")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Relationship Between Long-Term Objectively Measured Physical Activity and Glycemic Control in Type 2 Diabetes Mellitus Patients: A Prospective Cohort Study
Authors Masuda H , Ishiyama D, Yamada M, Iwashima F, Kimura Y, Otobe Y, Tani N, Suzuki M, Nakajima H
Received 22 February 2021
Accepted for publication 10 April 2021
Published 7 May 2021 Volume 2021:14 Pages 2057—2063
DOI https://doi.org/10.2147/DMSO.S307070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Hiroaki Masuda,1,2 Daisuke Ishiyama,2 Minoru Yamada,2 Fumiko Iwashima,3 Yosuke Kimura,2 Yuhei Otobe,2 Naoki Tani,2 Mizue Suzuki,2 Hideki Nakajima1
1Department of Rehabilitation, Toshima Hospital, Tokyo Metropolitan Health and Hospitals Corporation, Tokyo, Japan; 2Graduate School of Comprehensive Human Sciences, University of Tsukuba, Tokyo, Japan; 3Department of Endocrinology and Metabolism, Toshima Hospital, Tokyo Metropolitan Health and Hospitals Corporation, Tokyo, Japan
Correspondence: Hiroaki Masuda
Department of Rehabilitation, Toshima Hospital, Tokyo Metropolitan Health and Hospitals Corporation, 33-1 Sakaecho, Itabashi-ku, Tokyo, 173-0015, Japan
Tel +81-3-5375-1234
Fax +81-3-5944-3534
Email [email protected]
Introduction: Increasing physical activity (PA) improves glycemic control in patients with type 2 diabetes mellitus (T2DM). However, whether long-term objectively measured PA is related to glycemic control remains unclear. The aim of this study was to investigate the relationship between long-term objectively measured PA and glycemic control in T2DM patients.
Research Design and Methods: This prospective cohort study recruited T2DM patients admitted to a hospital-based diabetes management and education program. The primary outcome was glycemic control by hemoglobin A1c at 6 months after discharge. We defined poor glycemic control according to the Japanese Clinical Practice Guidelines. The PA was objectively measured using a three-axis accelerometer during 6 months’ period after discharge. The representative value of PA was the average daily steps during the measurement period and was divided into quartiles. To determine the relationship between the daily steps and poor glycemic control, we performed a multivariate logistic regression analysis.
Results: Ninety-four participants were enrolled in the study. Their median age was 59 years, and 38 (40.0%) of them showed poor glycemic control. Multivariate logistic regression analysis showed that the first (Q1, ≤ 6106 steps/day) and second quartiles (Q2, 6107– 8258 steps/day) had significantly elevated risks of poor glycemic control compared to Q4 (≥ 10,542 steps/day), with odds ratios of 8.55 [95% confidence intervals (CI) =1.43– 51.23] and 15.62 (95% CI 2.63– 92.87), respectively.
Conclusion: We found that lesser PA was significantly associated with poor glycemic control in T2DM patients. This finding may be beneficial for clinicians while providing long-term advice to diabetic patients.
Keywords: glycemic control, long-term, physical activity, type 2 diabetes
Introduction
Type 2 diabetes mellitus (T2DM) is one of the most common diseases associated with multiple serious complications, resulting in considerable morbidity and mortality worldwide.1,2 Previous epidemiological studies of T2DM suggest that the prevalence of T2DM is approximately 8.4%.3 Diabetes leads to various complications, including neuropathy, retinopathy, diabetic kidney disease, and cardiovascular diseases.4,5 The risk of these complications is known to increase with poor glycemic control.6–10 Therefore, better glycemic control by proper diet control, physical activity (PA), and pharmacologic therapy is an important strategy for diabetes management.11,12
Increasing PA is one of the major treatment strategies for T2DM patients13 and has been associated with improved glycemic control,14–17 reduced risk of cardiovascular diseases,18–20 and improved quality of life.21 PA includes elements of structured and unstructured activities. Structured activities include resistance or aerobic exercise, while playing, working, house chores, and recreational activities are unstructured activities.13 Additionally, previous behavioral intervention studies for T2DM patients have reportedly improved glycemic control with increased PA using an educational intervention.17,22–27 However, since most studies investigated PA using either objective devices (accelerometer or pedometer) for a short-period (within a week) or subjective questionnaires,23–26 it remains unclear how long-term objectively measured PA relate to glycemic control in T2DM patients.
