")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Renal Function Impairment and Associated Factors Among Adult HIV-Positive Patients Attending Antiretroviral Therapy Clinic in Mettu Karl Referral Hospital: Cross-Sectional Study
Authors Kefeni BT , Hajito KW , Getnet M
Received 16 January 2021
Accepted for publication 19 May 2021
Published 9 June 2021 Volume 2021:13 Pages 631—640
DOI https://doi.org/10.2147/HIV.S301748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Bilisumamulifna Tefera Kefeni,1 Kifle Woldemichael Hajito,2 Masrie Getnet2
1Department of Public Health, College of Health Sciences, Mettu University, Mettu, Ethiopia; 2Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, Jimma University, Jimma, Ethiopia
Correspondence: Bilisumamulifna Tefera Kefeni Tel +251-911-537-978
Email [email protected]
Background: Human immunodeficiency virus (HIV) affects every organ system in the body through impairment or by rendering the patient vulnerable to opportunistic infections. The kidney is the vital organ in the excretion of waste products and toxins (urea, creatinine and uric acid), and regulation of extracellular fluid volume, serum osmolality and electrolyte concentrations. The risk of kidney disease is greater in HIV-infected individuals than in the general population. This study aimed to assess the magnitude of renal function impairment and its associated factors among adult HIV-positive patients attending an ART clinic in Mettu Karl Referral Hospital, Mettu town, south-west Ethiopia.
Methods: The institution-based, cross-sectional quantitative study was conducted from March 8 to May 30, 2020. A total of 352 clients participated and a systematic sampling technique was used to allocate study participants. Data were entered into Epi data and exported to SPSS version 22 for analysis. Bivariate analysis was conducted to identify candidate variables for multivariate analysis at P < 0.25. Multivariable logistic regression analysis was conducted to determine the predictors of renal function impairment with ART. P value < 0.05 was considered to indicate statistical significance.
Results: A total of 352 HIV-infected patients participated in this study with a response rate of 98.1%. Out of 352 HIV patients on ART, 73 (20.7%) were found to have renal function impairment. Cigarette smoking [AOR = 9.60, 95% CI: 4.73– 19.48], diabetes mellitus [AOR = 6.16, 95% CI: 2.79– 13.59], hypertension [AOR = 4.71, 95% CI: 1.98– 11.17] and low CD4 count [AOR = 6.47, 95% CI: 3.31– 12.64] were found to be independent predictors of renal function impairment among adult HIV positive patients.
Conclusion: The prevalence of renal function impairment among HIV patients on ART is high. Hypertension, diabetes, cigarette smoking and low CD4 count were associated factors of renal function impairment. HIV patients on ART should be regularly screened for early diagnosis and management of renal function impairment.
Keywords: renal impairment, HIV positive, ART, Mettu
Background
Human immunodeficiency virus (HIV) affects every organ system in the body through impairment or by rendering the patient vulnerable to opportunistic infections.1 The kidney is the vital organ in the excretion of waste products and toxins (urea, creatinine and uric acid), and regulation of extracellular fluid volume, serum osmolality and electrolyte concentrations.2
Kidney is among the commonest sites of infection in HIV-positive patients.1 Renal disease in people with HIVmanifests in multiple ways, including acute kidney injury (AKI), HIV-associated kidney disease, comorbid chronic kidney disease (CKD), and treatment-related kidney toxicity.3 Screening for renal disease is recommended for all HIV-infected ptients at diagnosis of the infection and at the beginning of antiretroviral therapy (ART).4
Globally, renal function impairment among adults living with HIV estimated using the MDRD was 6.4%, using the CKD-EPI equation was 4.8% and using the Cockcroft-Gault (CG) formula was 12.3% and renal function impairment is different in various part of the world; its magnitude in North America was found to be 6.5%, in South America 6.2%, in Europe 2.7%.5
In sub-Saharan Africa (SSA) the prevalence of renal function impairment in people living with HIV (PLWHIV) has been shown to be high, ranging from 25–77%.6–8 In Ethiopia, two studies conducted in Bahir Dar town and Jimma showed that 30.1% and 18.2% of HIV patients, respectively had renal function impairment.9,10
The risk of kidney disease is greater in HIV-infected individuals than in the general population. It is associated with poor outcomes, including increased morbidity and risk of death.11 Early diagnosis and regular monitoring for renal impairment in HIV-positive patients is necessary for prognosis, medication dosing, and treatment. The World Health Organization recommends assessing creatinine clearance for patients at initiation of tenofovir and every 6 months “if feasible”, although inability to test does not preclude tenofovir use.12
Renal function impairment that might progress to end-stage renal disease requiring dialysis and renal transplant can be diagnosed in its earlier stage through routine screening and careful attention to changes in renal functions.13 In developing countries like Ethiopia where renal transplant and dialysis are rarely accessible, early detection of renal disease has clinical and financial implications for people living with HIV/AIDS.14
Among others, HIV RNA levels >4000 copies/mL, low CD4 counts, personal history of kidney disease, female gender, longer period on ART, dehydration, opportunistic infections, aging, hypertension and diabetes are factors that increase the risk for renal function impairment in PLWHIV. Recognition of common risk factors for kidney disease in PLWHIV is important to guide efforts aimed at prevention and early diagnosis. Despite this, data regarding renal impairment in HIV disease among Ethiopians are rare.
