")
Back to Journals » Journal of Inflammation Research » Volume 15
Resolved Hypereosinophilic Syndrome and Immune Thrombocytopenic Purpura in Ulcerative Colitis Patients Post Colectomy: A Case Series and Literature Review
Authors Subki AH , Bokhary MI, Alandijani SA, Aljehani MA, Alharbi AW, Alzahrani M, Almuhammadi SS, Albeirouti BT, Abduljabar MA, Danese S
Received 14 July 2022
Accepted for publication 3 November 2022
Published 21 November 2022 Volume 2022:15 Pages 6373—6380
DOI https://doi.org/10.2147/JIR.S365094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Ahmed Hussein Subki,1 Manal Ismail Bokhary,1 Sultan Abdulrahman Alandijani,1 Mohannad Abdulrahman Aljehani,1 Ahmed Wasel Alharbi,1 May Alzahrani,1 Saud Suliman Almuhammadi,2 Bassim Tahseen Albeirouti,3 Mohamed Abdulmajid Abduljabar,1 Silvio Danese4
1Department of Internal Medicine, King Faisal Specialist Hospital & Research Centre, Jeddah, Saudi Arabia; 2Department of Surgery, King Faisal Specialist Hospital & Research Centre, Jeddah, Saudi Arabia; 3Adult Hematology/Bone Marrow Transplant (BMT) Section, Department of Oncology, King Faisal Specialist Hospital and Research Centre, Jeddah, Saudi Arabia; 4Gastroenterology and Endoscopy, IRCCS San Raffaele Hospital and Vita-Salute San Raffaele University, Milan, Italy
Correspondence: Ahmed Hussein Subki; Manal Ismail Bokhary, Department of Internal Medicine, King Faisal Specialist Hospital & Research Centre, P.O.Box No 40047, Jeddah, 21499, Saudi Arabia, Email [email protected]; [email protected]
Introduction: Hypereosinophilic syndrome (HES) and immune thrombocytopenic purpura (ITP) have been reported to co-occur with ulcerative colitis (UC). However, the exact pathogenic mechanisms of their occurrence remain elusive. In this article, we aim to describe two cases of UC patients who developed refractory HES and ITP and elaborate on their potential pathogenesis.
Case Study: We report two middle-aged patients diagnosed with UC. The first patient developed HES that was refractory to conventional medical therapy of idiopathic HES, and the second developed refractory ITP that failed steroid and immunosuppressive therapy. Both conditions improved considerably following colectomy, suggesting they are of a reactive rather than idiopathic nature.
Conclusion: In patients with UC and refractory comorbid HES or ITP, the reactive nature of these comorbidities should be taken into consideration, and colectomy, therefore, should be considered if clinically indicated.
Keywords: hypereosinophilic syndrome, immune thrombocytopenic purpura, colectomy, ulcerative colitis
Introduction
Ulcerative colitis (UC) is an immune-mediated inflammatory bowel disease (IBD) mediated by complex pathogenic mechanisms involving both innate and acquired immune responses in genetically susceptible individuals.1 The gastrointestinal tract (GIT) has unique features that make it vulnerable to immune-mediated disorders.2 These features include the expression of class II major histocompatibility complex (MHC) on the intestinal epithelial cells surface, the antigen-translocation ability of the M cells, the antigen-processing ability of the Peyer’s patch, and immunoglobulin A (IgA) secretion.2–4 Such unique features enable the GIT to play key roles in immune responses, such as cell-mediated responses (eg, natural and antibody-dependent cytotoxicity), immediate-type hypersensitivity reaction, secretion of immunoglobulins (ie, IgA, IgD, IgE, IgG, and IgM), exporting immune cells to systemic lymphoid sites, and immune tolerance.2–4 When functioning in normal physiologic conditions, these immune responses protect the host from both commensal and invasive microorganisms.2–4
In the context of immune system dysregulation, however, the intestinal immune responses become pathogenic. In patients with UC, specific – yet unknown – environmental factors initiate and perpetuate pathogenic mucosal immune responses in genetically susceptible individuals.5 A complex inflammatory milieu of innate and adaptive immune cells infiltrates the intestinal lamina propria.5 As a part of innate immune responses, neutrophil survival is promoted, resulting in excess release of pro-inflammatory cytokines, reactive oxygen species (ROS), matrix metalloproteinases, and subsequent inflammatory tissue damage.5,6 The neutrophils then undergo uncontrolled necrosis and/or necroptosis, promoting a prominent serological response to perinuclear anti-p-neutrophil cytoplasmic antibodies (p-ANCA).7 Eosinophils migrate to the intestinal mucosa in response to eotaxins, especially eotaxin-1.8,9 Monocytes and macrophages also are recruited and release their pro-inflammatory cytokines, eg, interleukin-1 (IL-1), IL-6, and tumor necrosis factor-alpha (TNF-α).10 The released cytokines drive aberrant adaptive immune responses.11 Traditionally, the adaptive immune responses are mediated predominantly by T-helper 2 (Th2) responses (ie, elevated IL-4 and IL-13 levels) more than Th1/Th17 responses.12
