")
Back to Journals » International Journal of General Medicine » Volume 15
Relationship of the Triglyceride-Glucose Index with Subclinical White Matter Hypersensitivities of Presumed Vascular Origin Among Community-Dwelling Koreans
Authors Jung DH , Park B , Lee YJ
Received 8 November 2021
Accepted for publication 7 January 2022
Published 14 January 2022 Volume 2022:15 Pages 603—608
DOI https://doi.org/10.2147/IJGM.S346997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dong-Hyuk Jung, Byoungjin Park, Yong-Jae Lee
Department of Family Medicine, Yonsei University College of Medicine, Seoul, 03722, Republic of Korea
Correspondence: Yong-Jae Lee, Department of Family Medicine, Yonsei University College of Medicine, Gangnam Severance Hospital, 211 Eonju-ro, Gangnam-gu, Seoul, 06273, Republic of Korea, Tel +82-2-2019-2630, Fax +82-2-3463-3882, Email [email protected]
Dong-Hyuk Jung, Department of Family Medicine, Yonsei University College of Medicine, Yongin Severance Hospital, 363 Dongbaekjukjeondae-ro, Giheung-gu, Yongin-si, Gyeonggi-do, 16995, Republic of Korea, Tel +82-31-5189-8762, Fax +82-31-5189-8809, Email [email protected]
Purpose: The triglyceride-glucose (TyG) index, a widely accessible measure, has been a surrogate indicator of peripheral insulin resistance, and its clinical importance continues to grow in East Asia. We hypothesized that the TyG index is relevant to subclinical white matter hypersensitivities (WMHs) of presumed vascular origin among community-dwelling Koreans.
Methods: We investigated the relationship between the TyG index and WMHs on brain magnetic resonance imaging scans in 2417 Koreans over 45 years of age without a history of cancer, stroke, or ischemic heart disease. The study population was divided into four groups according to the TyG index quartiles. Using multiple logistic regression analysis, we assessed the odds ratios (ORs) and 95% confidence intervals (95% CIs) for WMHs across the TyG index quartiles.
Results: The prevalence of WMHs was significantly higher in the fourth TyG index quartile, with an overall rate of 9.3%. After adjusting for potential confounding variables, the ORs of WMHs for the TyG index quartiles were 1.00, 1.47 (95% CI, 0.91– 2.40), 1.76 (95% CI, 1.05– 2.97), and 6.79 (95% CI, 3.85– 1.54), respectively.
Conclusion: We found that higher TyG index values were associated with the brain’s WMHs of presumed vascular origin. Our findings suggest that the serum TyG index could be an additional valuable biomarker for assessing the risk of cerebral small vessel disease in the preclinical stage.
Keywords: triglyceride-glucose index, white matter hypersensitivities, endothelial dysfunction, insulin resistance, cerebral small vessel disease
Background
The brain’s white matter hypersensitivities (WMHs) are sometimes found in individuals without cerebral symptoms, especially in apparently healthy older people.1–3 Despite the considerable prevalence, they have received less attention for their clinical importance in brain health. Meanwhile, evidence suggests that WMHs seem asymptomatic but are not physiologic phenomena related to the aging process. They may have increased the risk of declining brain function, such as balance problems, emotional disturbance, pain susceptibility, and cognitive impairment.4–10 The plausible mechanism for WMHs is not fully understood until now, but cerebral minor vessel damage has been regarded as a crucial underlying cause.11
The triglyceride glucose (TyG) index, a simple and widely accessible measure, has emerged as a novel biomarker for cardiovascular and metabolic disorders.12–16 Higher TyG index indicates more hyperglycemic and dyslipidemic state, which could lead to the cerebro-cardiovascular atherosclerosis. Previous studies have shown that a high TyG index has a predictive value for arterial stiffness, coronary arterial calcification, functional kidney dysfunction, and ischemic cardiovascular events, and its clinical importance continues to grow in East Asia.12,13,17–19 Additionally, the TyG index may precede and predict metabolic syndrome and type 2 diabetes from the beginning.14,20,21
In this regard, an elevated TyG index could be a risk factor for cerebrovascular microangiopathy development, but data on this association are insufficient. Thus, we examined the relationship between the TyG index and the brain’s WMHs of presumed vascular origin.