Although guidelines and studies recommend the use of the chronic kidney disease epidemiological collaboration (CKD EPI) equation to calculate eGFR in HIV-infected patients compared with other equations,15,16 no study has considered the use of CKD EPI in Ethiopia. Therefore, the aim of this study is to assess the prevalence of renal function impairment and associated factors among adult HIV-positive patients attending ART clinic in Mettu Karl referral hospital.
Methods
Study Design and Setting
A hospital-based, cross-sectional study was conducted from March 8–May 30, 2020 at Mettu Karl Referral Hospital, south-west Ethiopia. The hospital is located in Mettu, which is 600 km away from Addis Ababa, the capital city of Ethiopia. It delivers diversified health services and clinics such as antenatal care (ANC) clinics, tuberculosis (TB) clinics, anti-retroviral therapy (ART) clinics, and ophthalmology clinics. The hospital has 1378 dult patients living with HIV/AIDS registered for follow-up care.
Study Population
All adult patients living with HIV/AIDS who were attending follow up in Mettu Karl referral hospital from March 8–May 30, 2020 were included in the study. However, those who were critically ill and unable to participate in the interview, pregnant women, patients with known renal disease before start of ART and also those who had an ART period of fewer than 6 months were excluded.
Sample Size Determination and Procedure
The sample size was determined by using a single population proportion formula. Expecting an overall renal function impairment rate of 25.4%17 at a 95% confidence interval (CI), and after adding 5% of the calculated sample size for possible non-response, 352 patients were interviewed. The representative sample was selected using a systematic random sampling technique. The individual patients were approached through calculating sampling interval Kth, [N/n]. Accordingly, of the total number of adults living with HIV/AIDS (N= 1378), n = 359 patients was the calculated final sample size, yielding a sampling interval of three. The first patient to be interviewed was selected using the lottery method from the first three individuals. Finally, study participants were picked by selecting every third patient that came to the ART clinic during the study period to make the exit interview.
Data Collection Method and Survey Instrument
Data were collected using a pre-tested structured questionnaire in order to capture information on socio-demographic characteristics, behavioral factors and bio-clinical (HIV-related) factors. A checklist was used to collect data from medical records for the outcome variables; creatinine was calculated as an estimate of renal function (eGFR) using the CKD-EPI equation. Renal impairment was classified according to National Kidney Foundation clinical practice guidelines based on the GFR as determined by the CKD-EPI equation, as recommended.15,16 Accordingly, estimated GFR values ≥ 90 mL/min/1.73 m2 normal, 60–89 mL/min/1.73m2 mild, 30–59 mL/min/1.73 m2 moderate, 15–29 mL/min/1.73 m2 severe and < 15 mL/min/1.73 m2 kidney failure. Renal function impairment was defined as eGFR < 60 mL/min/1.73 m2.18
Anthropometric Measurement
Anthropometric measurements consist of each client’s weight and height. Participants’ weight was measured by portable Seca digital floor scale. The scale was calibrated regularly to ensure accurate measurements. Participants were informed to wear minimum clothing and to stand upright and unsupported in the middle of the scale’s platform. Reading of weight was taken to the nearest 0.1 kg. Participants’ height was measured using a Seca measuring rod. Participants were informed to be barefoot, legs straight, shoulders relaxed and to look straight ahead at the horizontal plane. With each participant looking straight ahead, the headpiece was lowered to touch the crown of their head gently but firmly. Reading of height measurement was taken to the nearest 0.1 cm. Then, BMI of the participants was calculated as weight in kg divided by height in meters squared and subjects were considered as either underweight (BMI < 18.5 kg/m2), normal (BMI = 18.5–24.9 kg/m2) or overweight (BMI ≥ 25 kg/m2).9
Blood Sample Collection and Handling
Blood specimens were collected from each study participant for laboratory investigations. Five mL of venous blood was drawn from each participant into a syringe for renal function test. The blood sample was dispensed into a gel-coated serum separator test tube and centrifuged at 3500 rpm for 10 minutes for the separation of the serum. Serum was frozen at −18°C when analyses are not carried out immediately. Serum creatinine was estimated using a Roche/Hitachi 902 Analyzer, Germany. For better quality of laboratory results, blood specimens were collected, processed and analyzed following standard operating procedures (SOP).Quality control samples were used for all laboratory tests. The results of all laboratory tests were recorded in a standardized report format carefully and attached to the questionnaire according to the subject’s unique identification number.
Data Collection Personnel and Technique
Data were collected by two trained Bachelor degree holder nurses, a Bachelor degree holder laboratory technologist drew the blood samples and one medical doctor supervisor regulated and managed the data collection procedure. Data were collected using a face-to-face structured questionnaire. Medical records of adults living with HIV/AIDS were reviewed to extract data on baseline CD4, WHO stage, drug regimen, opportunistic infection, comorbidity, and regular follow-up.
Data Quality Control
Data quality was ensured by giving training for data collectors and strict supervision during data collection. A pre-test was conducted on 5% of the sample size in the Bedele general hospital before the actual data collection.
