")
Back to Journals » Infection and Drug Resistance » Volume 12
Resistance rates of non-albicans Candida infections in Taiwan after the revision of 2012 Clinical and Laboratory Standards Institute breakpoints
Authors Hii IM , Liu CE, Lee YL, Liu WL , Wu PF, Hsieh MH, Ho MW, Chen YH , Wang FD
Received 22 August 2018
Accepted for publication 27 November 2018
Published 15 January 2019 Volume 2019:12 Pages 235—240
DOI https://doi.org/10.2147/IDR.S184884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eric Nulens
Ing-Moi Hii,1 Chun-Eng Liu,1 Yu-Lin Lee,1 Wei-Lun Liu,2,3 Ping-Feng Wu,4,5 Min-Han Hsieh,6 Mao-Wang Ho,7 Yen-Hsu Chen,8–10 Fu-Der Wang4,5
1Division of Infectious Disease, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan; 2Department of Emergency and Critical Care Medicine, Fu Jen Catholic University Hospital, New Taipei City, Taiwan; 3School of Medicine, College of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan; 4Division of Infectious Disease, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 5School of Medicine, National Yang-Ming University, Taipei, Taiwan; 6Division of Infectious Diseases, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan; 7Division of Infectious Diseases, Department of Internal Medicine, China Medical University Hospital, China Medical University, Taichung, Taiwan; 8Department of Biological Science and Technology, College of Biological Science and Technology, National Chiao Tung University, HsinChu, Taiwan; 9Department of Internal Medicine, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan; 10School of Medicine, Graduate Institute of Medicine, Sepsis Research Center, Center of Dengue Fever Control and Research, Kaohsiung Medical University, Kaohsiung, Taiwan
Purpose: In 2012, the Clinical and Laboratory Standards Institute (CLSI) revised its breakpoints for drugs and species because of the increase in non-albicans Candida infections and their drug resistance. Following global trends, the non-albicans candidemia resistance rate has increased in Taiwan as well. To update the antifungal susceptibility of non-albicans candidemia isolates, we conducted a multicenter study using the revised break points.
Patients and methods: Patients with non-albicans candidemia infections were identified at five tertiary hospitals in Taiwan from July 1, 2011, to June 30, 2014. The broth microdilution method using a Sensititre YeastOne system was performed for the determination of minimum inhibitory concentration (MIC). The susceptibility was interpreted based on the guidelines of the CLSI (CLSI M27-S4 and M27-S3).
Results: Candida tropicalis was the predominant non-albicans candidemia pathogen (42.4%), and it showed increased fluconazole non-susceptibility (36.3%) when compared to the results from previous studies. In particular, C. tropicalis showed high cross-resistance to azole agents. C. tropicalis isolates that were found to be resistant to fluconazole also showed increased resistance to voriconazole (82.2%) and posaconazole (100%). The increased non-susceptibility of Candida glabrata to multiple antifungal agents, based on the revised break points, resulted from an increase in dose-dependent susceptibility (94.4%) rather than from an increase in resistance (5.6%).
Conclusion: The resistance rate of non-albicans candidemia isolates is increasing, particularly for C. tropicalis and C. glabrata.
Keywords: non-albicans candidemia, resistance, susceptibility
Introduction
Clinicians have used fluconazole to treat mucosal and invasive infections caused by Candida, Cryptococcus, and other opportunistic yeasts for nearly 30 years. In December 2012, the Clinical and Laboratory Standards Institute (CLSI), similar to the European Committee on Antimicrobial Susceptibility Testing (EUCAST), revised the antimicrobial break points for different species in CLSI M27-S4,1 because resistance to fluconazole and echinocandins had been documented.2–4 Accordingly, although Candida albicans is still the major pathogen responsible for candidiasis, many studies have reported the emergence of non-albicans Candida species.5,6 The revised susceptibility tests are more sensitive at detecting resistant Candida strains.7–9 The other species include Candida glabrata and Candida tropicalis, which have low susceptibility to azole antifungals. According to the CLSI M27-S4 guidelines,1 most non-albicans Candida species, except for Candida parapsilosis, show decreased susceptibility to multiple antifungal agents.1
The purpose of this study was to determine the resistance rates of non-albicans Candida species in Taiwan using the revised clinical break points defined by CLSI.
