")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Relationship Between Mood Episode and Employment Status of Outpatients with Bipolar Disorder: Retrospective Cohort Study from the Multicenter Treatment Survey for Bipolar Disorder in Psychiatric Clinics (MUSUBI) Project
Authors Konno Y , Fujino Y , Ikenouchi A , Adachi N , Kubota Y , Azekawa T , Ueda H, Edagawa K, Katsumoto E, Goto E, Hongo S, Kato M , Tsuboi T , Yasui-Furukori N , Nakagawa A , Kikuchi T, Watanabe K , Yoshimura R
Received 30 May 2021
Accepted for publication 19 August 2021
Published 7 September 2021 Volume 2021:17 Pages 2867—2876
DOI https://doi.org/10.2147/NDT.S322507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Yusuke Konno,1,2 Yoshihisa Fujino,2 Atsuko Ikenouchi,1,3 Naoto Adachi,4 Yukihisa Kubota,4 Takaharu Azekawa,4 Hitoshi Ueda,4 Koji Edagawa,4 Eiichi Katsumoto,4 Eiichiro Goto,4 Seiji Hongo,4 Masaki Kato,5,6 Takashi Tsuboi,5,7 Norio Yasui-Furukori,5,8 Atsuo Nakagawa,5,9 Toshiaki Kikuchi,5,9 Koichiro Watanabe,5,7 Reiji Yoshimura1,5
1Department of Psychiatry, University of Occupational and Environmental Health, Kitakyushu, Japan; 2Department of Environmental Epidemiology, Institute of Industrial Ecological Sciences, University of Occupational and Environmental Health, Kitakyushu, Japan; 3Medical Center for Dementia, University Hospital of Occupational and Environmental Health, Kitakyushu, Japan; 4The Japanese Association of Neuro-Psychiatric Clinics, Tokyo, Japan; 5The Japanese Society of Clinical Neuropsychopharmacology, Tokyo, Japan; 6Department of Neuropsychiatry, Kansai Medical University, Osaka, Japan; 7Department of Neuropsychiatry, Kyorin University School of Medicine, Tokyo, Japan; 8Department of Psychiatry, Dokkyo Medical University, Tochigi, Japan; 9Department of Neuropsychiatry, Keio University School of Medicine, Tokyo, Japan
Correspondence: Yusuke Konno
Department of Psychiatry, University of Occupational and Environmental Health, 1-1, Iseigaoka, Yahatanishiku, Kitakyushu, 807-8555, Japan
Tel +81-93-691-7401
Fax +81-93-692-4894
Email [email protected]
Objective: The objective of this study was to clarify the relationship between mood episode and employment in patients with bipolar disorder to help improve their employment status.
Methods: All medical records of patients with bipolar disorder who visited 176 member clinics of the Japanese Association of Neuro-Psychiatric Clinics in September–October 2016 were investigated in September–October 2017. Details of the medical care received were investigated using a survey sheet, which included employment status. Odds ratios of mood episodes for employment status were analyzed using a logistic regression model.
Results: Among patients aged 60 years or less, 2292 described their occupation. On univariate analysis, odds ratios were statistically significant for depressive episode (OR = 2.68 [1.50– 4.78] p = 0.001) and manic episode (OR = 2.64 [1.07– 6.47] p = 0.034), whereas no significant difference was noted for mixed episode (OR = 1.72 [0.69– 4.33] p = 0.246). On multivariate analysis, odds ratios were statistically significant for depressive episode (OR = 2.16 [1.13– 4.13], p = 0.020) and manic episode (OR = 3.55 [1.36– 9.25], p = 0.010), whereas no significant difference was noted for mixed episode (OR = 1.83 [0.65– 5.14] p = 0.254).
Conclusion: Employment status among these patients with bipolar disorder receiving outpatient treatment was 43.5%. Compared to remission episodes, manic and depressive episodes were associated with a higher risk of unemployment.
Keywords: mood disorder, continuous employment, occupational health, Japan
Introduction
Since bipolar disorder develops at a young age and follows a chronic course through alternating cycles of manic, hypomanic and depressive episodes, many patients are required to balance treatment and work. The lifetime prevalence of bipolar disorder is said to be 0.4–3%.1,2 Bipolar disorder often begins in late adolescence to early adulthood, and the age of onset is typically in the late teens through the 20s.3 According to the results of the Global Burden of Disease Study, disability-adjusted life years (DALYs) are also evident from the teenage years, and peak in the 20s.4 Treatment is often difficult, and 50–60% of patients undergoing remission maintenance are said to relapse within several years.5,6 Under such circumstances, the proportion of patients with bipolar disorder who are able to stay employed is reported to be 40–60%, and their employment rates are not high.7,8 Thus, bipolar disorder is a disease that occurs at a young age, involves cycles of mood episodes, and requires patients to balance continuous treatment and work.
Manic and depressive episodes are seen in bipolar disorder. Patients with bipolar disorder live a social life while experiencing these episodes, which creates a variety of difficulties. In brief, their activity levels increase during manic episodes and decrease during depressive episodes.9 In a mixed episode, manic and depressive symptoms occur simultaneously or in rapid succession.9
Patients with bipolar disorder live about half their life in a symptomatic state, primarily one of depressive symptoms, which may carry a risk of interfering with continuous employment.10,11 In patients with depressive symptoms, impairment of psychosocial function is more severe,12–14 and often prevents them from maintaining the ability to function at work.15 Patients with bipolar disorder have also been found to have functional impairment between episodes.16,17 Cognitive and working memory impairments are found in these functional disorders, and a relationship between these and employment disability has been noted.18,19 Functional impairment is reported to occur in the presence of psychotic symptoms, rapid cycling, psychiatric comorbidity, and substance abuse, which may affect employment.20–22 Bipolar patients live with these functional impairments, which can be obstructions to continuous employment.