Data Processing and Analysis
The responses from each study participant were analyzed using Statistical Package for the Social Sciences (SPSS) software version 22.0 for Windows (SPSS Inc., Chicago, IL) and were double-checked for accuracy. Descriptive aspects of analyses were done through calculating mean, standard deviation, frequencies, and percentages. Multivariable analysis was carried out to identify independent predictors of renal function impairment and to control confounders. The 95% CI and P-value < 0.05 were used to assess the significance of the association.
Operational Definitions
Renal impairment: defined as eGFR < 60 mL/min/1.73 m2 calculated by the Cockcroft-Gault formula.
Current smoking: at least one cigarette per day in the past 30 days.
Opportunistic infection: an infection caused by pathogens that take advantage of an opportunity not normally available.
Comorbidity: patients who had other chronic non-communicable disease/s that was previously diagnosed (e.g. hypertension, diabetes mellitus).
Ethics Approval
Ethical clearance and approval letter was obtained from the institutional review board of Jimma University, Institute of Health. An official letter of support was secured from Mettu Karl referral Hospital. Informed written consent was obtained from each participant after describing the benefits and risks of the study. Any information concerning the participants was kept confidential and the specimens collected from the participants were analyzed only for the intended purposes. Results where eGFR < 60 mL/min/1.73 m2 were communicated to the internal medicine unit in the hospital for appropriate management. This study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics
A total of 352 HIV infected patients participated in this study with response rate of 98.1%. Out of total participants, 198 (56.2%) were females. The mean (±SD) age of the study participants was 43.42 (± 13.95) years. The majority, 172 (48.9%), of the participants were Muslim, followed by Orthodox 112 (31.8%), and 207 (58.8%) of them were married. Out of the total, 161 (45.7%) had completed Diploma and above, 185 (52.6%) were government employees, 274 (77.8%) were urban residents and 177 (50.3%) had family monthly income of greater than 3500 birr (ETB) (Table 1).
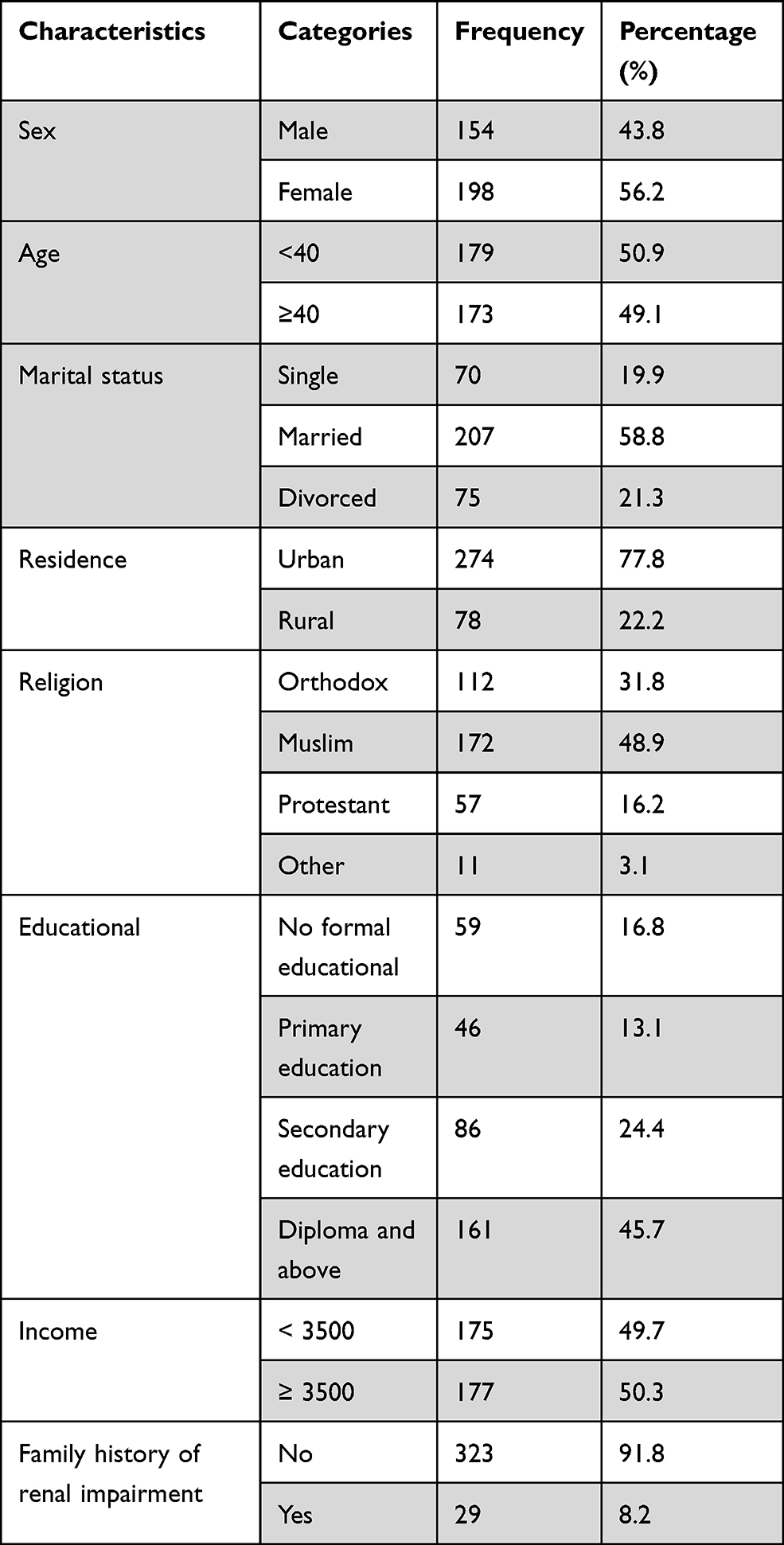 |
Table 1 Socio-Demographic Characteristics of HIV Patients on Treatment Attending ART Clinics in Mettu Karl Referral Hospital, Mettu Town, South-west Ethiopia, 2020 |
Behavioral Factors of Participants
Among the 352 participants 60 (17%) have history of smoking cigarettes. Sixty (17%) are current smokers, among these 55 (91.7%) smoke every day and the rest 5 (8.3%) smoke on some days.
