")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Relationship Between Hyperuricemia-Waist Phenotype and Obstructive Sleep Apnea in Type 2 Diabetes Mellitus
Received 14 February 2023
Accepted for publication 18 May 2023
Published 23 May 2023 Volume 2023:16 Pages 1505—1513
DOI https://doi.org/10.2147/DMSO.S408637
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Na Lu,1 Fuzai Yin1,2
1Department of Internal Medicine, Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Department of Endocrinology, The First Hospital of Qinhuangdao, Qinhuangdao, Hebei, People’s Republic of China
Correspondence: Fuzai Yin, Hebei Medical University, Shijiazhuang, Hebei Province, People’s Republic of China, Email [email protected]
Objective: This study aimed to propose the hyperuricemia-waist (HUAW) phenotype and investigate the relationship between the HUAW phenotype and obstructive sleep apnea (OSA) in type 2 diabetes mellitus (T2DM).
Methods: We enrolled 255 patients with T2DM (165 male and 90 female) from the First Hospital of Qinhuangdao. The sleep test was performed, and serum uric acid (UA) levels and waist circumference (WC) were calculated. The HUAW phenotype was defined as serum UA concentrations ≥ 420 μmol/L and WC ≥ 90 cm (male) and ≥ 85 cm (female). The participants were categorized into four phenotype groups based on the mentioned cutoffs: normal WC and normal UA concentrations (group A); normal WC and elevated UA concentrations (group B); enlarged WC and normal UA concentrations (group C); and enlarged WC and elevated UA concentrations (group D). Among these participants, 17.6% were characterized by the HUAW phenotype, 80.0% had OSA, and 47.0% had moderate-to-severe OSA. The prevalence of OSA was 43.4%, 71.4%, 89.7%, and 97.8% in groups A, B, C, and D, respectively. The prevalence of moderate-to-severe OSA was 7.5%, 28.6%, 56.9%, and 72.7% in groups A, B, C, and D, respectively. After adjusting for age, sex, duration of diabetes, glycosylated hemoglobin A1c, smoking, and drinking, the HUAW phenotype was found to be significantly associated with OSA and moderate-to-severe OSA.
Conclusion: The present study proposed the HUAW phenotype and demonstrated that in T2DM, the HUAW phenotype was associated with OSA, especially with moderate-to-severe OSA. Unlike T2DM without the HUAW phenotype, T2DM with the HUAW phenotype showed a significantly higher prevalence of OSA, especially moderate-to-severe OSA. Thus, early sleep studies should be routinely examined in individuals with T2DM who display the HUAW phenotype.
Keywords: hyperuricemia, obstructive sleep apnea, type 2 diabetes mellitus, waist circumference
Introduction
Obstructive sleep apnea (OSA), hyperuricemia, and obesity have been recognized as common comorbidities of type 2 diabetes mellitus (T2DM). Over the past decades, epidemiological and pathophysiological studies have found that OSA is associated with the development of T2DM and increases the risk of developing diabetes-related complications.1–3 Several studies reported that OSA treatment might be essential in preventing diabetes progression.4,5 However, OSA is usually underdiagnosed in T2DM.6 Therefore, efforts should be made to detect OSA early in T2DM so as to intervene early and ultimately improve health and quality of life. Obesity and serum uric acid (SUA) level are common indicators of OSA.
First, previous epidemiological studies have reported a relationship between obesity and sleep disturbances. There is a very high prevalence of OSA in patients with obesity and, conversely, a high prevalence of obesity in patients with OSA. Research suggests that 60–90% of patients with OSA are obese, while the prevalence of OSA in obese populations is approximately 40%.7 Obesity is a major risk factor for OSA. Compared with stable weight, a 10% increase in weight predicted a 32% increase in the apnea-hypopnea index (AHI). A 10% weight gain predicted a sixfold increase in the risk of developing moderate-to-severe sleep-disordered breathing.8 OSA may cause sleep deprivation, daytime somnolence, and disrupted metabolism, leading to worsening obesity.9,10 Waist circumference (WC) is a simple, inexpensive, widely used, and noninvasive tool to diagnose obesity, especially in patients with T2DM.11
Second, multiple studies suggested the close relationships of OSA with serum UA levels and gout. OSA causes hypoxic stress and can trigger UA overproduction.12 The comorbid disease burden and associated chronic inflammation and oxidative stress in hyperuricemia can be a risk factor for developing OSA.13 Multiple observational epidemiological studies have reported that patients with OSA have higher levels of serum UA; also, serum UA (SUA) is a marker of oxidative stress and tissue hypoxia in patients with OSA.14–16 Since the SUA level is an easily measurable indicator, the elevation of SUA levels as a clinical manifestation of OSA may trigger screening for OSA in turn.
As both SUA levels and obesity are associated with OSA, we hypothesized that the hyperuricemia-waist (HUAW) phenotype, defined as hyperuricemia and increased WC, might indicate the risk of OSA in T2DM. No previous study proposed the HUAW phenotype. Hence, this study aimed to analyze the relationship between the HUAW phenotype and OSA in T2DM.
Methods
A cross-sectional study was conducted after obtaining informed consent from patients with T2DM. All participants were recruited from the First Hospital of Qinhuangdao. They included men and women aged more than 18 years, with a diagnosis of T2DM (based on the American Diabetes Association diagnostic criteria).17 The exclusion criteria were as follows: (1) participants with type 1 diabetes; (2) participants with clinical evidence of other forms of endocrinopathy, such as Cushing’s syndrome, hyperthyroidism, and so forth; (3) participants taking medications known to affect UA metabolisms, such as febuxostat, benzbromarone, and allopurinol; (4) participants with moderate-to-severe OSA who had continuous positive airway pressure treatment or upper airway surgery and those with mild OSA who had oral appliance treatment; (5) patients with unstable cardiopulmonary disease such as congestive heart failure or intrinsic pulmonary disease; (6) patients with sleep disorders other than OSA, such as central sleep apnea syndrome and narcolepsy; (7) pregnancy; and (8) patients with acute and chronic inflammation. This study was approved by the ethics committee of the First Hospital of Qinhuangdao. All participants provided written informed consent before study initiation. This study complied with the Declaration of Helsinki.