These work-related problems concern not just the individuals themselves but society as well. The Global Burden of Disease Study attributed 8.4 million DALYs to bipolar disorder, and considered the condition to be a social burden.23 In the United States, the social cost incurred by bipolar disorder is estimated to be $45 billion per year.24 When divided into direct (eg, medical and social service expenses) and indirect cost (eg, morbidity and mortality expenses), the direct cost is estimated to be $7 billion and the indirect cost $38 billion. Within the indirect cost, expenses associated with employment status, such as decreased productivity and unemployment, are estimated to be $17 billion.24 Given that Japan has about 120,000 patients with bipolar disorder, the need to develop measures is both a medical and a social issue.25
Despite this mixture of medical and social issues, factors associated with continuous employment of patients with bipolar disorder are poorly known. Mood episode is one factor that may be linked to continuous employment. The several guidelines for bipolar disorder formulated to date all describe a treatment approach for individual mood episodes,26–30 indicating the importance of identifying mood episodes when administering treatment for bipolar disorder. Regarding the relationship with employment, while depressive episodes have been linked to an increased risk of unemployment, no findings have been reported for manic or mixed episodes.16,31,32
The objective of this study was to clarify the relationship between mood episode and employment in patients with bipolar disorder as a means of helping to improve their employment status.
Materials and Methods
Participants and Methods
The retrospective cohort investigation of the Multicenter Treatment Survey for Bipolar Disorder in Psychiatric Clinics (MUSUBI) projects33–37 was conducted at member clinics of the Japanese Association of Neuro-Psychiatric Clinics (JAPC). JAPC has 1650 member clinics, which examine about 30% of patients with mood disorders in Japan.38 In this study, 176 of 1650 member clinics of JAPC took part in the survey. Investigators at these clinics are psychiatrists, most of whom are psychiatric specialists certified by the Japanese Society of Psychiatry and Neurology or designated psychiatrists certified by the Japanese Ministry of Health, Labour and Welfare. All medical records of patients with bipolar disorder who visited the 176 member clinics of the Japanese Association of Neuro-Psychiatric Clinics in September-October 2016 were investigated in September-October 2017. We gathered information about age, sex, psychiatric comorbidity, physical comorbidity, substance abuse, rapid cycling, psychotic symptoms, suicidal ideation, medication details and mood episodes (remission, depressive episode, manic episode, and mixed episode) in addition to employment status at two time points, October-December 2016 and October-December 2017. The diagnosis of bipolar disorder was based on the 10th Revision of the International Classification of Diseases and Related Health Problems (ICD-10). Clinical psychiatrists who participated in the survey completed the questionnaire through a retrospective medical record survey. The questionnaire included patient characteristics (age, gender, and occupational status), psychiatric and physical comorbidities, substance abuse, bipolar disorder subcategories, rapid cycling, mood episodes, psychotic symptoms, suicide ideation, and details of pharmacological treatment. In this study, remission was defined as when the interviewing psychiatrist judged the patient to be in clinical remission with no depressive episodes, no manic episodes, and no mixed episodes. Episodes other than remission were also judged clinically. With respect to employment status, an individual who worked at least 30 hours a week was defined as a full-time worker. This criterion was noted on the survey form and was known to all participating psychiatrists prior to the start of the survey. An individual who was a full-time worker at baseline and still held a full-time job one year later was categorized as in “continuous employment,” and an individual who was a full-time worker at baseline but was unemployed one year later was categorized as “loss of employment.”
Ethics
This study was conducted in compliance with the Declaration of Helsinki and the Japanese Ethical Guidelines for Medical and Health Research Involving Human Subjects. This study was approved by the Ethics Committee of the Japanese Association of Neuropsychiatric Clinics and the Ethics Committee of Medical Research at the University of Occupational and Environmental Health. Since this was a retrospective investigation of medical charts, requirements pertaining to informed consent were waived. However, information on the study was disclosed on our web page, and patients were allowed to opt out.
Statistical Analysis
In the univariate analysis, logistic regression analysis was performed for each factor. Multivariate logistic regression analysis was then performed to avoid confounding effects of each factor. In the multivariate logistic regression analysis, the dependent variable was employment status. The odds ratios of mood episodes (remission, depressive episodes, manic episodes, and mixed episodes) for employment status were analyzed using a logistic regression model. The model included age, sex, psychiatric comorbidity, physical comorbidity, substance abuse, rapid cycling, psychotic symptoms, suicidal ideation, and medication details as confounding adjustment factors. Probability was set at the 5% level. The analyses were conducted using Stata SE/16 (StataCorp LLC, College Station, TX, USA).
Results
At baseline, the 176 clinics returned completed questionnaire sheets for 3137 outpatients with bipolar disorder. Descriptions of occupation were provided by 3081 of the 3137 patients. Of the 3081 patients, 2292 were under the age of 60, of whom 997 (43.5%) were full-time workers. Of these 997, 968 patients who were full-time workers aged under 58 years were included in the follow-up survey conducted one year later. In that survey, 816 patients (84.3%) participated, among whom 708 were still employed fulltime (= continuous employment) and 70 were unemployed (= loss of employment). Data of these 705 patients in the continuous employment group and the 70 in the loss of employment group are presented in Table 1. Between the groups, age and bipolar disorder subcategories were relatively similar, but differences were seen in other attributes, symptoms, and treatment details. Data by mood episode are shown in Table 2. Of the 775 patients, 398 patients were in remission, 268 were in a depressive episode, 50 were in a manic episode, and 59 were in a mixed episode. Data by mood episode are shown in Table 2. The two groups were relatively similar in age but differed in other attributes, symptoms and treatment details.