Immune thrombocytopenia (ITP) is an immune-mediated disorder reported to occur in patients with UC.13,14 Similarly to UC, the pathophysiology of ITP comprises complex B- and T-cell immune-mediated mechanisms.15 Platelets in ITP are destroyed in the blood, liver, and spleen. In the blood, the platelet destruction occurs via complement-mediated cytotoxicity, ie, the synthesized antibodies bind to the platelet’s surface glycoprotein, leading to activation of the classical complement pathway, formation of membrane attack complex (MAC), and, subsequently, platelet lysis.16 In the spleen, the opsonized platelets are phagocytosed by splenic macrophages.17 Simultaneously, bone marrow production is defective due to the involvement of the megakaryocytes with the autoimmune attack. Destruction of the megakaryocytes in the bone marrow is mediated by both antibody-dependent cellular cytotoxicity (ADCC) and cytotoxic T-lymphocyte-mediated cytotoxicity.15
Hypereosinophilic syndromes (HES) are a group of disorders that have also been reported to co-occur with UC.18,19 They are characterized by sustained elevation of eosinophilic count (≥1.5*109/L for at least six consecutive months) and organ damage due to eosinophilic infiltration.20 Several pathogenic mechanisms have been proposed in HES, ie, overproduction of eosinophilopoietic cytokines, promoting the eosinophil activity, and defective physiological suppression of eosinophils.20,21 Eosinophils production from the bone marrow is regulated by specific cytokines, ie, IL-3, IL-5, and granulocyte-macrophage colony-stimulating factor (GM-CSF).20 Overproduction of eosinophils in HES is proposed to be either due to the primary involvement of myeloid cells (ie, creation of the FIP1L1-PDGFRA fusion gene) or excessive production of IL-5 from clonally expanded T cells.22
In the literature, co-occurrence of ITP and HES with UC has been reported.13,14,18,19,23 The clinical presentation, treatment outcome, and prognosis of these cases vary. To date, the exact etiology of the occurrence of such comorbidities remains to be elucidated. However, evidence from the previous literature suggests molecular mimicry as a potential pathogenic mechanism for their co-occurrence.24 In this article, we present a case of HES and a case of ITP occurring in the context of active ulcerative pancolitis that was refractory to medical treatment and only responded to surgical colectomy.
Case Series
Case 1: Refractory HES Concomitant with UC
Our first case was a 24-year-old non-smoker gentleman diagnosed with UC since childhood. He was first seen at our tertiary center in May 2017 after being referred by his treating physician due to steroid-dependent colitis (Table 1). Throughout the follow-up in our medical facility, he failed all medical management lines for UC. In March 2020, the patient was noted to have persistent leukocytosis with eosinophilia (white blood cells (WBCs) 18,150 cells/cc3, absolute eosinophilic count 1880 cells/µL), anemia (hemoglobin (Hb) 9.5 g/dL, positive spherocytes), and reticulocytosis (reticulocytes count 4.83%). The patient was referred to the hematology department where secondary etiologies of eosinophilia were ruled out with an extensive work-up. Our patient had a persistent cholestatic derangement in the liver profile in the form of elevated alkaline phosphatase and hyperbilirubinemia since March 2019, for which magnetic resonance cholangiopancreatography was performed on the 30th of January 2020. It showed intrahepatic biliary ductal irregularities, supporting primary sclerosing cholangitis (PSC) given the background of UC, especially after ruling out the other common etiologies. Furthermore, the patient was also assessed by hematology following their workup that showed positive lupus anticoagulant on the 21st of September 2020 and labeled as antiphospholipid syndrome, for which he was started on lifelong anticoagulation therapy. Following investigations and multidisciplinary consultations from the gastroenterology, immunology, hematology, and rheumatology specialists, the patient was diagnosed as a case of HES with a background of UC, autoimmune hemolytic anemia, PSC, and APS. Despite this, the eosinophilia was persistent and reached up to 2400 cells/µL. A colonoscopy performed on the 17th of December 2020 showed severe pancolitis (Mayo Score 3). The patient failed mesalamine, methotrexate, adalimumab, infliximab, and vedolizumab. The patient was scheduled for a total colectomy with ileostomy as a case of UC refractory to medical therapy, and the surgery was carried out on January 11th, 2021. On February 3rd, 2021, the patient was seen for follow-up. His complete blood count (CBC) showed a reduction in the WBCs count and an improvement in anemia. On December 8th, 2021, the patient’s eosinophilia was resolved.
