")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Research Progress on the Efficacy and Safety of Spironolactone in Reversing Left Ventricular Hypertrophy in Hemodialysis Patients
Authors Sun Z, Chen Z, Liu R, Lu G, Li Z, Sun Y
Received 14 October 2022
Accepted for publication 10 January 2023
Published 23 January 2023 Volume 2023:17 Pages 181—190
DOI https://doi.org/10.2147/DDDT.S393480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Zuoya Sun,1 Zhiyuan Chen,1 Ruihong Liu,1 Gang Lu,1 Zhuo Li,1 Yi Sun2
1Department of Family Medicine, the University of Hong Kong-Shenzhen Hospital, Shenzhen, People’s Republic of China; 2Department of Nephrology, Beijing Huairou Hospital, Beijing, People’s Republic of China
Correspondence: Yi Sun, Department of Nephrology, Beijing Huairou Hospital, No. 9 Yongtai North Street, Huairou District, Beijing, 101400, People’s Republic of China, Tel +86-010-69644822, Fax +86-010-69622761, Email [email protected]
Abstract: The mineralocorticoid receptor antagonist spironolactone has been shown to improve cardiac function and reverse left ventricular hypertrophy in heart failure patients, but there are no consistent findings on the efficacy and safety in hemodialysis patients. Abnormal aldosterone secretion plays a critical role in the formation of left ventricular hypertrophy. Because of the existence of “aldosterone escape”, the routine use of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers does not completely inhibit aldosterone secretion. Low-dose spironolactone (25 mg/d) has been found in small-sample clinical studies to have a significant positive impact with respect to decreasing left ventricular mass index, increasing left ventricular ejection fraction, reversing left ventricular hypertrophy, and improving cardiovascular function while still being safe. More prospective multicenter clinical trials with large sample sizes are needed, however, to provide convincing evidence.
Keywords: spironolactone, hemodialysis, left ventricular hypertrophy, LVH, mineralocorticoid receptor antagonists, MRA, hyperkalemia
Introduction
Hemodialysis is a widely used clinical renal replacement therapy for patients with end-stage renal disease (ESRD). Cardiovascular disease morbidity and mortality are particularly high in hemodialysis patients, with a 5-year survival rate of 45% on average.1 Sudden cardiac death (SCD) accounts for 25% of all-cause mortality in ESRD patients.2 Left ventricular hypertrophy (LVH) is a common complication in patients with chronic kidney disease (CKD), and its prevalence rises to 75% at the onset of ESRD.3 A unique feature of cardiac morphology in ESRD patients is a marked increase in left ventricular mass (LVM). ESRD patients usually have increased blood pressure due to volume expansion, renin-angiotensin-aldosterone system (RAAS) activation, and heightened sympathetic activity. Furthermore, these patients can suffer from arterial calcification caused by abnormalities in bone mineral metabolism and collagen crosslinking, which results in a loss of large vessel compliance. Long-term hypertension and decreased arterial compliance cause increased afterload and LVM, resulting in a concentric pattern of LVH.4,5 LVM is directly correlated with the risk of SCD and all-cause mortality, and increased LVM is strongly associated with an increased risk of cardiovascular events (CV).6 In contrast, decreased LVM was closely associated with improved outcomes in ESRD patients.7 As a result, LVM has been shown to be an independent predictor of all-cause and cardiovascular mortality in the hemodialysis population.8
Serum aldosterone levels are increased in hemodialysis patients and are independently related to LVH.9,10 A recent study by Matsumoto et al confirmed that LVH could act as a surrogate endpoint for predicting better survival with spironolactone in dialysis patients, a result confirmed in a subsequent study.11 They also noted that in addition to promoting the reversal of LVH, spironolactone can reduce the risk of cardiovascular morbidity and mortality in hemodialysis patients. However, life-threatening hyperkalemia is the main risk of administering aldosterone antagonists in hemodialysis patients, which restricts their usage by clinicians. Systematic reviews and meta-analyses of multiple studies evaluating the safety and cardiovascular effects of spironolactone in the routine treatment of patients on hemodialysis showed that the additional use of low-dose spironolactone in combination with routine treatment in hemodialysis patients is safe and does not significantly increase serum potassium levels but improves LVH by reducing left ventricular mass index (LVMI) and increasing left ventricular ejection fraction (LVEF), which has a protective effect on the cardiovascular system.12–14 Jiang et al noted that the use of low-dose spironolactone (25 mg/d) in hemodialysis patients is safe and that it does not significantly alter the serum potassium level in their evaluation of the impact of mineralocorticoid receptor antagonists (MRAs) on the cardiovascular system of hemodialysis patients.15
The impact of spironolactone on cardiac function in hemodialysis patients remains controversial and requires confirmation by a large number of clinical studies. This article reviewed the literature in PubMed and EMBASE using mineralocorticoid antagonists, aldosterone antagonists or spironolactone combined with dialysis, renal disease, or kidney failure. We focused on trials using spironolactone intervention and including LVM, LVMI and LVEF as evaluation indicators of LVH and left ventricular systolic function. Our search yielded nine studies which we used to explore the efficacy and safety of spironolactone in hemodialysis patients.
“Aldosterone Escape” Mechanism, and the Role of Spironolactone in Hemodialysis Patients
In epithelial tissues, aldosterone maintains electrolyte homeostasis and intravascular volume balance. On the other hand, in nonepithelial tissues, aldosterone has direct effects on the vasculature and is linked to endothelial dysfunction, cardiac hypertrophy, myocardial fibrosis, left ventricular remodeling, and renal vascular damage. In patients with congestive heart failure (CHF), plasma aldosterone concentrations may reach 20 times normal levels, causing interstitial fibrosis and promoting left ventricular remodeling.16 In hemodialysis patients, the RAAS is activated at any time when hemodynamic instability and a reduction in the effective circulating blood volume threaten the extracellular volume, thereby increasing the production of aldosterone.