The aim of this study was to investigate the relationship between long-term objectively measured PA and glycemic control in T2DM patients. We hypothesized that low PA in the long term is associated with poor glycemic control.
Methods
Study Design and Participants
In this prospective observational cohort study, patients with diabetes admitted to Toshima Hospital between April 2016 and July 2020 for inpatient diabetes management and education programs were enrolled. Patients diagnosed with T2DM and aged 20 years or older were included, while patients with severe cognitive impairment, those in need of gait assistance, restrictions for PA, scheduled for surgery after discharge, refusal to participate in this study, or achieving favorable glycemic control at admission were excluded.28 This study was conducted in accordance with the Declaration of Helsinki, and the study protocol was reviewed and approved by the Ethics Committee of Toshima Hospital (Approval Number: 28-1). All participants provided written informed consent.
Diabetes Management and Education Program
All participants underwent an 11 days hospital-based education program for patients with type 2 diabetes. In this program, participants were admitted to the hospital, and were educated about diabetes management, including diagnosis and pathophysiology, complications, treatments (nutrition therapy, PA, oral hypoglycemic agents, and injectable agents), self-monitoring of blood glucose, hypoglycemia, and sick day rule by an endocrinologist, nurse, pharmacist, dietitian, medical technologist, or physical therapist. After discharge, all participants received several consultations from medical staff such as endocrinologists and dietitians once every 1–2 months. The PA was checked by physical therapists.
Measurements
Physical Activity
Physical activity was objectively measured using a three-axis accelerometer (model MT-KT02DZ, TERUMO, Tokyo, Japan).29 Participants were asked to wear the accelerometer placed in their trouser or coat pockets while they were awake and to take it off for bathing and to use it between admission to a hospital and 6 months after discharge. The number of steps and the time spent walking at a moderate-intensity (3–5.9 metabolic equivalents) were used as indices of physical activity, with a minimum of 16 valid days data (≥ 10 hours of wear time per day) in a month for the analysis.30,31 We calculated the averages of the participants’ daily steps for each period, namely, the period of hospitalization and 6 six-month period after discharge.
Outcome
The outcome measure was glycemic control defined by hemoglobin A1c (HbA1c) at 6 months after discharge. The individual glycemic control goal was set up taking into consideration the age, and the presence of medications, with the risk of severe hypoglycemia, such as insulin, sulfonylurea, and glinides. We defined poor glycemic control as follows according to the Japanese Clinical Practice Guidelines:28 HbA1c ≥ 7.0% for participants aged 64 years or younger; HbA1c ≥ 7.0% for participants aged 65 years or older without the use of medications, potentially associated with severe hypoglycemia; HbA1c ≥ 7.5% for participants aged 65 to 74 years with the use of medications, potentially associated with severe hypoglycemia; or HbA1c ≥ 8.0% for participants aged 75 years or older with the use of medications, potentially associated with severe hypoglycemia.
Other Variables
For demographic and clinical characteristics, the following 17 items were recorded: age, sex, body mass index (BMI), HbA1c, fasting plasma glucose (FPG), 2-h plasma glucose, duration of diabetes, diabetic microvascular complications, diabetic macrovascular complications, diabetes medications, comorbidities, past education hospitalization program, employment status, living alone, survey season, exercise habits, and physical activity before hospitalization. Comorbidities were assessed using the Charlson comorbidity index (CCI).32 Habit of exercise was recorded using the following question: “Do you perform exercise at least twice a week for 30 min over 1 year period ?”.33 We also assessed physical activity in terms of frequency (days per week) and duration (minutes per day) in each of the three specific levels of activity (walking, moderate-intensity activities, or vigorous-intensity activities) using the Short Version of the International Physical Activity Questionnaire (SF-IPAQ).34,35
Data Analysis
Initially, the participants were segregated into 2 groups according to the glycemic control (poor glycemic control and better glycemic control). The characteristics of the participants were compared between the groups by Student’s t-test, Mann–Whitney U-test, and chi-squared test. We then divided the patients into 4 groups according to quartiles of the average daily steps for 6 months’ period after discharge (1st quartile [Q1] - 4th quartile [Q4]). Finally, we used univariate and multivariate logistic regression analyses to assess the relationship between poor glycemic control and daily steps. In the multivariate analysis, we assessed each covariate and adjusted results for the average daily steps during hospitalization and characteristics that were significantly different between poor and better glycemic control. Statistical significance was set at a p-value of < 0.05 for all analyses. Statistical analyses were performed using SPSS software version 25.0 (IBM, Tokyo, Japan).
