")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 12
Reliability and Validity of Ethiopian Amharic Version of the PedsQLTM 4.0 Generic Core Scales and PedsQLTM 3.0 Diabetes Module
Authors Girma D , Abita Z , Wale A , Tilahun S
Received 22 March 2021
Accepted for publication 10 June 2021
Published 22 June 2021 Volume 2021:12 Pages 77—89
DOI https://doi.org/10.2147/AHMT.S312323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Alastair Sutcliffe
Desalegn Girma,1 Zinie Abita,2 Alemnew Wale,1 Semahagn Tilahun1
1Mizan-Tepi University, College of Health Science, Department of Midwifery, Mizan-Teferi, Ethiopia; 2Mizan-Tepi University, College of Health Science, School of Public Health, Department of Reproductive Health, Mizan-Teferi, Ethiopia
Correspondence: Desalegn Girma Tel +251933704490
Email [email protected]
Background: The PedsQLTM 4.0 generic core scales (GCS) assess the generic health by integrating with disease-specific PedsQLTM 3.0 diabetes module (DM). The PedsQLTM 3.0 DM measures the health-related quality of life (HrQoL) specific to diabetes. Even though there is no translation to Ethiopian Amharic, the instruments had translated to different languages and validated. The study is aimed to assess the validity and reliability of the Amharic version of the PedsQLTM 4.0 GCS and the PedsQLTM 3.0 DM in children and adolescents with diabetes.
Methods: PedsQLTM 4.0 GCS and the PedsQLTM 3.0 DM were administered on 193 children and adolescents with diabetes and their parents. The validity was examined by the exploratory factor analysis, multitrait/multi-item scaling analysis, and multitrait-multimethod and monotrait-multimethod analysis. Cronbach’s alpha coefficient checked the reliability.
Results: Cronbach’s alpha coefficient for the total PedsQLTM 4.0 GCS (α child self-report= 0.96; α parent proxy report= 0.95) and for total PedsQLTM 3.0 DM (α child self-report= 0.96; α parent proxy report=0.93) were acceptable at individual patient-level analysis. The monotrait-multimethod correlations were higher than multitrait-multimethod correlations. In multitrait/multi-item scale analysis, both total PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM had an excellent item convergent and discriminatory validity success rate.
Conclusion: The Amharic versions of the PedsQLTM 4.0 GCS and the PedsQLTM 3.0 DM were valid and reliable instruments to measure the HrQoL of children and adolescents with diabetes.
Keywords: quality of life, PedsQL™ 3.0 DM, PedsQLTM 4.0 GCS, validation, reliability
Background
Diabetes is one of the most common chronic diseases in children and adolescents; it affects about 1,106,500 children and adolescents worldwide.13 In Ethiopia, a study in Tikur Anbessa specialized hospital has reported a high prevalence of diabetes among school-age children, and it was 2.81 per 1000 cases.5
Children and adolescents with uncontrolled diabetes are at risk of complications such as diabetic ketoacidosis, hyperosmolar, hyperglycemic state, and chronic microvascular and macrovascular24 Thus, complications and the preventive treatment in diabetes interfere with the daily life of children and adolescents, and it has an impact on health-related quality of life.13,14
Health-related quality of life (HrQoL) is a patients’ perception of disease regarding physical functioning, psychological functioning (emotional and cognitive), independence, personal beliefs, and social function16 In modern clinical practice, measurement of HrQoL was increasingly recognized as necessary, to provide additional information for health professionals and predict disease outcomes in children and adolescents with chronic illness.4,9,11 It was related to glycemic control; previous studies have shown that patients who had a low score in HrQoL had poor glycemic controls.1,3,6,7,14,21,25
Recent studies have recommended the measurement of HrQoL in conjunction with medical treatment in chronic illnesses, like diabetes.11,22 So to measure HrQoL, many instruments have been designed and developed. However, most of these instruments were developed for adults and modified for children. Such as the diabetes quality of life for youth (DQOLY) designed by Ingersoll et. is modified from the adult version, which has been used in the Diabetes Control and Complications Tria.17 It measures the diabetes-specific quality of life in adolescents but does not measure the HrQoL of children younger than 11 years. The lack of tools to assess HrQoL in children aged less than 11 years inspired Varni to design the Pediatric Quality of Life Inventory(PedsQL),26 which includes PedsQLTM Generic Core and a scale specific to certain diseases, including Pediatric Quality of Life InventoryTM 3.0 Diabetes Module (PedsQLTM 3.0 DM) for children and adolescents with diabetes. The PedsQLTM was used to measure HrQoL across a broad age range.26 It has an advantage in that the generic core scale has covered the core domain of health defined by the World health organization (physical, social, and emotional function) and the role(school) functioning.31 The PedsQLTM can create disease-specific scales, which ucan be completed in conjunction with a generic core scale to assess the impact of specific disease on HrQoL to a particular patient.
In measuring HrQoL, the instruments must be brief, with reliability and validity to obtain accurate information, they must be easy to understand and scored, and lastly, the instruments must be sensitive to sudden changes in patients’ attitudes.27 Both PedsQLTM Generic Core and PedsQLTM 3.0 DM have been translated and validated for many languages, have been used in research. The PedsQLTM Generic Core Scales had a good feasibility y, reliability, and validity had confirmed in studies.2,15,18,19,23,28 Similarly, the PedsQLTM 3.0 Diabetes Module had confirmed in studies.2,10,20 However, there was no Amharic translation of PedsQLTM, and Still, the psychometric adequacy of these instruments has not been tested in Ethiopian children and adolescents with diabetes.
Therefore, the primary purpose of the current study was to examine the reliability and validity of Ethiopian Amharic translation of both PedsQLTM Generic Core Scales and PedsQLTM 3.0 Diabetes Module (DM) for children self-reports aged 8–18 years and parents’ proxy reports for their child for this age group.
Methods
Participants and Settings
A total of 193 children and adolescents (aged 8–18 years) with diabetes for at least three months and their parents/caregivers were surveyed between November 1/ 2018- December 1 /2018 from Addis Ababa Tikur Anbesa specialized hospital and Yekatit 12 Hospital diabetics clinic during regular follow up.
Measures
Pediatric Quality of Life Inventory 4.0 Generic Core Scale (PedsQLTM 4.0 GCS): was developed to measure the core health of healthy and patient populations. It was available for the age group (5–7, 8–12, 13–18, and > 19 years). It has a 23-items, multidimensional quality-of-life instrument. Items in each four sub Scales were Physical functioning (eight items), Emotional Functioning, Social Functioning, and School functioning (five items for each). It was reported with both child and parent. The participants rated how much of a problem there has been in the past one month on a five-point Likert- scale from 0–4. (0 = never a problem; 1 = almost never a problem; 2 = sometimes a problem; 3 = often a problem and 4 = almost always a problem). Then, each items were reversely scored and linearly transformed to a 0–100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0), so that higher scores indicate better health-related quality of life. Scale scores were computed as the sum of the Items divided by the number of items answered. If >50% of the items in the scale are missing, the scale score is not computed. The PedsQLTM 3.0 DM is a diabetes-specific instrument available for the age group (2–18 years). Both child and parent reported it. It has five scales: 1) diabetes symptoms (11 items); 2) treatment barriers (4 items); 3) treatment adherence (7 items); 4) worry (3 items) and 5) communication (3 items). The format instructions and scoring methods are similar to the generic core scale. The study was aimed to test the psychometric properties of the child and parent PedsQLTM 4.0 GSC and PedsQLTM 3.0 DM, which was reported for age group 8–12 years and 13–18 years. later on, to assess the HrQoL of children and adolescents with diabetes, based on the following initial hypothesis, that the hormonal change, and mood swings in adolescents, and the developmental changes of school-age children to adolescence, growth spurts, participation in sports, and social interactions with the school peers could be contributing to poor HrQoL.
Operational Definition
The Fasting blood glucose level has been used to measure the target glycemic level of children and adolescents with diabetes; based on Children and Adolescents: Standards of Medical Care in Diabetes, American diabetes association8 Controlled glycemic level fast blood glucose level 90–130 mg/d and uncontrolled blood glucose level fast blood glucose level <90 or >130 mg/d
Procedure
Permission to a forward translation of the original PedsQLTM 4.0 GCS and PedsQLTM3.0 DM was obtained from the Mapi Research Trust on behalf of the author, Dr. James Varni. The linguistic translation had been done based on the recommended guidelines. Based on this:-
Step 1: The original version of both PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM were independently translated from US English (source language) to Ethiopian Amharic (target language) by two local professional translators (psychiatrist and a clinical psychologist). The translators and investigators have discussed the two versions for any discrepancies, and after common consensus, the final forward translation has developed and was sent to Mapi Research trust.