In the classical RAAS pathway, renin secreted by periglomerular cells cleaves angiotensinogen synthesized in the liver to form angiotensin I (Ang I). Ang I is converted into active angiotensin II (Ang II) under the action of angiotensin-converting enzyme (ACE) in the pulmonary circulatory system, which can constrict blood vessels and promote the secretion of aldosterone. However, even if renin cannot be generated in a tissue or organ, angiotensin can still be synthesized under the regulation of other cascade components that locally synthesize RAAS, thereby promoting aldosterone secretion.17 According to some studies, myocardial necrosis and myocardial cells are stretched, and renin expression in the heart is greatly increased, which is another pathway of local RAAS activation under pathological conditions.18,19 Currently, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEIs/ARBs) are the most commonly used medications to antagonize the RAAS and improve renal function in patients with CKD.20 In patients with ESRD, ACEIs/ARBs can effectively lower blood pressure, improve cardiac remodeling, and play an important role in protecting cardiac and cerebrovascular functions in hemodialysis patients. These medications can also significantly reduce the mortality of hemodialysis patients.21 Despite the many advantages of ACEIs/ARBs, due to the phenomenon of “aldosterone escape”, even routine and sufficient use of ACEIs/ARBs cannot completely inhibit the production of aldosterone for an extended period of time, and it is difficult to maintain low blood aldosterone levels. Although aldosterone levels decrease for a short time, they gradually return to the previous or even higher concentrations.16 Bomback et al reported that 40–53% of patients are expected to experience a rebound in plasma aldosterone levels after receiving ACEI or ARB due to the phenomenon of aldosterone breakthrough.22 Abnormally high plasma aldosterone levels induce hyperfibrosis in cardiomyocytes and exacerbate ventricular remodeling.23
For hemodialysis patients, the cardiovascular protective effects of spironolactone are many, and include its diuretic and nondiuretic antihypertensive effects (such as reducing sympathetic tone, regulating endothelial cell function, and improving vascular compliance),24 antiatherosclerosis effect, reversal of LVH, and improvement of cardiac systolic function and heart rate variability.25
Related Clinical Researches of Spironolactone in Hemodialysis Patients
A growing number of researchers are examining whether spironolactone can reduce mortality and improve cardiovascular function in hemodialysis patients while ensuring safety. Despite the lack of large, randomized end-point trials, useful insights can be gained from a systematic review of the short-term, small clinical studies conducted to date. The basic characteristics and results of the clinical trials included in our study are shown in Table 1.
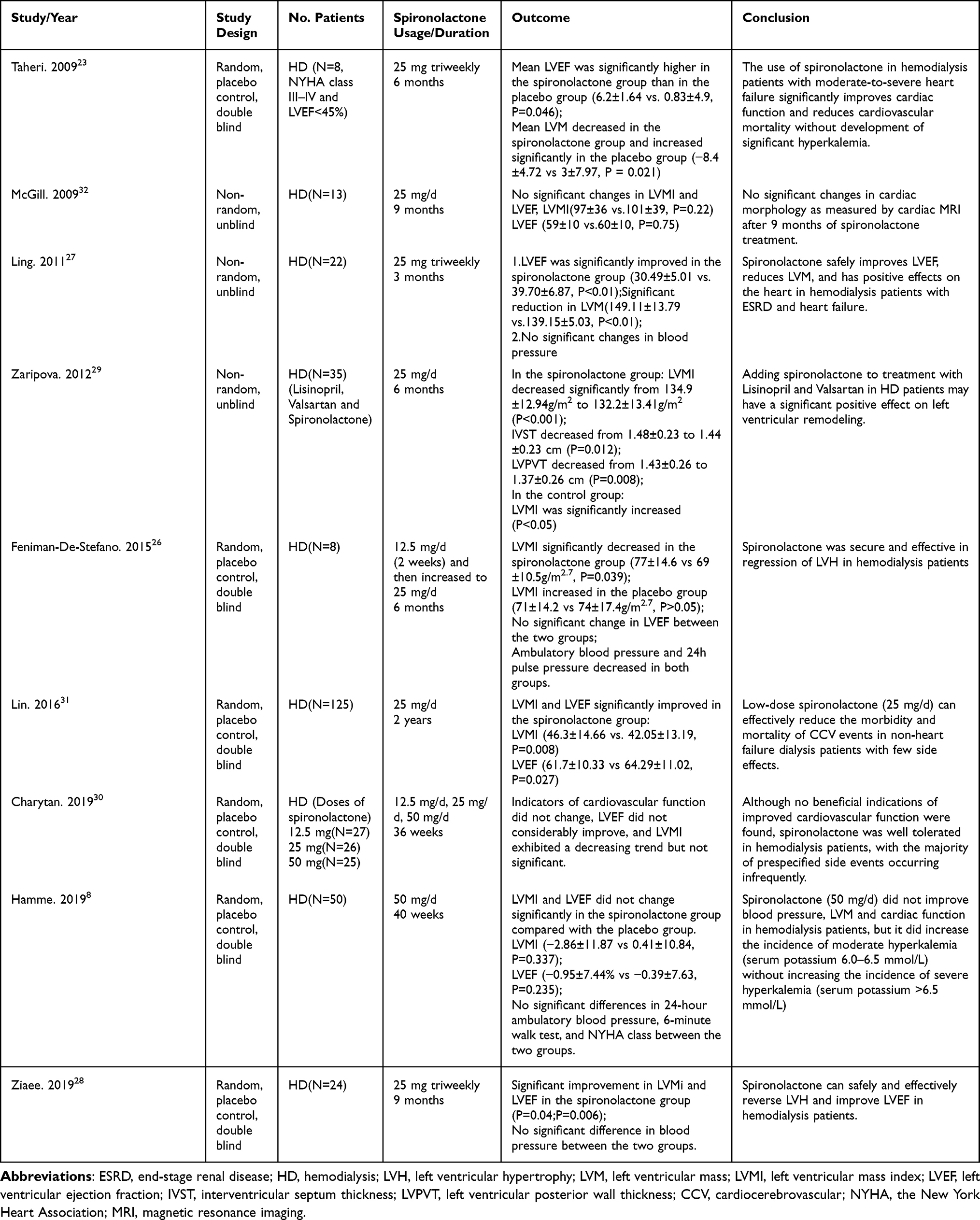 |
Table 1 Characteristics and Cardiovascular Outcomes of 9 Clinical Trials in Hemodialysis Patients |
Feniman-De-StefanoD et al performed a controlled, randomized, double blind study to verify the safety and efficacy of spironolactone in the treatment of LVH in hemodialysis patients without heart failure, 17 patients were included with spironolactone (maximum dose 25 mg/d).26 After 6 months, LVMI in the treatment group decreased from (77±14.6) g/m2.7 to (69±10.5) g/m2.7; however, the placebo group increased from (71±14.2) g/m2.7 to (74 ±14.7) g/m2.7. They concluded that LVH is the major risk factor for cardiovascular events in hemodialysis population. And spironolactone is safe and effective in the treating LVH in hemodialysis patients.