Results
The clinical and demographic characteristics of the participants are shown in Table 1. Based on the inclusion and exclusion criteria, a total of 125 patients admitted to the diabetes management and education program were included in the analysis, and complete follow-up data was obtained from 94 patients. The median age (IQR) of the study participants was 59.0 (46.0–68.0) years, 27 (28.7%) were female, and the median HbA1c at baseline (IQR) was 8.9 (8.0–10.9) %. The proportions of poor glycemic control group and the better glycemic control group were 40% (n = 38) and 60% (n = 56), respectively. Significant differences were observed in the duration of diabetes (p = 0.010), diabetic microvascular complications (p = 0.013), comorbidities (p = 0.010), past education hospitalization program (p < 0.001), living alone (p = 0.035), and steps for 6 months’ period after discharge (p = 0.009) between the two groups. The average daily steps for 6 months’ period after discharge in the Q4, Q3, Q2, and Q1 groups were ≥ 10,542 steps/day, 8259–10,541 steps/day, 6107–8258 steps/day, and ≤ 6106 steps/day, respectively.
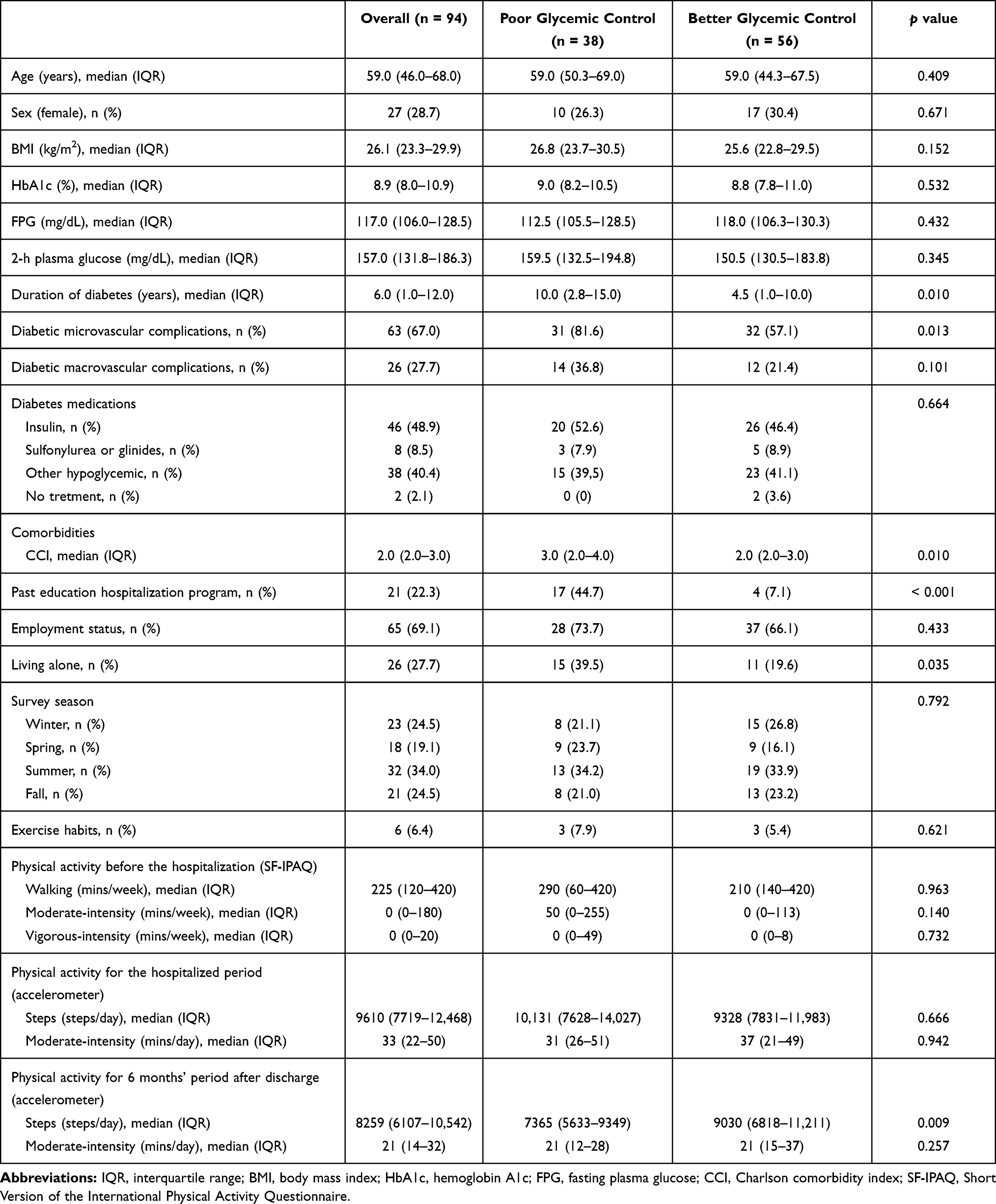 |
Table 1 Characteristics of the Participants |
The results of the logistic regression analysis for the relationship between average daily steps for 6 months’ period after discharge and poor glycemic control are shown in Table 2. Q1 (odds ratio [OR]: 8.55, 95% confidence interval [95% CI]: 1.43–51.23, p = 0.019) and Q2 (OR: 15.62, 95% CI: 2.63–92.87, p = 0.003) groups had significantly elevated risks of poor glycemic control according to multivariate analyses using Q4 as the reference.
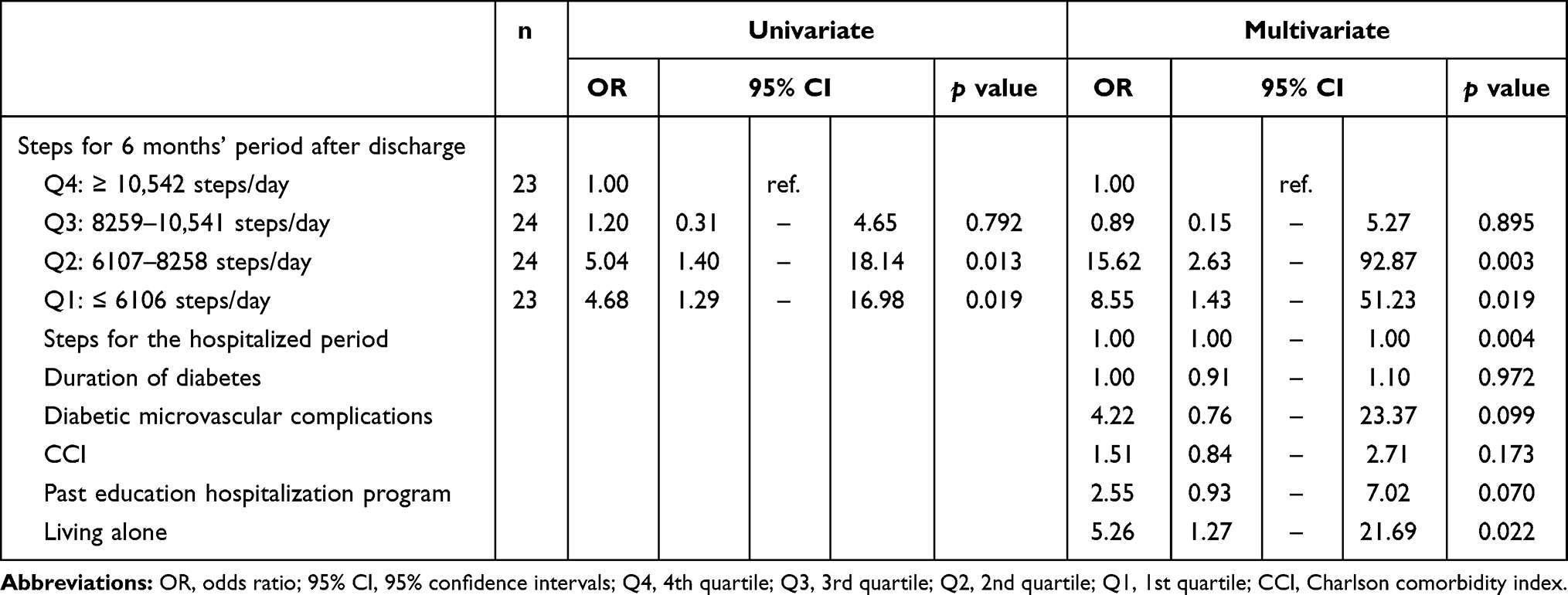 |