Step 2. The new Ethiopian Amharic (target language) version has been translated back to US English (source language) by two bilingual translators. Then it was sent to the Mapi Research trust, and they suggested no changes.
Step 3. Cognitive Interviewing was performed on 15 children and adolescents with diabetes (aged 8–18 years) and their parents. In this phase, any ambiguity in translated items to children or their parent was identified, modified and then a report was sent to Mapi Research trust.
Step 4. The final PedsQLTM 4.0 GCS and PedsQLTM3.0 DM Ethiopian Amharic version had been developed for the field test. Then field test was started by obtaining permission from Addis Ababa Tikur Anbessa specialized and Yekatit 12 hospitals. A total 193 of children and adolescents aged between 8–18 years with their parents/caregivers, diagnosed with diabetes for at least three months were recruited systematically with every other patient from November 1/ 2018- December 1 /2018 based on the time to they arrived at the endocrine clinic for follow up visits. The purpose of the study was explained, and confidentiality was assured; then, children and adolescents with their respective parents were interviewed separately by a trained data collector. Regular supervision was done by two trained health professionals throughout the survey.
Statistical Analysis
Data were entered by Epi data version 4.20 and analyzed by SPSS version 21. It was summarized by frequencies, percentage, mean and standard deviation and presented by a table Cronbach’s alpha coefficient tested scale Internal consistency reliability, and its value equal to or greater than 0.70 was considered satisfactory. Construct validity was evidenced by Convergent Validity and discriminant validity. The inter-correlations coefficient between Subscales explored convergent validity. Correlations are designated as weak (0.10–0.29), medium (0.30–0.49), and strong (=0.50). Discriminant validity is supported whenever an item has a higher correlation for its own hypothesized subscale than other subscales. A scaling success rate is determined when the correlation of the item to its scale is higher than the correlations of that item to another scale. Further, monotrait-multimethod correlations (eg, concordance between self-report and proxy-report for the same subscale) and multitrait-monomethod correlations (eg, correlations among subscales within the self-report and proxy report) have been conducted to strengthen the validity. Further, the construct validity was tested by the intercorrelations analysis between the total PedsQLTM 4.0 Generic Core Scale score and PedsQLTM3.0 Diabetes Module scales with the initial hypothesis, a higher PedsQLTM disease-specific subscale score could be correlated with a higher Generic Core Scale score. The external discriminant validity of the questionnaire was done across the dichotomous patients’ characteristics (such as sex, disease duration, and glycemic control). Exploratory factor analysis was used to evaluate the aggregating dimensions and structural relationships between the items of the PedsQL™ 4.0 GCS and PedsQL™3.0 DM. Principal Component Analysis was used to extract factors with oblique rotation (Direct Oblimin). Factors with an eigenvalue less than one were disregarded.
Data Quality Control
Data quality was ensured during collection, coding, entry, and analysis. The training was given to data collectors and supervisors. Regular supervision of data collectors was done. Before data entry, the filled questioner was checked by data collectors, supervisors, and principal investigators for completeness and clarity daily. Incomplete data were discarded.
Result
Characteristics of the Study Population
A total of 193 children aged 8–18 and their parents were included in the study. About 105 (54.4%) of them were males, and about 88 (45.6%) were females. The median duration of participants with diabetes was five years. They had 183.28±81.95 mg/dl mean levels of fasting blood sugar (FBS) (Table 1)
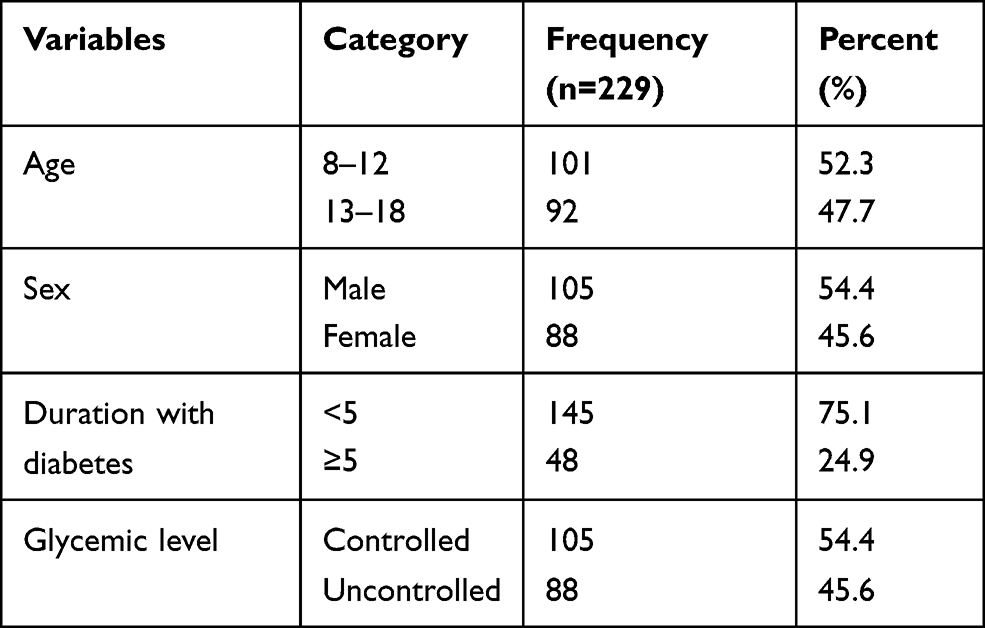 |
Table 1 Characteristics of Children and Adolescents with Diabetes |
Feasibility
The questionnaires were completed within 5–10 minutes (for GCS) and 10–15 minutes (for DM). There was no recorded missing for both child self and parent proxy reports of PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM.
Internal Consistency
A satisfactory Cronbach’s α coefficient level had recorded in all PedQL TM 4.0 GCS subscales, range, 0.83 to 0.90 for child self-report and 0.80 to 0.84 for parent proxy reports, Table 2. A similar result was seen in all PedsQLTM 3.0 DM subscale domains, range 0.84 to 0.86 for child self-report, and 0.74 to 0.77 for parent proxy reports, Table 3.
