")
Back to Journals » International Journal of Women's Health » Volume 13
Reliability and Dimensionality of EPREVO (“Experiencias de Parto Relacionadas a Violencia Obstétrica”): Development of a New Instrument, Ecuador
Authors Fors M , Falcon K, Brandão T, Vaca A, Cañadas S , Viada González CE
Received 9 February 2021
Accepted for publication 4 May 2021
Published 16 June 2021 Volume 2021:13 Pages 569—577
DOI https://doi.org/10.2147/IJWH.S305741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Martha Fors,1 Kirsten Falcon,1 Thais Brandão,1 Ana Vaca,1 Sofia Cañadas,1 Carmen Elena Viada González2
1Universidad de Las Américas, Quito, Pichincha, Ecuador; 2Centro de Inmunología Molecular, Havana City, Cuba
Correspondence: Kirsten Falcon
Universidad de Las Américas Ecuador, Quito, Pichincha, Ecuador
Email [email protected]
Background: A new instrument called EPREVO has been developed to measure obstetric violence in Ecuador and the objective of this work is to validate its reliability and structural dimensionality.
Methods: Using confirmatory factor analysis (CFA) with a tetrachoric correlation approach. We examined the factor structure of EPREVO, a Spanish instrument to measure obstetric violence. Kuder Richardson values were used to assess the internal consistency of the scale and dimensionality was confirmed with confirmatory factor analysis.
Results: Confirmatory factor analysis supported a 3-factor solution. Most item-to-factor-correlations presented moderate to strong magnitude. Total Kuder Richardson was 0.87, while for the three factors were 0.23, 0.47 and 0.94, respectively. The model’s goodness-of-fit indexes were satisfactory (χ 2 = 1458.83; χ 2/g.l = 2.60, p < 0.001; NNFI = 0.90; RMSEA = 0.09); most of the factor loads were greater than 0.30. A confirmatory factor analysis suggested a 3-dimensional structure of EPREVO.
Conclusion: The scale’s factor structure presented satisfactory validity and reliability results, except for one factor. The 30 items scale could potentially be used as an instrument for assessing obstetric violence in different healthcare settings.
Keywords: internal consistency, obstetric violence
Background
Obstetric violence is considered a violation of the rights to equality, non-discrimination, information, integrity, health, and reproductive autonomy of women. It occurs in both public and private medical practice during pregnancy, delivery, and postpartum care1.
There is increasing evidence of a group of disrespectful and violent medical practices experienced by women in some obstetric care centers at the hands of healthcare providers, especially during childbirth and the postpartum period.2,3
There is a growing global commitment to address this challenge, that has been supported by policy statements from the World Health Organization (WHO) which issued a declaration on the prevention and elimination of disrespect treatment and abuse during delivery in health units, calling the phenomenon “an important public health and human rights issue,” the WHO urged governments and development partners to investigate, recognize and correct maternity care.4
Medicalization and pathologizing abuse of natural birth processes have been identified as obstetric violence patterns. Indigenous women and women who live in rural areas are particularly vulnerable to this kind of abuse.5,6
Latin America, where many countries have relatively new human rights-based constitutions and law bodies, has taken the lead in creating legal structures to address this issue. Venezuela was one of the first jurisdictions to create a legal right of action that recognizes obstetric violence. Specifically, it is recognized as a form of gender violence as part of the Organic Law of the Right of Women to a Life Free of Violence.7
In Ecuador, there are demonstrations of obstetric violence in public and private health units, including indiscriminate vaginal touching, caesarean sections without medical reason, routine episiotomies, separation of the newborn from his mother, not offering help to start maternal breastfeeding, among others.8,9 The high number of obstetric violence in the country constitutes a serious public health subject that implies individual consequences in the short and long term, these are not only physical but also psychological and social.8,10
In an investigation in Quito9 where it was reported that 120 women who gave birth for the first time, 62 (51.7%) had an episiotomy. In the second stage of labor, the Kristeller maneuver was performed in 49 (19.4%) of 252 women. Overall, 196 (50.5%) women reported that they were not allowed to participate in early attachment, and 135 (34.8%) reported that they did not receive support for initiating breastfeeding.
In the National Survey on Family Relations and Gender Violence Against Women, ENVIGMU 2019, carried out in Ecuador, the section on obstetric violence questions is included for the first time and it is mentioned that this type of gender violence was not previously considered, due to that this type of violence was “naturalized” or normalized.11
Disrespectful and abusive treatment of women in labor might be the result of weaknesses in the health system, including what health providers learn in training and reinforcement at work, as well as various types of prejudice in a society.