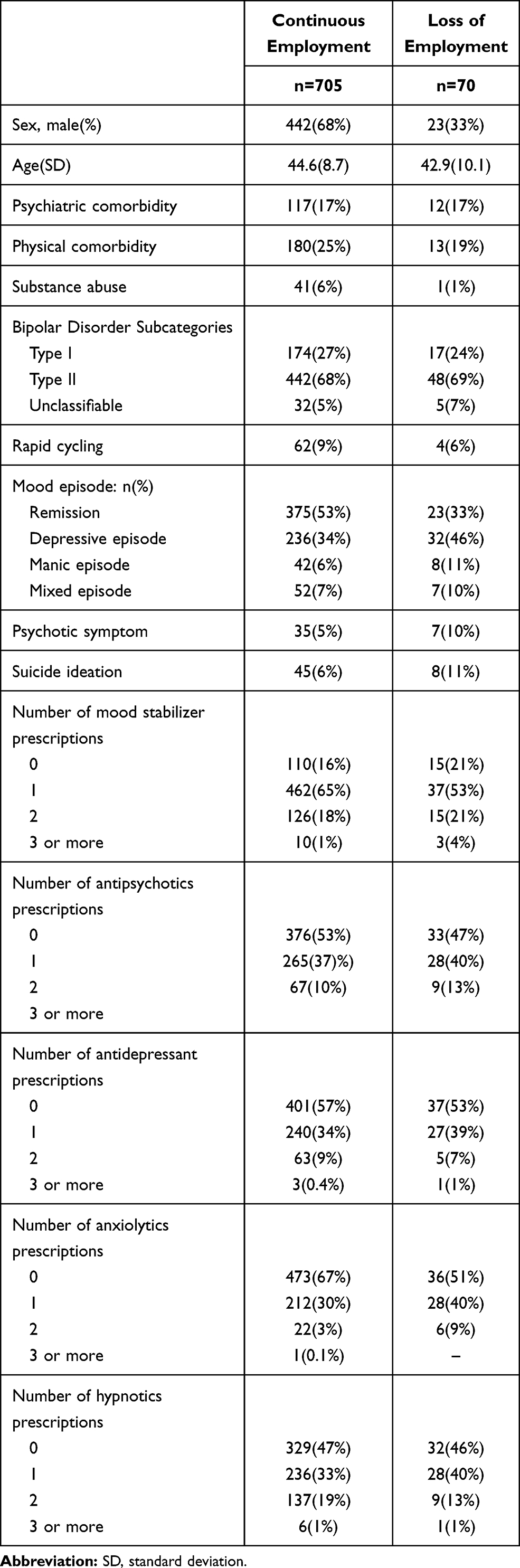 |
Table 1 Clinical Characteristics Between Patients with Continuous Employment and Loss of Employment |
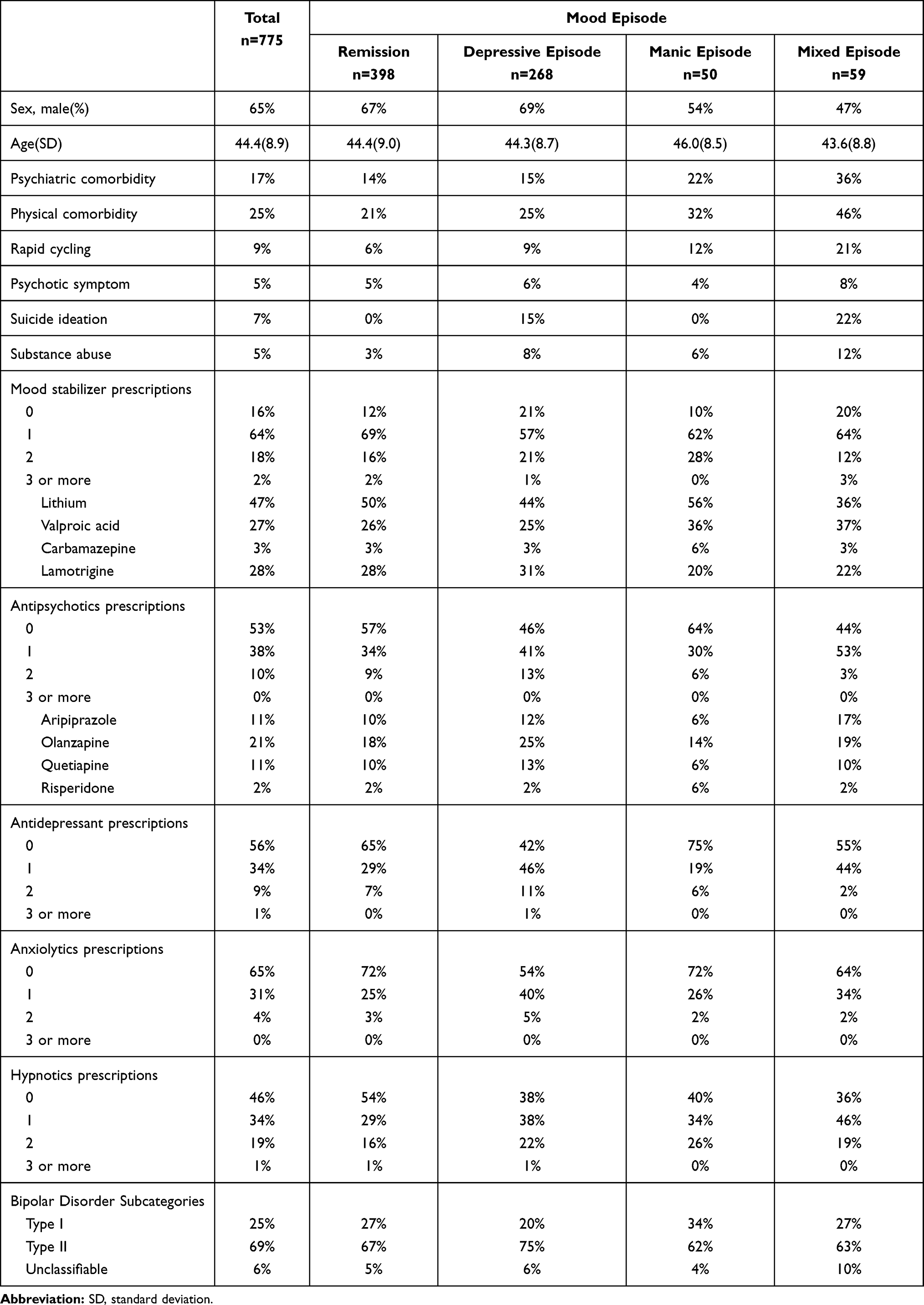 |
Table 2 Clinical Characteristics of Each Mood Episode |
The results of univariate and multivariate analyses are shown in Table 3. In the univariate analysis, the odds ratio for unemployment was statistically significant for depressive episode (OR = 2.68 [1.50–4.78] p = 0.001) and manic episode (OR = 2.64 [1.07–6.47] p = 0.034). In contrast, no significant difference was noted for mixed episode (OR = 1.72 [0.69–4.33] p = 0.246). In the multivariate analysis, the odds ratio was statistically significant for depressive episode (OR = 2.16 [1.13–4.13] p = 0.020) and manic episode (OR = 3.55 [1.36–9.25] p = 0.010). Again, no significant difference was noted for mixed episode (OR = 1.83 [0.65–5.14] p = 0.254).
 |
Table 3 Association Between Mood Episode and Continuous Employment |
In the multivariate analysis, no significant difference was noted for physical comorbidity (OR = 0.68 [0.36–1.31] p = 0.252), substance abuse (OR = 0.19 [0.26–1.45] p = 0.110), or rapid cycling (OR = 0.55 [0.19–1.60] p = 0.272).
Discussion
This study was conducted to investigate employment status among patients with bipolar disorder and the impact of mood episode on their continuous employment. To our knowledge, only a few studies have explored the relationship between employment status and mood episode in patients with bipolar disorder,16,31,32 and the present study is the first conducted in Japan. At baseline, 43.5% of the subjects were full-time workers. When we examined the impact of mood episode on the loss of employment, depressive episode and manic episode had a higher risk of unemployment than remission. The employment rate among patients with bipolar disorder has been reported to be 40–60% in studies published overseas,7,8 which is reasonably consistent from the result of our present study. Although only a handful of studies have investigated the relationship between mood episode and employment, some reported that depressive episode was a risk factor that may hinder continuous employment.16,31,32 With regard to the relationship between manic episode and employment, we found no conclusive studies.