Bio-Clinical Factors of the Study Participants
About 69 (19.6%) participants had opportunistic infections and the rest 283 (80.4%) had no opportunistic infections. Ninety-six (27.3%) participants had co-morbidity. Fifty (14.2%) of the participants were confirmed diabetics and were on medication and 42 (11.9%) of respondents were confirmed hypertensive and on medication. Twenty-nine (8.2%) of participants had a family history of renal disease. About 333 (89.4%) of the participants on ART were receiving first-line regimens and 252 (71.6%) a combination of tenofovir (TDF). Most (237; 67.3%) of the study participants were in advanced WHO clinical stage (Stages III & IV). The majority (225; 63.9%) of the participants had a normal body mass index (BMI). The mean CD4 count was 251 ±107.9 cells/mm3 and 134 (38.1%) of the participants on ART had CD4 count < 200 cells/mm3. The mean (±SD) creatinine level was 0.99 (± 0.74) mg/dl. The mean (±SD) serum creatinine was 104.2 (±40.04) mL/min/1.73 m2 (Table 2). Serum creatinine estimated by CKD-EPI indicated that 73 (20.7%) of the study participants had estimated GFR below 60 mL/min/1.73 m2. Therefore the prevalence of renal function impairment was 20.7%.
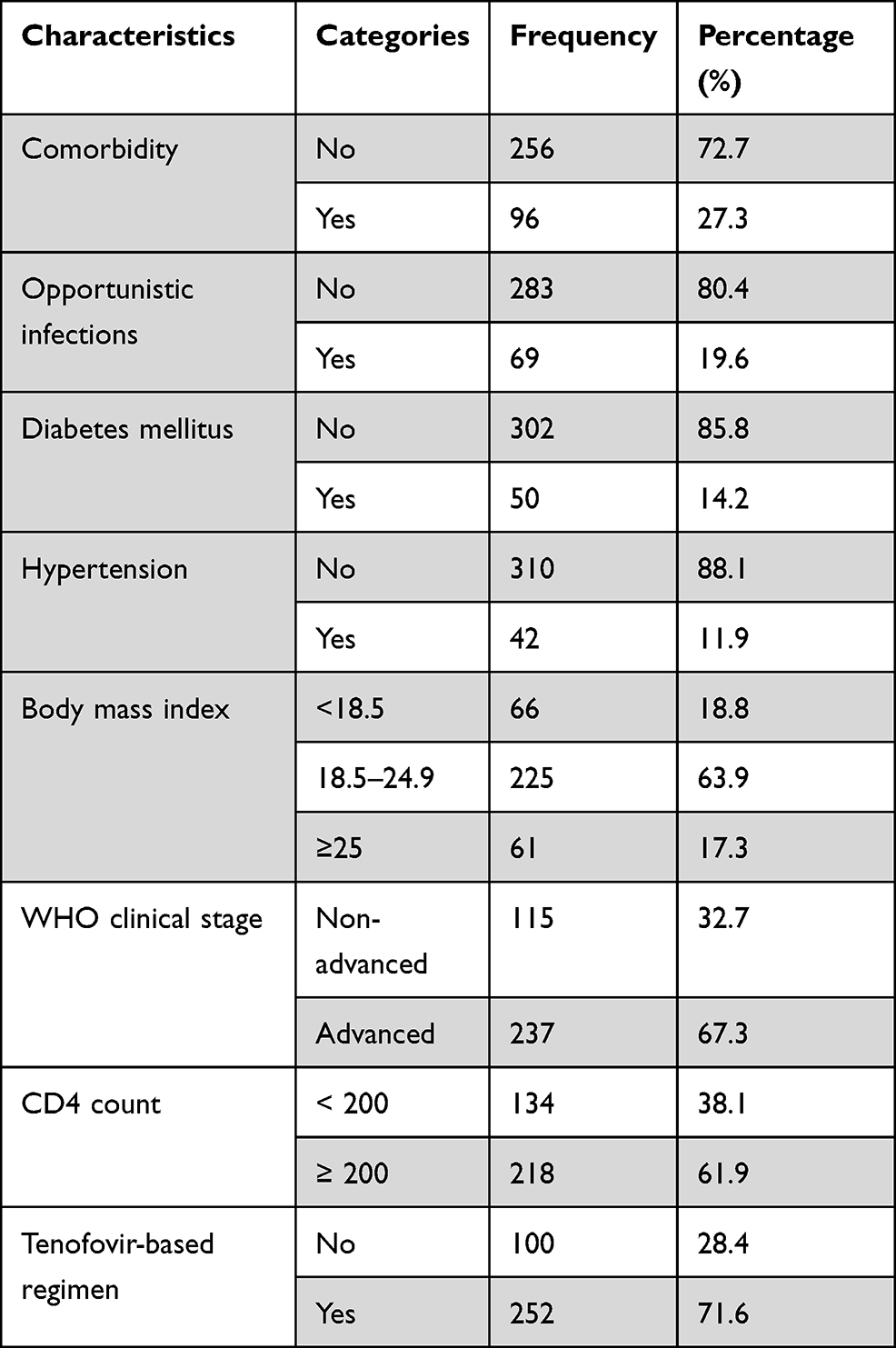 |
Table 2 Bio-Clinical Factors of HIV Patients on Treatment Attending ART Clinics in Mettu Karl Referral Hospital, Mettu Town, South-west Ethiopia, 2020 |
Factors Associated with Renal Function Impairment Among Adult HIV Positive Individuals
Bivariate and Multivariable Analysis
Bivariate analysis was done to see associations between each independent variable and renal function impairment. According to bivariate analysis, sex, cigarette smoking, presence of comorbidity, having diabetes mellitus, hypertension, tenofovir based regimen, abnormal body mass index, advanced WHO clinical stage and low CD4 count showed association with renal function impairment at P < 0.25 (Table 2). After controlling for possible confounders, cigarette smoking, diabetes mellitus, hypertension and low CD4 count were statistically significantly associated with renal function impairment at P < 0.05.
Accordingly, renal function impairment was statistically significantly associated with cigarette smoking (AOR = 9.60, 95% CI: 4.73–19.48), having diabetes mellitus (AOR = 6.16, 95% CI: 2.79–13.59), having hypertension (AOR = 4.71, 95% CI: 1.98–11.17) and having low CD4 count (AOR = 6.47, 95% CI: 3.31–12.64) (Table 3).
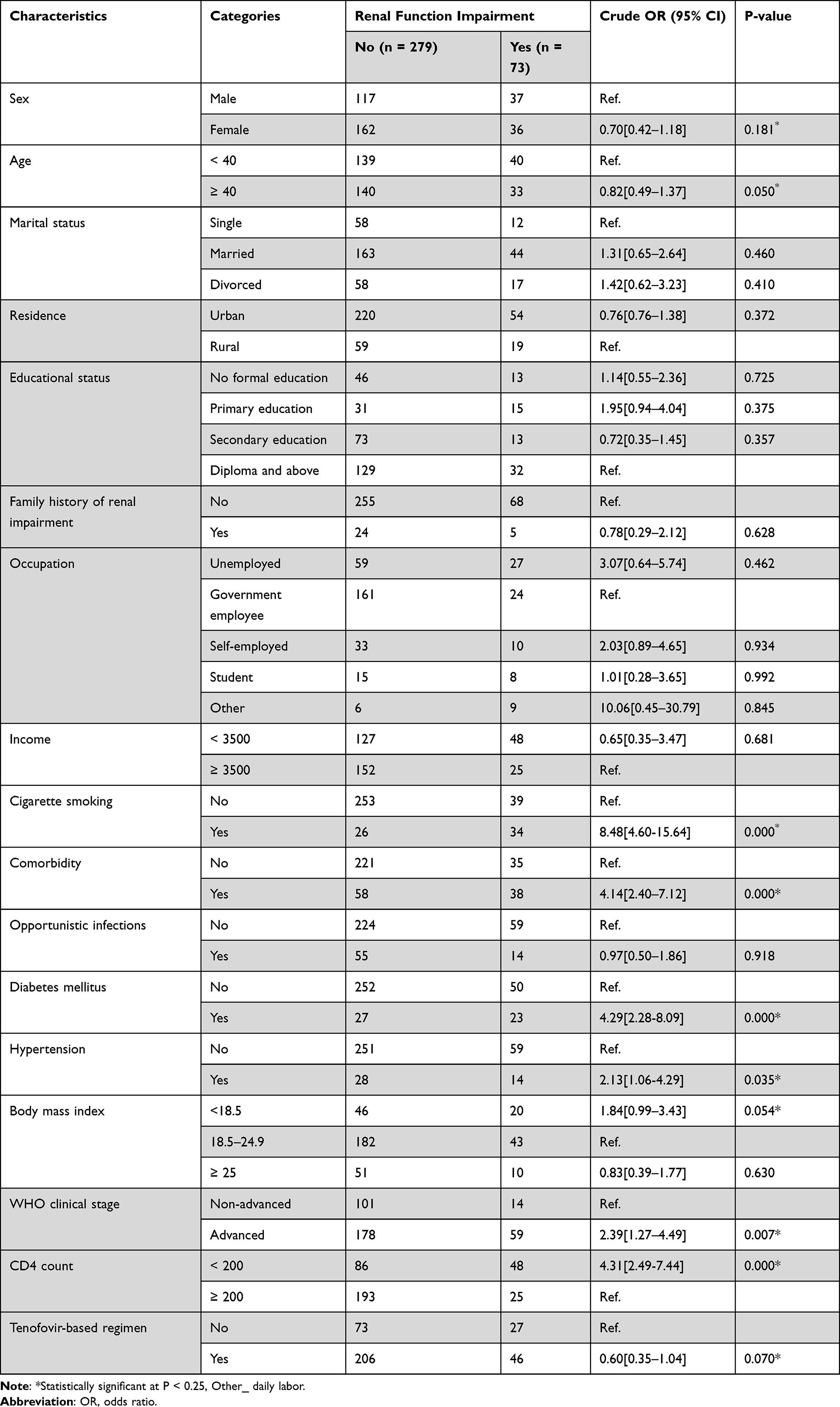 |