These are the reasons why this research team decided to design Experiencias de Parto Relacionadas a Violencia Obstétrica (EPREVO) an instrument to measure obstetric violence in healthcare settings in Ecuador. This questionnaire was developed by a group of medical specialists and nurses and this research is part of the validation process that is undergoing this instrument. The aim of the study is to assess the internal consistency (reliability) and the structural dimensionality of EPREVO.
Methods
Type of Study, Setting and Participants
Observational, cross-sectional validation study. Quantitative, methodological study conducted with a sample of 405 participants from public health institutions of Quito, Ecuador. Women over the age of 18 years old who granted their informed consent to participate were included in the study. All of them were evaluated following a standard protocol consisting in the review of inclusion and exclusion criteria, the process of obtain de consent to participate and the electronic questionnaire application. Information was collected from October 2018 to March 2019. Participant women received assistance in three different types of care setting of the country (public, private and social security).
Ethics
After receiving written informed consent, participants were informed about the aims, content and duration of the study by research team. They were informed that participation was voluntary, and completion of the study was anonymous. This study was approved by the Ethics committee from the Universidad San Francisco de Quito. We followed STROBE guidelines for the report of this study and this study was conducted in accordance with the Declaration of Helsinki.
Demographic Variables
The sociodemographic variables that were considered were school education, ethnic group, care setting and type of birth.
Measurement Instrument
The questionnaire was designed for this specific study. Obstetric violence was assessed using EPREVO a Spanish questionnaire of 36 items developed by the authors of this paper. The terms chosen for the development of this questionnaire were based on the criteria of Bowser and Hill (2010) who structured seven categories to measure obstetric violence: (1) physical abuse, (2) non-consented care, (3) non-confidential care, (4) non-dignified care (including verbal abuse), (5) discrimination based on specific patient attributes, (6) abandonment of care, and (7) detention in facilities. The analyses performed by Jewkes and Pen-Kekana (2015) were also taken into account to set the concepts the authors used in EPREVO; these authors problematize and deepen the way of measuring this phenomenon, suggesting grouping them into just 2 dimensions: intentional use of violence — physical abuse and structural disrespect.
EPREVO is based on 3 concepts:
1. Structural negligence: This factor measures the procedures carried out by health personnel who are inserted in an institutional structure that does not meet scientific evidence including physical violence, institutional and intentional oversights (by health personnel). It is comprised of 13 items.
2. Right to information: This factor measures the rights of the women to have information about all the procedures that are carried out with her or her baby. It is comprised of 9 items.
3. Right to presence/Supportive care: This factor measures the woman’s right to be accompanied during labor, delivery and postpartum. And the right of both (mother and newborn) to have immediate attachment after birth without complications. It is comprised of 8 items.
This is an instrument validation study measuring the reliability and structural dimensionality of EPREVO items. Most of the items were rated by respondents on a 2-point scale (0 = no, 1 = yes).
Sample Size
A sample of 405 women was evaluated to assess the reliability and structural dimensionality of EPREVO questionnaire. The sample met the criteria by Cochran formula more than 10 times of questionnaire items.12 A randomized clustered sampling was carried out to choose the participants healthcare institutes.
Statistical Analysis
To estimate the internal consistency of the scores, Kuder–Richardson coefficient (KR-20) was calculated on the sample of 405 participants. The values of this indicator above 0.5 show reasonable convergence and it was used as the criteria in the current study.
Structural dimensionality was performed via a confirmatory factor analysis (CFA using tetrachoric correlations). CFA was conducted to determine if the data fit the proposed 3-factor model proposed by the research team of the current study. CFA was performed using Robust Weighted Least Squares (WLSMV) as the extraction method and with a geomin rotation. This will estimate a tetrachoric correlation matrix for factor extraction. This method was chosen because of the binary format of the items and according to several recommendations for factor analyses in dichotomous variables.13 Factor solutions ranging from one to three factors were examined. The number of retained factors was determined by inspection of eigenvalues considering eigenvalues over one14 Kaiser–Meyer–Olkin (KMO) index and Bartlett’s sphericity test (BTS) were used to assess how adequate the sample size was by CFA. The values expected for the KMO test are between 0.5 and 1 and p < 00.5 for the BTS.15 Item correlation less than 0.30 was considered weak with poor clinical applicability; between 0.30 and 0.50 was considered moderate; and greater than 0.50 was considered strong (Weinberg, and Abramowitz 2008).