Taheri et al enrolled 16 patients with LVEF≤45% and moderate-to-severe heart failure in a study evaluating whether low-dose spironolactone could be administered in hemodialysis patients with moderate-to-severe heart failure.23 Eight patients in the treatment group received spironolactone 25 mg after each dialysis session, and the rest received a placebo. After 6 months of treatment, the mean LVEF increased significantly more in the treatment group than in the placebo group (6.2±1.64 vs 0.83±4.9, P=0.046). The mean LVM decreased in the treatment group, but increased significantly in the placebo group during the study period (−8.4±4.72 vs.3±7.97, P=0.021). This study found that spironolactone improved considerably cardiac function and decreased LVM in continuous hemodialysis patients with moderate to severe heart failure without developing significant hyperkalemia.
Likewise, the effectiveness and safety of spironolactone in hemodialysis patients with ESRD and heart failure were also evaluated by liang et al.27 The study included 44 patients with heart failure (the New York Heart Association (NYHA) class 3 and 4 and LVEF≤45%), the patients received spironolactone (25 mg three times/week) for 3 months. The results reveal that, when compared to the control group, there were significant differences in LVEF and LVM before and after the test, and that improvement in LVEF and LVM increased with treatment duration. Spironolactone was found to safely improve LVEF and lower LVM in hemodialysis patients with ESRD and heart failure. Furthermore, spironolactone may have an independent beneficial effect on LVM reduction. Ziaee et al used the same dose and frequency of spironolactone for hemodialysis patients.28 After 9 months, the LVMI and LVEF of the treatment group were significantly improved compared with the control group (P=0.04, P=0.006), however there was no difference in blood pressure between the two groups. Spironolactone was also proven to be safe and effective in reversing LVH and improving LVEF.
Because ACEIs or/and ARBs are often used by hemodialysis patients with heart failure, researchers are more concerned about the occurrence of hyperkalemia once spironolactone is added. Zaripova et al conducted a study evaluating the additional effect of spironolactone on LVH in anuric hemodialysis patients already receiving ACEI and ARB.29 The treatment group (n=36) in addition to Lisinopril and Valsartan received Spironolactone 25 mg daily, the control group (n=35) received Lisinopril and Valsartan. After 6 months, echocardiography in the treatment group showed that LVMI significantly decreased from 134.9±12.94 to 132.2±13.41 g/m2 (P<0.001), interventricular septum thickness (IVST) decreased from 1.48±0.23cm to 1.44± 0.23cm (P=0.012). And throughout the whole course of treatment, there were no cases of severe hyperkalemia in either group. They came to the conclusion that spironolactone may significantly improve left ventricular remodeling in hemodialysis patients receiving treatment with Lisinopril and Valsartan.
Charytan et al conducted a double-blind, placebo-controlled, multiple dosage spironolactone dialysis trial (SPin-D) involving 129 patients with hemodialysis. They were randomized to placebo (n=51) or spironolactone 12.5 mg (n=27), 25 mg (n=26), or 50 mg (n=25) daily.30 After 36 weeks of observation, compared to the placebo group, the multi-dose spironolactone group was well tolerated and safe in hemodialysis patients, however there were no significant changes in LVMI and LVEF, and no convincing improvements in cardiac structure or function. SPin-D differs from previous trials in that it evaluated the efficacy of various doses of spironolactone. According to this study, spironolactone 25 mg/d is safer for hemodialysis patients under proper monitoring than 50 mg/d, and 25 mg/d would be the best option if a single fixed dose is used.
Some small pilot studies have validated the potential advantages of spironolactone, however outcomes from several recently published research have not been as anticipated. The Mineralocorticoid Receptor Antagonists in End-Stage Renal Disease (MiREnDa) trial was a randomized, double-blind, placebo-controlled trial to investigate the efficacy and safety of spironolactone in hemodialysis patients.8 The primary efficacy endpoint of this study was the change of LVMI as measured by cardiac magnetic resonance (CMR) scans. And the safety endpoints were development of hyperkalemia and change in residual renal function. 97 hemodialysis patients were randomized to the spironolactone group (n=50) was given spironolactone 50 mg/d, and the placebo group (n=47). After 40 weeks of treatment, the LVMI of the spironolactone group was not significantly changed compared with the placebo group (−2.86±11.87 vs 0.41±10.84g /m2, P=0.337). In this study, treatment with spironolactone 50 mg/d did not change LVMI, cardiac function, or blood pressure in hemodialysis patients.