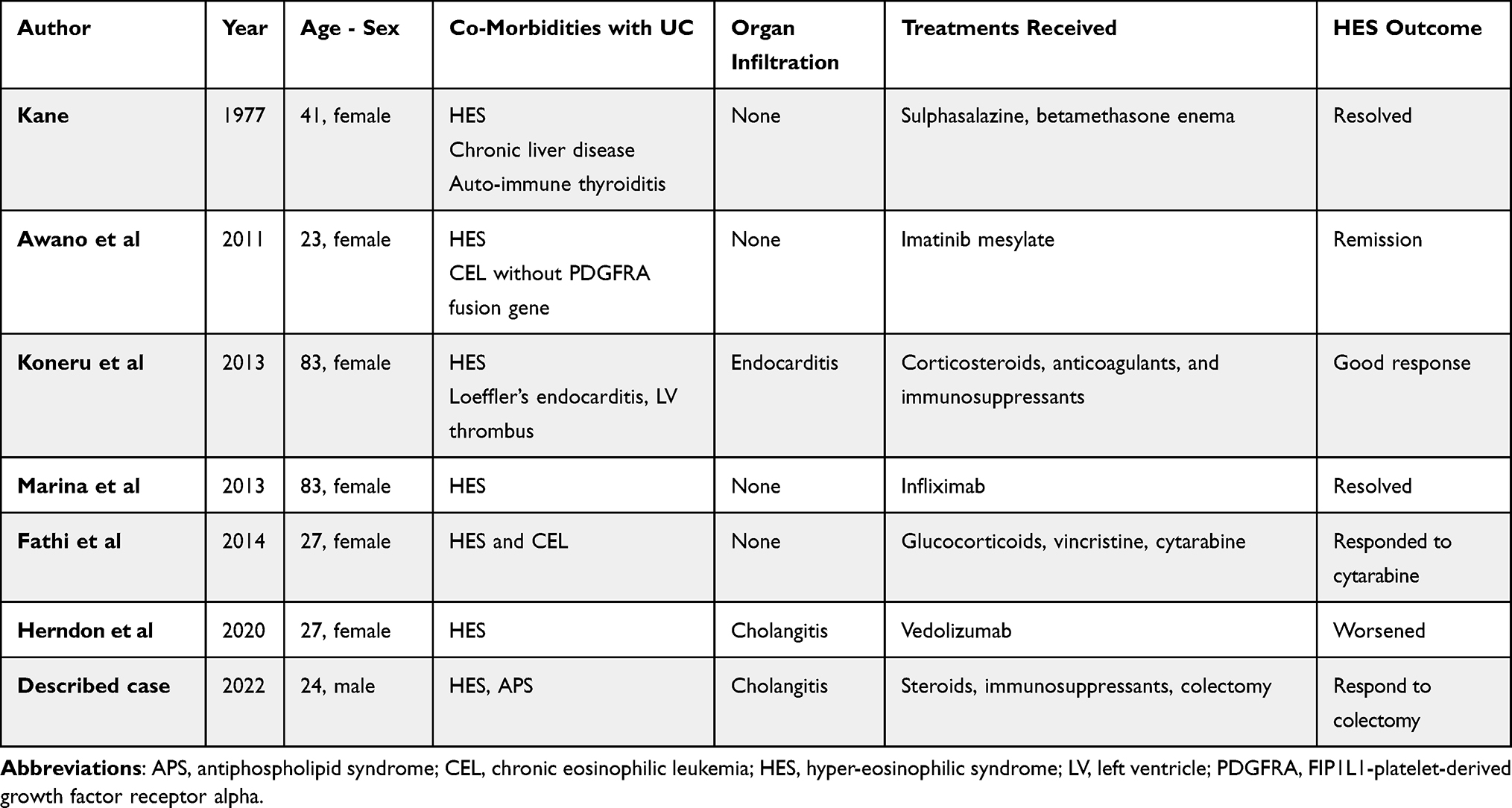 |
Table 1 Summary of Case Reports in Literature of UC and HES |
Case 2: Refractory ITP Concomitant with UC
Our second case was a 35-year-old lady diagnosed with UC and APS in 2011. She had been receiving infliximab. In 2015, she was diagnosed with ITP and was given prednisolone, azathioprine, rituximab, and intravenous immunoglobulin, with no improvement. Accordingly, she was referred to our tertiary center in December 2015 to receive romiplostim. Her CBC revealed severe anemia (Hb 5.5g/dL) and thrombocytopenia (32,000 cell/μL), but the WBCs count was within the normal range (6130 cell/μL). Following extensive work-up, she was diagnosed with ITP and paroxysmal nocturnal hemoglobinuria (PNH) in the context of IBD and APS. During the first three months of romiplostim therapy, there was a mild improvement in the platelet count which increased to 65,000 cells/μL. For the next two to three months, her platelets count was stable in the range of 52,000 to 65,000 cells/μL. Eltrombopag olamine was introduced in April 2016. However, the platelet count was trending down and a splenectomy was planned, but the patient refused. Concerning her UC, infliximab was discontinued due to adverse effects (febrile neutropenia), and vedolizumab failed to control her disease. Accordingly, surgery was indicated. On July 16th, 2019, she underwent the first step of total proctocolectomy with an ileal pouch and ileostomy. Her platelets count increased to 75,000 cells/μL postoperatively, and it remained stationary between 40,000 and 100,000 cells/μL until the time of publication of this report without medical treatment and without undergoing splenectomy.
Discussion
Conclusions and Rationale
In this article, we presented two cases of two comorbidities (HES and ITP) occurring in the context of chronic active UC and responding only to surgical colectomy. Though several cases of HES18,25–28 and ITP14,23,29–39 have been reported to co-occur with UC, the patients described in this article are unique in their presentation and treatment response. To the best of our knowledge, they represent rare cases of refractory comorbidities in the context of UC that failed conventional medical therapy and responded only to surgical treatment.