Table 3 Bivariable Analysis of Factors Associated with Renal Function Impairment Among HIV Patients Attending ART Clinics in Mettu Karl Referral Hospital, Mettu Town, South-west Ethiopia, 2020 |
Discussion
Renal impairment is a common result of HIV infection and it can be due to antiretroviral drugs or drugs used to treat certain opportunistic infections. Renal impairment, based on single creatinine clearance measurement, was very common among HIV-infected adults with clinically non-advanced HIV disease in most parts of Africa.19
The prevalence of renal function impairment in this study based on glomerular filtration rate using the CKD EPI equation was 20.7%. This finding is consistent with similar studies done in south-west Nigeria (23.7%), in south Nigeria (24.3%), and in Gondar (16.3%).20–22 It is higher than in studies which reported 14.5% in Ghana, 12.9% in Felege Hiwot referral hospital, north-west Ethiopia and 7.6% in Jimma University Specialized hospital, south-west Ethiopia.9,10,23 This variation may be due to differences in participants among studies; the study in Ghana did not include hypertensive and diabetic individuals and cigarette smokers were not included in the studies from north-west and south-west Ethiopia. In addition, the method used to estimate GFR was also different; modified diet of renal disease formula was used to estimate GFR in Ghana, Cockcroft-Gault method in north-west- and south-west Ethiopia, which might also contribute to the variation in the prevalence.
However, the prevalence of renal function impairment in this study is lower than studies from Cote d’Ivoire (26%), Burundi (45.7%), Tanzania (25%) and Addis Ababa (25.4%).24,26,36,37 This difference could be in part due to differences in ART regimen, study design, populations studied, stage of HIV infection and the sample size.
This study found that having hypertension heightened the risk of renal function impairment. This finding is concordant with studies conducted in Brazil,11 Washington,24 London,25 and Turkey.26 This might be due to the incidence of serum creatinine increases among hypertensive patients compared with patients with normal blood pressure.27 In addition, it may be because kidney is one of the principal target organs of hypertension and most disease of kidney is associated with blood pressure elevation.
The current study also found that having diabetes increased the risk of renal function impairment. This finding is in agreement with previous similar studies done in middle income countries,28 San Diego29 and southern Ethiopia.30 This could be because diabetic nephropathy, a common complication of diabetes, decreases the glomerular filtration rate.