Measurements
WC was accurately measured to the nearest 0.1 cm at the midway point between the lowest rib and the top of the iliac crest. All measurements were taken twice, and the two measurements were averaged for analysis. The sociodemographic variables were recorded, including age, sex, duration of diabetes, and smoking and drinking status.
Glycosylated hemoglobin A1c (HbA1c) was measured using high-performance liquid chromatography. The SUA level was measured by the uricase method.
All participants underwent the sleep test with Philips Respironics Alice NightOne Device (Respironics, Inc, USA) after hospitalization. The device provided seven data channels, including body position, pressure flow, snore, respiratory effort, SpO2, pleth, and pulse rate. The AHI was the average number of apneas/hypopneas per hour of sleep. The severity of OSA was categorized as non-, mild, moderate, and severe for AHI <5, 5–15, 15–30, and ≥30 times per hour, respectively.18 The severity of hypoxemia was categorized as non-, mild, moderate, and severe for the lowest oxygen saturation (LSaO2) during sleep≥90%, 90%–85%, 80%–85%, and <0%, respectively.19
Definition
The HUAW phenotype was defined as SUA concentrations ≥420 μmol/L and WC ≥90 cm (male) and 85 cm (female). The participants were categorized into four phenotype groups based on the mentioned cutoffs: normal WC (<90 cm for male and <85 cm for female) and normal SUA concentrations (<420 μmol/L) (group A); normal WC (<90 cm for male and <85 cm for female) and elevated SUA concentrations (≥420 μmol/L) (group B); enlarged WC (≥90 cm for male and ≥85 cm for female) and normal SUA concentrations (<420 μmol/L) (group C); and enlarged WC (≥90 cm for male and ≥85 cm for female) and elevated SUA concentrations (≥420 μmol/L) (group D).
Statistical Analyses
All analyses were performed using the SPSS 23 statistical software (SPSS 23 for Windows; SPSS, Inc., IL, USA). Normal-distribution-based numerical variables were reported as mean ± standard deviation. Comparisons were conducted between groups using analysis of variance. Non-normal-distribution-based numerical variables were reported as median and quartiles. The groups were compared using the Mann–Whitney U-test. Prevalence data were compared using χ2 analysis. Multiple logistic regression models were used for modeling the relationships between the HUAW phenotype and OSA. A P value <0.05 indicated a statistically significant difference.
Results
This study enrolled 255 patients with type 2 diabetes (165 male and 90 female), aged 52.05 ± 12.37 years, with the duration of diabetes 4.00 (1.00–9.00) years. Among these patients, 17.6% were characterized by the HUAW phenotype, 80.0% had OSA, and 47.0% had moderate-to-severe OSA. The HUAW phenotype was higher in male patients than in female patients (28.9% vs 8.9%, P < 0.05).
Table 1 shows the characteristics of subgroups classified based on WC and UA levels. The age, duration of diabetes, HbA1c, and smoking were similar in the four groups (P > 0.05). The UA levels, WC, and AHI were significantly higher in group D than in groups A, B, and C (P < 0.05). The level of LSaO2 was significantly lower in group D than in groups A, B, and C (P < 0.05). The prevalence of OSA was significantly higher in group D than in groups A and B (group A, 43.4%; group B, 71.4%; group C, 89.7%; group D, 97.8%, P < 0.05). The prevalence of hypoxemia was significantly higher in group D than in group A (95.6% vs 69.8%, P < 0.05). The prevalence of moderate-to-severe OSA was significantly higher in group D than in groups A, B, and C (group A 7.5%; group B 28.6%; group C 56.9%; group D 72.7%, P < 0.05). The prevalence of moderate-to-severe hypoxemia was significantly higher in group D than in groups A, B, and C (group A 45.3%; group B 38.1%; group C 67.6%; group D 84.4%, P < 0.05).