Chi-square test (χ2) was used to verify the model’s goodness of fit with significance greater than 0.05. Root Mean Square Error of Approximation (RMSEA), with acceptable values equal to or lower than 0.08 and Bentler and Bonett’s Non-normed Fit Index (NNFI) were calculated with acceptable values equal to or greater than 0.90.16 Commonality coefficients were also calculated, values above 0.6 were considered satisfactory17 SPSS version 24.0 and Stata version 14.2 were used to perform data analysis.
Results
Socio-Demographic Characteristics
The sample was composed of 405 women: all of them were young adults (aged 18–35 years), age mean of 26.5 with and standard deviation of 4.9. The 62.2% of participants had secondary education (nine years of schooling), and most of the participants identified themselves as Mestizas (82%). Half of them gave birth at a public health institution and the 60% had a vaginal delivery. Table 1 presents their socio-demographic characteristics of the sample.
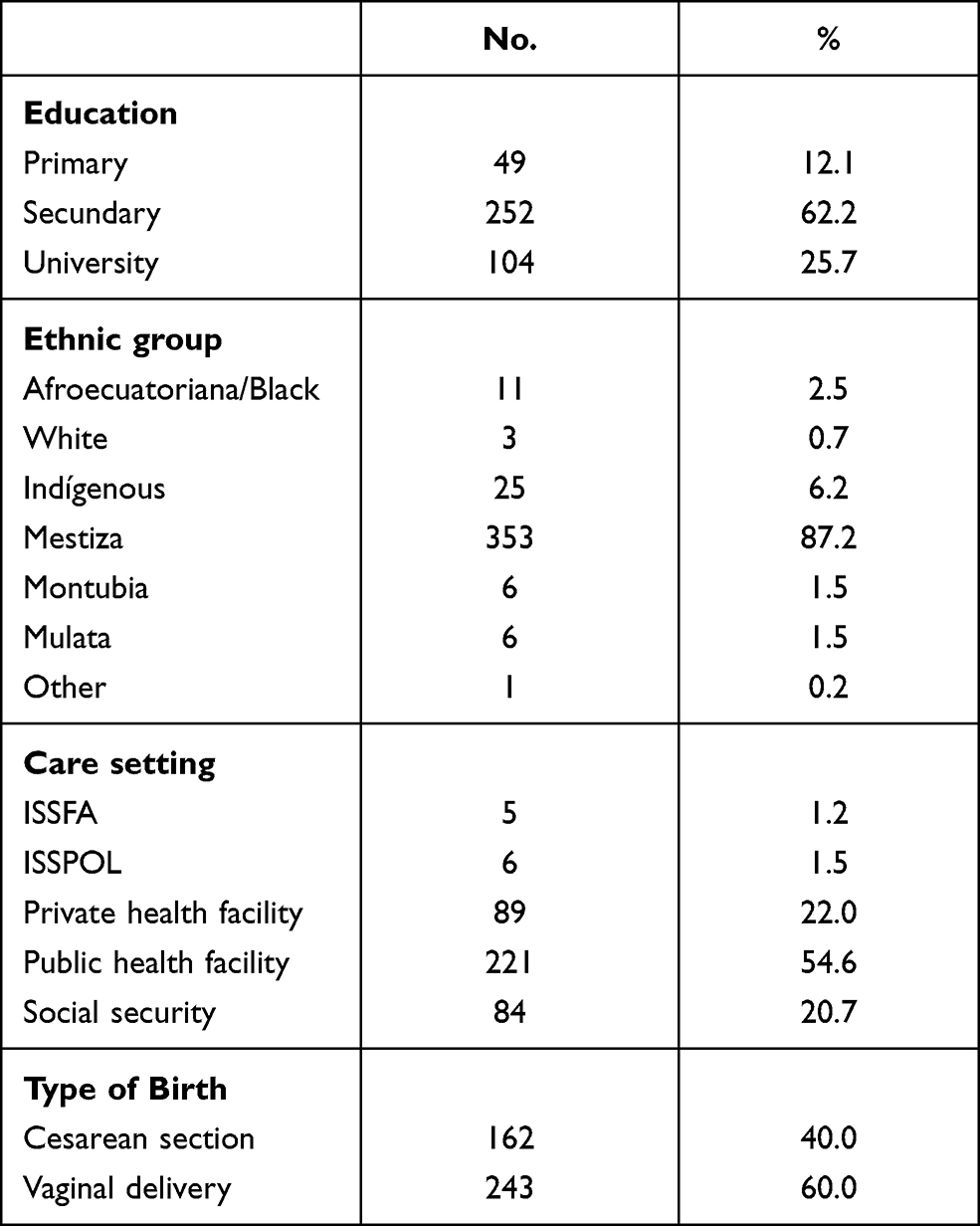 |
Table 1 Socio-Demographic Characteristics of Women Included |
Internal Consistency (Reliability)