This study shows that those patients with low CD4 count were found to be more likely to develop renal function impairment. This is consistent with previous studies done in north-west Ethiopia9 and south-west Ethiopia.10 Immunological AIDS (CD4 count <200 cell/μL) is known to be associated with development of opportunistic infections, malignancies and other organ diseases that affect kidney functions.
In this study, cigarette smoking was positively associated with renal function impairment. This finding is in agreement with previous studies done in Japan31 and France.32 The possible explanation as to how smoking leads to renal function impairment could be that vasodilator compounds such as nitric oxide and atrial natriuretic peptide repeatedly released after each cigarette smoked eventually cause chronic glomerular hyperfiltration.33 GFR is therefore decreased during smoking, and this was accompanied by a significant decrease of filtration fraction and an increase in renovascular resistance.34
Various studies found that old age is an independent predictor for renal function impairment.16, 66, 73–75 The current study however could not show a consistent result. This variation may be due to the population variation and different age classification methods used.
This study found that gender was not statistically significantly associated with renal impairment. This finding is not in line with the studies conducted in Gondar35 and Jimma10 that revealed being female is the main predictor of renal function impairment. The discrepancy could be explained by sociocultural differences, difference in sample size, and population variation.
Limitations and Strength of the Study
The present study assessed the magnitude of renal function impairment and its associated factors among adult HIV-positive patients attending an ART clinic in Mettu, where studies are limited. Therefore, the results of this study could be used as baseline data for further studies. Th study has some limitations. First of all, creatinine was measured at a single point in time; therefore, it may have included short-term, reversible causes of renal impairment which may overestimate renal impairment. Secondly, there was no assessment for proteinuria. Thirdly, this study was limited by its cross-sectional design, not longitudinal, and the underlying causes of renal impairment were unknown.