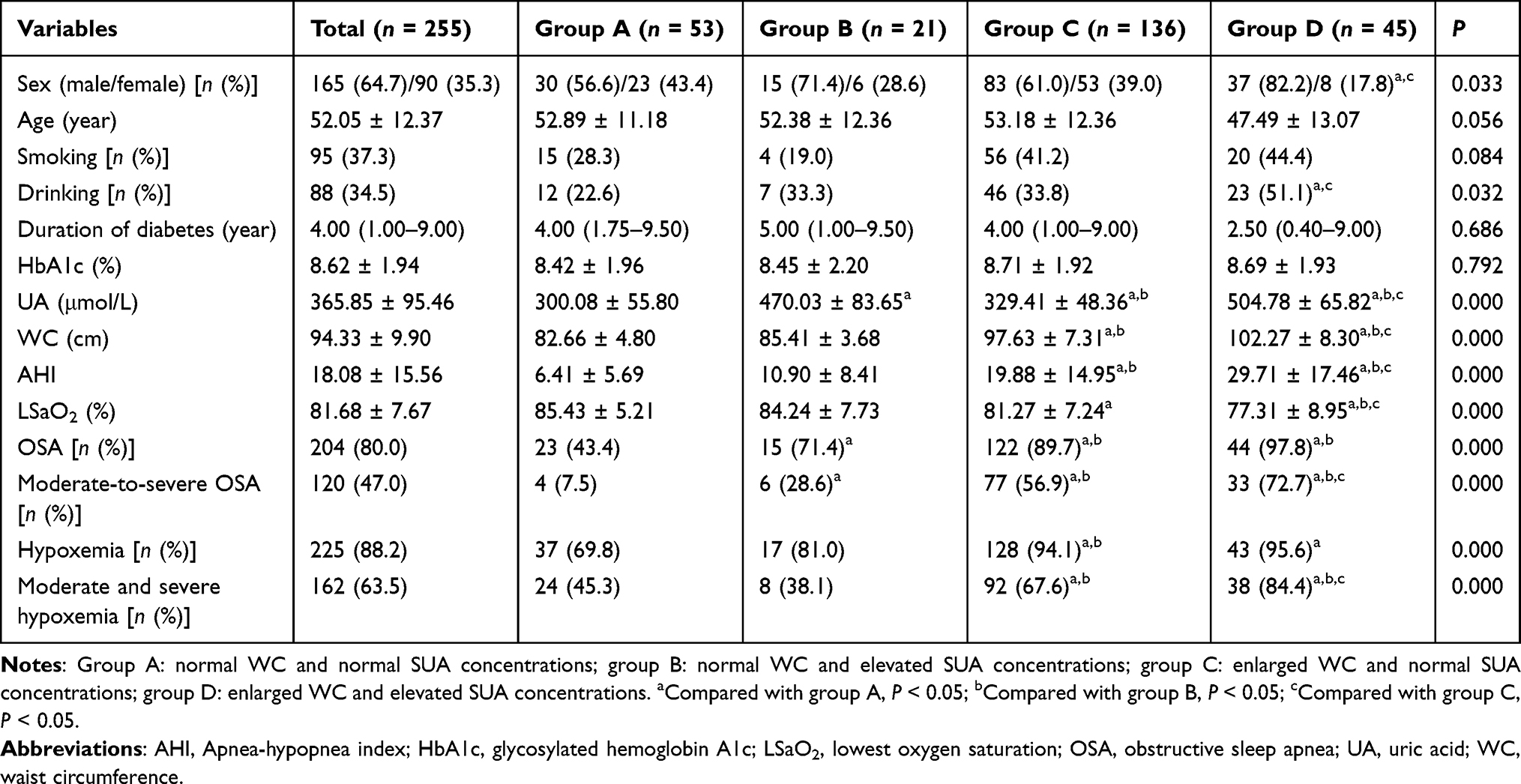 |
Table 1 Characteristics of Participants by Phenotypes of SUA Concentrations and WC |
Figures 1 and 2 show the composition of different severities of OSA in different groups by phenotypes of serum UA concentrations and WC. The prevalence of OSA was found to increase gradually from group A to group D. The proportion of moderate-to-severe OSA gradually increased.
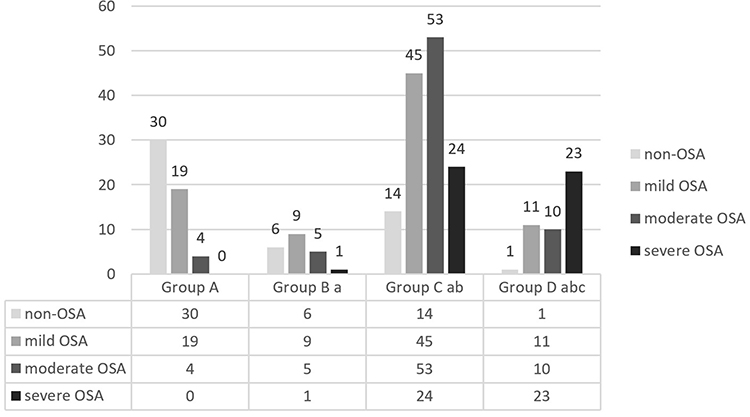 |
Figure 1 Composition of different severities of OSA in different groups by phenotypes of serum UA levels and WC (n). Notes: Group A: normal WC and normal serum UA levels; group B: normal WC and elevated SUA levels; group C: enlarged WC and normal SUA levels; group D: enlarged WC and elevated SUA levels. a: compared with group A, P < 0.05; b: compared with group B, P < 0.05; c: compared with group C, P < 0.05. |
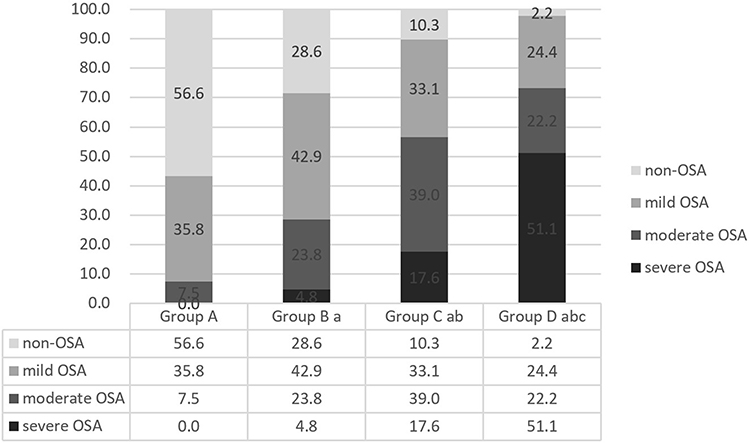 |
Figure 2 Composition of different severities of OSA in different groups by phenotypes of SUA levels and WC (%). Notes: Group A: normal WC and normal SUA levels; group B: normal WC and elevated SUA levels; group C: enlarged WC and normal SUA levels; group D: enlarged WC and elevated SUA levels. a: compared with group A, P < 0.05; b: compared with group B, P < 0.05; c: compared with group C, P < 0.05. |
Table 2 shows the adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for the risk of OSA according to the phenotypes of serum UA concentrations and WC. After adjusting for age, sex, duration of diabetes, HbA1c, smoking, and drinking, groups B, C, and D were significantly associated with OSA, defined as AHI ≥5 events/h, compared with group A (group B: OR 3.678, 95% CI 1.150–11.760, P = 0.028; group C: OR 12.112, 95% CI 5.342–27.463, P = 0.000; group D: OR 82.387, 95% CI 9.873–687.495, P = 0.000).