Analysis of item reliability revealed satisfactory internal consistency for the EPREVO questionnaire. For defining the reliability of the current study, Kuder Richardson 20 (KR-20) was used. Total Kuder Richardson value was of 0.82, which reveals good internal consistency, for the first factor (Structural negligence) KR-20 was 0.71, for the second (Right to information) it was 0.84 and for the third (Rights to presence/Supportive care) it was of 0.33. The Corrected Item-Total Correlation was low (<0.3) in 14 items. From 0.30 to 0.50, we had 9 items (moderate) and 13 items had strong correlations (more than 0.50). (Table 2)
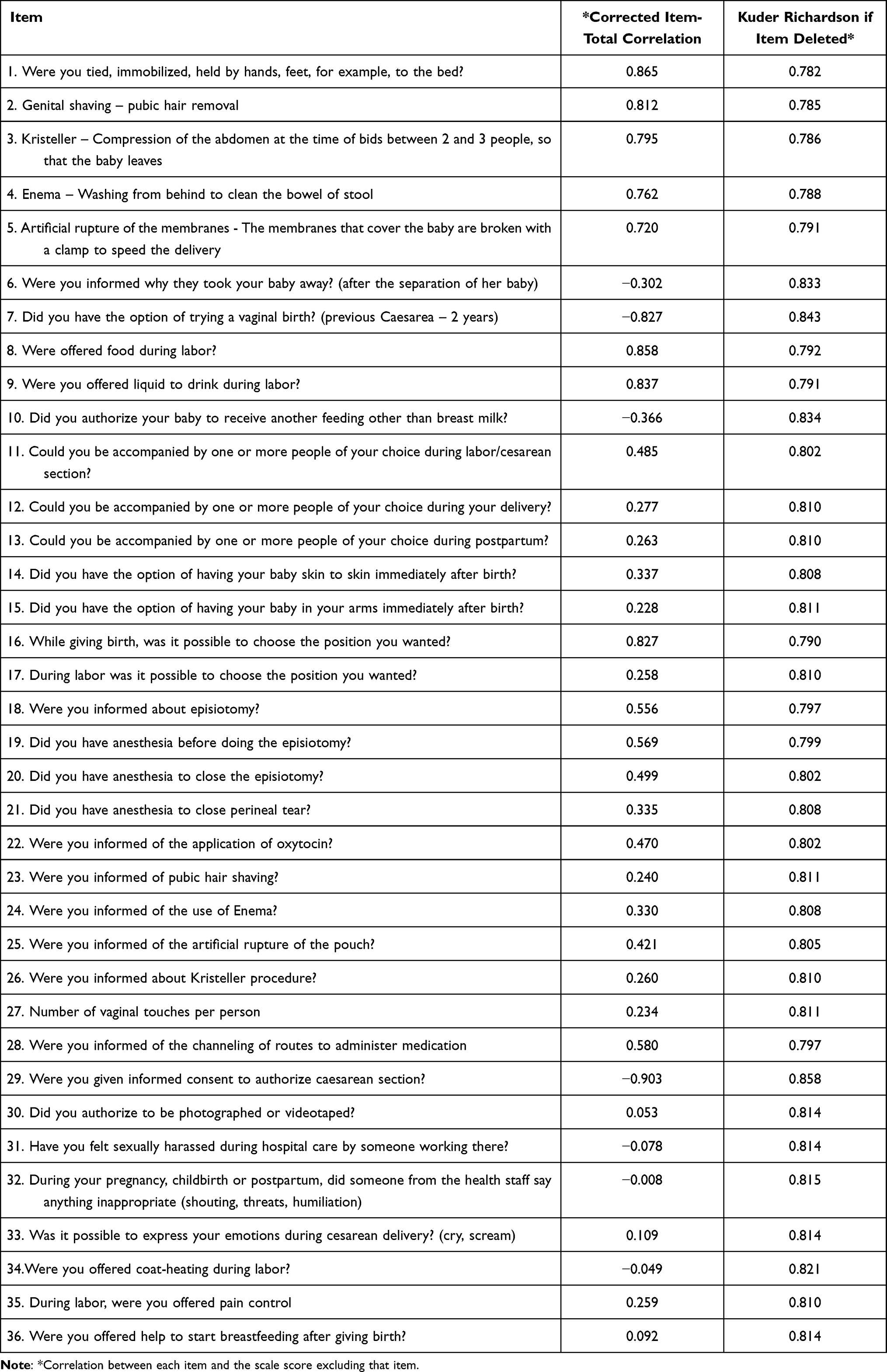 |
Table 2 Kuder Richardson 20. Item Analysis |
Structural Dimensionality. Confirmatory Factor Analysis
Bartlett’s test for sphericity reported a significant Chi-square value of with p=0.001, rejecting the null hypothesis that the data correlation matrix was an identity matrix while Kaiser–Meyer–Olkin (KMO), measure of sampling adequacy for the factor analysis was 0.85 within the established limits. These results show good fit of the data matrix to the factor analysis.