Patients and methods
Study design and setting
Candida specimens were obtained from adult patients who were positive for candidemia, from July 1, 2011, to June 30, 2014, at five tertiary hospitals in Taiwan: two in the south (Liouying Chi-Mei Medical Center, Kaohsiung Medical University), two in the central region (Changhua Christian Hospital, China Medical University Hospital), and one in the north (Taipei Veterans General Hospital). Non-duplicate samples were collected from abovementioned patients. The broth microdilution method was performed for the determination of minimum inhibitory concentration (MIC) according to the manufacturer’s instructions using a Sensititre YeastOne system (Trek Diagnostic Systems Ltd., East Grinstead, UK). Candida krusei ATCC 6258 and Candida parapsilosis ATCC 22019 were used as quality control strains. All isolates were tested for in vitro susceptibility to fluconazole, voriconazole, posaconazole, itraconazole, anidulafungin, caspofungin, micafungin, flucytosine, and amphotericin B using CLSI guidelines. We interpreted susceptibility as it is defined in the CLSI editions, CLSI M27-S4 and CLSI M27-S3.1,10 The designation of non-susceptibility included samples that were susceptible does-dependent (SDD), intermediate, and resistant. The medical ethics committees of the five participating hospitals approved this study, and the informed consent was waived due to no intervention for the study population and difficulties in recontacting them. The whole process of collecting information from the participants was confidential. The privacy was maintained by using de-linking, and only the code appeared in the analyzed data. The authority to obtain the data was limited to the researchers ourselves.
Statistical analyses
Differences in results obtained using the 2008 and 2012 break points were assessed for significance by the Chi-squared or Fisher’s exact test. A P-value of <0.05 was considered statistically significant.
Results
