")
Back to Journals » Patient Preference and Adherence » Volume 14
Reliability and Validity of the LifeWindows Information–Motivation–Behavioral Skills Antiretroviral Therapy Adherence Questionnaire Among HIV+ Patients in Shanghai
Authors Peng Z, Yu Y , Wei W, Hou Y, Sun Z, Wang Y, Zhang L, Zhou Y , Wang Q , Cai Y
Received 9 October 2019
Accepted for publication 1 February 2020
Published 5 March 2020 Volume 2020:14 Pages 507—515
DOI https://doi.org/10.2147/PPA.S234041
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Zihe Peng, 1,* Yuelin Yu, 1,* Wei Wei, 2 Yongchun Hou, 2 Zhenyu Sun, 3 Ying Wang, 4 Lin Zhang, 5 Ying Zhou, 5 Qian Wang, 1 Yong Cai 1
1School of Public Health, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Putuo District Center for Disease Control and Prevention, Shanghai, People’s Republic of China; 3Taopu Town Community Health Service Center, Shanghai, People’s Republic of China; 4Yichuan Street Community Health Service Center, Shanghai, People’s Republic of China; 5Shanghai Public Health Clinical Center, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong Cai; Qian Wang
School of Public Health, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
Tel +86 13611677244;
+86 133219663565
Email [email protected]; [email protected]
Objective: The purpose of this article was to examine the validity and reliability of the LifeWindows Information–Motivation–Behavioral Skills Antiretroviral Therapy (ART) Adherence Questionnaire (LW-IMB-AAQ) among HIV+ patients in Shanghai.
Methods: We surveyed 426 HIV+ patients in Shanghai’s Putuo District to examine the validity and reliability of the questionnaire. The questionnaire includes self-reported demographic characteristics, the modified version of the Community Programs for Clinical Research on AIDS Antiretroviral Medication Self-Report (CPCRA) and LW-IMB-AAQ. CPCRA was used to calculate ART adherence. LW-IMB-AAQ, including the information section, the motivation section and the behavioral skills section, was used to analyze patients’ ART adherence. We analyzed data by means, standard deviation, critical ratio, and item-total correlation. Reliability was assessed by internal consistency, split-half reliability, and test–retest reliability. Validity was assessed by exploratory factor analysis (EFA), confirmatory factor analysis (CFA), convergent validity and discriminant validity.
Results: Item analysis showed that except for motivation item 1, all items were acceptable. For reliability, Cronbach’s alpha coefficients for the three sections and the total scale were all higher than 0.7, with interclass correlation coefficients (ICC) all higher than 0.6 (p< 0.001). The Spearman–Brown coefficient for the total scale was 0.825. For validity, results showed that the information section could be divided into two subscales, motivation section and behavioral skills section could be divided into three and two subscales, respectively. The final model demonstrated good validity (p=0.471, χ 2/df=0.960, CFI=1.000, GFI=0.994 and RMSEA< 0.001) without motivation item 4.
Conclusion: Excluding motivation items 1 and 4, the LifeWindows Information–Motivation–Behavioral Skills ART Adherence Questionnaire (LW-IMB-AAQ) demonstrated good validity and reliability among HIV+ patients in Shanghai.
Keywords: HIV, validity, reliability, IMB model, China
Introduction
HIV (Human Immunodeficiency Virus) has long been a public health problem in the world since the first AIDS cases were reported in 1981. Although the estimated national HIV prevalence rate in China was around 0.06% in 2014, lower than that (0.35%) in the United States, yet, the annual percentage growth of HIV infection in China increased dramatically with a 16.3% increase between 2004 and 2013.1,2 The UN puts forward a 90-90-90 UNAIDS goal, hoping by 2020, 90% of all people living with HIV be aware of their HIV status, 90% HIV+ patients receive sustained ART, and 90% of those already receiving ART manage to gain viral suppression.3 This suggests that optimal adherence to antiretroviral therapy (ART) plays a significant role in helping HIV+ patients achieve effective viral suppression, better immune functions, and lower HIV transmissions.4–8 Although the ART therapy has been widely available to HIV+ patients, especially in developed and fast-developing countries, yet, patient adherence to the treatment differed, which can lead to markedly different outcomes. Studies showed that HIV+ patients could achieve the durable status of having undetected virus load at a 90–95% adherence level.9–13 However, the average proportion of adherence is relatively low. One meta-analysis research found that the overall adherence was 70% (95% CI 63–76; I = 98%) among Latin American and Caribbean population. Another meta-analytic review of 84 studies across 20 countries showed that only 32.1% (27 in 84) studies observed an optimal adherence above 90%.9,14,15
Many studies have focused on the barriers and facilitators to adherence, as sociodemographic (eg income, treatment self-efficacy) factors, psychosocial (eg depression, use of drugs) factors, as well as ART’s side effects (eg nausea, vomiting) could prevent HIV+ patients from correctly taking ART.16,17 A few studies adopted a theory-based model, the Information–Motivation–Behavioral Skills (IMB) model, to study inconsistent adherence to ART.18–20 These studies utilized the LifeWindows Information–Motivation–Behavioral Skills ART Adherence Questionnaire (LW-IMB-AAQ), which is comprised of three interrelated sections: information section, motivation section, and behavioral skills section.21 According to the IMB model, acquiring comprehensive information about ART serves as the prerequisite to the motivation and behavioral change of ART adherence.22 Fisher classified items in the information section into two dimensions: specific information about adherence and heuristics concerning adherence. The motivation section consists of both independent and interdependent dimensions. The independent dimension, personal motivation, addresses motivation from personal perspectives while the interdependent dimension, social motivation, addresses motivation from social perspectives. When HIV+ patients hold positive views of the advantage of adherence, and receive encouragement from important people within their social networks, they are more likely to foster stronger motivations to stay in optimal adherence to ART. Adherence-related behavioral skills refer to patients’ self-efficacy about adhering to ART and about their abilities of putting the skills and motivations into practice. Once HIV+ patients acquire relevant and comprehensive information about ART, have strong adherence-related motivations and behavioral skills, they should be more likely to adhere to ART treatment.