A 2-year multicentric, randomized, placebo-controlled study by Lin et al was to evaluate the long-term effects and adverse effects of spironolactone on hemodialysis patients.31 253 non–heart failure dialysis patients with ESRD were randomly assigned to the spironolactone group (25 mg/d, n=125) or the placebo group (n=128). During the 2-year follow-up, in the spironolactone group, LVMI decreased by 8.7 g/m2.7, LVEF increased by 5.1%, and the incidence of death due to cardiocerebrovascular (CCV) events or any cause in dialysis patients with ESRD was significantly reduced. Their study demonstrated that low-dose spironolactone is effective in reducing the risk of CCV morbidity and mortality in non-heart failure dialysis patients with few side effects. In the article of MiREnDa trial, authors discuss the differences from the study by Lin et al and the reasons for the different results.8 One explanation for these inconsistent results could be the pattern of renal replacement therapy: hemodialysis was used in MiREnDa, however, a mix of 60% hemodialysis and 40% continuous ambulatory peritoneal dialysis in the study by Lin et al. The important cause of LVH are recurrent volume expansions and the presence of an arteriovenous fistula in hemodialysis patients, both of which are absent on continuous ambulatory peritoneal dialysis. Another distinction is the measurement mode of LVM. CMR used in the MiREnDa trial, whereas echocardiography was used in the study of Lin et al. Furthermore, the difference in study duration (9 months vs 2 years) and the shorter observation period may not have been sufficient to observe changes in cardiac structure and function.
McGill et al treated 13 hemodialysis patients with spironolactone 25 mg/d for 9 months, but did not find any changes in LVM by CMR.32 In contrast, Taheri et al reported that spironolactone (25 mg, three times/week) was administered to 16 hemodialysis patients with moderate-to-severe heart failure, after 6 months of treatment, LVM (8.4±4.72 vs 3.0±7.97) and LVEF (6.2±1.64 vs 0.83±4.9) were significantly reduced by echocardiography, and the difference was statistically significant.23 Due to the small sample sizes and inconsistent measuring techniques, as well as the fact that many criteria are not unified, the results of the aforementioned studies different.
In a meta-analysis to evaluate the safety and cardiovascular effects of low-dose spironolactone on end-stage renal failure patients undergoing hemodialysis and conventional treatment, nine trials with a total sample size of 765 patients were included in the study, among them, there were 138 patients in the spironolactone group.12 The results showed that the LVMI of the spironolactone group was significantly lower than that of the control group [SMD=−0.58, 95% CI (−0.82, −0.34), P<0.00001]; the LVEF of the spironolactone group was significantly higher than that of the control group [MD=4.91, 95% CI (2.58, 7.24), P<0.00001], and significantly reduced all-cause mortality [OR=0.4, 95% CI (0.42, 0.66), P=0.0003] and CCV mortality [OR=0.4, 95% CI (0.22, 0.72), P=0.002].This study indicated that on the basis of conventional treatment, the addition of low-dose spironolactone can significantly improve LVMI and LVEF in hemodialysis patients, and have a protective effect on their cardiovascular system without significantly increasing serum potassium levels.
Safety of Spironolactone in Hemodialysis Patients
Is it safe for hemodialysis patients to take MRAs? This is an issue that treating physicians are rightfully concerned about and cannot ignore while considering using this class of therapies. For the examination of safety, researchers tend to focus on the incidence of hyperkalemia. Several studies have demonstrated that spironolactone can greatly improve the prognosis of patients with heart failure and myocardial infarction without renal insufficiency.4,33 Because of its “sodium excretion and potassium retention” effect, there are still some risks associated with the use of ESRD in hemodialysis. However, some researchers suggest that hyperkalemia may not be a problem in hemodialysis patients because the factors affecting serum potassium in dialysis patients are mostly controlled by dialysis rather than renal tubular function.31,34 In a meta-analysis evaluating the benefits and side effects of mineralocorticoid receptor antagonists in renal failure patients undergoing dialysis, 14 eligible randomized controlled trials from 2005 to 2020 were included, with a total of 1309 participants.35 The study showed that mineralocorticoid receptor antagonists may improve clinical outcomes in patients with renal failure without significantly increasing the risk of hyperkalemia. The safety of taking spironolactone in hemodialysis patients benefits from a steady potassium level in the body, and it must be emphasized that these patients undergo strict drug treatment monitoring throughout the process.26 An overview of the effects of spironolactone on serum potassium and adverse reactions in HD patients in 9 clinical trials is shown in Table 2.