Reference to Relevant Literature
Hypereosinophilic syndrome (HES) is a myeloproliferative disorder characterized by sustained eosinophilia (defined as an absolute eosinophil count of more than 1500/µL that persists for more than six months) that is associated with symptoms and signs of multiple organ damage.20 Eosinophilia can be idiopathic, which is a diagnosis of exclusion, and can be secondary to several etiologies or clonal eosinophilia.40 The most common etiologies for secondary eosinophilia include parasitic infections, allergy, malignancy, pulmonary diseases (eg, Churg-Strauss syndrome and Loeffler syndrome), connective tissue disorders, dermatitis, sarcoidosis, Addison’s disease, and IBDs. Clonal eosinophilia is diagnosed by bone marrow biopsy and molecular and cytogenetic analysis. Common molecularly defined disorders include chronic myeloid leukemia and systemic mastocytosis (PDGFRA and PDGFRβ-rearranged eosinophilia).40 Eosinophilia can also occur as a side effect of several medications.41
In UC, eosinophilia was reported to occur in approximately 22.2% of patients at any given point, and recurrent eosinophilia was reported in 3.4% of cases.42 Hypereosinophilia has been reported to be associated with an aggressive and severe clinical course and/or primary sclerosing cholangitis.42–44 Hypereosinophilic syndrome, however, rarely occurs and has been reported in a few case reports. In the literature, HES comorbid with UC was reported in patients with UC either separately19,28 or in the context of comorbid leukemia,25,26 Loeffler's endocarditis,18 autoimmune thyroiditis,28 and cholangitis27 (Table 1). Almost all the reported cases were responsive to medical therapy except the case of UC and sclerosing cholangitis reported by Herndon et al27 which was refractory to medical treatment, and the eosinophilia worsened on vedolizumab. In our first patient, eosinophilia occurred in the context of chronic active UC and following vedolizumab initiation. Vedolizumab was stopped to exclude the possible biologic-induced eosinophilia, as has been previously reported.27 However, eosinophilia persisted. An extensive work-up was performed to exclude the causes of secondary and clonal eosinophilia, neoplasms, allergies, and other rheumatological disorders. The two remaining differential diagnoses were idiopathic HES or reactive eosinophilia secondary to comorbid autoimmunity. Despite aggressive medical treatment, our patient did not improve until after surgical colectomy.
Concomitant occurrence of ITP and UC is rare.14,23,29–39 In patients with UC, ITP represents an extraintestinal manifestation of the disease mediated by immune-mediated mechanisms.29 The differential diagnosis of thrombocytopenia is broad. Infections, autoimmune and immunodeficiency disorders, connective tissue diseases, malignancies, liver diseases, splenomegaly, myelodysplastic syndromes, and other bone marrow diseases should be excluded prior to diagnosing ITP.45,46 In the literature, several cases of ITP comorbid with UC have been reported (Table 2). The thrombocytopenia reported in the vast majority of the reported cases responded adequately to conventional therapy (ie, steroids,14,32–34 immunosuppressants,23,32,33 granulocytapheresis32). Few cases, such as the case report described by Komeda et al,31 were refractory to conventional steroids and immunosuppressant therapies and responded only to Janus kinase (JAK) inhibitor, ie, tofacitinib. Other cases of ITP were attributed to disease-modifying therapies such as infliximab.35 Splenectomy was required in a proportion of patients who were refractory to medical therapy.32,33 Our second patient was a case of refractory ITP that failed steroids, azathioprine, rituximab, romiplostim, anti-TNF therapy, and vedolizumab. She did not require platelets transfusion or medical therapy for two years following surgery. Similarly to our patient, one of the patients reported by Mizuta et al32 failed steroid therapy and granulocytapheresis, and the ITP resolved only after colectomy. Ten of the cases reviewed by Chandra et al33 were also refractory to medical therapy and responded only to colectomy. This was also the case in a young boy with UC comorbid with refractory ITP, reported by Papadatou et al39 who failed on a high dose of steroids and IVIG and responded only to colectomy. Colectomy was also required in two cases reported by Dehal et al38 and Kwon et al.36 Similarly to adults, colectomy was reported to be of therapeutic benefit in children with UC comorbid with ITP.37 In Guarina et al37‘s case series of eight children with comorbid UC and ITP, two cases underwent colectomy and the ITP recovered postoperatively in one of them.