Table 2 Logistic Regression Analysis for Poor Glycemic Control |
Discussion
In this prospective cohort study, we investigated the relationship between objectively measured PA for 6 months’ period after discharge and glycemic control in T2DM patients. We found that the Q1 (≤ 6106 steps/day) and Q2 (6107–8258 steps/day) groups had significantly elevated risks of poor glycemic control according to multivariate analyses using Q4 (≥ 10,542) as the reference. This result supports our hypothesis that lower daily steps in the long-term are associated with poor glycemic control in T2DM patients.
Our results showed that T2DM patients with lower daily steps in the long-term tended to have poor glycemic control. Our finding is consistent with previous meta-analysis studies showing that increased PA is associated with improvement in glycemic control in T2DM patients.14,19 Thus, the findings of our study and previous studies both suggest the importance of maintaining a large number of daily steps in the long-term to obtain better glycemic control in T2DM patients.
In this study, glycemic control was influenced by the daily number of steps, but not the duration spent in daily walking at a moderate-intensity level. These parameters seem to suggest conflicting results: the number of daily steps was relatively high, and the duration spent daily walking at a moderate-intensity level was relatively low compared to those in previous studies.24,36–41 These discrepancies between our data and those of previous surveys may be explained by differences in participants’ demographics. Our study included participants who were younger, had higher PA, and had higher employment status than those of previous studies. Thus, it is considered that middle-aged workers, who comprised most of the study participants, maintained better glycemic control by increasing light-intensity PA, such as walking during their commute and moving within the workplace.
The present study has several strengths. Primary strength point is that a relatively long-term objectively measured PA in T2DM patients was assessed. This helped us conclude that lower daily steps in the long-term were significantly associated with poor glycemic control. On the other hand, two limitations of this study warrant mention. First, the influence of nutrition and pharmacologic therapy after discharge was not considered because we could not investigate detailed information about diet and medication after discharge. Glycemic control may have been affected by not only physical activity but also other factors, such as diet and medication; thus, we may have overestimated the impact of physical activity on glycemic control. Second, we enrolled only participants who were middle-aged workers and who underwent the diabetes management and education hospitalization program. Thus, the physical activity was higher in this study than in previous studies, and our findings are generalizable only to middle-aged populations. Further studies with a large longitudinal cohort or clinical trial design from many facilities are required to clarify these limitations.
Conclusion
This study explored the relationship of long-term objectively measured PA and glycemic control in T2DM patients. Our data revealed that lower daily steps in the long-term were significantly affected poor glycemic control in T2DM patients. This finding may be beneficial for clinicians when prescribing PA in the long term.