During the 3-year time frame of the study, 1,426 Candida samples were isolated from blood cultures. Of those, 815 were recognized as C. albicans and 611 as non-albicans Candida. The most common non-albicans Candida species were C. tropicalis (n=259; 42.4%), C. glabrata (n=213; 34.9%), C. parapsilosis (n=126; 20.6%), and C. krusei (n=13; 2.1%; Table 1). All other non-albicans Candida species were isolated infrequently (data not shown). MICs for the quality control strain of C. krusei ATCC 6258 and C. parapsilosis ATCC 22019 were 32 mg/L and 2 mg/L for fluconazole, 0.25 mg/L and 0.03 mg/L for voriconazole, 0.12 mg/L and 0.06 mg/L for posaconazole, 0.25 mg/L and 0.25 mg/L for itraconazole, 0.12 mg/L and 2 mg/L for micafungin, 0.25 mg/L and 0.5 mg/L for caspofungin, 0.12 mg/L and 2 mg/L for anidulafungin, 1 mg/L and 0.5 mg/L for amphotericin B, and 8 mg/L and 0.25 mg/L for flucytosine.
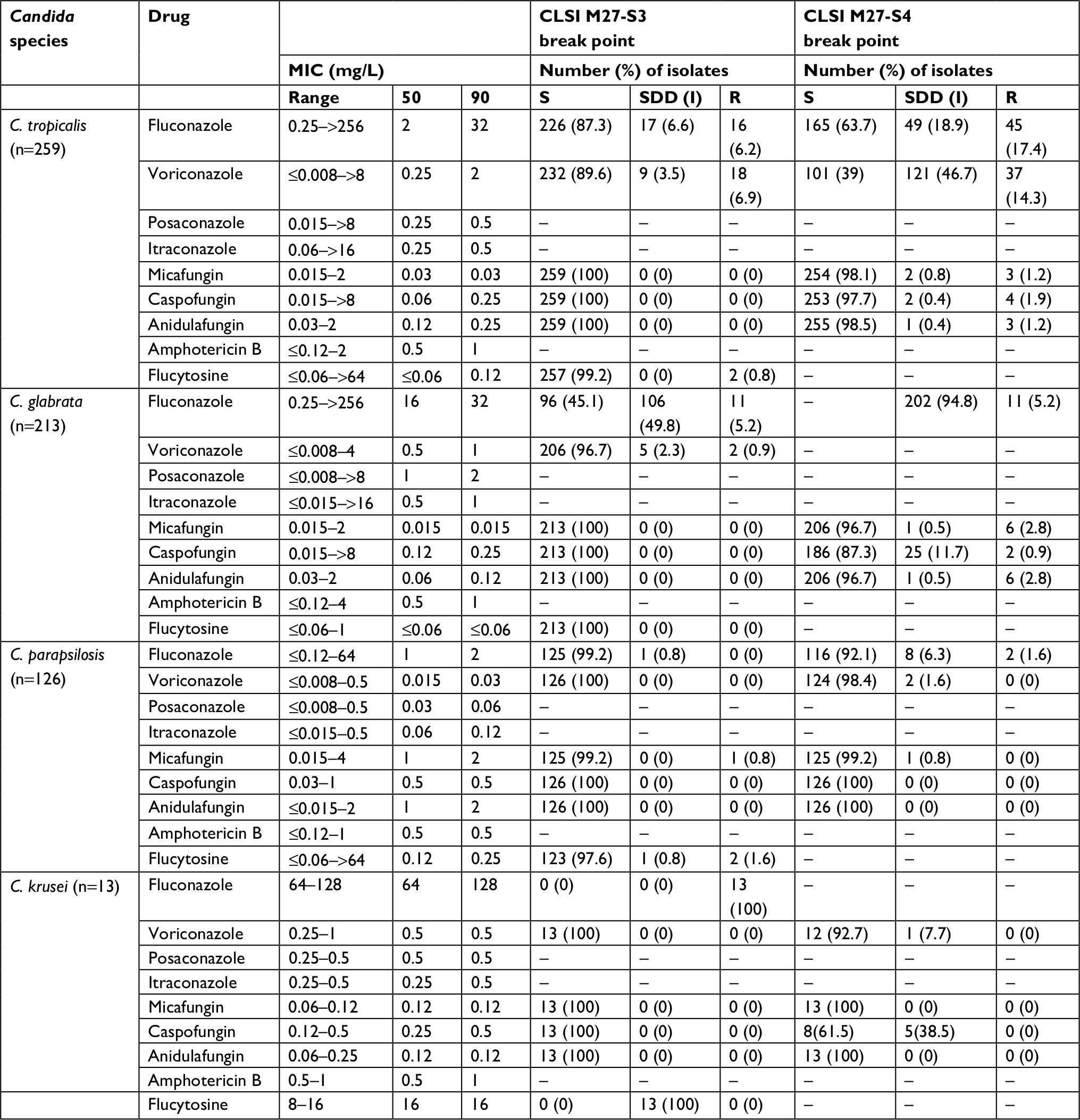 | Table 1 MIC ranges, MIC 50%, MIC 90%, and numbers and percentages of isolates classified as susceptible (S), susceptible does-dependent (SDD), intermediate (I), or resistant (R), based on the 2012 and CLSI M27-S3 break points for antifungal drugs Abbreviations: C. glabrata, Candida glabrata; C. krusei, Candida krusei; CLSI, Clinical and Laboratory Standards Institute; C. parapsilosis, Candida parapsilosis; C. tropicalis, Candida tropicalis; I, intermediate; MIC, minimum inhibitory concentration; R, resistant; S, susceptible; SDD, susceptible dose dependent. |
Table 1 summarizes the comparison of susceptibility rate according to CLSI criteria with different break points revised in 2008 (CLSI M27-S3)10 and 2012 (CLSI M27-S4).1 In this study, fluconazole susceptibility in non-albicans species was lower than 90% according to the 2012 revised break point, except for C. parapsilosis, of which the susceptibility was 92.1%. The three echinocandins were relatively effective in susceptibility tests against non-albicans species, except for C. glabrata and C. krusei, which showed 87.3% and 61.5% resistance to caspofungin, respectively.