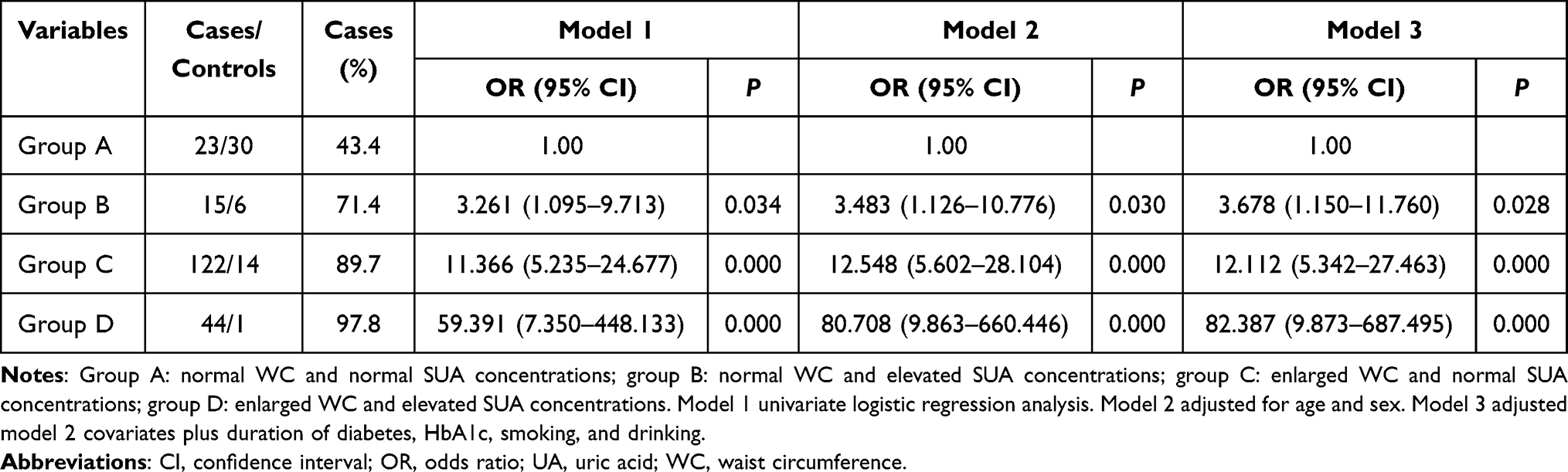 |
Table 2 Adjusted ORs and 95% CIs for OSA (AHI ≥5) Risk According to Phenotypes of Serum UA Concentrations and WC |
Table 3 shows the adjusted ORs and 95% CIs for the risk of moderate-to-severe OSA according to the phenotypes of serum UA concentrations and WC. After adjusting for age, sex, duration of diabetes, HbA1c, smoking, and drinking, groups B, C, and D were significantly associated with moderate-to-severe OSA, defined as AHI ≥15 events/h, compared with group A (group B: OR 4.744, 95% CI 1.117–20.146, P = 0.035; group C: OR 21.286, 95% CI 6.847–66.169, P = 0.000; group D: OR 55.110, 95% CI 14.854–204.462, P = 0.000; Table 3).
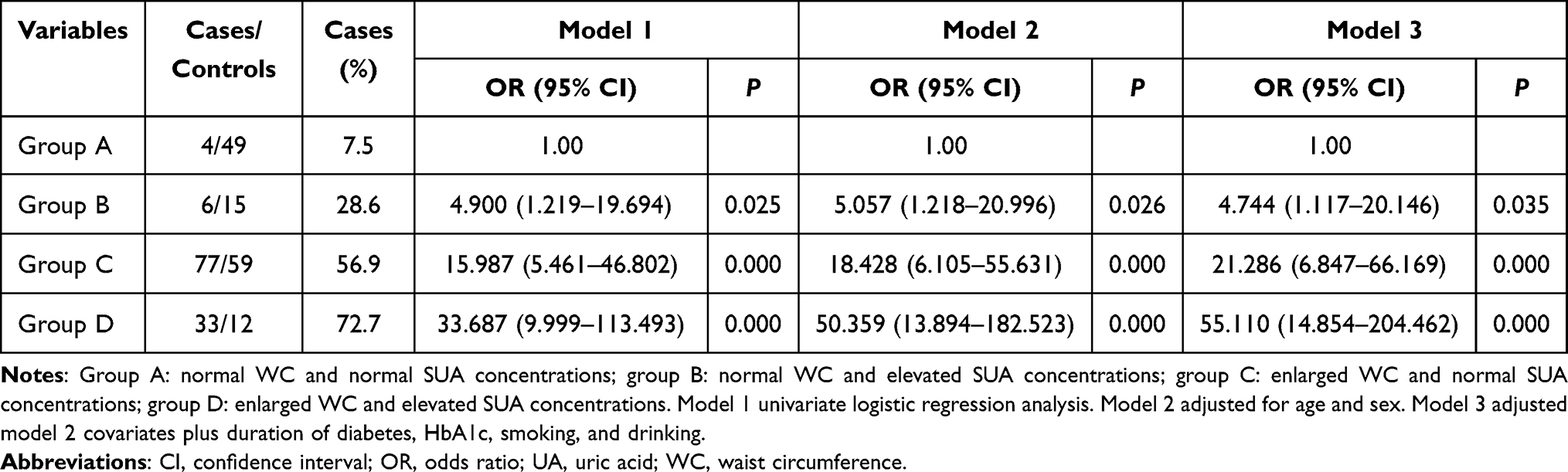 |
Table 3 Adjusted ORs and 95% CIs for Moderate-to-Severe OSA (AHI ≥15) Risk According to Phenotypes of Serum UA Concentrations and WC |
Table 4 shows the findings of multivariable logistic regression analyses for OSA and moderate-to-severe OSA. After adjusting for sex, age, smoking, drinking, duration of diabetes, and HbA1c, both UA and WC were the risk factors for OSA and moderate-to-severe OSA in T2DM.