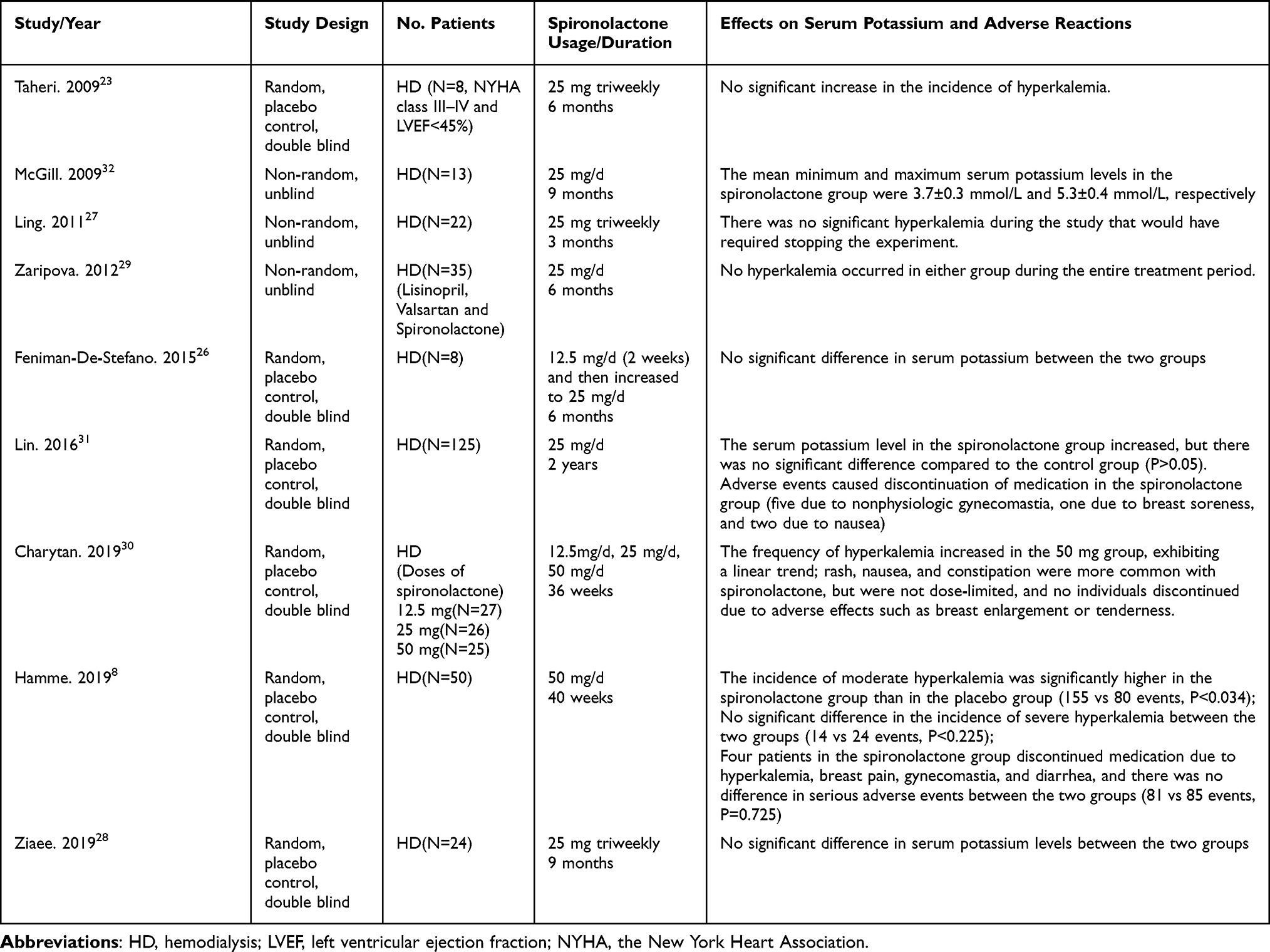 |
Table 2 Effects of Spironolactone on Serum Potassium and Adverse Reactions in HD Patients |
Lin et al discovered that after 2 years of follow-up, the serum potassium level in the spironolactone group (25 mg/d) increased, although there was no significant difference compared to the control group (P>0.05).31 In addition, adverse events caused discontinuation of medication in the spironolactone group (five due to nonphysiologic gynecomastia, one due to breast soreness, and two due to nausea). The authors also pointed out that the use of spironolactone is safer in dialysis patients than in non dialysis patients because potassium is metabolized very little through the kidneys and is excreted through dialysis, which can be a great advantage. In the MiREnDa trial, spironolactone increased the frequency of moderate hyperkalemia (potassium levels of 6.0–6.5 mmol/L) compared with the control group but did not increase severe hyperkalemia (≥6.5 mmol/L).8 In addition, 4 patients in the spironolactone group discontinued medication due to hyperkalemia, breast pain, gynecomastia, and diarrhea. Charytan et al evaluated the safety and efficacy of multiple spironolactone doses (12.5 mg/d, 25 mg/d, 50 mg/d) in a randomized placebo-controlled, double-blind experiment (Spin-D).30 After 36 weeks of follow-up in 129 hemodialysis patients, the incidence of hyperkalemia was similar between the spironolactone and placebo groups; however, a significant linear trend, with an increase in the incidence of hyperkalemia at the 50 mg/day dose was reported. In terms of other adverse reactions, spironolactone was well tolerated by patients across the different doses of spironolactone examined compared with the placebo group. There were no patients who discontinued use owing to the adverse events of breast enlargement or tenderness, and although the incidence of constipation and rash increased, the increases were minor and generally not dose-limiting.
In several of the studies included in this article, patients were treated with spironolactone after hemodialysis to avoid transient potassium elevations, and some of these studies followed hemodialysis patients on spironolactone 25 mg daily for 6 months to 12 months.23,27,28 Although variables such as dietary potassium consumption, dialysate potassium concentration, spironolactone dose, and use of ACEIs/ARBs differed between studies, the incidence of hyperkalemia in patients treated with spironolactone did not increase. This outcome is thought to be connected to the promptness and sufficiency of dialysis as well as the adjustability of the dialysate potassium concentration. Therefore, even if spironolactone is administered in combination with ACEIs and/or ARBs, the risk of serious hyperkalemia is very minimal, provided that serum potassium is closely monitored and that dialysate composition is promptly adjusted.