Methods and Materials
Participants
Our study is part of the Health Risk Assessment Study (HERAS) cohort to evaluate risk factors for cardiometabolic diseases in Koreans, as described in previous studies.22,23 The present research included 2859 individuals over 45 years of age who underwent magnetic resonance (MR) imaging scans for brain health screening. The exclusion criteria for appropriate analysis were as follows: a 12-h fasting unmet for the accurate evaluation of fasting plasma glucose and fasting triglyceride: those who had been diagnosed with a malignancy, had a history of stroke or ischemic heart disease in the past (n=442). Consequently, 2417 participants were included in the final analysis. Each participant provided informed consent. This study was conducted following the ethical principles of the Declaration of Helsinki. This study was approved by the Institutional Review Board of the Yonsei University Gangnam Severance Hospital, Seoul, Korea.
Study Design
We assessed lifestyle and medical history using structured questionnaires for all participants. Body mass index (BMI) was evaluated by dividing the weight in kilograms by the square of height in meters. The average value was obtained for blood pressure (BP) estimation after measuring twice at heart height at 5-min intervals from the right upper arm.
Blood collection was performed after overnight fasting for 12 h, and the inter-and intra-coefficients of variation (CVs) were 2.8 and 3.9% for fasting plasma glucose and fasting triglyceride, respectively. The TyG index was calculated using the following formula: ln [fasting triglyceride level (mg/dl) × fasting glucose level (mg/dl)/2]. We divided the study population according to the TyG index quartiles as follows: Q1 ≤8.12 (≤25th percentile]; Q2: 8.13–8.50 (26 to 50th percentile]; Q3: 8.51–8.89 (51 to 75th percentile]; and Q4 ≥8.90 (≥76th percentile]).
We defined hypertension as systolic BP of 140 mmHg or higher, diastolic BP of 90 mmHg or higher, or current BP-lowering medication use;23 defined type 2 diabetes as a fasting plasma glucose level ≥ 126 mg/dL or taking diabetes drugs;24 defined metabolic syndrome as at least three of the following metabolic conditions: BMI ≥ 25.0 kg/m2, systolic BP of 130 mmHg or more, diastolic BP of 85 mmHg or more, or use of BP-lowering drugs; fasting plasma glucose levels ≥ 100 mg/dL or anti-diabetic agents use; triglyceride levels ≥ 150 mg/dL; and high-density lipoprotein cholesterol < 40 mg/dL for men and < 50 mg/dL for women.25 To evaluate endothelial dysfunction, we measured brachial‐ankle pulse wave velocity (baPWV) (automatic waveform analyzer model BP‐203RPE; Colin Co., Japan).
Brain MR Imaging Scans
All MR scans were performed after administration of gadolinium-diethylenetriamine-pentaacetic acid contrast agent, using a standard head coil with a 3.0-T MR scanner (GE Signa VH/I, Milwaukee, WI, USA). Two radiologists evaluated the brain MR features and were blinded to the clinical and laboratory data. The presence of WMHs was assessed using well-described radiological criteria: increased brightness on T2-weighted images in the white matter near the subcortical areas or the lateral ventricles.26
Statistical Analysis
The baseline characteristics were compared according to the TyG index quartiles using the chi-square test, a one-way analysis of variance, or the Kruskal–Wallis test. Using multiple logistic regression analysis, we assessed the odds ratios (ORs) and 95% confidence intervals (95% CIs) for WMHs across the TyG index quartiles after adjusting for potential confounding variables across the SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA). All statistical tests were two-sided, and statistical significance was set at P-value < 0.05.