The LW-IMB-AAQ has been well implemented to strengthen adherence to ART in many Western countries.18–20,23 However, few studies have examined LW-IMB-AAQ in relation to ART adherence among HIV+ populations in Asia. And almost no data is available on the reliability and validity of this questionnaire among HIV+ populations in China. Rongkavilit et al applied the IMB model to assess ART adherence among Thai HIV+ youth, a representative Asian population, and found the model definitions for information and behavioral skills were suitable for that population, while model definition for motivation needed further support considering the different context of cultural background (for example, different religions such as Buddhism, Moslem, Taoism and so on).24 However, compared with its role in the Thai culture, religion has a lesser role to play in shaping the national culture in China. In this study, we applied the IMB model to a representative sample of HIV+ population in Shanghai, China, and examined the psychometric properties of the LW-IMB-AAQ. We sought to extend the applicability of the questionnaire to explain HIV+ patients’ ART adherence based on the IMB model to the Chinese population, and to lay the foundation for further research using the IMB model in this population.
Methods
Participants
Participants were recruited from 11 community health centers in Shanghai’s Putuo district. Eligibility requirements included being at least 18 years old, reporting an HIV seropositive status, using ART, residing in Shanghai, and willing to complete the questionnaire. All participants were required to provide informed consent. We took measures to ensure participants’ privacy during recruitment and enrollment, and all questionnaires will be destroyed after 2 years. Every participant is rewarded with 50 yuan (approximately $7) for completing the questionnaire. Meanwhile, 50 participants were recruited from Shanghai public health clinical center, Shanghai, China. Eligibility requirements and the protection of participants’ privacy were as same as above. These people were asked to finish firstly the print-out questionnaire and secondly, the electronic edition of the questionnaire and the interval was 3 months. The collecting data from these 50 participants were used for test–retest reliability.
Questionnaire
The questionnaire includes self-reported demographic characteristics, the modified version of the Community Programs for Clinical Research on AIDS Antiretroviral Medication Self-Report (CPCRA) and the LifeWindows Information–Motivation–Behavioral Skills ART Adherence Questionnaire (LW-IMB-AAQ). The CPCRA contains the name, daily frequency and dose of proscribed drugs, and the exact amount of drugs that they have missed in the past 7 days. ART adherence was calculated by the ratio of the drug doses that they actually took to their prescribed drug doses. The sample was divided into two groups based on ART adherence: a high adherence group (>95% adherence) and a low adherence group (<95% adherence).25 The LW-IMB-AAQ was translated into Chinese to assess ART-related information (9 items), motivation (10 items), and behavioral skills (13 items). Each of the nine items used to assess ART-related information had a score of 0 or 1, and the total score ranged between 0 and 9. Items in the motivation and behavioral skills constructs are scored from 1 to 5. The total score for the motivation construct ranges from 10 to 50, and ranged from13 to 65 for the behavioral construct.
Data Analysis
Item Analysis
The mean and standard deviation (SD) of every item in the questionnaire was described. Then, the critical ratio (CR) was calculated for every item by SPSS 22. The critical ratio (CR) should be higher than 3 and statistically significant.26 Meanwhile, the correlation coefficient between each item and the total scale scores was checked.
Reliability
Internal consistency, split-half reliability and test–retest reliability were assessed for the whole questionnaire. Cronbach’s α coefficient was used for internal consistency of the three sections and total questionnaire, along with Spearman–Brown coefficient for split-half reliability of the total scale, while the interclass correlation coefficient (ICC) was assessed for the test–retest reliability of the three sections and total questionnaire. A value of α above 0.7 is considered as acceptable.27 The bigger the Spearman–Brown coefficients, the more stable the scale is.28 ICC lower than 0.4 is considered low, with 0.4–0.6 considered normal, 0.6–0.8 considered moderate and higher than 0.8 considered high.29
Validity
Exploratory factor analysis (EFA) was firstly conducted with SPSS 22 to extract the factor structure of the three model sections: information, motivation and behavioral skills. In EFA, principal components analysis with varimax rotation was used. The Kaiser-Meyer-Olkin measure and Bartlett’s sphericity were conducted for the legitimacy of the analysis. Then, confirmatory factor analysis (CFA) was employed with SPSS AMOS 24 to test the fitness of the questionnaire. The fit indices were calculated byχ2, degree of freedom (df), p-value, χ2/df, comparative fit index (CFI), goodness of fit index (GFI) and root-mean-square error of approximation (RMSEA). The reference values for every fitness index were p>0.05, χ2/df<3, CFI>0.9, GFI>0.9 and RMSEA<0.08.30 Then, the convergent validity was tested by the value of the average variance extracted (AVE), which was considered acceptable if the value of AVE was higher than 0.5. Discriminant validity was decided by comparison of the subscale’s value of the square root of AVE with the correlation coefficients of the specific subscale with those of other subscales.31
Results
Adherence-Related Behavior and Demographic Characteristics
We recruited 426 participants from 11 community health centers in Shanghai’s Putuo district, of which, 95.3% reported a high level of adherence (>95% adherence). Of these 426 participants (Table 1), 60.8% were 18–40 years old, 94.4% were male, 51.6% were homosexual, 65.5% were single, 54.7% reported homosexual transmission, 75.6% were in the HIV infection stage, 67.0% achieved a college degree or above and 92.5% earned more than 3000 yuan every month. None of these demographic characteristics were relevant to ART adherence (p>0.05). As is shown in Table 2, the mean scores of the information section and the social behavioral skills section are significantly different between high and low adherence groups (p<0.05) while there is no difference in the motivation section between the two groups.