In this study, patients with depressive episode had an increased risk of losing a job than those in remission. This is considered primarily attributable to functional reasons. A person with depressive episode may exhibit symptoms such as depressed mood, loss of interest/pleasure, weight loss/gain, decreased/increased appetite, insomnia/hypersomnia, psychomotor agitation/retardation, fatigue/listlessness, feelings of worthlessness and guilt, reduced thinking ability and concentration, difficulty in decision making, and suicidal ideation.9 These symptoms can delay work progress and frequently cause the person to show up late for work, leave work early, or be absent from work, leading to the loss of employment. In a depressive episode, the person’s ability to function at work deteriorates, resulting in unemployment. To prevent such job loss and improve employment status among patients with bipolar disorder, the maintenance of remission is desired. However, even in remission, 70–90% of the patients with bipolar disorder are believed to relapse within 5 years,39 and so the possibility of a recurrence of symptoms needs to be kept in mind. It is important to recognize a depressive episode at an early stage and initiate an intervention. Although bipolar disorder shares the same depressive symptoms as major depressive disorder (MDD), treatment for depression differs from that for the depression phase of bipolar disorder. Additionally, patients with bipolar disorder are reported to have more severe work impairment than those with MDD.40 Therefore, it is important to be aware that bipolar disorder should be examined with even greater care than MDD.
Manic episode was also found to be associated with a higher risk of unemployment than remission. The increased risk of unemployment in patients with manic episode is considered attributable to both social and functional reasons. A person with manic episode may exhibit symptoms such as inflated and exaggerated self-esteem, decreased desire for sleep, talkativeness or urgency, flight of ideas, distraction, increased goal-oriented activities, psychomotor agitation, and engagement in activities that could be potentially troublesome.9 Distraction causes the person to become unable to pay attention to details at work, leading to increased mistakes. Flight of ideas causes the person to undertake different tasks one after another, leaving them all unfinished. Inflated self-esteem causes the person to take on reckless challenges and become arrogant and uncooperative. In a manic episode, the person’s ability to function at work deteriorates in this manner, resulting in unemployment. Unlike people with depressive episode, those with manic episode may also lose their job for social reasons in addition to functional decline. To prevent unemployment in this manner, it is also important to recognize manic episode at an early stage and initiate an intervention, as with depressive episode.