CFA was performed upon 36 items and showed that almost all items were distinctively and significantly loaded into respective three factors or dimensions. Factor analysis with cumulative explained variance of 47.7%. Of the 36-initial scale items, 30 had factor loadings of 0.30 or greater. Items were allocated to the factor with the highest load. In this study, we detected items that did not seem to work the same way as the rest, so we suggest deleting six items of the initial scale since they did not weight highly in any of three factors (A criterion was used, and items whose weight was lower than 0.30 were eliminated). The overall fitting results were χ2 = 1458.83; χ2/g.l = 2.60. p < 0.000; RMSEA = 0.06 and NNFI = 0.90. These results show the model’s satisfactory fitting based on adequacy criteria. The presentation of factor loads, and communalities was made according to domains we established (Table 3).
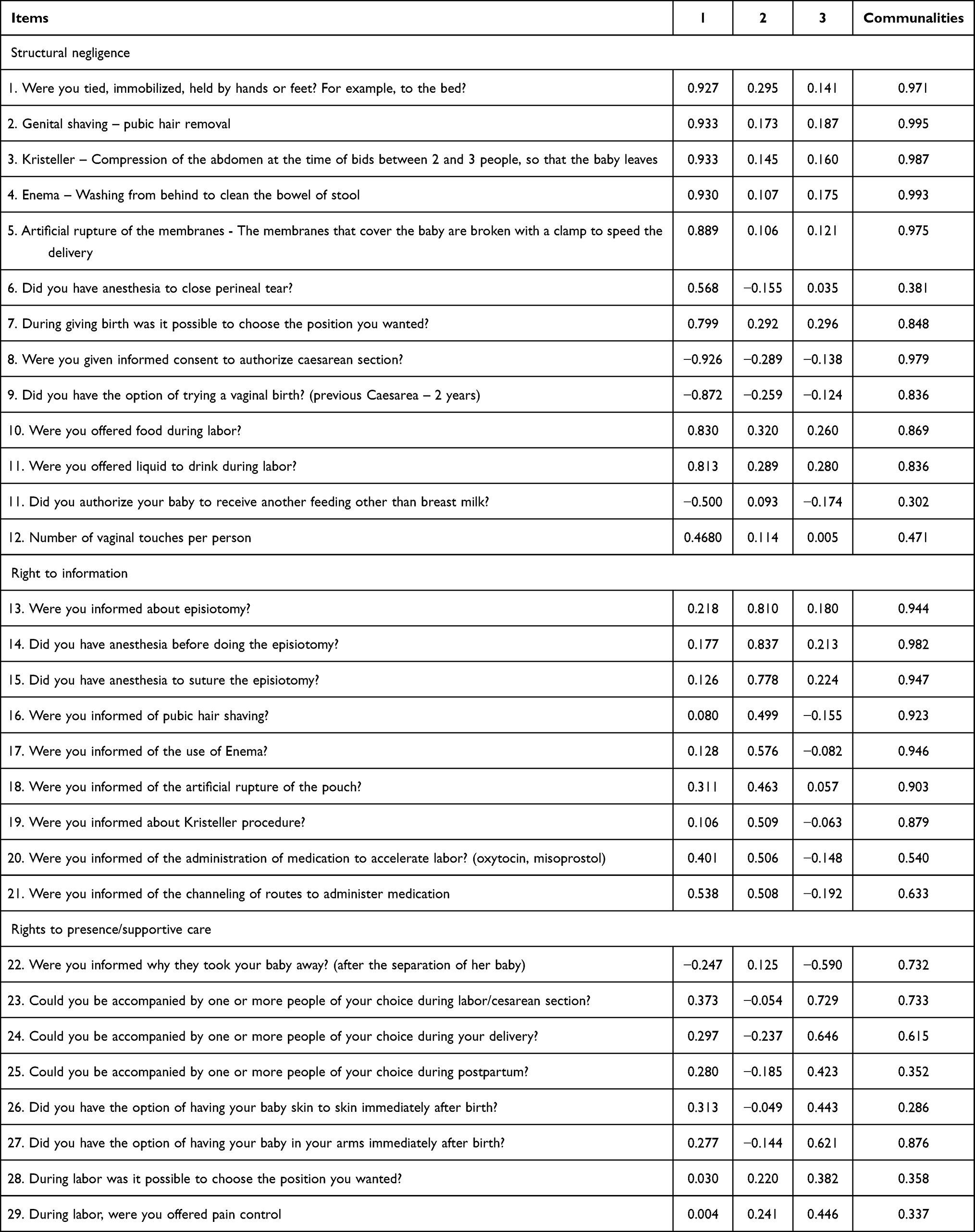 |