Conclusion and Recommendations
The prevalence of renal function impairment was high among adult HIV-positive patients attending an antiretroviral therapy clinic in Mettu Karl referral hospital. Hypertension, diabetes mellitus, low CD4 count and cigarette smoking was associated with renal function impairments in the study participants. What is clear from this study is that renal function impairment is common in HIV patients. Hence, HIV patients on ART should be regularly screened for early diagnosis and management of renal function impairment. Those patients with low CD4 count and cigarette smokers should be closely followed.
Abbreviations
AIDS, acquired immune deficiency syndrome; AKI, acute kidney injury; ART, antiretroviral therapy; ATV, antiretroviral; BMI, body mass index; CD4, cluster of differentiation 4; CG, Cockcroft-gGault; CKC, chronic kidney disease; CKDEPI, chronic kidney disease epidemiology collaboration; CrCl, creatinine clearance; eGFR, estimated glomerular filtration rate; ESRD, end stage renal disease; GFR, glomerular filtration rate; HIV, human immunodeficiency virus; HIVAN, human immune deficiency virus associated nephropathy; MDRD, Modification of Diet Renal Disease; TDF, tenofovir disoproxil fumarate; WHO, World Health Organization.
Data Sharing Statement
Data will be available from the corresponding author upon request.
Ethical Approval and Consent to Participate
Ethical clearance and approval letter were obtained from institutional review board of Jimma University, Institute of Health. An official letter of support was secured from Mettu Karl referral Hospital. Informed written consent was obtained from each participant after describing the benefits and risks of the study. Anonymity was kept; during specimen collection and interview. Any information concerning the participants was kept confidential and the specimens collected from the participants were analyzed only for the intended purposes. Results where eGFR < 60mL/min/ 1.73 m2 were communicated to internal medicine unit in the hospital for appropriate management.
Acknowledgment
Our heartfelt gratitude goes to the Jimma University, College of Health and Medical Sciences for support by all necessary services. Additionally, we appreciate the support from Hospitals administrations and data collector.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The Jimma University has covered the costs of data collectors and supervisors per diem. However, the University had no role in study design, data collections, and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Torre D, Speranza F, Martegani R. Impact of highly active antiretroviral therapy on organ-specific manifestations of HIV-1 infection. HIV Med. 2005;6(2):66–78. doi:10.1111/j.1468-1293.2005.00268.x
2. Mocroft A, Lundgren JD, Ross M, et al. Cumulative and current exposure to potentially nephrotoxic antiretrovirals and development of chronic kidney disease in HIV-positive individuals with a normal baseline estimated glomerular fi ltration rate: a prospective international cohort study. Lancet HIV. 2016;3(1):e23–32. doi:10.1016/S2352-3018(15)00211-8
3. Wyatt. Kidney disease and HIV infection. Kidney Dis HIV. 2017;25(1):13–16.
4. Fine DM. Renal disease and toxicities: issues for HIV care providers. Top HIV Med. 2006;14(5):164–169.
5. Ekrikpo UE, Kengne AP, Bello AK, et al. Chronic kidney disease in the global adult HIV- infected population: a systematic review and meta-analysis. 2018;1–24.
6. Msango L, Downs JA, Kalluvya SE, et al. Renal dysfunction among HIV-infected patients starting antiretroviral therapy. AIDS. 2011;25(11):1421–1425. doi:10.1097/QAD.0b013e328348a4b1
7. Sarfo FS, Keegan R, Appiah L, et al. High prevalence of renal dysfunction and association with risk of death amongst HIV-infected Ghanaians. J Infect. 2013;67(1):43–50. doi:10.1016/j.jinf.2013.03.008
8. Mpondo BCT, Kalluvya SE, Peck RN, et al. Impact of antiretroviral therapy on renal function among HIV-infected tanzanian adults: a retrospective cohort study. 2014;9(2):1–5.
9. Kahsu G, Birhan W, Addis Z, Dagnew M, Abera B. Renal function impairment and associated risk factors among human immunodeficiency virus positive individuals at flege Hiwot Referral Hospital, Northwest Ethiopia. J Interdiscip Histopathol. 2013;1(5):252. doi:10.5455/jihp.20130508063833
10. Mekuria Y, Yilma D, Mekonnen Z, Kassa T.Renal function impairment and associated factors among HAART Na ï ve and experienced adult HIV positive individuals in Southwest Ethiopia: a comparative cross sectional study. 2016;1–11. doi:10.1371/journal.pone.0161180
11. Menezes M, Jr JT, Poeta J, Sprinz E. Prevalence and risk factors associated to chronic kidney disease in HIV-infected patients on HAART and undetectable viral load in Brazil. PloS one. 2011;6(10):6–10.
12. Szczech LA. Renal disease: the effects of HIV and antiretroviral therapy and the implications for early antiretroviral therapy initiation. Curr Opin HIV AIDS. 2009;4(3):167–170. doi:10.1097/COH.0b013e328329c646
13. Msangoa L, Downsa JA, Kalluvyaa SE, et al. Renal Dysfunction among HIV-infected patients starting antiretroviral therapy in Mwanza, Tanzania. AIDS. 2011(11):1421–1425.
14. Ababa A, Eneyew K, Seifu D, Amogne W, Menon MKC. Assessment of renal function among HIV-infected patients on combination antiretroviral therapy at Tikur Anbessa Specialized Hospital. Technol Invest. 2016;(August):107–122.