Results
Clinical Characteristics of Study Participants
In Table 1, we compared the lifestyle variables and laboratory features of the study participants among the quartiles of the TyG index. The prevalence of WMHs was significantly higher in the fourth TyG index quartile, with an overall rate of 9.3%. For health behaviors, current smokers and alcohol drinkers were more prevalent with increasing TyG index quartiles. For laboratory characteristics, total cholesterol levels, leukocyte counts, and baPWV were highest in the fourth TyG index quartile group. In contrast, high-density lipoprotein cholesterol levels decreased according to serum TyG index quartiles. The highest proportions of hypertension, type 2 diabetes, and metabolic syndrome were the members of the highest TyG index quartile.
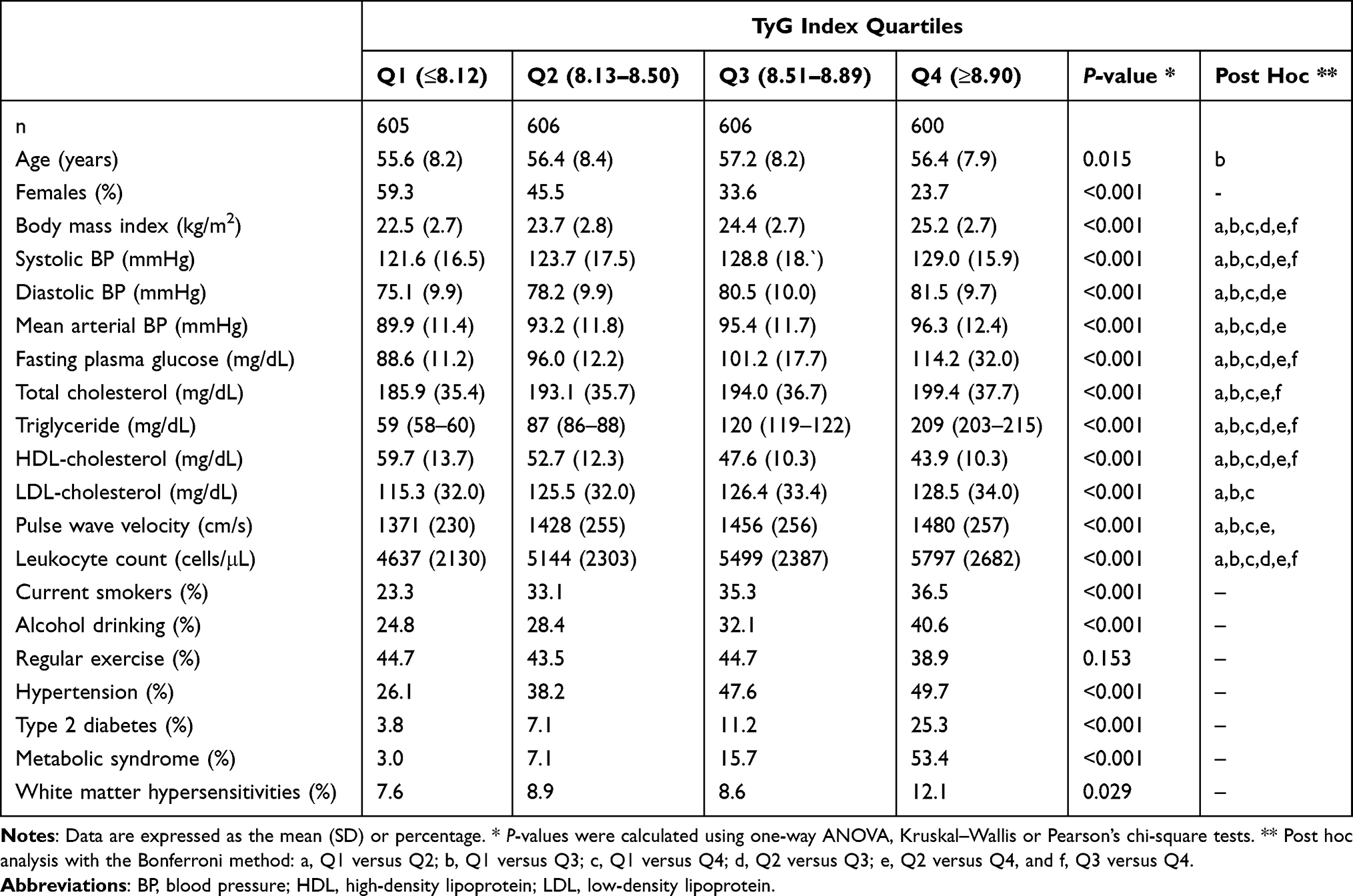 |
Table 1 Clinical Characteristics of the Study Population According to TyG Index Quartiles |
Odds Ratios for WMHs on Brain MR Imaging Scans
Table 2 shows the multivariate ORs for WMHs with increasing TyG index quartiles. Compared with the referent quartile, the OR (95% CI) of the Q3 and Q4 TyG index quartiles for WMHs were 1.76 (95% CI 1.05–2.97) and 6.79 (95% CI 3.85–11.54) after adjusting for age, sex, BMI, smoking status, alcohol intake, regular exercise, mean arterial pressure, C-reactive protein, total cholesterol, high-density lipoprotein cholesterol level, low-density lipoprotein cholesterol level, hypertension, and type 2 diabetes.