Although no gender difference is thought to exist in the course of bipolar disorder, the proportion of men in our present study was higher in the continuous employment group. In comparison, a survey by the Ministry of Health, Labor and Welfare reported an employee turnover rate for full-time workers in Japan in 2019 of 13.4% for men and 18.2% for women, and thus higher for women.41 This result is therefore considered to reflect the social gender difference in Japan. The percentages of psychotic symptoms and suicidal ideation were lower in the continuous employment group. However, there was no difference in the percentage of psychiatric comorbidity, while the percentages of physical comorbidity, substance abuse, and rapid cycling were higher in the continuous employment group than in the loss of employment group. These symptoms and comorbidities are considered to be factors for a poor prognosis in bipolar disorder and are unlikely to contribute to continuous employment.42 We consider that these results are likely to be affected by unmeasured bias. In the future, it is considered necessary to conduct studies on these symptoms, comorbidities and continuous employment.
Limitations
Several limitations of our study warrant mention. First, due to the relatively short retrospective follow-up period (1 year), the risk of long-term unemployment is unknown. Considering the treatment duration for bipolar disorder, investigation over a longer period is desirable.
Second, although the retrospective one-year follow-up rate was relatively good, at 84%, the impact of dropouts is unknown. When baseline characteristics were compared between dropouts and follow-up completers, there was no difference in sex, age, manic episode, or mood stabilizer or antipsychotic use. While depressive episode and mixed episode were more common in dropouts, antidepressants, psychiatric comorbidity, and psychotic symptoms were more common in follow-up completers.
Third, since this study focused on the relationship between mood status at baseline and unemployment, the modified effects of treatment details, concomitant symptoms, and detailed comorbidities are unknown. In particular, as treatment details are clinically managed by the patients’ primary physicians, the impact of specific treatment regimens is unknown. This study considered factors such as drug therapy, but did not consider blood concentrations of mood stabilizers or non-drug therapies such as psychotherapy.
Fourth, because this study was conducted in parallel with daily clinical practice, the assessment was conducted as a single interview, and a structured clinical interview was not required. Accordingly, although the assessments were conducted by well-trained physicians, the presence of inter-rater variability cannot be ruled out.
Fifth, baseline functioning was not assessed, and rating scales such as the Hamilton Depression Rating Scale (HAM-D), Montgomery Åsberg Depression Rating Scale (MADRS), and Young Mania Rating Scale (YMRS) were not used, which may have made the assessment less accurate.
Sixth, the characteristics of this study may limit its generalizability to other populations. In Japan, employees are allowed to take leave due to illness. This period may vary among workplaces and may range from a few months to several years. During this period, the employee will generally not receive any salary, but will be entitled to receive an injury and illness allowance from the health insurance association for a period of one year and six months. This applies to all workers, but some companies offer more generous guarantees of their own. The system for leave of absence differs among countries, which may undermine the external validity of our results in countries other than Japan.
Conclusion
In the MUSUBI-J-Study, 43.5% of patients with bipolar disorder undergoing outpatient treatment were full-time workers. Depressive and manic episodes were associated with higher risk for unemployment than remission. Employment rates among patients with bipolar disorder need to be improved. In patients with bipolar disorder who work in a depressive or manic episode, the risk of future unemployment is high; therefore, an appropriate intervention should be provided.
Approval of the Research Protocol
This study was approved by the Ethics Committee of the Japanese Association of Neuropsychiatric Clinics (ID: 20160822, 20180723) and the Ethics Committee of Medical Research at the University of Occupational and Environmental Health, Japan (approval no. UOEHCRB20-112).
Informed Consent
Information on the study was disclosed on our web page, and patients were allowed to opt out.
Acknowledgments