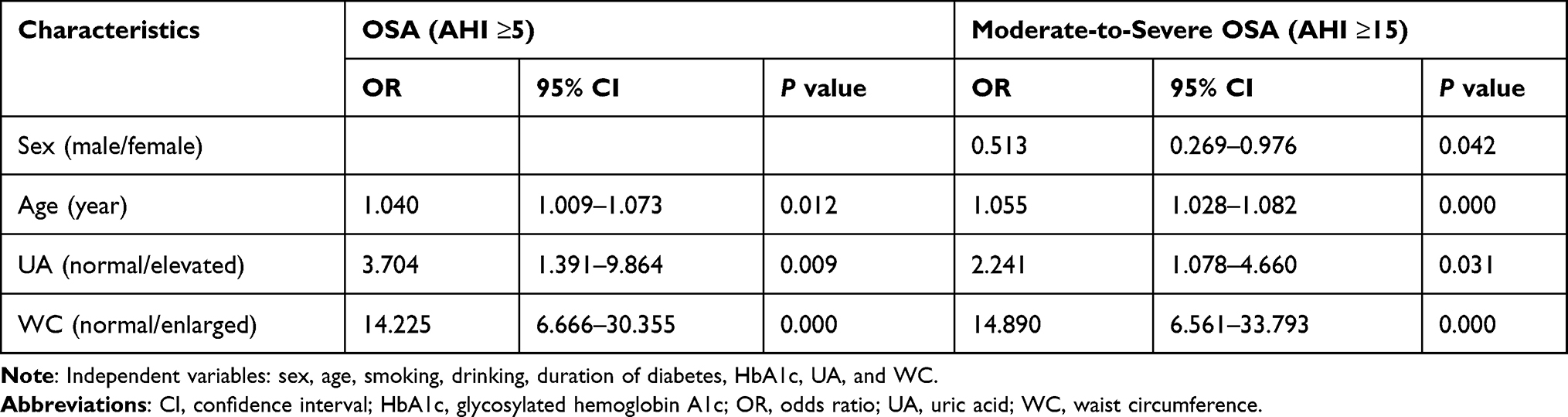 |
Table 4 Multivariable Logistic Regression Analysis for OSA |
Discussion
No previous study proposed the HUAW phenotype and explored the relationship between the HUAW phenotype and OSA in T2DM. In this study, we defined the HUAW phenotype as SUA concentrations ≥420 μmol/L and WC ≥90 cm (male) and ≥85 cm (female). The diagnostic criteria were based on the definition of hyperuricemia proposed by the Chinese Society of Endocrinology and the definition of metabolic syndrome proposed by the Chinese Diabetes Society.20,21 The diagnostic criteria were race specific and based on epidemiological evidence. Our study showed that 17.6% of patients with T2DM were characterized by the HUAW phenotype, 80.0% had OSA, and 47.0% had moderate-to-severe OSA. Patients with T2DM had a high prevalence of OSA. Patients with the HUAW phenotype had a significantly higher prevalence of OSA than those without the HUAW phenotype. Almost all patients with the HUAW phenotype had OSA, and more than half had moderate-to-severe OSA. The HUAW phenotype was significantly associated with an increased OSA risk in T2DM. These findings remained significant after model adjustment.
OSA is a common and underdiagnosed medical condition characterized by repeated partial and complete upper airway collapse and oxygen desaturation during sleep. It is closely correlated with T2DM. Intermittent hypoxia and sleep fragmentation in patients with OSA can induce sympathetic nervous system activation, systemic inflammation, oxidative stress, appetite-regulating hormone alterations, and hypothalamic–pituitary–adrenal axis activation, which, in turn, promote the development of insulin resistance and T2DM.22,23 Several studies revealed a significantly higher prevalence of OSA in patients with T2DM compared with the general population. In a substudy of the Look AHEAD (Action for Health in Diabetes) trial, the prevalence of OSA in T2DM was 86% and that of moderate-to-severe OSA was 53%.24 A study of consecutive patients with T2DM referred to a diabetes clinic reported the prevalence of moderate-to-severe OSA as 36%.25 In the Sleep Heart Health Study, 23.8% of participants had moderate or severe OSA.26 However, in this study, the prevalence of OSA was 80%, and the prevalence of moderate-to-severe OSA was 47%. The treatment of the sleep disorder might be possible to prevent diabetes progression.4,5 Therefore, efforts should be made to diagnose and treat sleep disorders in T2DM so as to ultimately improve health and, therefore, quality of life. However, clinically, patients with T2DM are not positively screened for OSA.27 The diagnosis and screening of OSA rely on polysomnography28 or portable home-based cardio-respiratory Type III devices.29 The limited availability of these devices poses a major constraint in diagnosing and screening OSA. Popularizing the use of sleep studies in all patients with T2DM in many medical institutions, such as clinics and even hospitals, is a challenging task. For OSA intervention, detecting high-risk groups and performing targeted sleep monitoring is important, which requires a simple, inexpensive, and accurate tool for identifying OSA. The present study demonstrated that the HUAW phenotype was a helpful tool for detecting the presence of OSA in T2DM.