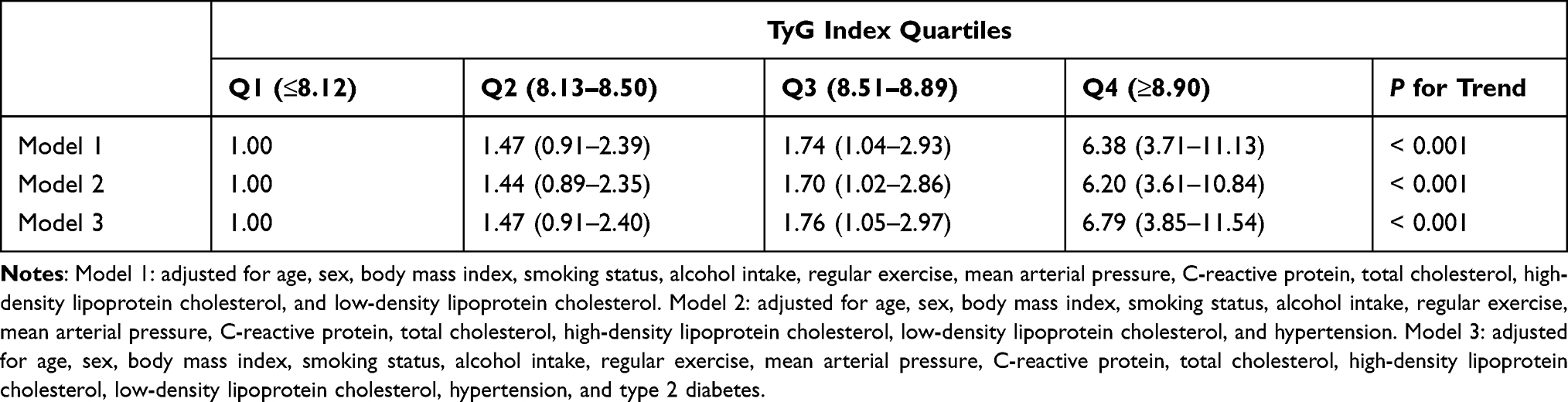 |
Table 2 Odds Ratios and 95% Confidence for White Matter Hypersensitivities According to TyG Index Quartiles |
Discussion
We found that higher TyG index values have higher likelihoods of having WMHs in middle-aged and older Koreans without cerebral symptoms after controlling for potential confounding factors, including health behaviors and metabolic conditions. Our findings are in agreement with previous results that higher TyG index is linked to increased risk of microvascular and macrovascular complications, including coronary arterial diseases, ischemic cerebrovascular events, and kidney functional damage.12,13,17–19,27
The exact mechanism by which a higher TyG index confers the brain’s WMHs is not well elucidated, but we can find putative mechanisms by some possible explanations for this association. First, endothelial dysfunction, a crucial step in the progression of small vessel disease, may play an important role in the pathophysiology of WMHs. Previous studies have reported evidence of endothelial dysfunction in individuals with ischemic cerebral microangiopathy and WMHs.11,18,28 The fluid leakage from the cerebral bloodstream followed by endothelial damage leads to structural changes in the perivascular spaces, resulting in white matter lesions.29 Consistent with previous results,17,30,31 endothelial dysfunction assessed by baPWV gradually increased across the TyG index quartiles in the present study.