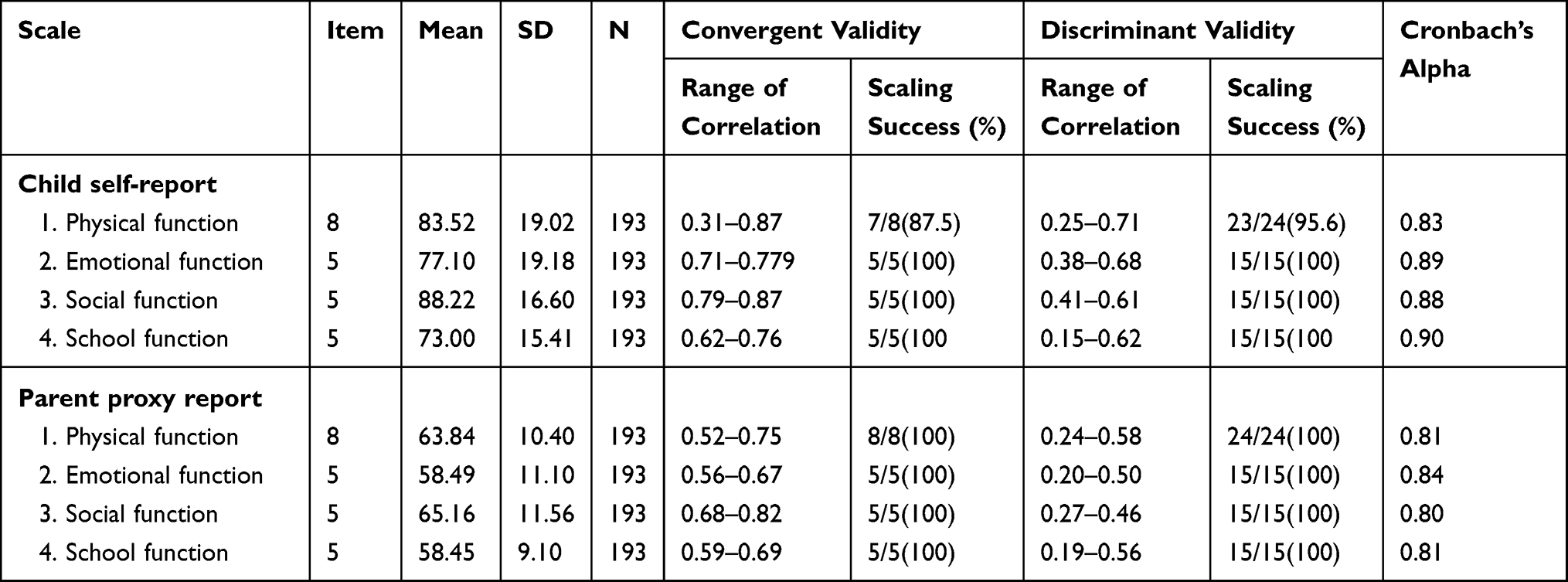 |
Table 2 Item Scaling Tests: Convergent and Discriminant Validity for the PedsQL™ 4.0 Generic Core Scales Subscales |
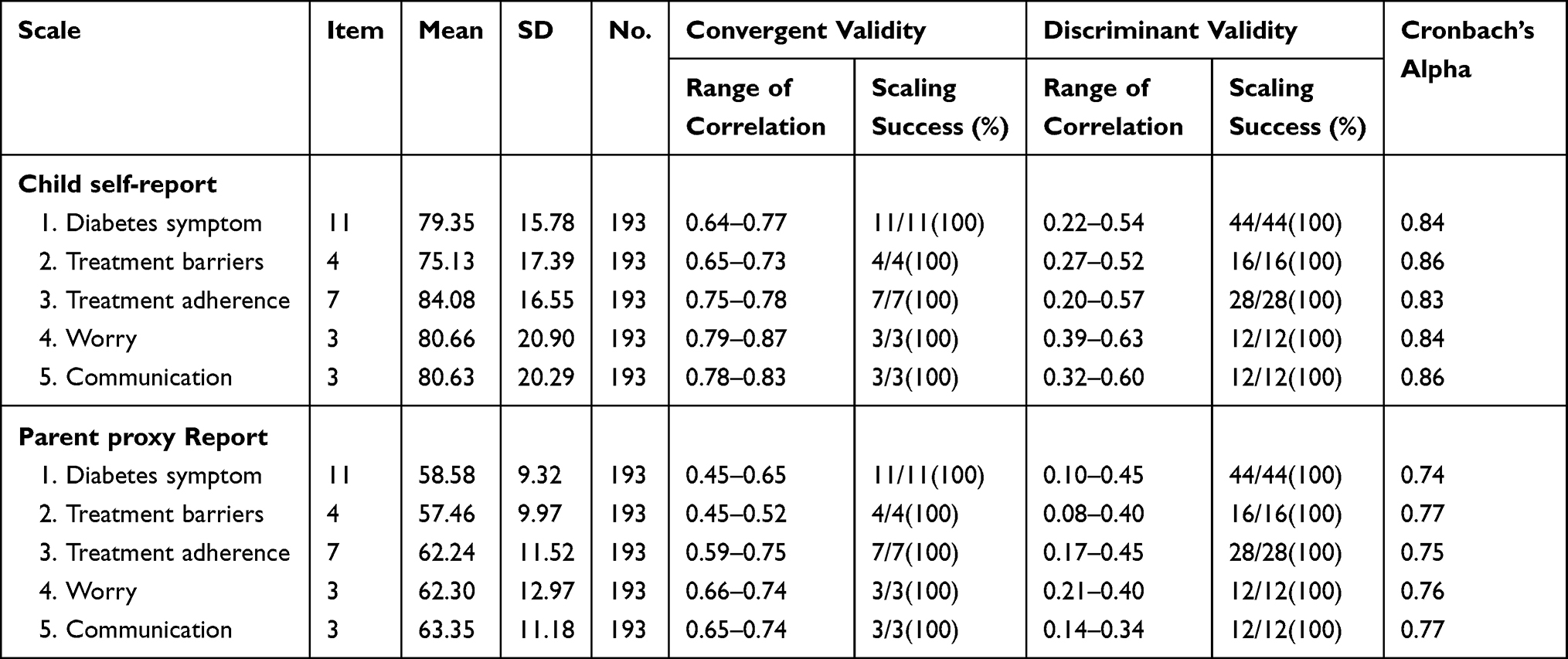 |
Table 3 Item Scaling Tests: Convergent and Discriminant Validity for the PedsQL™ 3.0 Diabetes Module Subscales |
Construct Validity
The item-to-scale correlation for both PedsQLTM 4.0 GCS and PedsQLTM3.0 DM was presented in Tables 2 and 3, respectively. This result shows that the scaling success rates for convergent validity for all PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM subscales were 100% except for physical function in the generic core scale. The success rate for items discriminatory validity of PedsQLTM 4.0 GCS was 98.6%(68/69) for children’s report and 100%(69/69) for parent proxy report. The items discriminatory validity success rate of PedsQLTM 3.0 DM was 100% (112/112) for both child self-report and parent proxy reports.
The intercorrelations of PedSQLTM 4.0 GCS subscales and PedsQLTM 3.0 DM subscales have shown in Tables 4 and 5, respectively. In both versions, the Monotrait multimethod correlations were statistically significant in all subscales; it was higher when compared to the multitrait-multimethod correlation. In Monotrait multimethod, all subscales are supposed to measure a similar disease impact had the highest convergent correlations in the intercorrelation matrix. In the multitrait-multimethod correlation, all scales supposed to measure different disease’s impact had a lower intercorrelation, were valid to diverge.
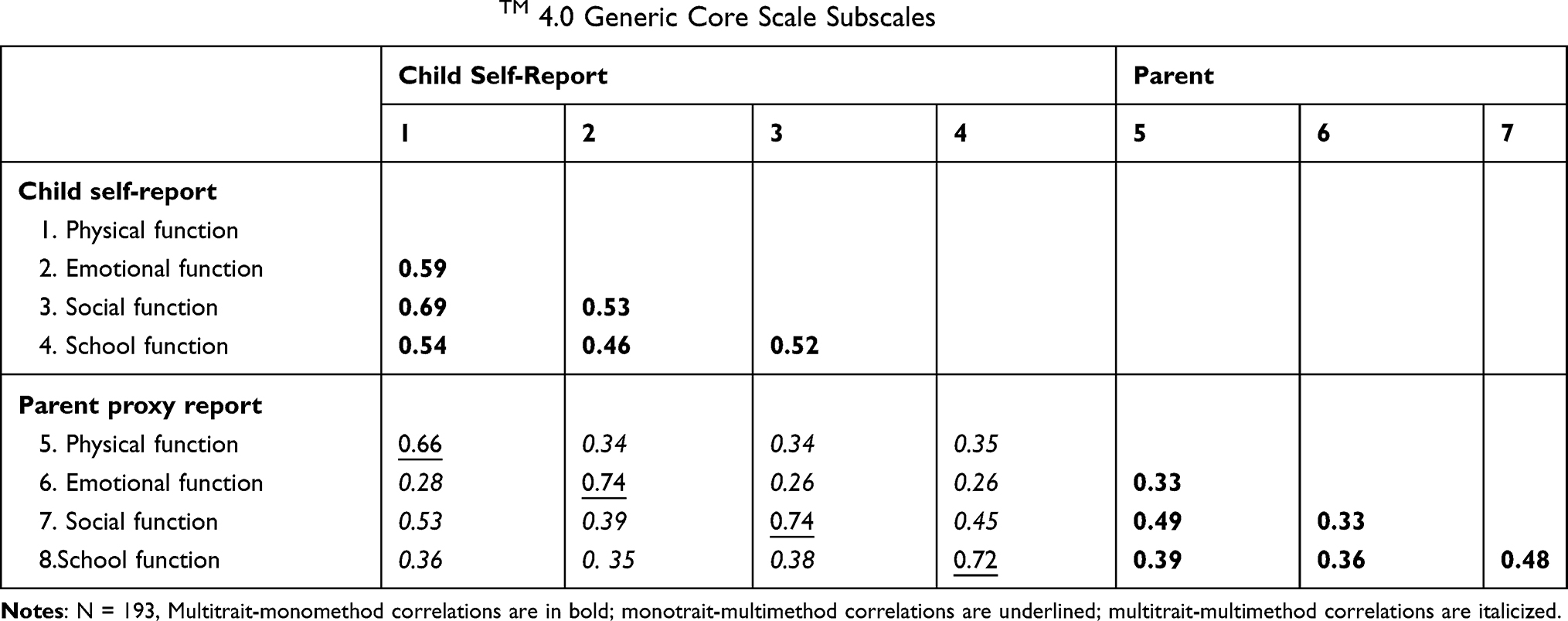 |
Table 4 Intercorrelations Among PedsQLTM 4.0 Generic Core Scale Subscales |
 |
Table 5 Intercorrelations Among PedsQLTM 3Diabetes Module Subscales |
The construct validity had also examined by the relation of intercorrelations analysis among the total PedsQLTM 4.0 Generic Core Scale score with the PedsQTM 3.0 Diabetes Module scales scores, indicated in Table 6. The intercorrelation between the total PedsQLTM 4.0 generic core scale and the total PedsQLTM 3.0 diabetes module scores for the child report was 0.78 and for the parent proxy report was 0.73. In the child report, the total PedsQLTM 4.0 generic core scale was strongly correlated with the subscale of the PedsQLTM 3.0 diabetes module except for the subscale (0.47 in the communication). The intercorrelation between the total parents PedsQTM Generic Core Scale and the total child PedsQLTM 3.0 diabetes module was 0.53; the intercorrelation for total child PedsQTM Generic Core Scale and total parent PedsQLTM 3.0 diabetes module was 0.55.