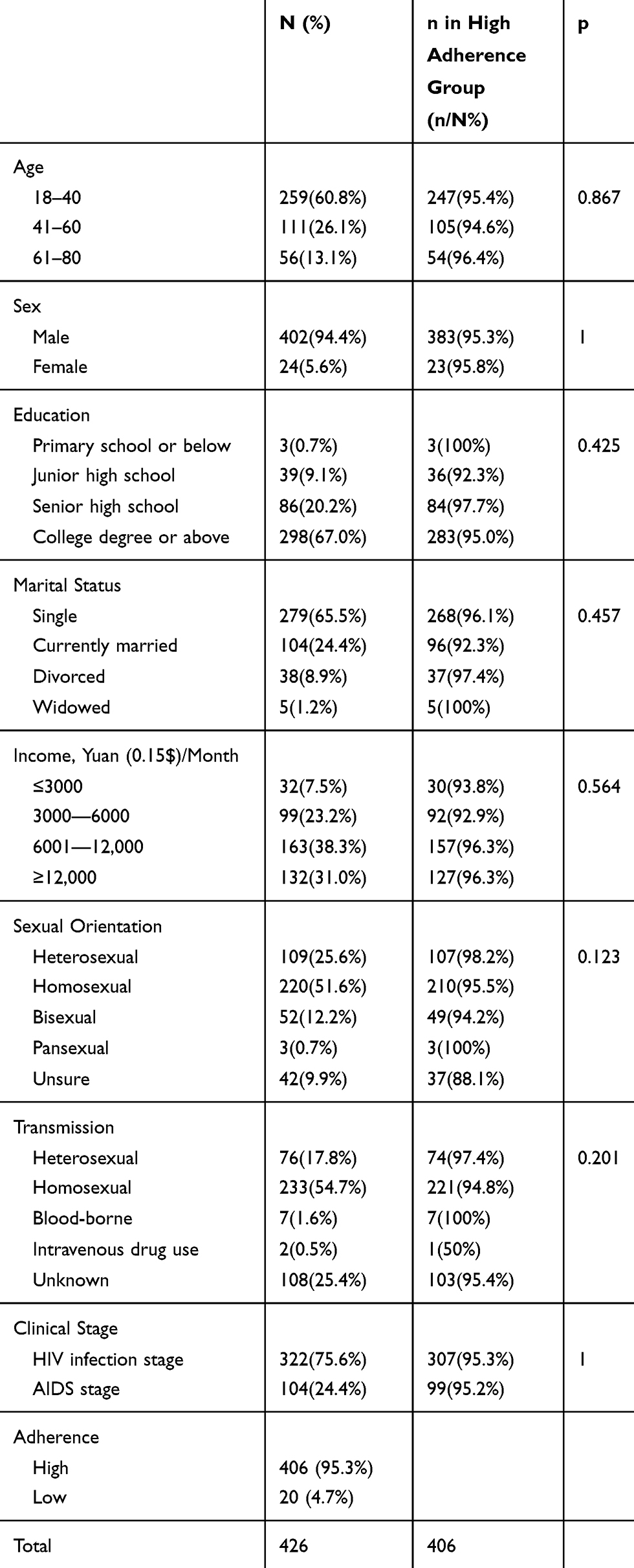 |
Table 1 Demographic Characteristics of the Participants (N=426) and Their Relationship with ART Adherence |
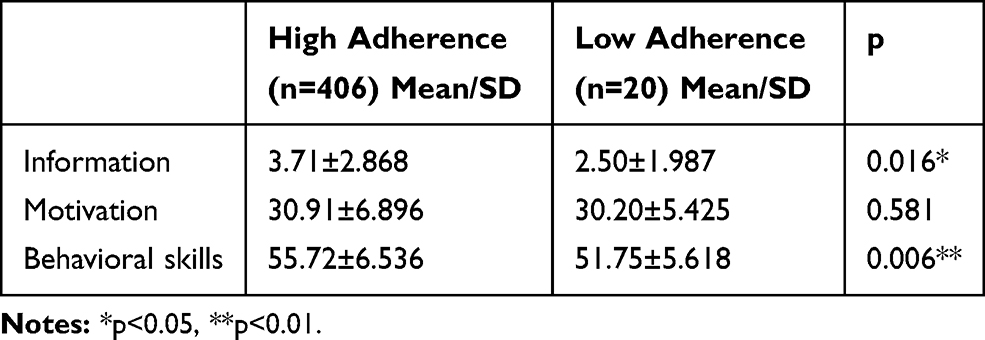 |
Table 2 The Mean Scores of Three Sections in Two Groups (N=426) |
Item Analysis
The results are shown in Table 3. Except motivation item 1, the CR coefficients of all items are higher than 3 (p< or = 0.001). Similarly, except motivation item 1, the scores of every item are significantly correlated with the total scores (p<0.001). Therefore, motivation item 1 is deleted for its low CR and item-total correlation.