Next, low-grade inflammation may be another contributor to the relationship between the TyG index and WMHs. A significant number of studies suggest that reactive oxidative stress and low-grade inflammation play significant roles in the pathophysiology of endothelial dysfunction. Previous studies have suggested that proinflammatory cytokines are closely linked to cerebral hypoperfusion and WMHs.32 A linear increase in white blood cell counts according to the TyG index quartiles in our study supports the close link between TyG index and systemic inflammation.
Third, insulin resistance could be an important underlying mechanism to explain this associations.33 Insulin resistance plays a major role in the pathogenesis of metabolic syndrome and type 2 diabetes. The prevalence of WMHs increased in patients with insulin resistance-related diseases.34–36 Insulin resistance could affect cerebral perfusion independent of inflammation, leading to segmental arteriolar wall disorganization called lipohyalinosis in the brain.37 The small vessel disease associated with insulin resistance reduced the luminal diameter of arterioles, another pathophysiology of WMHs.38 Moreover, the TyG index is closely correlated with homeostatic model assessment for insulin resistance (HOMA-IR) and a useful biomarker for the prediction of type 2 diabetes.20,21 Recent retrospective cohort study in Koreans demonstrated that individuals with baseline TyG indexes ≥ 8.8 had a 2.5 times higher risk of new-onset type 2 diabetes regardless of BMI stratification.21 Following previous findings, we observed increased prevalence of metabolic syndrome with increasing TyG index quartiles in the present study.
A major strength of this study was that WMH diagnoses were made in the process of general population screening rather than through identification by doctors in charge of cerebral symptoms. Therefore, we minimized the misclassification of asymptomatic patients with WMHs as normal subjects, leading to a decrease in cohort bias. Potential cerebral-related confounding factors were assessed using blood tests and baPWV, together with traditional risk factors.
There were several limitations to our study and interpretation. First, we used a cross-sectional design, suggesting that caution should be exercised in causal interpretations. Thus, further large-scale prospective studies with extended follow-up periods are warranted to elucidate the cause-and-effect link of the TyG index to WMHs. Second, this study was an exploratory study designed retrospectively and did not evaluate the scale of WMHs and cerebral grey matter conditions. WMH severity, voxel-based morphometry, or cortical thickness analysis were not fully considered in the present study. Lastly, we did not assess education, cognitive scales, or hypoglycemic episodes, which may be associated with the WMHs in the brain. In-depth prospective studies considering these factors are necessary for practical clinical application.
Conclusion
Individuals with the highest TyG index quartile have significantly increased their probability of having WMHs in middle-aged and older Koreans without cerebral symptoms. Our findings suggest that the serum TyG index could be an additional valuable measure for assessing and managing cerebral small vessel disease risk in the preclinical stage.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fazekas F, Barkhof F, Wahlund LO, et al. CT and MRI rating of white matter lesions. Cerebrovasc Dis. 2002;13(Suppl 2):31–36. doi:10.1159/000049147
2. De Leeuw FE, de Groot JC, Achten E, et al. Prevalence of cerebral white matter lesions in elderly people: a population based magnetic resonance imaging study. The Rotterdam Scan Study. J Neurol Neurosurg Psychiatry. 2001;70(1):9–14. doi:10.1136/jnnp.70.1.9