The authors thank the following psychiatrists belonging to the Japanese Association of Neuro-Psychiatric Clinics: Drs. Kazuhira Miki, Toshihiko Lee, Norio Okamoto, Makoto Nakamura, Junkou Sato, Kazunori Otaka, Satoshi Terada, Tadashi Ito, Munehide Tani, Atsushi Satomura, Hiroshi Sato, Hideki Nakano, Yoichi Nakaniwa, Eiichi Hirayama, Keiichi Kobatake, Koji Tanaka, Mariko Watanabe, Shiguyuki Uehata, Asana Yuki, Nobuko Akagaki, Michie Sakano, Akira Matsukubo, Yukihisa Kibota, Yasuyuki Inada, Hiroshi Oyu, Tsuneo Tsubaki, Tatsuji Tamura, Shigeki Akiu, Atsuhiro Kikuchi, Keiji Sato, Kazuyuki Fujita, Fumio Handa, Hiroyuki Karasawa, Kazuhiro Nakano, Kazuhiro Omori, Seiji Tagawa, Daisuke Maruno, Hiroaki Furui, You Suzuki, Takeshi Fujita, Yukimitsu Hoshino, Kikuko Ota, Takaharu Azekawa, Akira Itami, Kenichi Goto, Yoshiaki Yamano, Kiichiro Koshimune, Junko Matsushita, Takatsugu Nakayama, Kazuyoshi Takamuki, Nobumichi Sakamoto, Eiichi Katsumoto, Miho Shimizu, Muneo Shimura, Norio Kawase, Ryouhei Takeda, Takuya Hirota, Hideko Fujii, Yoichiro Watanabe, Riichiro Narabayashi, Yutaka Fujiwara, Kazu Kobayashi, Yuko Urabe, Miyako Oguru, Osamu Miura, Yoshio Ikeda, Hitoshi Ueda, Hidemi Sakamoto, Yosuke Yonezawa, Yoichi Takei, Toshimasa Sakane, Kiyoshi Oka, Kyoko Tsuda, Shigemitsu Hayashi, Kunihiko Kawamura, Yasushi Furuta, Kazuko Miyauchi, Yoshio Miyauchi, Mikako Oyama, Keizo Hara, Misako Sakamoto, Shigeki Masumoto, Yasuhiro Kaneda, Yoshiko Kanbe, Masayuki Iwai, Naohisa Waseda, Nobuhiko Ota, Takahiro Hiroe, Ippei Ishii, Hideki Koyama, Terunobu Otani, Osamu Takatsu, Takashi Ito, Norihiro Marui, Toru Takahashi, Tetsuro Oomori, Toshihiko Fukuchi, Kazumichi Egashira, Kiyoshi Kaminishi, Ryuichi Iwata, Satoshi Kawaguchi, Yoshinori Morimoto, Hirohisa Endo, Yasuo Imai, Eri Kohno, Aki Yamamoto, Naomi Hasegawa, Sadamu Toki, Hideyo Yamada, Hiroyuki Taguchi, Hiroshi Yamaguchi, Hiroki Ishikawa, Sakura Abe, Kazuhiro Uenoyama, Kazunori Koike, Yoshiko Kamekawa, Michihito Matsushima, Ken Ueki, Sintaro Watanabe, Tomohide Igata, Yoshiaki Higashitani, Eiichi Kitamura, Junko Sanada, Takanobu Sasaki, Kazuko Eto, Ichiro Nasu, Kenichiro Shinkawa, Yukio Oga, Michio Tabuchi, Daisuke Tsujimura, Tokunai Kataoka, Kyohei Noda, Nobuhiko Imato, Ikuko Nitta, Yoshihiro Maruta, Satoshi Seura, Toru Okumura, Osamu Kino, Tomoko Ito, Ryuichi Iwata, Wataru Konno, Toshio Nakahara, Masao Nakahara, Hiroshi Yamamura, Masatoshi Teraoka, Eiichiro Goto, Masato Nishio, Koji Edagawa, Miwa Mochizuki, Tsuneo Saitoh, Tetsuharu Kikuchi, Chika Higa, Hiroshi Sasa, Yuichi Inoue, Muneyoshi Yamada, Yoko Fujioka, Kuniaki Maekubo, Hiroaki Jitsuiki, Toshihito Tsutsumi, Yasumasa Asanobu, Seiji Inomata, Kazuhiro Kodama, Aikihiro Takai, Asako Sanae, Shinichiro Sakurai, Kazuhide Tanaka, Masahiko Shido, Haruhisa Ono, Wataru Miura, Yukari Horie, Tetso Tashiro, Tomohide Mizuno, Naohiro Fujikawa, Hiroshi Terada, Kenji Taki, Kyoko Kyotani, Masataka Hatakoshi, Katsumi Ikeshita, Keiji Kaneta, Ritsu Shikiba, Tsuyoshi Iijima, Masaru Yoshimura, Naoto Adachi, Masumi Ito, Shunsuke Murata, Seiji Hongo, Mio Mori, and Toshio Yokouchi.
Disclosure
Yusuke Konno, Yoshihisa Fujino, Atsuko Ikenouchi, Naoto Adachi declare no Conflict of Interests for this article. Yukihisa Kubota has received consultant fees from Pfizer and Meiji-Seika Pharma and speaker’s honoraria from Meiji-Seika Pharma, Eli Lilly, Janssen Pharmaceutical, Dainippon Sumitomo Pharma, Mitsubishi Tanabe Pharma, Yoshitomi Yakuhin, Otsuka Pharmaceutical, and Eisai. Takaharu Azekawa has received speaker’s honoraria from Eli Lilly, Otsuka Pharmaceutical, and Pfizer. Hitoshi Ueda has received manuscript fees or speaker’s honoraria from Eli Lilly, Janssen Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Pfizer, Sumitomo Dainippon Pharma, Takeda Pharmaceutical, and Yoshitomi Yakuhin. Koji Edagawa has received speaker’s honoraria from Eli Lilly, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Pfizer, Sumitomo Dainippon Pharma, Kyowa and Yoshitomi Yakuhin. Eiichi Katsumoto has received speaker’s honoraria from Daiichi Sankyo, Eisai, Eli Lilly, Janssen Pharmaceutical, Kyowa Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Pfizer, Sumitomo Dainippon Pharma, and UCB. Eiichiro Goto has received manuscript fees or speaker’s honoraria from Eli Lilly, Janssen Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, and Sumitomo Dainippon Pharma. Seiji Hongo has received manuscript fees or speaker’s honoraria from Eli Lilly, Janssen Pharmaceutical, Kyowa Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, Otsuka Pharmaceutical, Pfizer, Shionogi, Sumitomo Dainippon Pharma, and Yoshitomi Yakuhin. Masaki Kato has received grant funding from the Japan Society for the Promotion of Science, SENSHIN Medical Research Foundation and the Japan Research Foundation for Clinical Pharmacology, and speaker’s honoraria from Dainippon-Sumitomo Pharma, Otsuka, Meiji-Seika Pharma, Eli Lilly, MSD K.K., GlaxoSmithKline, Pfizer, Janssen Pharmaceutical, Shionogi, Mitsubishi Tanabe Pharma, Takeda Pharmaceutical and Ono Pharmaceutical. Takashi Tsuboi has received consultant fees from Pfizer and speaker’s honoraria from Eli Lilly, Meiji-Seika Pharma, MSD, Janssen Pharmaceutical, Dainippon Sumitomo Pharma, Mitsubishi Tanabe Pharma, Yoshitomi Yakuhin, Mochida Pharmaceutical, Otsuka Pharmaceutical, Kyowa Pharmaceutical, and Takeda Pharmaceutical. Norio Yasui-Furukori has received grant/research support or honoraria from, and received speaker’s honoraria of Dainippon-Sumitomo Pharma, Mochida Pharmaceutical, MSD, and Otsuka Pharmaceutical. Atsuo Nakagawa has received lecture fees from Pfizer, Eli Lilly, Otsuka, Janssen Pharmaceutical, Mitsubishi Tanabe, Mochida, Dainippon Sumitomo and NTT Docomo, and participated in an advisory board for Takeda, Meiji Seika and Tsumura. Toshiaki Kikuchi has received consultant fees from Takeda Pharmaceutical and the Center for Cognitive Behavioral Therapy and Training. Koichiro Watanabe has received manuscript