Table 3 Loading Factors in Confirmatory Factor Analysis. Rotated Tetrachoric Matrix |
The scree plot resulted in three dimensions that explained 47.7% of the total variance, while each presented eigenvalue greater than 1 (11.04, 3.66 and 1.97) and explained 31.55%, 10.47% and 5.63% of the scale’s variance, respectively. Extracted components number as determined by the scree plot, percentage of variance explained by each one and number of eigenvalues over one. The analysis suggests retaining 3 factors but with a first factor explaining a major part of the variance. Figure 1 showed a clear inflection after the first factor.
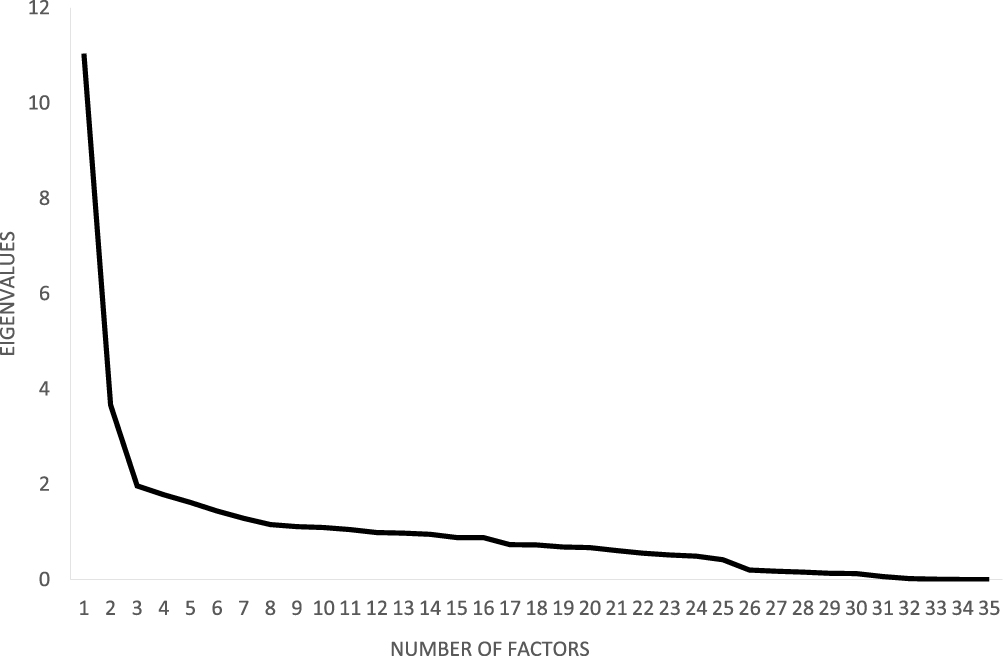 |
Figure 1 Factor analysis of the version of EPREVO: scree plot with eigenvalues indicating a 3-factor model. |
Discussion
The first version of Experiencias de Parto Relacionadas a Violencia Obstétrica (EPREVO) was developed by a group of researchers, who belonged to Universidad de Las Américas, Quito, Ecuador.