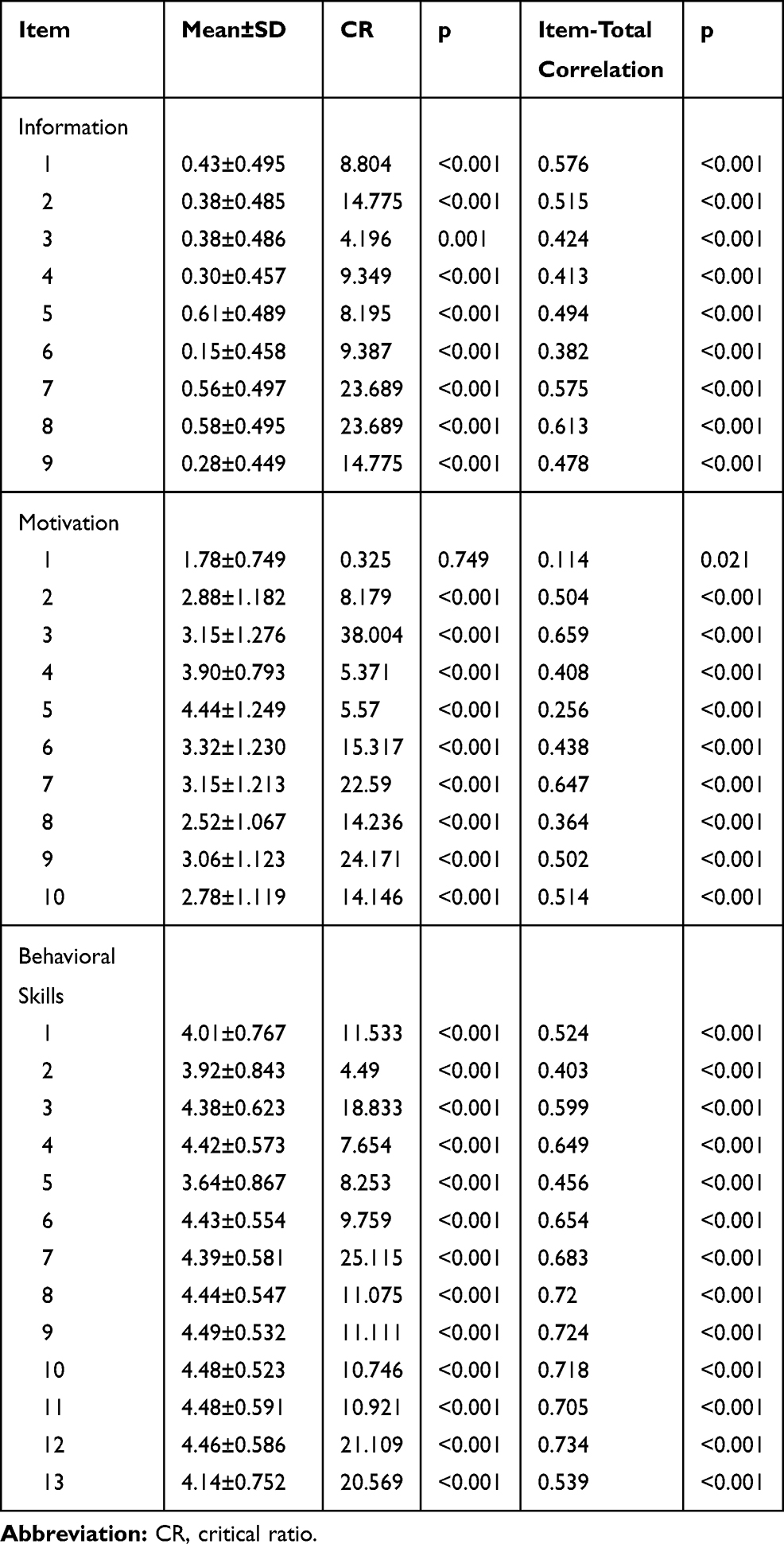 |
Table 3 Item Analysis for the LW-IMB-AAQ |
Reliability
The results are shown in Table 4. All Cronbach’s α coefficients for the three sections and total questionnaire are higher than 0.7, with ICC all higher than 0.6 (p<0.001). And the Spearman–Brown coefficient for the total scale is 0.825. The reliability of the questionnaire is considered acceptable.
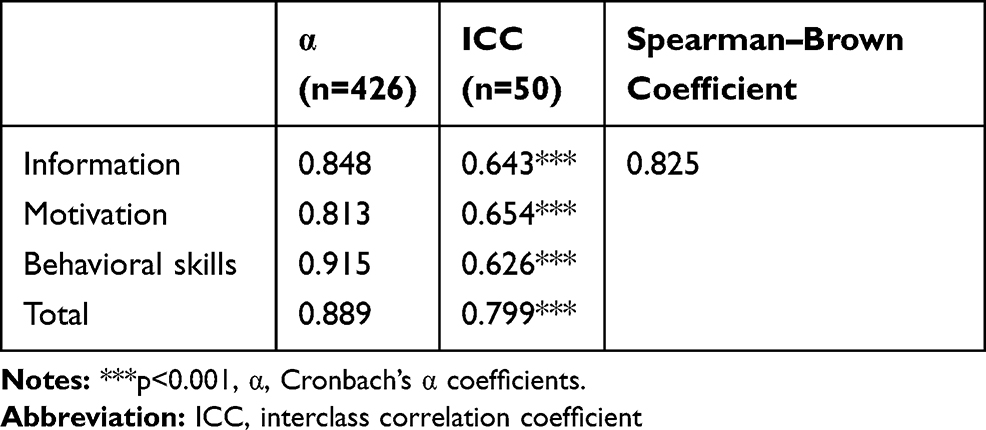 |
Table 4 The Reliability of the LW-IMB-AAQ |
Validity
EFA
Table 5 shows the result of the questionnaire. The KMO value of the Information section is 0.851 and Bartlett’s sphericity is χ2 = 1368.327 (p <0.001). And all items are reserved. The KMO value of the motivation section is 0.864 and Bartlett’s sphericity is χ2 = 1395.851 (p <0.001). And all items without motivation item 1 are reserved. The KMO value of the Behavioral Skills section is 0.944 and Bartlett’s sphericity is χ2 = 4539.052 (p <0.001). And all items are reserved.