 |
Table 6 Intercorrelations Among Total PedsQLTM 4.0 Generic Core Scales Score and PedsQLTM 3.0 Diabetes Module Subscale |
The study revealed four-factor structures of PedsQLTM 4.0 GCS for both children’s self-report and parent proxy report, indicated in Tables 7 and 8, respectively. In child self-report, the items related to physical health and social function had loaded in one factor, and the rest items of subscales had clear loading. The parent proxy report items related to a school function were split into two factors, and items such as “ pay attention in class” “forgetting things” and “keeping up with schoolwork” had loaded in one factor with social function items.
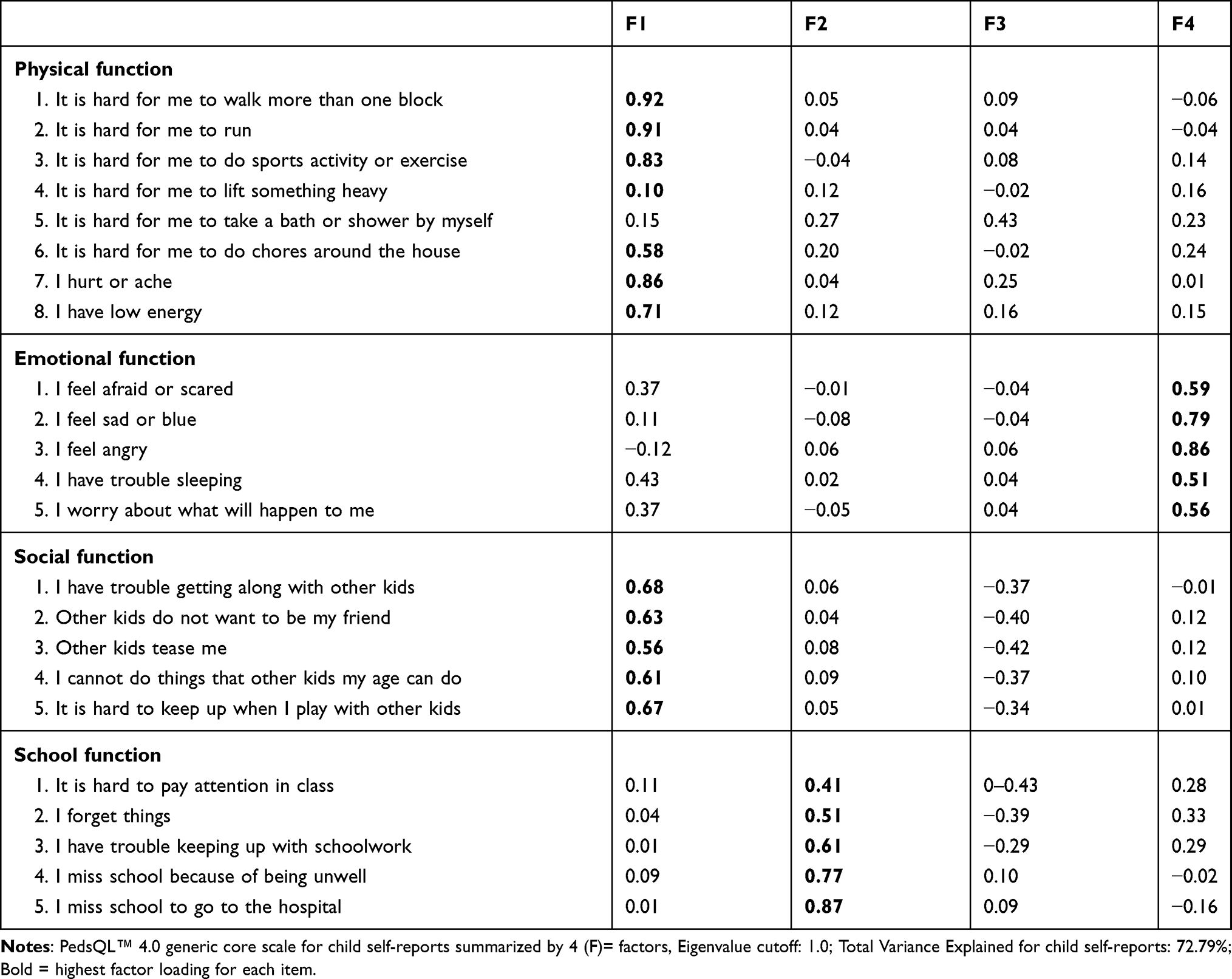 |
Table 7 PedsQL™ 4.0 Generic Core Scale Questionnaire Factor Loadings for Child Self-Reports |
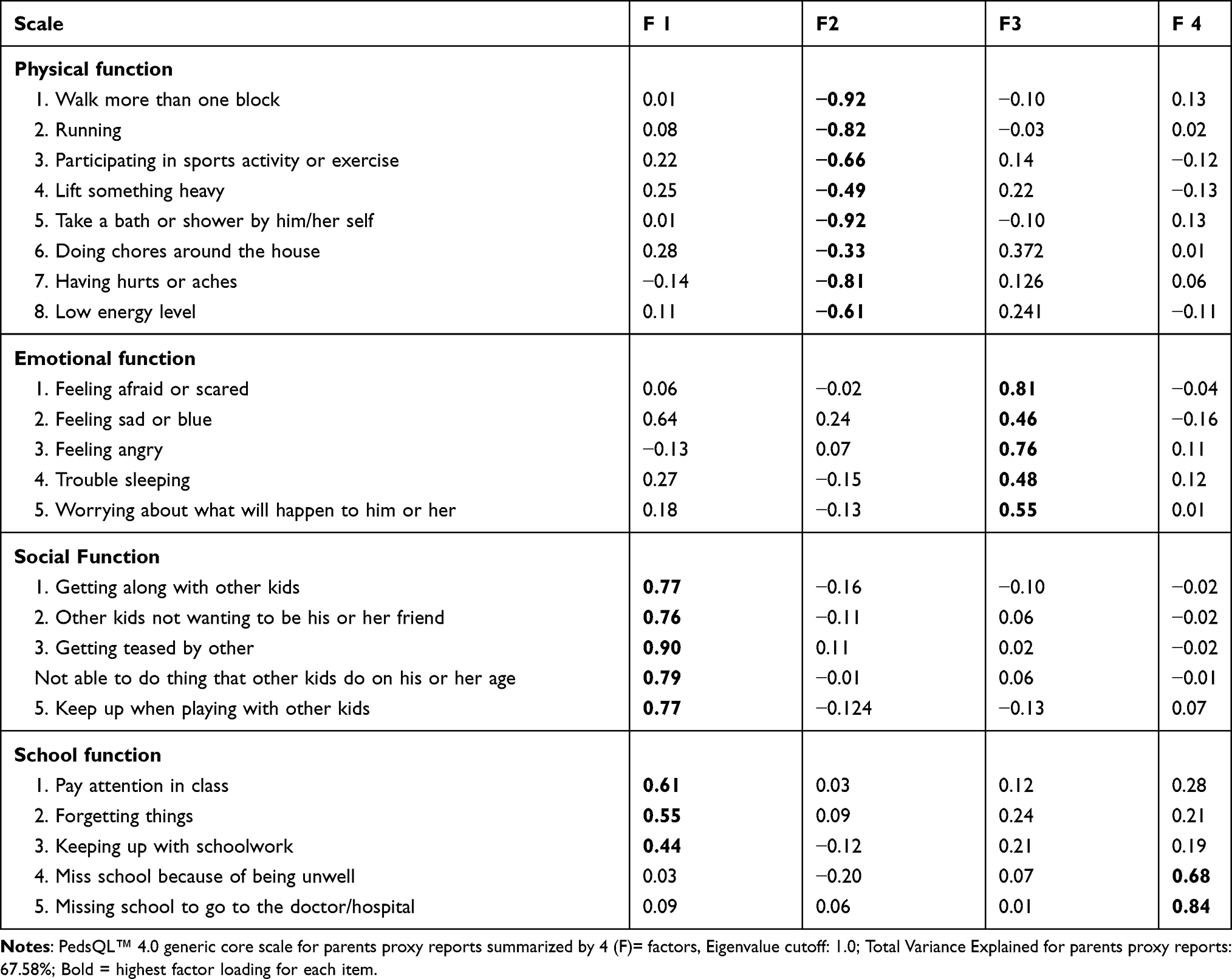 |
Table 8 PedsQL™ 3 PedsQL™ 4.0 Generic Core Scale Questionnaire Factor Loadings for Parent Proxy |
The study also revealed a five factors solution of PedsQLTM 3.0 DM; the results for child and parents proxy reports were presented in Tables 9 and 10, respectively. In child self-items of diabetes, the symptom was split into the two-factor structure, and the items of treatment adherence and communication were loaded in one factor. Similarly, in parent reports, items in diabetes symptoms were split into two factors, and items of communication and treatment barriers were loaded in a one-factor solution.