15. Ibrahim F, Hamzah L, Jones R, et al. Comparison of CKD-EPI and MDRD to estimate baseline renal function in HIV-positive patients. Nephrol Dialysis Transplant. 2012;27(November 2011):2291–2297. doi:10.1093/ndt/gfr657
16. Shamu T, Wellington M, Pascoe M, Gwanzura L, Ndhlovu CE. Incidence of nephropathy in hiv infected patients receiving highly active antiretroviral therapy at Newlands Clinic: a Retrospective Study. World J AIDS. 2015;(June):113–123.
17. Yazie TS, Orjino TA, Degu WA. Reduced kidney function in tenofovir disoproxil fumarate based regimen and associated factors: a hospital based prospective observational study in ethiopian patients. Int J Nephrol. 2019;2019. doi:10.1155/2019/9172607
18. Milik A, Hrynkiewicz E. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. IFAC Proc. 2014;19(1):4477–4483. doi:10.3182/20140824-6-ZA-1003.01333
19. Mocroft A, Kirk O, Gatell J, et al. Chronic renal failure among HIV-1-infected patients. Aids. 2007;21(9):1119–1127. doi:10.1097/QAD.0b013e3280f774ee
20. Umeizudike T, Mabayoje M, Okany C, et al. Prevalence of chronic kidney disease in HIV positive patients in Lagos, south-west Nigeria. 2012;4.
21. Onodugo OD, Chukwuka C, Onyedum C, et al. Baseline renal function among antiretroviral therapy-naive. HIV-Infected Patients in Southeast Nigeria. 2014;13(5):476–480.
22. Manaye GA. Chronic Kidney Disease and associated factors among HIV/AIDS Patients on HAART at University of Gondar Referral Hospital, Northwest Ethiopia. 1–21.
23. Wkba O. Renal insufficiency in Ghanaian HIV infected patients: need for dose adjustment. J Commun Dis. 1997;29(2):101–111.
24. Haroun MK, Jaar BG, Hoffman SC, Comstock GW, Klag MJ, Coresh J. Risk factors for chronic kidney disease: a prospective study of 23, 534 men and women in Washington County, Maryland. 2010;2934–2941.
25. Herrington WG, Smith M, Bankhead C, et al. Body-mass index and risk of advanced chronic kidney disease: prospective analyses from a primary care cohort of 1. 4 million adults in England. 2017;1–15.
26. Sengul S, Erdem Y, Batuman V, Erturk S. Hypertension and chronic kidney disease in Turkey. Kidney International Supplements. 2013;3(4):308–311. doi:10.1038/kisup.2013.64
27. Shulman NB, Ford CE, Hall WD, Blaufox MD, Simon D. Prognostic value of serum creatinine and effect of treatment of hypertension on renal function. Hypertension. 2015;5.
28. Grinsztejn B, Friedman RK, Cunha CB, Coelho LE, Cardoso SW, Veloso VG. Screening for decreased glomerular filtration rate and associated risk factors in a cohort of HIV-Infected Patients in a Middle-Income Country. PLoS One. 2014;9:4.
29. Crum-Cianflone N, Ganesan A, Teneza-Mora N, Riddle M, et al. Prevalence and factors associated with renal dysfunction among hiv-infected patients. AIDS Patient Care STDS2010;24(6): 353-360. doi:10.1089/apc.2009.0326.
30. Fiseha T, Kassim M, Yemane T. Prevalence of chronic kidney disease and associated risk factors among prevalence of chronic kidney disease and associated risk factors among diabetic patients in southern Ethiopia. BMC Nephrol. 2014;15(August). doi:10.1186/1471-2369-15-198
31. Unit D, General O, Maintenance H. Influence of smoking and obesity on the development of proteinuria. Kidney Int. 2002;62(3):956–962. doi:10.1046/j.1523-1755.2002.00506.x
32. Ebranchu Y, Ichet J, Vol S. Effects of current smoking and smoking discontinuation on renal function and proteinuria in the general population. Kidney Int. 2000;58(3):1285–1292. doi:10.1046/j.1523-1755.2000.00284.x
33. Halimi J, Philippon C, Mimran A. Nephrology Dialysis Transplantation Contrasting Renal e Ff Ects of Nicotine in Smokers and Non-Smokers. 1998:940–944.
34. Nephrol JAS. Effects of smoking on renal hemodynamics in healthy volunteers and in patients. J Am Soc Nephrol. 1998;1798–1804.
35. Birhane H, Biadgo WKB. Assessment of the effect of antiretroviral therapy on renal and liver functions among HIV-infected patients: a retrospective study. 2017;1–7.
36. Mpondo BCT, Kalluvya SE, Peck RN, Kabangila R, Kidenya BR, Ephraim L, et al. Impact of Antiretroviral Therapy on Renal Function among HIV-Infected Tanzanian Adults: A Retrospective Cohort Study 2014;9(2):1–5.
37. Taklo Simeneh Yazie, Teferra Abula Orjino and WA, Degu. Reduced Kidney Function in Tenofovir Disoproxil Fumarate Based Regimen and Associated Factors: A Hospital Based Prospective Observational Study in Ethiopian Patients. 2019.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.