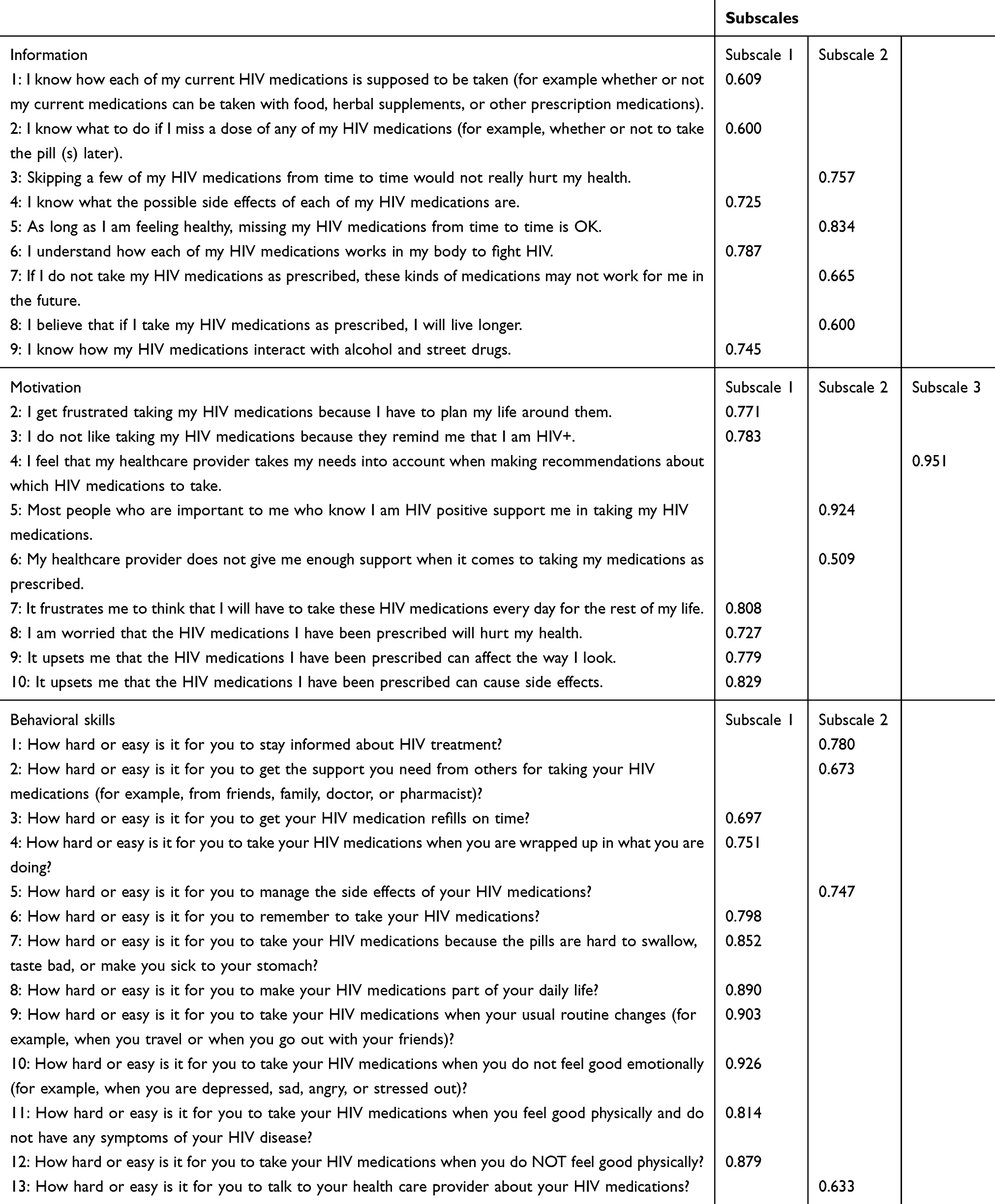 |
Table 5 Exploratory Factor Analysis of the Questionnaire |
CFA
The CFA is performed to test the fitness of the questionnaire without the motivation subscale3 for that this scale is not suitable in this model. The result is shown in Table 6. The construct of the questionnaire is acceptable for p=0.381 (>0.05), χ2/df=1.068 (<3), CFI=0.999 (>0.9), GFI=0.995 (>0.9) and RMSEA=0.013 (<0.08). The final model includes three sections: information (2 subscales), motivation (2 subscales), behavioral skills (2 subscales). By referring to the pioneer study by Fisher and looking for commonness among the items in the same subscale, names of these subscales are defined.21 The information section has two subscales: the effect of ART on health, knowledge about ART and how to take it. The motivation section is classified as personal motivation and social motivation. The behavioral skills section includes self-efficacy about insisting on taking ART and objective abilities of using skills to improve ART adherence.