Acknowledgments
We thank the rehabilitation therapists of our hospitals for their contributions to the data collection. We are also grateful to our laboratory members for their helpful advice on drafts of this manuscript.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Rawshani A, Rawshani A, Franzén S, et al. Mortality and cardiovascular disease in type 1 and type 2 diabetes. N Engl J Med. 2017;376(15):1407–1418. doi:10.1056/NEJMoa1608664
2. Harding JL, Pavkov ME, Magliano DJ, et al. Global trends in diabetes complications: a review of current evidence. Diabetologia. 2019;62:3–16. doi:10.1007/s00125-018-4711-2
3. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
4. American Diabetes Association. 10. Cardiovascular Disease and Risk Management: standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43:S111–34. doi:10.2337/dc20-S010
5. American Diabetes Association. 11. Microvascular complications and foot care: standards of Medical Care in Diabete-2020. Diabetes Care. 2020;43:S135–51. doi:10.2337/dc20-S011
6. Stratton IM, Adler AI, Neil HAW, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. Br Med J. 2000;321:405–412. doi:10.1136/bmj.321.7258.405
7. Lund SS, Rossing P, Vaag AA. Follow-up of intensive glucose control in type 2 diabetes [1]. N Engl J Med. 2009;360:416–418. doi:10.1056/NEJMc082275
8. Roussel R, Steg PG, Mohammedi K, et al. Prevention of cardiovascular disease through reduction of glycaemic exposure in type 2 diabetes: a perspective on glucose-lowering interventions. Diabetes Obes Metab. 2018;20:238–244. doi:10.1111/dom.13033
9. Zoungas S, Arima H, Gerstein HC, et al. Effects of intensive glucose control on microvascular outcomes in patients with type 2 diabetes: a meta-analysis of individual participant data from randomised controlled trials. Lancet Diabetes Endocrinol. 2017;5:431–437. doi:10.1016/S2213-8587(17)30104-3
10. Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995;28(2):103–117. doi:10.1016/0168-8227(95)01064-K
11. American Diabetes Association. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43:S48–65. doi:10.2337/dc20-S005
12. American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43:S98–110. doi:10.2337/dc20-S009
13. Colberg SR, Sigal RJ, Yardley JE, et al. Physical activity/exercise and diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2016;39(11):2065–2079. doi:10.2337/dc16-1728
14. Pai LW, Li TC, Hwu YJ, et al. The effectiveness of regular leisure-time physical activities on long-term glycemic control in people with type 2 diabetes: a systematic review and meta-analysis. Diabetes Res Clin Pract. 2016;113:77–85. doi:10.1016/j.diabres.2016.01.011
15. Boulé NG, Haddad E, Kenny GP, et al. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of controlled clinical trials. J Am Med Assoc. 2001;286:1218–1227. doi:10.1001/jama.286.10.1218
16. Boniol M, Dragomir M, Autier P, et al. Physical activity and change in fasting glucose and HbA1c: a quantitative meta-analysis of randomized trials. Acta Diabetol. 2017;54:983–991. doi:10.1007/s00592-017-1037-3
17. Umpierre D, Ribeiro PAB, Kramer CK, et al. Physical activity advice only or structured exercise training and association with HbA 1c levels in type 2 diabetes: a systematic review and meta-analysis. JAMA. 2011;305(17):1790–1799. doi:10.1001/jama.2011.576
18. Figueira FR, Umpierre D, Cureau FV, et al. Association between physical activity advice only or structured exercise training with blood pressure levels in patients with type 2 diabetes: a systematic review and meta-analysis. Sports Med. 2014;44:1557–1572. doi:10.1007/s40279-014-0226-2
19. Qiu S, Cai X, Schumann U, et al. Impact of walking on glycemic control and other cardiovascular risk factors in type 2 diabetes: a meta-analysis. PLoS One. 2014;9(10):e109767. doi:10.1371/journal.pone.0109767
20. Boulé NG, Kenny GP, Haddad E, et al. Meta-analysis of the effect of structured exercise training on cardiorespiratory fitness in type 2 diabetes mellitus. Diabetologia. 2003;46:1071–1081. doi:10.1007/s00125-003-1160-2
21. Cai H, Li G, Zhang P, et al. Effect of exercise on the quality of life in type 2 diabetes mellitus: a systematic review. Qual Life Res. 2017;26:515–530. doi:10.1007/s11136-016-1481-5