Spironolactone is safe in the short-term treatment of hemodialysis patients, according to reviews of six prospective trials by Chua et al and ten studies by Baker et al, however more large controlled trials are required before definitive treatment recommendations can be given.34,36 A recent meta-analysis of nine trials, including a total of 1128 chronic dialysis patients, examined the effectiveness and safety of low-dose MRAs in dialysis patients who received low-dose MRA (25 mg/day spironolactone or 50 mg spironolactone 3 times/week).37 The authors concluded that low-dose MRAs increase the incidence of mild hyperkalemia (serum potassium level 5.5 mmol/L) but not moderate or severe hyperkalemia (serum potassium level 6.0 mmol/L and 6.5 mmol/L). The fact that low-dose MRAs do not raise the risk of moderate-to-severe hyperkalemia and necessitate close monitoring of serum potassium levels supports the idea that low-dose MRA use may be safe. Similarly, in a review evaluating the benefits and harms of aldosterone receptor antagonists in ESRD patients receiving hemodialysis and peritoneal dialysis, Hasegawa et al found that aldosterone antagonists have little or no effect on the risk of developing hyperkalemia and may lower the risk of cardiovascular and cerebrovascular diseases.38 Furthermore, studies have shown that the SPin-D and MiREnDa trials are reliable in terms of spironolactone dose and safety; as long as the patient is properly monitored and the relevant factors affecting serum potassium (eg, diet, dialysate potassium concentration, and drugs that affect potassium metabolism) are taken into account, spironolactone up to 25 mg/d is quite safe.13,39
In terms of side effects, the second-generation steroid MRA eplerenone has higher mineralocorticoid receptor (MR) selectivity than spironolactone and therefore is less likely to cause anti-androgenic and progestational side effects due to unspecific binding to androgen and progesterone receptors.40,41 However, eplerenone lacks the potency of spironolactone because its affinity for MR is 40 times lower than that of spironolactone.42 Walsh et al conducted a placebo-controlled, multicenter randomized controlled trial to investigate the safety and tolerability of eplerenone in hemodialysis patients.43 The participants were randomly assigned to receive eplerenone 50 mg daily (n = 77) or a placebo (n = 77) for 13 weeks. The results showed that 9 patients (11.7%) in the eplerenone group developed hyperkalemia (potassium level > 6.5 mEq/L) compared with 2 patients (2.6%) in the placebo group. They concluded that eplerenone increased the risk of hyperkalemia but did not result in an excess need to permanently discontinue the drug. It is also worth noting that none of the sex hormone-related side effects, including gynecomastia, breast pain, erectile dysfunction, etc., were observed in this trial using eplerenone. Additionally, finerenone is a novel nonsteroidal MRA with high affinity and a higher selectivity for MR than spironolactone or eplerenone (over 500-fold more selective for MR than for any other steroid receptor), and thereby effectively avoids the adverse effects of traditional steroidal MRAs.40,42 Finerenone is distributed almost equally between cardiac and renal tissues, reducing accumulation in the kidney.44 Studies have suggested that finerenone has better safety and tolerability than other MRAs in patients with renal impairment.45,46 Despite the fact that eplerenone and finerenone appear superior to spironolactone in terms of adverse effects, multicenter, large-sample randomized controlled trials in patients with MHD are necessary to confirm this relative advantage.
Currently, there are two ongoing large, multicenter, major-outcome clinical trials, both of which are using spironolactone up to 25 mg/d: ACHIEVE (Aldosterone blockade for Health Improvement Evaluation in End stage renal disease trial; NCT03020303) and ALCHEMIST (Aldosterone antagonist Chronic Hemodialysis Interventional Survival Trial; NCT01848639). ALCHEMIST aims to recruit 825 high-risk chronic hemodialysis patients, and ACHIEVE aims to recruit 2750 chronic hemodialysis or peritoneal dialysis patients. We look forward to more convincing results from these two large multicenter clinical studies.
Conclusion
According to the current small pilot trials, adding low-dose spironolactone (25 mg/d) to the treatment protocol of hemodialysis patients is safe and effective at reversing LVH and improving cardiovascular function. In addition, we acknowledge that this conclusion is subject to publication bias, presumably as a result of the multiple positive small center series. Whether 25 mg/d is the ideal dose in terms of safety and efficacy remains a crucial question; results from additional prospective, large-scale, multicenter clinical trials are required to establish the optimal dose and confirm clinical efficacy. We anticipate more persuasive data from the two large multicenter clinical trials that are presently underway.
Abbreviations
CKD, Chronic kidney disease; ESRD, End-stage renal disease; SCD, Sudden cardiac death; LVH, Left ventricular hypertrophy; LVM, Left ventricular mass; LVMI, Left ventricular mass index; LVEF, left ventricular ejection fraction; RAAS, Renin-angiotensin-aldosterone system; MRAs, Mineralocorticoid Receptor Antagonists; ACEIs/ARBs, Angiotensin-converting enzyme inhibitors/Angiotensin receptor blockers; CV, Cardiovascular; CCV, Cardiocerebrovascular; CHF, Congestive heart failure; NYHA, the New York Heart Association; IVST, Interventricular septum thickness; CMR, Cardiac magnetic resonance; MR, the mineralocorticoid receptor.
Acknowledgments
We would like to appreciate all members participated in this work and the Department of Family Medicine of the University of Hong Kong-Shenzhen Hospital for their support.
Funding
This review was funded by Shenzhen Key Medical Discipline Construction Fund (NO.SP2018-C0071).
Disclosure
The authors declare no potential conflicts of interest in this work.