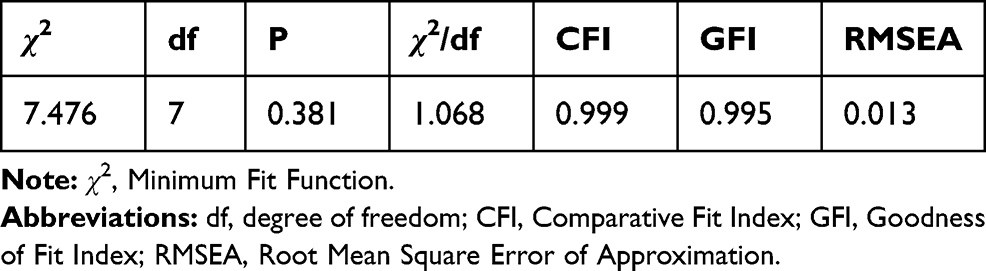 |
Table 6 Fitness of the LW-IMB-AAQ |
Convergent and Discriminant Validity
Table 7 shows the value of AVE of each subscale, the square root of every AVE value, and correlation coefficients between subscales. Except for the subscale about the effect of ART on health (approximately 0.5), the values of AVE of the other subscales are higher than 0.50, showing suitable convergent validity. The square roots of AVE are higher than any other correlation coefficients of every subscale with other subscales, which suggests acceptable discriminant validity.
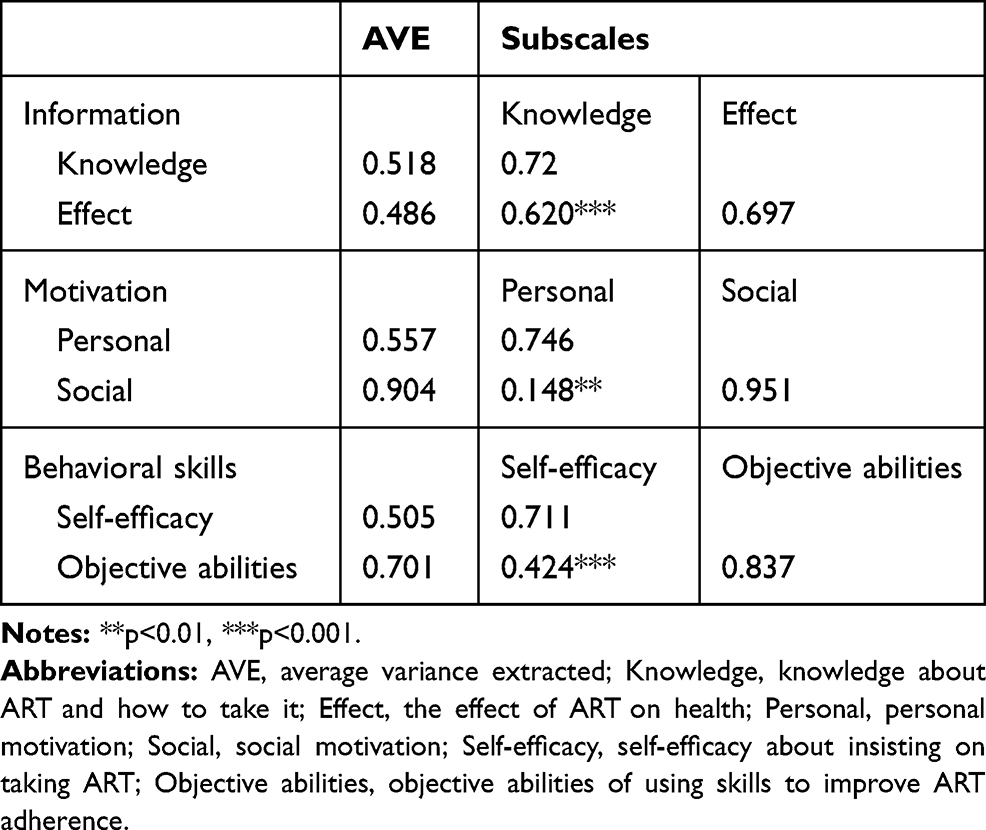 |
Table 7 Convergent Validity and Discriminant Validity of the Questionnaire |
Discussion
The final version of the LW-IMB-AAQ included 30 items measuring ART-related information, motivation and behavioral skills. Our results indicate that the questionnaire had good reliability and validity to asses ART adherence in Chinese HIV+ populations.