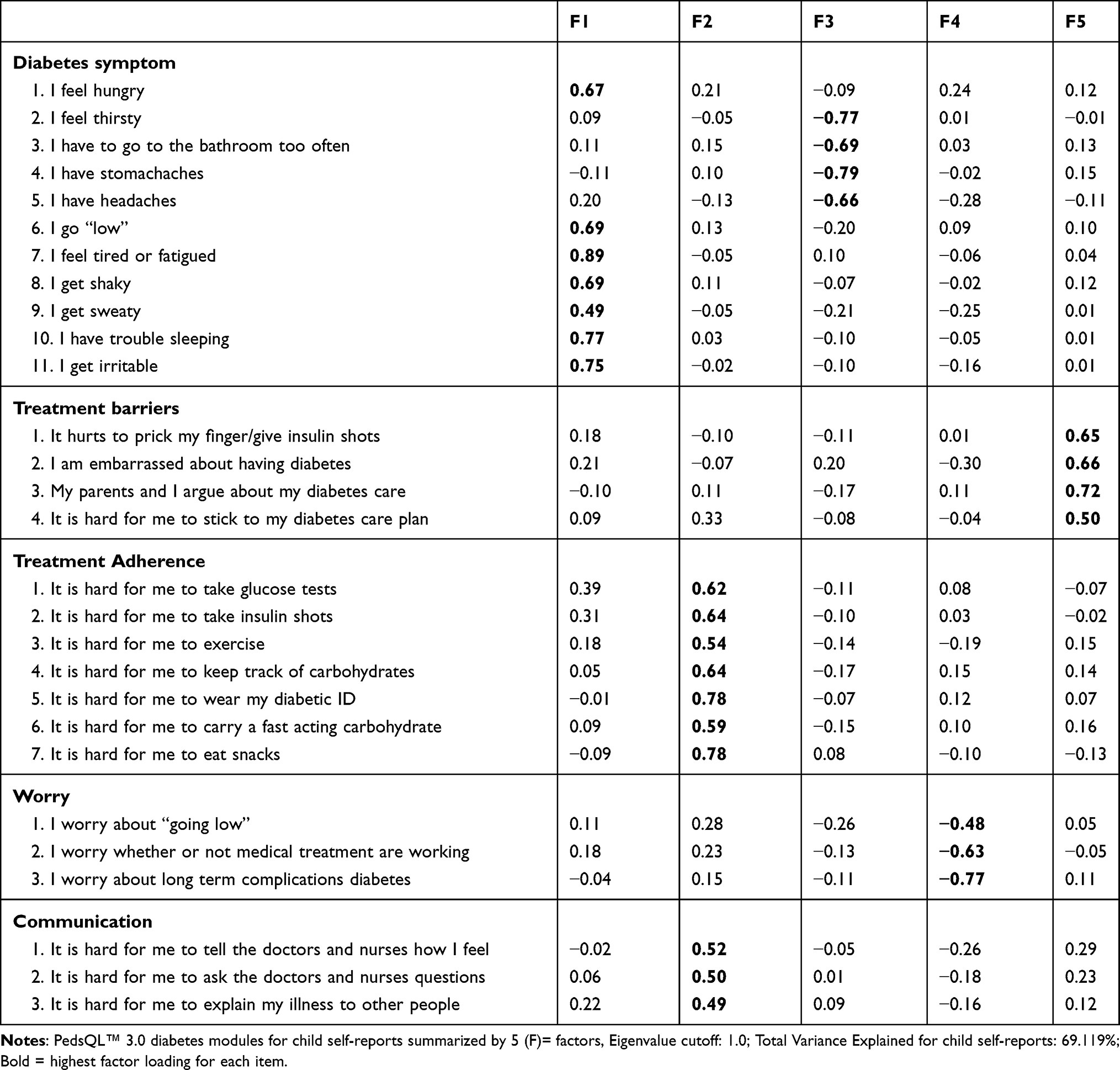 |
Table 9 PedsQL™ 3.0 Diabetes Module Questionnaire Factor Loadings for Child Self-Reports |
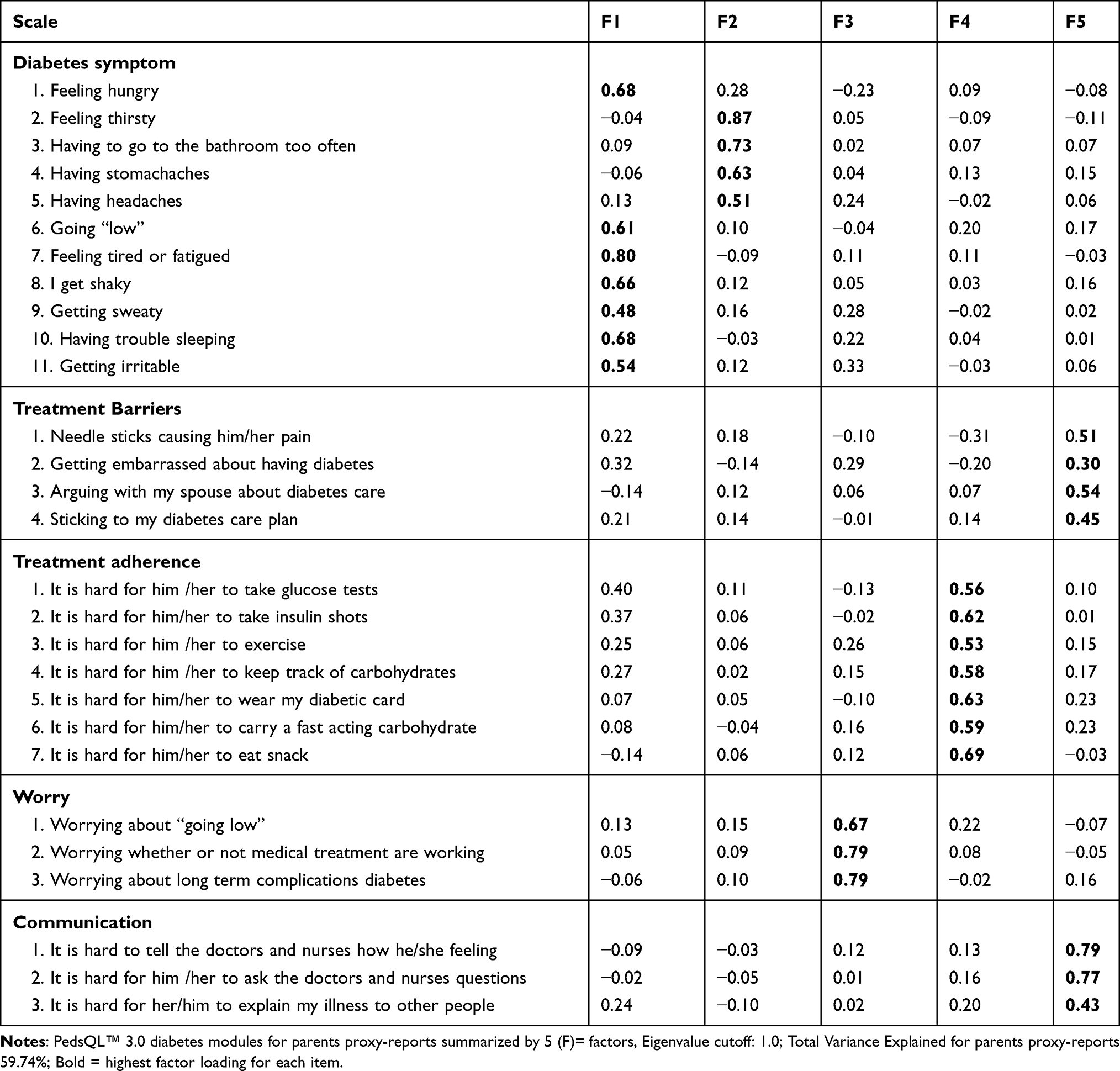 |
Table 10 PedsQL™ 3.0 Diabetes Module Questionnaire Factor Loadings for Parent Proxy -Report |
The external discriminant validity for both the PedsQL™4.0 GCS and PedsQL™3.0 Diabetes Module child self report was done across gender, age, duration with diabetes, and glycemic levels indicated in the Tables 11 and 12, respectively. In PedsQL™4.0 GCS, differences in mean were observed with age group; the mean value for children aged 8–12 years was statistically different when compared to that of children aged 13–18 years in total PedsQL™4.0 GCS (t =2.24, P=0.02 and in physical function (t=2.15, p=0.03). A mean difference across sex was observed in total PedsQL™4.0 GCS (t=2.14, P=0.03), in Social function (t=2.18,p=0.03) and in school function (t= 2.41,p=0.02) and there was also a statistical mean difference between controlled and uncontrolled glycemic levels; in total PedsQL™4.0 GCS (t=6.84, p=0.0001), in Physical function (t=7.38, p=0.0001), in Emotional function (t=3.30,p=0.001), in Social function (t=6.62, p=0.0001) and in School function (t=4.58, t=0.0001). In PedsQL™3.0 Diabetes, there was a mean difference between controlled and uncontrolled glycemic levels in total PedsQL™3.0 DM (t=7.10, p=0.0001), in diabetes Symptoms (t=4.58, p=0.0001), in Treatment Barriers (t=4.46, p=0.0001), in Treatment Adherence (t=4.18,p=0.0001), in Worry (t=5.41, p=0.0001) and in communication (t=5.73, p=0.0001).