3. Wen W, Sachdev PS, Li JJ, Chen X, Anstey KJ. White matter hyperintensities in the forties: their prevalence and topography in an epidemiological sample aged 44–48. Hum Brain Mapp. 2009;30(4):1155–1167. doi:10.1002/hbm.20586
4. Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2010;341:c3666. doi:10.1136/bmj.c3666
5. Wardlaw JM, Doubal F, Armitage P, et al. Lacunar stroke is associated with diffuse blood-brain barrier dysfunction. Ann Neurol. 2009;65(2):194–202. doi:10.1002/ana.21549
6. Appelman AP, Vincken KL, van der Graaf Y, et al. White matter lesions and lacunar infarcts are independently and differently associated with brain atrophy: the SMART-MR study. Cerebrovasc Dis. 2010;29(1):28–35. doi:10.1159/000255971
7. Longstreth WT
8. Teodorczuk A, Firbank MJ, Pantoni L, et al. Relationship between baseline white-matter changes and development of late-life depressive symptoms: 3-year results from the LADIS study. Psychol Med. 2010;40(4):603–610. doi:10.1017/S0033291709990857
9. Starr JM, Leaper SA, Murray AD, et al. Brain white matter lesions detected by magnetic resonance [correction of resosnance] imaging are associated with balance and gait speed. J Neurol Neurosurg Psychiatry. 2003;74(1):94–98. doi:10.1136/jnnp.74.1.94
10. Binnekade TT, Perez RS, Maier AB, et al. White matter hyperintensities are related to pain intensity in an outpatient memory clinic population: preliminary findings. J Pain Res. 2019;12:1621–1629. doi:10.2147/JPR.S158488
11. Hassan A, Hunt BJ, O’Sullivan M, et al. Markers of endothelial dysfunction in lacunar infarction and ischaemic leukoaraiosis. Brain. 2003;126(Pt 2):424–432. doi:10.1093/brain/awg040
12. Luo E, Wang D, Yan G, et al. High triglyceride-glucose index is associated with poor prognosis in patients with acute ST-elevation myocardial infarction after percutaneous coronary intervention. Cardiovasc Diabetol. 2019;18(1):150. doi:10.1186/s12933-019-0957-3
13. Shi W, Xing L, Jing L, et al. Value of triglyceride-glucose index for the estimation of ischemic stroke risk: insights from a general population. Nutr Metab Cardiovasc Dis. 2020;30(2):245–253. doi:10.1016/j.numecd.2019.09.015
14. Moon S, Park JS, Ahn Y. The cut-off values of triglycerides and glucose index for metabolic syndrome in American and Korean adolescents. J Korean Med Sci. 2017;32(3):427–433. doi:10.3346/jkms.2017.32.3.427
15. Liu J, Guan L, Zhao M, et al. Association between the triglyceride-glucose index and outcomes of nonalcoholic fatty liver disease: a large-scale health management cohort study. Diabetes Metab Syndr Obes. 2021;14:2829–2839. doi:10.2147/DMSO.S316864
16. Jiang H, Li L, Liu J, et al. Triglyceride-glucose index as a novel biomarker in the occurrence of kidney stones: a cross-sectional population-based study. Int J Gen Med. 2021;14:6233–6244. doi:10.2147/IJGM.S334821
17. Lee SB, Ahn CW, Lee BK, et al. Association between triglyceride glucose index and arterial stiffness in Korean adults. Cardiovasc Diabetol. 2018;17(1):41. doi:10.1186/s12933-018-0692-1
18. Park K, Ahn CW, Lee SB, et al. Elevated TyG index predicts progression of coronary artery calcification. Diabetes Care. 2019;42(8):1569–1573. doi:10.2337/dc18-1920
19. Zhao S, Yu S, Chi C, et al. Association between macro- and microvascular damage and the triglyceride glucose index in community-dwelling elderly individuals: the Northern Shanghai Study. Cardiovasc Diabetol. 2019;18(1):95. doi:10.1186/s12933-019-0898-x
20. Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–3351. doi:10.1210/jc.2010-0288