fees or speaker’s honoraria from Daiichi Sankyo, Eisai, Eli Lilly, GlaxoSmithKline, Janssen Pharmaceutical, Kyowa Pharmaceutical, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka Pharmaceutical, Pfizer, Shionogi, Sumitomo Dainippon Pharma, Takeda Pharmaceutical, and Yoshitomi Yakuhin, has received research/grant support from Astellas Pharma, Daiichi Sankyo, Eisai, MSD, Mitsubishi Tanabe Pharma, Meiji Seika Pharma, Otsuka Pharmaceutical, Pfizer, Shionogi, Sumitomo Dainippon Pharma, and is a consultant for Eisai, Eli Lilly, Kyowa Pharmaceutical, Otsuka Pharmaceutical, Pfizer, Sumitomo Dainippon Pharma, Taisho Toyama Pharmaceutical, and Takeda Pharmaceutical. Reiji Yoshimura has received speaker’s honoraria from Eli Lilly, Janssen, Dainippon Sumitomo, Otsuka, Meiji, Pfizer and Shionogi. The authors report no other conflicts of interest in this work.
References
1. Merikangas KR, Jin R, He J-P, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry. 2011;68(3):241–251. doi:10.1001/archgenpsychiatry.2011.12
2. Pedersen CB, Mors O, Bertelsen A, et al. A comprehensive nationwide study of the incidence rate and lifetime risk for treated mental disorders. JAMA Psychiatry. 2014;71(5):573–581. doi:10.1001/jamapsychiatry.2014.16
3. Bauer M, Glenn T, Alda M, et al. Influence of birth cohort on age of onset cluster analysis in bipolar I disorder. Eur Psychiatry. 2015;30(1):99–105. doi:10.1016/j.eurpsy.2014.10.005
4. Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–1586. doi:10.1016/S0140-6736(13)61611-6
5. Perlis RH, Ostacher MJ, Patel JK, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry. 2006;163(2):217–224. doi:10.1176/appi.ajp.163.2.217
6. Gignac A, McGirr A, Lam RW, Yatham LN. Recovery and recurrence following a first episode of mania: a systematic review and meta-analysis of prospectively characterized cohorts. J Clin Psychiatry. 2015;76(9):1241–1248. doi:10.4088/JCP.14r09245
7. Marwaha S, Durrani A, Singh S. Employment outcomes in people with bipolar disorder: a systematic review. Acta Psychiatr Scand. 2013;128(3):179–193. doi:10.1111/acps.12087
8. Kupfer DJ, Frank E, Grochocinski VJ, Cluss PA, Houck PR, Stapf DA. Demographic and clinical characteristics of individuals in a bipolar disorder case registry. J Clin Psychiatry. 2002;63(2):120–125. doi:10.4088/JCP.v63n0206
9. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association; 2013.
10. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry. 2002;59(6):530–537. doi:10.1001/archpsyc.59.6.530
11. Judd LL, Schettler PJ, Akiskal HS, et al. Long-term symptomatic status of bipolar I vs. bipolar II disorders. Int J Neuropsychopharmacol. 2003;6(2):127–137. doi:10.1017/S1461145703003341
12. Van Rheenen TE, Rossell SL. Objective and subjective psychosocial functioning in bipolar disorder: an investigation of the relative importance of neurocognition, social cognition and emotion regulation. J Affect Disord. 2014;162:134–141. doi:10.1016/j.jad.2014.03.043
13. Rosa AR, González-Ortega I, González-Pinto A, et al. One-year psychosocial functioning in patients in the early vs. late stage of bipolar disorder: functioning in patients with first- vs. multiple-episode bipolar disorder. Acta Psychiatr Scand. 2012;125(4):335–341. doi:10.1111/j.1600-0447.2011.01830.x
14. Oldis M, Murray G, Macneil CA, et al. Trajectory and predictors of quality of life in first episode psychotic mania. J Affect Disord. 2016;195:148–155. doi:10.1016/j.jad.2016.02.018
15. Judd LL, Schettler PJ, Solomon DA, et al. Psychosocial disability and work role function compared across the long-term course of bipolar I, bipolar II and unipolar major depressive disorders. J Affect Disord. 2008;108(1–2):49–58. doi:10.1016/j.jad.2007.06.014
16. Simon GE, Ludman EJ, Unützer J, Operskalski BH, Bauer MS. Severity of mood symptoms and work productivity in people treated for bipolar disorder. Bipolar Disord. 2008;10(6):718–725. doi:10.1111/j.1399-5618.2008.00581.x
17. Solé B, Bonnin CM, Torrent C, et al. Neurocognitive impairment and psychosocial functioning in bipolar II disorder. Acta Psychiatr Scand. 2012;125(4):309–317. doi:10.1111/j.1600-0447.2011.01759.x
18. Dickerson FB, Boronow JJ, Stallings CR, Origoni AE, Cole S, Yolken RH. Association between cognitive functioning and employment status of persons with bipolar disorder. Psychiatr Serv. 2004;55(1):54–58. doi:10.1176/appi.ps.55.1.54
19. Huxley N, Baldessarini RJ. Disability and its treatment in bipolar disorder patients. Bipolar Disord. 2007;9(1–2):183–196. doi:10.1111/j.1399-5618.2007.00430.x
20. Bowie CR, Best MW, Depp C, et al. Cognitive and functional deficits in bipolar disorder and schizophrenia as a function of the presence and history of psychosis. Bipolar Disord. 2018;20(7):604–613. doi:10.1111/bdi.12654
21. Harford TC, Yi H-Y, Grant BF. Other- and self-directed forms of violence and their relationships to DSM-IV substance use and other psychiatric disorders in a national survey of adults. Compr Psychiatry. 2013;54(7):731–739. doi:10.1016/j.comppsych.2013.02.003
22. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry. 2003;60(9):914–920. doi:10.1001/archpsyc.60.9.914
23. World Health Organization. Global health estimates: leading causes of DALYs. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/global-health-estimates-leading-causes-of-dalys.