According to the CLSI M27-S3 criteria,10 C. tropicalis showed 100% susceptibility to the echinocandins (micafungin, caspofungin, and anidulafungin) and high susceptibility to the azoles (fluconazole: n=226, 87.3%; voriconazole: n=232, 89.6%). However, according to the CLSI M27-S4 criteria, a high percentage of isolates were found to be non-susceptible to azoles (Tables 1 and 2). In particular, 36.3% of isolates were not susceptible to fluconazole (SDD: 18.9%, n=49; R: 17.4%, n=45), and 61.0% were not susceptible to voriconazole (SDD: 46.7%, n=121; R: 14.3%, n=37). MIC50 and MIC90 of C. tropicalis for fluconazole in the present study were 2 mg/L and 32 mg/L, respectively, whereas for voriconazole, they were 0.25 mg/L and 2 mg/L, respectively (Table 1). MIC50 and MIC90 of C. tropicalis were 0.03 mg/L for micafungin, 0.06 mg/L and 0.25 mg/L for caspofungin, and 0.12 and 0.25 mg/L for anidulafungin, respectively (Table 1).
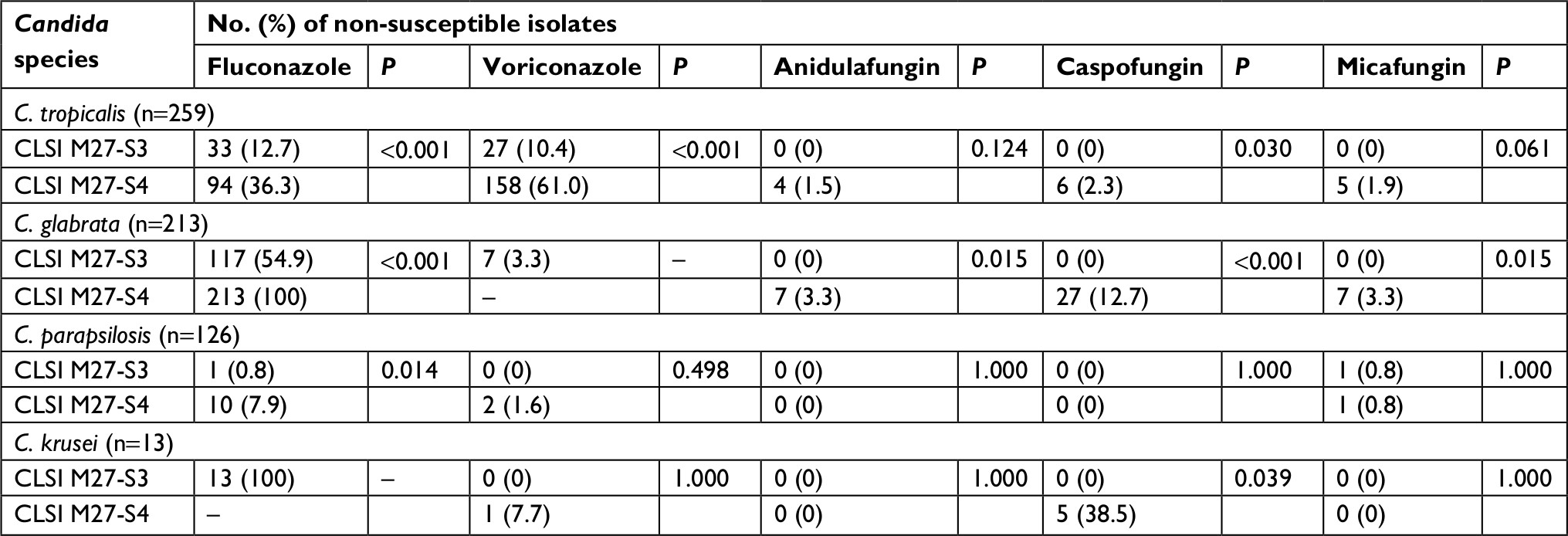 | Table 2 Non-albicans Candida isolates non-susceptible to fluconazole, voriconazole, micafungin, caspofungin, and anidulafungin according to the CLSI M27-S4 and CLSI M27-S3 break points Abbreviations: C. glabrata, Candida glabrata; C. krusei, Candida krusei; CLSI, Clinical and Laboratory Standards Institute; C. parapsilosis, Candida parapsilosis; C. tropicalis, Candida tropicalis. |
Among the isolates of C. glabrata, the rate of non-susceptibility, especially non-susceptible to fluconazole (SDD: 94.8%, n=202; R: 5.2%, n=11), increased when interpreted according to CLSI M27-S41 (Tables 1 and 2). The rate of C. glabrata, non-susceptible to fluconazole, was extremely high, based on the new break point, because of an increased number of dose-dependent strains, rather than because of an increased number of resistant strains. The break point for voriconazole was not reinterpreted in the new guidelines. According to the revised break points, the susceptibility of C. glabrata to anidulafungin and micafungin remained high (96.7% for each), although the susceptibility to caspofungin decreased from 100% (CLSI M27-S3) to 87.3% (CLSI M27-S4; Tables 1 and 2). MIC50 and MIC90 of C. glabrata were 16 mg/L and 32 mg/L for fluconazole and 0.5 mg/L and 1 mg/L for voriconazole, respectively. MIC50 and MIC90 were 0.015 mg/L for micafungin, 0.12 mg/L and 0.25 mg/L for caspofungin, and 0.06 mg/L and 0.12 mg/L for anidulafungin (Table 1).