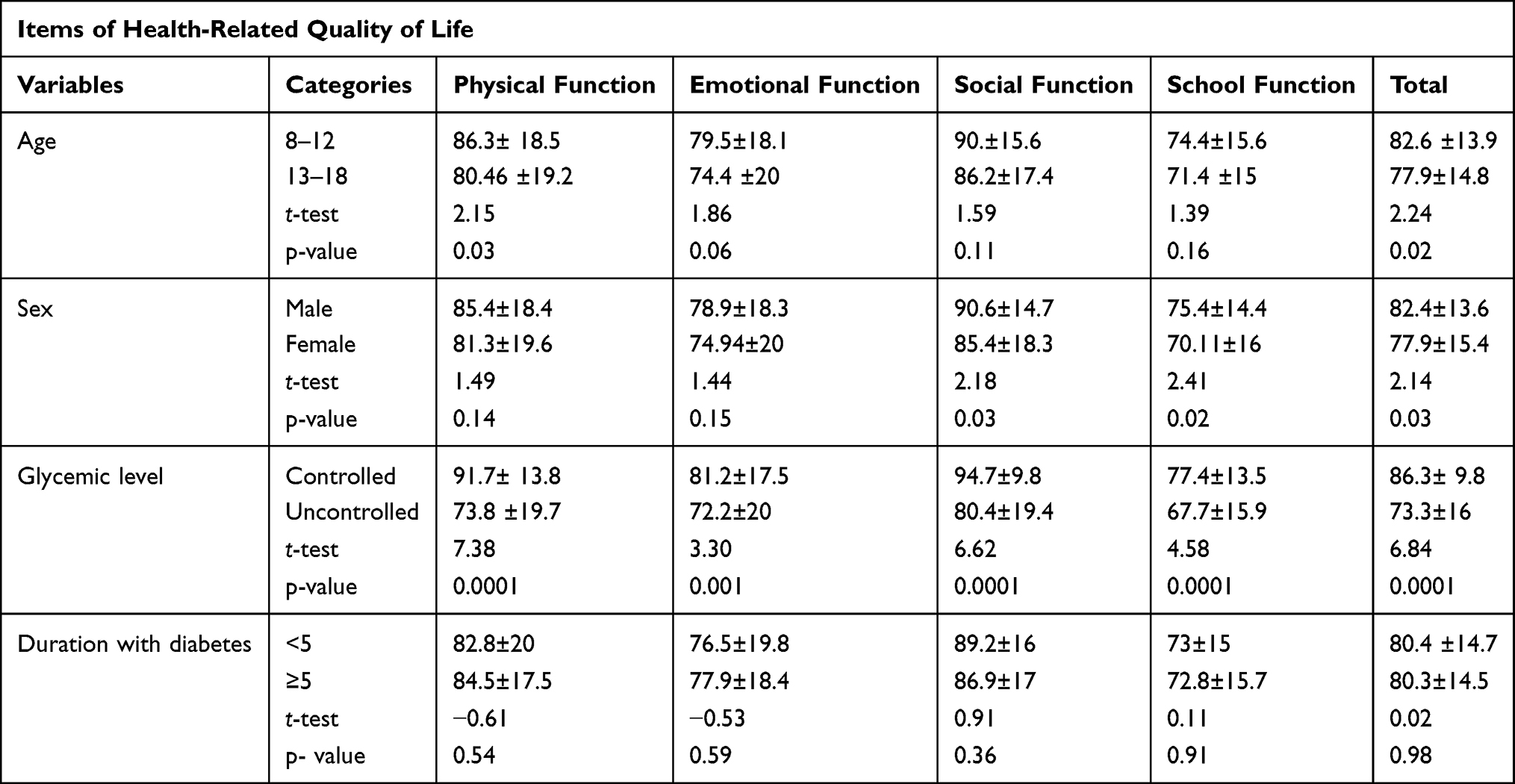 |
Table 11 Discriminatory Validity of PedsQL™ 4.0 Generic Score Across the Patient Characteristics |
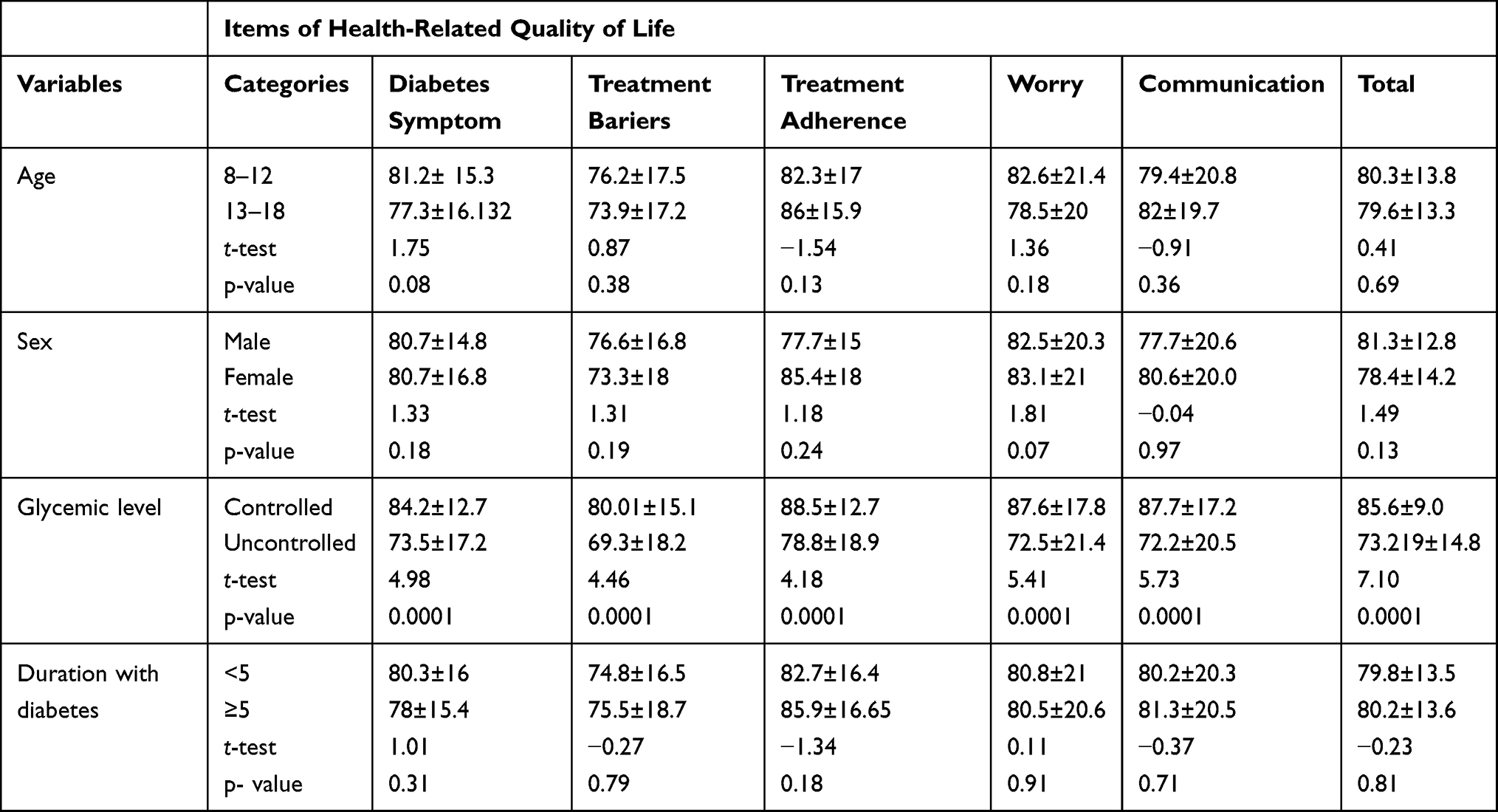 |
Table 12 Discriminatory Validity of PedsQL™ 3.0 Diabetes Module Across the Patient Characteristics |
Discussion
The study had disclosed the psychometrics properties of the Amharic version of PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM in Ethiopian children and adolescents with diabetes. The PedsQLTM 4.0 GCS, similarly to the studies done in Iran,18 and Kuwait,2 and the PedsQLTM 3.0 DM, similarly to the studies10,12,20 confirmed that the child and parents proxy report could be used to measure the HrQoL of children and adolescents with diabetes.