22. Avery L, Flynn D, van Wersch A, et al. Changing physical activity behavior in type 2 diabetes: a systematic review and meta-analysis of behavioral interventions. Diabetes Care. 2012;35:2681–2689. doi:10.2337/dc11-2452
23. Balducci S, D’Errico V, Haxhi J, et al. Effect of a behavioral intervention strategy for adoption and maintenance of a physically active lifestyle: the Italian diabetes and exercise study 2 (IDES-2): a randomized controlled trial. Diabetes Care. 2017;40:1444–1452. doi:10.2337/dc17-0594
24. Dasgupta K, Rosenberg E, Joseph L, et al. Physician step prescription and monitoring to improve ARTERial health (SMARTER): a randomized controlled trial in patients with type 2 diabetes and hypertension. Diabetes Obes Metab. 2017;19:695–704. doi:10.1111/dom.12874
25. Allen NA, Fain JA, Braun B, et al. Continuous glucose monitoring counseling improves physical activity behaviors of individuals with type 2 diabetes: a randomized clinical trial. Diabetes Res Clin Pract. 2008;80:371–379. doi:10.1016/j.diabres.2008.01.006
26. Plotnikoff RC, Pickering MA, Glenn N, et al. The effects of a supplemental, theory-based physical activity counseling intervention for adults with type 2 diabetes. J Phys Act Health. 2011;8:944–954. doi:10.1123/jpah.8.7.944
27. Kim SH, Lee SJ, Kang ES, et al. Effects of lifestyle modification on metabolic parameters and carotid intima-media thickness in patients with type 2 diabetes mellitus. Metabolism. 2006;55:1053–1059. doi:10.1016/j.metabol.2006.03.017
28. Haneda M, Noda M, Origasa H, et al. Japanese Clinical Practice Guideline for Diabetes 2016. Diabetol Int. 2018. doi:10.1111/jdi.12810
29. Morita E, Yokoyama H, Imai D, et al. Aerobic exercise training with brisk walking increases intestinal bacteroides in healthy elderly women. Nutrients. 2019;11:868. doi:10.3390/nu11040868
30. Troiano RP, Berrigan D, Dodd KW, et al. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40:181–188. doi:10.1249/mss.0b013e31815a51b3
31. Aoyagi Y, Shephard RJ. Habitual physical activity and health in the elderly: the Nakanojo Study. Geriatr Gerontol Int. 2010;10:S236–S243. doi:10.1111/j.1447-0594.2010.00589.x
32. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383. doi:10.1016/0021-9681(87)90171-8
33. Fujihara K, Matsubayashi Y, Harada Yamada M, et al. Combination of diabetes mellitus and lack of habitual physical activity is a risk factor for functional disability in Japanese. BMJ Open Diabetes Res Care. 2020;8:1–5. doi:10.1136/bmjdrc-2019-000901
34. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-Country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
35. Cleland C, Ferguson S, Ellis G, et al. Validity of the International Physical Activity Questionnaire (IPAQ) for assessing moderate-to-vigorous physical activity and sedentary behaviour of older adults in the United Kingdom. BMC Med Res Methodol. 2018;18. doi:10.1186/s12874-018-0642-3
36. de Greef K, Deforche B, Tudor-Locke C, et al. Increasing physical activity in Belgian type 2 diabetes patients: a three-arm randomized controlled trial. Int J Behav Med. 2011;18:188–198. doi:10.1007/s12529-010-9124-7
37. Shenoy S, Guglani R, Sandhu JS. Effectiveness of an aerobic walking program using heart rate monitor and pedometer on the parameters of diabetes control in Asian Indians with type 2 diabetes. Prim Care Diabetes. 2010;4:41–45. doi:10.1016/j.pcd.2009.10.004
38. Mueller MJ, Tuttle LJ, Lemaster JW, et al. Weight-bearing versus nonweight-bearing exercise for persons with diabetes and peripheral neuropathy: a randomized controlled trial. Arch Phys Med Rehabil. 2013;94:829–838. doi:10.1016/j.apmr.2012.12.015
39. Alghafri TS, Alharthi SM, Al-Farsi Y, et al. “MOVEdiabetes”: a cluster randomized controlled trial to increase physical activity in adults with type 2 diabetes in primary health in Oman. BMJ Open Diabetes Res Care. 2018;6:e000605. doi:10.1136/bmjdrc-2018-000605
40. Kirk A, Mutrie N, Macintyre P, et al. Increasing physical activity in people with type 2 diabetes. Diabetes Care. 2003;26(4):1186–1192. doi:10.2337/diacare.26.4.1186
41. Sperl-Hillen JA, Beaton S, Fernandes O, et al. Comparative effectiveness of patient education methods for type 2 diabetes: a randomized controlled trial. Arch Intern Med. 2011;171:2001–2010. doi:10.1001/archinternmed.2011.507
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.