There were no major differences in the drug susceptibility of C. parapsilosis isolates determined using the CLSI M27-S3 and CLSI M27-S4 break points (Tables 1 and 2). C. krusei is assumed to be intrinsically resistant to fluconazole. However, this species showed significantly lower susceptibility (62%) to caspofungin based on the CLSI M27-S4 break point (P<0.039; Tables 1 and 2). MIC50 and MIC90 for the different non-albicans Candida species are listed in Table 1.
Table 3 summarizes the cross-resistance between fluconazole and echinocandins. According to the CLSI M27-S4 break points and epidemiological cutoff values,11,12 our results indicate that C. tropicalis and C. glabrata showed cross-resistance between fluconazole and voriconazole. Among the C. tropicalis isolates (n=259), there were 45 fluconazole-resistant isolates. Of those, 80.0% (36/45) were also resistant to voriconazole (P<0.001). Regarding 11 isolates of C. glabrata with resistance to fluconazole, 90.9% (10/11) and 54.5% (6/11) were also resistant to voriconazole and posaconazole, respectively. Despite a strong correlation between fluconazole and voriconazole resistance in both C. tropicalis and C. glabrata, the susceptibility to echinocandins remained high (above 90%) in these two non-albicans Candida species.
 | Table 3 Cross-resistance to azole and echinocandin drugs among fluconazole-resistant isolates of C. tropicalis and C. glabrata Abbreviations: C. glabrata, Candida glabrata; C. tropicalis, Candida tropicalis; R, resistant; S, susceptible; SDD, susceptible-dose dependent. |
Discussion
Our study showed that among all the Candida species that cause bloodstream infections, C. albicans remains the predominant pathogen in Taiwan (57.2%), in a similar fashion to studies conducted in other Asian countries such as Korea, Singapore, and Vietnam.11 Of the non-albicans candidemia isolates, C. tropicalis was the most common species (42.4%), and this species distribution trend is likely as that reported in Asia or Taiwan from previous literatures.12–15 In southern Taiwan, C. albicans was the most common Candida species (48.7%, 345/709) and C. tropicalis was the most common non-albicans Candida species (40.7%, 148/364).15 In northern Taiwan, the percentages of C. albicans and C. tropicalis were 62.15% and 15.4%, respectively.16 This divergence of species distribution among non-albicans candidemia between Asian and Western countries indicated the importance of comprehension and update about local epidemiology in each region around the world.
Using the revised CLSI guideline, we found that the susceptibility of C. tropicalis to fluconazole decreased from 87.3% to 63.7%, whereas the susceptibility to voriconazole decreased from 89.6% to 39.0%. On the other hand, it appeared that C. glabrata showed dose-dependent susceptibility to fluconazole in majority under the revised break points.