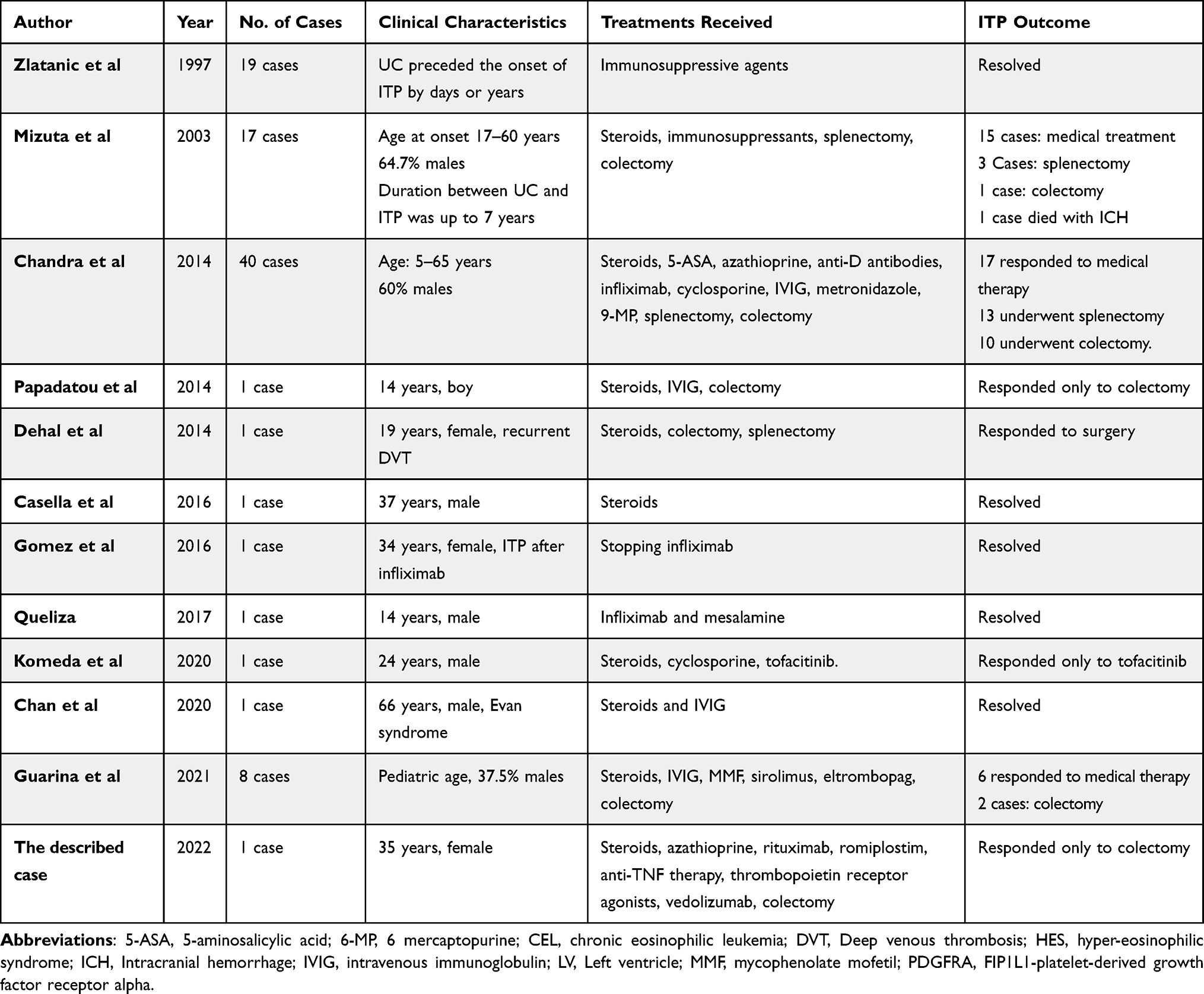 |
Table 2 Summary of Case Reports and Case Series in Literature of UC and ITP |
Comparison to the Current Gold Standard of Care
Management of HES in patients with UC is based on the patients’ clinical presentation.19 The “wait and see” approach can be implemented in asymptomatic cases with adequate and close monitoring.19 When the syndrome becomes symptomatic, medical treatment should be initiated with empiric steroids initially.19 If refractory to steroids, patients can be administered other medications, eg, hydroxyurea, Imatinib (for PDGFRA or PDGFRB variants), or leukopheresis.19,35 Interferon-α, methotrexate, cyclosporine, cladribine, chlorambucil, vincristine, and etoposide can also be provided in specific cases.47,48 Our first patient had severe ulcerative pancolitis that failed adalimumab (due to adverse effects) and infliximab. He then developed HES after one year of treatment with a high dose of vedolizumab. Given the diagnosis of idiopathic HES, a therapeutic trial of long-term steroids and Imatinib was initiated. Despite this, the condition persisted, and the eosinophilia was sustained above 1500 cells/µL for over six months. After colectomy, the HES resolved, and the WBCs dropped from above 30,000 cells/cc3 to normal and the absolute eosinophil count normalized. The patient was managed presumptively as a case of idiopathic HES with a prolonged trial of Imatinib and high doses of steroids. Nonetheless, the fact that he had normalization of absolute neutrophil count post colectomy while off Imatinib for more than seven months further supports the non-myeloproliferative clonal and neoplastic HES etiologies and precludes the need to continue Imatinib and steroids. The most likely diagnosis of this patient, then, would be secondary (or reactive) HES to UC. The role of vedolizumab in the induction of the condition cannot be excluded.
Similarly, the cornerstone of managing ITP in patients with UC is to treat the underlying UC flare.33 If the ITP persists, steroids, IVIG, and immunosuppressants should be administered.33 Refractory cases may require surgery, such as splenectomy and/or colectomy.32,33 Our second patient failed steroid and immunosuppressant therapy and responded only to surgical colectomy. The fact that she had a spontaneous rise of platelet count from 5000 to 75,000 cells/µL after colectomy and maintained a platelet level between 40,000 and 100,000 cells/µL for approximately two years while off treatment, and without requiring splenectomy, suggests the reactive nature of this thrombocytopenia.