In this study, almost all items of PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM Amharic version have been answered in both child self and parent proxy reports. About 5–10 minutes and 10–15 minutes has required to fill the PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM, respectively; This was comparable to the Arabic translation2 and Italian translation.10 This indicates the tools have taken a short time to fill, and the patients can easily complete the questioner.
Children and adolescents with diabetes had a comparable mean score of HrQoL to the original US English version26 and Arabic translation.2 Such tools were acceptable to measure the HrQoL of children and adolescents with diabetes.
The internal consistency coefficient for the total PedsQLTM 4.0 GCS Amharic version was (α=0 0.96) for child self-report and (α=0.95) for parent proxy reports; which was comparable with the reliability reported by the original PedsQLTM 4.0 GCS US English version.29 And the total PedsQLTM 3.0 DM Amharic version had internal reliability (α=0.96) for child self-reports and (α=0.93) for parent proxy reports; which was comparable to the Brazil-Portuguese translation,12 Hungarian Version,20 and it was above the Italian translation.10 Generally, the internal consistency coefficient value for both total PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM had exceeded the minimum recommended coefficient value (α=0.90) to evaluate the HrQoL at the individual patient level, whereas the subscales in both versions had a minimum recommended internal consistency coefficient value for group comparisons (α=0.70).30
There was a good item convergent validity and item discriminatory validity of total PedsQLTM 4.0 GCS; Its subscales have 100% items convergent and items discriminatory validity success rate except for child report on Physical function (87.5% items convergent validity,95.6% items discriminatory validity success rate), this was comparable with the Persian version.18 The items discriminatory success rate for total PedsQoLTM 3.0 DM was 100% in both child and parent proxy reports, this was higher than the Persian version,18 and the Italian version;10 this implies, items were strongly correlated in their hypothesized scale than other scales (convergent validity) and items were weakly correlated in another scales than its scale (discriminatory validity).
Unlike the original US PedsQLTM 4.0 GCS version29 and similar to the Persian version,18 the current study supports a four-factor solution. In child self-reports, items related to physical health and social health had loaded in one factor. This is true: intact physical health was the first line to have children and adolescents a good social function with their peers. Despite this, the item discriminatory validity success rate was satisfactory (physical function =95.6% and social function =100%), which implies, items should have been scored and grouped under its scale as the original version. In parent proxy reports, the first three items related to a school function, “hard to concentrate,” “forget things,” “trouble keeping up with school work,” and social function was loaded together in a one-factor structure; however, items have a strong correlation within its subscale than other subscales. In parents proxy reports, similar to the Norwegian version;23 the last two items of school function “miss school because not feeling well,” “miss school because of doctor appointment” loaded in other factors this might be the items were more related to physical aspect than cognitive components; hence, the items should have been grouped and scored under physical function subscale in clinical practices.
Like the original US PedsQLTM 3.0 DM,26 factor analysis in this study supports a five-factor structure for both child self and parents report. This was different from the Italian translation.10 In child self-report, items related to communication were loaded in one factor with treatment adherence, and in parents proxy reports, items related to communication were loaded in one factor with treatment Barries. The possible justification might be that wise communication with doctors and nurses or other people for any raising problem or any barriers related to disease has a paramount role in good treatment adherence. The items in each subscale were strongly correlated with its scale than other scales; so in clinical practices, items should have been scored and grouped in the respective scale as the original version. In factor analysis, items in diabetes symptoms were split into two-factor solutions in both child self and parent proxy reports, that all items were not grouped under postulated scale, i.e diabetes symptoms. So items such as, “I go low”, “I get shaky”, “I get sweaty”, “I have trouble sleeping”, “I get irritable” and “I feel hungry” should have been named, grouped, and scored as one subscale, and items such as, “I feel thirsty”, “I have to go to the bathroom too often”, “I have stomachaches”, and “I have headaches” should have been named, and grouped, and scored as one subscale.
Like to the Norwegian version,23 In the current study, the monotrait-multimethod correlations (correlation of subscales supposed to measure same “trait”) were higher than multitrait-multimethod correlations (correlation of subscales supposed to measure different “trait”) in all subscale of PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM. This test was examined the scale to scale level validity of the two different instruments (i.e.the, the child pedsQLTM, the parent pedsQLTM) reported for child HrQoL. Which confirms, subscales which supposed to measure the same “trait” in the two different instruments had a strong correlation with each other (convergent validity), whereas subscales which supposed to measure different “trait” had a weak correlation with each other (discriminatory validity) as an initial hypothesis.
Similar to the original US English PedsQLTM,26 the study has confirmed a strong intercorrelation between the PedsQLTM Generic Core Scales and PedsQLTM 3.0 diabetes modules. Which implies the instrument had good construct validity; based on the initial hypothesis that a higher score in disease symptom (fewer symptom), a higher score in treatment barriers, and treatment adherence (fewer problems with barriers and adherence), and higher scores on the worry and communication scales (less worry and better communication, respectively) could be correlated with a higher Generic core scale score.
The external discriminant validity of the PedsQL™4.0 GCS and PedsQL™3.0 Diabetes Module were compared across gender, age, duration with diabetes, and glycemic level. There were significant mean differences across age, sex, and Glycemic level in total PedsQL™4.0 GC Scores. Similar to the Italian version10 a mean difference in total PedsQL™3.0 DM was observed across the glycemic level.
Limitation
The main limitation of the study was; Test-retest reliability has not reported. The study has no comparable group (healthy children). The study is age-restricted; it was not addressed the psychometric properties of both PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM for toddlers (aged 2–4) and young children (aged 5–7). The study will recommend this limitation to consider in future investigations.
Conclusion
The Amharic version of PedsQLTM 4.0 GCS and PedsQLTM 3.0 DM was a valid and reliable instrument for assessing children and adolescents’ health-related quality of life with diabetes.
Abbreviation
PedsQLTM 4.0 GCS, Pediatrics Quality of Life Inventory Version 4.0 Generic Core Scale; HrQoL, Health-Related Quality of Life; PedsQLTM 3.0 DM, Pediatrics Quality of Life Inventory version 3.0 Diabetes module; T1DM, Type 1 Diabetes.
Data Sharing Statement
When the ethics statement was obtained from the Addis Ababa Health Bureau, we have agreed and signed not to publish the raw data retrieved from the patients. However, the datasets collected and analyzed for the current study are available from the corresponding author and can be obtained at a reasonable request.