Although our results have shown that the susceptibility of C. tropicalis to fluconazole has decreased according to these revised break points, this trend is not confirmed in other studies conducted in Taiwan. Chen et al15 reported that the susceptibility of C. tropicalis to fluconazole was as high as 85.8%. Yang et al17 reported that the susceptibility to fluconazole and voriconazole was 99.6% and 100%, respectively. However, these studies did not exclusively consider bloodstream infections, but they also included other sterile site specimens. Huang et al18 reported the susceptibility of C. tropicalis to fluconazole and voriconazole to be 86.7% and 78.6%, respectively. When comparing to our results, the higher susceptibility of C. tropicalis observed in previous studies could be explained by the fact that these authors only considered one hospital during their researches. The disparity of our study method with the Taiwan Surveillance of Antimicrobial Resistance of Yeasts (TSARY)17 resulted in different susceptibility results. Among the five hospitals in this study, there was only one hospital in which C. tropicalis susceptibility to fluconazole attained 70%. In addition, none of C. tropicalis samples tested were susceptible to voriconazole beyond 50%. In this study, we found that the resistance rate of C. glabrata to fluconazole under the revised break points did not vary compared to that under the former break points. We noticed that the non-susceptible rate changes were mostly due to the increase in the SDD C. glabrata strains. The susceptibility test of C. parapsilosis to fluconazole had minor variation and was similar to the previous break points.
Caspofungin susceptibility significantly decreased when using the new break points of each species (Tables 1 and 2). In the study by Espinel-Ingroff et al,19 caspofungin susceptibility had interlaboratory variation against each species, except for C. parapsilosis and Candida guilliermondii. Therefore, there was no MIC used to perform this test.
As C. tropicalis isolates were resistant to fluconazole in our study, those were 80.0% resistant to voriconazole and 100% resistant to posaconazole. However, their susceptibilities to echinocandin were excellent (>93%). In the same way, although C. glabrata was resistant to fluconazole, the susceptibility rate to echinocandins (>90%) was shown to be similar as that of C. tropicalis. Candida resistance mechanisms have mainly been described to include increased efflux of the azole drug, overexpression of the ERG11 gene, or a point mutation in the ERG11 sequence. Regarding C. tropicalis, changes in the permeability of the fungal membrane may be associated with the function of Erg11p and result in cross-resistance to azole agents.20 Empirical antifungal agents should be used with prudence after the revision of the break points. Pfaller et al21 used fluconazole to predict susceptibility and resistance to voriconazole. In this study, we showed a similar pattern, because when C. tropicalis was found to be resistant to fluconazole, it was likely to be resistant to voriconazole as well.
Conclusion
This is the first epidemiological study of candidemia in Taiwan, which included susceptibility tests. In our study, C. tropicalis was the predominant non-albicans Candida species detected, similar to other Asian countries. However, non-susceptibility of non-albicans Candida species to azoles increased after the break point revision and it was widely different compared to the reports from Western countries. The cross-resistance to azoles is a concern in non-albicans Candida. A high resistance rate to voriconazole (80%) was observed if the sensitivity test of C. tropicalis showed resistance to fluconazole; the results of sensitivity test in echinocandins were similar for C. tropicalis and C. glabrata when the isolates of these two non-albicans Candida species were resistant to fluconazole. There was no genetic analysis of the species in this study, and there was no correlation of the data with the clinical outcomes; these are the limitations of this paper.
Acknowledgments
We thank Yee-Chun Chen, Department of Medicine, National Taiwan University Hospital, Taipei, for consultation and advice. We are grateful to the mycology staff at each hospital for their efforts for this study. This study was supported by grants from Taipei Veterans General Hospital (VGH-105-C-051).
Disclosure
The authors report no conflicts of interest in this work.