The information section demonstrated good reliability and validity. Furthermore, the results of EFA showed that the information section can be divided into two subscales, one measuring the effect of ART on health, and the other measuring knowledge about ART and how to take it. This finding is consistent with Fisher’s study, as is mentioned before, in which he divided the information section into specific information about adherence and heuristics concerning adherence.21 The first section, the specific information about adherence, is similar to the subscale measuring knowledge about ART and how to take it in our study, including the regimen, correct ART use, side effects and drug interactions. However, the second section, heuristics concerning adherence, is a little different from the subscale measuring the effect of ART on health in our study. Heuristics concerning adherence refer to patients’ negative beliefs toward ART adherence. On top of this, the subscale measuring the effect of ART on health in our study also contains one item representing patients’ positive beliefs. And being cognizant of the positive effects of ART on health often leads to positive emotions, which in turn is related to positive behavior toward normalizing life.32
Item analysis suggests that motivation item 1 (“I am worried that other people might realize that I am HIV+ if they see me taking my HIV medications”) was not suitable for this model. After deleting motivation item 1, other items are divided into three subscales. But in the final CFA model, subscale3 (motivation item 4: “I feel that my healthcare provider takes my needs into account when making recommendations about which HIV medications to take”) should be deleted for that it is not considered as part of the motivation in the Putuo population in Shanghai. Therefore, the motivation section in the final model only has two subscales: personal motivation and social motivation, which is as same as the classification in the pioneer study by Fisher.21 Personal motivation refers to HIV+ patients’ negative emotions toward taking ART. Negative emotions come from persistent health problems and contribute to loss of hope. Hope motivates adherence-related behaviors and help HIV+ patients deal and live with HIV/AIDS positively.32 Therefore, negative emotions lead to non-adherence through the loss of hope. Besides, social motivation refers to social support from others such as doctors and families. A number of researches have demonstrated that social support has a great impact on ART adherence.33–35
All items in the behavioral skills section have been reserved for the acceptable validity and reliability. These items are divided into 2 subscales, one representing self-efficacy about insisting on taking ART and the other one representing objective abilities of using skills to improve ART adherence, which is as same as the classification in the pioneer study by Fisher.21 Self-efficacy is one’s confidence in completing a task or carrying out a certain action.36 HIV treatment self-efficacy refers to one’s confidence in his or her ability of adhering to a therapeutic regimen in spite of difficulties.37 And numerous studies have proved that adherence self-efficacy is able to predict optimal ART adherence.34,37,38
Limitations
The final version of the LW-IMB-AAQ is suitable for this population excluding items motivation items 1 and 4. However, this study has two limitations. Firstly, this study is limited to only one district in Shanghai and the sample is not that big. Besides, the participants are all managed by their communities while we have no access to HIV+ patients who are out of management. Therefore, this study may not be completely representative of the whole HIV+ patients in Shanghai.
Conclusion
The validity and reliability of this LW-IMB-AAQ are acceptable. The final questionnaire includes 30 items: 9 items in the information section (5 in the subscale measuring the effect of ART on health and 4 in the subscale measuring knowledge about ART and how to take it), 8 items in the motivation section (6 in the personal motivation subscale and 2 in the social motivation subscale) and 13 items in the behavioral skills section (9 items in the subscale representing self-efficacy about insisting on taking ART and 4 items in the subscale representing objective abilities of using skills to improve ART adherence).
Ethics Approval and Informed Consent
Participants filled out questionnaires with their community doctors’ help when they came to doctors for an annual check. Community doctors were requested to sign a form pledging that they had made clear explanations to the participants and answered all questions from them. All participants needed to provide written informed consent. A 50-yuan (about $7) compensation was given to each subject investigated to improve the compliance. We made the claim that in the whole process of dealing with our participants, we strictly complied with the Declaration of Helsinki. This study was approved by the Ethics Committee of the School of Public Health Shanghai Jiao Tong University.
Disclosure
All of the authors have no conflict of interest, financial or otherwise.
References
1. Huang MB, Ye L, Liang BY, et al. Characterizing the HIV/AIDS epidemic in the United States and China. Int J Environ Res Public Health. 2015;13(1):30. doi:10.3390/ijerph13010030
2. Yang S, Wu J, Ding C, et al. Epidemiological features of and changes in incidence of infectious diseases in China in the first decade after the SARS outbreak: an observational trend study. Lancet Infect Dis. 2017;17(7):716–725. doi:10.1016/S1473-3099(17)30227-X
3. Unaids Joint United Nations Programme on Hiv/aids. 90-90-90 An Ambitious Treatment Target to Help End the AIDS Epidemic. Geneva Switzerland: UnaidsJoint United Nations Programme on Hiv/aids; 2014.
4. Lucas GM. Antiretroviral adherence, drug resistance, viral fitness and HIV disease progression: a tangled web is woven. J Antimicrob Chemother. 2005;55(4):413–416. doi:10.1093/jac/dki042
5. Abdool Karim SS, Naidoo K, Grobler A, et al. Timing of initiation of antiretroviral drugs during tuberculosis therapy. N Engl J Med. 2010;362(8):697–706. doi:10.1056/NEJMoa0905848
6. Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505. doi:10.1056/NEJMoa1105243
7. Montaner JS, Hogg R, Wood E, et al. The case for expanding access to highly active antiretroviral therapy to curb the growth of the HIV epidemic. Lancet. 2006;368(9534):531–536. doi:10.1016/S0140-6736(06)69162-9
8. Wood E, Milloy MJ, Montaner JS. HIV treatment as prevention among injection drug users. Curr Opin HIV AIDS. 2012;7(2):151–156. doi:10.1097/COH.0b013e32834f9927
9. Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. doi:10.7326/0003-4819-133-1-200007040-00004
10. Mastro TD. Intermittent use of triple-combination therapy is predictive of mortality at baseline and after 1 year of follow-up. AIDS. 2003;17(Suppl 4):S123–124. (). doi:10.1097/00002030-200317004-00025
11. Bangsberg DR, Perry S, Charlebois ED, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15(9):1181–1183. doi:10.1097/00002030-200106150-00015
12. Byrd KK, Hou JG, Hazen R, et al. Antiretroviral adherence level necessary for HIV viral suppression using real-world data. J Acquir Immune Defic Syndr. 2019;82:245–251. doi:10.1097/QAI.0000000000002142
13. Bartlett JA. Addressing the challenges of adherence. J Acquir Immune Defic Syndr. 2002;29(Suppl 1):S2–S10. doi:10.1097/00126334-200202011-00002
14. Ortego C, Huedo-medina TB, Llorca J, et al. Adherence to highly active antiretroviral therapy (HAART): a meta-analysis. AIDS Behav. 2011;15(7):1381–1396. doi:10.1007/s10461-011-9942-x
15. Kelly JD, Giordano TP. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS. 2011;25(8):1137. (). doi:10.1097/QAD.0b013e32834670d7
16. Abara WE, Adekeye OA, Xu J, Heiman HJ, Rust G. Correlates of combination antiretroviral adherence among recently diagnosed older HIV-infected adults between 50 and 64 years. AIDS Behav. 2016;20(11):2674–2681. doi:10.1007/s10461-016-1325-x
17. Beer L, Skarbinski J. Adherence to antiretroviral therapy among HIV-infected adults in the United States. AIDS Educ Prev. 2014;26(6):521–537. doi:10.1521/aeap.2014.26.6.521
18. Amico KR, Barta W, Konkle-parker DJ, et al. The information-motivation-behavioral skills model of ART adherence in a deep south HIV+ clinic sample. AIDS Behav. 2009;13(1):66–75. doi:10.1007/s10461-007-9311-y
19. Norton WE, Amico KR, Fisher WA, et al. Information-motivation-behavioral skills barriers associated with intentional versus unintentional ARV non-adherence behavior among HIV+ patients in clinical care. AIDS Care. 2010;22(8):979–987. doi:10.1080/09540121003758630
20. Santillan Torres Torija C, Villagran Vazquez G, Robles Montijo SS, de Lourdes Eguiluz Romo L. The information and motivation and behavioral skills model of ART adherence among HIV-positive adults in Mexico. J Int Assoc Provid AIDS Care. 2015;14(4):335–342. doi:10.1177/2325957415581903
21. Fisher JD, Fisher WA, Amico KR, Harman JJ. An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychol. 2006;25(4):462–473. doi:10.1037/0278-6133.25.4.462
22. Bertholon DR, Rossert H, Korsia S. The patient’s perspective on life with antiretroviral treatment: results of an 887-person survey. AIDS Read. 1999;9(7):462–469.
