaglione M. Antithrombotic prophylaxis during pregnancy in women with deficiency of natural anticoagulants. Blood Coagul Fibrinolysis. 2008;19(3):226–230. | ||
Ramidi G, Khan N, Glueck CJ, Wang P, Goldenberg N. Enoxaparin-metformin and enoxaparin alone may safely reduce pregnancy loss. Transl Res. 2009;153(1):33–43. | ||
Brenner B. Thrombophilia and pregnancy loss in first intended pregnancy. J Thromb Haemost. 2005;3(10):2176–2177. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.