24. Wyatt RJ, Henter I. An economic evaluation of manic-depressive illness–1991. Soc Psychiatry Psychiatr Epidemiol. 1995;30(5):213–219.
25. Welfare LA. Patient survey. Available from: https://www.mhlw.go.jp/toukei/list/10-20.html.
26. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97–170.
27. Fountoulakis KN, Grunze H, Vieta E, et al. The International College of Neuro-Psychopharmacology (CINP) Treatment Guidelines for Bipolar Disorder in Adults (CINP-BD-2017), part 3: the clinical guidelines. Int J Neuropsychopharmacol. 2017;20(2):180–195.
28. Ostacher MJ, Tandon R, Suppes T. Florida best practice psychotherapeutic medication guidelines for adults with bipolar disorder: a novel, practical, patient-centered guide for clinicians. J Clin Psychiatry. 2016;77(7):920–926. doi:10.4088/JCP.15cs09841
29. National Collaborating Centre for Mental Health (UK). Bipolar Disorder: The NICE Guideline on the Assessment and Management of Bipolar Disorder in Adults, Children and Young People in Primary and Secondary Care. The British Psychological Society and The Royal College of Psychiatrists; 2018.
30. Malhi GS, Bassett D, Boyce P, et al. Royal Australian and New Zealand college of psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry. 2015;49(12):1087–1206.
31. Bonnín CM, Martínez-Arán A, Torrent C, et al. Clinical and neurocognitive predictors of functional outcome in bipolar euthymic patients: a Long-Term, Follow-Up Study. J Affect Disord. 2010;121(1–2):156–160. doi:10.1016/j.jad.2009.05.014
32. Burdick KE, Goldberg JF, Harrow M. Neurocognitive dysfunction and psychosocial outcome in patients with bipolar I disorder at 15-year follow-up. Acta Psychiatr Scand. 2010;122(6):499–506. doi:10.1111/j.1600-0447.2010.01590.x
33. Adachi N, Kubota Y, Goto E, et al. Numbers of patients with mood disorder in JAPC clinics: assumption and interpretation from the collaboration study preliminary survey. J Jpn Assoc Psychiatr Clin. 2016;42:7–9.
34. Kato M, Adachi N, Kubota Y, et al. Clinical features related to rapid cycling and one-year euthymia in bipolar disorder patients: a multicenter treatment survey for bipolar disorder in psychiatric clinics (MUSUBI). J Psychiatr Res. 2020;131:228–234. doi:10.1016/j.jpsychires.2020.09.030
35. Tokumitsu K, Yasui-Furukori N, Adachi N, et al. Real-world clinical features of and antidepressant prescribing patterns for outpatients with bipolar disorder. BMC Psychiatry. 2020;20(1):555. doi:10.1186/s12888-020-02967-5
36. Tsuboi T, Suzuki T, Azekawa T, et al. Factors associated with non-remission in bipolar disorder: the Multicenter Treatment Survey for Bipolar Disorder in Psychiatric Outpatient Clinics (MUSUBI). Neuropsychiatr Dis Treat. 2020;16:881–890. doi:10.2147/NDT.S246136
37. Yasui-Furukori N, Adachi N, Kubota Y, et al. Factors associated with doses of mood stabilizers in real-world outpatients with bipolar disorder. Clin Psychopharmacol Neurosci. 2020;18(4):599–606. doi:10.9758/cpn.2020.18.4.599
38. Adachi N, Azekawa T, Edagawa K, et al. Estimated model of psychotropic polypharmacy for bipolar disorder: analysis using patients’ and practitioners’ parameters in the MUSUBI Study. Hum Psychopharmacol. 2020;36:e2764.
39. Perlis RH, Delbello MP, Miyahara S, et al. Revisiting depressive-prone bipolar disorder: polarity of initial mood episode and disease course among bipolar I systematic treatment enhancement program for bipolar disorder participants. Biol Psychiatry. 2005;58(7):549–553. doi:10.1016/j.biopsych.2005.07.029
40. Goldberg JF, Harrow M, Grossman LS. Course and outcome in bipolar affective disorder: a longitudinal follow-up study. Am J Psychiatry. 1995;152(3):379–384.
41. Ministry of Health, Labour and Welfare. Summary of 2019 employment trends survey results. Available from: https://www.mhlw.go.jp/toukei/itiran/roudou/koyou/doukou/20-2/dl/kekka_gaiyo-01.pdf.
42. Suppes T, Dennehy EB, Gibbons EW. The longitudinal course of bipolar disorder. J Clin Psychiatry. 2000;61(Suppl 9):23–30.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.