Obesity is one of the major risk factors for OSA30 and is also commonly found in patients with T2DM. OSA may contribute to obesity or excess weight through increased sympathetic activation, sleep deprivation, and changes in leptin, ghrelin, and orexin levels, thus increasing caloric intake.9,10 Obesity can increase fat deposits around the upper airway, narrow the upper airway, and diminish the activity of the muscles in this region, collapsing the airway during sleep and thus resulting in OSA.9,31–33 Also, central obesity may indirectly cause OSA due to restricted thoracic volume, resulting in diminished airway caliber or obesity-related hypoventilation.34 Visceral fat has been associated with an increased risk of T2DM in those with OSA.35,36 In another study, waist but not neck circumference was seen as an associated risk factor for OSA in obese patients with T2DM.24 Previous studies demonstrated that waist might serve as a useful predictor for OSA in patients with T2DM.
Hyperuricemia is an independent risk factor for developing T2DM.37 Previous studies observed a relationship between OSA and increased SUA levels.14,16,38–41 A meta-analysis of 18 studies, comprising 157,607 patients (32,395 with OSA and 125,212 without OSA) and 12,262 patients with gout, showed that SUA levels were higher in patients with OSA and the relationship between OSA and SUA levels was quite robust.42 UA has been linked with OSA mainly through oxidative stress as a common pathway. It has been postulated that recurrent hypoxia in OSA leads to increased adenosine triphosphate degradation and associated purine catabolism that may increase UA levels.12 However, the effect of OSA therapy on UA levels yielded conflicting results. A meta-analysis, published in 2019, involving 5 studies with 270 patients, showed no change in UA levels before and after continuous positive airway pressure (CPAP) treatment in patients with OSA.43 However, after 2 years, a retrospective study, including 604 patients with OSA, showed that UA levels decreased significantly after CPAP treatment for 6 months [median: 7.0 (6.4, 8.1) mg/dL vs 6.4 (6.2, 6.8) mg/dL].44 As both diabetes and OSA were related to SUA levels, the measurement of SUA level might be a useful marker of oxidative stress of OSA among patients with T2DM.
In the present study, the levels of AHI gradually increased, the levels of LSaO2 gradually decreased, and the prevalence of OSA and moderate-to-severe OSA gradually increased from group A to group D. The present results illustrated that when patients with T2DM had both enlarged WC and elevated SUA levels, a superimposed effect on OSA might exist. Patients with T2DM having the HUAW phenotype should undergo early sleep testing. Interestingly, the AHI and the prevalence of OSA were significantly higher in group C than in group B. This might be attributed to the stronger relationships between obesity and OSA compared with the relationship between hyperuricemia and OSA.
The strengths of this study included its first proposal of HUAW phenotype and exploration of the relationship between HUAW phenotype and OSA. However, the study had several potential limitations. First, we could not identify the causal relationship between HUAW phenotype and OSA because of the cross-sectional design of this study. Second, polysomnography is the gold standard for diagnosing OSA. However, limited by the conditions of this study, the assessment of overnight sleep quality was performed using the Alice NightOne home sleep testing device. Third, the sample size of this study was small, leading to low accuracy of prevalence and relationships and low reproducibility of results. The confidence interval is wide in Table 2 and Table 3, which might be due to the small sample size. A larger-sample study should be conducted in the future to confirm the relationship between the HUAW phenotype and OSA. Fourth, all participants were recruited from North China, and all participants had T2DM. This was a highly selected population, and the proportion of patients with OSA was extremely high. These factors limited the generalizability of the results to other populations. Finally, some confounding factors were not controlled.
Conclusions
The present study proposed the HUAW phenotype and demonstrated that the HUAW phenotype in T2DM was associated with OSA. Compared with T2DM without the HUAW phenotype, T2DM with the HUAW phenotype showed a significantly higher prevalence of OSA, especially moderate-to-severe OSA. Hence, more attention should be given to UA levels and WC in the clinical screening of patients with T2DM. Early sleep studies should be routinely performed in patients with T2DM having the HUAW phenotype.
Data Sharing Statement
The datasets used and analyzed in this study are available from Fuzai Yin, the corresponding author, on reasonable request.
Ethics Approval and Consent to Participate
This study followed the principles of the Declaration of Helsinki and was approved by the ethics committee of the First Hospital of Qinhuangdao. Written informed consent was obtained from all participants.
Disclosure
The authors report no conflicts of interest related to this study.