A standard approach to defining and measuring mistreatment of women during childbirth, through the development of validated measurement tools, would therefore permit standardized comparisons of prevalence data across settings and over time.18
This study has been conducted to verify internal consistency or reliability of the scale’s items and the factor structure to meet criteria concerning structural dimensionality with a sample of 405 women. We are reporting a structure that obtained excellent goodness-of-fit index after excluding six items and describing and listing three factors. This questionnaire is composed by 30 items that assess three factors: Structural negligence, Right to information and Right to presence/Supportive care.
We structured our questionnaire with the three categories presented, including the right to information as an important and already worked component of obstetric violence. Different terms have been used to describe the mistreatment during childbirth, such as obstetric violence, disrespect and abuse, and respectful maternity care.18
We also considered internationally researched models in the field of disrespect and abuse.18,19 Despite the lack of international consensus on the terminology of this phenomenon discussed by these authors, we prefer to use obstetric violence, as it is used mostly in Latin America since Venezuela enacted the first official law (2007).
In Meijer et al, it is mentioned that the World Health Organization (WHO) and the International Federation of Gynecology and Obstetrics (FIGO) suggested the community participation to protect the right to be informed and the use of informational material as feasible interventions that guarantee the rights of women during the childbirth process. In Ecuador, this right is also regulated in protection laws for public and private institutions.11
There are many ways to identify and measure obstetric violence but we identify these factors as those that can summarize three major user rights abuses within the health system: information and support, which are the rights of any patient and neglect of the institution, which is a structural problem that also includes improper and voluntary actions (bad practices) of health personnel.
KR20 was high (KR20=0.80) for the complete instrument. Validation study findings showed that Structural negligence and Right to information (KR20=0.71 and KR20=0.84) had an excellent internal consistency indicating that the items consistently measure the same latent variable and are thus reliable, while domain Right to presence/Supportive care had a KR20 of 0.33. This comparatively low internal consistency score for this dimension maybe due to small number of items of the construct. This was acceptable and was considered a good test as KR20 tends to result in more conservative estimates than Cronbach’s alpha.20
Most correlations among the items of the 3 factors were from moderate magnitude (r = 0.30 to r = 0.50) to strong (more than 0.50) according to Ajzen and Fishbein.21
Fit statistics evaluated suggested adequacy of the fit of a three-dimension model. Values of RMSEA and NNFI were considered as acceptable providing confirmation that questions grouped together in the EPREVO questionnaire on conceptual grounds are empirically related.16
The p-value of the chi-square test of fit was less than 0.050, which indicates that the observed covariance matrix is statistically significantly different from the expected matrix predicted by the hypothesized model we used.
According to Kubinger,13 tetrachoric correlations would lead to more content valid results in case of dichotomous variables because factor analysis is based on Pearson correlations which require interval scaled variables.
EPREVO questionnaire includes concepts relating to obstetric violence and all the factors have been identified as factors contributing to assess it. The existence of violations of this type of care, as well as the invisibility of this aspect of violence against women is a significant impediment to the patient’s safety, in any institution that provides childbirth care. Likewise, as obstetric violence is a type of gender violence, it is subject to the same variables of inequality and vulnerability towards women, such as socioeconomic factors, age, educational level and sociodemographic aspects analyzed in EPREVO.
Our results suggest a valid measure of the reliability and dimensionality of EPREVO and that three dimension structure fits the data. Nevertheless, there is a need for further investigations of the psychometric properties of the scale, possibly including different age groups and population and a balance in the number of items for each factor.
Conclusions
To date, an Ecuadorian instrument to assess obstetric violence does not exist. The results of this study provide evidence that EPREVO is a reliable and valid instrument for assessing obstetric violence in women. Dimensionality by means of factor analysis indicated that the grouping of items from this questionnaire is three factors. In general, the three-factor models presented satisfactory fit indices, good reliability, and convergent and discriminant validity. It is recommended that further be undertaken in order to confirm this structural model proposed.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank all the participants who participated in the study and Universidad de Las Américas for its financial support to perform this investigation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.”.