21. Lee DY, Lee ES, Kim JH, et al. Predictive value of triglyceride glucose index for the risk of incident diabetes: a 4-year retrospective longitudinal study. PLoS One. 2016;11(9):e0163465. doi:10.1371/journal.pone.0163465
22. Jung DH, Lee YJ, Park B. Joint effect of hepatic steatosis and alanine aminotransferase within the normal range on incident ischemic heart disease: a prospective study in Koreans. Clin Interv Aging. 2021;16:513–523. doi:10.2147/CIA.S301741
23. Park B, Lee YJ, Lee HS, Jung DH. The triglyceride-glucose index predicts ischemic heart disease risk in Koreans: a prospective study using National Health Insurance Service data. Cardiovasc Diabetol. 2020;19(1):210. doi:10.1186/s12933-020-01186-2
24. Kim MK, Ko SH, Kim BY, et al. 2019 clinical practice guidelines for type 2 diabetes mellitus in Korea. Diabetes Metab J. 2019;43(4):398–406. doi:10.4093/dmj.2019.0137
25. Einhorn D, Reaven GM, Cobin RH, et al. American College of Endocrinology position statement on the insulin resistance syndrome. Endocr Pract. 2003;9(3):237–252. doi:10.4158/EP.9.S2.5
26. O’Sullivan M. Leukoaraiosis. Pract Neurol. 2008;8(1):26–38. doi:10.1136/jnnp.2007.139428
27. Hassan A, Hunt BJ, O’Sullivan M, et al. Homocysteine is a risk factor for cerebral small vessel disease, acting via endothelial dysfunction. Brain. 2004;127(Pt 1):212–219. doi:10.1093/brain/awh023
28. Xiao A, Ge QM, Zhong HF, et al. White matter hyperintensities of bilateral lenticular putamen in patients with proliferative diabetic retinopathy: a voxel-based morphometric study. Diabetes Metab Syndr Obes. 2021;14:3653–3665. doi:10.2147/DMSO.S321270
29. Mayda AB, Westphal A, Carter CS, DeCarli C. Late life cognitive control deficits are accentuated by white matter disease burden. Brain. 2011;134(Pt 6):1673–1683. doi:10.1093/brain/awr065
30. Li M, Zhan A, Huang X, et al. Positive association between triglyceride glucose index and arterial stiffness in hypertensive patients: the China H-type hypertension registry study. Cardiovasc Diabetol. 2020;19(1):139. doi:10.1186/s12933-020-01124-2
31. Won KB, Park GM, Lee SE, et al. Relationship of insulin resistance estimated by triglyceride glucose index to arterial stiffness. Lipids Health Dis. 2018;17(1):268. doi:10.1186/s12944-018-0914-2
32. Fornage M, Chiang YA, O’Meara ES, et al. Biomarkers of inflammation and MRI-defined small vessel disease of the brain: the cardiovascular health study. Stroke. 2008;39(7):1952–1959. doi:10.1161/STROKEAHA.107.508135
33. Nam KW, Kwon HM, Jeong HY, Park JH, Kwon H, Jeong SM. High triglyceride-glucose index is associated with subclinical cerebral small vessel disease in a healthy population: a cross-sectional study. Cardiovasc Diabetol. 2020;19(1):53. doi:10.1186/s12933-020-01031-6
34. Lucatelli P, Montisci R, Sanfilippo R, et al. Is there an association between leukoaraiosis volume and diabetes? J Neuroradiol. 2016;43(4):273–279. doi:10.1016/j.neurad.2015.11.003
35. Bokura H, Yamaguchi S, Iijima K, Nagai A, Oguro H. Metabolic syndrome is associated with silent ischemic brain lesions. Stroke. 2008;39(5):1607–1609. doi:10.1161/STROKEAHA.107.508630
36. Tamura Y, Araki A. Diabetes mellitus and white matter hyperintensity. Geriatr Gerontol Int. 2015;15(Suppl 1):34–42. doi:10.1111/ggi.12666
37. Manschot SM, Brands AM, van der Grond J, et al. Brain magnetic resonance imaging correlates of impaired cognition in patients with type 2 diabetes. Diabetes. 2006;55(4):1106–1113. doi:10.2337/diabetes.55.04.06.db05-1323
38. Geerlings MI, Appelman AP, Vincken KL, Mali WP. van der Graaf Y. Association of white matter lesions and lacunar infarcts with executive functioning: the SMART-MR study. Am J Epidemiol. 2009;170(9):1147–1155. doi:10.1093/aje/kwp256
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.