References
1. Wang X, Bi Y, Zhang Q, Pan F. Obstructive sleep apnoea and the risk of type 2 diabetes: a meta-analysis of prospective cohort studies. Respirology. 2013;18(1):140–146. PMID: 22988888. doi:10.1111/j.1440-1843.2012.02267.x
2. Pallayova M, Banerjee D, Taheri S. Novel insights into metabolic sequelae of obstructive sleep apnoea: a link between hypoxic stress and chronic diabetes complications. Diabetes Res Clin Pract. 2014;104(2):197–205. PMID: 24485855. doi:10.1016/j.diabres.2014.01.007
3. Reutrakul S, Mokhlesi B. Obstructive sleep apnea and diabetes: a state of the art review. Chest. 2017;152(5):1070–1086. PMID: 28527878; PMCID: PMC5812754. doi:10.1016/j.chest.2017.05.009
4. Schipper SBJ, Van Veen MM, Elders PJM, et al. Sleep disorders in people with type 2 diabetes and associated health outcomes: a review of the literature. Diabetologia. 2021;64(11):2367–2377. PMID: 34401953; PMCID: PMC8494668.10. doi:10.1007/s00125-021-05541-0
5. Faria A, Laher I, Fasipe B, Ayas NT. Impact of obstructive sleep apnea and current treatments on the development and progression of type 2 diabetes. Curr Diabetes Rev. 2022;18(9):e160222201169. PMID: 35170415. doi:10.2174/1573399818666220216095848
6. Heffner JE, Rozenfeld Y, Kai M, Stephens EA, Brown LK. Prevalence of diagnosed sleep apnea among patients with type 2 diabetes in primary care. Chest. 2012;141(6):1414–1421. PMID: 22095313. doi:10.1378/chest.11-1945
7. Svatikova A, Wolk R, Gami AS, Pohanka M, Somers VK. Interactions between obstructive sleep apnea and the metabolic syndrome. Curr Diab Rep. 2005;5(1):53–58. PMID: 15663918. doi:10.1007/s11892-005-0068-2
8. Peppard PE, Young T, Palta M, Dempsey J, Skatrud J. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA. 2000;284(23):3015–3021. PMID: 11122588. doi:10.1001/jama.284.23.3015
9. Pillar G, Shehadeh N. Abdominal fat and sleep apnea: the chicken or the egg? Diabetes Care. 2008;31(7):S303–9. PMID: 18227501; PMCID: PMC2453667. doi:10.2337/dc08-s272
10. Wolk R, Shamsuzzaman AS, Somers VK. Obesity, sleep apnea, and hypertension. Hypertension. 2003;42(6):1067–1074. PMID: 14610096. doi:10.1161/01.HYP.0000101686.98973.A3
11. Khanna D, Welch BS, Rehman A. Pathophysiology of Obesity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022. PMID: 34283442.
12. Saito H, Nishimura M, Shibuya E, et al. Tissue hypoxia in sleep apnea syndrome assessed by uric acid and adenosine. Chest. 2002;122(5):1686–1694. PMID: 12426272. doi:10.1378/chest.122.5.1686
13. Singh JA, Cleveland JD. Gout and the risk of incident obstructive sleep apnea in adults 65 years or older: an observational study. J Clin Sleep Med. 2018;14(9):1521–1527. PMID: 30176977; PMCID: PMC6134232. doi:10.5664/jcsm.7328
14. Hira HS, Shukla A, Kaur A, Kapoor S. Serum uric acid and lactate levels among patients with obstructive sleep apnea syndrome: which is a better marker of hypoxemia? Ann Saudi Med. 2012;32(1):37–42. PMID: 22156638; PMCID: PMC6087645. doi:10.5144/0256-4947.2012.37
15. Bouloukaki I, Mermigkis C, Tzanakis N, et al. Evaluation of inflammatory markers in a large sample of obstructive sleep apnea patients without comorbidities. Mediators Inflamm. 2017;2017:4573756. PMID: 28831208; PMCID: PMC5555019. doi:10.1155/2017/4573756
16. Hirotsu C, Tufik S, Guindalini C, Mazzotti DR, Bittencourt LR, Andersen ML. Association between uric acid levels and obstructive sleep apnea syndrome in a large epidemiological sample. PLoS One. 2013;8(6):e66891. PMID: 23826169; PMCID: PMC3691311. doi:10.1371/journal.pone.0066891
17. American Diabetes Association. Diagnosis and classification of diabetes mellitus, Diabetes Care. 2013;36(Suppl 1):S67–74. PMID: 23264425; PMCID: PMC3537273. doi:10.2337/dc13-S067
18. Qaseem A, Holty JE, Owens DK, Dallas P, Starkey M, Shekelle P. Clinical guidelines committee of the American college of physicians. Management of obstructive sleep apnea in adults: a clinical practice guideline from the American college of physicians. Ann Intern Med. 2013;159(7):471–483. PMID: 24061345. doi:10.7326/0003-4819-159-7-201310010-00704
19. Sleep Breathing Disorder Group. Respiratory disease branch of Chinese medical association. Guideline for the diagnosis and treatment of obstructive sleep apnea-hypopnea syndrome (2011). Chin J Tuberc Respir Dis. 2012;35(1):9–12. doi:10.3760/cma.j.issn.1001-0939.2012.01.007
20. Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes Mellitus. 2021;13(4):317–411. doi:10.3760/cma.j.cn115791-20210221-00095
21. Chinese Society of Endocrinology, Chinese Medical Association. Guideline for the diagnosis and management of hyperuricemia and gout in China (2019). Chin J Endocrinol Metab. 2020;36(1):1–13. doi:10.3760/cma.j.issn.1000-6699.2020.01.001
22. Storgaard H, Mortensen B, Almdal T, Laub M, Tarnow L. At least one in three people with Type 2 diabetes mellitus referred to a diabetes centre has symptomatic obstructive sleep apnoea. Diabet Med. 2014;31(11):1460–1467. PMID: 24766227. doi:10.1111/dme.12477