Relevant Hypothesis Generation
The refractory HES and ITP noted in the described patients do not seem to be cases of idiopathic immune-mediated comorbidities occurring in the context of the systemic immune responses associated with UC flare, as has long been reported in the literature.49 In our opinion, the two cases represent cases of reactive eosinophilia and thrombocytopenia that occurred secondary to the ongoing local intestinal inflammation. The fact that the two conditions resolved and remained in remission for long periods following colectomy generates a hypothesis about the reactive nature of these conditions.
Implications of Clinical Practice
From our experience with the described cases, we suggest considering surgical colectomy to manage refractory immune-mediated disorders comorbid with UC, such as HES and ITP. Whilst these conditions were suggested to be idiopathic,50 the considerably good and sustained response to colectomy highly suggests their reactive nature. In patients with UC, immune complexes escape from the gut to the circulating blood due to increased mucosal permeability during disease activity.24 They cross-react with the platelet surface antigens, which carry similar peptides to bacterial glycoproteins in the gut and, subsequently, result in ITP.24 Moreover, the autoreactive T-cells secrete eosinophilopoietic cytokines that promote eosinophils’ survival, enhance their activity, and hinder their suppressive regulatory mechanisms.20,21 Colectomy, therefore, would stop these pathogenic mechanisms and subsequently prevent platelets destruction and hypereosinophilia.
Strength and Limitations
The main strength of this study is that it is the first, to the best of our knowledge, to report resolution of refractory HES following colectomy in a patient with UC. Long follow-up is another strength. The main limitation, on the other hand, is a deviation from the protocol of ITP management when splenectomy was deferred, but this was due to the patient’s refusal. Such deviation might lead to misinterpretation of the severity of the case and the need to undergo colectomy. Therefore, future case reports should aim to elaborate on similar cases’ responses to the step-by-step treatment algorithm for such comorbidities.
Conclusion
We presented two cases of refractory immune-mediated disorders, HES and ITP, that occurred comorbid with UC that failed conventional medical therapy. Surgical colectomy was performed for both cases and resulted in a considerable improvement of the two conditions, even when medical treatment was on hold for several months. This suggests a possibly reactive, rather than idiopathic, etiology of these comorbid conditions. Further research is required to investigate the possibly reactive nature of both HES and ITP.
Learning Points/Take Home Messages
- Hypereosinophilic syndrome and immune thrombocytopenic purpura can occur in the context of UC.
- These comorbidities can be idiopathic or reactive to intestinal immune dysregulation.
- Surgical colectomy should be offered to refractory HES and/or immune thrombocytopenic purpura.
Ethical Statement
This article was performed in accordance with the principles of Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of, our hospital, King Faisal Specialist Hospital & Research Centre, Jeddah, Saudi Arabia. The approval reference number is IRB 2022-CR-24. Written consent was obtained from both patient for the publication of her case and accompanying data.
Acknowledgements
We are immensely grateful to our generous patients for allowing us to publish their cases.
Disclosure
Prof. Dr Silvio Danese reports personal fees from Abbvie, Alimentiv, Allergan, Amgen, Astrazeneca, Athos Therapeutics, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Celltrion, Dr Falk Pharma, Eli Lilly, Enthera, Ferring Pharmaceuticals Inc., Gilead, Hospira, Inotrem, Janssen, Johnson & Johnson, MSD, Mundipharma, Mylan, Pfizer, Roche, Sandoz, Sublimity Therapeutics, Takeda, Teladoch, TiGenix, UCB Inc., and Vifor, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Abraham C, Medzhitov R. Interactions between the host innate immune system and microbes in inflammatory bowel disease. Gastroenterology. 2011;140(6):1729–1737. doi:10.1053/j.gastro.2011.02.012
2. Rabinowitz K, Mayer L. Working out mechanisms of controlled/physiologic inflammation in the GI tract. Immunol Res. 2012;54(1–3):14–24. doi:10.1007/s12026-012-8315-5
3. Scharl M, Rogler G. Inflammatory bowel disease pathogenesis: what is new? Curr Opin Gastroenterol. 2012;28(4):301–309. doi:10.1097/MOG.0b013e328353e61e
4. MacDermott RP, Nash GS, Auer IO, et al. Alterations in serum immunoglobulin g subclasses in patients with-ulcerative colitis and crohn’s disease. Gastroenterology. 1989;96(2):764–768. doi:10.1016/S0016-5085(89)80074-5
5. Ho GT, Porter RJ, Kalla R. Ulcerative colitis: recent advances in the understanding of disease pathogenesis. F1000Research. 2020;9. doi:10.12688/f1000research.20805.1
6. Phillipson M, Kubes P. The neutrophil in vascular inflammation. Nat Med. 2011;17(11):1381–1390. doi:10.1038/nm.2514
7. Satsangi J, Landers CJ, Welsh KI, Koss K, Targan S, Jewell DP. The presence of anti-neutrophil antibodies reflects clinical and genetic heterogeneity within inflammatory bowel disease. Inflamm Bowel Dis. 2007;4(1):18–26. doi:10.1002/ibd.3780040105
8. Al-Haddad S, Riddell RH. The role of eosinophils in inflammatory bowel disease. Gut. 2005;54(12):1674–1675. doi:10.1136/gut.2005.072595
9. Jacobs I, Ceulemans M, Wauters L, et al. Role of eosinophils in intestinal inflammation and fibrosis in inflammatory bowel disease: an overlooked villain? Front Immunol. 2021;12. doi:10.3389/fimmu.2021.754413
10. Friedrich M, Pohin M, Powrie F. Cytokine networks in the pathophysiology of inflammatory bowel disease. Immunity. 2019;50(4):992–1006. doi:10.1016/j.immuni.2019.03.017
11. Graham DB, Luo C, O’Connell DJ, et al. Antigen discovery and specification of immunodominance hierarchies for MHCII-restricted epitopes. Nat Med. 2018;24(11):1762–1772. doi:10.1038/s41591-018-0203-7
12. Bouma G, Strober W. The immunological and genetic basis of inflammatory bowel disease. Nat Rev Immunol. 2003;3(7):521–533. doi:10.1038/nri1132
13. Chetri K, Aggarwal R, Sharma B, Nityanand S, Naik SR. Ulcerative colitis and immune thrombocytopenia: a report of two cases. Indian J Gastroenterol. 1999;18(4):174.