References
1. Pippias M, Jager KJ, Kramer A, et al. The changing trends and outcomes in renal replacement therapy: data from the ERA-EDTA Registry. Nephrol Dial Transplant. 2016;31(5):831–841. doi:10.1093/ndt/gfv327
2. Wheeler DC, London GM, Parfrey PS, et al. Effects of cinacalcet on atherosclerotic and nonatherosclerotic cardiovascular events in patients receiving hemodialysis: the evaluation of cinacalcet hcl therapy to lower cardiovascular events (EVOLVE) trial. J Am Heart Assoc. 2014;3(6):e001363. doi:10.1161/JAHA.114.001363
3. Middleton RJ, Parfrey PS, Foley RN. Left ventricular hypertrophy in the renal patient. JASN. 2001;12(5):1079–1084. doi:10.1681/ASN.V1251079
4. Zannad F, Alla F, Dousset B, Perez A, Pitt B. Limitation of excessive extracellular matrix turnover may contribute to survival benefit of spironolactone therapy in patients with congestive heart failure: insights from the randomized aldactone evaluation study (RALES). rales investigators. Circulation. 2000;102(22):2700–2706. doi:10.1161/01.CIR.102.22.2700
5. Glassock RJ, Pecoits-Filho R, Barberato SH. Left ventricular mass in chronic kidney disease and ESRD. CJASN. 2009;4(Suppl 1):S79–S91. doi:10.2215/CJN.04860709
6. Mostovaya IM, Bots ML, van den Dorpel MA, et al. Left ventricular mass in dialysis patients, determinants and relation with outcome. Results from the COnvective TRansport STudy (CONTRAST). PLoS One. 2014;9(2):e84587. doi:10.1371/journal.pone.0084587
7. Paoletti E, Bellino D, Signori A, et al. Regression of asymptomatic cardiomyopathy and clinical outcome of renal transplant recipients: a long-term prospective cohort study. Nephrol Dial Transplant. 2016;31(7):1168–1174. doi:10.1093/ndt/gfv354
8. Hammer F, Malzahn U, Donhauser J, et al. A randomized controlled trial of the effect of spironolactone on left ventricular mass in hemodialysis patients. Kidney Int. 2019;95(4):983–991. doi:10.1016/j.kint.2018.11.025
9. Sato A, Funder JW, Saruta T. Involvement of aldosterone in left ventricular hypertrophy of patients with end-stage renal failure treated with hemodialysis. Am J Hypertens. 1999;12(9 Pt 1):867–873. doi:10.1016/S0895-7061(99)00066-7
10. Steigerwalt S, Zafar A, Mesiha N, Gardin J, Provenzano R. Role of aldosterone in left ventricular hypertrophy among African-American patients with end-stage renal disease on hemodialysis. Am J Nephrol. 2007;27(2):159–163. doi:10.1159/000100106
11. Matsumoto Y, Mori Y, Kageyama S, et al. Spironolactone reduces cardiovascular and cerebrovascular morbidity and mortality in hemodialysis patients. J Am Coll Cardiol. 2014;63(6):528–536. doi:10.1016/j.jacc.2013.09.056
12. Zeng Q, Zhou X, Xu G. Safety evaluation and cardiovascular effect of additional use of spironolactone in hemodialysis patients: a meta-analysis. Drug Des Devel Ther. 2019;13:1487–1499. doi:10.2147/DDDT.S189454
13. Rossignol P, Frimat L, Zannad F. The safety of mineralocorticoid antagonists in maintenance hemodialysis patients: two steps forward. Kidney Int. 2019;95(4):747–749. doi:10.1016/j.kint.2018.12.006
14. Bhinder J, Patibandla S, Gupta CA, Levine A, Gass AL, Lanier GM. Mineralocorticoid receptor antagonist use in heart failure with reduced ejection fraction and end-stage renal disease patients on dialysis: a literature review. Cardiol Rev. 2020;28(3):107–115. doi:10.1097/CRD.0000000000000286
15. Jiang M, Bi W. The effect of aldosterone receptor antagonists on cardiovascular system in maintenance hemodialysis patients. J Clin Nephrol. 2020;20(3):239–242.
16. Lakkis J, Lu WX, Weir MR. RAAS escape: a real clinical entity that may be important in the progression of cardiovascular and renal disease. Curr Hypertens Rep. 2003;5(5):408–417. doi:10.1007/s11906-003-0087-9
17. Kurdi M, De Mello WC, Booz GW. Working outside the system: an update on the unconventional behavior of the renin-angiotensin system components. Int J Biochem Cell Biol. 2005;37(7):1357–1367. doi:10.1016/j.biocel.2005.01.012
18. Passier RC, Smits JF, Verluyten MJ, Daemen MJ. Expression and localization of renin and angiotensinogen in rat heart after myocardial infarction. Am J Physiol. 1996;271(3 Pt 2):H1040–H1048. doi:10.1152/ajpheart.1996.271.3.H1040
19. Malhotra R, Sadoshima J, Brosius FC, Izumo S. Mechanical stretch and angiotensin II differentially upregulate the renin-angiotensin system in cardiac myocytes In vitro. Circ Res. 1999;85(2):137–146. doi:10.1161/01.RES.85.2.137
20. Wu CK, Yang YH, Juang JJ, et al. Effects of angiotensin converting enzyme inhibition or angiotensin receptor blockade in dialysis patients: a nationwide data survey and propensity analysis. Medicine. 2015;94(3):e424. doi:10.1097/MD.0000000000000424
21. Efrati S, Zaidenstein R, Dishy V, et al. ACE inhibitors and survival of hemodialysis patients. Am J Kidney Dis. 2002;40(5):1023–1029. doi:10.1053/ajkd.2002.36340
22. Bomback AS, Klemmer PJ. The incidence and implications of aldosterone breakthrough. Nat Clin Pract Nephrol. 2007;3(9):486–492. doi:10.1038/ncpneph0575
23. Taheri S, Mortazavi M, Shahidi S, et al. Spironolactone in chronic hemodialysis patients improves cardiac function. Saudi J Kidney Dis Tran. 2009;20(3):392–397.