Ethical Considerations
Ethical clearance was obtained from the Ethical review committee of the college of health science at Mizan Tepi University. An official letter of cooperation was written to the Addis Ababa health bureau and each health institution. After explaining the purpose of the study, Written informed assents and consents were obtained by minors aged ≥12 years and parents, respectively. Participants were also informed that participation was voluntary and that they can withdraw at any time if they are not comfortable with the questionnaire. Personal identifiers were not included in the written questionnaires to ensure participants’ confidentiality. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We would like to pass our gratitude to the Mizan Tepi University for the approval of ethical clearance and technical support. Our heartfelt goes to Dr. Varni for his permission to translate the PedsQL™ to Ethiopian Amharic. Our thank goes to Iliana Petkova and Magdalena Heluszka from Mapi Research Trust Institute; they help us as a ladder for communication and announcing all decision has passed by the author, and for their contribution in sending all needed documents. Finally, we thank you to our data collector and participants for their cooperative and time.
Author Contributions
All authors contributed to data analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Abdul-Rasoul M, AlOtaibi F, Abdulla A, Rahme Z, AlShawaf F. Quality of life of children and adolescents with type 1 diabetes in Kuwait. Med Princ Pract. 2013;22(4):379–384. doi:10.1159/000347052
2. Abdul-Rasoul M, AlOtaibi F, AlMahdi M, AlKandari H. Reliability and validity of the arabic version of the Pedsql Tm 4.0 generic ore scales and Pedsql Tm 3.0 diabetes module. 2012.
3. Abolfotouh MA, Kamal MM, El-Bourgy MD, Mohamed SG. Quality of life and glycemic control in adolescents with type 1 diabetes and the impact of an education intervention. Int J Gen Med. 2011;4:141. doi:10.2147/IJGM.S16951
4. Brown A, Aguiree F, Cho NH. et al. IDF diabetes atlas. 2013.
5. Alemayehu T, Shimelis D, Abebe W. Prevalence of diabetes mellitus in 7–12 years old school children presenting to department of pediatrics and child health, Tikur Anbessa Specialized Teaching Hospital, Addis Ababa, Ethiopia. Ethiop Med J. 2017;55(1):43–47.
6. Ali B, Abdelhakm AA, Mohamed M, Tawfik NK. Quality of life in children with type i diabetes mellitus in Minia Governorate, Egypt: relationship with mood and family attitudes. Pediatr Diabetes. 2015;16:142.
7. Alvarado-Martel D, Velasco R, Sánchez-Hernández RM, Carrillo A, Nóvoa FJ, Wägner AM. Quality of life and type 1 diabetes: a study assessing patients’ perceptions and self-management needs. Patient Prefer Adherence. 2015;9:1315. doi:10.2147/PPA.S87310
8. American Diabetes Association. 12. Children and adolescents: standards of medical care in diabetes—2018. Diabetes Care. 2018;41(Supplement 1):S126–S36. doi:10.2337/dc18-S012
9. Baş VN, Bideci A, Yeşilkaya E, Soysal AŞ, Çamurdan O, Cinaz P. Evaluation of factors affecting quality of life in children with type 1 diabetes mellitus. J Diabetes Metab. 2011;2(08):154–158. doi:10.4172/2155-6156.1000154
10. d’Annunzio G, Gialetti S, Carducci C. Italian translation, cultural adaptation and validation of the Pedsql™ 3.0 diabetes module questionnaire in children with type 1 diabetes and their parents. Health Qual Life Outcomes. 2014;12(1):115. doi:10.1186/s12955-014-0115-2
11. Delamater AM, Maartje DW, McDarby V, Malik J, Acerini CL. Psychological care of children and adolescents with type 1 diabetes. Pediatr Diabetes. 2014;15(S20):232–244. doi:10.1111/pedi.12191
12. Garcia LF, Della Manna T, Passone CD, de Oliveira LS. Translation and validation of pediatric quality of life inventory™ 3.0 diabetes module (Pedsql™ 3.0 diabetes module) in Brazil-Portuguese language. J Pediatr (Rio J). 94;2018.
13. Internasional Diabetes Federation. Idf Diabetes Atlas International Diabetes Federation. Brussels, Belgium; 2017.
14. Ismail TA, Gadallah MA, Aty NS. Health related quality of life among children with type i diabetes, Assiut City, Egypt. J Nurs Educ Pract. 2017;10:73.
15. Gkoltsiou K, Dimitrakaki C, Tzavara C, Papaevangelou V, Varni JW, Tountas Y. Measuring health-related quality of life in Greek children: psychometric properties of the Greek version of the pediatric quality of life inventory Tm 4.0 generic core scales. Qual Life Res. 2008;17(2):299–305. doi:10.1007/s11136-007-9294-1
16. Whoqol Group. The World Health Organization quality of life assessment (Whoqol): position paper from the World Health Organization. Soc Sci Med. 1995;41(10):1403–1409. doi:10.1016/0277-9536(95)00112-K
17. Ingersoll GM, Marrero DG. A modified quality-of-life measure for youths: psychometric properties. Diabetes Educ. 1991;17(2):114–118. doi:10.1177/014572179101700219
18. Jafari P, Forouzandeh E, Bagheri Z, Karamizadeh Z, Shalileh K. Health related quality of life of iranian children with type 1 diabetes: reliability and validity of the persian version of the Pedsql™ generic core scales and diabetes module. Health Qual Life Outcomes. 2011;9(1):104. doi:10.1186/1477-7525-9-104
19. Klatchoian DA, Len CA, Terreri MTRA. Quality of life of children and adolescents from São Paulo: reliability and validity of the brazilian version of the pediatric quality of life inventorytm version 4.0 generic core scales. J Pediatr (Rio J). 2008;84(4):308–315. doi:10.1590/S0021-75572008000400005
20. Lukacs A, Varga B, Barótfi S, Kiss-Tóth E, Barkai L. Health-related quality of life of youths with type 1 diabetes: reliability and validity of the Hungarian version of the Pedsql 3.0 diabetes module. J Diabetes Metab. 2012;3(04):2–6. doi:10.4172/2155-6156.1000191
21. Mills SA, Hofman PL, Jiang Y. Health-related quality of life of Taranaki children with type 1 diabetes. Ethnicity. 2015;16:
22. Özyazıcıoğlu N, Avdal EÜ, Sağlam H. A determination of the quality of life of children and adolescents with type 1 diabetes and their parents. Int J Nurs Sci. 2017;4(2):94–98. doi:10.1016/j.ijnss.2017.01.008
23. Reinfjell T, Diseth TH, Veenstra M, Vikan A. Measuring health-related quality of life in young adolescents: reliability and validity in the Norwegian version of the pediatric quality of life inventory™ 4.0 (Pedsql) generic core scales. Health Qual Life Outcomes. 2006;4(1):61. doi:10.1186/1477-7525-4-61
24. Soltész G. Worldwide childhood type 1 diabetes epidemiology. Endocrinol Nutr. 2009;56:53–55. doi:10.1016/S1575-0922(09)73520-X
25. Tahirović H, Toromanović A, Tahirović E, Begić H, Varni JW. Health-related quality of life and metabolic control in children with type 1 diabetes mellitus in Bosnia and Herzegovina. Coll Antropol. 2012;36(1):117–121.
26. Varni JW, Burwinkle TM, Jacobs JR, Gottschalk M, Kaufman F, Jones KL. The Pedsql™ in type 1 and type 2 diabetes: reliability and validity of the pediatric quality of life inventory™ generic core scales and type 1 diabetes module. Diabetes Care. 2003;26(3):631–637. doi:10.2337/diacare.26.3.631
27. Varni JW, Burwinkle TM, Lane MM. Health-related quality of life measurement in pediatric clinical practice: an appraisal and precept for future research and application. Health Qual Life Outcomes. 2005;3(1):1–9. doi:10.1186/1477-7525-3-34
28. Varni JW, Burwinkle TM, Seid M, Skarr D. The Pedsql™* 4.0 as a pediatric population health measure: feasibility, reliability, and validity. Acad Pediatr. 2003;3(6):329–341. doi:10.1367/1539-4409(2003)003<0329:TPAAPP>2.0.CO;2
29. Varni JW, Seid M, Kurtin PS. Pedsql™ 4.0: reliability and validity of the pediatric quality of life inventory™ version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800–812. doi:10.1097/00005650-200108000-00006
30. Varni JW, Seid M, Rode CA. The Pedsql™: measurement model for the pediatric quality of life inventory. Med Care. 1999;37(2):126–139. doi:10.1097/00005650-199902000-00003
31. World Health Organization. Preamble to the constitution of the World Health Organization as adopted by international health conference. New York,19–22 June,1946; Signed on 22 July 1946 by the representatives of 16 state and entered into force 7 April 1948. 1948.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.