14. Casella G, Antonelli E, Villanacci V, et al. Immune thrombocytopenia in ulcerative colitis. Tech Coloproctol. 2016;20(7):499–500. doi:10.1007/s10151-016-1471-1
15. Kashiwagi H, Tomiyama Y. Pathophysiology and management of primary immune thrombocytopenia. Int J Hematol. 2013;98(1):24–33. doi:10.1007/s12185-013-1370-4
16. Singh A, Uzun G, Bakchoul T. Primary immune thrombocytopenia: novel insights into pathophysiology and disease management. J Clin Med. 2021;10(4):1–21. doi:10.3390/jcm10040789
17. Audia S, Moulinet T, Ciudad-Bonté M, et al. Altered distribution and function of splenic innate lymphoid cells in adult chronic immune thrombocytopenia. J Autoimmun. 2018;93:139–144. doi:10.1016/j.jaut.2018.07.015
18. Koneru S, Koshy G, Sharp C, Khalafallah AA. Hypereosinophilic syndrome associated with ulcerative colitis presenting with recurrent Loeffler’s endocarditis and left ventricular thrombus treated successfully with immune suppressive therapy and anticoagulation. BMJ Case Rep. 2013;2013(2):bcr2013200919–bcr2013200919. doi:10.1136/bcr-2013-200919
19. Ángel F. Case report: hypereosinophilic syndrome response to infliximab in a patient with ulcerative colitis. Gastroenterol Hepatol Open Access. 2016;5(5). doi:10.15406/ghoa.2016.05.00158
20. Curtis C, Ogbogu P. Hypereosinophilic syndrome. Clin Rev Allergy Immunol. 2016;50(2):240–251. doi:10.1007/s12016-015-8506-7
21. Abo Shdid R, Azrieh B, Alebbi S, Mansour S, Naeem M. Idiopathic hypereosinophilic syndrome with multiple organ involvement. Case Rep Oncol. 2021;14(1):249–255. doi:10.1159/000511396
22. Gleich GJ, Leiferman KM. The hypereosinophilic syndromes: current concepts and treatments. Br J Haematol. 2009;145(3):271–285. doi:10.1111/j.1365-2141.2009.07599.x
23. Queliza K, Ihekweazu FD, Ali A, Kellermayer R. Inflammatory bowel disease and immune thrombocytopenic purpura: combined immune dysregulation in an adolescent. Ann Clin Lab Sci. 2017;47(2):226–228.
24. Epistola R, Do T, Vankina R, et al. Immune thrombocytopenic purpura (ITP) as an uncommon extraintestinal complication of crohn’s disease: case vignette and systematic literature review. Case Rep Hematol. 2020;2020:1–6. doi:10.1155/2020/4785759
25. Awano N, Ryu T, Yoshimura N, Takazoe M, Kitamura S, Tanaka M. Successful treatment of ulcerative colitis associated with hypereosinophilic syndrome/chronic eosinophilic leukemia. Intern Med. 2011;50(16):1741–1745. doi:10.2169/internalmedicine.50.5569
26. Fathi AT, Dec GWJ, Richter JM, et al. Case 7-2014: a 27-year-old man with diarrhea, fatigue, and eosinophilia. NEJM. 2014;370(9):861–872. doi:10.1056/NEJMCPC1302331
27. Herndon JS, Vitta S, Weber FH. Marked eosinophilia in a 27-year-old woman with recent onset ulcerative colitis. Gastroenterology. 2021;160(1):29–30. doi:10.1053/j.gastro.2020.08.030
28. Kane SP. Ulcerative colitis with chronic liver disease, eosinophilia and auto-immune thyroid disease. Postgrad Med J. 1977;53(616):105–108. doi:10.1136/pgmj.53.616.105
29. Zlatanic J, Korelitz BI, Wisch N, et al. Inflammatory bowel disease and immune thrombocytopenic purpura: is there a correlation? Am J Gastroenterol. 1997;92(12SUPPL):2285–2288.