24. Rahmouni K, Sibug RM, De Kloet ER, et al. Effects of brain mineralocorticoid receptor blockade on blood pressure and renal functions in DOCA-salt hypertension. Eur J Pharmacol. 2002;436(3):207–216. doi:10.1016/S0014-2999(01)01586-2
25. Michea L, Vukusich A, González M, Zehnder C, Marusic ET. Effect of spironolactone on K(+) homeostasis and ENaC expression in lymphocytes from chronic hemodialysis patients. Kidney Int. 2004;66(4):1647–1653. doi:10.1111/j.1523-1755.2004.00931.x
26. Feniman-De-Stefano GM, Zanati-Basan SG, De Stefano LM, et al. Spironolactone is secure and reduces left ventricular hypertrophy in hemodialysis patients. Ther Adv Cardiovasc Dis. 2015;9(4):158–167. doi:10.1177/1753944715591448
27. Liang Y. The effects of spironolactone on LVEF and LVM in hemodialysis patients with end stage renal disease. Chin J Clin. 2011;5(18):5271–5275.
28. Ziaee S, Karvandi M, Ziaee N, Ghozloujeh Z, Shahrbaf M, Roshan A. Effects of spironolactone on cardiovascular complications in hemodialysis patients of Taleghani Hospital during the period of 2016–2017: a randomized double-blind controlled clinical trial. Iranian Heart J. 2019;20(1):45–52.
29. Zaripova I, Kayukov I, Essaian A, Nimgirova A. Renin angiotensin aldosterone system blockade and left ventricular hypertrophy in maintenance hemodialysis patients. Nephrol Dial Transplant. 2012;27(Suppl 2):ii238.
30. Charytan DM, Himmelfarb J, Ikizler TA, et al. Safety and cardiovascular efficacy of spironolactone in dialysis-dependent ESRD (SPin-D): a randomized, placebo-controlled, multiple dosage trial. Kidney Int. 2019;95(4):973–982. doi:10.1016/j.kint.2018.08.034
31. Lin C, Zhang Q, Zhang H, Long-Term LA. Effects of low-dose spironolactone on chronic dialysis patients: a randomized placebo-controlled study. J Clin Hypertens. 2016;18(2):121–128. doi:10.1111/jch.12628
32. Mcgill RL, Biederman RW, Getts RT. Cardiac magnetic resonance imaging in hemodialysis patients. J Nephrol. 2009;22(3):367–372.
33. Hayashi M, Tsutamoto T, Wada A, et al. Immediate administration of mineralocorticoid receptor antagonist spironolactone prevents post-infarct left ventricular remodeling associated with suppression of a marker of myocardial collagen synthesis in patients with first anterior acute myocardial infarction. Circulation. 2003;107(20):2559–2565. doi:10.1161/01.CIR.0000068340.96506.0F
34. Chua D, Lo A, Lo C. Spironolactone use in heart failure patients with end-stage renal disease on hemodialysis: is it safe? Clin Cardiol. 2010;33(10):604–608. doi:10.1002/clc.20838
35. Chen KT, Kang YN, Lin YC, et al. Efficacy and safety of mineralocorticoid receptor antagonists in kidney failure patients treated with dialysis: a systematic review and meta-analysis. CJASN. 2021;16(6):916–925. doi:10.2215/CJN.15841020
36. Baker WL, White WB. Safety of mineralocorticoid receptor antagonists in patients receiving hemodialysis. Ann Pharmacother. 2012;46(6):889–894. doi:10.1345/aph.1R011
37. Zhu Y, Liu Y, Cai R, et al. The safety and efficacy of low-dose mineralocorticoid receptor antagonists in dialysis patients: a meta-analysis. Medicine. 2021;100(8):e24882. doi:10.1097/MD.0000000000024882
38. Hasegawa T, Nishiwaki H, Ota E, Levack WM, Noma H. Aldosterone antagonists for people with chronic kidney disease requiring dialysis. Cochrane Database Syst Rev. 2021;2(2):Cd013109. doi:10.1002/14651858.CD013109.pub2
39. Roehm B, Gulati G, Weiner DE. Heart failure management in dialysis patients: many treatment options with no clear evidence. Semin Dial. 2020;33(3):198–208. doi:10.1111/sdi.12878
40. Kintscher U, Bakris GL, Kolkhof P. Novel non-steroidal mineralocorticoid receptor antagonists in cardiorenal disease. Br J Pharmacol. 2022;179(13):3220–3234. doi:10.1111/bph.15747
41. Patel V, Joharapurkar A, Jain M. Role of mineralocorticoid receptor antagonists in kidney diseases. Drug Dev Res. 2021;82(3):341–363. doi:10.1002/ddr.21760
42. Capelli I, Gasperoni L, Ruggeri M, et al. New mineralocorticoid receptor antagonists: update on their use in chronic kidney disease and heart failure. J Nephrol. 2020;33(1):37–48. doi:10.1007/s40620-019-00600-7
43. Walsh M, Manns B, Garg AX, et al. The safety of eplerenone in hemodialysis patients: a noninferiority randomized controlled trial. CJASN. 2015;10(9):1602–1608. doi:10.2215/CJN.12371214
44. Heinig R, Kimmeskamp-Kirschbaum N, Halabi A, Lentini S. Pharmacokinetics of the novel nonsteroidal mineralocorticoid receptor antagonist finerenone (BAY 94-8862) in individuals with renal impairment. Clin Pharmacol Drug Dev. 2016;5(6):488–501. doi:10.1002/cpdd.263
45. Pitt B, Kober L, Ponikowski P, et al. Safety and tolerability of the novel non-steroidal mineralocorticoid receptor antagonist BAY 94-8862 in patients with chronic heart failure and mild or moderate chronic kidney disease: a randomized, double-blind trial. Eur Heart J. 2013;34(31):2453–2463. doi:10.1093/eurheartj/eht187
46. Bakris GL, Agarwal R, Chan JC, et al. Effect of finerenone on albuminuria in patients with diabetic nephropathy: a randomized clinical trial. JAMA. 2015;314(9):884–894. doi:10.1001/jama.2015.10081
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.