References
Wayne PA. Clinical and Laboratory Standards Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Fourth International Supplement. CLSI document. 2012:M27–S4. | ||
Cleveland AA, Harrison LH, Farley MM, et al. Declining incidence of candidemia and the shifting epidemiology of Candida resistance in two US metropolitan areas, 2008-2013: results from population-based surveillance. PLoS One. 2015;10(3):e0120452. | ||
Arendrup MC, Dzajic E, Jensen RH, et al. Epidemiological changes with potential implication for antifungal prescription recommendations for fungaemia: data from a nationwide fungaemia surveillance programme. Clin Microbiol Infect. 2013;19(8):e343–e353. | ||
Sandven P, Bevanger L, Digranes A, et al. Candidemia in Norway (1991 to 2003): results from a nationwide study. J Clin Microbiol. 2006;44(6):1977–1981. | ||
Diekema D, Arbefeville S, Boyken L, Kroeger J, Pfaller M. The changing epidemiology of healthcare-associated candidemia over three decades. Diagn Microbiol Infect Dis. 2012;73(1):45–48. | ||
Arendrup MC. Epidemiology of invasive candidiasis. Curr Opin Crit Care. 2010;16(5):445–452. | ||
Pfaller MA, Andes D, Diekema DJ, Espinel-Ingroff A, Sheehan D; CLSI Subcommittee for Antifungal Susceptibility Testing. Wild-type MIC distributions, epidemiological cutoff values and species-specific clinical breakpoints for fluconazole and Candida: time for harmonization of CLSI and EUCAST broth microdilution methods. Drug Resist Updat. 2010;13(6):180–195. | ||
Pfaller MA, Andes D, Arendrup MC, et al. Clinical breakpoints for voriconazole and Candida spp. revisited: review of microbiologic, molecular, pharmacodynamic, and clinical data as they pertain to the development of species-specific interpretive criteria. Diagn Microbiol Infect Dis. 2011;70(3):330–343. | ||
Pfaller MA, Diekema DJ, Andes D, et al; CLSI Subcommittee for Antifungal Testing. Clinical breakpoints for the echinocandins and Candida revisited: integration of molecular, clinical, and microbiological data to arrive at species-specific interpretive criteria. Drug Resist Updat. 2011;14(3):164–176. | ||
Wayne PA. Clinical and Laboratory Standards Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Fourth International Supplement. CLSI document. 2008:M27–S3. | ||
Tan TY, Hsu LY, Alejandria MM, et al. Antifungal susceptibility of invasive Candida bloodstream isolates from the Asia-Pacific region. Med Mycol. 2016;54(5):471–477. | ||
Falagas ME, Roussos N, Vardakas KZ. Relative frequency of albicans and the various non-albicans Candida spp among candidemia isolates from inpatients in various parts of the world: a systematic review. Int J Infect Dis. 2010;14(11):e954–e966. | ||
Wang H, Xu YC, Hsueh PR. Epidemiology of candidemia and antifungal susceptibility in invasive Candida species in the Asia-Pacific region. Future Microbiol. 2016;11(11):1461–1477. | ||
Lin CC, Liu CP, Hsieh FC, Lee CM, Wang WS. Antimicrobial susceptibility and clinical outcomes of Candida parapsilosis bloodstream infections in a tertiary teaching hospital in Northern Taiwan. J Microbiol Immunol Infect. 2015;48(5):552–558. | ||
Chen YC, Kuo SF, Chen FJ, Lee CH. Antifungal susceptibility of Candida species isolated from patients with candidemia in southern Taiwan, 2007–2012: impact of new antifungal breakpoints. Mycoses. 2017;60(2):89–95. | ||
Chen LY, Liao SY, Kuo SC, et al. Changes in the incidence of candidaemia during 2000-2008 in a tertiary medical centre in northern Taiwan. J Hosp Infect. 2011;78(1):50–53. | ||
Yang YL, Chen HT, Lin CC, Chu WL, Lo HJ; TSARY Hospitals. Species distribution and drug susceptibilities of Candida isolates in TSARY 2010. Diagn Microbiol Infect Dis. 2013;76(2):182–186. | ||
Huang YT, Liu CY, Liao CH, Chung KP, Sheng WH, Hsueh PR. Antifungal susceptibilities of Candida isolates causing bloodstream infections at a medical center in Taiwan, 2009-2010. Antimicrob Agents Chemother. 2014;58(7):3814–3819. | ||
Espinel-Ingroff A, Arendrup MC, Pfaller MA, et al. Interlaboratory variability of Caspofungin MICs for Candida spp. Using CLSI and EUCAST methods: should the clinical laboratory be testing this agent? Antimicrob Agents Chemother. 2013;57(12):5836–5842. | ||
Forastiero A, Mesa-Arango AC, Alastruey-Izquierdo A, et al. Candida tropicalis antifungal cross-resistance is related to different azole target (Erg11p) modifications. Antimicrob Agents Chemother. 2013;57(10):4769–4781. | ||
Pfaller MA, Messer SA, Boyken L, et al. Use of fluconazole as a surrogate marker to predict susceptibility and resistance to voriconazole among 13,338 clinical isolates of Candida spp. Tested by clinical and laboratory standards institute-recommended broth microdilution methods. J Clin Microbiol. 2007;45(1):70–75. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.