30. Edwards FC, Truelove SC. The course and prognosis of ulcerative colitis: part II long-term prognosis. Gut. 1963;4(4):309–315. doi:10.1136/gut.4.4.309
31. Komeda Y, Sakurai T, Sakai K, et al. Refractory case of ulcerative colitis with idiopathic thrombocytopenic purpura successfully treated by Janus kinase inhibitor tofacitinib: a case report. World J Clin Cases. 2020;8(24):6389–6395. doi:10.12998/wjcc.v8.i24.6389
32. Mizuta Y, Isomoto H, Kadokawa Y, et al. Immune thrombocytopenic purpura in patients with ulcerative colitis. J Gastroenterol. 2003;38(9):884–890. doi:10.1007/s00535-002-1166-4
33. Chandra S, Finn S, Obah E. Immune thrombocytopenic purpura in ulcerative colitis: a case report and systematic review. J Community Hosp Intern Med Perspect. 2014;4(2):23386. doi:10.3402/jchimp.v4.23386
34. Chan KH, Lim SL, Are G, DaCosta T, Shaaban HS, Rare A. Case of Evans syndrome in a patient with ulcerative colitis. Gastroenterol Res. 2020;13(4):158–160. doi:10.14740/gr1316
35. Gomez G, Umar S, Bilal M, Strahotin C, Clarke K. Febrile neutropenia with thrombocytopenia after infliximab induction in a patient with ulcerative colitis. Case Rep Gastroenterol. 2016;10(3):596–599. doi:10.1159/000448071
36. Kwon JH, Lee C, Choi JM, et al. A case of immune thrombocytopenic purpura associated with preexisting ulcerative colitis treated with colectomy and splenectomy. Intest Res. 2013;11(4):310. doi:10.5217/ir.2013.11.4.310
37. Guarina A, Barone A, Tornesello A, et al. Association of immune thrombocytopenia and inflammatory bowel disease in children. J Clin Med. 2021;10(9):1940. doi:10.3390/jcm10091940
38. Dehal A, Patel S, Johna S, Nguyen P. Acute ulcerative colitis, thrombocytopenia, and venous thromboembolism treated with combined laparoscopic splenectomy and colectomy. CRSLS MIS Case Reports from SLS. 2014;18(4). doi:10.4293/crsls.2014.00298
39. Papadatou B, Bracci F, Knafelz D, et al. Ulcerative colitis and acute thrombocytopenia in a pediatric patient: a case report and review of the literature. Health. 2014;6(12):1497–1502. doi:10.4236/health.2014.612184
40. Wang SA. The diagnostic work-up of hypereosinophilia. Pathobiology. 2019;86(1):39–52. doi:10.1159/000489341
41. Rauscher C, Freeman A. Drug-induced eosinophilia. Allergy Asthma Proc. 2018;39(3):252–256. doi:10.2500/aap.2018.39.4120
42. Barrie A, Mourabet E, Weyant K, et al. Recurrent blood eosinophilia in ulcerative colitis is associated with severe disease and primary sclerosing cholangitis. Dig Dis Sci. 2013;58(1):222–228. doi:10.1007/s10620-012-2329-7
43. Click B, Anderson AM, Koutroubakis IE, et al. Peripheral eosinophilia in patients with inflammatory bowel disease defines an aggressive disease phenotype. Am J Gastroenterol. 2017;112(12):1849–1858. doi:10.1038/ajg.2017.402
44. Machicado JD, Kabbani T, Rivers CR, et al. Sa1187 peripheral blood eosinophilia in patients with inflammatory bowel disease is associated with worse outcomes: a 5-year prospective study. Gastroenterology. 2015;148(4):S251. doi:10.1016/s0016-5085(15)30827-1
45. Cooper N, Radia D. Thrombocytopenia. Medicine. 2021;49(4):217–220. doi:10.1016/j.mpmed.2021.01.007
46. Stasi R. How to approach thrombocytopenia. Hematology Am Soc Hematol Educ Program. 2012;2012:191–197. doi:10.1182/asheducation.v2012.1.191.3798260
47. Gotlib J. World Health Organization-defined eosinophilic disorders: 2014 update on diagnosis, risk stratification, and management. Am J Hematol. 2014;89(3):325–337. doi:10.1002/ajh.23664
48. Bergua JM, Prieto-Pliego E, Román-Barberá A, et al. Resolution of left and right ventricular thrombosis secondary to hypereosinophilic syndrome (lymphoproliferative variant) with reduced intensity conditioning allogenic stem cell transplantation. Ann Hematol. 2008;87(11):937–938. doi:10.1007/s00277-008-0505-9
49. Zabrowski D, Abraham D, Rosenthal G, Kader H. Development of peripheral eosinophilia in inflammatory bowel disease patients on infliximab treated at a tertiary pediatric inflammatory bowel disease center is associated with clinically active disease but does not result in loss of efficacy or adverse o. JGH Open. 2020;4(4):636–641. doi:10.1002/jgh3.12308
50. Diny NL, Rose NR, Čiháková D. Eosinophils in autoimmune diseases. Front Immunol. 2017;8. doi:10.3389/fimmu.2017.00484
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.