23. Horvath KJ, Smolenski D, Amico KR. An empirical test of the information-motivation-behavioral skills model of ART adherence in a sample of HIV-positive persons primarily in out-of-HIV-care settings. AIDS Care. 2014;26(2):142–151. doi:10.1080/09540121.2013.802283
24. Rongkavilit C, Naar-king S, Kaljee LM, et al. Applying the information-motivation-behavioral skills model in medication adherence among Thai youth living with HIV: a qualitative study. AIDS Patient Care STDS. 2010;24(12):787–794. doi:10.1089/apc.2010.0069
25. Gordon CM. Commentary on meta-analysis of randomized controlled trials for HIV treatment adherence interventions. Research Directions and Implications for Practice. J Acquir Immune Def Syndr 2006;43(Suppl 1):S36–S40. doi:10.1097/01.qai.0000248347.87512.ba
26. Dilorio CK. Measurement in Health Behavior: Methods for Research and Education. Sanfrancisco: Jossey Bass; 2005.
27. Kwon M, Kim DJ, Cho H, Yang S. The smartphone addiction scale: development and validation of a short version for adolescents. PLoS One. 2013;8(12):e83558. doi:10.1371/journal.pone.0083558
28. Berglund AL, Ericsson K. Different meanings of quality of life: a comparison between what elderly persons and geriatric staff believe is of importance. Int J Nurs Pract. 2003;9(2):112–119. doi:10.1046/j.1322-7114.2003.00414.x
29. Samuel DB, South SC, Griffin SA. Factorial invariance of the five-factor model rating form across gender. Assessment. 2015;22(1):65–75. doi:10.1177/1073191114536772
30. McDonald RP, Ho MH. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002;7(1):64–82. doi:10.1037/1082-989X.7.1.64
31. Chen TF, Chou KR, Liao YM, Ho CH, Chung MH. Construct validity and reliability of the Chinese version of the disaster preparedness evaluation tool in Taiwan. J Clin Nurs. 2015;24(7–8):1132–1143. doi:10.1111/jocn.12721
32. Siril H, Fawzi MC, Todd J, et al. Hopefulness fosters affective and cognitive constructs for actions to cope and enhance quality of life among people living with HIV in Dar Es Salaam, Tanzania. J Int Assoc Provid AIDS Care. 2017;16(2):140–148. doi:10.1177/2325957414539195
33. Dalmida SG, McCoy K, Koenig HG, et al. Examination of the role of religious and psychosocial factors in HIV medication adherence rates. J Relig Health. 2017;56(6):2144–2161. doi:10.1007/s10943-017-0377-1
34. Ammassari A, Trotta MP, Murri R, et al. Correlates and predictors of adherence to highly active antiretroviral therapy: overview of published literature. J Acquir Immune Defic Syndr. 2002;31(Suppl 3):S123–S127. doi:10.1097/00126334-200212153-00007
35. Falagas ME, Zarkadoulia EA, Pliatsika PA, Panos G. Socioeconomic status (SES) as a determinant of adherence to treatment in HIV infected patients: a systematic review of the literature. Retrovirology. 2008;5:13. doi:10.1186/1742-4690-5-13
36. Bandura A. Human agency in social cognitive theory. Am Psychol. 1989;44(9):1175–1184. doi:10.1037/0003-066X.44.9.1175
37. Johnson MO, Neilands TB, Dilworth SE, Morin SF, Remien RH, Chesney MA. The role of self-efficacy in HIV treatment adherence: validation of the HIV treatment adherence self-efficacy scale (HIV-ASES). J Behav Med. 2007;30(5):359–370. doi:10.1007/s10865-007-9118-3
38. Catz SL, Kelly JA, Bogart LM, Benotsch EG, McAuliffe TL. Patterns, correlates, and barriers to medication adherence among persons prescribed new treatments for HIV disease. Health Psychol. 2000;19(2):124–133. doi:10.1037/0278-6133.19.2.124
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.