Funding
Universidad de Las Américas funded this research.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Lalonde AB, Miller S. Mother-baby friendly birthing facilities initiative. Int J Gynecol Obstet. 2014;128(2):93–94. doi:10.1016/j.ijgo.2014.11.002
2. D´Oliveira AFPL, Diniz SG, Schraiber LB. Violence against women in health-care institutions: an emerging problem. Lancet. 2002;359(9318):1681–1685. doi:10.1016/S0140-6736(02)08592-6
3. Bohren MA, Vogel JP, Hunter EC, et al. The mistreatment of women during childbirth in health facilities globally: a mixed-methods systematic review. PLoS Med. 2015;12(6):1–32. doi:10.1371/journal.pmed.1001847
4. World Health Organization. The prevention and elimination of disrespect and abuse during facility-based childbirth: WHO statement. World Heal Organ. 2015:4. Available from: https://apps.who.int/iris/bitstream/handle/10665/134588/WHO_RHR_14.23_cze.pdf.
5. Castro R, Frías SM. Obstetric violence in Mexico: results from a 2016 national household survey. Violence Against Women. 2019;26(6–7):555–572. doi:10.1177/1077801219836732
6. Goli S, Ganguly D, Chakravorty S, Rammohan A. A framework to study labor room violence in a resource-poor setting. Framew Study Labor Room Violence Resour Setting. 2020. doi:10.4135/9781529743609
7. Pérez D’Gregorio R. Obstetric violence: a new legal term introduced in Venezuela. Int J Gynecol Obstet. 2010;111(3):201–202. doi:10.1016/j.ijgo.2010.09.002
8. Meijer M, Brandão T, Cañadas S, Falcon K. Components of obstetric violence in health facilities in Quito, Ecuador: a descriptive study on information, accompaniment, and position during childbirth. Int J Gynecol Obstet. 2019;355–360. doi:10.1002/ijgo.13075
9. Brandão T, Cañadas S, Galvis A, Moreno M, Meijer M, Falcon K. Childbirth experiences related to obstetric violence in public health units in Quito, Ecuador. Int J Gynecol Obstet. 2018:1–5. DOI:10.1002/ijgo.12625
10. OMS. Recomendaciones de la OMS Para los cuidados durante el parto, Transformar la atención a mujeres y neonatos para. 2018:1–8. Available from: http://apps.who.int/iris/bitstream/handle/10665/272435/WHO-RHR-18.12-spa.pdf?ua=1.
11. Ministerio de Salud Pública del Ecuador. Norma Técnica Atención Víctimas de Violencia de Género y Graves Violaciones a los Derechos Humanos. 2019. Available from: https://aplicaciones.msp.gob.ec/salud/archivosdigitales/documentosDirecciones/dnn/archivos/AC-00040-2019%20SEPT%2010.pdf .
12. Cochran WG, Wiley J, York N, et al. Sampling Technique s.
13. Kubinger KD. On artifi cial results due to using factor analysis for dichotomous variables. Psychol Sci. 2003;45(1):106–110.
14. Patil VH, Singh SN, Mishra S, Todd Donavan D. Efficient theory development and factor retention criteria: abandon the “eigenvalue greater than one” criterion. J Bus Res. 2008;61(2):162–170. doi:10.1016/j.jbusres.2007.05.008
15. Kaiser HF. An index of factorial simplicity. Psychometrika. 1974;39(1):31–36. doi:10.1007/BF02291575
16. Little T Longitudinal structural equation modeling; 2013. Available from: https://www.guilford.com/books/Longitudinal-Structural-Equation-Modeling/Todd-Little/9781462510160.
17. Field A. Discovering Statistics Using SPSS ISM. London, England: Introducing Statistical Methods Series; 2009.
18. Bohren MA, Vogel JP, Fawole B, et al. Methodological development of tools to measure how women are treated during facility-based childbirth in four countries: labor observation and community survey 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Med Res Methodol. 2018;18(1):1–15. doi:10.1186/s12874-018-0603-x
19. Sando D, Abuya T, Asefa A, et al. Methods used in prevalence studies of disrespect and abuse during facility based childbirth: lessons learned Prof. Suellen Miller. Reprod Health. 2017;14(1):1–18. doi:10.1186/s12978-017-0389-z
20. Gadermann AM, Guhn M, Zumbo BD. Estimating ordinal reliability for likert-type and ordinal item response data: a conceptual, empirical, and practical guide. Pract Assessment, Res Eval. 2012;17(3):1–13.
21. Ajzen I, Fishbein M. Attitudes and normative beliefs as factors influencing behavioral intentions. J Pers Soc Psychol. 1972;21(1):1–9. doi:10.1037/h0031930
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.