23. Martínez Cerón E, Casitas Mateos R, García-Río F. Sleep apnea-hypopnea syndrome and type 2 diabetes. A reciprocal relationship? Arch Bronconeumol. 2015. 51(3):128–139. English, Spanish. PMID: 25145320. doi:10.1016/j.arbres.2014.06.017
24. Foster GD, Sanders MH, Millman R, et al.; Sleep AHEAD Research Group. Obstructive sleep apnea among obese patients with type 2 diabetes. Diabetes Care. 2009;32(6):1017–1019. PMID: 19279303; PMCID: PMC2681024. doi:10.2337/dc08-1776
25. Einhorn D, Stewart DA, Erman MK, Gordon N, Philis-Tsimikas A, Casal E. Prevalence of sleep apnea in a population of adults with type 2 diabetes mellitus. Endocr Pract. 2007;13(4):355–362. PMID: 17669711. doi:10.4158/EP.13.4.355
26. Resnick HE, Redline S, Shahar E, et al. Sleep heart health study. Diabetes and sleep disturbances: findings from the sleep heart health study. Diabetes Care. 2003;26(3):702–709. PMID: 12610025. doi:10.2337/diacare.26.3.702
27. Tahrani AA. Obstructive sleep apnoea in diabetes: does it matter? Diab Vasc Dis Res. 2017;14(5):454–462. PMID: 28610436. doi:10.1177/1479164117714397
28. McNicholas WT. Diagnosis of obstructive sleep apnea in adults. Proc Am Thorac Soc. 2008;5(2):154–160. PMID: 18250207. doi:10.1513/pats.200708-118MG
29. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504. PMID: 28162150; PMCID: PMC5337595. doi:10.5664/jcsm.6506
30. Gottlieb DJ, Punjabi NM. Diagnosis and management of obstructive sleep apnea: a review. JAMA. 2020;323(14):1389–1400. PMID: 32286648. doi:10.1001/jama.2020.3514
31. Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47–112. PMID: 20086074; PMCID: PMC3970937. doi:10.1152/physrev.00043.2008
32. Brennick MJ, Pack AI, Ko K, et al. Altered upper airway and soft tissue structures in the New Zealand Obese mouse. Am J Respir Crit Care Med. 2009;179(2):158–169. PMID: 18996996; PMCID: PMC2633061. doi:10.1164/rccm.200809-1435OC
33. Nino G, Gutierrez MJ, Ravindra A, Nino CL, Rodriguez-Martinez CE. Abdominal adiposity correlates with adenotonsillectomy outcome in obese adolescents with severe obstructive sleep apnea. Pulm Med. 2012;2012:351037. PMID: 23251797; PMCID: PMC3518792. doi:10.1155/2012/351037
34. Isono S. Obesity and obstructive sleep apnoea: mechanisms for increased collapsibility of the passive pharyngeal airway. Respirology. 2012;17(1):32–42. PMID: 22023094. doi:10.1111/j.1440-1843.2011.02093.x
35. Vgontzas AN, Papanicolaou DA, Bixler EO, et al. Sleep apnea and daytime sleepiness and fatigue: relation to visceral obesity, insulin resistance, and hypercytokinemia. J Clin Endocrinol Metab. 2000;85(3):1151–1158. PMID: 10720054. doi:10.1210/jcem.85.3.6484
36. Ip MS, Lam B, Ng MM, Lam WK, Tsang KW, Lam KS. Obstructive sleep apnea is independently associated with insulin resistance. Am J Respir Crit Care Med. 2002;165(5):670–676. PMID: 11874812. doi:10.1164/ajrccm.165.5.2103001
37. Lv Q, Meng XF, He FF, et al. High serum uric acid and increased risk of type 2 diabetes: a systemic review and meta-analysis of prospective cohort studies. PLoS One. 2013;8(2):e56864. PMID: 23437258; PMCID: PMC3577701. doi:10.1371/journal.pone.0056864
38. Drager LF, Lopes HF, Maki-Nunes C, et al. The impact of obstructive sleep apnea on metabolic and inflammatory markers in consecutive patients with metabolic syndrome. PLoS One. 2010;5(8):e12065. PMID: 20711453; PMCID: PMC2920316. doi:10.1371/journal.pone.0012065
39. Verhulst SL, Van Hoeck K, Schrauwen N, et al. Sleep-disordered breathing and uric acid in overweight and obese children and adolescents. Chest. 2007;132(1):76–80. PMID: 17505038. doi:10.1378/chest.06-2930
40. Pływaczewski R, Bednarek M, Jonczak L, Górecka D, Sliwińiski P. Hiperurykemia u meiczyzn chorych na obturacyjny bezdech senny (obs) [Hyperuricaemia in males with obstructive sleep apnoea (osa)]. Pneumonol Alergol Pol. 2005;73(3):254–259. Polish. PMID: 16989162.
41. Ruiz García A, Sánchez Armengol A, Luque Crespo E, et al. Valores de ácido úrico en sangre en pacientes con trastornos respiratorios del sueño [Blood uric acid levels in patients with sleep-disordered breathing]. Arch Bronconeumol. 2006. 42(10):492–500. Spanish. PMID: 17067515. doi:10.1016/s1579-2129(06)60575-2
42. Shi T, Min M, Sun C, et al. A meta-analysis of the association between gout, serum uric acid level, and obstructive sleep apnea. Sleep Breath. 2019;23(4):1047–1057. PMID: 30903565. doi:10.1007/s11325-019-01827-1
43. Chen Q, Lin G, Chen L, et al. Does continuous positive airway pressure therapy in patients with obstructive sleep apnea improves uric acid? A meta-analysis. Oxid Med Cell Longev. 2019;2019:4584936. PMID: 31636804; PMCID: PMC6766132. doi:10.1155/2019/4584936
44. Bartziokas K, Papaioannou AI, Haniotou A, Nena E, Kostikas K, Steiropoulos P. Serum uric acid and arterial lactate levels in patients with obstructive sleep apnea syndrome: the effect of CPAP treatment. Postgrad Med. 2021;133(5):518–524. PMID: 33395325. doi:10.1080/00325481.2020.1866891
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.